
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Lateral ankle sprains are a commonly incurred injury in sports. They have a high recurrence rate and can lead to the development of persistent injury associated symptoms. We performed a quantitative synthesis of published case reports documenting the kinematics of acute lateral ankle sprains and episodes of ‘giving-way’ of the ankle joint to provide a comprehensive description of the mechanisms. A systematic literature search was conducted to screen records within MEDLINE® and EMBASE®. Additional strategies included manual search of specific journals, as well as contacting researchers in relevant communities to retrieve unpublished data. Twenty-four cases were included in the quantitative synthesis, 11 from individual case reports and 13 from four separate case series. Two authors independently reviewed all the articles and extracted ankle joint kinematic data. Excessive ankle inversion was the most pronounced kinematic pattern observed across all included cases, with a mean peak inversion angle of 67.5° (range 2.0 to 142) and a mean peak inversion velocity of 974°/s (range 468 to 1752). This was followed by internal rotation and plantar flexion, respectively. A homogeneous linear function revealed a mean inversion velocity across all cases of 337°/s (range 117 to 1400; R2 = 0.78; p < 0.0001).
Introduction
Lateral ankle sprains are the most common injury incurred by individuals who participate in sports (Fong et al., Citation2007). Although often considered as innocuous injuries (Doherty et al., Citation2014), lateral ankle sprains have a high recurrence rate, are often compounded by the development of persistent injury-associated symptoms, and ultimately result in high annual health care costs (Gribble et al., Citation2016). It is thus not surprising that the International Ankle Consortium (IAC) has highlighted the prevention of lateral ankle sprains as one of its eight research priorities (Gribble et al., Citation2016).
The ability to optimise injury prevention/risk-reduction programmes may be limited by an incomplete understanding of the mechanisms of injuries (Delahunt & Remus, Citation2019). To this end, Bahr and Krosshaug (Citation2005) developed a comprehensive injury-causation model. In this model, they propose that quantification of the biomechanical properties of the mechanisms of injuries can be used to guide the development of injury prevention/risk-reduction initiatives and the design of protective equipment (Bahr & Krosshaug, Citation2005). With recent advances in sports biomechanics techniques, numerous approaches have emerged to quantify the mechanisms of common sports-related injuries (Krosshaug et al., Citation2005).
It is obvious that the observation of real injury incidents is critically important for the understanding of how injuries occur (Krosshaug et al., Citation2005). However, it remains highly unethical and practically impossible to perform experiments during which test participants are purposefully injured (Fong et al., Citation2009). Lateral ankle sprains are, however, particularly common in indoor sports settings (Doherty et al., Citation2014; Fong et al., Citation2007; Vuurberg et al., Citation2018), where this injury most often occurs without any distorting object between the injured foot and floor (Herzog et al., Citation2019). Therefore, it is only natural that this common injury has occasionally occurred in biomechanical laboratories with calibrated motion analysis equipment (Fong et al., Citation2009; Gehring et al., Citation2013; Kristianslund et al., Citation2011; Terada & Gribble, Citation2015). While some ankle distortions lead to injury of the lateral ankle ligaments, others do not. These latter incidents have also been observed during laboratory experiments (Kosik et al., Citation2019; Y. Li et al., Citation2019; Remus et al., Citation2018). Some of these have, in recent times, been referred to as episodes of ‘giving-way’ of the ankle joint and with a mechanism that seemingly closely resembles that of an acute lateral ankle sprain (Gribble et al., Citation2014). These have more specifically been defined as: ‘the regular occurrence of uncontrolled and unpredictable episodes of excessive inversion of the rear foot (usually experienced during initial contact during walking or running), which do not result in an acute lateral ankle sprain’ (Delahunt et al., Citation2010).
Far more injury incidents are naturally captured (unintentionally) during televised sports events and competitions than during controlled laboratory experiments. Recent technologies have enabled the quantitative analysis of injuries captured during televised sports events. This is achieved through a Model-Based Image-Matching (MBIM) forensic motion analysis technique that allows for 3-dimensional kinematic analyses of human motion from uncalibrated video sequences (Krosshaug & Bahr, Citation2005). Although originally used to analyse mechanisms of anterior cruciate ligament (ACL) injuries (Krosshaug et al., Citation2007), this technique has since been used to quantify the mechanisms of televised lateral ankle sprain injury cases (Fong et al., Citation2012; Mok et al., Citation2011a).
Until now, no study has consolidated the kinematic outcomes of published quantitative case reports of lateral ankle sprains and episodes of ‘giving-way’. As a result, the aim of this review was to identify and quantitatively synthesise published case reports documenting the kinematics of acute lateral ankle twists resulting in sprains and episodes of ‘giving-way’ of the ankle joint.
Materials and methods
The impetus for this review was developed following a scientific session (‘Quantitative analysis of the mechanism of ankle inversion sprain injury’), which was presented at the 2019 International Ankle Symposium (Biennial meeting of the International Ankle Consortium) on 4 October 2019 in Amsterdam, The Netherlands. In this symposium, authors of some previously published quantitative case reports presented their cases and analyses. Some of these cases described the kinematics of acute lateral ankle sprains, while others reported upon the kinematics of ‘giving-way’ episodes of the ankle joint. We hope that this state-of-the-art review will enhance understandings of the mechanisms of acute lateral ankle sprains and ‘giving-way’ episodes of the ankle joint. This information is integral to the development of efficacious injury prevention/risk-reduction initiatives and the design of protective equipment.
Literature search
The authorship group already had a good knowledge of the existing literature within this area, by virtue of being the authors of most of the published case reports. However, to reduce the risk of missing other published cases, a literature search was conducted. EMBASE and OVID search tools were used to systematically screen records within MEDLINE® and EMBASE® including the following possible status besides MEDLINE and EMBASE: Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily and Versions(R) 1946 to present, with a final search being conducted on 7 October 2021 using the following search string in MEDLINE: (ankle[Title] AND sprain[Title] OR giving-way[Title]) AND (case[Title] OR cases[Title] OR episode[Title] OR episodes[Title] OR accident[Title] OR accidents[Title] OR accidental[Title] OR recorded[Title] OR captured[Title] OR televised[Title]), and (ankle:ti AND sprain:ti OR ‘giving way’:ti) AND (case:ti OR cases:ti OR episode:ti OR episodes:ti OR accident:ti OR accidents:ti OR accidental:ti OR recorded:ti OR captured:ti OR televised:ti) in EMBASE. Additional non-systematic searches were conducted in Google Scholar and other general search engines. Unpublished laboratory-recorded lateral ankle sprains, twists, and episodes of giving-way were invited for inclusion in this review by informally asking around in scientific communities.
Criteria for article and case selection
A priori selection criteria were determined for limiting articles to quantitative reports of lateral ankle distortions, whether resulting in injury or not, as well as cases of ‘giving-way’ of the ankle joint. Any studies describing more than one lateral ankle twist, or ‘giving-way’ episode had their episodes included as separate cases.
Article assessment
Two authors (FGL and YW) independently reviewed all articles to determine eligibility for inclusion in this review. Same two authors extracted all information from the included cases, such as individual’s information and anthropometrics, event scenario, event severity, as well as all a priori agreed upon quantitative kinematic and kinetic outcomes, including initial ankle joint angles, peak ankle joint angles, peak ankle joint angular velocities, average ankle joint angular velocities, and ankle joint moments (Supplementary Appendix 2). All outcomes were determined by consensus between the two reviewers.
Data analysis and statistics
Individuals’ characteristics in the form of age, height, and body mass were retrieved directly from the case reports. In cases where this information has not been provided in the published article, we retrieved this information via the individuals’ respective sports association/federation (Association of Tennis Professionals, Women’s Tennis Association, Badminton World Federation, and International Association of Athletics Federations).
Event scenario was retrieved directly from the case reports or from re-watching available videos (Supplementary Video 1). In some cases where the severity of a televised event was not available in the case reports, this was retrieved via Google Search, as well as by re-watching the game/competition, to assess whether they resumed their activity or were forced to withdraw. Additionally, the location of contact between shoe and floor at initial contact was retrieved via visual inspection whenever possible.
Ankle joint kinematics and kinetics (when available) were reported following the recommendations of the International Society of Biomechanics (Wu et al., Citation2002), and retrieved directly from the case reports. In some reports, these outcomes were only graphed but not reported in exact numbers. Here, the data points of interest were estimated digitally by using a y-axis-calibrated ruler in Kinovea (v. 0.9.5, www.kinovea.org).
Descriptive statistics were conducted in Microsoft Excel and used to summarise the quantitative outcomes from the included case reports. Means were used to describe the measures of central tendency, while the variability between the cases was described using standard deviation (SD) (Barde & Barde, Citation2012). Linear regression analyses were conducted on the total change in joint displacement (∆θ), and time elapsed from initial contact to peak displacement (i.e., average joint angular velocity, as calculated via EquationEquation 1(1)
(1) ), using Microsoft Excel Analysis ToolPak (Microsoft Corporation, Washington, USA).
Results
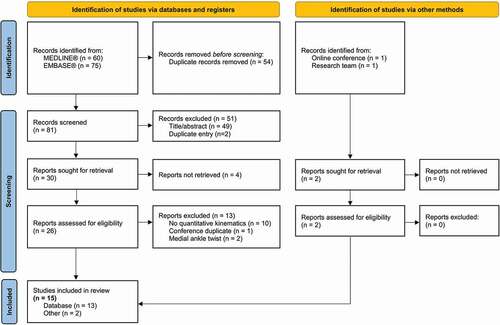
The systematic search process (Supplementary Appendix 1) produced a total of 81 potentially eligible articles after duplicates were removed (). Of these, 51 were directly excluded in the title and abstract screening, while additional four reports could not be retrieved. Of the 26 reports assessed for eligibility, 13 were excluded: Ten reports did not contain kinematic or kinetic outcomes of the described event, two for being medial ankle sprain analyses (X. Li et al., Citation2016; Wade et al., Citation2018), and one for being a conference abstract of an included case report (Chin et al., Citation2020). The 13 included studies were accompanied by two additional reports retrieved via other methods: One case from within the authorship group (Lysdal et al., Citation2018), and one case presented at the 38th Conference of the International Society of Biomechanics in Sports, and retrieved from the conference proceedings (Trejo Ramírez et al., Citation2020).
Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Individuals’ characteristics
The 15 included studies produced at total of 24 separate quantitative case reports incurred by 24 individuals (). Most of the incidents were sustained by men (63%). Fourteen were elite athletes, and 10 recreationally active individuals. The mean age at the time of the incidents was 24 years (SD 4.4; range 18 to 33). The mean height and body mass of the individuals were 1.81 m (SD 0.13; range 1.60 to 2.11), and 76.0 kg (SD 17.0; range 57.0 to 111.1), respectively.
Table 1. Chronological list of studies, case numbers and individual’s characteristics
Chronological case description
The first quantitative case report of a lateral ankle twist was published in 2009. Here, a recreationally active man, with no previous ankle sprain history, accidentally sustained a mild lateral ankle sprain during a laboratory test while performing a 180-degree pivot turn (Supplementary Table 1) (Fong et al., Citation2009).
Cases 2 and 3 occurred during the Olympic Games in Beijing in 2008 and were caught on camera during competition, and had since been quantified using MBIM analysis. The first of these incidents was a lateral ankle sprain sustained during the High Jump competition in the final take-off step. The second case was a lateral ankle sprain injury sustained in Field Hockey by stepping onto the opponent’s foot (after initial heel contact on the turf) while fighting for the ball. Both athletes were forced to withdraw from their competition (Mok et al., Citation2011a).
Case 4 was a laboratory accident in which a healthy (no previous ankle injury) elite female handball player sustained a lateral ankle sprain while performing a 40-degree sidestep cut (Kristianslund et al., Citation2011).
Cases 5–9 were published as a quantitative case series study using MBIM analysis on five lateral ankle sprain injuries that were captured on TV during professional tennis competitions between 1995 and 2010 (Fong et al., Citation2012). All five televised tennis injuries occurred in singles matches, by two men and three women. Three of the incidents forced the affected player to retire from the match, while two were able to continue playing, of which one of them won the match. Three injuries were sustained on an outdoor clay surface, of which two cases (#6 and #8) occurred after a sudden stop while sliding, and one during a lateral shuffle after a backhand return (#7). The remaining two injuries were sustained on indoor carpet and hardcourt surfaces, both in the context of a backhand return, one while running to the short backhand corner (#5), the other during a lateral shuffle landing (#9) (Supplementary Table 1).
Case 10 was an accidental mild lateral ankle sprain sustained in the laboratory, by an individual with recurring ankle problems, during a 180-degree pivot turn while testing different pairs of studded football boots on artificial grass (Gehring et al., Citation2013).
Case 11 was sustained in a biomechanics laboratory during a bilateral stop-jump task by an individual with chronic ankle instability (Terada & Gribble, Citation2015). This incident resulted in a mild lateral ankle sprain injury and stopped the testing (Supplementary Table 1).
Case 12–15 all occurred during Basketball match play in the National Basketball Association (NBA) and quantified using MBIM. All four incidents occurred following a step onto an opponent’s foot. Three of the incidents forced the player to withdraw from the match, while one could continue playing (Panagiotakis et al., Citation2017).
Case 16 was a mild lateral ankle sprain that occurred in a biomechanics laboratory during a 40-degree sidestep cut (Lysdal et al., Citation2018). The incident occurred during the only control condition, while the participant was testing Spraino, an ankle sprain preventive device (Lysdal et al., Citation2021).
The next four cases (17–20) all occurred during laboratory testing, and all incidents were classified as episodes of ‘giving-way’ sustained by four individuals diagnosed with chronic ankle instability (CAI). Here, none of the participants suffered any injury and continued testing.
In Case 17, the incident occurred during a 90-degree side-cut in the run-to-shuffle transition in the agility t-test (Remus et al., Citation2018).
Case 18 occurred during a single-leg landing task (Kosik et al., Citation2019).
Case 19 and 20 both occurred in the same laboratory as part of the same study while performing drop-landing tasks onto a 25-degree-tilted force platform (Y. Li et al., Citation2019).
Case 21 was an accidental ankle twist sustained in a laboratory during a 90-degree cut while testing stud configurations for football boots. The participant was uninjured and testing continued (Trejo Ramírez et al., Citation2020).
Case 22 was a laboratory accident where a female elite ice hockey player twisted her ankle during a 180-degree pivot turn. There was only minor local soreness associated with this incident and full (unrestricted) sports participation the following day (Chin et al., Citation2021).
Case 23 was an MBIM analysis of a severe lateral ankle sprain injury that occurred during the 2012 Thomas Cup in badminton, while the player was performing a lateral backwards step towards the long forehand corner (Fong et al., Citation2021).
Case 24 was a ‘giving-way’ episode recorded in the laboratory, while a participant with CAI was walking in unstable footwear (Takeda et al., Citation2021).
Kinematics
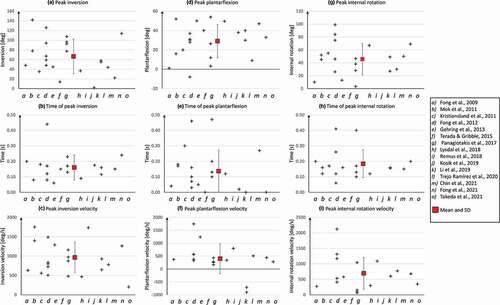
Twelve cases occurred during dynamic movement analyses in a laboratory setting, of which 10 cases were recorded using calibrated marker-based motion capture systems, and two by inertial measurement units. The other 12 cases were kinematically quantified using MBIM analysis. Twenty-two cases reported plantarflexion and inversion angles, of which 20 cases also reported on internal rotation angle (). The remaining two cases recorded using inertial measurement units only reported joint velocities (Remus et al., Citation2018; Takeda et al., Citation2021).
Figure 2. Peak ankle joint angle (a, d, g), time to peak ankle joint angle (b, e, h), and peak ankle joint velocity (c, f, i) of the case reports with respect to each study. Adapted and updated based on (Fong et al., Citation2021).
Initial contact ankle joint kinematics
The 22 cases reporting ankle inversion and plantarflexion angles had an average initial contact inversion angle of 8.2 degrees (SD 10.7; range −17.0 to 30.0) and initial plantarflexion angle of 9.3 degrees (SD 21.1; range −41.0 to 41.0) (). The average initial internal rotation angle from the 20 cases with this information was 6.5 degrees (SD 13.9; range −15.5 to 40.0) ().
Table 2. Summarising table of initial contact ankle joint angles and shoe-surface contact location
Peak ankle joint kinematics
The 22 cases reporting ankle inversion angle reached an average peak inversion of 66.5 degrees (SD 36.0; range 2.0 to 142.0) (); )) after 0.20 seconds (SD 0.08; range 0.06 to 0.44) following initial contact (); )). The 21 cases with information on inversion velocity reported an average peak inversion velocity of 928 deg/s (SD 418; range 204 to 1752) (); )).
Table 3. Summarising table of peak ankle joint kinematics
The 22 cases reporting plantarflexion angle reached an average peak plantarflexion of 29.1 degrees (SD 17.2; range −8.0 to 52.0) (); )) after 0.10 seconds (SD 0.14; range 0.00 to 0.47) following initial contact (); )). The 18 cases with information on plantarflexion velocity reported an average peak plantarflexion velocity of 394 deg/s (SD 567; range −900 to 1748) (); )).
The 22 cases reporting ankle internal rotation angle reached an average peak internal rotation of 45.7 degrees (SD 24.3; range 3.4 to 99.0) (); )) after 0.20 seconds (SD 0.09; range 0.06 to 0.41) following initial contact (); )). The 21 cases with information on internal rotation velocity reported an average peak internal rotation velocity of 674 deg/s (SD 504; range 66 to 2124).
Case correlation
Linear regression analyses on total inversion motion and time from initial contact until the occurrence of peak inversion (EquationEq. 1(1)
(1) ), revealed an average inversion velocity of 336.8 deg/s with a correlation coefficient (R-squared) of 0.78 (p < 0.001), an average plantar flexion velocity of 106.7 deg/s (R-squared = 0.60, p < 0.001), and an average internal rotation velocity of 179.9 deg/s (R-squared = 0.65, p < 0.001) ().
Figure 3. Scatterplot of total ankle joint displacement angle (y-axis) and time to peak displacement (x-axis). The homogenous linear function illustrates the correlation between total joint displacement and time from initial contact to peak joint displacement.
The ‘two peaks’ of the lateral ankle sprain
Four laboratory cases (Case 1, 4, 10 and 16; Fong et al., Citation2009; Gehring et al., Citation2013; Kristianslund et al., Citation2011; Lysdal et al., Citation2018), and one match case from tennis (Case 6; Fong et al., Citation2012), reported two distinct peaks in ankle inversion angle (). The first peak occurred between 30 and 80 milliseconds after foot strike, and the second peak between 100 and 200 milliseconds (). When looking at inversion velocity, this prominent two-peak process in ankle joint inversion is also seen in Case 21 (Trejo Ramírez et al., Citation2020) and Case 23 (Fong et al., Citation2021).
Figure 4. The two phases of the non-contact ankle inversion twist.
A two-step process was also apparent in the internal rotation of the ankle joint with seven separate cases (Case 2, 4, 7, 9 15, 16, 21) reporting two distinct peaks in the internal rotation angle (Fong et al., Citation2009; Fong et al., Citation2012; Kristianslund et al., Citation2011; Lysdal et al., Citation2018; Mok et al., Citation2011a; Panagiotakis et al., Citation2017; Trejo Ramírez et al., Citation2020). When including internal rotation moment, this two-peak process was evident in eight cases with the addition of Case 10 (Gehring et al., Citation2013).
The opposing motions of the ‘giving-way’ episode
Five cases (Case 17, 18, 19, 20, 24) of giving-way of the ankle joint reported distinct counteracting movements during the episodes (Kosik et al., Citation2019; Y. Li et al., Citation2019; Remus et al., Citation2018; Takeda et al., Citation2021). In Case 17, 18 and 24, the inversion phase of the ankle joint was followed up by a faster and more significant correcting eversion movement of the ankle (Kosik et al., Citation2019; Remus et al., Citation2018; Takeda et al., Citation2021). In the two drop-jump cases (Case 19 and 20), the internal rotation was corrected to be an excessive external rotation movement (Y. Li et al., Citation2019).
Kinetics
Five studies and six cases reported kinetics of the ankle joint during the stance of the events (). The inversion moment ranged from −95 to −85 Nm in the two drop-jump cases to 175 Nm in case 10, which also presented the highest internal rotation moment of 220 Nm (). The two cases (4 and 10) with the highest inversion and internal rotation moments resulted in time-loss injury for the affected participants (Supplementary Table 1).
Table 4. Summarising table of peak ankle joint kinetics
Compared to the cases' respective control trials, Case 4 reported similar initial peak in plantarflexion moment but a lower second peak and pronounced inversion and internal rotation moments—instead of eversion and external rotation moments observed in control trials (Kristianslund et al., Citation2011). Case 10 reported a plantarflexion moment instead of dorsiflexion moment in control trials, and much higher inversion and internal rotation moments (Gehring et al., Citation2013). Case 18 reported higher plantarflexion and inversion moments than control trials (Kosik et al., Citation2019). Case 19 reported a lower plantarflexion moment compared to control trials, similar eversion moment, and similar external rotation moment, albeit shifted following a brief period of less external rotation moment in the early landing phase (Y. Li et al., Citation2019). Case 20 reported higher plantarflexion, eversion and external rotation moments compared to control trials, with a brief period of less external rotation moment in the early landing phase (Y. Li et al., Citation2019). Case 22 reported higher dorsiflexion moment, but lower inversion and internal rotation moments than in control trials (Chin et al., Citation2021).
Discussion and implications
Our review quantitatively synthesised published case reports documenting the kinematics of acute lateral ankle sprains and episodes of ‘giving-way’ of the ankle joint; and as such, provides a comprehensive description of the most commonly reported mechanisms of acute lateral ankle sprain injuries and ‘giving-way’ episodes of the ankle joint.
Classification of quantitative events
Half of the cases retrieved in this review occurred during laboratory testing. The other half were game and competition events recorded on TV. Apart from this distinctive parameter, it can be difficult to distinguish between cases, as evident in Case 22, being first published as a (non-time-loss) mild lateral ankle sprain injury in a conference abstract (Chin et al., Citation2020), and later as a ‘giving-way’ episode in the published article (Chin et al., Citation2021). It could be argued that this case should simply have been labelled as a ‘non-injury lateral ankle distortion’. This was the only quantitative ‘giving-way’ episode reported in a participant without CAI. Coupled with the fact that this episode did not exhibit the excessive ‘rescue’ eversion/external rotation pattern found in previous ‘giving-way’ episodes (Kosik et al., Citation2019; Y. Li et al., Citation2019; Remus et al., Citation2018). Particularly ‘giving-way’ is a characteristic feature reported by individuals with CAI (Delahunt et al., Citation2010). It was also the only ‘giving-way’ case that did provoke some level of localised soreness (Supplementary Table 1).
Based on the non-negligible discrepancy between some cases retrieved for this review, we consequently suggest the following four-way classification of quantitative events (), where one simply has to ask two questions: First, in what setting did the injury occur? A) laboratory/test event, or B) competition/game event. Secondly, did the event result in injury? 1) A musculoskeletal injury with some level of time-loss from activity/test, or 2) No injury or an episode of ‘giving-way’. This could potentially help make future comparisons between case reports easier, as we expect considerably more quantitative forensic analyses to carried out in the coming years, while one cannot rule out the occasional laboratory incident.
Table 5. Case distinction
In this study, 14 out of 24 cases resulted in immediate restriction from further testing or sports participation. This was the case for 5 out of 12 events that occurred in a laboratory setting (, A1), while seven of the laboratory events did not result in any time-loss injury or were considered episodes of ‘giving-way’ (, A2). Nine of the game/competition events resulted in an immediate time-loss from sports participation (, B1), while three cases did not cause any time-loss (, B2).
All cases, apart from one ‘giving-way’ episode (Takeda et al., Citation2021), exceeded the previously proposed 300 degrees per second-threshold in inversion velocity for detection of ankle sprain motion (Chu et al., Citation2010). The five laboratory events that yielded time-loss from activity were by far and large considered mild (i.e., Jackson Grade I). In contrast, time lost from sports participation was the direct outcome in 9 of the 12 competitive cases that also displayed significantly higher inversion and internal rotation velocities, and with some of these events resulting in substantial time-loss. This difference is, however, likely explained by the less vigorous intensity also observed in training compared to match play (Dawson et al., Citation2004; Hartwig et al., Citation2011) while also acknowledging that the competitive events analysed are more likely to be a worst-case-scenario.
Overall, the difference in clinical outcome reported among the different cases might be explained by different structural preconditions between the 24 individuals. Differences in laxity and joint stiffness may well contribute to the fact that the same kinematics might result in injury to one individual and no harm to another.
Kinematics
An inverted position of the ankle joint at initial contact is considered a particularly vulnerable position (Wright et al., Citation2000), which has been identified as a key characteristic feature of lateral ankle sprain injury mechanisms (Delahunt & Remus, Citation2019). Initial ankle inversion was indeed present among the majority of the 24 reported cases, and nine cases even reported an initial ankle inversion of ≥10 degrees at first ground contact (). A recent study compared similar non-injury movements, performed by that same tennis player of Case 8, to the injury she sustained, and found that the inverted foot position was an inciting moment for her ankle sprain injury (Mok et al., Citation2021).
It is, however, also worth noting that multiple cases in this review occurred despite the ankle joint being in an initially everted position (Chin et al., Citation2021; Fong et al., Citation2021; Gehring et al., Citation2013; Kosik et al., Citation2019; Terada & Gribble, Citation2015). This could suggest that the very first instance of initial contact might not be as critical as the first few milliseconds that follow immediately after initial ground contact.
Multiple cases exhibited two peaks in inversion and internal rotation angles, intertwined by what appears to be an unsuccessful/incomplete joint realignment (Fong et al., Citation2009; Gehring et al., Citation2013; Kristianslund et al., Citation2011; Lysdal et al., Citation2018). This two-peak process was naturally more prominent when also looking at joint velocities (Fong et al., Citation2021; Trejo Ramírez et al., Citation2020), by the virtue of being an integral of the positional data. In some of these cases it seemed that the injury was initiated close to (or even before) initial contact, where the athlete probably senses the problem and tries to unload. However, the injury progression is already past a point-of-no-return, and a further load/angular excursion develops (Kristianslund et al., Citation2011).
The cases with two peaks in the inversion angle had a 32–50% lower inversion velocity than the average of all cases combined, apart from Case 10 with a higher inversion velocity. This case, however, also saw its first peak exceed the excursion of the second peak (Gehring et al., Citation2013).
An early unloading is probably less likely to occur during the five direct contact injury cases identified. However, in the remaining six televised cases, it remains possible that the injury sequences simply happened too fast for the cameras to record this early unloading mechanism, whereby they were smoothed out in the interpolation between data points.
The retrieved cases suggest that the lateral ankle sprain can probably occur at any time during the phases of stance. Although an incident might be most likely to occur during absorption (Medina McKeon & Hoch, Citation2019) (i.e., Case 23), it also seems to occur during propulsion (i.e., Case 1), as well as during the transition in-between (i.e., Case 2) (Supplementary Video 1). This highlights a potentially informative kinematic classification of events, where the use of whole-body kinematics could be a helpful tool to define these phases with high precision over the course of the injury.
A high degree of plantar flexion at initial contact was previously branded a risk factor for lateral ankle sprain injuries, due to the increased moment about the subtalar joint axis (Wright et al., Citation2000), as well as the proposed mechanical ‘locking’ of the subtalar joint when the foot is in dorsiflexion, while loaded on the forefoot due to the conical shape of the talus (Hamel et al., Citation2004). This fell well in line with what used to be a common understanding of lateral ankle sprain injury mechanisms, which was described as a combination of excessive inversion and plantar flexion (Andersen et al., Citation2004). More recent studies, however, now confirm that inversion of the ankle joint can proceed irrespective of sagittal plane motion (Fong et al., Citation2012), and that plantar flexion is not required for a lateral ankle sprain injury to occur (Fong et al., Citation2009; Kristianslund et al., Citation2011; Mok et al., Citation2011a; Skazalski et al., Citation2018).
However, while plantar flexion might not play a crucial role in the occurrence of a lateral ankle sprain, cadaver and simulation studies suggest that plantar flexion has a direct influence on the loading of the specific structures that comprise the lateral ligament complex (Bennett, Citation1994). Inversion alone only results in tissue damage to the calcaneofibular ligament. Inversion in combination with internal rotation strains both the calcaneofibular ligament and anterior talofibular ligament (Panagiotakis et al., Citation2017). However, when the foot is inverted while in plantarflexion, the anterior talofibular ligament is typically the first to be injured (Bennett, Citation1994; Khor & Tan, Citation2013; Panagiotakis et al., Citation2017). Inversion alone strains ATFL to 10% and CFL to 12%. Adding plantarflexion and/or internal rotation further increased the strain to 16–20% (Wei et al., Citation2014).
The homogenous linear function that we applied to the kinematic parameters supports this notion that plantarflexion is less essential in lateral ankle sprain injuries. With a larger variance in pattern, and low correlation with the time at which plantarflexion occurred in the excursion sequence. In some of the included injury cases, further plantar flexion never occurred after initial contact, while in other cases, it preceded or exceeded the primary injury mechanism (Fong et al., Citation2012). Internal rotation seemingly plays a greater role, while inversion of the ankle was the only joint movement exclusive to all quantitative cases. This was also reflected in the joint excursion velocities, with inversion velocity being 337°/s on average, followed by an internal rotation at 180°/s and plantarflexion 107°/s.
Unfortunately, we do not have ligament-specific injury information for these cases. Hence, we cannot confirm whether the differences in plantarflexion resulted in specific ligament injury patterns, compared to inversion and internal rotation.
Study limitations
This review is not without limitations. One of the major limitations is that, despite being the most common musculoskeletal injury, only 24 quantitative case reports of an ankle twist could be retrieved to this date, of which only 14 resulted in musculoskeletal injury.
We acknowledge the risk of potentially confounding results by consolidating the kinematic outcomes from both incidences of lateral ankle sprains and episodes of ‘giving-way’. The ‘giving-way’ episodes are, however, largely within the range of the sprain cases. It might still be beneficial to distinguish between case type, as the number of respective cases increase, i.e., by our proposed classification.
Half of the included case reports were subsequent quantitative analyses using MBIM software. This system has previously been validated but is known to be less accurate than a marker-based motion capture system (Mok et al., Citation2011b). However, when considering the very limited number of laboratory injuries, these analyses are essential for our understanding of the injury mechanism. Importantly, the difference between televised injuries and laboratory cases is much greater than the method error, so there is without doubt a real difference between incidents. Unfortunately, only five studies and six cases have reported ankle joint kinetics from laboratory incidents, and only two cases where the incident caused injury. Ankle joint kinetics is important for our understanding, and the lack of especially injury kinetics is a major limitation to an in-depth understanding of the injury mechanism.
Employing a homogenous linear function on total plantarflexion with respect to time before peak plantarflexion is also a major limitation, since this analysis does not take dorsiflexion into account. This would be exemplified in cases where maximum plantarflexion occurred at initial contact (i.e., a forefoot landing from a jump). Here, the foot naturally dorsiflexes during load acceptance, but this negative plantarflexion velocity would be presented as zero. This might distort the regression analysis and/or the potential importance of plantarflexion.
Finally, we did not conduct a formal risk of bias assessment (Boutron et al., Citation2021) of the individual case reports/series. This is not considered a major limitation of the present review, since all included studies are descriptive in nature, and thus do not consider the effect of an intervention. Instead, the transparent and chronological presentation of cases allows the reader to draw their own conclusions. We are, however, authors of most of the previous laboratory and televised incidents, and we acknowledge the obvious risk of selection bias in this review. In our effort towards minimising this risk, we adopted a systematic approach in both search strategy, data extraction and quantitative data analysis, as well as having two separate authors independently reviewing the articles, before finding a common ground.
Implications for practice and future research
Despite being a commonly incurred injury (Fong et al., Citation2007), documented/published cases of lateral ankle sprains sustained during controlled testing in biomechanical laboratories are rare. We should, however, of course not ‘expect’ or warrant more injury cases to occur during laboratory experiments, despite the invaluable information they might provide. However, the ever-increasing media coverage of sporting events (i.e., in the NBA), coupled with the use of multiple high-quality cameras with higher framerate currently used in the production of sports entertainment means the chance of capturing injury incidents and their inciting events remain greater than ever. This, coupled with advances in computer processing capabilities, allows for many more quantitative case reports of already captured lateral ankle sprains (e.g., via MBIM analysis). This would present a valuable tool to further enhance our understanding of the mechanism of sports injuries. Here, we specifically suggest that future quantitative analyses should also investigate the relationship between the centre of mass and the position of the foot around the event (i.e., was the foot directly under the centre of mass or located away?). Mapping the centre of mass position (and velocity) could open the opportunity to further explore the relationship of the entire kinetic chain to meet absorption demands in various high-risk movement tasks. A deeper understanding hereof could potentially help clinicians shape functional task environments for rehabilitation and prevention strategies (Gokeler et al., Citation2020).
We also welcome a deeper understanding of whether a correlation might exist between the degree of joint distortion, velocity, and the amount of structural damage (i.e., injury severity). Future forensic analyses should also assess whether the early unloading phase presented in this review is also detectable in high-intensity sprain situations during match play.
It is widely acknowledged in the literature that an incorrect foot position at touchdown is the highest risk factor for lateral ankle sprain injury (Delahunt & Remus, Citation2019). Some of this literature is, however, based on simulation studies (Wright et al., Citation2000), and multiple cases in this review demonstrate that injuries still occur despite a correct landing at initial foot strike. The importance of having a ‘correct’ joint position at initial contact in relation to the occurrence of injury should be further investigated. More research is therefore needed on actual competitive injury cases to investigate the role of foot positioning at initial contact on actual injury outcomes, as well as the protective role of having proper muscle activation and increased joint stiffness prior to landing.
Greater knee varus angles after landings have recently been demonstrated to increase the risk of non-contact lateral ankle sprains in a prospective cohort (Mineta et al., Citation2021). Future research should therefore target a deeper understanding of whole-body biomechanics, and proximal joint position, in relation to both injury and episodes of ‘giving-way’, and how this might deviate from non-injury trials.
Analysing the ankle sprain injury mechanism in relation to the type of sport, injury scenario and/or playing position should be the natural next step, especially when considering the large variety of injury mechanism (Andersen et al., Citation2004; Skazalski et al., Citation2018). This would increase the relevance and could possibly help tailor sport-specific preventive strategies.
At present, the outcomes of this review suggest that inversion is the most important movement of the ankle joint in relation to the injury mechanism, and present across all cases. This also highlights that injury prevention should most likely have a primary focus on preventing excessive inversion, compared to both internal rotation and plantar flexion. However, this ought to be interpreted with caution, due to the limited number of reported quantitative case reports.
Supplemental Material
Download Zip (104.5 KB)Supplemental Material
Download MS Word (21 KB)Supplemental Material
Download MP4 Video (139 MB)Disclosure statement
No authors have any financial interests to declare in relation to this study. The team of authors are, however, independently affiliated with most of the published case reports within the scope of this review, and our findings are thus subjected to confirmation bias and self-citation incentives.
ED is Co-Executive Director, and DTPF is an Executive Committee member of the International Ankle Consortium. DTPF is Editor-in-Chief of Sports Biomechanics and KMM is an Associate Editor of Sports Biomechanics.
Data availability statement
The authors are happy to share the data upon reasonable request.
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
References
- Andersen, T. E., Floerenes, T. W., Arnason, A., & Bahr, R. (2004). Video analysis of the mechanisms for ankle injuries in football. The American Journal of Sports Medicine, 32(1Suppl), 69S–79S. https://doi.org/https://doi.org/10.1177/0363546503262023
- Bahr, R., & Krosshaug, T. (2005). Understanding injury mechanisms: A key component of preventing injuries in sport. British Journal of Sports Medicine, 39(6), 324–329. https://doi.org/https://doi.org/10.1136/bjsm.2005.018341
- Barde, M. P., & Barde, P. J. (2012). What to use to express the variability of data: Standard deviation or standard error of mean? Perspectives in Clinical Research, 3(3), 113–116. https://doi.org/https://doi.org/10.4103/2229-3485.100662
- Bennett, W. F. (1994). Lateral ankle sprains. Part I: Anatomy, biomechanics, diagnosis, and natural history. Orthopaedic Review, 23(5), 381–387.
- Boutron, I., Page, M., Higgins, J., Altman, D., Lundh, A., & Hróbjartsson, A. (2021). Chapter 7: Considering bias and conflicts of interest among the included studies. In J. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M. Page, & V. Welch (Eds.), Cochrane Handbook for systematic reviews of interventions version 6.2. Cochrane.
- Chin, M., Leppänen, M., Kulmala, J.-P., Parkkari, J., Vasankari, T., & Pasanen, K. (2020). A 3D motion capture analysis of an accidental lateral ankle sprain injury during a 180-degree pivot turn. 2020 CASEM Poster Presentations, 30(3), e101–e102. https://doi.org/https://doi.org/10.1097/JSM.0000000000000844
- Chin, M., Leppänen, M., Kulmala, J.-P., Vasankari, T., Parkkari, J., & Pasanen, K. (2021). A 3D motion capture analysis of a giving-way ankle episode during a 180-degree pivot turn: A case report. Journal of Biomechanics, 118, 110318. https://doi.org/https://doi.org/10.1016/j.jbiomech.2021.110318
- Chu, V. W.-S., Fong, D. T.-P., Chan, -Y.-Y., Yung, P. S.-H., Fung, K.-Y., & Chan, K.-M. (2010). Differentiation of ankle sprain motion and common sporting motion by ankle inversion velocity. Journal of Biomechanics, 43(10), 2035–2038. https://doi.org/https://doi.org/10.1016/j.jbiomech.2010.03.029
- Dawson, B., Hopkinson, R., Appleby, B., Stewart, G., & Roberts, C. (2004). Comparison of training activities and game demands in the Australian Football League. Journal of Science and Medicine in Sport, 7(3), 292–301. https://doi.org/https://doi.org/10.1016/S1440-2440(04)80024-0
- Delahunt, E., Coughlan, G. F., Caulfield, B., Nightingale, E. J., Lin, C.-W. C., & Hiller, C. E. (2010). Inclusion criteria when investigating insufficiencies in chronic ankle instability. Medicine and Science in Sports and Exercise, 42(11), 2106–2121. https://doi.org/https://doi.org/10.1249/MSS.0b013e3181de7a8a
- Delahunt, E., & Remus, A. (2019). Risk factors for lateral ankle sprains and chronic ankle instability. Journal of Athletic Training, 54(6), 611–616. https://doi.org/https://doi.org/10.4085/1062-6050-44-18
- Doherty, C., Delahunt, E., Caulfield, B., Hertel, J., Ryan, J., & Bleakley, C. (2014). The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies. Sports Medicine, 44(1), 123–140. https://doi.org/https://doi.org/10.1007/s40279-013-0102-5
- Fong, D. T. P., Ha, S. C. W., Mok, K. M., Chan, C. W. L., & Chan, K. M. (2012). Kinematics analysis of ankle inversion ligamentous sprain injuries in sports: Five cases from televised tennis competitions. American Journal of Sports Medicine, 40(11), 2627–2632. https://doi.org/https://doi.org/10.1177/0363546512458259
- Fong, D. T. P., Hong, Y., Chan, L. K., Yung, P. S. H., & Chan, K. M. (2007). A systematic review on ankle injury and ankle sprain in sports. Sports Medicine, 37(1), 73–94. https://doi.org/https://doi.org/10.2165/00007256-200737010-00006
- Fong, D. T. P., Hong, Y., Shima, Y., Krosshaug, T., Yung, P. S. H., & Chan, K. M. (2009). Biomechanics of supination ankle sprain: A case report of an accidental injury event in the laboratory. American Journal of Sports Medicine, 37(4), 822–827. https://doi.org/https://doi.org/10.1177/0363546508328102
- Fong, D. T. P., Mok, K.-M., Thompson, I. M., Wang, H. Y., Shan, W., & King, M. A. (2021). A lateral ankle sprain during a lateral backward step in badminton: A case report of a televised injury incident. Journal of Sport and Health Science. (in press). https://doi.org/https://doi.org/10.1016/j.jshs.2021.03.007
- Gehring, D., Wissler, S., Mornieux, G., & Gollhofer, A. (2013). How to sprain your ankle - a biomechanical case report of an inversion trauma. Journal of Biomechanics, 46(1), 175–178. https://doi.org/https://doi.org/10.1016/j.jbiomech.2012.09.016
- Gokeler, A., McKeon, P. O., & Hoch, M. C. (2020). Shaping the functional task environment in sports injury rehabilitation: A framework to integrate perceptual-cognitive training in rehabilitation. Athletic Training & Sports Health Care, 12(6), 283–292. https://doi.org/https://doi.org/10.3928/19425864-20201016-01
- Gribble, P. A., Bleakley, C. M., Caulfield, B. M., Docherty, C. L., Fourchet, F., Fong, D. T. P., Hertel, J., Hiller, C. E., Kaminski, T. W., McKeon, P. O., Refshauge, K. M., Verhagen, E. A., Vicenzino, B. T., Wikstrom, E. A., & Delahunt, E. (2016). Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. British Journal of Sports Medicine, 50(24), 1496–1505. https://doi.org/https://doi.org/10.1136/bjsports-2016-096189
- Gribble, P. A., Delahunt, E., Bleakley, C., Caulfield, B., Docherty, C., Fourchet, F., Fong, D. T.-P., Hertel, J., Hiller, C., Kaminski, T., McKeon, P., Refshauge, K., van der Wees, P., Vincenzino, B., & Wikstrom, E. (2014). Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. British Journal of Sports Medicine, 48(13), 1014–1018. https://doi.org/https://doi.org/10.1136/bjsports-2013-093175
- Hamel, A. J., Sharkey, N. A., Buczek, F. L., & Michelson, J. (2004). Relative motions of the tibia, talus, and calcaneus during the stance phase of gait: A cadaver study. Gait & Posture, 20(2), 147–153. https://doi.org/https://doi.org/10.1016/J.GAITPOST.2003.07.003
- Hartwig, T. B., Naughton, G., & Searl, J. (2011). Motion analyses of adolescent rugby union players: A comparison of training and game demands. Journal of Strength and Conditioning Research, 25(4), 966–972. https://doi.org/https://doi.org/10.1519/JSC.0b013e3181d09e24
- Herzog, M. M., Mack, C. D., Dreyer, N. A., Wikstrom, E. A., Padua, D. A., Kocher, M. S., DiFiori, J. P., & Marshall, S. W. (2019). Ankle sprains in the National Basketball Association, 2013-2014 through 2016-2017. The American Journal of Sports Medicine, 47(11), 2651–2658. https://doi.org/https://doi.org/10.1177/0363546519864678
- Khor, Y. P., & Tan, K. J. (2013). The anatomic pattern of injuries in acute inversion ankle sprains: A magnetic resonance imaging study. Orthopaedic Journal of Sports Medicine, 1(7), 2325967113517078. https://doi.org/https://doi.org/10.1177/2325967113517078
- Kosik, K. B., Hoch, M. C., Heebner, N. R., Hartzell, J., & Gribble, P. A. (2019). A laboratory captured “giving way” episode during a single-leg landing task in an individual with unilateral chronic ankle instability. Journal of Biomechanics, 90, 153–158. https://doi.org/https://doi.org/10.1016/j.jbiomech.2019.05.009
- Kristianslund, E., Bahr, R., & Krosshaug, T. (2011). Kinematics and kinetics of an accidental lateral ankle sprain. Journal of Biomechanics, 44(14), 2576–2578. https://doi.org/https://doi.org/10.1016/j.jbiomech.2011.07.014
- Krosshaug, T., Andersen, T. E., Olsen, O. E. O., Myklebust, G., & Bahr, R. (2005). Research approaches to describe the mechanisms of injuries in sport: Limitations and possibilities. British Journal of Sports Medicine, 39(6), 330–339. https://doi.org/https://doi.org/10.1136/bjsm.2005.018358
- Krosshaug, T., & Bahr, R. (2005). A model-based image-matching technique for three-dimensional reconstruction of human motion from uncalibrated video sequences. Journal of Biomechanics, 38(4), 919–929. https://doi.org/https://doi.org/10.1016/j.jbiomech.2004.04.033
- Krosshaug, T., Slauterbeck, J. R., Engebretsen, L., & Bahr, R. (2007). Biomechanical analysis of anterior cruciate ligament injury mechanisms: Three-dimensional motion reconstruction from video sequences. Scandinavian Journal of Medicine & Science in Sports, 17(5), 508–519. https://doi.org/https://doi.org/10.1111/j.1600-0838.2006.00558.x
- Li, X., Fong, D. T.-P., & Chan, K.-M. (2016). Kinematic analysis of ankle eversion sprain in sports: Two cases during the FIFA world cup. Proceedings of the 2016 International Combined Meeting of Orthopaedic Research Societies, 7, 135. https://doi.org/https://doi.org/10.1016/j.jot.2016.06.193
- Li, Y., Ko, J., Zhang, S., Brown, C. N., & Simpson, K. J. (2019). Biomechanics of ankle giving way: A case report of accidental ankle giving way during the drop landing test. Journal of Sport and Health Science, 8(5), 494–502. https://doi.org/https://doi.org/10.1016/j.jshs.2018.01.002
- Lysdal, F. G., Bandholm, T., Tolstrup, J. S., Clausen, M. B., Mann, S., Petersen, P. B., Grønlykke, T. B., Kersting, U. G., Delahunt, E., & Thorborg, K. (2021). Does the Spraino low-friction shoe patch prevent lateral ankle sprain injury in indoor sports? A pilot randomised controlled trial with 510 participants with previous ankle injuries. British Journal of Sports Medicine, 55(2), 92–98. https://doi.org/https://doi.org/10.1136/bjsports-2019-101767
- Lysdal, F. G., Grønlykke, T. B., & Kersting, U. G. (2018). Biomechanics of a lateral ankle sprain: And the effect of a minimized lateral shoe-surface friction. In Program and Abstracts, International Foot and Ankle Biomechanics Meeting, i-FAB 2018, New York, USA [ Poster No. 15].
- Medina Mckeon, J. M., & Hoch, M. C. (2019). The ankle-joint complex: A kinesiologic approach to lateral ankle sprains. Journal of Athletic Training, 54(6), 589–602. https://doi.org/https://doi.org/10.4085/1062-6050-472-17
- Mineta, S., Inami, T., Hoshiba, T., Higashihara, A., Kumai, T., Torii, S., & Hirose, N. (2021). Greater knee varus angle and pelvic internal rotation after landing are predictive factors of a non-contact lateral ankle sprain. Physical Therapy in Sport, 50, 59–64. https://doi.org/https://doi.org/10.1016/J.PTSP.2021.04.001
- Mok, K.-M., Fong, D. T.-P., Krosshaug, T., Engebretsen, L., Hung, A. S.-L., Yung, P. S.-H., & Chan, K.-M. (2011a). Kinematics analysis of ankle inversion ligamentous sprain injuries in sports: 2 cases during the 2008 Beijing Olympics. The American Journal of Sports Medicine, 39(7), 1548–1552. https://doi.org/https://doi.org/10.1177/0363546511399384
- Mok, K. M., Fong, D. T. P., Krosshaug, T., Hung, A. S. L., Yung, P. S. H., & Chan, K. M. (2011b). An ankle joint model-based image-matching motion analysis technique. Gait & Posture, 34(1), 71–75. https://doi.org/https://doi.org/10.1016/j.gaitpost.2011.03.014
- Mok, K. M., Ha, S. C. W., Chan, Z. Y. S., Yung, P. S. H., & Fong, D. T. P. (2021). An inverted ankle joint orientation at foot strike could incite ankle inversion sprain: Comparison between injury and non-injured cutting motions of a tennis player. Foot, 48, 101853. https://doi.org/https://doi.org/10.1016/j.foot.2021.101853
- Panagiotakis, E., Mok, K. M., Fong, D. T. P., & Bull, A. M. J. (2017). Biomechanical analysis of ankle ligamentous sprain injury cases from televised basketball games: Understanding when, how and why ligament failure occurs. Journal of Science and Medicine in Sport, 20(12), 1057–1061. https://doi.org/https://doi.org/10.1016/j.jsams.2017.05.006
- Remus, A., Caulfield, B., Doherty, C., Crowe, C., Severini, G., & Delahunt, E. (2018). A laboratory captured “giving way” episode in an individual with chronic ankle instability. Journal of Biomechanics, 76, 241–246. https://doi.org/https://doi.org/10.1016/j.jbiomech.2018.05.015
- Skazalski, C., Kruczynski, J., Bahr, M. A., Bere, T., Whiteley, R., & Bahr, R. (2018). Landing-related ankle injuries do not occur in plantarflexion as once thought: A systematic video analysis of ankle injuries in world-class volleyball. British Journal of Sports Medicine, 52(2), 74–82. https://doi.org/https://doi.org/10.1136/bjsports-2016-097155
- Takeda, R., Nakajima, K., Anzai, E., Tanaka, S., Ohta, Y., & Matsumoto, T. (2021). A ‘Giving way’ captured during walking by gyroscopes and plantar force sensors. Journal of Biomechanics, 129, 110754. https://doi.org/https://doi.org/10.1016/j.jbiomech.2021.110754
- Terada, M., & Gribble, P. A. (2015). Jump landing biomechanics during a laboratory recorded recurrent ankle sprain. Foot & Ankle International, 36(7), 842–848. https://doi.org/https://doi.org/10.1177/1071100715576517
- Trejo Ramírez, M. P., Wheat, J., James, D., Warmenhoven, J., & Hamilton, N. (2020). Case study of an accidental ankle twist: A kinematic analysis using functional data analysis. ISBS Proceedings Archive, 38(1), 196–199.
- Vuurberg, G., Hoorntje, A., Wink, L. M., van der Doelen, B. F. W., van den Bekerom, M. P., Dekker, R., van Dijk, C. N., Krips, R., Loogman, M. C. M., Ridderikhof, M. L., Smithuis, F. F., Stufkens, S. A. S., Verhagen, E. A. L. M., de Bie, R. A., & Kerkhoffs, G. M. M. J. (2018). Diagnosis, treatment and prevention of ankle sprains: Update of an evidence-based clinical guideline. British Journal of Sports Medicine, 52(15), 956. https://doi.org/https://doi.org/10.1136/bjsports-2017-098106
- Wade, F. E., Mok, K.-M., & Fong, D. T.-P. (2018). Kinematic analysis of a televised medial ankle sprain. Asia-Pacific Journal of Sports Medicine, Arthroscopy, Rehabilitation and Technology, 12, 12–16. https://doi.org/https://doi.org/10.1016/j.asmart.2018.02.001
- Wei, F., Fong, D. T.-P., Chan, K.-M., & Haut, R. C. (2014). Estimation of ligament strains and joint moments in the ankle during a supination sprain injury. Computer Methods in Biomechanics and Biomedical Engineering, 18(3), 243–248. https://doi.org/https://doi.org/10.1080/10255842.2013.792809
- Wright, I. C., Neptune, R. R., Van Den Bogert, A. J., & Nigg, B. M. (2000). The influence of foot positioning on ankle sprains. Journal of Biomechanics, 33(5), 513–519. https://doi.org/https://doi.org/10.1016/S0021-9290(99)00218-3
- Wu, G., Siegler, S., Allard, P., Kirtley, C., Leardini, A., Rosenbaum, D., Whittle, M., D’lima, D. D., Cristofolini, L., Witte, H., Schmid, O., & Stokes, I. (2002). ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion–part I: Ankle, hip, and spine. International Society of Biomechanics. Journal of Biomechanics, 35(4), 543–548. https://doi.org/https://doi.org/10.1016/s0021-9290(01)00222-6