

IS-01-025 Glucocorticoids and epigenetic modifications during development
M. Drake
University of Edinburgh, Edinburgh, UK
Numerous epidemiological studies have demonstrated a link between low birth weight and subsequent cardio-metabolic disease including insulin resistance, type 2 diabetes, hypertension and the metabolic syndrome. This has given rise to the hypothesis that events in fetal life permanently programme subsequent cardiovascular risk. It is also clear from both human and animal studies that these effects may not be limited to the first generation offspring. Epidemiological studies in humans suggest intergenerational effects on birth weight, cardiovascular risk factors and type 2 diabetes and transgenerational effects on birth weight, glucose tolerance, blood pressure and the hypothalamic-pituitary-adrenal (HPA) axis have been reported in animal models.
In the dexamethasone-programmed rat, fetal overexposure to glucocorticoid results in low birth weight and adult hyperinsulinaemia and hyperglycaemia, underpinned by increased activity of the gluconeogenic enzyme, phosphoenolpyruvate carboxykinase (PEPCK). We have explored intergenerational effects in this model of programming. We have shown that the male offspring of female rats which had been exposed prenatally to dexamethasone, but were not manipulated in their own pregnancy, also had reduced birth weight, glucose intolerance and elevated hepatic PEPCK activity. These effects resolved in a third generation. Similar intergenerational programming was observed in offspring of male rats exposed prenatally to dexamethasone mated with control females.
Thus, programming effects are transmitted to a second generation by both maternal and paternal lines, indicating that the transmission of programming effects can not solely be explained by programmed alterations in maternal physiology. Epigenetic factors may therefore be important in the intergenerational inheritance of the programming phenotype, providing a basis for the inherited association between low birth weight and cardiovascular risk factors.
IS-01-026 The fetal endocrine pancreas and the long term effect
F.A. Van Assche, C. Morens
Fac. of Medicine, Univ. of Leuven, Leuven, Belgium
The fetal endocrine pancreas undergoes important changes in fetal macrosomia as well as in intra uterine growth restriction. In the human, fetal asymmetric macrosomia is related to maternal diabetes. The fetal endocrine pancreas shows islet hypertrophy and B cell hyperplasia. In situations of very high blood sugar in the mother, we even observe degranulation of the insulin producing B cells.
In intrauterine growth restriction a reduced amount of endocrine tissue and of B cells is found.
Foreover asymmetric macrosomia is linked with high levels of Insulin and IGF; whereas intrauterine growth restriction is linked with low levels of Insulin and IGF.
These changes in the endocrine pancreas are also present in experimental conditions in the rat.
Research in animals facilitates the exploration of the working mechanisms.
In maternal diabetes with fetal asymmetric macosomia, fetal B cells are over stimulated. This may explain the reduced capacity of Insulin secretion in later life.
In intrauterine growth restriction, there is underdevelopment of the fetal B cells and a reduced insulin receptor formation. This finding may explain Insulin resistance in later life.
Obesity and over nutrition play a crucial role in fetal programming. This relation will be further explored in the European Research project EARNEST.
IS-01-029 Interventional ultrasound, what does 3d-4d add?
J.M. Troyano, M. Alvarez de la Rosa, I. Martinez-Wallin
Ultrasound Unit and Fetal Medicine, Dept. of Obstetrics and Gynecology, University Hospital of Canary Islands, Tenerife
Objective: We evaluate, among others, the efficiency of using 3D-4D ultrasound as an invasive technique procedure in Obstetrics and Gynecology.
Prenatal invasive techniques by 4D echography gives us information in three planes and allows us to ensure the optimal critical point of puncture with a 100% success rate.
Methods: Invasive techniques using 3D-4D echography were recorded in 56 cases:
Conventional prenatal invasive procedures, 30 cases: 22 amniocentesis, 5 chorionic villus sampling (CVS) and 3 cordocentesis.
Fetal biopsies, 3 cases: 2 aspiratives nephrostomies and 1 Liver biopsy.
Regarding to aspirative technique in Gynecology, 26 cases: 18 breast punction (12 cysts, 6 solid nodules) and 8 ovarian cysts.
In all cases, first of all, we identified the needle under 2D monitoring (conventional ultrasound) and we continued by 3D-4D ultrasound in real time.
Results: Success rate (100%) in all prenatal diagnosis and Gynecological cases, even fetal biopsies.
Mean time used: Amniocentesis 7 minutes, CVS 9 minutes, and cordocentesis 7 minutes.
Regarding to Gynecological biopsies: Breast punction 4 minutes, ovarian aspiraive punction 5 minutes.
We reported a funicular hemorrhage over 1 minute in one cordocentesis without other complications.
Conclusions: Even though 2D ultrasound remains unreplaceable in both obsterical and gynecological punction techniques, 3D-4D ultrasound (real time) is becoming a complementary procedure, for the moment, increasing the safety and efficiency of the punction, helping the tridimensional identification of the critical point puncture and, due to this, reducing the duration of the technique. In the future, this will be the way for invasive techniques within our speciality.
IS-01-031 Advances of 3d in neonatal period
M. Stanojevic
General Hospital “Sv. Duh”, Sv. Duh 64, Zagreb, Croatia
Introduction: In the 1990's, a new exciting technique of 3D and 4D ultrasonography (USG) was developed, enabling depiction of neonatal organs in the third dimension in real-time. Brain ultrasound became the most widely used technique for the evaluation of brain morphology and cerebral lesions in neonates. It can confirm prenatal diagnosis and identify not only the presence of lesions but also their type and extent.
Aim: To present the socio medical aspect and the indications for 3D USG in neonatal period, with the accent on neurosonography.
Material and methods: 3D will be used in selected group of newborns in order to prove it's advantages or disadvantages in the comparison with 2D USG.
Results: 3D is more convinient than 2D, because the time of data acquisition is shorter, while the «off line» analysis is longer than by 2D. 3D ultrasound plays very important role as a diagnostic tool for the determination of the prognosis of the diseases or conditions in newborns, which can possibly influence the quality of life not only of the newborns, but the entire family as well. 3D ultrasound is valuable imaging modality for depiction of neonatal brain, but appears to be useful in neonatal echocardiography, nephrology, orthopedics, ophthalmology and other fields o pediatrics. 3D is used for diagnostics of the neonatal spinal canal pathology, soft tissues and musculoskeletal changes, diagnostics of tumors, and many other conditions. 3D is an accurate method for the assessment of volumes of many organs and pathological changes in neonates.
Conclusion: 3D USG in neonatal period has been considered a significant improvement compared to the conventional 2D, due to: shorter time of data acquisition with unlimited number of planes, possibility of comprehensive and thorough analysis of obtained data set, volume rendering, volumetric studies, color and power Doppler studies, and sending 3D images electronically, without necessity of referring the patient.
IS-02-002 Vaginal obstetric operations – an up-date
R. Erkkola
Department of Obstetrics and Gynecology, University Central Hospital, Turku, Finland
Forceps delivery (FD), and vacuum extraction (VE) are operations to hasten the natural vaginal delivery. An important prerequisite is a full dilatation of cervix. In Finland, the rate of these operations varies from 5% to 7% of all deliveries.
There are two main indications. 1) The first is a lengthened 2nd stage of labor. The birthing process is an outcome of three P-factors: passage, passenger and power and the situation must be analyzed by having these factors in mind. A small disproportion may be solved with a good judgment and experience by using either VE or FD. Malpresentation may be instrumentally corrected. Further, the driving force may be increased by up to 15 kilo pounds. 2) Fetal distress is another important indication. Previously, the use of forceps was faster to use, but the present soft cup extractors are also very rapid. Still, by using forceps, the failure to deliver occurs less frequently. In Finland, and in many countries of Europe, VE has almost totally replaced the FD. The main reasons are: 1) the relative easiness of VE in comparison to FD. 2) FD may be followed by a greater risk of soft tissue tears and pelvic floor dysfunction. 3) The training to FD may have become less efficient. In case of difficult delivery of the aftercoming head, an adequately performed FD is still required. If the principle of the indications for VE/FD is accepted, the main issue is the adequate conduction of these operations. The cornerstones are the high-quality training and the solid, professional judgment by the obstetrician responsible of the delivery. For the official purposes, the guidelines must be defined how to prepare the clinical report of the procedure.
IS-02-003 Who should decide upon the mode of delivery – medical indication versus shared decision making
P. Husslein
University of Wien, Wien, Austria
Over the past 20 years, the rate of caesarean section has undergone a marked increase on a global level, and it appears unlikely that this trend will be reversed in the near future.
This fact has also raised a number of questions regarding the growing preference for elective caesarean section following a complication-free pregnancy and in the absence of medical indications. This is amply illustrated by the results of a study questioning British obstetricians, which shows that 31% of female obstetricians elected to deliver by means of caesarean section in cases where there was no medical necessity whatsoever.
Both the mortality rate of carefully prepared procedures of this kind and the attending morbidity rate have been successfully reduced in recent years owing to improvements in section technique, causing certain of the maternal and fetal risks accompanying vaginal delivery to come under closer scrunity than before. The potential damage to the perineum during birth – and the impairment of the parturient's sexuality this may cause – in conjunction with the fact that vaginal delivery continues to expose the infant to certain risks which cannot be ruled out entirely has made the choice between vaginal delivery and caesarean section increasingly difficult. The argument most frequently cited in favor of vaginal delivery concerns the unimpaired birth experience it offers. Many women, however, do not consider this a high priority.
Recently it has been shown that newborns after elective caesarean section show a reduced stress response especially in comparison to newborns after difficult vaginal delivery. This difference can still be documented 6 weeks post partum.
In keeping with the greater importance currently being assigned to patients preferences, the author supports the view that the parturient herself should be enabled to decide what level of risk is acceptable to her, including stating her preference for a delivery by caesarean section.
It cannot be stressed enough that, in this context, comprehensive information and rigorous documentation are indispensable requirements.
IS-02-006 Patient choice cesarean: Evidence and ethics
F. Chervenak1, L. McCullough2
1Weill Medical College of Cornell University, 525 E 68th St, J-130, New York, NY, USA; 2Baylor College of Medicine, Houston, Houston, TX, USA
Patient choice cesarean is a current clinical controversy. Ethics is an essential dimension of addressing this controversy in a clinically appropriate fashion. In this lecture, current evidence is presented regarding the benefits and risks of elective cesarean delivery. This evidence, which is understood as the ethical principle of beneficence, is balanced with autonomy and justice-based considerations, as well as professional integrity issues.
An argument will be presented that at the present time patient choice cesarean should not be routinely recommended or offered. When a patient presents with a request for an elective cesarean delivery, the obstetrician is obligated to ensure that she understands the risks of cesarean delivery to herself and her newborn, appreciates that those risks could occur, and makes a voluntary decision. The obstetrician should also ask her to reconsider her request. Requests that persist and reflect deeply held values which she reaffirms meet the test of being well supported in autonomy based clinical judgment. In such circumstances, it is appropriate for the obstetrician to accede to such requests and perform the cesarean delivery, if the obstetrician is comfortable with implementing such a request. If not, an appropriate referral should be made. There should be no influence of economic or other conflicts of interest in the counseling process for the decision to perform a cesarean delivery.
By neither dismissing patients' requests regarding cesarean delivery, nor automatically acquiescing to them, physicians maintain both professional integrity and their respect for their patients' autonomy.
IS-02-007 Vaginal delivery for breech presentation
R. Erkkola
Department of Obstetrics and Gynecology, University Central Hospital, Turku, Finland
The total incidence of breech presentation is around 4% and at term 3.3%. It is by far the most common abnormal fetal presentation. To carry out a safe vaginal breech delivery (VBL) belongs to the traditional art of obstetrics. Retrospective reports maintain that VBL at term brings about an almost 4-fold risk of either perinatal death or neonatal morbidity in comparison to caesarean section (CS). Consequently, recommendations exist to perform a routine elective CS for all breeches. Many facts are not in favor of this recommendation. 1) Maternal mortality or morbidity after CS are many fold in comparison to VBL. 2) Costs of CS far exceed those of VBL. 3) Neonates delivered by CS due to breech fare worse than neonates delivered by CS in vertex presentation; fetuses in breech presentation may carry along some inherent health problems. 4) CS for breech presentation may bring about complications due to difficulties in extraction. 5) No randomized prospective trial has ever shown that CS is superior to a selected VBL, managed by an experienced obstetrician. By applying good judgment and skillful techniques the route of breech delivery has no impact on the outcome. Instead, VBL does lead to less maternal complications and lower economical costs.
IS-02-008 Is there still a role for postnatal corticosteroids?
H.L. Halliday
Regional Neonatal Unit, Royal Maternity Hospital, Belfast, Northern Ireland; Department of Child Health, Queen's University Belfast, Belfast, Northern Ireland
Objective: To debate the role of postnatal corticosteroid therapy in the prevention and treatment of chronic lung disease in preterm infants.
Methods: The results randomised controlled trials (RCTs) and systematic reviews of RCTs will be used to develop evidence-based guidelines for postnatal corticosteroid therapy in preterm infants at risk of developing chronic lung disease (CLD) or bronchopulmonary dysplasia. The results are presented as relative risks (RR) and numbers needed to treat (NNT) or harm (NNH) each with their 95% confidence intervals (CI).
Results: The systematic reviews in the Cochrane Library show that postnatal corticosteroids given at any time in the neonatal period reduce the risk of CLD at 36 weeks (e.g. for moderately early RR 0.62; 95% CI 0.47–0.82; NNT 5; 95% CI 3–11). However, there are apparent adverse neurological effects e.g. abnormal CNS examination (early RR 1.81; 95% CI 1.33–2.47; NNH 10; 95% CI 7–20 and delayed RR 1.90; 95% CI 1.08–3.33; NNH 6; 95% CI 4–33). Cerebral palsy, however was only increased in the early (<4 days) treated infants (RR 1.69; 95% CI 1.20–2.38; NNH 17; 95% CI 9–50). Further analysis of the outcomes of over 4000 preterm infants who had been enrolled in these RCTs using meta-regression shows that the risk of developing cerebral palsy is inversely related to the risk of developing CLD. This means that use of corticosteroids in babies at low risk of developing CLD increases the risk of later cerebral palsy. It also explains why the risk of cerebral palsy is increased only in preterm infants who were treated early.
Conclusions: Postnatal corticosteroids should be avoided in the first 4 days of life and reserved for babies at high risk of developing CLD or who already have CLD. When used corticosteroids should be used in the lowest dose for the shortest possible duration. There is still a limited role for corticosteroids in the neonatal period and further research is needed to refine the indications for their use.
IS-02-008 Postnatal corticosteroids – dangerous and avoidable
E.S. Shinwell1
1Kaplan Medical Center, PO Box 1, Rehovot, Israel; 2Hadassah Medical School, Hebrew University, Jerusalem, Israel
Corticosteroids have seen fluctuating popularity in the prevention and treatment of Bronchopulmonary Dysplasia in preterm infants over the past 3 decades. In the late 1990's, evidence accumulated showing increased risk of cerebral palsy and neurodevelopmental delay in preterm infants treated with steroids, particularly when the treatment was administered close to birth and when continued for a prolonged course. More recently, studies in neonatal animal models have shown that steroids caused marked inhibition of brain growth. Volume MRI studies in human infants have likewise shown growth inhibition, particularly of grey matter, especially in the frontal lobes and more so in males.
Since 1998, the large neonatal networks have documented a gradual reduction in the use of postnatal corticosteroids. We have recently conducted an analysis of the consequences of this change in practice using the Israel Very Low Birth Weight Infant Database between 1997 and 2002. Steroid therapy fell from 23.5% in 1997–98 to 12.8% in 2001–02. Concurrently, a 1.4–1.5-fold increase in the need for oxygen at 28 days of age and 36 weeks post-menstrual age was seen. However, the duration of oxygen therapy was increased only by a few days overall and mortality decreased over this period.
These data suggest that a highly-selective policy of limited steroid use is reasonable and demonstrates careful balancing of the risks and potential benefits of this therapeutic intervention.
IS-02-011 Fetal monitoring and frequency of operative deliveries
K.G. Rosen
Perinatal Centre, University of Goteborg and Neoventa Medical, Sweden
Caesarian section has become the most common operative procedure worldwide. The consequences of this development have become a political issue and in some countries, obstetricians are an endangered species due to medico-legal consequences of inadequacies in fetal monitoring.
With accumulating data on side effects such as neonatal and maternal morbidity, socio-economic and health care cost as well as uncertainty about haw to manage future pregnancies, we may wish for improvements. Insufficient information and uncertainty about the clinical interpretation of the fetal heart rate tracing appears to be a major factor affecting acute intervention rates.
The STAN methodology bringing a physiological basis and strict clinical guidelines to fetal surveillance in labour has been shown to break the trend of increasing intervention rates. Defining new guidelines means that standards are set for how the methodology should be used. Only then are you able to assess the potential impact.
Although the Swedish RCT showed reduced ODFD rates, these became more significant when considering only adequately recorded cases showing a reduction in CS rates from 2.9% (standard CTG) to 1.9% (CTG + ST) (OR; 0.66 95th CI; 0.44–0.97). Furthermore when the staff got more experienced during the 2nd phase of the study even lower C/S rates were noted; 2.4% vs. 1.4% (0.61, 0.43–0.86), corresponding to the reduced CS rates noted in the Plymouth RCT from 2.5% to 1.2% (0.49, 0.25–0.95). It should be noted that the fetal outcome (CA met acidosis rates) improved as well.
To what extent are these figures applicable to every-day obstetric care? Currently we have annual rates of CS for fetal distress from a small set of hospitals.
The primary aim with intrapartum fetal surveillance is to identify and intervene in case of fetal hypoxia. Although CS rates were somewhat higher, cord artery metabolic acidosis rates were well within the range noted in the SRCT (0.69%). This outcome measure seems to be more easily achieved then that of low CS rate. However, with increasing experience of the STAN methodology we may see reduced operative intervention rates approaching those of the RCTs.
This work has been supported by the EU commission through a BioPattern NoE.
IS-02-013 Internal poudalic version and breech extraction – do they still have a role in obstetrics?
R. Erkkola
Department of Obstetrics and Gynecology, University Central Hospital, Turku, Finland
In the past, IPV has been a widely performed and favored procedure. In ancient times, the indications were: 1) delivery of second twin or twin B, 2) shoulder presentation, 3) cord prolapse, 4) placental previa, and 5) delivery of the rump following embryotomy. The other indications have become almost obsolete, yet the delivery of twin B in transverse lie remains still an optional indication. Options to deliver the twin B in transverse lie are: 1) external version, 2) IPV, 3) caesarean section. In the case of signs of threatening fetal asphyxia, heavy bleeding suggesting placental ablation or cord prolapse after delivery of twin A, IPV followed by BE is without doubt the fastest way to deliver the twin B. It is almost mandatory to perform an abdominal ultrasound examination to define precisely the fetal position before attempting the IPV. If the membranes are still unruptured, the fetal feet can be crabbed from outside the membranes for IPV, amniotic fluid giving space for version. If the membranes are ruptured, and the uterus is contracting, intravenous nitroglycerin is reported to facilitate the version. The person doing the IPV and BE must have had a theoretical and fantom training. After IPV, with one or both feet visible at introitus, it is wise to check the fetal heart rate. If it is satisfactory, there is no hurry to perform BE; it is advisable to let the fetus recover and pull the arms on the breast. The BE can be performed with smooth moves imitating the rotations occurring at normal breech delivery.
IS-02-015 The complications of caesarean delivery
A. Roztočil, CSc.
Department of Obstetrics and Gynecology, Nemocnice Jihlava, Vrchlického 59, Jihlava, Czech Republic
The Caesarean section is in the developped countries the most frequent major obstetrical surgery. The rate of this operation in CZ reached 16.3% in 2004. With the developpement of surgical techniques of caesarean section, pre, intra and postpartum care and the rise of the rate of this conduct of labor that lead to the improvement in skils of the operating teams, the frequency of at least major complications decreased. Newertheless the caesarean section complications represent a very important pool of maternal morbidity and mortality.
The major causes of these complications are the following: important pregnancy and intrapartum health disturbances in mother and foetus, emergency pregnancy termination, previous abdominal surgery, unsufficient operating theatre team and equippmemnt quality.
The complications are classified from the time point of view as perioperative (immediate), early and late, from the importance as minor or major, concerning the speciality as anesthesiologic, obstetrical, urologic, gastroenterologic, haematologic, neonatologic and others, maternal and neonatal, somatic and psychological, treatable and fatal.
The intraoperative surgery complications include the following: abdominal wall, hysterotomy and atonia bleedings, bladder and ureteral injuries, amniotic fluid embolism.
Early complications: postoperative pain, trombembolic (pulmonary embolism and deep venous trombosis), bleeding (abdominal wall haematomas, haemoperitoneum, uterine atony, placental residua, hysterotomy suture bleeding, haemocoagulation disorders – DIC), local and general inflammatory complications: endomyometritis, uterine suture infection, parametritis, wound infection, sepsis. Urinary tract infection, gastrointestinal complications (paralytic ileus).
IS-02-018 Current screening for fetal anomalies
P. Calda
Charles University, First Medical School, Apolinarska 18, Prague, Czech Republic
Ultrasound examination of the fetus at 11+0–13+6 weeks of pregnancy allows early diagnosis of many conditions, but the ultrasound scan betwen 18–22 weeks remains essential in detection of fetal malformations. Management of anomalous fetuses in twin pregnancies needs special aproaches. First-trimester combined test, which incorporates nuchal translucency, nasal bone, crown-rump length, pregnancy-associated plasma protein-A, and free beta-human chorionic gonadotropin, has the potential to maximize detection rates of Down syndrome and trisomy 18 and minimizes the screen-positive rate. There is worldwide discussion about the best screening strategy for the presence of fetal Down's syndrome: to perform first-trimester screening, to perform second-trimester screening, or to use strategies incorporating measurements in both trimesters. First-trimester combined screening at 11 weeks of gestation is better than second-trimester quadruple screening but at 13 weeks has results similar to second-trimester quadruple screening. Both stepwise sequential screening and fully integrated screening have high rates of detection of Down's syndrome, with low false positive rates. (FASTER trial). Individual risk-orientated two-stage first-trimester screening can potentially identify, in the first trimester of pregnancy, more than 90% of affected fetuses for a false-positive rate of 2–3%. Women should be counseled about the limited sensitivity and specificity of the tests, psychologic implications of a positive test, the potential impact of delivering a child with Down syndrome, risks associated with invasive prenatal diagnosis and second-trimester abortion, and delays inherent in the process.
IS-02-020 Qf-pcr – new windows in prenatal diagnosis
The-Hung Bui
The Karolinska Institute, Clinical Genetics Unit, Department of Molecular Medicine, & Center for Fetal Medicine, Department of Obstetrics and Gynecology, Karolinska University Hospital, Stockholm, Sweden. Email: [email protected]
For the last 35 years, karyotype analysis of cultured fetal cells has been the gold standard for cytogenetic prenatal diagnosis. This analysis has proved to be highly reliable for identifying numerical chromosome abnormalities (aneuploidy) and large structural rearrangements in fetal cells obtained invasively by amniocentesis or chorionic villi sampling. Screening tests for fetal aneuploidy are now widely used. As a result, there has been an increased demand by all parties for more rapid diagnostic methods that do not require cell culture. Fluorescence in situ hybridisation (FISH) on interphase cells and quantitative fluorescence PCR (QF-PCR) have been introduced to allow rapid diagnosis (1 or 2 days) of the common aneuploidies (trisomy 13, 18 and 21 and aneuploidy of the sex chromosomes). Both methods have been shown to be robust in prenatal diagnosis; however, QF-PCR has the additional advantage of being much cheaper and allowing the processing of much larger number of samples than FISH. It has replaced interphase FISH in an increasing number of genetic laboratories.
Based on a restropective study of 16 400 consecutive invasive tests and validation studies of QF-PCR, a new policy of QF-PCR as a stand alone analysis was introduced in January 2005 in Stockholm as an option to karyotyping when prenatal diagnosis is performed for advanced maternal age or anxiety. About 2600 prenatal QF-PCR analyses and only 600 karyotype were performed during 2005. The advantages and limitations of this approach will be discussed.
IS-02-022 Echocardiography in detection of fetal heart abnormalities
D. Maulik
Winthrop University Hospital, Mineola, USA
Congenital heart disease (CHD) is the most common single organ malformation of the fetus with a frequency of 8/1000 births. Identification of CHD before birth allows appropriate prognostication, patient counseling and management, and significantly improves the outcome. Fetal echocardiography offers the main approach for prenatal diagnosis and encompasses two dimensional B mode imaging, M-mode, spectral Doppler, and color Doppler sonography. Basic fetal cardiac imaging is an integral part of fetal anatomical assessment and includes the 4 chamber view and the outflow tracts. Comprehensive fetal echocardiography however encompasses more extensive assessment of the fetal heart. Despite the advances in fetal cardiac imaging over the last two decades, most cases of CHD are not diagnosed prenatally with population detection rates of only 10–25%. This emphasizes the continuing need for education and training, and also for advances in the technology. The latter includes the advent of 3 dimensional (3D) echocardiographic techniques: (a) the newly developed real time true 3D imaging with 2D x-matrix probe, and (b) the reconstructed 3D imaging using the STIC technology. The presentation will critically review the strengths, limitations and potential of these approaches.
IS-02-029 The first few breaths of life
Anthony D. Milner
Dept. of Pediatrics, St. Thomas' Hospital, London, UK
Respiratory movements commence at around 11 weeks of gestation.
The first breaths occur with a mean delay of 10 seconds. Factors involved include extrinsic factors (cooling, pain, audiovisual, tactile) and intrinsic factors central including sensitivity to CO2 and removal of respiratory inhibitory mechanisms. Denervation of the peripheral chemoreceptors does not prevent the onset.
The first studies into the onset of breathing were carried out by Karlberg and colleagues in the late 1950s using oesophageal balloons and a reverse plethysmograph. They obtained measurements on 11 babies with inspiratory pressures of 3 to 72 cm · H2O and inspiratory volume of 12 to 67 ml. Only 5 showed an opening pressure. Their theories for this were chest wall recoil frog breathing, and pulmonary priapism!
In our first studies an opening pressures was rarely seen, all but one had a functional residual capacity with the first breath. Five babies had inspiratory pressures of less than 20 cm · H2O.
Further investigation were commenced with the trunk still within the birth canal. On no occasion did the lung volume rise after delivery until breathing had started, excluding chest wall recoil. Descent down the birth canal was sometimes associated with a fall in lung volume, indicating that thoracic compression creates a potential space for the FRC. The mean negative inspiratory pressure was 33 cm · H2O, inflation volume 40.3 ml and a FRC 18 m.
Data were also obtained on 12 babies born by elective caesarean section. Only 5 of the 11 had an FRC by the end of the first breath compared to all of 11 after emergency caesarean section.
50 babies were studied using a two pressure transducers only accepting results when the distal pressure transducer was in the stomach and the proximal in the lower oesophagus as incorrect placing of the device leads to underrecording. Only 24 of the studies met these criteria. These results had similar volume changes, but none of the first breaths were less than 28 cm · H2O and a mean of 52 cm · H2O.
Our conclusions from these studies are as follows:
Passage down the birth canal may aid the formation of an FRC.
Chest wall recoil does not lead to lung expansion.
Opening pressures are rarely seen, air entering the respiratory tract as soon as the intrathoracic pressure falls as air/water interface is in the upper airways.
The mean first inspiratory pressure is 52 cm · H2O (range 28 to 105).
The mean inspiratory volume is in the region of 40 ml, with an FRC of 15 to 18 ml.
IS-02-032 Oxygen delivery and distribution in a fetus and a very preterm infant: How much is too much?
W. Tin
The James Cook University Hospital, UK
Oxygen is the most commonly used drug and has been widely accepted as an integral part of respiratory support in neonatal intensive care units. It has also been known for more than 50 years that it is easy to damage the eyes of a preterm infant by giving too much oxygen especially in the first few weeks of life Citation[1]. Despite this knowledge there is still a wide variation in approaches to oxygen monitoring (and therapy) within the neonatal nurseries Citation[2], highlighting the uncertainty – How much oxygen is too much?
The ultimate “goal” of oxygen therapy is to achieve adequate delivery and distribution of oxygen to tissues, but without creating oxygen toxicity and oxidative stress. Tissue oxygenation depends on several factors, including: (1) fractional inspired oxygen concentration, (2) gas exchange mechanism within the lungs, (3) oxygen carrying capacity of the blood, (4) cardiac output, and (5) local tissue oedema or ischaemia. In addition to these factors, oxygen delivery in a fetus also depends on transport of oxygen across the placenta and the maternal circulatory status. As fetal haemoglobin (HbF) has higher oxygen affinity and lower P50 (oxygen tension at which 50% of haemoglobin is saturated at a standard pH and temperature), adequate transfer of oxygen from placenta to fetus is achieved at relatively low PO2. High oxygen affinity of HbF however has disadvantage in oxygen delivery to the fetal tissue but because fetal oxygen-haemoglobin saturation curve is much steeper, adequate dissociation of oxygen from haemoglobin can occur with relatively small decrease in oxygen tension at tissue level Citation[3].
The preterm infant grows without any difficulty in utero with arterial blood that is only about 70% saturated with oxygen Citation[4], but as oxygen consumption of most newborn animal species significantly increases from the first few days of life, arterial oxygen saturation (as well as PaO2) in a preterm infants needs to be higher than fetal level. However, there is no sufficient evidence to suggest what is the optimal oxygen saturation or PaO2 for a preterm infant who is vulnerable to oxidative stress and oxygen toxicity. A prospective observational study of every baby born alive before 28 weeks gestation to a mother resident in the north of England in 1990–1994 came out with some fairly provocative findings in 2001 Citation[5]. This study suggested that using a “restrictive” approach of oxygen therapy by aiming to keep saturations between 80 and 90% compared to a “liberal” approach, targeting to keep saturations between 94 and 98% (whilst these babies received supplemental oxygen) was associated with significant reduction in the risk of severe retinopathy, duration of ventilation and duration of oxygen therapy. Survival rate at one year and the risk of cerebral palsy amongst the survivors were not different between the two groups. A recently completed follow up study on the same cohort of children also showed that low oxygen saturation targeting was not associated with any disadvantages in terms of cognitive function, adaptive ability and behaviour in children at about 10 years of age Citation[6]. Several other recent observational studies Citation[7],Citation[8],Citation[9] also suggested the potential clinical benefits of targeting low oxygen saturations in these vulnerable preterm babies, highlighting the urgent need of a large randomised trial.
It was collaboration across the continents that helped clinicians to identify the cause of retinopathy in the preterm baby more than 50 years ago Citation[1]. It seems likely that similar collaboration (for large randomised trial/s) is going to be required a second time if we are ever to be able to optimise the use of oxygen – a product capable of doing great harm as well as great good.
IS-02-033 Assessment of exhaled H2O2 in ventilated premature infants as a marker of oxidative stress?
P. Zoban1, M. Vizek2
1Department of Neonatollogy, 2nd Medical School, Charles University, V uvalu 84, Prague, Czech Republic; 2Department of Pathophysiology, 2nd Medical School, Charles University, Plzenska, Prague, Czech Republic
Objective: Although an enhancement of ROS production (incl. H2O2) is likely a crucial component of acute lung injury, a reliable assessment of an oxidative load in the lungs of premature newborns is not available. Because of its position in the metabolic pathway of ROS, its relative stability and the fact that it can be detected in expired air, H2O2 could be useful marker of immediate oxidative load in the immature lungs.
Methods: Eleven premature infants (including 4 ELBW infants: 803 ± 69 g, and 5 VLBW infants: 1350 ± 33 g), and 3 term newborns (3137 ± 211 g) entered the study. The repeated collection of exhaled breath condensate - EBC (3 times) was performed in 5 premature babies (1152 ± 288 g). All babies were mechanically ventilated with SIMV mode. The EBC's were collected at 5, 24 and 48 hours after birth. Expired gases were directed into glass chamber submerged in a salt/ice bath. The H2O2 concentrations were measured by chemiluminiscence.
Results: The H2O2 production was measured altogether in 27 attempts in 14 babies. In 5 ventilated premature newborns measured repeatedly during 48 hrs after delivery the production of H2O2 decreased from 812.2 ± 33.98 pmol/20 min to 388.6 ± 20.81 and 258.6 ± 25.90 pmol/20 min respectively. In these infants the production correlated with the time elapsed from the delivery (rxy = 0.85, p < 0.05).
Conclusions: In attempt to measure H2O2 production we adapted the technique of EBC collection in small laboratory animals and for ventilated premature infants. The pilot clinical study showed that in premature babies, ventilated with FIO2 ≤ 0.4, H2O2 production significantly decreased during 48 hrs after delivery. Obtained values of H2O2 production are consistent and therefore may increase the effort to use analysis of EBC also in the newborns. (Supported by MZO 00064203)
IS-02-34 Response of pulmonary vascular bed to chronic hypoxia
J. Herget
Department of Physiology, 2nd Medical School, Prague and Centre for Cardiovascular Research, Prague
Chronic lung hypoxia results in hypoxic pulmonary hypertension (HPH) due to increase in vascular tone and structural remodeling of pulmonary blood vessels. Muscularization and fibrotization of the walls of prealveolar arteries is the main cause of high vascular resistance to lung blood flow in advanced HPH. Structural remodeling results from hypoxia–induced radical injury to lung vessels. Increased release of oxygen radicals and nitric oxide participate Citation[1]. Mast cells attracted to prealveolar vessels express and release collagenolytic metalloproteinases. Turnover of connective tissue proteins is increased Citation[2]. Low molecular weight collagen fragments (matrikines) stimulate, among other factors, mesenchymal proliferation. HPH in adults is completely reversible Citation[3]. On the contrary, the experimental hypoxia in rats applied perinatally results in permanent increase in reactivity of pulmonary vasculature which persists till adulthood Citation[4]. Effect of perinatal hypoxia manifests more in female and depends on activity of ovaries Citation[5].
Supported by grants GAČR 305/05/0672 and Ministry of Education 1M0510.
FC-01-001 Caesarean section or spontaneous birth? maternal request in Germany and USA
B. Schuecking1, C. Hellmers1, A. Sanderson2
1University of Osnabrueck, Osnabrueck, Germany; 2Boston University, Dep. of MCH, SchPH, Boston, MA, USA
Objective: To find out the preferences and predictive impact of healthy first mothers – to be according to mode of birth in correlation to general well being/depression.
Methods: The results to be presented combine the samples of 2 quantitative prospective studies including 366 German and 54 American primiparae: 2 questionnaires used internationally established instruments such as EPDS, WHO5, SOC. T1: 28–35 weeks of pregnancy/T2: 7–18 weeks postpartum. Data analysis with SPSS.
Results: More than 95% of all women in both samples preferred a spontaneous birth, for various reasons. The few women opting for CS were more anxious/depressive. Wish for a CS proved to be predictive for a later CS, whereas a wish for spontaneous birth was not.
Conclusions: The results show – comparable to the literature – that maternal request for CS is not predominant. Those who prefer a CS belong to a vulnerable group.
FC-01-002 Caesarean section on maternal request: A comparison of obstetricians' attitudes in eight european countries
M. Cuttini1, M. Habiba2, M. Kaminski3, M. Da Fré4, K. Marsal5, O. Bleker6, J. Librero7, H. Grandjean8, P. Gratia9, S. Guaschino10, W. Heyl5, D. Taylor2
1Ospedale Pediatrico Bambino gesù, Rome, Italy; 2University of Leicester, Leicester, UK; 3Inserm U.149, Baudeloque, Villejuif, France; 4Agenzia Regionale di Sanità della Toscana, Florence, Italy; 5University Hospital, Lund, Sweden; 6Amsterdam Medical Center, Amsterdam, The Netherlands; 7Salud Publica Area 13, Valencia, Spain; 8Inserm U.518, Hôpital de la Grave, Toulose, France; 9Centre Hospitalier de Luxembourg, Luxembourg, Luxembourg; 10Istituto per l'Infanzia Burlo Garofalo, Trieste, Italy
Objective: To explore the attitudes of European obstetricians to performing a caesarean section on maternal request in the absence of medical indication.
Methods: Within a European collaborative project (EUROBS), NICU-associated maternity units were selected by census in Luxembourg, Netherlands and Sweden, and by geographically stratified random sampling in France, Germany, Italy, Spain, and UK. An anonymous, self-administered questionnaire was used for data collection.
Results: One hundred and five units and 1530 obstetricians participated in the study (response rates 70% and 77% respectively). Compliance with a hypothetical woman's request for elective caesarean section simply because it was “her choice” was lowest in Spain (15%), France (19%) and Netherlands (22%), highest in Germany (75%) and UK (79%), and intermediate in the remaining countries. Using weighted multivariate logistic regression, country of practice, fear of litigation, and working in a University-affiliated hospital were associated with physicians' likelihood to agree to patient's request. The subset of female doctors with children was less likely to agree (OR 0.29, 0.20–0.42).
Conclusions: The differences in obstetricians' attitudes are not founded on concrete medical evidence. Cultural factors, legal liability and variables linked to the specific perinatal care organisation of the various countries play a role. Greater emphasis should be placed on understanding the motivation, values and fears underlying a woman's request for elective caesarean delivery.
FC-01-003 The guidance of labours in women with previous caesarean section in low gestational week
T. Binder1, Z. Hájek2, P. Zoban1, R. Plavka2
1Dep. of OB/GYN 2nd Medical School and Teaching Hospital Motol, Prague, Czech Republic; 2Dep. of OB/GYN 1st Medical School and General Teaching Hospital, Prague, Czech Republic
Type of the study: Randomised prospective study.
Aim: To evaluate the safeness and successfulness of vaginal labors in women with previous s.c. on uterus with non-developed low uterine segment (high placed transverse U scission).
Methodology: In the years 1996–2005, 296 pregnant women with non-complicated U scission in their history were enrolled to the study. 259 of them had noncomplicated course of pregnancy and reached the maturity of the fetus. The criteria of selection for vaginal delivery were from the medical viewpoint the same as in women with classic Geppert s.c., but is necessary to establish that the outcome of previous child has played great role in the decision of the mode of labour.
Results: 166 women were selected for vaginal mode of the delivery. In 129 (78%) of them started labour spontaneously, the mean gestational age was 39 + 6. 37 (22%) women underwent the delicate attempt of labour induction, the mean gestational age was 41 + 3. All labours were monitored continuously. The rate of successful vaginal labours were in the whole group 123 (74%), 107 (83%) in the group with spontaneous beginning of labour and 17 (43%) in the group with induction. The mean of neonate birthweight was 3418 g s.d. 532 g. No case of uterine rupture, blood loss >500 ml or poor neonate outcome. The pospartal digital revision of uterine cavitiy was the method of choice, all women underwent the ultrasound control of uterine wall third postpartal day. The reasons for acute caesarean were in the first group dystokia 14 (64%), signs of fetal imminent hypoxia 7 (32%) and signs of imminent uterine rupture l (4%). In the group with the induction attempt the reasons were the unsuccessful induction of labour 8 (40%), dystokia 7 (35%) and signs of imminent fetal hypoxia 5 (25%). The mean of the birthweight in caesarean group was 3230 g s.d. 615 g.
Conclusions: The vaginal labour in women with previous caesarean made by technique high placed transverse U scission is as safety or risky as the vaginal labour in women which underwent the classic Geppert caesarean. The medical criteria of the selection for vaginal labour also doesn't differ.
FC-01-004 Lack of correlation between rates of caesarean section and perinatal mortality in iceland
R. Bjarnadottir1, G. Jónsdóttir2, A. Smarason3, R. Geirsson1
1National University Hospital, Dept. of Obstetrics and Gynecology, V/Hringbraut, Reykjavik, Iceland; 2University of Iceland, Dept. of Medicine, V/Hringbraut, Reykjavik, Iceland; 3Akureyri Hospital, Dept. of Obstetrics and Gynecology, Eyrarlandsvegi, Akureyri, Iceland
Introduction: Cesarean section (CS) rates have increased over the past decades without a decrease in perinatal mortality (PNM) rate. In Iceland, where the PNM is low, the same trend has been seen. Crude PNM rates give limited information about whether the increase in CS rates leads to a lower perinatal death rate of term non-malformed singletons. The relation between CS and PNM rates in singleton, non-malformed infants of birthweight ≥2500 g in Iceland during 1989–2003 was studied.
Materials and Methods: Information about gestational length, birthweight, parity, onset of labour and previous CS was collected for singleton births ≥2500 g from the Icelandic Birth Registration and maternity case records. The same data were obtained for all perinatal deaths ≥2500 g excluding malformed infants irrespective of mode of delivery. The caesarean section and perinatal mortality rates were calculated and the relation between these evaluated by Pearson's correlation coefficient.
Results: The total number of deliveries in the study period was 64514 and the mean perinatal mortality rate 6.4/1000 (range: 3.6–9.2/1000). A significant increase was found in the overall CS rate, from 11.6% to 18.2% (p < 0.001). There were 61633 singleton infants ≥2500 g and 8332 were born by CS. There were 111 perinatal deaths among this cohort giving a mean PNM rate of 1.8/1000 (range 0.8–4.1/1000). While for singleton non-malformed infants the CS rate increased from 10.4% to 16.7% (p < 0.001), the PMN did not decrease significantly. For primiparous women the CS rate increased from 12% to 18% with no correlation with the PNM (0.6/1000).
Conclusion: Despite a 60% rise in the CS rate during the study period, no reduction of the PNM rate among infants ≥2500 g was found in this population with a prior low PNM, neither among primi- nor multiparous women.
FC-01-005 Elective caesarean section and respiratory morbidity in the neonate
A.K. Hansen, N. Uldbjerg, K. Wisborg, T.B. Henriksen
Perinatal Epidemiology Research Unit, Aarhus University Hospital, Skejby, Aarhus, Denmark
Objective: Elective caesarean section (CS) has been associated with an increased risk of respiratory morbidity in the newborn. Studies have shown a 1.5–15 times increased risk of respiratory morbidity when comparing infants delivered by elective CS to vaginally delivered infants after 37 completed weeks of gestation. The aim of this study is to evaluate the risk of respiratory morbidity in a cohort of women with singleton pregnancies, careful assessment of gestational age and detailed information on indications for CS, taking into account gestational age and potential confounders.
Methods: The study is based on data from The Aarhus Birth Cohort which holds information about 70,000 pregnancies and deliveries. Only women who attended routine antenatal care at Aarhus University Hospital 1989–2005 with singleton pregnancies carried beyond 37 completed weeks were included (n = 63,000). Information on lifestyle factors, social factors, obstetric and medical history and maternal characteristics were obtained from self-administered questionnaires completed in 2nd trimester. Detailed information about pregnancy and delivery was obtained from registration forms completed by the tending midwife, while information about neonatal morbidity (RDS, TTN, PPHN, perinatal asphyxia and sepsis) was obtained from routine discharge registration forms and a structured coding sheet completed by neonatologists.
Results: A total of 2600 (4.2%) infants were delivered by elective CS. Preliminary analysis indicate that approximately 6.1% of the infants delivered by elective CSs were admitted to a neonatal intensive care unit with respiratory morbidity compared to 2.3% of singletons delivered vaginally at 37 weeks or beyond. Further results will be presented.
— Cancelled
FC-02-001 An analysis of caesarean sections performed at our institute in 2003–2005
J. Hanacek, P. Velebil, P. Darebny, J. Feyereisl
The Institute for the Care of Mother and Child, Prague, Czech Republic
Objective: Since the 1980s there has been a significant increase in the incidence of caesarean sections in the Czech Republic. In 1982, the incidence was 8.2%, in 2003 15.75%, and in 2004 already 16.6%. A similar trend is seen in one of the largest perinatology centers in the Czech Republic. In 1982, the incidence was 9.5%, in 2003 19.3% and in 2005 25.7%. It was found that an increase in the incidence of caesarean sections above 10–12%, does not lead to a decrease in perinatal mortality, which in the last 5 years has been around 4.4%.
Methods: A retrospective analysis of all caesarean sections performed at our Institute in the years 2003–2005. In the years 2003–2005, we had 11,258 deliveries, 2551 of these were caesarean sections. We analyzed the data from our electronic database as well as the patients' documentation. We evaluated various patient characteristics: parity, maternal age, BMI, previous obstetric history, and pregnancy complications. Further we analyzed the indications for caesarean section, whether planned or urgent, confirmation of fetal hypoxia, cervical dilatation, spontaneous or induced labour, medications during labour, and results of culture for B-haemolytic Streptococcus. Neonatal status was evaluated using the ABB and 5-minute Apgar score. Other data included in the analysis were type of anesthesia used, complications post-partum, and antibiotic prophylaxis or treatment.
Results: A detailed analysis of the indications for caesarean sections, their clinical outcomes in one of the largest perinatology centres in the Czech Republic.
Conclusion: Knowledge of the spectrum of indications for caesarean section and the relationships among the individual variables could lead to their more specific and rational use.
FC-02-002 Outcomes and complications of repeated (3–8) caesarean sections
M. Khalil
Security Forces Hospital, Malaz, Riyadh, Saudi Arabia
Objective: A prospective study to evaluate outcomes in caesarean sections repeated several times.
Methods: Three hundred and twenty-seven patients who had had three or more (3–8) caesarean sections were studied and compared with a control group of 330 patients undergoing third caesarean section during the period from August 2001–March 2005 at Taif Maternity Hospital and Security Forces Hospital, Riyadh, Kingdom of Saudi Arabia.
Results: Three or more caesarean sections were associated with a longer operative time as well as an increased rate of dense adhesions. There was no significant difference in the blood transfusion rate, Apgar score of the neonate, neonatal admission rate to intensive care unit, uterine scar rupture, placenta praevia, bladder injury, incidence of caesarean hysterectomy, incidence of post partum pyrexia, wound infection, and urinary tract infection between the two groups. There was no maternal death in the two groups.
Conclusion: No absolute upper limit for the number of repeat caesarean sections can be given and no specific additional risk for the mother or the neonate due to the higher order (3–8) caesarean sections.
FC-02-003 Maternal health outcomes and mothers' views of their childbirth experience two years after term breech delivery
J. Molkenboer1, S. Debie1, F. Roumen1, L. Smits2, J. Nijhuis2
1Atrium Medical Centre, Heerlen, The Netherlands; 2University Hospital Maastricht, Maastricht, The Netherlands
Objective: To evaluate maternal health outcomes and mothers' views of their childbirth experience two years after term breech delivery.
Design: A nonrandomized single-centre prospective cohort study.
Methods: Mothers were asked to fill out questionnaires concerning breastfeeding, relationship with infant and partner, health problems, and fertility two years after term breech delivery. Their breech birth experience and their view about the care provided to them while giving birth were also evaluated. Outcomes of the planned caesarean section (CS) group were compared with outcomes of the planned vaginal delivery (VD) group, whether or not a vaginal birth was realized or an emergency caesarean section was performed.
Results: One hundred and eighty-three mothers (90.1%) completed the follow-up questionnaires after two years. Forty-three women were in the planned CS group, and 140 in the planned VD group. In the planned VD group more breech presentations were complete, whereas in the planned CS group more women delivered at ≤41 weeks gestation. No differences in maternal experiences concerning breastfeeding, taking care of her child and the relationship with her partner were found between the two groups. Also no differences were found in all investigated maternal health items, nor in sexual activity or fertility.
Significantly less women in the planned CS group than in the planned VD group felt worried about the health of their baby (25.6% vs. 45.0%, adjusted OR 0.36, 95% CI [0.15–0.91]), and they were more often reassured about their baby's health (67.4% vs. 37.9%, adjusted OR 3.86, 95% CI [1.65–9.06]). Of the women in the planned VD group, 30.7% experienced childbirth as very painful. 46.9% experienced more pain during labour and delivery than expected. In the planned VD group 24.5% of the women indicated they had no active say in decision making, in contrast with 2.3% of the women in the planned CS group (p = 0.001).
Conclusion: Maternal health outcomes two years after term breech delivery were generally not significantly different after planned CS and planned VD, but more women in the planned VD group were worried about their child's health, experienced more pain than expected, and reported less involvement in decision-making.
FC-02-004 Re-attempt of external cephalic version under spinal anaesthesia: Improves successful rate and reduces the force required for successful version
T.Y. Leung1, L.W. Law1, L.W. Chan1, D.S. Sahota1, K.S. Khaw2, T.K. Lau1
1Department of Obstetrics and Gynaecology, The Chinese University of Hong Kong, Shatin, Hong Kong, Hong Kong; 2Department of Anaesthesia, The Chinese University of Hong Kong, Shatin, Hong Kong, Hong Kong
Objective: To investigate if the use of spinal anaesthesia (SA) during re-attempts of external cephalic version (ECV) (1) improves successful rate, and (2) affects the degree of force applied during version.
Methods: Patients with an uncomplicated singleton breech-presenting pregnancy were eligible for ECV without SA. During ECV, the operator wore a pair of gloves which had thin piezo-resistive pressure sensors able to measure the contact pressure between the operator's hands and maternal abdomen (as described in our papers: Citation[1-3]). The total pressure applied during a version attempt was denoted by Pressure-time integral (PTI: mmHgsec). When ECV was failed after 3 trials, patients would then be put under SA. ECV was re-attempted and the applied force was measured in the same manner. The PTI before and after the use of SA were compared (Wilcoxon test).
Results: 5 patients who had a failed ECV without SA underwent a re-attempt with SA. All of them had successful version finally. The PTI of the successful attempts were lower than that of the previous failed attempts performed without SA (p = 0.043) as summarised below:
Conclusion: SA improves the success rate of ECV as well as reduces the force required for successful version.
FC-02-005 Incidence of urinary incontinence and sexual dysfunction in the relation to pregnancy and labour
O. Sottner, J. Zahumensky, M. Krcmar, H. Brtnicka, M. Dvorska, Z. Masopustova, D. Kolarik, D. Driak, K. Hurt, M. Halaska
Department of OB/Gyn, Teaching Hospital Na Bulovce, Charles University, Prague, Czech Republic
Objective: The aim of our study is to objectify the influence of pregnancy and labour on the incidence of urinary incontinence and sexual dysfunction.
Methods: All primiparas who gave birth at our maternity ward from June 12, 2004 through February 28, 2005 were included into our study, i.e. 499 females were asked for cooperation. The data on occurrence of urinary incontinence and sexual dysfunction was collected via two questionnaires. We used modified questionnaires from the Oxford study of Barrett et al. The first questionnaire was distributed on the day two or three after the delivery and the second one six months after it. We had these standard questionnaires in six versions (Czech, English, Chinese, Vietnamese, Russian and Ukrainian). All our findings were statistically analysed.
Results: The response rate was approximately 75%. We found the statistically significant increase in the occurrence of urinary incontinence during pregnancy followed by the significant decrease immediately after the delivery (p = 0.0001). 63% of females reported urinary incontinence at the end of pregnancy on the contrary to the baseline prevalence before it of approximately 15%. This prevalence decreased back to 16% six months after the labour. We proved the significance of just one obstetrical factor – it was the protective influence of Caesarean Section. 43% of females report worsening of sexual life and 19% of them suffer from the significant dyspareunia six months after the labour. We found significance of some risk factors (both obstetrical and else) for the occurrence of dyspareunia – education, episiotomy, rupture of vaginal wall extended to the vault, duration of the second stage of a labour more than 60 minutes and a longer healing process of the wound.
Conclusions: Our results document the importance of pregnancy as a risk period for the onset of urinary incontinence but most of it seems to be transitional. Although we documented some factors for worsening of sexual life after the delivery, we are not able to propose the universally effective recommendations at this stage of our study.
FC-03-001 Yolk sac diameter and shape – predictors of outcome in the first trimester of pregnancy complicated with type 1 diabetes mellitus
M. Ivanisevic1, J. Delmis1, D. Jalsovec2
1Department of OB/GYN, Zagreb, Croatia; 2Department of OB/GYN, Cakovec, Croatia
Information on the predictive value in normal and pregnancy complicated with type 1 diabetes mellitus outcome, of yolk sac (YS) measurement and YS morphology has been scant. During first trimester, peripherally placed (within gestational sac) YS measuring 5 mm or less is likely to be normal. YS may be smaller or larger than 5 mm in abnormal pregnancies than in intact pregnancies of equal size.
Aim: To compare the size and shape at transvaginal sonography (TVS) of the YS in normal and type 1 diabetic pregnancies and to correlate these characteristics with perinatal outcome.
Patients and Methods: 60 healthy pregnancies and 60 pregnancies with type 1 DM underwent TVS in the first trimester to establish the normal size and shape. TVS was performed at least 2 times between 6–12 weeks of menstrual age (MA), and HCG was measured at the same day of the TVS as well.
We calculated the correlation coefficients between YS and menstrual age, YS and crown-rump length, YS and gestational sac diameter and YS and HCG. Student t-test and Mann Whitney test were used for statistical analysis with SPSS 10 software.
Results: The high statistical positive correlation was found between YS diameter and MA, crown rump length and diameter of gestational sac for both studied groups. The YS diameter in type 1 DM pregnancies was statistically significantly larger for MA than that of healthy pregnant women. YS in type 1 DM showed slower regression after 10 weeks of MA than in healthy pregnancies.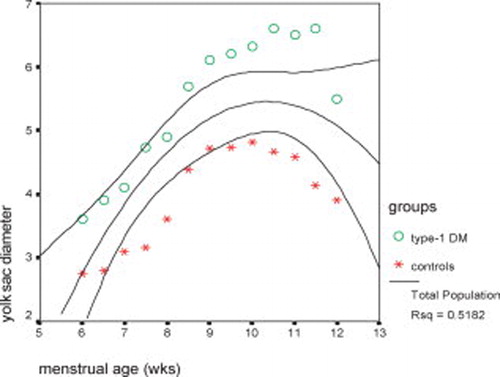
The unfavorable perinatal outcome in healthy pregnant women in this study was connected with YS measuring 5 mm and less with hyperechogenic sonographic characteristics. YS measuring more than 6 mm was found in 30/60 of type 1 diabetes mellitus group. Perinatal outcome was favorable in 20/30 women with large YS and in 10 spontaneous abortion without cytogenetic malformation occurred in the type 1 DM group.
It is unknown if abnormalities of the YS are related primarily to the YS or secondarily to the embryonic maldevelopment. Gross change in its size and/or shape, may indicate or reflect significant dysfunction of the maternofetal transport system in early pregnancy. The larger size of YS could be because of maternal hyperglycemia and accumulation of nutritive secretions not used by embryo, resulting more frequently in diabetic embryopathia.
FC-03-002 Antenatal screening for heritable thrombophilia
D. Tutunaru1, S.I. Avram2
1Elias Emergency Hospital, Marasti, Bucharest, Romania; 2Coltea Clinic Hospital, Bratianu, Bucharest, Romania
Background: Hemostasis represents a delicate balance between thrombosis and bleeding and is coordinated through a large number of interacting proteins. Mutations in some of the genes encoding these proteins have been identified and it is clear that hereditary factors contribute significantly to thromboembolic events that eventually lead to recurrent pregnancy loss.
Aim: To evaluate the prevalence of factor V encoding gene G1691A point mutation among patients with reccurent pregnancy loss.
Materials: Prospective, non-randomised, group controlled study. Inclusion criteria: study group: women in fertile age with recurrent pregnancy loss. These patients were matched for age and gestational status with women with no pregnancy loss. Exclusion criteria: long term use of oral contraceptives, hyperlipaemia, heavy smoking.
Methods: Genetic analysis regarding mutation for genes encoding coagulation Factor V were carried out. Blood samples were processed by hypotonic lysis method for DNA extraction. DNA sample was used as a matrix for a PCR amplification of a mutant region (G1691A) from factor V encoding gene, according to manufacturer instructions, Third Wave, USA. Patient DNA sample was processed in parallel with 4 other DNA control samples: normal, heterozygote, homozygote and blanc.
Results: From 41 cases enrolled in the study group, 13 carried a heterozygote G1691A point mutation (31.7%) and 3 were homozygote (7.3%). The rest of 25 patients were normal. From the 37 control group there were only 2 patients (5.4%) with heterozygote mutation and none with homozygote status.
Conclusion: Antenatal screening for heritable thrombophilia due to factor V mutation is a perfect tool to distinguish between cases of recurrent pregnancy loss due to thrombophilia and those due to immunologic factors as APLS. Thus we could select patients who were reliable for anticoagulant therapy (LMWH) and those who could benefit from immunologic therapy approach (hCG).
FC-03-003 Primary vesicoureteral reflux detected following foetal pelvis dilatation. A prospective clinical and imaging study
J. Goedseels1, M. Alexander1, F. Avni2, M. Hall2, K. Ismaili2
1Hopitaux Iris Sud Universite Libre de Bruxelles, Brussels, Belgium; 2HUDERF Universite Libre de Bruxelles, Brussels, Belgium
Objective: To assess the clinical outcome and imaging features of neonatal primary vesicoureteral reflux (VUR). We also investigated the evolution of renal function in children with high-grade reflux.
Methods: We prospectively followed 43 infants with primary VUR identified among a cohort of 497 infants with foetal renal pelvis dilatation. Postnatal renal US examinations were performed at day 5 and months 1, 3, 6, 12, 24 after birth. Voiding cystourethrography was performed in the neonatal period and repeated at 12 and 24 months when VUR was persistent. At least 2 radioisotopic examinations, including a 99mTc-MAG3 renogram and a plasma clearance of Cr-51 EDTA were performed in all children with high-grade reflux.
Results: The incidence of primary VUR was of 9%. Among the 43 patients followed, 11 (26%) infants had high-grade VUR (IV-V) and 32 (74%) infants had low-grade (I-III) VUR. There was complete resolution of reflux in 2 of 11 (18%) patients with high-grade VUR and 29 of 32 (90.6%) patients with low-grade VUR at 2 years of age (p < 0.001). Whereas 91% of low-grade refluxing kidneys were normal on US at 2 years, this was only the case in 40% of high-grade refluxing kidneys. During follow-up, split renal function was within a normal range and single kidney GFR increased significantly in 13 of 17 high-grade refluxing kidneys between a median age of 3 and 24 months. Furthermore, we found a strong association between hypoplasia and poor renal function outcome.
Conclusion: Reflux resolution and US normalisation were slow in high-grade VUR kidneys. In contrast, renal function maturation occurred in the majority of these cases.
FC-03-004 Assessment of fetal lung maturity by comparing four tests (tap test, shake test, TDx FLM, lamellar bodies)
V. Miketic1, D. Popovic2
1Department of Gynecology and Obstetrics, Clinical Centre of Montenegro, Podgorica, Yugoslavia; 2Department of Laboratory Medicine, Clinical Centre of Montenegro, Podgorica, Yugoslavia
Objective: This study was performed to determine the sensitivity, specificity, predictive positive and negative values of four diagnostic tests of fetal lung maturity (FLM).
Methods: Samples of amniotic fluid were obtained from 166 patients between 28 and 39 weeks of gestation. All patients gave birth within 72 hours following these tests and none received corticosteroids during this period. The neonates observed during 48 hours by attending neonatologist. The results of the tests were compared with the clinical incidence of neonatal respiratory distress syndrome.
Results: The sensitivity of the shake test was 96% for FLM, while for the tap test it was between 98 and 100%, lamellar bodies 96% and TDx 98%. Specificity for tap test were 68–88% correct, while all other tests were 68–70% correct. The positive predictive value for maturity was 98–100% for tap test (5th and 10th min), for shake test 96%, for TDx 98–100% and for lamellar bodies 97%. Negative predictive values were 43–65% for tap test, 47% for shake test, and 45% for TDx and 42% lamellar bodies test.
Conclusion: All tests showed high sensitivity (∼95%) and predictive value for assessing maturity (∼97%). However, they have only modest specificity (∼65%) and low predictive value (∼50%) for immaturity.
FC-03-005 Screening group b streptococcus colonization in 98.6% of pregnant women – is it enough?
C. Santos1, G. Mendinhos1, L. Sancho2, J.M. Garrote1, M.J. Brito1, F. Exposto2, I. Vitorino1, R. Barroso1, H. Carreiro1, M.C. Machado2
1Hospital Fernando Fonseca, Amadora, Portugal; 2Lisbon Tropical Medicine Institute, Lisboa, Portugal
Objective: To determine the prevalence of group B Streptococcus carriers and report the outcome of an intervention to reduce early-onset GBS disease.
Methods: Prospective study, from 1st October 2004 to 31st March 2005, including all pregnant women. GBS was isolated and identified according to CDC recommendations, from vaginal and rectal swabs performed at 35–37 weeks of gestation or during delivery room admission.
Results: Of 2104 pregnant women, 98.6% (2076) were screened, detecting 18% (381) colonized for GBS. We randomly analysed data from 223 GBS carriers and compared it with 223 GBS-negative women. 175 (78%) colonized women were 19 to 34 years, 137 (61%) European women, 121 (54%) with low school grade. There were 158 (70.8%) vaginal deliveries and 47 (21%) caesarean deliveries with labour. Intrapartum chemoprophylaxis was administered properly to 88.7% (134/151) of cases that had indication, to 95% (24/25) of preterm deliveries and to all cases of intrapartum maternal fever (3) and duration of membrane rupture ≥18 hours (14). Serotipe III was the most prevalent (35%).
Comparing above data with those of GBS-negative group (n = 223), we found that GBS-positive culture was more frequent in African women (p = 0.009), with no significant differences about age group, school level, socioeconomic status, parity or misscarriage. Intrapartum chemoprophylaxis was administered to 16.9% (27) of GBS-negative women, with preterm labour (4), membrane rupture ≥18 hours (7), suspected amnionitis (8), intrapartum maternal fever (5) and unknown GBS status (3).
In both groups, there was no neonatal GBS infection, but among the 28 not screened pregnant women, we documented two cases of fatal early-onset sepsis (0.9:1000 live births).
Conclusions: The percentage of screened women was excellent (98.6%) but the existence of two cases of serious neonatal infection strengthens the importance of pregnant women screening and of intrapartum chemoprophylaxis.
FC-03-006 Perinatal management in congenital cystic adenomatoid malformation of the lung (ccaml): 10 years retrospection
R. Devlieger1, N. Raus1, A. Debeer2, K. Allegaert2, J. D'Haese2, M. Cannie3, D. Van Schoubroeck1, L. Lewi1, J. Jani1, C. Vanhole2
1Department of Obstetrics and Gynaecology, Leuven, Belgium; 2Department of Neonatology, Leuven, Belgium; 3Department of Radiology, Leuven, Belgium
Introduction: CCAML is a rare tumour of the fetal lung resulting from disturbed airway embryogenesis. We here wanted to review the perinatal management of fetuses and neonates diagnosed with this condition.
Methods: Clinical antenatal and postnatal charts of all neonates diagnosed with CCAML between 1995 and 2005 were reviewed. Characteristics of prenatal follow-up, birth and postnatal care were retrospectively collected and analysed.
Results: Based on foetal ultrasound, CCAML was diagnosed in 13 cases of which one presenting with hydrops and a large solid lesion died in utero. A second foetus underwent thoraco-amniotic shunting because of a large cystic mass and hydrops. Based on 17 tentative pre-surgical diagnoses in neonates, data on 15 cases of histologically proven CCAML were available for analysis of whom 12/15 were diagnosed before birth. 5/13 were macrocystic, 1/13 microcystic and 7/13 were mixed lesions, 2/15 unclassified. There was no postnatal mortality. 6/15 neonates were asymptomatic at birth and 9/15 displayed respiratory symptoms of which in 6 CCALM was already diagnosed before birth. One neonate was symptomatic at birth following thoraco-amniotic shunting in utero. A second neonate diagnosed before birth with a small cystic lesion developed important air trapping shortly after birth. Of the asymptomatic (n = 8) neonates at birth, 2 neonates were not (yet) operated, 2 underwent surgery after a complication occurred (infection) while 4 underwent elective surgery. Median length of stay after surgery was 10 (6–18) days.
Conclusions: Optimal perinatal management of CCAML involves multidisciplinary collaboration. MRI studies are useful in the antenatal management and diagnosis. Hydrops remains an important prenatal clinical sign, but in the presence of a macrocystic component, thoraco-amniotic shunting can be life-saving. Finally, delivery in tertiary center is advocated even for small lesions because of potential respiratory deterioration at birth.
FC-04-002 High frequency of abdominal pregnancy in east timor and the difficulties with diagnostics
O. Simetka1, S. Huseyn-Zade2, J. Revilla2
1University Hospital Ostrava, Ostrava, Czech Republic; 2UNFPA East Timor, Dili, East Timor
Objective: Presentation of high frequency of abdominal pregnancy cases among East Timorese women.
Methods: Case study.
Results: Over 18 months period we managed 6 cases of abdominal pregnancy in East Timor, a country with population of 1 million. Four mothers presented with post-term pregnancy and dead fetus, 1 presented with alive fetus in breech presentation at term and 1 mother presented at 22 weeks with pregnancy attached to ovary. Only 1 mother was seen antenatally by doctor on ultrasound but the condition was not diagnosed. All mothers experienced abdominal pain between 20–30 weeks, they all felt the pregnancy “different” compared to their previous pregnancies and apart from 1 they all came to hospital only after they stopped to feel fetal movements. In 5 of them labour was induced by prostaglandins and they all underwent surgery indicated for failure to progress. One mother underwent surgery primarily for suspicion of abdominal pregnancy. In 5 cases the placenta was left intact in abdominal cavity, in 1 case the placenta was removed with extensive bleeding, the postoperative period has been uneventful in all cases. The resorption of the placenta took several months.
Conclusions: Term abdominal pregnancy is a rare diagnosis with higher frequency in developing countries with inadequate antenatal care. If not diagnosed early, the diagnosis after 20 weeks is very difficult. Ultrasound, external and vaginal examination are helpful but often the diagnosis comes as a surprise during “caesarean section”. When diagnosed before 24 weeks, a laparotomy is indicated, otherwise it should be observed and removed after 36 weeks. Removing abdominal pregnancy can be difficult, abdominal cavity must be entered carefully so as to avoid placenta or adherent bowels. Placenta should be left in the abdomen and no drain inserted to avoid introduction of infection.
FC-04-003 Hemodynamic examination of fetal cardiopathies with doppler-echocardiography
M. Katona1, H. Orvos2, K. Mader1, E. Horvath3, A. Pal2
1Department of Pediatrics, University of Szeged, Koranyi, Szeged, Hungary; 2Department of Obstetrics and Gynecology, University of Szeged, Semmelweiss, Szeged, Hungary; 3Department of Genetics, University of Szeged, Somogyi, Szeged, Hungary
Examination of the fetal heart with echocardiography often fails to reveal the severity of cardiopathy. Abnormal hemodynamics, as heart failure, decreased cardiac output can be assessed with fetal color Doppler-echocardiography (FCDE).
Aim: This study was performed to evaluate the prognosis of fetal cardiopathies by measuring cardiac function with FCDE.
Patients and Methods: 1524 pregnancies were examined between the 17–40 gestational weeks during 6 years. Cardiopathy was revealed in 51 fetuses, who were then examined with FCDE. Doppler velocimetry was used to measure blood flow through the ductus arteriosus (DA), ductus venosus (DV), aorta, pulmonary artery (PA), tricuspid valve and mitral valve using an ACUSON XP-128 Doppler-echocardiograph with a 7 MgHz transducer.
Results: 33 congenital heart defects (CHD), 8 fetal hydrops, 3 cardiomyopathies (CMP), 5 sustained tachycardias (ST) and 2 twin-to-twin transfusions (TTT) were diagnosed. Tricuspid insufficiency (TI), retrograde aortic flow and inverted DV flow were found in fetuses with hypoplastic left heart syndrome (8 cases). Mitral insufficiency (MI) and decreased PA flow were found in 2 cases with CMP and in 2 cases with right heart obstruction. Simultaneous evaluation of left ventricular inflow and outflow was successful in diagnosing the origin of ST requireing antenatal medication (digoxin, verpamil). TI and/or MI was detected in 8 fetuses with hydrops and in 2 fetuses with TTT. There were 18 deaths (8 abortions, 1 in utero death and 9 postnatal deaths); 9 neonates underwent cardiac surgery.
Conclusions: 1) Assessment of the severity of cardiopathies with FCDE provides clues for the indication of antenatal therapy or cardiac surgery. 2) Retrograde flow in the great arteries from the DA confirms a ductal-dependent CHD. 3) Pulmonary velocity higher than aortic velocity confirms CHD with right heart obstruction. 4) Severe TI and/or MI and/or reverse DV flow in fetuses with CHD was predictive for increased mortality.
FC-04-004 Prediction of term birth weight based on ultrasound and maternal characteristics
M.G. Halaska1, R. Vlk1, P. Feldmar1, M. Hrehorcak1, M. Krcmar2, I. Mala3, L. Rob1
12nd Medical Faculty, Charles University, Prague 5, Czech Republic; 21st Medical Faculty, Charles University, Prague 8, Czech Republic; 3University of Economics, Prague 3, Czech Republic
Objective: The aim of the study was to compare an ultrasound-based prediction formula of Shepard, Hadlock, our new equation and equation of Nahum based on maternal characteristics.
Methods: We have collected three groups of healthy term pregnant women: 125 (Group A) and 130 (Group B), 225 (Group C). We performed standard ultrasonographic measurements and recorded maternal characteristics. A new birth weight equation was developed by multiple stepwise regression analysis from the Group A data and then compared to the different birth weight prediction equations of Hadlock, Shepard and Nahum. The accuracy to predict birth weight over 4000 g using ultrasonographic methods was tested on Group C.
Results: New prediction equation: log10 EFW = 0.64041 ∗ BPD−0.03257 ∗ BPD2 + 0.00154 ∗ AC ∗ FL. The results of our new (Halaska's) ultrasound estimations are comparable to Hadlock's equation. Halaska's estimation method exhibits higher overall accuracy, Hadlock's estimation provide better prediction of fetuses over 4000 g. Both equations are superior to Shepard and Nahum's equations. The Nahum's equation is comparable to the Shepard estimation.
Conclusions: The Halaska and Hadlock's estimations are comparable to one another; the Nahum's equation is comparable to Shepard's and can be used as simple, inexpensive and approximative estimate.
FC-04-005 Planned and unplanned pregnancy – comparison of a female sexuality and the course of a labour
J. Zahumensky, O. Sottner, M. Krcmar, H. Brtnicka, M. Dvorska, Z. Masopustova, D. Kolarik, D. Driak, M. Halaska
Department of Ob/Gyn, Teaching Hospital Na Bulovce, Charles University, Prague, Czech Republic
Objective: The aim of this study is to compare several parameters of sexual life and the course of a labour in women with planned and unplanned pregnancy.
Methods: 339 primiparas participated in our study. They filled in questionnaire concerning their sexual life during pregnancy on the second day after the delivery. We used a modified questionnaire from the Oxford study of Barrett et al. and we had it in six versions (Czech, English, Chinese, Vietnamese, Russian and Ukrainian). One question also stressed planning of pregnancy. 246 females (72.57%) indicated planned pregnancy and 93 pregnancies (27.43%) were not planned. There were no significant differences in variables e.g. age or marital status between these two groups. All our findings were statistically analysed.
Results: There was a significant decrease of a coital activity, number of orgasms and increase in sexual dysfunctions in pregnancy in the whole study group. Significant differences between women with planned and unplanned pregnancy were observed only in the frequency of vaginal dryness and pelvic pain. We indicated that the positive relation to the fetus develops successively during pregnancy in women becoming pregnant accidentally as well as in women desiring a baby. The equal rate of partner's presence at delivery shows the high involvement of the partners of unmarried women.
Conclusions: According to the results of our study, unplanned pregnancy has no adverse effect on parameters of the course of a labour but it has impact on the sexual life of female.
FC-05-001 Both first trimester crown rump length and maternal serum levels of pregnancy associated plasma protein a are independent predictors of birth weight
T.Y. Leung, L.W. Chan, D.S. Sahota, T.N. Leung, T.Y. Fung, L.W. Law, T.K. Lau
The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, Hong Kong, Hong Kong
Objective: To study if first trimester crown rump length (CRL), maternal serum levels of pregnancy associated plasma protein A (PAPP-A) and free beta-human chorionic gonadotropin (fb-hCG) are independent predictors of second trimester fetal growth parameters.
Methods: It was a prospective observational study over 1 and half year in patients underwent first trimester combined screening for Down's syndrome in a University Fetal Medicine Unit. After excluding cases with multiple pregnancies and congenital malformations, fetal CRL (expressed in standardised z score (z-CRL)), maternal PAPP-A and fb-hCG levels (expressed in log10 of multiple of medians) were correlated with birth weight (z-BW) using Pearson test, followed by multiple regression analysis. The sensitivity for small for gestational age (SGA, defined as birth weight less than 5th percentile) using these predictors were then analysed.
Results: A total of 2760 cases were included. All z-CRL, log10 PAPP-Amom, and log10 fb-hCG were positively correlated with z-BW (p < 0.01), but only z-CRL and log10 PAPP-Amom were independent predictors (p < 0.01). Both CRL and PAPP-A had a sensitivity of 10.7% for SGA at a false-positive rate of 7.4% and 4.7% respectively. By combining the two markers, the sensitivity increased to 17.5% at a false-positive rate of 11.3%.
Conclusion: First trimester CRL and PAPP-A are independent factors that influence the final birth weight. Combination of these two markers detects 17.5% of SGA at a false-positive rate of 11.3%.
FC-05-002 Complete fetal heart block: A case of successful in utero therapy
C. Cardoso, L. Graca, A. Marques
Hospital de Santa Maria, Lisbon, Portugal
Congenital complete heart block is often associated with maternal anti-SSA/Ro and/or anti-SSB/La antibodies, which injure the fetal cardiac conduction system and the myocardium. This situation usually has a poor prognosis.
Clinical Case: Our case refers to an apparently healthy 33-year-old woman, gravida 3, para 1, medical termination 1. Her 1st pregnancy was uneventful and a healthy baby was born. During her 2nd pregnancy a fetal bradyarrythmia was detected at 24 weeks gestation. The echocardiogram confirmed a complete atrioventricular (AV) block with a ventricular rate of 40 beats/min. No structural cardiac anomalies were present but the fetus was severely hydropic and a medical termination of pregnancy was decided. Subsequent investigation revealed the presence of maternal anti-SSA and anti-SSB antibodies. At the index pregnancy, a fetal bradyarrhytmia was noticed at 25 weeks. The echocardiogram showed a structurally normal heart with a complete AV block and a ventricular rate of 55–60 beats/min. No signs of cardiac insufficiency were present. Medical therapy was initiated – dexametasone 4 mg/day until the end of pregnancy. Ultrasonographic surveillance revealed persistence of the block with a ventricular rate of 60 beats/min and absence of cardiac insufficiency. A repeat caesarean section occurred at 35 weeks. A 2.250 g baby with a ventricular rate of 60 beats/min was born. He is now 4 months old and is doing well with no need for a pace-maker.
Comment: As suggested in recent literature, our case underlines the fact that congenital complete fetal heart block associated with maternal anti SSA and/or anti SSB antibodies, may respond to steroid therapy.
FC-05-003 Results of fetal renal pyelectasis at 18–23 weeks ultrasound in an unselected population
M. Khalil
Security Forces Hospital, Malaz, Riyadh, Saudi Arabia
Objective: A prospective study to evaluate the value of mild or moderate/severe fetal renal pelvis dilatation detected at 18–23 weeks in an unselected obstetric population in the prediction of significant need post-natal treatment.
Methods: During the period from August 2001–January 2005 at Taif Maternity Hospital and Security Forces Hospital, Riyadh, 204 women with fetal hydronephrosis, detected at 18–23 weeks' gestation, in a routine obstetric population were studied. Fetal hydronephrosis was diagnosed as ‘mild’ if the antero-posterior renal pelvic diameter (APRPD) measured ≥4 mm (group A) and as ‘moderate/severe’ if the APRPD measured ≥7 mm (group B). The postnatal outcome of fetuses with persistent hydronephrosis (≥10 mm in the third trimester) was determined.
Results: Fetal hydronephrosis was identified in 1.7% (206/12,000) of women. Mild hydronephrosis was present in 77% (157/204 group A) and moderate/severe hydronephrosis in 23% (47/204 Group B). The hydronephrosis resolved in the antenatal and early neonatal period in 83.5% (147/176) of fetuses. None of the fetuses with mild hydronephrosis, 33.3% (14/42) of fetuses with moderate/severe hydronephrosis in the second trimester and 19.7% (14/71) of fetuses with persistent moderate/severe hydronephrosis in the third trimester required postnatal surgery.
Conclusion: This study has highlighted the excellent prognosis associated with mild hydronephrosis found at 18–23 weeks' gestation and has stressed the need for thorough urological assessment of neonates with an antenatal diagnosis of moderate/severe hydronephrosis, as defined by third-trimester APRPD of ≥10 mm.
— Cancelled
FC-05-005 Prevalence of factor v leiden, prothrombin G20210a, mthfr C677t and selected pregnancy variables in women with placental abruption
M. Procházka1, M. Lubušký1, L. Slavík2, M. Kudela1, P. Lindqvist3
1Department of Obstetrics and Gynecology, Medical Faculty of Palacký University, Olomouc, Czech Republic; 2Department of Hematooncology, Medical Faculty of Palacký University, Olomouc, Czech Republic; 3Department of Obstetrics and Gynaecology, University Hospital MAS, Malmö, Sweden
Objective: A growing view holds that inherited or acquired thrombophilia may predispose to a woman towards an adverse pregnancy outcome. The aim of this study was to investigate risk factors for placental abruption due to such thrombophilias (as carriership of factor V Leiden, prothrombin G20210A gene mutation and homozygous MTHFR C677T); and to determine if anamnestic variables such as heredity of thrombosis or recurrent fetal loss might be used as a predictor for placental abruption.
Methods: A retrospective case-control study at the University Hospital, Palacky University, Olomouc, Czech Republic. One hundred and eighty women with placental abruption out of 20,175 deliveries (0.79%) who were compared to 196 unselected gravidae. A detailed anamnesis was taken with special reference to factors related to hypercoagulation and blood was drawn for PCR analysis. The prevalence of factor V Leiden, prothrombin G20210A and MTHFR C677T and selected anamnestic variables were related to placental abruption.
Results: In 20/142 cases (14.1%) the heterozygous form of FVL was present in the placental abruption group, as compared to 10/196 (5.1%) among the control group (odds ratio [OR] 3.0 95% confidence interval [CI] 1.4–6.7). As compared to controls, women with placental abruption were related to an 12-fold increased prevalence of prior recurrent fetal loss and an 6-fold increased prevalence of heredity of thrombosis.
Conclusions: We found that factor V Leiden, recurrent fetal loss, and heredity of thrombosis to be significant risk factors for placental abruption.
The study was supported by the grant of the Ministery of Health of the Czech Republic IGA MZd. NH/6986-3, 2002.
FC-05-006 Practical usefulness of common tests for prenatal inflammation in severe prematurity
P. Kopecký1, V. Sebroň1, R. Plavka1, I. Vítková2, Z. Hájek1
1Department of Obstetrics and Gynaecology – Neonatology, General Hospital Prague, Prague 2, Czech Republic; 2Institute of Pathology, General Hospital Prague, Prague 2, Czech Republic
Objective: Prenatal inflammation is related to the increased perinatal morbidity and mortality. The purpose of this study is to verify the value of common diagnostic tests of prenatal inflammation in current clinical practice.
Methods: In 245 premature infants born between 23 + 0 and 30 + 6 gestational weeks (median 28 + 2) with birth weight from 370 to 1890 g (median 1030) histological examinations of placenta and umbilical cord were performed (according to Salafia). Capability of the following signs to detect histologicaly proven inflammation were tested: maternal temperature >37.5°C (MT > 37.5), vaginal discharge (VD), PPROM, PPROM > 24 hours, CRP > 8 and >19 mg/l, WBC > 15 × 109/l, positive vaginal swab and positive GBS culture using sensitivity, specificity, positive predictive value and negative predictive value calculations for each test.
Results:
Conclusions: Clinical signs of inflammation are more specific, laboratory signs more sensitive. GBS colonisation increases the risk of prenatal inflammation. This analysis supports the idea that common diagnostic tests can help to diagnose prenatal inflammation in a part of pregnancies at risk for premature labour but are not sensitive enough to rule it out in the rest.
FC-06-001 Maternal complication rate and perinatal mortality data do not justify the first trimester reduction of triplets to twins
E. Hruby
1st Department of Obstetrics and Gynecology, Semmelweis University Faculty of Medicine, Budapest, Hungary
Objective: To justify or to reject the concept of first trimester reduction of triplets to twins based on the maternal complication rate and perinatal mortality data observed in triplet and twin population of a single institute.
Methods: We conducted a prospective cohort study comparing the maternal complication rate (premature labour, pregnancy induced hypertension, gestational diabetes mellitus, thrombocytopenia, postpartum bleeding and surgery) and the perinatal mortality data (late fetal death, early and late neonatal death, perinatal mortality) in triplets and twins. The study group consisted of 103 triplets delivered between 1st September 1990 and 31st August 2005 in our institution (inclusion criterion: all 3 fetuses were alive in the 20th weeks of pregnancy). The control group consisted of 152 twin pairs delivered in the last 9 months of the study period in the same institution (inclusion criterion: both of fetuses were alive in the 20th weeks of pregnancy, exclusion criterion: embryo reduction of high order multiple pregnancy to twins in the first trimester). The statistical comparison was made with Fisher's exact test and Student's t-test as appropriate. The level of significance was set as two tailed p < 0.05.
Results: The rate of midtrimester pregnancy loss was 3.88% in triplets and 3.28% in twins (NS). The median of the maternal age at delivery was 30 (20–39) and 31 (17–42) years (NS). The rate of pregnancy induced hypertension, gestational diabetes mellitus, premature labour and thrombocytopenia were 8.18% vs. 16.64% (NS), 17.17% vs. 12.24% (NS), 60.6% vs. 34.69% (NS) and 19.19% vs. 15.64% (NS) respectively. The rate of postpartum bleeding and postpartum surgery (hypogastric artery ligatura, hysterectomy) were 10.1% vs. 8.64% (NS) and 1.01% vs. 3.4% (NS). The gestational age at delivery was 31.8 ± 2.74 and 33.4 ± 3.77 weeks (p = 0.001). The birth weight was 1677 ± 425 and 2019 ± 698 g (p < 0.001).
The rate of the late fetal death, early and late neonatal death were 20.2‰ vs. 34.0‰ (NS), 48.1‰ vs. 14.0‰ (p = 0.02) and 13.7‰ vs. 17.6‰ (NS). Neonatal mortality (early and late) was 61.8‰ vs. 31‰ (NS). Perinatal mortality was 80.8‰ in triplets and 64.6‰ in twins (NS). The perinatal mortality after exclusion of fetuses delivered before the 24th weeks of pregnancy and/or birth weight <500 g was 57.2‰ vs. 64.6‰ (NS), respectively.
Conclusions: The maternal mortality rate and the perinatal mortality data do not support the indication of first trimester reduction of triplets to twins from a biological aspect. Social aspects were beyond the scope of our study.
FC-06-002 Comparison of pregnancy course and outcome with color and radiographic angiography of the placenta in a monochorionic triplet pregnancy
A.J. Kruse1, M. Havenith2, B. Arabin3
1Department of Perinatology, Isala Clinics, Zwolle, The Netherlands; 2Department of Pathology, Isala Clin, Zwolle, The Netherlands; 3Clara Angela Foundation, Witten, Germany
Objective: The pathophysiology of feto-fetal transfusion syndrome (FFTS) is linked to placental vascular anastomoses between monochorionic (MC) monozygotic fetuses and an unbalanced interfetal transfusion mediated by arterio-venous (AV) anastomoses with inadequate compensation along superficial arterio-arterial (AA) anastomoses. We have analyzed “inter-triplet” vascular anastomoses by color and contrast computer angiogram and compared the findings with the development and outcome in a MC triplet pregnancy.
Methods: A patient with spontaneous MC triamniotic triplet pregnancy developed symptoms of FFTS at 18 weeks of gestation with one donor (oligohydramnios) and one receptor (polyhydramnios) triplet. Amniotic-fluid volume returned to normal after 24 weeks. At 32 weeks, a caesarean section was performed due to intra-uterine growth restriction of the donor triplet. Postpartum placental color and contrast computer angiograms were performed to demonstrate inter-triplet superficial (AA or veno-venous) and deep (AV) anastomoses.
Results: Placental color angiograms identified only AA anastomoses between all triplets, and not AV anastomoses. Tiny deep vascular AV communications were only found by computer angiography between the placental circulation of two of the triplets who had appeared as donor and recipient that were not seen by placental color angiogram.
Conclusions: All triplets of this pregnancy developed uneventfully. It seems probable that this was due to the kind of AA anastomoses present between all triplets and the kind of deep AV anastomoses present only between two triplets. Detailed analysis of placental vascular communications by use of color injection angiogram of the chorionic plate and computer angiogram demonstrating deep anastomoses beneath the chorionic plate helps to understand the individual pathophysiology and clinical course in patients with FFTS, which is even more complex in MC triplet compared to MC twin pregnancies.
FC-06-003 Intrauterine laser therapy in twin-to-twin transfusion syndrome improves outcome of very preterm infants
R. Lenclen, A. Paupe, M. Deleplanque, S. Couderc, M. Nassar, Y. Ville
Departments of Neonatology and Obstetrics, Centre Hospitalier Poissy-St Germain, Poissy, France
There remain significant perinatal mortality and morbidity in pregnancies complicated by twin-to-twin transfusion syndrome (TTTS), principally related to the high preterm birth rate. Serial amnioreduction is still the most widely used therapy. More recently, endoscopic laser coagulation of anastomoses has been reported to improve survival in a randomized control study.
Objective: To evaluate the impact of treatment modalities on neonatal outcome in MC pregnancies complicated by TTTS managed in a specialised center for laser therapy.
Methods: In this retrospective study, neonatal outcomes of 64 MC twin pregnancies with TTTS (110 infants) delivered between 24 and 34 weeks of gestation at our center between 2000 to 2005 were collected. Data were analysed according to treatment modalities: laser therapy (LASER group; n = 80 infants) vs. amnioreduction (AMNIO group; n = 30 infants).
Results: Gestational age (29.8 ± 3.1 vs. 29.3 ± 2.5, p = 0.45) and birth weight were not different between groups. The neonatal mortality rate in the LASER and AMNIO group was 9% and 33% respectively (RR = 0.42, 95% CI 0.27–0.66; p = 0.001). The rate of severe cerebral lesions on ultrasound was lower in the LASER group (14.1% vs. 33%; RR = 0.48, 95% CI 0.27–0.87; p = 0.003). The incidence of adverse neonatal outcome (neonatal death, major neonatal morbidity, or severe cerebral lesions) was lower in the LASER group (16.3% vs. 43.3%; RR = 0.52, 95% CI 0.34–0.79; p < 0.001). Logistic regression analysis demonstrated that gestational age and laser therapy are independent significant protective factors of adverse neonatal outcome.
Conclusions: Laser therapy is associated with a higher neonatal survival rate and reduced neurological adverse outcome.
FC-06-004 Monochorionic twins affected by ttts treated in utero with laser: Long-term neurologic and neurodevelopmental evaluation
C. Ruiz, I. Ridaura, J. Perapoch, E. Gratacos, M. Olivares
Vall d'Hebron Hospital, Barcelona, Spain
Objective: Long-term neurologic and neurodevelopmental evaluation of a group of monochorionic twins affected by TTTS treated with selective endoscopic laser photocoagulation.
Methods: We evaluated 64 children between 11 and 17 months old with a standardized neurologic examination and the Bayley Scales for Infant Development-II. The neurologic examination is defined as normal or abnormal and the neurodevelopment is defined by a psychomotor development index (PDI) and a mental development index (MDI) as normal, mildly delayed or significantly delayed.
Results: Neurologic examination was normal in 89.1%. Both normal mental and psychomotor development was found in 57.8%, while 42.2% presented delayed psychomotor development (significant in 14.1%). Mental development was normal in 85.9% of cases, and severely delayed only in 1.6%. We found statistical significance in the association between <32 weeks gestation and abnormal neurologic examination (p < 0.05), and also between <28 w and MDI score (p < 0.001). There was a strong statistical significance between the “Single twin alive” group and abnormal neurological examination (OR 8.4, 1.4–48.4), delayed MDI (OR 7.1, 1.5–32.9) and significantly delayed PDI (OR 15.0, 2.5–88.4).
Conclusions: The more premature infants were, the more likely they were to be neurodevelopmentally handicapped. The greatest risk factor for an abnormal neurological examination and a retarded psychomotor and mental development was the single intrauterine death of one fetus. Our results are similar to other important researches' and support the laser technique for the management of TTTS.
FC-06-005 Neonatal outcome in monochorionic twins with twin-to-twin transfusion syndrome and dichorionic twins: A case control study
R. Lenclen, A. Paupe, M. Deleplanque, F. Castela, B. Nassar, Y. Ville
Departments of Neonatology and Obstetrics, Centre Hospitalier Poissy-St Germain, Poissy, France
Monochorionic (MC) pregnancies complicated by twin-to-twin transfusion syndrome (TTTS) are at increased risk for prematurity as well as perinatal mortality and morbidity. Although perinatal outcome in TTTS has improved after laser therapy, neonatal mortality and morbidity remain high. The respective role of prematurity and of fatal disease are ill-defined.
Objective: To compare neonatal outcomes between TTTS infants and dichorionic (DC) twins, and to evaluate the impact of TTTS treatment modalities.
Methods: This was a case-control retrospective study carried out between 2000–2005. Neonatal outcome was assessed in 122 TTTS infants treated in utero with laser (n = 45 pregnancies) or other therapies (n = 26 pregnancies). Control group consisted of 122 DC twins (81 DC pregnancies) delivered between 24–34 weeks of gestation and matched for gestational age at birth with the cases.
Results: Gestational age at delivery was similar in both groups (median = 29.0, IQR 27.0–32.0 wks), as well as birth weight. Overall incidence of adverse outcome was significantly higher in TTTS infants than in the DC group both in terms of neonatal mortality (17.5% vs. 8%; p = 0.05) and of severe cerebral lesions (22.7% vs. 10.7%; p = 0.03). This difference was mainly due to the subgroup of TTTS infants not treated with laser who had the highest mortality and neuromorbidity rates. Neonatal outcome in the sub-group of TTTS infants treated with laser was not significantly different from those of DC infants: mortality (9% vs. 9.2%), severe cerebral lesions (12.8% vs. 7.9%).
Conclusion: Neonatal mortality and morbidity rates are higher in TTTS infants than in DC infants matched for gestational age, but this difference is significantly reduced in cases treated with laser in utero.
FC-06-006 Neonatal outcome of 189 triplets
T. Wörner, J. Sanchez-de-Toledo, J. Perapoch, R. Rossich, T. Higueras, A. Fina
Vall d'Hebron Hospital, Barcelona, Spain
Objective: To determine neonatal morbidity and mortality in triplets.
Method: Retrospective study of 189 triplets born between January 1998 and December 2004.
Results: Mean maternal age was 33 years. 71.4% of pregnancies were achieved using fertilization techniques. 84.1% received antenatal steroids. 96.8% were born by caesarean section. The mean gestational age was 32 weeks (246–355), with a mean birth weight of 1500 g (450–2660). 53.4% were female. 81.6% did not need cardiopulmonary resuscitation (CPR) at birth, 13.5% needed ventilation with bag-mask and 4.9% required advanced CPR. 27% of the infants presented low/moderated respiratory distress syndrome (oxygen/CPAP), and 19% required mechanical ventilation and surfactant. 12.2% showed patent ductus arteriosus, 4.4% necrotizing enterocolitis, 18% sepsis, 1.7% grade III retinopathy and 12.4% bronchopulmonary dysplasia. 3.9% presented grade III intraventricular haemorrhage, 0.6% grade IV and 3.3% periventricular leukomalacia. Survival rate at discharge from hospital was 95.2%. 13.3% of the survivals showed risk of serious sequelae defined as: grade III–IV intraventricular haemorrhage (6 of 180 survivals), periventricular leukomalacia (6 cases, 5 of them associated with grade III–IV intraventricular haemorrhage), grade III retinopathy (2 cases) and broncopulmonary dysplasia(22 cases).
FC-07-001 Cervical ripening with prostaglandin-e2 at preterm
N. Melamed, A. Ben-Haroush, E. Hadar, R. Chen, Y. Yogev, M. Hod
Department of Obstetrics and Gynecology, Rabin Medical Center, Petah Tiqwa, Israel
Objective: To evaluate the efficacy and safety of PGE2 for cervical ripening at preterm and to identify factors predicting induction failure and mode of delivery.
Methods: The study group included women admitted for cervical ripening with PGE2 vaginal tablets at preterm (gestational age <37 weeks) with a Bishop-Score <7 (group 1, n = 444). PGE2 vaginal tablets were administrated at 6–8 hour interval until either cervical ripening was achieved or ripening failure (Bishop-Score < 7 after administration of four PGE2 tablets). Data were compared to women with spontaneous onset preterm labor (group 2, n = 684) and women admitted for cervical ripening with PGE2 vaginal tablets at term (group 3, n = 1029). A multivariate logistic regression analysis was performed to detect factors predicting induction failure and mode of delivery.
Results: Women at preterm required a significantly higher number of PGE2 tablets compared to women at term (2.0 ± 1.1 vs. 1.6 ± 0.9, p < 0.001). The overall induction failure and caesarean section rates associated with labor induction at preterm were significantly higher than at term (37.7% vs. 2.4% and 25.9% vs. 16.9%, respectively, p < 0.001), and were inversely related to gestational age. Maternal age, nulliparity, gestational age, P-PROM, and the number of PGE2 tablets used were significant predictors of induction failure and caesarean section. Perinatal outcome was similar for the three groups.
Conclusions: The use of PGE2 for cervical ripening at preterm appears to be safe, but may be associated with increased risk for induction failure and caesarean section, especially among women of older age, nulliparas, and at gestational age <32 weeks.
FC-07-002 Expectant management in patients with cervical dilatation (5–10 cm) or protrusion of membranes
A. Merien2, F. Tjin Asoe1, D. van Zoeren1, J. van Eyck1, B. Arabin2
1Department of Perinatology and Neonatology, Isala Clinics, Zwolle, The Netherlands; 2Clara Angela Foundation, Witten, Germany
Objective: Fetal Inflammatory Response Syndrome (FIRS) is increased in early spontaneous preterm birth (SPB). Risks of prematurity and infection have to be balanced and analyzed in cases with progressive dilatation.
Methods: In selected patients with a cervical dilatation of >5 cm or ballooning, pregnancy was prolonged for ≥2 days. Patients were monitored for maternal or fetal infection. Corticosteroids and tocolysis were administered. In exceptional cases with vaginal fetal position, peridural anaesthesia was performed during several days. Postnatally, neonates were examined for sequelae of infection and prematurity.
Results: Up to now, 13 singleton, 10 twin and 2 triplet pregnancies with a mean gestational age at admission of 26 + 5 (21–29 + 6) gestational weeks were included. The mean prolongation of pregnancy was 13 (2–48) days. The mean gestational age at birth was 28 + 2 weeks. Out of the 39 neonates there was 1 neonatal death, no severe asphyxia but some neonatal complications: Persistent ductus arteriosus: 11, IVH grade 3–4: 5, clinical signs of sepsis: 14, positive blood culture: 7, BPD: 12, PVL: 7.
The perinatal and neonatal mortality was 1/39, which is lower than expected according to gestational age at birth. Long-term follow-up will be investigated.
Conclusions: According to the literature, microbial invasion of the amniotic cavity occurs in up to 50% in women presenting with cervical dilatation in the midtrimester, in general in 20% of singleton and around 10% of twin pregnancies. However, these data do not necessarily reflect the rate of neonatal complications. This is a pilot study to evaluate whether prolongation of pregnancy might be justified to prevent prematurity but taking the risk of FIRS. Prospective trials should be performed to further evaluate whether prolongation of more than 48 hours is a reasonable approach in those patients if there is a safety net to deliver patients with symptoms of infection.
FC-07-003 Study of the use of atosiban in hospital sant joan de deu (barcelona)
N. Porta, A. Torres, M.D. Gomez, S. Ferrero, S. Cabre, E. Marimon, J.M. Lailla
Servei d'Obstetricia i Ginecologia, Sant Joan de Déu University Hospital, Barcelona, Esplugues de Llobregat (Barcelona), Spain
Objective: Preterm labour is the main cause of perinatal morbimortality. In our hospital we have been using atosiban for 2 years and the objective of this study is to evaluate the results. Our treatment guidelines include atosiban as first tocolytic option in multiple pregnancies, gestational diabetes and ritodrine contraindication or intolerance.
Material and Methods: A retrospective, observational study was carried out at the Sant Joan de Déu University Hospital. All the patients who have received atosiban treatment since May 2003 to December 2005 were studied.
Results: 106 patients were included until July 2005. Of these patients, 47 (44.3%) were singleton pregnancies and 59 (53.7%) were multiple pregnancies. The 6.6% of patients presented premature labour before 25 weeks of pregnancy, the 26.4% between 25 and 30 weeks, and the 54.7% between 30 and 34 weeks. Among patients without premature rupture of membranes, only in the 6.1% the labour could not be stopped and the labour occurred before 24 hours, making impossible the two doses of corticoids to promote maturation of fetal lungs. The secondary effects were vomiting in the 4.8%, hypotension in the 1.8%, cefalea in the 0.9% and severe complications as acute pulmonary edema were observed in 2 cases (1.8%). The perinatal morbimortality was determined by the gestational age. The mean weight was 2306 ± 1390 g. There were 5 cases of exitus, all in newborns with less than 26 weeks. Other major neonatal complications as pulmonary distress were observed in the 11.1% and jaundice in the 9.5%.
Conclusions: Atosiban is a valid tocolytic therapeutic option in selected cases, with few secondary effects and good perinatal results.
FC-07-004 Pprom between 19 and 28 weeks pregnancy
M. Aerts, C. Van Mol, C. Vandeputte, T. Vanderheyden
St. Augustinus, Wilrijk, Belgium
Objective: Preterm premature rupture of membranes (PPROM) is a serious cause of neonatal complications such as pulmonary hypoplasia. The purpose of the study was to determine the effects of PPROM and to give better counselling to the parents.
Methods: We retrospectively identified 12 patients with PPROM from 19 to 28 weeks. All cases were managed expectant based on the same treatment protocol (beta-methasone and 10 days of oral antibiotics). The latency period, gestational age (GA) by PPROM and delivery, birth weight, days of ventilation and serious complications in mother and child were noted.
Results: The median GA at presentation of PPROM was 24 weeks and 3 days (19 5/7–27 3/7) and at delivery 28 weeks 3 days (24–31 5/7). The median latency of PPROM was 27 days (3–67). Maternal sepsis did not occur. The median neonatal birth weight was 1152 g (830–1800). All babies were ventilated, of which one baby only for 2 hours before starting respiratory support and the longest ventilation was 36 days. The median was 11 days. The baby with PPROM from 19 weeks 5 days died 10 hours after birth, due to extreme pulmonary hypoplasia, complicated by bilateral pneumothorax. Other complications were: pneumothorax (1/12), broncho-pulmonary dysplasia(2/12) not oxygen-dependant at discharge, pulmonary hypertension (1/12) and neonatal sepsis (1/12). Complications due to prematurity also occurred: a grade IV intra-cranial bleeding (1/12) and a necrotic enterocolitis (1/12).
Conclusions: According to our study, the mortality and morbidity due to early PPROM is more encouraging compared with the previous literature. Long-term follow-up will be needed to give correct counselling to the parents.
FC-07-005 Preterm delivery is associated with adenoviral genome detection in placenta tissue
E. Tsekoura1, D.A. Kafetzis1, S. Papadopoulou2, D. Yfanti2, N. Spanakis2, N. Nikolaidis3, A. Tsakris2, N.J. Legakis2, A. Antsaklis4
1Department of Paediatrics, Medical School University of Athens, Athens, Greece; 2Department of Microbiology, Medical School University of Athens, Athens, Greece; 3Nicu, Papageorgiou Hospital, Thessaloniki, Greece; 4Alexandra's Maternity Hospital, 1st Department of Obstetrics and Gynecology, Medical School University of Athens, Athens, Greece
Preterm birth, defined as birth occurring at less than 37 weeks gestational age is one of the most important problems in obstetrics and neonatal medicine in the developed world. Its etiology is multifactorial. Infection is considered as one of the most important associated factors as it has been implicated in up to 40% of spontaneous preterm births. Many studies have investigated various bacterial infections in association with preterm birth but still there is limited evidence for the possible role of viral infection. The purpose of this study was to test the hypothesis that detection of adenovirus in placenta tissue could be associated with preterm birth. We collected placenta speciments from 71 deliveries at gestational age less than 37 weeks (defined as preterm cases) and 122 term controls (gestational age above 37 weeks). All speciments were collected at the same approximate time for cases and controls from two different hospitals. For the detection of adenovirus genome placenta extracted samples were tested by polymerase chain reaction (PCR) assay using a specific primer pair. Adenovirus genome was identified in a total 54 placentas out of 193 samples (28%). A significant increase in the frequency of adenovirus genome was detected in preterm cases vs. term controls ((29/71 = 41% vs. 25/122 = 20%; P = 0.002). The probability for a delivery ≤36 weeks GA to be tested positive by PCR analysis for adenovirus was almost 2 and a half times higher compared to term controls (OR = 2.6, 95% CI {1.4–5.1}). The same pattern of association was observed when comparing preterm cases with GA ≤29 weeks and ≥30–≤33 weeks to term controls (OR = 2.8, 95% CI {1.1–7.0} and OR = 2.7, 95% CI {1.1–6.5} respectively), while in the subgroup ≥34–≤36 weeks GA the association was at the borderline of statistical significance (OR = 2.6, 95% CI {0.9–7.0}). The seasonal variation of adenovirus occurrence in the sample was in accordance to the known, with virus detection being more common from March to June. This is the first study to investigate adenovirus DNA detection in placenta specimens in relation to spontaneous preterm birth and suggests that there could be an association between adenovirus acquisition during pregnancy and preterm delivery.
FC-07-006 The influence of gestational age on the vasoactive response pattern of serotonin in human umbilical arteries perfused in vitro
G. Haugen
Rikshospitalet, University of Oslo, Oslo, Norway
Objective: Serotonin (5-hydroxytryptamine) is a potent vasoactive substance in human umbilical arteries. In preparations from term pregnancies perfused in vitro serotonin induces a vasoconstriction that is preceded by a partially endothelial dependent vasodilatation. The aim was to investigate the response pattern of serotonin in the umbilical arteries from pregnancies complicated by preterm deliveries as compared to uncomplicated term pregnancies.
Methods: Umbilical cord segments were perfused in vitro. These were taken from pregnancies complicated by preterm delivery before 32 weeks gestation (group 1, n = 7), between 32 and 37 weeks gestation (group 2, n = 13), and uncomplicated term pregnancies (group 3, n = 18). All women were normotensive and without proteinuria.
Results: Serotonin induced monophasic vasoconstrictory responses or biphasic responses with a transient vasodilatation succeeded by a vasoconstriction. The frequency of preparations displaying a biphasic response increased with gestational age. The frequencies were 0/7, 4/13 and 13/18 in groups 1, 2 and 3, respectively (p = 0.002). The correlation between the maximum dilatatory response obtained in each preparation and gestational age was positive and highly significant (r = 0.55, p < 0.001). No significant differences were observed in the constrictory responses between the groups.
Conclusions: In human umbilical arteries perfused in vitro the partially endothelial dependent vasodilatatory response is dependent on gestational age.
FC-08-001 Hellp and preeclampsia are two diverse pregnancy complications according to placental pathology
J. Nasiell1, M.T. Nilsson1, N. Papadogiannakis2
1Obstetrics and Gynecology, Karolinska Institutet, Stockholm, Sweden; 2Pathology, Karolinska Institutet, Stockholm, Sweden
Introduction/Aim: Preeclampsia (PE) and HELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome are pregnancy complications associated with significant maternal and neonatal morbidity and, often extensive, placental involvement. There is an ongoing debate whether it is the same disease with slightly different clinical manifestations or if they represent two diverse disease entities, possibly reflecting different pathogenetic mechanisms.
In this study we have examined placentas from patients with HELLP as compared to placentas from patients with PE.
Materials and Methods: 112 placentas from PE-complicated pregnancies and 26 placentas from HELLP patients were reviewed retrospectively. The placentas were submitted for routine histopathologic analysis to the Department of Pathology, Huddinge, during the years 2000–2004. All the placentas were examined by a senior perinatal pathologist and several placental parameters were assessed and correlated to maternal demographic data and birth weight (live born or stillborn). Statistical analysis was performed using the chi-square test.
Results: Placentas from HELLP patients had increased number of large placentas for gestational age (P = 0.0041) compared to PE patients. The HELLP placentas had less infarction (P = 0.0032). Furthermore small for gestational age (SGA) rate was increased in PE pregnancies compared to HELLP (P = 0.05).
Conclusions: The histopathologic profile and the range of placental lesions were very distinct in HELLP vs. PE placentas, indicating dissimilar underlying pathogenetic mechanisms. Thus, placentas from HELLP pregnancies seem to have less signs associated to reduced organ perfusion compared to PE. The findings that placenta is larger and that the babies are not SGA indicate that HELLP syndrome might represent a disease of the mother with less direct influence on the placenta and baby compared to PE.
FC-08-002 Peri-partal pyogenes infections: A retrospective study
E. Christiaensen1, J. Van Schaeren1, C. Lammens2, T. Vanderheyden1
1St. Augustinus General Hospital, Wilrijk, Belgium; 2University Hospital Antwerp, Edegem, Belgium
Objective: Streptococcus pyogenes is an uncommon but serious cause of peri-partal infections. This group A β haemolytic streptococcus (GAS) can cause early onset of shock and organ failure and can even be life-threatening. Nowadays GAS infections occur through carrier status of the patient or through acquired infections of health workers. According to our hospital records the incidence of GAS has increased the last 5 years and is much higher then literal references. In this study we try to describe the characterises of the infection to facilitate early detection and right treatment of the infection.
Methods: We retrospectively identified 7 peri-partal GAS infections during the last 5 years in our hospital (incidence: 1/1614 births). We looked at patient characterics, obstetric conditions, symptoms and time they presented, extention of the infection and therapy. To identify clusters of GAS infection caused by infected health care workers we additionaly subtyped by sequencing of the type-specific region of the M virulence protein gene.
Results: The GAS infections had a fulminant start on postpartum day 1–3, with general malaise, puerperal fever and endometritis as most common features. Four patients acquired intensive care admission. There were no maternal deaths. The subtype analysis did not show clusters (few results still pending).
Conclusion: A combined therapy with penicillin G and clindamycine is mandatory. When septic shock and organ failure occur, a multidisciplinair approach is essential. One GAS infection should enhace surveillance and isolate storage, 2 cases caused by the same strain should prompt the culture of specimens of linked health-care workers.
FC-08-003 Interleukin (il)-8 and monocyte chemotactic protein (mcp)-1 Mrna levels in perinatally infected and asphyxiated preterm neonates
E. Petrakou, A. Mouchtouri, E. Levi, N. Lipsou, M. Xanthou, S. Fotopoulos
Aghia Sophia Children's Hospital, Goudi, Athens, Greece
Background: Inflammation due to perinatal infection and asphyxia may cause damage to various tissues and very often to the immature brain of the fetus and the newborn. Previously we have shown that the neonatal immune system has the ability to produce increased chemokine protein levels in the serum during the inflammatory response caused by perinatal infection and asphyxia.
Aim: To investigate mRNA levels of the proinflammatory chemokines IL-8 and MCP-1 in infected and asphyxiated neonates.
Methods: Forty-two premature neonates were studied; 11 with perinatal infection (PI), 16 with perinatal asphyxia (PA) and 15, without PA and PI, were used as controls. IL-8 and MCP-1 mRNA levels were investigated in whole blood and in PHA-activated lymphocytes using semi-quantitative PCR and real time PCR, respectively.
Results: IL-8 mRNA levels were significantly increased in whole blood both during PA and PI, while MCP-1 mRNA levels were not. In vitro activated lymphocytes expressed significantly increased IL-8 mRNA levels during PI, whereas no increase was observed during PA. MCP-1 mRNA levels were significantly increased in activated lymphocytes during perinatal asphyxia while no increase was observed during PI.
Conclusions: Our data show that chemokine mRNA levels expressed by activated lymphocytes during inflammation caused by perinatal infections are different to those expressed during perinatal asphyxia. These findings might have important implications during the administration of specific chemokine antagonists in order to prevent or reduce tissue damage caused by inflammation.
FC-08-004 Erythropoietin prevents icam-1 and pecam-1 expression induced in human umbilical vein endothelial cells by TNF-α
M. Szczepanski1, M. Kamianowska1, M. Pietruczuk2, K. Wnuczko1
1Department of Neonatology, Białystok, Poland; 2Department of Haematological Diagnostics, Białystok, Poland
Background/Aims: Tumor necrosis factor-α (TNF-α) is one of the main cytokines of inflammatory and immunological response. Transendothelial trafficking of leukocytes during inflammation requires the expression of ICAM-1 and PECAM-1 on the endothelial cells and their corresponding receptors on surface of leukocytes. Erythropoietin (Epo), a sensitive to hypoxia physiological erythropoiesis regulator, is described as a cytoprotective and anti-inflammatory factor. In the present study, we examined an effect of TNF-α on ICAM-1 and PECAM-1 expression in human umbilical vein endothelial cells and a protective effect of Epo.
Methods: Human umbilical vein endothelial cells were cultured in a standard medium (M 199); some cells were pretreated (24 hours) with Epo (20 IU/ml). The control culture cells and the cells from Epo were incubated for 6 hours with a TNF-α (10, 20, 40 ng/ml). Expression levels of ICAM-1 and PECAM-1 in the HUVEC were quantified by flow cytometry.
Results: In the control culture cells expression of ICAM-1 and PECAM-1 amounted to 20.9 ± 0.4 and 28.4 ± 0.6, respectively. After HUVEC stimulation with 10, 20, 40 ng/ml of TNF-α, ICAM-1 expression amounted to 80.4 ± 3.3; 83.4 ± 2.3 and 86.5 ± 0.7 for PECAM-1 to 65.1 ± 3.8; 70.0 ± 3.9 and 73.1 ± 5.3 respectively for and. It was significantly statistically higher than expression of ICAM-1 and PECAM-1 in the cultures pretreated with Epo 57.7 ± 0.7 and 59.3 ± 0.6 respectively.
Conclusions: Erythropoietin inhibits ICAM-1 and PECAM-1 expression induced in HUVEC by TNF- α.
— Cancelled
FC-08-006 Bullous systemic lupus erythematosus: A case report
P. Goncalves1, R. Correia2, M.J. Silva2, S. Capela1, A. Marques1, L. Pinto1, M.L. Tuna1, M.C. Cardoso1, L.M. Queiroz1
1Hospital de Santa Maria, Lisbon, Portugal; 2Hospital de S. João, Portugal
Background: Bullous systemic lupus erythematosus (BSLE) is a rare blistering disease with a distinctive combination of clinical, histological and immunopathologic features which constitute a unique bullous phenotype.
Case Description: 25-year-old caucasian pregnant female with a 2-year history of systemic lupus erythematosus with renal and central nervous system involvement medicated with prednisolone 40 mg/day. In the second trimester of pregnancy, she developed a widespread erythematosus eruption associated with tense, fluid-filled blisters and crusts. Biopsy showed subepidermal blistering and a neutrophilic infiltrate. Immunofluorescence showed positive IgG and C3 deposition. Rheumatoid factor, anti-Ro, anti-La and aPL antibodies were all negative. High titers of ANA (1/1000) and of anti-dsDNA (551 UI/ml) were found. Anti-Sm antibodies were also positive. Complement components were decreased. Treatment with prednisolone in increasing doses and immunoglobuline perfusion were ineffective. Subsequent treatment with dapsone led to a rapid and sustained remission of skin symptoms. At 27 weeks she developed hypertension and at 30 weeks she was admitted at the High-Risk Pregnancy Unit due to symptoms and signs of preeclampsia. A Cesarean section was performed at 35 weeks because of severe preeclampsia. A male healthy newborn (2700 g, Apgar score 9/10) was born.
Comments: BSLE is a rare condition not characteristic of any other primary bullous disease and, so far, only seen in lupus patients. According to our search, this is the first case of BSLE ever described during pregnancy.
FC-09-001 Systematic analysis of thrombophilia after preeclampsia: Prevalence and impact on subsequent pregnancies
J. Van Eyck1, J. Bosma1, B. Arabin2
1Department of Perinatology Isala Clinics, Zwolle, The Netherlands; 2Clara Angela Foundation, Witten, Germany
Objective: To assess the prevalence of thrombophilia and its impact on subsequent pregnancies within patients with preeclampsia.
Methods: Up to now 400 patients with preecclampsia (252 with early-onset <32 weeks) were examined 3 months postnatally for protein S and proteion C deficiency, APC resistance, factor V Leiden, prothrombin G20210A-mutation (Factor II), anticardiolipin antibodies, lupus anticoagulans, ATIII deficiency, hyperhomocysteinemia. Subsequent pregnancies were analyzed according to the kind of thrombophilia, preventive therapy such as aspirin, low molecular weight heparin (LMWH), folic acid and pyridoxine, the re-occurance of pre-eclampsia, birth weight and gestational age of delivery.
Results: Thrombophilia was present in 37% of patients with early- and 31% of patients with late-onset of preeclampsia. Protein S deficiency and prothrombin G20210A mutation were significantly more involved in early preeclampsia compared to the prevalence in the general Dutch population. The recurrance risk in patients without thrombophilia was 46.6% in non-treated but 16.5% in women who received aspirin. For patients with ≥1 thrombophilia the recurrance risk was 33% in non-treated or only aspirin-treated women but 13.5% in women treated with LMWH or vitamin B6 combined with folic acid.
Conclusions: Our data suggest that the impact of thrombophilia on pregnancy outcome can be neglected if former preeclamptic women are treated with aspirin or specific therapy in a subsequent pregnancy. We now participate in a randomized trial to evaluate the impact of LMWH.
FC-09-002 Doppler assessment of uterine artery resistance index in antiphospholipid syndrome vs. Impaired trophoblast invasion
D. Tutunaru1, D. Herghelegiu2, B. Alexandru1
1Elias Emergency Hospital, Marasti, Bucharest, Romania; 2Polizu Obstetrics Gynecology Hospital, Polizu, Bucharest, Romania
Background: From the 14th week of gestation there is a spectacular growth of human fetal brain which forces trophoblast to a second wave of invasion which interests the myometrial segment of the spiralate arteries. This invasion replaces the endothelial and muscular layers and leads to uteroplacental hemodynamic alterations which shows conversion from a high pressure to a “low pressure–high debit” regimen.
Aim: To investigate the causes of abnormal uterine arteries Doppler RI in pregnancies with and without APLS.
Methods: Prospective, non-randomised, parallel group study. Inclusion criteria: pregnant women with increased uterine RI (over 0.70) after 16th week of gestation. One arm: pregnant women positive for ACL, antiβ2 GP I and/or LAC. Second arm was negative for the same markers. Doppler wave form and RI were analyzed. Both arms were matched for age, parity and gestational age.
Results: In the APLS arm were included 47 patients, and 73 in the other arm. Uterine arteries RI analysis carried out at 16th week of gestation showed a marked increase in the RI with a median of 0.73 (0.70–0.88) in APLS arm and 0.81 (0.73–0.93) in the APLS-free arm. Doppler waveform showed 22 cases of diastolic notch, whereas in the other arm there were 61 cases. At the 20th week of gestation a second assessment showed elevated RI in only 34 from 47 patients in the APLS arm and in 68 from 73 in the other arm. The presence of diastolic notch was noted in only 14 cases from the first group and in 67 from the other group.
Conclusion: In APLS there is thrombosis of the uteroplacental vasculature so increased impedance in the uterine arteries can lead to elevated uterine arteries RI but without waveform anomalies. In pregnancies with impaired trophoblast invasion there is not only elevated uterine RI but also an abnormal waveform (diastolic notch) which is a sign of incomplete spiralate arteries conversion.
FC-09-003 The value of cardiotocography in predicting fetal outcome in women who present with decreased fetal movement
N. Daly1, C. O'Herlihy2
1National Maternity Hospital, Dublin, Ireland; 2School of Medicine and Medical Science, University College Dublin, Dublin, Ireland
Background: Maternal perception of decreased fetal movement causes concern in late pregnancy and is a common presenting complaint at maternity hospitals. However, the clinical significance of this complaint remains uncertain. Is it possible to reassure a mother when she presents with decreased fetal movement and has a reactive cardiotocograph?
Objectives: To determine the value of cardiotocography in predicting fetal outcome in women presenting with decreased fetal movement. Endpoints chosen for this study were rates of obstetric intervention and perinatal asphyxia, morbidity and mortality.
Methods: Patient records were reviewed retrospectively, focussing on the three nominated endpoints as discussed above. A total of 109 patients, 28 weeks' gestation or more, who presented to the National Maternity Hospital with decreased fetal movement, from 1st January 2005–30th June 2005, were included.
Results: Obstetric intervention: Instrumental deliveries and caesarean section rates were increased when compared with total rates in 2004. Perinatal asphyxia, morbidity and mortality: There were 8 abnormal cardiotocographs. There was 1 perinatal death (an intrauterine death diagnosed at presentation). Seven patients with abnormal cardiotocographs were admitted. Three of these cardiotocographs indicated immediate caesarean section; two had abnormal perinatal outcome. The remaining 4 patients subsequently delivered on this admission, one of whom required admission to the neonatal unit. There were 4 admissions to the neonatal unit subsequent to a reactive cardiotocograph at the initial presentation. These babies followed a normal neonatal course after a short hospital stay. There was no perinatal death following a normal cardiotocograph.
Conclusion: These results support current practice of reassuring and discharging women who present with decreased fetal movement and have a normal cardiotocograph.
FC-09-004 Assessment of fetal heart rate variability and reactivity during labour – a novel approach
K.G. Rosén
Perinatal Centre, Dept. of Physiology, Medicinaregat, Gothenburg, Sweden
Objective: To resolve the problem of a FHR signal that may vary extensively during labour and not allowing continuous mathematical modelling.
To assess a new measure of fetal heart rate (FHR) variability (FHRV) from fetal ECG recordings during labour allowing for the non-stationary nature of FHR.
Design: Initially, FHRV was studied in 34 fetuses divided into 2 groups; 4 index cases with adverse perinatal outcome and a predominant pattern of reduced FHRV and 30 cases with a normal outcome of labour but with a FHR pattern requiring scalp pH. The parameter setting identifying decreasing and/or low FHRV was then validated in a 6600 case EU database of STAN recordings.
Methods: A piecewise polynomial function was adapted to a 2 minutes sequence of R-R data allowing the approximation of the “median” FHR.
Residuals (Res) calculated by subtracting the median R-R component from the recorded R-R were used to record the extent to which the recorded R-R deviated from the calculated median FHR. A low Res value (ms) would indicate a FHR tracing that would follow close to the median FHR, whereas a high Res value would indicate R-R values varying from the calculated median FHR. The the Res parameter would provide a measure of instantaneous variations in FHR and accepting the variations of decelerations, altered baseline and accelerations. Res was quantified by calculating the 95th percentile (95th Pct) in consecutive 2 minute époques of R-R data.
Results: We found that the median 95th Pct and the variance of the 95th Pct calculated for 20 minute running blocks of FHR provided a relevant measure of changes in FHRV during labour. Lack of FHRV was identified by median 95th Pct <2.3 ms and variance of <0.1. Such époques exceeding 60 minutes duration identified a non-reactive FHR as demonstrated by the index cases with a sensitivity of 100% and a specificity of 97% (Kappa index 0.87). Furthermore, a significant linear fall in the median 95th Pct over 2 hrs also identified an abnormal FHR response to the stress of labour.
Conclusions: FHRV may be assessed objectively by applying a new technique, named residuals measurements, allowing the specific identification of situations of low or decreasing FHRV. This enables us to continuously assess fetal reactivity to assist in the interpretation of FHR patterns during labour.
This work has been supported by the EU commission through a BioPattern NoE.
FC-09-005 The influence of maternal epidural analgesia upon intrapartum fetal oxygenation
G. Caracostea1, F. Stamatian1, M. Lerintiu1, D. Herghea2
11st Gynecology Clinic, University of Medicine and Pharmacy “I. Hatieganu”, Cluj-Napoca, Romania; 2Oncology Institute “Constantin Chiricuta”, Cluj-Napoca, Romania
Objective: The use of epidural analgesia in labor may be associated with non-reassuring fetal heart rate (FHR) patterns. We aimed to assess changes in fetal oxygen saturation (FSpO2) during epidural analgesia.
Methods: A prospective observational study. Twenty healthy parturients were enrolled following the inclusion criteria. Informed consent was obtained. Ropivacaina in low concentration (1 mg/ml) was used with Fentanyl 2.5 μg/ml. The values of fetal oxygen saturation have been registered continuosly 10 minutes before administration of the analgesic drug and during the following 30 minutes after administration. Pulse oximetry was used simultaneously with cardiotocography (CTG).
Results: The average value for oxygen fetal saturation before the analgesic drug administration was 44.3 ± 8.8%; during the first 10 minutes after administration it was 41.3 ± 7.2% (p = 0.25) and during the following 20 minutes since administration was 43.05 ± 6.9% (p = 0.63). There was no direct relationship between the non-reassuring CTG pattern appearance and FSpO2 <30% (RR = 1.11; CI 95% [0.76–1.64]). No significant correlation was obtained between FSpO2 values within the first 30 minutes of epidural analgesia and the neonatal acidotic status (PH ≤7.00 RR = 0.33; CI 95% [0.04–3.09] and BE ≤−12 mmol/l RR = 1; CI 95% [0.21–4.71]).
Conclusions: There were no differences in FSpO2 values in the first 30 minutes following administration of analgesic drugs. In case of a non-reassuring CTG pattern, during epidural analgesia, the knowledge of the fetal oxygenation may be a useful way to get informed upon the real fetus status in utero.
FC-09-006 Ursodeoxycholic acid in intrahepatic cholestasis of pregnancy
P. Kascak, M. Hlavacik, M. Kascak, J. Pastvova
Hospital with Policlinic, Trencin, Slovak Republic
Objective: Intense pruritus and the risk of stillbirths and premature deliveries justify the search for an effective pharmacologic treatment of intrahepatic cholestasis in pregnancy. The aim of this retrospective study was to compare the management, treatment, efficacy and pregnancy outcome in two different groups of these patients. The main interest was to test the efficacy and report our experience in managing the disease with ursodeoxycholic acid treatment.
Methods: All cases of intrahepatic cholestasis in pregnancy diagnosed at our hospital from January 1992 to December 2004 were analyzed. Analysis on medical and obstetric history, symptoms, laboratory results, treatment, mode of delivery and pregnancy outcome was performed. The treatment with ursodeoxycholic acid was introduced at our department in January 1997.
Results: A total of 90 pregnant women with intrahepatic cholestasis were identified and analyzed. From January 1992 to December 1996 (group A) patients were treated with hepatoprotectives and vitamins. From January 1997 to December 2004 (group B) ursodeoxycholic acid therapy was administrated. The prevalence of disease was 0.46% of all births, all patients were presented with pruritus. The mean gestational age at onset of symptoms was 34.1 weeks. All babies were born alive, the mean gestational age at delivery was 37.69 (group A) vs. 38.64 (group B). The mean birth weight was 2801 (A) vs. 3760 (B) grams. The incidence of Caesarean section was 37.5% (A) and 23.8% (B), while the average incidence of Caesarean section increased from 8.45% to 14.33% during study period. The delivery was induced in 14.6% (A) and 35.7% (B). The mean Apgar score at first minute was 8.25 and 9.57 respectively. Statistical analysis and controversies are discussed.
Conclusions: Ursodeoxycholic acid is effective and safe in pregnant patients with intrahepatic cholestasis. Relevant aspects of fetal outcome were also improved in patients receiving ursodeoxycholic acid compared to our previous strategies.
FC-10-002 Premature birth and perinatal morbidity and mortality
S. Petakovic, S. Arbanas, Z. Petrovic, D. Malobabic, B. Mitrovic
Health Care Center, Department for Gynecology, Obstetrics, and Neonatology, Sremska Mitrovica, Serbia
Introduction: Premature birth significantly influences neonatal morbidity and mortality.
Aim: Review of perinatal outcome for premature newborns in two time intervals: I (1987–1994) and II (1995–2002).
Materials and Methods: Statistical analysis of data on the total number of births, incidence of premature birth, gestation age of premature infants (28–36 GW), perinatal morbidity and mortality, as well as referal of premature infants to neonatology centres.
Results: A total of 24,977 births were registered for both periods (I 13,253, II 11,724), of which 1,273 (5.1%) premature (I 740, II 533). The total number of both full term and premature birth shows a downward trend. In both periods there were 4 times more premature births at 33–36 GW: 1029 (80.95%), compared to 28–32 GW: 244 (19.05%). In the 1987–1994 period 81.92% premature births were at 33–36 GW, and 18.08% at 28–32 GW; in 1994–2002 80.08% were at 33–36 GW, and 19.92% at 28–32 GW. Most frequent types of morbidity were hyperbilirubinemia (I 21.54%, II 26.87%), and perinatal asphyxia (I 20.39%, II 21.52%), RD (I 17.40%, II 14.58%); HIC (I 10.12%, II 8.33%), infection (I 3.13%, II 3.75%) and congenital malformations (I 4.70%, II 5.20%). There is a visible drop in total perinatal mortality (I Xmean 15.02‰, II Xmean 11.24‰) and perinatal mortality of premature infants (I Xmean 10.30‰, II Xmean 8.24‰).
Conclusion: The preterm infant requires a high level of readiness, training and equipment of obstetricians and neonatologists.
FC-10-003 Socio-demographic factors and obstetric history – the influence on the cervical length during pregnancy
A. Novakov Mikic1, V. Mandic2, Dj. Petrovic2, Z. Potic3
1Klinika za Ginekologiju i Akuserstvo, Novi Sad, Serbia; 2Ginekolosko-Akuserska Klinika “Narodni front”, Belgrade, Serbia; 3Institute for Cardiovascular Diseases, Sr Kamenica, Serbia
Objectives: To examine the relationship between maternal demographic characteristics, obstetric history and cervical length.
Methods: In this cervical length was measured by transvaginal ultrasound in women with singleton pregnancies between 11 and 36 weeks. The significance of differences in median cervical length between subgroups was calculated according to maternal age, pregravid body mass index (BMI), cigarette smoking and previous obstetric history.
Results: The cervix was measured in 579 women. In 64% of cases women were younger than 30 years, 50% were nuligravidas, of those with previous pregnancies 67% were primiparas, 14% had spontaneous abortions, 15% had artificial abortions and 23% were smokers. The mean pre-pregnancy BMI was 22. The mean cervical length in first trimester was 35.3 mm, in second 34.8 mm and in the third 34.6 mm. There was no statistical difference in cervical length between women younger and older than 30 years (p = 0.212), neither between nuligravidas and women that had previous pregnancies (p = 0.150). In the group of women that had a previous vaginal delivery cervix was significantly longer in the second trimester (p = 0.003), as well as overall (p = 0.011), but there was no significant difference in the first and third trimester. There was no statistically significant difference in the length of cervix between women that had abortions of any kind and those that did not have them (p = 0.392), nor between smokers and non-smokers (p = 0.253). Among the women in the first trimester the correlation between cervical length and pre-pregnancy BMI was negative, whereas among women in the second trimester the length of the cervix did not change with BMI and among women in the third trimester the correlation was changed to positive.
Conclusions: Out of all the variables in our study the length of the cervix was significantly different only between women that had one or more vaginal births and those that did not have a vaginal birth.
FC-10-004 Maternal body mass index in twin gestation: Monochorionic and dichorionic
A.I. Cordeiro, A.C. Júlio, E. Dias, H.T. Simoes
Maternidade Dr Alfredo Da Costa, Lisbon, Portugal
Objective: To identify the influence of maternal body mass index (BMI) on pregnancy outcome in twin gestations.
Methods: A retrospective comparative analysis of women with twin gestations, in surveillance program in our maternity between January 1996 and December 2005 was performed. Monochorionic and dichorionic pregnancies were considered separately and data were divided according to pregravid body mass index in 3 groups (less than 20, 20–29.99 and 30 or greater). Maternal age, gestational age at delivery, mode of delivery and birth weight were identified. Pearson χ2 test and independent samples T-test were used for statistical analysis (SPSS 10.0, Inc.).
Results: Data were analysed for 570 twin pregnancies, 440 dichorionic and 130 monochorionic. The mean maternal age was 29.8 years (15–48; SD 4.88). Women with a BMI less than 20 had a lower incidence of labor before 34 weeks than those with greater BMI, in both dichorionic and monochorionic gestations (p < 0.05). Cesarean section was the most frequent mode of delivery (64.9%). The highest BMI was associated with a significant rise in caesarean section rates (p < 0.05). Analysis of newborn birth weight revealed no significant difference in frequency of very low birth weight (VLBW, less than 1500 g).
Conclusions: Thinner women had less premature labour (before 34 weeks' gestation) and had vaginal delivery more frequently than the others. There were no statistically significant differences between dichorionic and monochorionic gestations. Pre-pregnancy high body mass index may be a risk factor for worst twin pregnancy outcome.
— Cancelled
FC-10-006 Congenital heart defects associated with syndromes and extracardiac malformations
A. Meberg1, J. Hals2, E. Thaulow3
Department of Paediatrics, 1Vestfold Hospital, Tonsberg, and 2Buskerud Hospital, Drammen, Norway; 3Department of Paediatric Cardiology, The National Hospital, Oslo, Norway
Background: An increasing prevalence of CHDs caused by improved detection of (often minor) CHDs may have changed the panorama of syndromes/extracardiac defects in such patients.
Objectives: To register the occurrence and types of syndromes/extracardiac defects in patients with CHDs.
Method: Population-based prospective observational study.
Results: In 56,410 infants born alive during 1982–2005, CHDs were detected in 656 (1.2%). Of these 145 (22%) had syndromes/extracardiac defects (61 (42%) had chromosomal disorders, 21 (14%) recognizable syndromes, 16 (11%) multiple and 47 (32%) single malformations). In perimembraneus ventricular septal defects (VSDs) syndromes/extracardiac defects occurred in 20/67 (30%) compared to 30/299 (10%) in VSDs located to the muscular part of the septum (p = 0.005), and in 17/218 (8%) of muscular VSDs with spontaneous closure compared to 13/81 (16%) in muscular VSDs which did not close spontaneously (p = 0.035). The prevalences at birth for CHDs in total were the same for the cohorts born 1982–1993 and 1994–2005 (1.1 vs. 1.2% respectively). The prevalence of CHDs with syndromes/extracardiac defects increased significantly between the two periods (0.2 vs. 0.3% respectively) (p = 0.014), caused by increase of CHDs associated with chromosomal disorders (0.07 vs. 0.15%; p = 0.006).
Conclusions: The occurrence of syndromes/extracardiac defects in CHD cases (22%) is somewhat lower than earlier reported. This may be caused by a high detection rate of minor CHDs (mostly muscular VSDs with spontaneous closure) associated with a relatively low incidence of associated syndromes/extracardiac defects. The prevalence at birth of CHDs with syndromes/extracardiac defects was found to increase, caused by an increased occurrence of CHDs associated with chromosomal disorders.
IS-03-003 Inflammation and its role in pregnancy
D. Maulik
Winthrop University Hospital, Mineola, USA
Pregnancy is characterized by maternal immunological tolerance toward the semiallogenic fetus. A main aspect of this tolerance is the suppression of maternal innate immunity at the maternal-fetal interface by immune modulators including progesterone and anti-inflammatory cytokines. Parturition is initiated when these blocking mechanisms are withdrawn resulting in the expression of proinflammatory cytokines such as interleukin (IL)-1β, IL-6, IL-8, tumor necrosis factor-α and interferon-γ in the myometrium, the cervix and the fetal membranes. A cascade of proinflammatory molecular events consequently ensues including the production of matrix metalloproteinases and prostaglandins, and migration of natural killer cells and macrophages. These events result in the initiation of myometrial contractions, cervical softening, and decrease in the tensile strength of the fetal membranes culminating in the onset of labor. Infection and stress may initiate these processes prematurely resulting in uterine contractions, cervical dilation and effacement, and prelabor rupture of membranes leading to preterm birth.
IS-03-004 Intraamniotic infection and the mode of delivery
A. Kafkaslı
Inonu University School of Medicine, Department of Obstetrics and Gynecology, Malatya, Turkey
Clinical intraamniotic infection (IAI) occurs in 10% of the pregnancies. The major concern of this clinical situation is neonatal sepsis. Main treatment modalities are broad spectrum antibiotic administration and the delivery of the fetus. Delivery has two main advantages as evacuation of the infected contents like fetus, placenta and the membranes, and removal of the fetus from infected environment. Studies up to now are limited to suggest the most convenient time and the mode of delivery to prevent maternal and fetal complications. Most of the reports point out the positive correlation between the preterm premature rupture of the membranes, reduced amount of amniotic fluid and the short latent period preceding delivery which was related to rapid invasion of placenta and the membranes with microorganisms. The common time interval between beginning of spontaneous labor and the clinical diagnosis of intraamniotic infection is less than 12 hours.
Mode of delivery in these patients depends widely on the viability of the fetus and the progression of the labor. Although IAI is not an indication for the abdominal delivery and maternal morbidity is low with vaginal route, rate of caesarean section is high. The common cause of the abdominal delivery is dysfunctional labor related to myometrial infection. The rate of unresponsive myometrium to the uteotonic agents is well correlated with the virulence of the microorganisms. In term pregnancies aggressive antimicrobial therapy and the vaginal delivery within 12 hours of latent period must be the preferred management. Abdominal delivery should be taken into consideration for the patients with unresponsive uterus, maternal septicemia or obstetric indications. Perinatal outcome is related to gestational weeks rather than IAI.
IS-03-005 Inflammatory events and pulmonary morbidity of preterm infants
C.P. Speer
University Children's Hospital, Wurzburg, Germany
Increasing evidence indicates that bronchopulmonary dysplasia (BPD) results – at least in part – from an imbalance between proinflammatory and anti-inflammatory mechanisms, with a persistent imbalance that favours proinflammatory mechanisms. The inflammatory response is characterized by an accumulation of neutrophils and macrophages in the airways and pulmonary tissue of preterm infants and, moreover, by an arsenal of proinflammatory mediators which affect the alveolar capillary unit and pulmonary tissue integrity. Besides proinflammatory cytokines and toxic oxygen radicals, various lipid mediators as well as potent proteases may be responsible for acute lung injury. During the last decade it has become evident that there are multiple pre- and postnatal events contributing to the development of BPD in preterm infants. Chorioamnionitis and cytokine exposure in utero, plus sequential lung injury caused by postnatal resuscitation, oxygen toxicity, volu-barotrauma and infection all lead to a pulmonary inflammatory response which is most likely associated with aberrant wound healing and an inhibition of alveolarisation as well as vascular development in the immature lungs of very preterm infants, causing the “new BPD”.
IS-03-006 Biochemical and biophysical markers of myocardial injury in the course of perinatal asphyxia
M. Matuszczak-Wleklak, M. Szymankiewicz, J. Gadzinowski
Department of Neonatology, K. Marcinkowski University of Medical Sciences, Poznan, Poland
Introduction: Although perinatal hypoxia is a crucial problem there are no routine assessments of hypoxic myocardial injury in neonates.
Aim: To investigate the usefulness of cardiac troponin T (cTnT), creatinine-kinase (CK-MB), echo and electrocardiography in the diagnosis of myocardial injury in the course of perinatal hypoxia and to correlate other biochemical markers of hypoxia.
Material and Method: Material consisted of 105 term newborns. Hypoxia (umbilical pH < 7.1 and BE < −12mmol/l) was diagnosed in 45 neonates – group I. Group II consisted of 60 healthy newborns. Quantitative determination of cTnT and CK-MB in blood serum were performed between 12th and 24th hour of life using Elecsys STAT Immunoassay. At the same time ECHO and ECG were performed. We evaluated: shortening fraction of left ventricle (FS), cardiac output (CO), cardiac index (CI), mitral (MI) and tricuspid valve (TI) insufficiency. The morphology of ST segments, T waves, PQ, QTc (corrected QT) intervals.
Results: Mean pH and BE for group I and II were 7.00 ±0.09 vs. 7.29 ± 0.08 (p < 0.000001) and −12.30 ± 4.52 vs. −1.29 mmol/1 (p < 0.000001), respectively. Median of Apgar score at 1st and 5th minute were 4–9 in group I and 8–10 in group II (p < 0.00001). Newborns in the group I had higher values of cTnT (mean 0.121 ± 0.103 ng/ml) compared with group II (mean 0.054 ± 0.039 ng/ml), p < 0.00001. Similarly CK-MB values were higher in the group I (mean 19.71 ± 16.97 ng/ml) compared with group II (mean 13.05 ± 8.01 ng/ml), p < 0.05. CO, CI and FS values were within normal limits in both groups. TI was high in group I (40%) than in group II (3.3%) (p < 0.00001). Ventricular hypertrophy, elevation or depression of ST segment with inverted or flattened T wave, PQ, QTc intervals values were comparable in both groups (NS). None of group II and 19/45 (42.2%) neonates of group I demonstrated: tachycardia (11.1%, p < 0.05) hypotension (8.9%, p < 0.05) and respiratory distress requiring mechanical ventilation (22.2%, p < 0.05).
Conclusions: Perinatal asphyxia is associated with myocardial dysfunction demonstrated by cTnT, CK-MB, ECHO and ECG examination between the 12th and 24th hour of life. These findings warrant close monitoring of cardiac function in asphyxiated infants.
IS-03-008 Effects of histopathological chorioamnionitis on prematurity and poor neonatal outcome
G. Erdemir1, O. Zekioglu2, B. Cakmak1, M. Yalaz1, F. Akercan3, S. Calkavur1, S. Sagol3, M. Akısu1, N. Kultursay1
1Department of Pediatrics, Ege University Faculty of Medicine, Izmir, Turkey; 2Department of Pathology, Ege University Faculty of Medicine, Izmir, Turkey; 3Department of Obstetrics and Gynecology, Ege University Faculty of Medicine, Izmir, Turkey
Objective: To evaluate the effects of chorioamnionitis on premature births and early neonatal outcome.
Methods: A prospective mother-infant cohort study was conducted on infants delivered at a gestational age less than 35 weeks, between October 2004 and May 2005. The whole group was divided into two according to the histopathologic examination of placentas. Group1: Histopathologic chorioamnionitis (HC) group and Group 2: Placentas without HC. Maternal pregnancy characteristics and outcomes of infants were compared between the two groups of infants.
Results: A total of 43 mothers and 57 infants were included (group 1; 10 mothers, 12 infants and Group 2; 33 mothers and 45 infants). The overall incidence of HC was 23.2%. HC was significantly associated with an increased risk of extreme preterm delivery. Group 1 showed an increased mortality and morbidity with increased incidence of early neonatal sepsis, respiratory distress syndrome (RDS), bronchopulmonary dysplasia (BPD) and patent ductus arteriosus (PDA). In group 1 and 2 the incidence of preterm premature rupture of membranes (PPROM) was similar, and maternal antenatal antibiotic therapy did not affect neonatal outcomes significantly. Clinical symptoms of chorioamnionitis was found in only one mother in Group 1 (10%). WBC counts and CRP levels did not differ in both groups. These data show that clinical findings are not reliable in the diagnosis of HC.
Conclusions: Our study justifies the need to assess the immediate and routine histopathologic examination of placenta in every premature birth. Consequently, with aggresive and appropriate medical approach, improvement of neonatal prognosis of affected infants could be achieved.
IS-03-010 Biochemical markers and prediction of preterm birth
J.M. Carrera, B. Serra, E. Scazzochio, M. Torrents, A. Munoz, M. Echevarria, M. Garcia-Yuste
Institut Universitari Dexeus, Barcelona, Spain
Objective: To assess the usefulness of two biochemical markers (Fibronectin and IGFBP-I) to predict spontaneous preterm delivery (PD) in low risk (LR) pregnancies, compared with the cervical evaluation by transvaginal ultrasound.
Methods: A prospective observational study was carried out from 2000 to 2005 involving 2000 subjects with singleton pregnancies at LR for preterm delivery in two steps; at 20–22 weeks of gestation the cervix was evaluated by ultrasound measuring its length, and afterwards a Fibronectin or IGFBP-I detection test was done at 24–26 weeks.
Results: Positive Fibronectin test had a sensitivity of 19.2%, a specificity of 93.9%, a PPV of 14.7% and a NPV of 95.5% for predicting preterm delivery before 37 weeks of gestation. On the other hand the IGFPB-1 test had a sensitivity of 15.2%, a specificity of 96%, a PPV of 28.5% and a NPV of 91.7%. Finally the CL below 28 mm at 20–22 weeks only reached a sensitivity of 10.2%, a specificity of 96.6%, a PPV of 2.3% and a NPV of 99.3%.
Conclusion: Both biochemical markers (Fibronectin or IGFBP-I) reached higher sensitivities and PPVs than CL measurement. On the contrary the ultrasonographic marker had a better specificity and NPV. Probably the combined use of both types of markers is the best option.
IS-03-012 Screening for vaginal infection in low gestational age
Z. Hajek1, J. Kobilkova2, M. Koucky1, A. Paskova1, R. Ondrackova1
1Obstet. Gynaec. Dept., Medical School, Charles University, General Hospital, Prague, Czech Republic; 2Institute for Care of Mother and Child, Prague, Czech Republic
Objective: The purpose of this study is to find and treat the bacterial vaginal pathogens in the group of threatened premature labour and in the group of high risk pregnancies with the history of previous prematurity or miscarriages.
Methods: Diagnostics of vaginal infection has been done using routine bacterial culture in combination with urine analysis and Bethesda smear (system 2001). Sexually transmitted diseases (STD) have been detected by the detection of antibodies from maternal serum and by DNA analysis. The screenings were done in the group of 180 symptomatic patients (preterm deliveries) and in the group of 210 asymptomatic patients (term deliveries). Histological examination of the placenta and the umbilical cord were also evaluated.
Results: The higher incidence of bacterial vaginosis (BV), STD and B-streptococcus (GBS) were detected in the group of threatened premature labour in comparison with the group of term deliveries. Action of microorganisms on the vaginal epithelium develop the typical morphological changes in the cell nucleus and in the cytoplasm. Bethesda examination correlate with routine bacterial culture (Fischer test p = 0.0003, OR 12.9) and is able to detect earlier the warning signs of the termination of pregnancy. Histological signs of prenatal inflammation occured more frequently in the premature newborns in comparison with term delivered newborns. Chorioamnionitis 72% vs. 35% (p = 0.005), funisitis 48% vs. 22% (p = 0.009) were detected.
Conclusions: The screening for vaginal infection has been indicated in the group of threatened premature labour and in high risk group of pregnant women. In the contrary the screening and antibiotic treatment has been not indicated in the group of asymptomatic patients. Bethesda system should be included in the complex of antenatal examination of prenatal inflammation.
IS-03-018 Operative or vaginal delivery in suspected intrauterine infection
Z. Papp
I. Dept. of Obstetrics and Gynecology, Semmelweis University, Baross u. 27, Budapest, Hungary
Intrauterine infection (IUI) is a major cause of premature labor with or without intact membranes, however, access of bacteria to the amniotic fluid is well documented at term as well. Since transabdominal amniocentesis at the time of preterm labor is not a routine diagnostic procedure, IUI is an under-diagnosed and under-reported complication of pregnancy. Bacterial invasion of the amniotic cavity is associated with significant acute neonatal morbidity and mortality and, at least to some degree, with neurological impairments (periventricular leukomalacia, intraventricular hemorrhage, cerebral palsy) and chronic lung disease in the preterm infant. Full-term neonates exposed to IUI also are at significantly inceased risk for sepsis, encephalopathy and cerebral palsy. The strong correlation between IUI and adverse neonatal outcome is a continuous motivation to regularly reevaluate timing of labor and route of delivery in pregnant women with established or suspected IUI. As a general rule, the optimal interval for delivery occurs when the risks of immaturity are outweighed by the risks of pregnancy prolongation. Operative delivery for suspected or established IUI is aimed at avoiding traumatic injuries. A gestational age approach to management, however, is important, and should be adjusted for each department's neonatal intensive care unit. In this review, vaginal and abdominal route of delivery as well as timing are critically examined.
IS-03-019 Monitoring of mother and fetus in a case of pprom
P. Janků
Dept. of Obstetrics and Gynecology, Masaryk University, University Hospital Brno, Brno, Czech Republic
The preterm premature rupture of membranes (PPROM) is associated with significant maternal, fetal and neonatal risk. In 50% of PPROM it comes to a fetal inflammatory response syndrome (FIRS).
The monitoring of the mother concentrates especially on the risk of intrauterine infection and on compromise to cardiovascular system under the influence of betamimetics.
Monitoring of the fetus after PPROM is to be directed towards the infection and hypoxia which are intensified by the prematurity. The risk of hypoxia is unfavorably influenced, with exception of infection, by oligohydramnion and the possibility of a partial compression of the umbilical cord. The risk of the intrauterine infection of the fetus is followed by means of inflammatory markers in the mother's blood. It is also necessary to observe the clinical condition of the mother and the result of the vaginal bacterial cultivation or the cultivation of amniotic fluid obtained by amniocentesis. Amniotic fluid Gram stain, glucose and leukocyte esterase can be used as rapid tests to predict intraamniotic infection.
The risk of the fetus hypoxia is monitored by the CTG – nonstress test (NST), biophysical profile (BPP), ultrasound and Doppler. The optimal method and the importance of the mentioned methods are discussed. With NST there is estimated the optimal frequency of examination from once a day to twice a week. BPP and Doppler of umbilical artery does not predict intraamniotic infection. Intensive fetus monitoring needs a special attitude even during the labor. In the peripartal period after the beginning of contractions the fetus should be continually observed by means of cardiotocography. Lately modern methods of the fetus monitoring, as intrapartal fetal pulse oximetry and S-T analysis of the fetal ECG, are tested.
IS-03-020 Short and long-term outcome of premature rupture of membrane (prom) babies
M.A. Aksit
Department of Neonatology, Eskisehir Osmangazi University Medical Faculty, Eskisehir, Turkey
Objective: Pregnancy is initiated by the zygot formation. Althought zygot is originated from the mother's own cell, it is an immunologically different cell. When you implanted a foreign cell in to an organism, rejection reactions must be expected. Rejection is a complex inflamation mechanism. In pregnancies we don't expect such inflamation reactions. Several factors can be indicated not to performing the rejection. But in some cases the inflamation mechanisms can be encountered, in unique or complex types.
Methods: All deliveries and newborn infants are retrospectively evaluated from December 2005, at the Intensive Care Unit and Obstetrics of Eskisehir Osmangazi University Medical Faculty. The main category depends on the PROM and non-PROM cases. In both groups clinical and laboratory findings are based on the inflammatory reactions. The inflammation reactions depend on the immunological basis: IMBALANCE; I: Infection, M: Mediator Release, B: Blood; coagulation, A: Apoptosis, L: Labile: Super antigen, A: Antigen presentation, N: Neutrophil activation, C: Complement system, E: Effects on Tissues. The clinical evaluations are stand on the functional basis: FUNCTIONAL; F: Functional variations, U: Unacceptable adaptation, N: Non destructive disturbances, C: Compensation period, T: Tissue reactions started, I: Impairments noticed, O: Oxidative Stress and Degeneration, N: Noticeable findings, A: Abnormal tissue reactions, L: Lysis, cell and/or tissue death. Results are scored from 0 to 4 + ; “0” = None/negative, “?” = N/A, “ + ” = Suspicious, “ + + ” = Slight, “ + + + ” = Obvious, “ + + + + ” = Severe.
Results: The mortality and morbidity are noticeble in PROM group than the non-PROM ones, these results are close correlation with the inflammation reactions, based on IMBALANCE mechanisms. We have to indicate that, infection is one of the encountered inflammation responses.
Conclusions: Inflammation reaction, mostly rejection type response can be noticed when a cell/tissue is implanted to an organism, because of the immune difference. In pregnancy state this is not evident. When looking from inflammation/immunological mechanism perspective, some clinical problems at the mother and the infant's, can be fit to some inflammation responses, like PROM. The severity of reactions guides to the early and late prognostic indicator of the PROM cases.
IS-03-022 Nitric oxide induction of cervical ripening: A new approach
F. Facchinetti, S. Paganelli, G. Dante, V. De Pace
Mother Infant Dept. Obstetric and Gynecology Unit, University of Modena and Reggio Emilia, Modena, Italy
Endogeneous NO is a free radical gas produced from L-Arginin by NO synthetase (NOS). The current opinion is that NO acts upon myometrium exacting muscular relaxation in the same way as it operates inside other smooth muscular cells, through sGC activation. During physiological pregnancy NO is synthesized inside myometrium and it is required keeping uterus quiescent. Inside throphoblast high iNOS levels were detected. They decrease gradually towards term.
In contrast with myometrim quiescence, cervical iNOS activation (after inflammatory stimulation) leads to a rapid increase of NO which allows cervical ripening determining a considerable increase of jaluronic acid, water percentage and a decrease of collagen content.
The role of NO on cervical ripening is supported by experimental models through administration of NO donors as isosorbide mononitrate and sodium nitroprusside applied inside vagina or cervix. After their administration, at histological approach, collagen fibres appear wide spaced and picnotic vesicles are observed as a sign of digestive fibroblast activity. NO cervical activity is also identified by Matrix Metallo-proteinase action, namely MMP-9, and cellular apoptosis.
MMP-9 is an enzymatic protein produced by macrophages and it controls cellular matrix composition. NOx and natriuretic peptide, both using cGMP as second messenger, show antifibrinolitic action by inhibition of collagen synthesis and MMP-9 activation. Another way is rapresented by apoptosi activation; when NOx is in right concentrations to activate sGC, apoptosis is begun by kynasi G-dependent protein or by direct modification on proteins without utilization enzymes as modulators (s-Nitrosilation).
Apoptosis is a process leading to cellular death through new enzymatic proteins production which causes nuclear fragmentation, chromatin thickening, loss of cellular adhesion and other process.
The same mechanisms operate also preterm. Patients with preterm uterine contractions and shortening of the cervix slow increased levels of NO, Interleukin-1 and IL6 in cervical fluid respect with asymptomatic contest. This suugest that mechanism behind the onset of preterm labour involve a local activation of NO.
High concentration of NO in cervix near parturition is supported by administration of PGE2 (Dinoprostone) in preinduction of labour. Prostaglandin induced cervical ripening is associated with local NO relase six hours after drug stimulation. Then NO plays an active role in cervical remodelling since it positively correlates with cervical shorteing at ultrasound evaluation.
In conclusion, NO seems the main driver of cervical ripening in different conditions throughout pregnancy.
IS-03-027 The use of pharmacogenetics to improve pain treatment in the newborn
J.N. van den Anker
Division of Pediatric Clinical Pharmacology, Children's National Medical Center, Washington, DC, USA; Departments of Pediatrics, Pharmacology and Physiology, George Washington University School of Medicine and Health Sciences, Washington, DC, USA; Department of Pediatrics, Erasmus MC-Sophia Children's Hospital, Rotterdam, The Netherlands
Aim: To help you understand the potential role of pharmacogenetics for improving pharmacotherapy of pain in newborn infants.
Methods: The two most important determinants (ontogeny and pharmacogenetics) of age-associated differences in the clearance of drugs frequently used in neonatal pain management will be presented. More specifically, the impact of different metabolizing enzymes (i.e. CYP2D6, CYP2C8, CYP2C9, CYP3A4) and different receptors and genes (i.e., μ-opioid receptor, catechol-O-methyltranferase [COMT] gene, β-arrestin-2 gene) will be discussed using morphine, tramadol and ibuprofen as examples.
Results: Developmental changes in activity of several drug metabolizing enzymes and drug transporters show different patterns during the first weeks/months of life. These developmental changes are superimposed on the pharmacogenetic background of the individual neonate. However, for many medicines we still need to discover the delicate interrelationship between pharmacogenetics and growth and development.
Conclusions: There is a lack of knowledge on the impact of pharmacogenetics on the developmental changes in drug metabolizing and drug transporting capacity. It is therefore crucial to investigate the close relationship between genetics and development to further improve drug therapy in the neonate. Eventually this will lead to personalized pain management in this fragile patient population.
IS-03-028 Nasal cpap: Finally a ventilator mode that permits alveolar formation in preterm neonates
K.H. Albertine, R.H. Lane, D.M. Null, L. Moyer-Mileur, M.J. Dahl, A. Shumway
University of Utah, 295 Chipeta Way, Salt Lake City, USA
Background: In the premature infant, volume trauma from conventional ventilation (CV) contributes to the pathogenesis of chronic lung disease (CLD), which is characterized by poor gas exchange and alveolar simplification. Similarly consequences occur in preterm lambs. Nasal continuous positive airway pressure (nCPAP) is being used more because CLD incidence is less than with CV. We have used nCPAP to manage preterm lambs for up to 3d. Their gas exchange and secondary septation are better than CV. Whether those benefits persist in preterm lambs managed for 21d has not been determined.
Objective: We hypothesized that management of preterm lambs for 21d, using nCPAP, will result in improved gas exchange and alveolar secondary septation compared to CV.
Design/Methods: Preterm lambs were delivered at 132d gestation. Lambs were treated with antenatal steroids and postnatal surfactant, and managed with nCPAP (n = 5) or CV (n = 3) for 21d. An oscillatory circuit delivered CPAP to the nose. Target PaO2 was 60–70 mmHg; target PaCO2 was 50–60 mmHg.
Results: For the target PaO2, the fractional inspired O2 was significantly less in nCPAP lambs (30 ± 8 mmHg; mean ± SD) vs. CV lambs (54 ± 14 mmHg) at weeks 1, 2, and 3 of life (p < 0.05). For the target PaCO2, peak inspiratory pressure, positive end-expiratory pressure, and mean airway pressure also were significantly less in nCPAP lambs (19 ± 5, 5 ± 3, 4 ± 2, cmH2O, respectively) vs. CV lambs (26 ± 8, 9 ± 3, 6 ± 2, cmH2O) at weeks 1, 2, and 3 of life (p < 0.05). Alveolar secondary septation was significantly greater in nCPAP lambs, as reflected by greater radial alveolar count (6 ± 2 vs. 2 ± 1 for CV; p < 0.05) and secondary septal volume density (22 ± 4% vs. 5 ± 3% for CV; p < 0.05).
Conclusions: NCPAP in preterm lambs for 21d resulted in improved gas exchange and alveolar secondary septation. [Support: CHRC, HL62875, HL56401]
IS-03-033 Perinatal injury of immature brain: Current concepts of pathogenesis
H. Hagberg
Perinatal Center, Sahlgrenska Academy, East Hospital, Goteborg, Sweden
Brain injury in term and preterm infants continues to be a clinical problem. The etiology behind these lesions is multifactorial but cerebral hypoxia-ischemia (HI) and infection-inflammation are likely contributors. There are evidence that brain injury after severe birth asphyxia develops with a considerable delay and recent hypothermia studies provide proof of concept that post-HI neuroprotective treatment is a clinical possibility. Therefore, we urgently need to achieve a better understanding in the pathogenesis.
Mitochondria are key regulators of cell death through their role in energy metabolism and calcium homeostasis, their ability to release apoptogenic proteins and to produce reactive oxygen species. We find that secondary brain injury is preceded by impairment of mitochondrial respiration, signs of membrane permeability transition, intra-mitochondrial accumulation of calcium and release of pro-apoptotic proteins like cytochrome C and apoptosis inducing factor, AIF. These mediators will induce both caspase-dependent and caspase non-dependent cell death as supported by the protective effect of some caspase inhibitors, transgenic upregulation of the anti-apoptotic protein X-linked inhibitor of apoptosis (XIAP) and downregulation of AIF.
It is still unclear, however, what upstream mechanisms that are responsible mitochondrial impairment and permeabilization. We hypothesize that the following three routes are critical: 1) Necrotic route. Overactivation of excitatory amino acids and voltage-gated receptors will lead to elevation of intracellular calcium. NMDA receptor activation and inflammation leads to the production of nitric oxide (NO)/reactive oxygen species (ROS), which will open the membrane permeability transition (MPT) pore spanning across the inner and outer mitochondrial membrane; 2) Apoptotic route. An increased pro-/antiapoptotic Bcl-2 family protein balance will lead to Bax-mediated permeabilization of the outer mitochondrial membrane through protein-protein interactions. Bcl-2 proteins, in turn are affected by mitogen activated protein kinases (MAPK) like JNK, PI3 kinase/Akt and several trophic factors (IGF-1, secretagogues, BDNF and EPO). 3) DNA damage/PARP route. ROS/NO and other mediators induce DNA damage that activates the DNA repair enzyme poly(ADP-ribose) polymerase (PARP)-1 and the formation of poly(ADP-ribose) polymers (PAR). PAR, in turn, trigger, via unknown mechanisms, the mitochondrial release of AIF.
Summary: HI and inflammation will activate necrotic and apoptotic pathways and trigger DNA damage that will lead to mitochondrial permeabilization (MPT-pore and outer membrane pore) accompanied by metabolic impairment, disturbances in intracellular calcium regulation and release of pro-apoptotic proteins.
IS-03-036 Inflammation and cytokines and perinatal brain injury: Clinical implication
E. Saliba
INSERM 619, CHRU, Universite Francois Rabelais, Tours, France
It is now well established that infection and inflammation play an important role in the pathogenesis of neonatal brain damage. Brain cells can produce cytokines and chemokines, and can express adhesion molecules that enable in situ inflammatory reaction. The accumulation of neutrophils early after brain injury is also believed to contribute to the degree of tissue loss. Intrauterine infection is now recognized as one important initiator of premature rupture of the membranes and as a risk for premature birth, especially birth before 30 weeks gestational age. The role of the cytokines cascade in the induction of preterm labor and premature rupture of the membranes has been discussed in detail by many authors. Chorioamnionitis is associated with a 3-fold increased risk of delivery before term with intact membranes and a 4-fold increased risk of preterm birth due to prelabor rupture of membranes. Bacterial vaginosis at 23–26 weeks of gestation increases the risk of preterm delivery by 50%. Some of these intra-amniotic cytokines that link intra-uterine infection with preterm delivery seem to be of fetal origin. Fetal umbilical vein cytokine levels, but not maternal serum values, seem to correlate with the presence and severity of chorioamnionitis and umbilical vasculitis. These observations support the hypothesis that the cytokine cascade leading to labor has fetal origins. IL-6 levels are higher in the cord blood of newborns whose mothers had clinical and histological chorioamnionitis than in their unexposed control. In a large prospective study we have shown that elevated cytokine levels in the blood serum and the CSF are associated with severe chorioamnionitis and fetal vasculitis.
Brain ischemia is also associated with the expression of inflammatory mediators in the central nervous system. Hypoxia-ischemia induces an inflammatory response in the immature and adult rodent brain, characterized by the expression of IL-1 and TNF-α.
A rapidly expanding body of evidence implicates diverse pro-inflammatory cytokines as potential mediators of perinatal brain injury. Hypoxia-ischemia and fetal infection appear to share some characteristics including elevated levels of cytokines. The relevance of cytokine actions to a variety of neurological disorders has opened a potentially fruitful area of research and therapeutic development.
IS-03-38 The impact of shoulder dystocia training for delivery room staff on the incidence of brachial plexus injury
A. Whitelaw2, J. Crofts1, E. Yard1, S. McKenna1, S. Wilson1, G. Attilakos1, T. Sibanda1, C. Winter1, T. Draycott1
1Obstetrics & Gynaecology, Southmead Hospital, a, Bristol, U.K.; 2Clinical Science, University of Bristol, a, Bristol, U.K.
Objective: Shoulder dystocia can occur unexpectedly after an otherwise normal pregnancy and can produce persistent disability from brachial plexus injury. Nerve injury is sometimes due to inappropriate traction on the shoulder. It has been suggested that skilled manipulation can reduce nerve injury more than episiotomy. We have developed a novel pelvic mannequin for shoulder dystocia training (1). The purpose of this study was to determine whether such training was followed by a reduction in brachial plexus injury.
Methods: In August 2000 compulsory training in obstetric emergencies was instigated for all delivery room staff. This intrapartum training included a hands-on session with the shoulder dystocia mannequin. Retraining is mandatory every year. We used a prospectively maintained neonatal database to identify brachial plexus injury from January 1st 1999 until September 30th 2002. This period was divided into pre-training (Jan 1999 – Aug 2000) and post-training (Sept 2000–September 2002).
Results: During pre-training 9 cases of dystocia-related brachial plexus injury occurred in 5106 vaginal births (1.76/1000). During post-training there were 3 such brachial plexus injuries in 6516 vaginal births (0.46/1000). Relative risk 0.26 (CI 0.07 to 0.97).
Conclusions: Our findings lend support to the hypothesis that practice in manipulating out of shoulder dystocia can reduce brachial plexus injury.
IS-03-39 Parental stress and reduced interaction with preterm infants: Cluster randomised trial of a parenting intervention during neonatal intensive care
A. Whitelaw3, C. Glazebrook1, N. Marlow1, C. Israel2, T. Croudace3, S. Johnson1, I.R. White4
1Psychiatry and Child Health, University of Nottingham, a, Nottingham, U.K.; 2Clinical Science, University of Bristol, a, Bristol, U.K.; 3Psychiatry, University of Cambridge, a, Cambridge, U.K.; 4MRC Biostatistics Unit, Cambridge, a, Cambridge, U.K.
Objective: Maternal stress, decreased interaction and delayed neurobehavioural development are common after preterm birth. We aimed to evaluate a parenting intervention commenced shortly after birth.
Methods: The design was a cluster-randomised controlled trial with a crossover design and 3 month washout period, conducted in 6 neonatal intensive care units (ICUs). Infants born at less than 32 weeks gestation were eligible. The intervention was the Parent Baby Interaction Programme (PBIP) – a series of activities designed to promote maternal sensitivity to infant cues – was delivered by research nurses, from 7–14 days after birth, until 6 weeks post-discharge. Trial outcomes were Neurobehavioral Assessment of the Preterm Infant (NAPI) at 35 weeks gestation, Nursing Child Assessment Teaching Scale (NCATS) at hospital discharge, Parenting Stress Inventory (PSI) at 3 months post term and responsivity subscale for Home Observation for Measurement of the Environment (HOME) at 3 months post term.
Results: 112 infants were recruited in the intervention phases and 121 in the control phases. Mean standardised NAPI scores at 35 weeks did not differ between the groups. Both groups had low but similar NCATS caregiver scores prior to discharge (36.6 in the PBIP group and 37.4 in control, mean difference −0.7, 95% CI −2.7 to 1.4) and at 3 months adjusted age. Mean PSI scores for the PBIP group were 71.8 compared to 67.9 for controls (mean difference 3.85, 95% CI −4.7 to 12.4) and HOME-responsivity scores were similarly distributed between groups.
Conclusions: Less than one hour per week of a parenting interaction programme had no measurable effects on infant neurobehavioural function, mother-child interaction or parenting stress.
FC-11-001 Keeping a population perspective: Mortality in 10 population-based european cohorts of very preterm births from the mosaic study
E.S. Draper1, J. Zeitlin2, A. Fenton3, T. Weber4, G. Breart2, B. Misselwitz5, G. Martens6, J. Gerrits7
1University of Leicester, Leicester, UK; 2INSERM, Paris, France; 3Royal Victoria Infirmary, Newcastle, UK; 4Hvidovre Hospital, Hvidovre, Denmark; 5Institute of Quality Assurance, Hesse, Germany; 6Centre for Perinatal Epidemiology, Brussels, Belgium; 7UMC ST Radboud, Nijmegen, Netherlands Antilles
Aims: The survival of very preterm (VPT) babies has improved dramatically since the 1980s. However, accurate estimates of mortality after VPT birth are not available in most countries. Many studies include only babies admitted to NIC, excluding babies that are not resuscitated at birth, while population based registers differ in inclusion criteria and completeness. Here, the MOSAIC birth cohort is used to illustrate mortality rates variations resulting from the use of different population definitions for births <32 weeks gestation.
Methods: All births, including terminations of pregnancy, late fetal losses and stillbirths, 22+0 to 31+6 weeks gestation were included in the MOSAIC birth cohorts in 10 European regions. Data were collected using a standardized instrument, verifying inclusions against birth registers to ensure completeness. 7230 babies were followed to death or discharge home. Mortality rates were computed using several denominators: all births, births alive at onset of labour, live births and babies admitted to NIC.
Results: Overall mortality rates (including SBs but excluding TOPs for congenital anomalies) ranged from 24 to 50% by region. Mortality rates ranged from 15 to 35% for fetuses known to be alive at the onset of labour, 11 to 35% for live born infants and 8 to 33% for those infants admitted to NIC. Regional rankings differed depending on which measure of mortality was used: in the 2 regions from France and the Netherlands mortality among babies admitted to NIC was low: 12% (ranking 3rd/4th out of the 10 regions), but was much higher for fetuses alive at the onset of labour (29 and 28% respectively, ranking 8th and 9th). In contrast, differences between these rates was much less marked in Hesse in Germany (12% vs. 9%) and in Eastern Denmark (15% and 11%). Differences were most marked for VPT babies, but also affected regional rankings for mortality among babies 28 to 31 weeks of GA.
Conclusions: The inclusion of information on SBs, intrapartum and labour ward deaths is essential for assessing the mortality of VPT births, especially <28 weeks gestation. In many countries, decision making about viability takes place in the maternity unit, reflecting differences in obstetrical practices and health system factors. Comparison of the mortality of VPT babies between countries using data from NICUs will give biased results.
FC-11-002 In-hospital mortality and morbidity of very preterm babies in 10 regions of europe in 2003 in the mosaic study
J. Zeitlin1, J. Gadzinowski2, E.S. Draper3, K. Boerch4, L. Gortner6, L. Kollee5, E. Papiernik7
1INSERM U149, Paris, France; 2Dept. of Neonatology, Department of Medical Science, Poznan, Poland; 3Department of Epidemiology, University of Leicester, Leicester, UK; 4H.S. Hvidovre Hospital Paediatrics, Hvidovre, Denmark; 5University Medical Center Nijmegen, Nijmegen, The Netherlands; 6University of the Saarland, Pediatric and Neonatal Clinic, Homburg, Germany; 7Maternité Port-Royal, Paris, France
Context: Very preterm babies face a high risk of death in infancy and of longer term disabling impairments. The MOSAIC study provides comparable information on population-based cohorts of very preterm babies in 2003 in 10 European regions.
Methods: All babies delivered between 22 and 31 weeks of gestational age and followed to discharge home from hospital were included in the MOSAIC study in ten regions in 9 European countries (Denmark, Belgium, France, Germany, Italy, the Netherlands, Poland, Portugal and UK). Data were collected using a common instrument and protocol. This analysis compares mortality and morbidity of live births delivered from 24 to 31 + 6 weeks of gestation without lethal congenital anomalies (N = 4913 babies) standardized for gestational age and sex.
Results: For babies born alive before 28 weeks of gestation, mortality rates are half as high in lower mortality regions (18–25%) in comparison with higher mortality regions (50–58%). In most regions (6 out of 10), however, outcomes are similar – between 35 and 40% die before discharge home. At 28 to 31 weeks GA, in-hospital mortality is 3% in low mortality regions vs. around 7% in most other regions. Among survivors to discharge, regions with similar mortality rates differ in the prevalence of IVH grades III and IV and cystic PVL: 3 to 4% vs. 7 to 13%. Some tradeoffs are observed between mortality and morbidity: lower mortality countries have higher morbidity linked to the lower gestational age of their survivors, however this does not explain the variation in morbidity rates.
Conclusion: There are significant differences in in-hospital mortality and morbidity for very preterm babies born alive in European regions. Both measures of mortality and morbidity are necessary to provide a complete description of health outcomes for these babies and assess the longer-term health consequences related to very preterm birth.
FC-11-003 A multicenter, pilot study of aerosurf™ delivered via nasal cpap to prevent rds in pre-term neonates
J. Mazela1, N. Finer2, A. Merritt3, G. Bernstein4, L. Job5, G. Liu1
1Discovery Laboratories, Warrington PA, USA; 2Univ. CA – San Diego, University, San Diego CA, USA; 3Oregon HSU, University, Bend OR, USA; 4Sharp Mary Birch Hosp., Hosp., San Diego CA, USA; 5Loma Linda Med. Center, Medical, Loma Linda CA, USA
Background: Surfactants significantly reduce mortality and morbidity in pre-term infants, but require endotracheal (ET) administration that may result in iatrogenic sequelae. Nasal continuous positive airway pressure (nCPAP) has been proposed as an alternate treatment strategy. Failure rates using nCPAP alone, have been reported as high as 70% (Reininger et al. 2005). Whereas pharyngeal instillation of surfactant may be an alternate delivery route, aerosolization delivered via nCPAP to preterm infants has not been systematically studied.
Objective: Establish the feasibility of aerosolizing a novel peptide-containing synthetic surfactant, Aerosurf (aerosolized lucinactant), delivered prophylactically by nCPAP to preterm infants at risk for respiratory distress syndrome (RDS).
Design/Methods: Neonates were stratified by GA (30–32 wks; 28–29 wks), and enrolled into 2 groups at 4 centers in the USA. Aerosurf 20 mg/ml was delivered via a vibrating membrane nebulizer [Aeroneb® Pro, Artemis Med. UK]. Initial 3-hr treatments began within 30 min of life; 3 additional treatments were permitted within 48 h of life, based on clinical response. Each treatment was separated by at least 3 hrs in the group 1, and 1 hr in group 2.
Results: Of the17 infants studied (BW 1033–2296 gm), 11 of 30–32 wks GA, and 6 of 28–29 wks, 11 (64%) required only the initial treatment, and 1 infant received 4 doses. All infants survived; 6 (36%) required subsequent ET surfactant. FiO2 (mean/median) at baseline was 0.4/0.3, and at 4 hrs 0.32/0.25. The 24-h RDS rate was 24%, and 28-day BPD rate was 11.7%. The procedure was generally well tolerated; transient desaturation during dosing was not associated with bradycardia or hypotension.
Conclusions: The safe administration of an aerosolized surfactant (Aerosurf) via nCPAP in preterm infants at risk for RDS may provide an alternative to intratracheal surfactant administration. Further studies are needed to evaluate this approach for surfactant replacement in the premature infant.
FC-11-004 Positioning stabilize the states and the autonomic nervous activity in preterm infants
M. Miyata1, T. Hata2, H. Mizutani1, M. Takeuchi1, M. Kubota1, T. Yamazaki1
1Dept. of Pediatrics, School of Medicine, Fujita Health University, Toyoake, Japan; 2Division of Clinical Pathophysiology, School of Health Science, Fujita Health University, Toyoake, Japan
Objective: The purpose of this study is to evaluate the effect of positioning on the states and the autonomic nervous activity in preterm infants.
Methods: Twelve preterm infants (GA: 32.1 weeks, BW: 1545 g, post-conceptional ages: 32 to 36 weeks) were enrolled. For the first 3 days, they received routine cares including the change of their body position at prone, supine and side-lying, and did not receive any other interventions. Thereafter, they received nesting with special aids to keep their body and extremities in appropriate position for the next 3 days. The video recordings and the biosignal recordings including ECG, EOG and EEG were performed on each third day. States of infants were assessed with the Brazelton Neonatal Behavioral Assessment Scale. Heart rate variability (HRV) spectrum was obtained by using the fast-fourier transformation. Power spectrum density (PSD) of low frequency area (LF) and high frequency area (HF) and LF/HF were obtained from HRV spectrum. Paired and unpaired Student's t-tests were used for statistical analysis.
Results: The times of state 1 and 2 were significantly longer in the intervention period (p = 0.025). PSDs of LF and HF were decreased by positioning (LF: p < 0.0001, HF: p < 0.0001). LF/HF did not change significantly.
Conclusions: From our results, the ratio of sympathetic nervous activity to parasympathetic nervous activity did not change, while sympathetic nervous tone was reduced by positioning. It is concluded that positioning may stabilize not only the behavioral state but also the autonomic nervous activity in preterm infants.
FC-11-005 A randomized controlled trial of an early intervention program in preterm infants: Outcome at two years corrected age
P.I. Kaaresen1, J. Tunby2, J.A. Ronning2, S.E. Ulvund3, L.B. Dahl1
1Pediatric Department, University Hospital North Norway, Sykehusvn, Tromso, Norway; 2Institute of Clinical Medicine, University of Tromso, Sykehusvn, Tromso, Norway; 3Institute for Educational Research, University of Oslo, Blindern, Oslo, Norway
Objective: To examine whether an early intervention program can improve cognitive and behavioral outcome and reduce parenting stress in preterm infants.
Methods: A randomized controlled trial of preterm babies with a birth weight (BW) <2000 g treated at the University Hospital North Norway, Tromso, Norway (March 1999 to August 2002). A term control group (N = 75) was also recruited. The intervention program was a modified version of The Mother-Infant Transaction Program and consisted of seven daily sessions during the week prior to discharge, followed by four home visits by specially trained nurses. The unit's standard discharge procedure was followed in the preterm controls (PC). Cognitive outcome was assessed with Bayley's MDI. The Child Behavior Checklist/2–3 (CBCL) and Parenting Stress Index were administered to the mothers and fathers.
Results: Mean BW was 1407 (SD 434) in the preterm intervention group (PI) (n = 66) and 1398 (426) in PC (n = 69). MDI was 95.1 (17.3) in PI compared to 90.3 (19.9) in PC and 104.1 (11.1) in term controls. When adjusting for maternal education, the mean difference between the preterm groups was 3.8 (95% CI – 2.6–10.2), p = 0.24. Both mothers and fathers in PI reported consistently lower scores in the CBCL, but no difference was significant. The mothers in the PI reported significantly lower stress than the mothers in PC in all domains, while the fathers in the PI reported significantly lower stress in Child Domain.
Conclusion: This early intervention program did not improve cognitive or behavioral outcome at two years corrected age, but reduced Parenting Stress to a level comparable to term controls. Further follow-up is in progress.
FC-11-006 Dna repair capacity in newborns after oxidative stress
R. Ciardelli1, K. De Bont2, I. Decordier2, G. Delanghe1, I. Van Herreweghe1, M. Kirsch-Volders2, D. Haumont1
1Neonatal Unit, St-Pierre University Hospital, Brussels, Belgium; 2Laboratory of Cellular Genetics, Brussels, Belgium
Oxidative stress (OS) might be an important contributor to neonatal complications. Effects of OS on DNA damage are not well documented in this age group.
Aim: To investigate in vitro DNA damage and repair after OS in healthy term newborns compared to adults and to analyse the importance of genotypes in the DNA repair systems.
Methods: Lymphocytes from cord blood and adult peripheral blood from ten mother-daughter couples were exposed in vitro to H2O2. Genotoxic effects were tested using alkaline comet assay and micronucleus assay. Secondly genotypes of some important repair genes were defined for all individuals: hOGG326(BER), XRCC1194(BER), XRCC1280(BER), XRCC1399(BER), XPD312(NER), XPD751(NER), and XRCC3241(DSBR). The MTHFR222 genotype was also investigated.
Results: Initial DNA damage was similar for neonates compared to their mothers but because of a better DNA repair capacity final DNA damage was lower for newborns. When correlating DNA damage to the different genotypes, only MTHFR222 variant genotype had a significant negative effect. The amount of fixed DNA damage was not significantly different. Multivariate analysis showed a significant protective effect of maternal antioxidant supplementation during pregnancy.
Conclusions: Newborns tend to have a better DNA repair capacity after OS compared to adults. A better knowledge of the influence of the genotypes of DNA repair genes should allow a better understanding of individual susceptibility to OS. This is a preliminary study to assess healthy newborn's sensitivity to DNA damage after OS. Further studies concerning the premature infants are needed.
FC-12-001 Thrombocytopoiesis in preterm newborns
A. Wasiluk1, M. Mantur2, H. Kemona2, M. Szczepanski1
1Department of Neonatology, Medical University of Bialystok, Bialystok, Poland; 2Department of Clinical Laboratory Diagnostics, Medical University of Bialystok, Bialystok, Poland
Background/Aims: Thrombopoietin (c-mpl ligand) is, in fact, a proliferative factor for MK-CSF. C-mpl is a receptor specific to the megakariocyte lineage. The regulation mechanism of the circulating TPO level in human preterm newborns remains poorly recognized. Reticulated platelets (PLRET) constitute the youngest platelet population. The measurement of PLRET may be useful for evaluation of thrombopoietic response. Therefore decided to evaluate the values of TPO, PLRET and PLT in preterm newborns.
Patients and Methods: The study was undertaken on 51 preterm newborns, 25 girls and 26 boys. They fitted all criteria for preterm newborns. Blood was collected from the umbilical artery immediately after cutting the umbilical cord. The evaluation of thrombocytopoiesis was performed by the following methods: TPO-Quantikine human TPO kit, PLRET – Retic-Count kit, PLT – Technicon H3 System.
Results: Concentrations of TPO and percentages of reticulated platelets were greater in the female group (116.8 pg/ml; 3.56%) than in the male group (105 pg/ml; 3.42%). The changes were not statistically significant, perhaps as a result of the very wide range of parameters tested. The blood platelet count was higher in female preterm newborns 256 × 109/l) than in male preterm newborns (237 × 109/l).
Conclusion: The presented data may indicate that thrombocytopoiesis is more active in female than in male preterm newborns.
FC-12-002 Cord blood or postnatal arterial blood for the diagnosis of severe birth asphyxia?
J. De Buyst1, D. Vermeylen2, A. Pardou2, J.-L. Wayenberg1
1Hopital Francais, Universite Libre de Bruxelles, Brussels, Belgium; 2Hopital Erasme, Universite Libre de Bruxelles, Brussels, Belgium
Objective: To evaluate the value of parameters of acidosis determined in cord blood and in postnatal arterial blood as potential markers of the neurological neonatal evolution after birth asphyxia (BA).
Methods: BA was defined as base deficit (BD) ≥10 mEq/l either in arterial cord blood (UA), venous cord blood (UV) or radial artery blood (ART) taken between the first 30 to 60 min. of life. Term BA infants born from 1998 to 2005 (n = 147) were included if pH and blood gases were measured in both UA/UV and ART. Severe birth asphyxia (SBA) was defined as BA followed by moderate/severe neonatal encephalopathy. Differences in pH, pCO2 and BD between UA/UV and ART samples were checked using paired t-test. The clinical value of each parameter for diagnosing SBA was assessed using the ROC curve methodology.
Results: One hundred and one patients met the inclusion criteria, 15 of whom developed moderate/severe encephalopathy. All differences between UA/UV and ART parameters were statistically significant (p < 0.05 for pH; p < 0.001 for pCO2; p < 0.001 for BD). The area under the ROC curve (±SE) of parameters for SBA was: 72.5% ± 8.1% for UApH, 65.7% ± 9.5% for UABD and 71.6% ± 9.6% for UApCO2; 49.9% ± 12.5% for UVpH, 58.3% ± 12.8% for UVBD and 37.5% ± 11.2% for UVpCO2; 85.9% ± 6.3% for ARTpH, 89.1% ± 5.7% for ARTBD and 43.5% ± 8.3% for ARTpCO2.
Conclusions: For the diagnosis of severe birth asphyxia the pH and BD measured in postnatal arterial blood should be considered.
FC-12-003 Nitration pattern of plasma proteins in newborns suffering from perpartal asphyxia: Preliminary results
S.P. Bottari1, A. Csibi1, D. Vermeylen2, E. Damis3, C. Cavedon4, J. Touma4, A. Salame4, J.L. Wayenberg4
1CHU, Université de Grenoble, La Tronche, France; 2HU Erasme, ULB, Brussels, Belgium; 3CHIREC, Brussels, Belgium; 4Hopital francais-Cesar de Paepe, ULB, Brussels, Belgium
Hypoxo-ischemia is known to induce an increased generation of peroxynitrite, which is able to nitrate specific cellular and plasmatic proteins.
Objective: To identify plasma proteins whose nitration is increased in newborns who suffered perpartal asphyxia.
Methods: Plasma was prepared from arterial cord blood (UA), venous cord blood (UV), and venous blood taken at days 1 and 4 (V1 and V4) from normal or asphyxiated newborns. Samples were subjected to SDS-PAGE and subsequently transferred to PVDF membranes. Blots were probed with a polyclonal anti-nitrotyrosine antibody and revealed with HRP-conjugated anti-rabbit IgG.
Results: Variations in the degree and the pattern of plasma protein nitration were observed in asphyxiated vs. normal newborns.
Conclusion: The nitration pattern of plasma proteins in newborns indicates the occurrence of a nitrating stress in perpartal asphyxia and should allow the identification of specific nitroproteins which could be used as potential markers in the follow-up of asphyxiated newborns.
FC-12-004 Plasma creatinine levels in extremely premature infants
S. Thayyil, S. Shaik, A.K. Sinha, S.T. Kempley
Royal London Hospital, Whitechapel, London, UK
Background: Plasma creatinine is the most widely used marker of renal function, with levels above 150 μmol/l considered indicative of renal failure in infants and children. Whilst it is accepted that creatinine values are higher in extremely premature infants there is little reference data for this population for first few days after birth. The best available data suggest creatinine levels rise to 221 μmol/l (95% CI 195–247) in the first 3 days of life in babies of 23–26 weeks gestation, and 179 μmol/l (95% CI 158–200) at 27–29 weeks.
Aim: To determine creatinine levels in a more recent cohort of extremely premature infants.
Methods: Analysis of plasma creatinine levels in the first 8 weeks of life (measured using modified Jaffe reaction as part of routine clinical care) from 161 consecutive premature infants ≤28 weeks gestation admitted to a single neonatal intensive care unit. Infants with renal malformations or major perinatal hypoxia were excluded.
Results: Mean gestation was 26.0 weeks (SD 1.6) and mean birth weight was 894 g (SD 246). 30/161 (18%) died. 83 (76%) had antenatal steroids. Creatinine levels peaked between 40–78 hours of age at a mean peak level of 119 (23) μmol/l. Birth weight (r = −0.37) and gestation (r = −0.38) correlated inversely with peak creatinine levels on multiple regression (p < 0.05).
Mean creatinine values with 10th & 90th percentiles.
Conclusion: Plasma creatinine levels in this cohort were much lower than previously published data. Age (gestational and chronological) based reference charts should be used to interpret creatinine results in extremely premature babies.
FC-12-005 Nitrated albumin as a potential marker of nitrating stress in newborns: Preliminary results
C. Cavedon1, S.P. Bottari2, D. Vermeylen3, E. Damis4, J. Touma1, A. Salame1, J.L. Wayenberg1
1Hopital francais-Cesar de Paepe, Universite Libre de Bruxelles, Brussels, Belgium; 2CHU, Universite de Grenoble, Domaine de la Merci, La Tronche, France; 3HU Erasme, Universite Libre de Bruxelles, Brussels, Belgium; 4CHIREC, Brussels, Belgium
Hypoxia-ischemia is known to induce an increased generation of peroxynitrite, which is able to nitrate specific proteins among which albumin.
Objective: To develop a suitable dosage of nitrated albumin (nitralbumin) in plasma and to establish reference values in normal newborns.
Methods: We have developed a novel double-sandwich ELISA for assaying plasma nitralbumin. An affinity-purified anti-nitrotyrosine IgG was used as capture antibody, peroxidase-conjugated anti-human albumin IgG as detection antibody and nitrated human serum albumin as a standard. Nitralbumin determinations were performed in normal newborns on arterial cord blood (UA), venous cord blood (UV) and venous blood taken at days 1 and 4 (V1 and V4) of life. Blood samples were collected in EDTA containing tubes and rapidly centrifuged at 4°C.
Results: The sensitivity of the assay is 1 ng/ml, the intra/interassay CV's were <10%. The median nitralbumin concentration in pooled adult plasma was 10 ng/ml. The median (25th and 75th percentile) nitralbumin concentration in UA (n = 40), UV (n = 43), V1 (n = 23) and V4 (n = 34) were 4.6 ng/ml (2.6, 11.6), 6.3 ng/ml (2.8, 10.5), 4.4 ng/ml (3.0, 7.0), and 4.9 ng/ml (2.5, 6.6), respectively.
Conclusion: The double-sandwich ELISA technique is a sensitive quantitative method for assaying nitrated albumin plasma concentration and is currently being tested in neonatal practice as a potential guidance for management and follow-up of newborns potentially affected by nitrating injury.
FC-12-006 Early onset hyperkalemia in premature babies
S. Thayyil, S. Shaik, A.K. Sinha, S.T. Kempley
Royal London Hospital, Whitechapel, London, UK
Background: Early onset hyperkalemia is associated with a high morbidity and mortality in premature babies. It is thought to be due to a transient deficiency in Na/K ATPase resulting in reduced potassium secretion by renal tubules.
Aim: To determine the incidence and risk factors of early onset hyperkalemia in premature babies.
Methods: Analysis of plasma potassium levels in the first week of life from 154 consecutive premature infants ≤28 weeks gestation admitted to a single NICU. Infants with renal malformation or renal failure were excluded. Potassium ≥7 mmol/l was taken as hyperkalemia.
Results: Mean gestation (25.8 [216] vs. 26 [1.6] wks), birth weight (915 g [216] vs. 982 g [255], CRIB score (5.5 [4.2] vs. 5.2 [4.1]) and steroid use (67% vs. 75%) were not significant different in babies with and without hyperkalemia. Babies who had urea levels of ≥12 mmol/l at 24 hours or phosphate level ≥2.4 mmol/l had higher chances of having hyperkalemia (54% vs. 11%, OR 9.3 (95% CI 3.2, 27) and 56% vs. 13% (OR 8.5 (95% CI 3.3, 22)). Calcium levels were inversely related to the potassium levels at 24 hrs (r = −0.47, p < .01). See .
Conclusion: Early onset hyperkalemia is common (21%) in the first 4 days of life in extremely premature infants and was associated with high phosphate, high urea levels, high birth potassium and hypocalcemia (without any increase in sodium and creatinine) suggesting a catabolic state in these babies.
FC-13-001 Increase of prematurity rate in flanders, belgium (1995–2004)
P. Jeannin1, G. Martens2, I. Debaere2
1Jan Palfijnhospital, H. Dunantlaan, Gent, Belgium; 2Studycenter of Perinatal Medicine, Hallepoortlaan, Brussels, Belgium
In the last ten years, a constant increase in the rate of prematurity has been observed. While looking for the causes of this phenomenon, different assumptions were made and tested. Before testing our assumptions, it was decided to limit the study to singletons.
The first of these assumptions was that better neonatal care and outcome could have led to a higher rate of induction in premature infants. Although an increase has indeed been observed, this was not enough to explain the whole phenomenon.
Better neonatal care could also have led obstetricians to perform caesarian sections at an earlier stage in pregnancy. Again, an increase has been observed.
There was also a significant rise in the rate of prematurity in the group of medically assisted pregnancies.
After carefully re-examining the data, excluding the previously mentioned groups, there was still a significant increase in prematurity rates.
The primary cause of this increase seems to be the age of the mother: the age-group of mothers older than 35 increased by one third, which led to an increase in prematurity rate for this group of more than 100%.
FC-13-002 The mosaic project*: Practices for extremely preterm births in the netherlands
L.A. Kollee1, J. Gerrits-Kuiper1, A.L. den Ouden2
1Univ. Med. Center, Nijmegen, The Netherlands; 2IGZ, Den Haag, The Netherlands
Objective: To study perinatal management at the lower limit of viability.
Methods: Regional units, participating in MOSAIC (n = 18), and all level 3 units (n = 10) received a questionnaire. Of all 22–31 weeks births in 2003 (n = 399) data were collected. Active obstetrical policy (for foetal survival) was defined as: level 3 referral, antenatal corticosteroids and/or caesarean section and active neonatal policy as: neonatal admission, level 3 transfer, surfactant and/or mechanical ventilation.
Results: Lowest gestational age for a caesarean section because of foetal distress was 24–27 weeks. Obstetricians would call the paediatrician for spontaneous labour 1 week earlier. In all level 3 units and in 13/18 regional units decisions to withhold or withdraw mechanical ventilation occur and parents always are involved in them. At 22/23 weeks, active obstetric policy occurred in 5% of births. For 24 weeks, this was 11%, for 25 weeks 24%. From 26 weeks on, active obstetrical policy was usual. Before 25 weeks, no liveborn infants were admitted. All died in the delivery room, usually after a decision not to treat. Of the 8 babies, liveborn after active obstetrical policy at 25 weeks, 2 were admitted. However, in none of the infants, liveborn before 25 weeks, active neonatal policy was practiced. At 25 weeks, there was active policy in 36% (5/14) of the liveborn infants but they died after a decision not to continue treatment. From 26 weeks on, active neonatal policy occurred in >95% of infants.
Conclusions: In the Netherlands, active policy at 24–26 weeks is limited, despite the existing guidelines for level 3 referral.
FC-13-003 Placental anatomopathological examination in birth asphyxia
M. Wolf, M. Depierreux, J.-L. Wayenberg
Hopital Francais, ULB, Brussels, Belgium
Whilst the exact role of birth asphyxia in the development of neonatal encephalopathy (NE) and late neurological sequels is still debated, little is known about potential placental abnormalities in this condition.
Objective: Our aim was to determine whether, after birth asphyxia, NE is associated with placental lesions.
Methods: We retrospectively collected the results of placental examination data obtained in asphyxiated term infants born from January 1999 to September 2005. Birth asphyxia was defined as significant metabolic acidosis (base deficit >10 mEq/l). Exclusion criteria were the lack of knowledge of the neurological neonatal evolution (ventilated babies) and causes of neonatal impairment other than asphyxia, such as congenital malformations, severe intrauterine growth retardation and perinatal infections. Patients were divided into two groups according to Finer's criteria: NE, or normal neurological neonatal evolution. Placental variables were weight, micro-calcifications, thrombosis, infarction, inflammation and cord implantation. Placental variables were related to NE using ANOVA and χ2 tests.
Results: Out of 86 asphyxiated infants (9, 11 and 3 with mild, moderate and severe NE, respectively), placentae were examined in 60 (6, 10 and 2 with mild, moderate and severe NE, respectively). The placental weight was significantly lower in patients who developed NE than in patients who did not (462 ± 114 g vs. 545 ± 107 g, p < 0.02). Placental infarcts were significantly found more often in NE patients (9 infarcts/18 NE patients vs. 8 infarcts/42 normal patients, p < 0.02).
Conclusion: Placental infarct and low placental weight were associated with the occurrence of NE after birth asphyxia in the term infant. Our results suggest that placental pathology may play a substantial role in the development of NE.
FC-13-004 Cancer and pregnancy: Neonatal morbidity in 21 cases
V. Alzina1, M. Suárez1, M. Martín1, M. Garraus1, P. Bastero1, S. Raggio2
1Pediatrics Department, University Hospital of Navarra, Pamplona, Spain; 2Centro de Salud San Vicente del Raspeig II, San Vicente del Raspeig, Alicante, Spain
Backround: Cancer is the second most common cause of death in women during the reproductive years, and complicates between 0.02% and 0.1% of all pregnancies. This incidence is expected to rise with the concomitant increase in age of childbearing.
Objectives: To evaluate fetal risk involved in the administration of chemotherapy during gestation and to asses the long-term efects on the exposed babies. Patients and methods: We have reviewed the clinical data of 21 newborns that were exposed in utero to chemotherapeutic agents from 1990 to 2005. Control group consists of 78 healthy newborns.
Results: Fifteen of the newborns were preterm and six were full term birth. Ten caesarean deliveries were performed in premature group and two in the other. The gestational ages were between 28 and 40 weeks. Time since the last chemotherapy treatment and delivery was between 3 days and 6 weeks. Postnatal complications were: Hyaline membrane disease (three cases), Transient Tachypnea (three) Neurosensitive deafness (two), Fetal growth retardation (two) There were no instances of placental invasion or congenital malformations. We found no significant differences between the above cases and control group with regards hemoglobine value and platelets count. Leucocytes count in cases group seems to be significantly lower than those of control group.
Comments: Cancer treatment during pregnancy is a multidisciplinary decision to be made on the basis of the specific circumstances of each patient individually. Treatment after the first trimester, when organogenesis is almost complete, is reasonably safe.
FC-13-005 Minor disabilities of premature children: How are parents coping with the possibility?
H. Bouza1, I. Antoniadou2, H. Antonopoulou2, M. Morozini2, J. Sarafidou2, M. Anagnostakou1, F. Anatolitou1, M. Xanthou1
1Aghia Sophia Children's Hospital, Goudi, Athens, Greece; 2Institute of Child Health, Goudi, Athens, Greece
Objective: The purpose of this study is to assess Very Low Birth Weight Children at a preschool age in order to detect mild neurodevelopmental disabilities and compare the results with the opinion of their parents.
Methods: Forty children, which were neonates with a birth weight < 1500 g, participated in our study. Following discharge from the NICU, the children were followed up longitudinally. During the follow up the parents were informed about the high risk of minor disabilities in that population and importance was given in early stimulation. At the age of 3 years premature children were encouraged to attend playschools with structured educational program. At the age of 4 years, they had a detailed neurodevelopmental assessment with a combination of tests: the Touwen's, the Griffiths and the Miller. A questionnaire was handed to the parents concerning the opinion they had on their child's condition.
Results: 85% of the parents believed that their child was normal, 12.5% having some difficulties and 2.5% having important problems. Among children considered normal by their parents, some presented suboptimal scores at the different subscales of the different tests mainly in coordination and performance: between 9.4–46.9% for the most representative tasks of the Touwen's test, between 24.2–40.6% for the most representative tasks of the Griffiths test and between 29.4–44.1% for the most representative tasks of the Miller test. However only 47.5% of the children had attended playschool because of the concern of the parents for viral infections.
Conclusions: Parents are giving a more optimistic view of the performance of their children compared to the results of the tests. However they prefer a more protective environment instead of the stimulating programs of playschools. Nevertheless the incidence of minor disabilities is relatively high.
FC-13-006 Maternal level of education associated with perinatal outcome
H. Cammu, G. Martens
Studycentre for Perinatal Epidemiology, Brussels, Belgium
Objective: Is there a relation between the outcome of the offspring and the education of the mother?
Study Design: Between 1999 and 2004, we linked the perinatal outcome of all deliveries in Flanders (Northern Belgium) with the level of education of the corresponding mothers. Mothers aged <20 years were excluded. Finally, 360,730 deliveries were included in the study. Five levels of education were distinguished: level (1) <6 years/ (2) 9 years/(3) 12 years/ (4) 15 years/ (5) >15 years.
Results: The educational level was strongly related to the foetal (p < 0.001) and to a lesser degree to the neonatal death (p = 0.001) suggesting a difference in health awareness between the educational levels. The perinatal death was respectively 1.21% (level 1), 0.89% (level 2), 0.56% (level 3), 0.40% (level 4) and 0.36% (level 5). Fetal mortality showed a more pronounced gradient than did the neonatal mortality. Fetal mortality: 0.89% (level 1), 0.57% (level 2), 0.35% (level 3), 0.30% (level 4) and 0.21% (level 5). Neonatal mortality: 0.32% (level 1), 0.32 (level 2), 0.21% (level 3), 0.20% (level 4) and 0.20% (level 5). The incidence of low birthweight and prematurity also showed an inverse relation with the educational level of the mother, the highest level of education had the lowest level of prematurity and low birthweight. And vice versa. Vaginal delivery, caesarean section and epidural analgesia were not correlated with the educational level of the mother.
Conclusion: The maternal level of education is an important determinant of, especially, the fetal, and, to a lesser degree, the neonatal mortality. Every step in the educational level is attended by a lowering of the perinatal death rate. Mothers with the highest level of education experienced the lowest perinatal mortality rate.
FC-14-001 The mosaic project*: Ethical decision-making policies of european maternity and neonatal units
L.A.A. Kollee1, J. Zeitlin2, M. Cuttini3, A.L. Den Ouden4, P. VanReempts5
1Univ. Med. Center, Nijmegen, The Netherlands; 2INSERM U149, Paris, France; 3Paed. Hosp. Bambino Gesù, Rome, Italy; 4IGZ, Den Haag, The Netherlands; 5UZ Antwerpen, Edegem, Belgium
Objective: In the MOSAIC project (Models of OrganiSing Access to Intensive Care for very preterm births in Europe), maternity and neonatal units policies towards ethical decision-making were explored.
Methods: In ten regions in Denmark, Belgium, France, Germany, Italy, the Netherlands, Poland, Portugal and UK, 104 maternity and neonatal units with ≥5 annual 22–31 weeks births or admissions were surveyed by a structured questionnaire.
Results: In 32% of the units, written protocols for forgoing treatment of extremely preterm deliveries or newborns were available. Of the neonatal units 76% involve parents in the decision-making. The lowest gestational age when a caesarean section would be performed for fetal distress varies between 24 weeks (Germany) and 26 weeks (France, the Netherlands). When parents are against aggressive treatment this limit moves up with 1.2 weeks and only a minority of units would perform a caesarean section before 26 weeks. In most maternity units decisions about resuscitation <25 weeks are made by a multidisciplinary team. In case of severe congenital anomalies, this proportion is even higher (80%). An ethics committee is available in 62/104 hospitals. However, in 24 of them the committee is never involved in decision-making and in 27 only in selected cases.
Conclusions: The most common lower limit of active treatment is 24 weeks, with wide variations between individual units. Neonatologists usually participate in obstetrical decisions. Most units involve parents in ethical decision-making. Decisions usually are taken without consultation of ethics committees.
FC-14-002 Doctors, patients and parents – life-and-death decisions in newborn intensive care
I.E. Engelund
Stein Rokkan Centre for Social Studies, University of Bergen, Bergen, Norway
Objective: This paper is part of a larger, qualitative doctoral project in sociology, related to life-and-death decisions in newborn intensive care. The objective is to explore and describe how neonatologists talk about and consider the parents' role in the decision-making process, and how they argue for alternative solutions.
Methods: Qualitative, semi-structured, and in-depth interviews were carried out with 15 neonatologists employed at the NICU in three different Norwegian university hospitals. The interviews were recorded and later transcribed, coded and analyzed. Data were also collected through intensive fieldwork at the same NICUs.
Results: There seems to be a common agreement among the neonatologists interviewed that the decision of whether or not to stop treatment of a critically sick newborn should rest upon the doctor. However, all of the doctors emphasized that the decision should be thoroughly discussed with the parents, and some mentioned that it would be impossible to withdraw life-supporting treatment against the parents' will. As good as none of the doctors interviewed could recall ever ending treatment against the parents' will, and a few had been in situations where the parents were the ones who started a discussion about whether it was appropriate to continue the treatment or let the infant die.
Conclusion: According to the views of the neonatologists interviewed, the decision of whether or not to stop life-supporting treatment in critically sick newborns belongs to the doctors – in close cooperation with the parents.
FC-14-003 Withholding (intensive) care in extremely premature neonates: Consensus is difficult to achieve
M. Alexander1, S. Alexander2
1Pediatrie Maternite His Bruxelles, Brussels, Belgium; 2Perinatal Epidemiology & Reproductive Health Unit, Ecole de Sante Publique, Brussels, Belgium
In Belgium, obstetricians as well as neonatologists are attempting to reflect on the difficult topic of the extreme limits of viability. From a practical viewpoint the question pertains mostly to whether there is – at present – a gestational age below which intrauterine transfer would not be recommended. Reaching agreement is however a difficult process: we will present here three examples.
1) Important contributions to thought are the protocols published by teams from countries at the borders of Belgium: the “Groningen protocol” for the Netherlands or the “Port Royal protocole” in France. The French protocol is more concerned about withholding than about withdrawing care, and is mainly targeted at hospitals which do not have intensive neonatal care (Tsatsaris et al. 2004). It recommends that intrauterine transfer is the commendable attitude from 25 weeks on, and that, earlier, it should be done, only if the parents formally demand it. In Belgium, during two meetings of the “Fonds de la Recherche Scientifique Médicale”, this position was discussed: there was agreement on the concept, but no consensus could be achieved as to which gestational age was appropriate.
2) A survey of 98 French speaking Belgian obstetricians attending a meeting of their college in 2003, showed that for ruptured membranes at 24 weeks, one third considered termination, one third “wait and see” and one third intrauterine transfer.
3) A third example of disagreement was reported in the daily newspapers. A mother, who is herself a health professional, delivered prematurely and considered that neonatal care should not be given. The obstetrical team accepted this demand, however, but the pediatric team did not and the case was brought to court.
In conclusion, we suggest with these three examples, that on this important topic there is still much work to be done, why not by a European taskforce?
FC-14-004 Funisitis and low concentrations of clara cell protein (CC10) in tracheobronchial aspirate fluid (TAF) of vlbw infants in the first days of life
W. Thomas1, N. Kawczynska-Leda2, S. Seidenspinner1, M. Chmienicka-Kopaczyk3, A. Marx4, M. Szymankiewicz2, J. Gadzinowski2, C.P. Speer1
1University Children's Hospital, Wurzburg, Germany; 2Department of Neonatology, University of Medical Sciences, Poznan, Poland; 3Department of Pathology, University of Medical Sciences, Poznan, Poland; 4Department of Pathology, University of Würzburg, Wurzburg, Germany
Objective: CC10 is the major secretory protein of Clara Cells. In vitro it inhibits leucocyte and fibroblast migration, stabilizes surfactant and suppresses the activity of phospholipase A2. In vivo studies suggest that it plays a pivotal role in lung protection as an anti-inflammatory agent. Our hypothesis was that systemic intrauterine inflammation might be associated with lower CC10 concentrations in TAF of VLBW infants in early postnatal life.
Methods: TAF was obtained three times a day on days of life 1, 3, 5, 7, 10 and 15 from ventilated VLBW infants. Specimens were centrifuged, supernatants of one day were pooled and CC10 concentrations measured by ELISA. The secretory component for IgA (SC) was used as reference protein. Placental tissue, membranes and umbilical cords of the VLBW infants were examined microscopically in order to distinguish three groups: chorioamnionitis, funisitis and control without inflammation.
Results: TAF of 42 infants (18 males) was examined. The mean gestational ages and birthweights (standard deviation) were 28.1 weeks (1.2) and 1048 g (186) for 16 controls, 27.1 (2.1) and 1087 (241) for 17 infants with funisitis and 26.5 (1.8) [p = 0.032 vs. control] and 827 (186) [p < 0.05 vs. control and funisitis] for 9 infants with chorioamnionitis. On the first day CC10 in TAF of infants with funisitis was lower (16.4 ng/μgSC; 10.5–30.6) (Median, 25th and 75th percentile) than in TA of controls (53.8, 30.2–97.1) [p = 0.004]. There was a trend for a lower concentration compared with chorioamnionitis (56.1, 16.7–92.0) [p = 0.065]. CC10 stayed lower on day 3 and 5 in the funisitis group but this difference was not significant.
Conclusions: In our cohort of VLBW infants funisitis was associated with lower TAF CC10 concentrations in the first days of life. Decreased levels of the anti-inflammatory mediator could be a considerable risk factor in the pathogenesis of pulmonary inflammation contributing to an imbalance between pro- and antiinflammator factors.
FC-14-005 Effect of MgSO4 on erythrocytes membrane lipid peroxidation – is there a correlation with observed reduced rate of bpd?
E. Gulczynska1, M. Kesiak1, A. Zjawiona1, E. Lerch1, A. Grodzicka1, J. Gadzinowski1, L. Zylinska2
1Research Institute of Polish Mother's Memorial Hospital, Rzgowska, Lodz, Poland; 2Department of Molecular Neurochemistry, Medical University of Lodz, Kosciuszki, Lodz, Poland
Objectives: Recently MgSO4 that is widely used in treatment for imminent eclampsia, is also suggested as a neuroprotective agent in preterm newborns. Now it is well documented that some perinatal conditions (e.g. PIH) produces a significant increase of TBARS in both maternal and neonatal erythrocytes. Because Mg very rapidly cross the placenta, we evaluated whether it may have an effect on lipid peroxidation of erythrocytes membranes.
Methods: The study groups consist of neonates with BBW ≤ 1500 g born from mother receiving MgSO4 (n = 24) and control group (n = 20) without Mg administration. Lipid peroxidation in erythrocyte ghosts was determined as TBARS. We have compared the TBARS level assayed just after the birth, and 24 h later. Moreover, the differences in neonatal outcome between antenatally exposed to MgSO4 neonates (n = 78) and control group (n = 293) were analyzed.
Results: In erythrocyte membranes of control group the amount of TBARS was nearly twice as high (mean 1.84; 1.46–2.82 and 1.99; range 1.44–3.2 after 24 h) as in Mg-treated newborns (mean 1.21; range 1.02–1.53 and 1.34; range 1.06–1.92/10 μg of protein, respectively). A statistically significant correlation was found between antenatal Mg treatment and rate of bronchopulmonary dysplasia (r = −0.23, p<0.001). Multiple logistic regression analysis was used to control for effect of potential confounders and association between maternal MgSO4 treatment and selected neonatal outcomes in studied population. This analysis confirmed that BPD was negatively associated with GA, BBW, Mg-administration as well as PROM, and positively with PDA, chorioamnionitis, and PIH.
Conclusion: Our results demonstrate that prenatal administration of MgSO4 markedly decreased erythrocyte membrane lipid peroxidation, and it could suggest its protective role in the reduction of BPD rate.
Supported by the grants No. 5P05E 09224 from the State Committee for Scientific Research, and No. 503-686-2 from the Medical University of Lodz.
FC-14-006 Palivizumab prophylaxis for RSV-LRTI. The czech experience
M. Cihar1, K. Liska2, K. Klenkova1
1Department of Neonatology, University Hospital Motol, Praha, Czech Republic; 2Department of Neonatology, General University Hospital, Prague, Czech Republic
Background: Respiratory Syncytial Virus (RSV) has shown to be the major cause of lower respiratory tract infection (LRTI) especially in premature infants and those with bronchopulmonary dysplasia (BPD). The RSV hospitalization rate was reduced in patients receiving palivizumab (Synagis®). Palivizumab was proven to be safe and effective.
The Czech Society of Neonatology has authorized the prescription of palivizumab for the patients with BPD since the year 2000.
Objective: To evaluate the follow-up in indicated patients after palivizumab administration.
Methods: The indication criteria used in the Czech Republic limited the number of indicated patients. The criteria included the newborns with the highest risk of serious course of RSV infection – from the point of view of serious acute LRTI, and from the point of view of a long-term morbidity.
Results: Four hundred and seventy-four patients were included. All infants received 15 mg/kg monthly. Five doses were administered by IM injection every month during the RSV seasons from 2000 to 2006. Thirty-eight infants had LRTI (8%) and only 6 were hospitalized (1.2%), but RSV was not detected in those cases.
Conclusion:
In the cohort of children with high risk of severe RSV infection, treated with palivizumab, no hospitalization related to RSV was observed. No deaths were reported. No serious adverse events occurred;
Palivizumab could be useful to prevent the nosocomial outbreak of RSV infection;
We intend to include this condition into indicative criteria;
Our data support efficacy data previously reported for Synagis;
Synagis was positively accepted by medical community and became an important part of farmacotherapy in newborns;
Our scheme of organization of imunoprophylaxis became a guide for the countries with limited financial resources.
FC-15-001 Preterm premature rupture of membranes: Does it matter?
I. Dorronsoro, L. Olazar, J. Perez Rodriguez, A. Martin Vega, J. Quero Jimenez
La Paz Hospital, Madrid, Spain
Objectives: To evaluate the frequency and neonatal consequences of prelabour preterm rupture of membranes (PPROM) in terms of lung disease, infection, necrotising enterocolitis, neurological outcome and mortality.
Methods: We performed a retrospective study and analyzed 321 cases of preterm newborns with neonatal birth weight less than 1500 grs (very low birth weight: VLBW) which were born between 2002 and 2003. Children with rupture of membranes of more than 24 hours were defined as cases, and divided in two groups: those with rupture of membranes between five days and 24 hours and those with PPROM lasting more than five days. Each case group was compared with a control group. A control group with PROM <24 hours was created with the next preterm infant with the same gestational age. As the group with PPROM ≥24 hrs and <120 hrs was too small we included some patients from year 2004. We analyzed maternal morbidity, antenatal steroids, respiratory distress (RD), early neonatal sepsis (ENS), persistent hyperechogenicity (PH), skeletal abnormalities, necrotizing enterocolitis (NEC) and mortality. Exclusion criteria were defined as multiple birth (46), malformations (7) and extremely very preterm infants who were not reanimated in the delivery room (3).
Results: Prevalence of PPROM in VLBW infants in our hospital is 33.3%. Results are shown in (*p < 0.01).
Conclusion: PPROM does not increase prevalence of lung disease, which could be explained by the beneficial effect of antenatal steroids treatment and maturation induced by inflammatory cytoquines.
Neonatal sepsis occurs more often in children with PPROM ≥120 hours, although most mothers had been treated with antibiotics. PPROM <120 hours does not increase sepsis;
We observed significant increase of persistent hyperechogenicity in newborns with PPROM ≥120 hours;
Chorioamnionitis were associated with higher rates of cranial ultrasound abnormalities in children with PPROM ≥120 hours;
PPROM related skeletal abnormalities have a very low incidence in VLBW infants, probably due to their small size.
FC-15-002 In vitro fertilization and preterm delivery
K. Wisborg, T.B. Henriksen
Perinatal Epidemiology Research Unit, Dept. of Obst. and Ped., Aarhus University Hospital, Brendstrupgaardsvej, Aarhus, Denmark
Background: In vitro fertilization (IVF) has been associated with an increased risk of preterm delivery. This is vastly explained by a higher number of twin pregnancies. However, also singleton IVF pregnancies have been shown to be at increased risk of preterm delivery compared to spontaneously conceived singleton pregnancies. Furthermore, previous studies have found a trend toward an excess risk of delivery before 32 weeks gestation. This finding is important to explore further as a slight increase in very preterm deliveries would have a dramatic effect upon health costs and childhood health.
Aim: The aim of this study was to assess the risk of preterm delivery (<37 weeks) and very preterm delivery (<32 weeks) in women who conceived by IVF treatment and sub-fertile women (conceived spontaneously after 12 + months of trying to conceive (TTP = time to pregnancy)) in comparison to fertile women (conceived spontaneously after less than 12 months TTP).
Population: This study was based on data from The Aarhus Birth Cohort, Aarhus University Hospital, Denmark and included information about 24,837 primiparous, singleton deliveries during 1989–2004. Information on fertility treatment and TTP was prospectively collected during early second trimester along with information about maternal characteristics, lifestyle factors, and socio-demographic variables. Information about gestational age at delivery, birth weight, and admission to the NICU was obtained from hospital files.
Results: Compared to fertile women, women with IVF pregnancies had a 30% increased risk of preterm delivery (adjusted odd ratio (aOR) 1.3, 95% confidence interval (CI); 1.0–1.7; p = 0.08) and sub-fertile women a 10% increased risk (aOR 1.1, 95% CI; 0.9–1.4; p = 0.30). The risk of delivery before 32 weeks of gestation was (aOR 1.0, 95% CI; 0.4–2.5; p = 1.0) and (aOR 0.7, 95% CI; 1.3–1.7; p = 0.72), respectively.
Conclusion: Compared to couples with normal fertility we found a similar and not significantly increase in the risk of preterm delivery among IVF pregnancies and sub-fertile women. We found no association between infertility and delivery before 32 weeks of gestation. Our results indicate that the increased risk of preterm delivery may not be related to the IVF treatment as such, but could be associated with some underlying reproductive problems related to infertility.
FC-15-003 The structure of perinatal care in greece, in 2004. postnatal transports from thessaly region
A. Gounaris1, E. Apazidou1, T. Christoforaki1, E. Diamanti2, G. Miliagos3, A. Andreou4
1University Neonatal Department, University Hospital of Larissa, Mezourlo, Larissa, Greece; 2University Neonatal Department, Ippokration Hospital, Botsari, Thessaloniki, Greece; 3University Neonatal Department, Papageorgiou Hospital, Thessaloniki Ring Road, Thessaloniki, Greece; 4Neonatal Department, Ippokration Hospital, Botsari, Thessaloniki, Greece
Objective: It is doubtful whether regionalization of Health System in Greece, have taken due notice of every region's perinatal needs. The aim of this study was to investigate whether the abovementioned regions serve their needs in perinatal care, as well as, how postnatal transports outside a region affect neonatal prognosis.
Methods: We have recorded all childbirths in each one of the 17 regions of the Greek Health System within 2004, as well as, all the level II and III existing Neonatal Units in Greece. We have also studied the prognosis of neonates who were transported outside the Thessaly region in 2004.
Results: In 7 out of 17 regions, in which 12,834 live births were recorded, out of a total of 105,444 in Greece overall, there is no level II or III Neonatal Unit and all neonates needed postnatal care, were transported in one of the 20 NICUs existing in Greece. Another 6674 pregnant women living in these 7 regions, born their babies far away their homes, mostly in Athens. From Thessaly region, although incorporating an NICU, 65 neonates were transported, mostly to Thessaloniki. Out of the 65 neonates, 14 suffered surgical problems, 7 cardiological and the other 44 a VLBW and/or respiratory problems. Out of the 25 neonates with a BW < 1500 g, 8 died (32%) while 11 neonates suffered periventricular-intraventricular hemorrhage (65%).
Conclusions: It is obvious that 8 out of 17 regions of the Greek Health System do not cover their perinatal needs. Moreover, postnatal transports to a long distance, under the current circumstances, result in a particular weak prognosis of the transported neonates.
FC-15-004 Campomelic dysplasia syndrome in newborn – case report
E. Gulczynska, E. Lerch, B. Pawlowska, M. Kesiak, A. Grodzicka, J. Gadzinowski
Research Institute of Polish Mother's Memorial Hospital, Lodz, Poland
Campomelic dysplasia syndrome (CD) is a rare genetic disorder with prevalence estimated to range between 0.05–2:10,000 births. The gene responsible for the condition is SOX9 (SRY-related HMG – box gene) and is on 17q24–q25. The inheritance is autosomal dominant. About 75% of reported 46 XY patients exhibit sex reversal with completely female phenotype: the external and internal genitals are female.
Characteristic features are skeletal hypoplasias and anomalies affecting the face, head, scapulae, spine, pelvis and upper and lower limbs. The limbs are short with anterior bowing of the legs, often with pretibial skin dimples. Other extraskeletal anomalies involve the central nervous system, cardiovascular system and genitourinary system. Mental development is also abnormal. It is usually lethal in early infancy.
Diagnosis can be established by ultrasonography as early as 18 weeks of gestation.
CD should be differentiated between osteogenesis imperfecta type I and II, hypophosphasia, thanatophoric dysplasa, mesomelic dysplasia.
Authors describe a male newborn with Campomelic Dysplasia Syndrome who was born in the Polish Mother's Memorial Hospital Research Institute. The baby was born by caesarean section at 36 weeks of GA with birth weight 2300 g, Apgar score 6 at first minute of life. Congenital anomalies were found prenatally at 25 GA and osteogenesis imperfecta was suspected. The newborn had all characteristic features of CD syndrome and diagnosis was confirmed after radiological examinations.
FC-15-005 Classification of neonates in ancient greece
M. Christodoulaki, G. Moshaki, G. Tsoukalas, S. Fiotaki, S. Blazaki, E. Balomenaki, E. Xidaki, I. Tsoukalas, M. Karavitakis
General Hospital of Chania, Mournies, Chania, Greece
Aim: To review the opinion of ancient Greece, regarding the classification of neonates, the determination of the lowest limit of viability and the neonatal mortality.
Method: We examined texts written by Hippocrates, Aristotle, Homer and other authors.
Results: Neonates were classified according to the duration of gestation: a) preterm: Neonates born before the 9th month which were separated to these of 6 months, 7 months and 8 months. b) term: These born at the end of the 9th month of pregnancy and had the best prognosis. c) post-term: These born after the completion of the 9th month.
Causes of preterm birth were the premature rupture of follicle, placental insufficiency, various diseases of mother during gestation, the young or old age of parents and the multiple gestation.
Neonates were also classified to those with normal weight for the age of gestation with good prognosis of survival and those with lower weight for the age of gestation, with worse prognosis.
Causes of birth LBW newborns were considered the weather conditions, the diseases of fetus (congenital infections), the frequent small bleedings during the gestation, small size of uterus, placental insufficiency and others.
Homer considers the 28th week of gestation as the lowest limit of viability, opposing to Hippocrates who determines the 182 days, that is the 26th week of gestation. The limit of 182 days was accepted by most ancient authors-doctors and was also popular at the Byzantine period.
Neonatal mortality can be distinguished to “early” during the first 7 days of life and “late” during the first 40 days of life.
Conclusion: The ancient writers through their empiric knowledge placed the foundation stone in the classification of neonates and created the appropriate base for the consolidation of this opinion today.
FC-15-006 Survival factors of newborns with respiratory failure
M. Markovic1, S. Maglajlic-Djukic2
1Department of Gynecology and Obstetrics, Clinical Centre of Montenegro, Krusevac, Podgorica, Yugoslavia; 2University Clinic for Child Disease, Tirsova, Belgrade, Yugoslavia
Objective: The risk assessment of mortality on the basis of factors related to anamnesis and clinical factors as well as on the severity of the illness represents a model by which it is possible to determine the probability of survival of a newborn who suffers from such illness. To that view we have applied scoring system (Berlin Score System) that allows for identification of newborns who have a similar severity of illness and enables comparison among treatment ways, different conditions and different time. The research goal has been set as to monitor the effects and results of treatments, as well as to determine prognostic importance of used parameters of scoring after the application of Berlin Score System on newborns with respiratory failure.
Methods: The study has encompassed 75 newborns with signs of respiratory distress. The data on pregnancy and on infants have been scored by Berlin Score System with small mortality risk defined at 18 points, moderate risk from 19 to 23 points, high risk from 24–28 and extremely high risk at more than 28 (up to 40) points.
Results: The result of this work has enabled us to make the following conclusions: that birth weight is not a reliable indicator of mortality risk that it does not have a prognostic value and that it does not influence the result of the illness. However, the Apgar score is considerably important parameter of mortality risk of a newborn with respiratory failure.
Conclusions: The reanimation at birth, taking O2 and artificial ventilation as well as the duration of their use do have influence on the effect of therapy and the result i.e. they increase mortality risk, while the acidity weight and discrepancy have a prognostic value, and do increase mortality risk. Berlin Score System be applied with a view to determine probability of a survival of a premature and full-term newborn with respiratory failure.
FC-16-001 Adverse maternal and perinatal outcomes of anemia during pregnancy
N. Ahluwalia, O. Parant, H. Grandjean
INSERM U558, Epidemiology & Public Health, Hospital Paule de Viguier, Toulouse, France
Objective: We examined the association of anemia during pregnancy with several maternal and neonatal outcomes in a retrospective cohort of women.
Methods: Computerized medical information was retrieved for 19,925 women who had received prenatal care in the University hospital (CHU) in Toulouse during the years 1994 to 2000. Complete data on maternal characteristics, and maternal and perinatal outcomes were available on 16,968 women (age: 30 ± 5 years). Anemia on medical charts was defined as hemoglobin (<10 g/dl) which reflects moderate severity of anemia.
Results: The prevalence of moderate anemia (hemoglobin <10 g/dl) was 6.1%. Maternal age (<18 years), lower level of education, multiparity, ethnicity (African or Asian origin), and infections were associated with anemia during pregnancy. Odds ratio for these risk factors ranged between 1.3 for infections to 6.1 for having African descent. After accounting for maternal age, marital situation, parity, smoking, prepregnancy BMI, ethnicity, and infections during pregnancy, anemia remained independent risk factor for several pregnancy outcomes. Specifically, the adjusted odds ratios (95% confidence intervals) for premature birth, caesarean delivery, hemorrhagic delivery, and infections in the newborn in the first week of life were 1.6 (1.4–2.0), 1.5 (1.3–1.8), 1.5 (1.3–1.9), and 1.2 (1.01–1.4), respectively.
Conclusions: These findings suggest that low hemoglobin levels in pregnancy constitute an independent and important risk factor for poor maternal and neonatal outcomes. The prevention and treatment of anemia during pregnancy is important to ensure optimal pregnancy outcome.
FC-16-002 Lipid metabolism is regulated by the liver x receptor in the fetal mouse liver
E.M.E. van Straten, N.C.A. Huijkman, J.F.W. Baller, F. Kuipers, T. Plösch
Department of Pediatrics, University Medical Centre Groningen, Hanzeplein, Groningen, The Netherlands
Objective: The Liver X Receptor (Lxr) is vitally important in regulating cholesterol and fatty acid metabolism in the adult. Lxr is expressed in mouse fetuses from day 11,5 postcoitum on. The role of Lxr in the fetus and the newborn has not been defined so far. Aim of this study was to elucidate the role of Lxr in the regulation of lipid homeostasis in utero.
Methods: Pregnant mice were fed a diet containing the synthetic LXR agonist T0901317 (0.015%) from day 10.5 pc on. Gene expression and lipid levels were measured in fetuses and dams at various time points.
Results: In the developing mouse, hepatic expression of Lxr target genes, e.g. Srebp1c, Fas and Abcg5, is low during gestation and increases after birth. Upon administration of the Lxr agonist T0901317 to the diet of the dam, Lxr target genes are activated in the fetus: Hepatic expression of the canalicular cholesterol transporter Abcg5 is 45 times induced upon Lxr activation. The hepatic expression levels of the Lxr target genes Srebp1c and Fas are increased 2.0- to 5.3-fold and 1.7- to 2.0-fold, respectively, upon Lxr activation. Consequently, triglyceride concentrations in fetal liver and plasma are raised up to 2.7- and 1.5-fold, respectively, after one week of treatment. Cholesterol levels in plasma are higher upon treatment (2-fold), whereas hepatic cholesterol concentrations are unchanged.
Conclusion: Here we present for the first time evidence that Lxr is functionally active in fetal liver when stimulated with the agonist T0901317. Moreover, the pathways controlled by Lxr in adult liver can be influenced by administration of this agonist to the diet of the mother. This may give more insight in the regulation of cholesterol homeostasis and de novo lipogenesis in the fetus and provide a means for experimentally interfering with lipid homeostasis in utero.
Supported by the Dutch Heart Foundation (2004T048).
FC-16-003 Bodyweight in pregnancy: ten years retrospection
R. Devlieger1, S. Hausmans1, J. Verhaeghe1, B. Spitz1, M. Hanssens1, I. Guelinckx2, G. Van Sant2
1Department of Obstetrics and Gynaecology, Leuven, Belgium; 2Department of Preventive Medicine, Leuven, Belgium
Background: Obesity is becoming one of the most important health issues. In pregnancy, overweight mothers are at risk for hypertensive disorders, operative complications, thromboembolic disease, instrumental delivery and neonatal morbidity and mortality. Our goal was describe the evolution of bodyweight and weight gain during pregnancy over the past decade.
Methods: We analysed the electronic registers for preconceptional weight and weight at the time of delivery in all mothers who gave birth in the University Hospital of Leuven (Belgium) from 1993 until 2002. We compared cohorts of consecutive deliveries from 1993 and 2003. We analysed body weight at delivery, preconceptional weight, maternal length, placental and neonatal weight and complications during pregnancy. The mean (±SD) values obtained of the two cohorts were compared using a student's t-test.
Results: We obtained data in 24411 pregnancies. Non-pregnant body weight increased by 2.8 (±2.8) kg in ten years (p < 0.05). Accordingly, weight gain during pregnancy was 1.4 kg (±0.4) higher in 2002 compared to 1993 (p < 0.05). We found no difference in length, weight of the baby and weight of the placenta.
Discussion: Our study shows an important increase in body weight and weight gain during pregnancy that cannot be explained by an increase in maternal length, fetal or placental weight. It is therefore crucial tat obstetricians have an increased awareness for the problem of obesity and pregnancy.
FC-16-004 A comparison of placental pathology between mild and severe preeclampsia
N. Papadogiannakis1, M.T. Nilsson Vinnars1, J. Nasiell2
1Karolinska Institute, Division of Pathology, Huddinge, Stockholm, Sweden; 2Karolinska Institute, Department of Obstetrics, Huddinge, Stockholm, Sweden
Objective: Preeclampsia (PE) is a pregnancy complication associated with significant maternal and neonatal morbidity and, often extensive, placental involvement. There is a general impression that two types of PE may exist, i.e. mild and severe PE, possibly reflecting different pathogenetic mechanisms. In this study we have examined the spectrum of placental findings in mild as compared to severe PE.
Methods: One hundred and fourteen placentas from PE-complicated pregnancies were reviewed retrospectively. The placentas were submitted for routine histopathologic analysis to the Department of Pathology, Huddinge, during the years 2000–2004. Mild (n = 60) and severe (n = 54) PE was defined according to ACOG criteria. Control placentas (n = 114) were recruited from normotensive pregnancies, matched for gestational age.
Results: The majority of placentas from mild as well as severe PE were low for gestational age, but showed high Placental/Fetal ratios. Approximately 80% and 50% of the placentas showed signs of infarction and intervillous thrombosis, respectively. No significant differences were noted between the two PE groups. Severe PE placentas showed significantly (P = 0.0002) higher degree of accelerated maturation in the villi, and slightly higher degree of decidua arteriopathy, however not significant, as compared to mild PE. Approximately 50% of the babies in both groups were small for gestational age (SGA).
Conclusions: The histopathologic profile and the extent of placental lesions were very similar in mild and severe PE, indicating common underlying pathogenetic mechanisms. The notable exception was accelerated maturation in the villi (significantly higher in severe PE). Thus, so-called mild PE is nevertheless associated with considerable placental pathology (low placental weight, infarctions, intervillous thromboses), and high frequency of SGA babies. Our results suggest that all placentas from clinically mild PE should be submitted to careful histopathologic examination.
FC-16-005 Serum adipokines in the first 24 hours of neonatal life
O. Kastanidou2, M. Skouroliakou2, K. Fotiou1, G. Liossis1
1Neonatal unit, Elena Venizelou Perinatal Center, Athens, Greece; 2Harokopio University Dept. of Science of Nutrition and Dietetics, Kallithea, Greece
Objective: To study serum adipokine levels of neonates in relation to anthropometric parameters (birth-weight, length, head circumference and BMI), placental weight and gender and also assess the net real fluctuations of these molecules between birth and 24 h later.
Methods: Twenty-nine healthy term newborns were included in this study. Blood samples were collected from the newborns at time of birth from venous cord blood and 24 h later from peripheral venous. Maternal blood samples were collected half an hour before delivery. The analysis of all adipokines was performed by Cytarometric Bead array (Luminex Multiplexed assays, Linco Biosource kits).
Results: Adiponectin cord levels showed significant positive correlation with insulin and PAI-1 levels at birth and 24 hours later (r = 0.506*, r = 0.494* and r = 0.651**, r = 0.706** respectively) and with birth body length (r = 0.647*). Adiponectin levels between birth and 24 h after didn't differentiate (r = 0.739**). Adiponectin levels were much higher compared with maternal (47.952 ± 6.18 mg/ml vs. 17.34 ± 1.78) (p < 0.000). Leptin measurements showed a high significant correlation with BMI (r = 0.574**), TNF-α (r = 0.394*) and placental weight (r = 0.532**). Leptin levels showed significant decline from time of birth to 24 hours later (8461 ± 862 pg/ml vs. 2995 ± 1487) (p < 0.02). Cord TNF-a was found to be positively significant correlated with IL-6 (r = 0.581**), insulin (r = 0.472*), MCP- (r = 0.845**) at birth and their levels 24 h later. Sexual dimorphism was observed with males having higher levels (p < 0.049). TNF-α was significantly increased from birth to 24 h later (P < 0.017). IL-6 was also positively correlated with MCP-1 (r = 0.580**). Males had higher levels than females (p < 0.01).
Conclusions: Placenta and adipose tissue play a fundamental role in neonatal growth and development. By producing and secreting an array of molecules, which interact in a complicated network.
FC-16-006 Glycemic profile characteristics during active labor and delivery in non-diabetic subjects
R. Chen, Y. Yogev, A. Ben-Haroush, M. Hod
Department of Obstetrics and Gynecology, Rabin Medical Center, Petah Tiqwa, Israel
Objective: As no information exists regarding the physiology of glycemic profile during labor, we aimed to assess glycemic profile during labor and early post-partum period in non diabetic subjects.
Method: 12 non-diabetic gravid subjects were evaluated using Continuous Glucose Monitoring System-CGMS. CGMS measures glucose levels every 5 minutes for a total of 288 measurements daily. Evaluation initiated during latent phase until 24-h post partum. Eligibility was limited to healthy non diabetic women with singleton pregnancies, >37 weeks, who did not receive fluids containing glucose during labor and who had uncomplicated vaginal delivery.
Results: 1) Mean maternal age was 27.3 ± 3.1 years, gestational age at delivery was 39.2 ± 1.1 weeks, BMI of 24.4 ± 2.6. 2) Overall, 5470 glucose determinations were obtained during the study period, the mean time of evaluation was 38 ± 11 hours and the mean blood glucose determinations for each subjects was 452 ± 64. 3) No significant difference was found in mean blood glucose (MBG) during latent and active phase (82 ± 19 and 79 ± 21 mg/dl, respectively p = 0.23). 4) During second stage of labor significant lower MBG was recorded (71 ± 14 mg/dl) p = 0.001, and 3/12 of the women had hypoglycemic event (blood glucose <40 mg/dl for more than 10 consecutive minutes) with no alteration in fetal heart rate. 5) MBG during the 24-h postprandial was significantly higher in comparison to labor and delivery (89 ± 17 mg/dl, p = 0.02).
Conclusions: During normal labor there is a gradual physiological decrease in glucose levels which peaks during the second stage.
FC-17-001 Glycemic control and pregnancy in type 1 diabetes: multiple daily injections versus continuous subcutaneous insulin infusion (CSII)
R. Chen, A. Brenner, A. Ben-Haroush, N. Melamed, Y. Yogev, M. Hod
Department of Obstetrics and Gynecology, Rabin Medical Center, Petah Tiqwa, Israel
Objective: To compare glycemic control and pregnancy outcome in type 1 diabetic pregnant patients treated by two modes of treatment: multiple daily injections of insulin (MDI) and continuous subcutaneous insulin infusions (CSII).
Methods: Using a retrospective matched control study, patients treated by MDI were compared to patients treated by CSII in a ratio of 2:1. Pregnancy outcome was evaluated by mode of delivery, birth trauma, shoulder dystocia, birthweight, congenital anomalies and short-term neonatal outcome.
Results: Ninety pregnancies of patients with pregestational diabetes mellitus were analyzed: 30 used CSII and 60 used MDI. In all patients CSII started before pregnancy. Most diabetic control parameters tested were similar ( ). Higher rate of diabetic ketoacidosis was found in the CSII group, 13% vs. 2% (p = 0.044). Most pregnancy outcome parameters were similar (). The rate of neonatal hypoglycemia was significantly higher in the CSII group.
Conclusions: Glycemic control and pregnancy outcome in pregnant women with type 1 diabetes mellitus appear to be similar using either CSII or MDI. CSII may be associated with higher rate of neonatal hypoglycemic events.
FC-17-002 Diurnal glycemic profile characterization in non-diabetic non-obese subjects during the first trimester
Y. Yogev, R. Chen, A. Ben-Haroush, M. Hod
Department of Obstetrics and Gynecology, Rabin Medical Center, Petah Tiqwa, Israel
Objective: In diabetic pregnancy, the association between hyperglycemia during the first trimester with spontaneous abortion and fetal malformation is well established; however, scarcity of data exists concerning the ambulatory normal glycemic profile in non diabetic subjects during this time period which can be applicable for the level of desired glycemic control.
Method: Daily glycemic profile was evaluated during the 1st trimester in 42 non-diabetic non obese gravid patients using Continuous Glucose Monitoring System-CGMS. CGMS measures glucose levels every 5 minutes for 72 consecutive hours for a total of 288 measurements daily. All women were asked to refrain from any lifestyle modification or dietary restriction.
Results: 1) Overall, during the study period, an average of 774 ± 41 glucose measurements was recorded for each woman. 2) Gestational age was 8.1 ± 2.4 weeks and mean BMI was 24.1 ± 1.4 Kg/m2. 3) For the total 126 days (42 women × 3 days) of continuous monitoring glucose characteristics revealed a daily mean glucose level of 79.3 ± 7 mg/dl, mean fasting glucose of 74.5 ± 11 mg/dl, and a mean preprandial glucose level of 77.6 ± 9 mg/dl. 4) Further analysis was performed in relation to meals. The 1-h post prandial glucose peak value was 108.7 ± 16.9 mg/dl and the time interval required to reach this peak value was 65.4 ± 28 min. 5) During study period, no hypoglycemic events (glucose < 40 mg/dl) were identified.
Conclusions: Our data characterize the definition of normoglycemia in early pregnancy and can be utilized to identify the threshold for the degree of glucose abnormality during diabetic pregnancy in the first trimester.
FC-17-003 The incidence of obesity and insulin resistance in offspring of diabetic mothers
K. Wroblewska-Seniuk1, E. Wender-Ozegowska2, J. Szczapa1
1Department of Neonatal Infectious Diseases, Chair of Neonatology, Poznan, Poland; 2Chair of Obstetrics and Gynecology, Poznan, Poland
Objective: The aim of the study was to assess the incidence of obesity and insulin resistance (IR) in children born to mothers with gestational (GDM) and pregestational (PGDM) diabetes.
Methods: A total of 43 offspring of mothers with PGDM and 34 of mothers with GDM were examined at 4.5–10 years of age. The control group consisted of 108 children of healthy mothers. In all children body measurements were taken to calculate BMI and BMI z-score. Obesity was diagnosed if BMI z-score exceeded +1.6 and overweight if BMI z-score was between +1.1 and +1.6. In all children of the study groups and in 29 children of the control group, plasma glucose and insulin concentrations were determined in fasting condition. The IR index was calculated using HOMA method (IR >3.0).
Results: Obesity was diagnosed in 9 (26.5%) children of mothers with GDM, 5 (11.3%) children of mothers with PGDM and 17 (15.7%) children of control group (NS) and overweight respectively in 3 (8.8%), 3 (7.0%) and 8 (7.4%) children (NS). No significant differences between groups were found with respect to fasting serum glucose concentration. On the contrary the insulin secretion was statistically higher in children born to mothers with GDM compared to control group (GDM – 7.53 μIU/ml, NGDM – 5.21 μIU/ml, control group – 4.75 μIU/ml). IR determined by HOMA method was observed in 3 (8.8%) children born to mothers with GDM, in 1/29 (3.4%) child of the control group and in no children born to mothers with PGDM (NS). Median and range of HOMA index were respectively 1.11 (0.37–15.12) – GDM group, 0.94 (0.2–2.79) – PGDM group and 0.75 (0.22–4.29) – control group (GDM vs. control p < 0.05).
Conclusions: Children of mothers with GDM seem to be the group of higher risk of obesity and insulin resistance in pre-school and early school age. The metabolic disturbances observed in these children suggest the necessity of early prophylaxis and treatment.
FC-17-004 The effects of the pro12ala polymorphism of the peroxisome proliferator activated receptor-g2 gene on glucose/insulin metabolism interact with prenat
S.R. de Rooij1, R.C. Painter1, D.I.W. Phillips2, C. Osmond2, M.W.T. Tanck1, R.P.J. Michels3, J.C. Defesche4, P.M.M. Bossuyt1, O.P. Bleker5, T.J. Roseboom1
1Department of Clinical Epidemiology and Biostatistics, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; 2MRC Epidemiology Resource Centre at the University of Southampton, Southampton, UK; 3Department of Internal Medicine, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; 4Department of Vascular Medicine, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; 5Department of Obstetrics and Gynaecology, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands
Objective: An adverse fetal environment may permanently modify the effects of specific genes on glucose tolerance, insulin secretion and insulin sensitivity. In the present study, we assessed a possible interaction of the PPAR-γ2 Pro12Ala polymorphism with prenatal exposure to famine on glucose and insulin metabolism.
Methods: We measured plasma glucose and insulin concentrations after an oral glucose tolerance test and determined the PPAR-γ2 genotype among 675 term singletons born around the time of the 1944–1945 Dutch famine.
Results: A significant interaction effect between exposure to famine during mid gestation and the PPAR-γ2 Pro12Ala polymorphism was found on the prevalence of impaired glucose tolerance and type 2 diabetes. The Ala allele of the PPAR-γ2 gene was associated with a higher prevalence of impaired glucose tolerance and type 2 diabetes, but only in participants who had been prenatally exposed to famine during mid gestation. Similar interactions were found for area under the curve for insulin and insulin increment ratio, which were lower for Ala-carriers exposed to famine during mid gestation.
Conclusions: The effects of the PPAR-γ2 Pro12Ala polymorphism on glucose and insulin metabolism may be modified by prenatal exposure to famine during mid gestation. This is possibly due to a deficit in insulin secretion.
FC-17-005 SSRI exposure in utero and pregnancy outcome
N. Lund1, L.H. Pedersen2, T.B. Henriksen3
1Perinatal Epidemiology Reseach Unit, Aarhus University Hospital, Skejby, Aarhus N, Denmark; 2Dept. of Epidemiology & Centre for Clinical Pharmacology, University of Aarhus, Aarhus C, Denmark; 3Department of Paediatrics, Aarhus University Hospital, Skejby, Aarhus N, Denmark
Objective: To investigate the effect of in utero exposure to selective serotonin reuptake inhibitors (SSRIs) on birth weight (BW), gestational duration, head circumference (HC) and admission to neonatal intensive care unit (NICU).
Methods: From 1989–2004 the cohort of pregnant women intending to give birth at Aarhus University Hospital was invited to complete a questionnaire on lifestyle, height and weight, and obstetric and medical history, including medication. At birth the tending midwife completed a structured coding sheet on the course of delivery and newborn characteristics. All analyses were restricted to singleton pregnancies and adjusted for potential confounders (parity, maternal age, smoking, alcohol intake, BMI and maternal medical disease and psychiatric history) by multivariate analyses. Analyses on BW and HC were also adjusted for gestational age by linear regression. Adjusted analyses on preterm birth (<37 completed weeks) and admission to NICU were carried out by logistic regression.
Results: The cohort comprised 53,856 pregnancies; 265 were treated with SSRIs during pregnancy. For term infants exposed to SSRIs mean BW was 33 gram (95% CI −101; 36) lower than for unexposed. Mean HC was 0.24 cm smaller (95% CI −0.46; −0.02). The odds ratio for preterm birth was 1.8 (95% CI 1.1; 2.8) and for admission to NICU 2.3 (95% CI 1.6; 3.2) for SSRI-exposed compared to non-exposed.
Conclusions: Exposure to SSRIs during pregnancy increased the risk of preterm birth. The HC adjusted for gestational age was smaller in infants of women treated with SSRIs and they were more than twice as likely to be admitted to the NICU. The effect could be due to the medication or depression per se.
FC-17-006 Association between mother skin phototype and vitamin D status of mother–newborn pairs
Z. Hatzistamatiou3, J. Kaleyias1, A. Papadopoulou3, E. Floropoulou1, A. Koutrouba1, Ch. Costalos1, A. Antsaklis2, P. Nikolaidou3
1NICU, State Maternity Hospital of Athens “Alexandra”, Lourou, Athens, Greece; 21st Department of Obstetrics and Gynecology, University of Athens “Alexandra” Hospital, Lourou, Athens, Greece; 33rd Department of Pediatrics, University of Athens, “Attiko” Hospital, Haidari, Athens, Greece
Introduction: A high concentration of melanin in the skin could limit the synthesis of vitamin D shielding the skin from UV radiation.
Aim: To investigate the correlation of the mother skin phototype with the levels of vitamin D of mother-newborn pairs.
Material and Methods: 123 mother-newborn pairs were included in the study during one-year period. The identification of the mother's phototype followed three-type classification (I: blond, II: brown, III: black) derived from the classification proposed by Fitzpatrick. Blood samples were obtained from mothers 30 minutes before delivery and umbilical cord blood was collected immediately after clamping. 25 (OH) D was performed by chemiluminescence immunoassay.
Results: Most of the participants (67.5%) were classified in phototype II, 13.8% in I and 18.7% in III. Mothers with darker phototypes had lower serum 25 (OH) D [16.5 (10.6–21.5) ng/ml and 13.6 (9.1–18.5) ng/ml in phototype II and III, respectively] than those with fair phototype [18.6 (16–26.1) ng/ml] (I vs. III, p = 0.023). The overall incidence of hypovitaminosis D (<10 ng/ml) was 19.5%. No mother classified in phototype I had hypovitaminosis D, while 20% and 30% of mothers classified in II and III respectively had hypovitaminosis D (p = 0.04 I vs. II, p = 0.012 I vs. III, p = ns II vs. III). The levels of 25 (OH) D in the fetus of mothers with phototype I were significantly higher [31.4 (21–37.5) ng/ml] in comparison with those of mothers with phototypes II 19.37 (13.8–28.5) ng/ml (p = 0.025, I vs. II) and phototype III 17.9 (10–30) ng/ml (p = 0.003, I vs. III). The overall incidence of hypovitaminosis D in the neonates was 8.1%. None neonate of mother with phototype I presented hypovitaminosis; 7% of the neonates of mothers with phototype II and 17% of phototype III had hypovitaminosis.
Conclusion: Mothers with dark phototype and their neonates had lower levels of vitamin D in comparison with mothers with fair phototypes and their neonates.
FC-18-001 Effect of milking of umbilical cord on postpartum adaptation and anemia of prematurity in infants weighing 1000 to 1499 G
S. Hosono, T. Kitamura, H. Fujita, H. Miyabayashi, M. Shimada, M. Minato, T. Okada, H. Mugishima, S. Takahashi, K. Haada
Nihon University School of Medicine, Itabashi Hospital, Itabashi, Tokyo, Japan
Objective: The purpose of present study is to investigate the clinical effects of milking of umbilical cord in preterm infants.
Methods: A total of 37 infants were prospectively randomized and 33 infants weighting 1000 to 1499 g were eligible for the study between 2001 and 2002. A length of approximately 20 cm of cord was vigorously milked towards the umbilicus two to three times before clamping the cord.
Results: Gestational weeks and birth weight were 29.5 ± 1.3 weeks and 1225 ± 149 g, respectively in 33 infants. Seventeen were in the milking group and other 16 infants were in non-milking group. There were no statistically differences in birth weight and gestational week. There were statistically a significant increase in initial hemoglobin value (17.9 ± 1.8 vs. 14.9 ± 1.0 g/dl: p < 0.01) and a significant decrease in frequency of administration of erythropoietin (13.1 ± 5.2 vs. 17.0 ± 5.5/hospital stay/infant: p = 0.02) compared with the non-milking group. No infants received red cell transfusions in both groups, on the other hand in the milking group one infant did not need erythropoietin therapy. Hemoglobin value at starting erythropoietin therapy, hemoglobin value at discharge, or duration of hospital stay were similar. Although the milking group exhibited a decrease in the frequency of use of volume expander (p = 0.04), and/or dopamine (p = 0.04), blood pressure was higher compared with non-milking group (p < 0.05) during the first 6 hours and after 48 to 96 hours of life. There were no infants with intraventricular hemorrhage in both groups. Polycythemia was not observed in both groups.
Conclusions: In preterm infants weighing 1000 to 1499 g, milking of the umbilical cord is feasible and safe. It reduces the use of volume expander, inotropic agents, and erythropoietin. It might contribute the stabilization of blood pressure. It is possible for critical ill preterm infants who need aggressive resuscitations to perform the procedure compared with late clamping.
FC-18-002 Erythrocyte transfusion compared with recombinant human erythoropoietin in premature infants
S. Bulatovic-Stajkovic
Institute for Neonatology, Belgrade, Yugoslavia
Objective: Anemia of prematurity is characterized by low reticulocyte counts and inadequate erythropoietin production; of iatrogenic blood loss is large, anemia can reduce the amount of available oxygen till the critical value, therefore premature infants receive frequent erythrocyte transfusions. It is investigated if an early use of recombinant human erythropoietin (rHuEPO) reduces number and volume of erythrocytes transfusions in premature infants.
Methods: This study comprises 65 premature infants with gestation less or equal 34 weeks, birth weight less or equal 2000 g and capillary hematocrit value 45–50% on day 5; 35 of them received rHuEPO, but as five infants were excluded from the study (for the reason of exsanguinous transfusion), the total number was 30.
EPO group received 250 IU/kg s.c. rHuEPO, three times of week from day 5 to day 42 (for a total of 16 doses). Control group (30 infants) did not receive rHuEPO. Both groups received iron: 6 mg/kg/day in EPO and 4 mg/kg/day in control, from day 8 onward. The criteria for transfusions were not strict.
Results: In the EPO group 30% of infants received transfusions, and in the control group 63.3% (p < 0.01). The volume of transfused blood in the EPO group was also significantly lower (per single transfusion/12.5: 14.1 ml/kg, p < 0.01 and per transfusioned patient 18.67: 31.79 ml, p < 0.001). No toxic effects were observed in the EPO group.
Conclusions: The use of rHuEPO reduced the number and the volume of erythrocyte transfusions in premature infants.
FC-18-003 Antenatal magnesium sulfate (MgSO4) exposure and incidence of patent ductus arteriosus (PDA) in extremely low birth weight infants (ELBW)
T. del Moral, V.H. Gonzalez-Quintero, N. Claure, S. Vanburskit, E. Bancalari
University of Miami, Miami, USA
Objective: Antenatal exposure to MgSO4 either for tocolysis or seizure prophylaxis can have significant clinical effects in ELBW infants. Among these, it may adversely influence the closure of the ductus arteriosus.
The purpose of this study was to explore the relationship between antenatal exposure to MgSO4 and the incidence of PDA in ELBW infants.
Study Design: A total of 952 neonates with birth weight between 500–1000 g born at our institution between January 1996 and December 2003, and who survived more than 3 days were followed until death or discharge from the hospital. A research nurse prospectively collected Perinatal and hospital course data. The incidence of PDA was compared in infants exposed to MgSO4 with those not exposed, and between infants exposed to different maternal doses of MgSO4. Indications for the administration of MgSO4 to the mother were preeclampsia and tocolysis.
Results: The incidence of PDA was significantly higher in the group of infants exposed to MgSO4 compared to non exposed (67% vs. 60%, p = 0.0178). When stratified by gestational age the differences were significant only in the group of infants with gestational age >26 weeks (58% vs. 49%, p = 0.0399). There was no relationship between prenatal exposure to MgSO4 and the duration of PDA. Logistic regression analysis to adjust for co variables confirmed the increased risk of PDA in infants exposed to MgSO4 (OR 1.60, CI 1.18–2.16).
Furthermore, the risk of PDA increased with higher doses of MgSO4 exposure (OR 1.24 CI 1.09–1.42 per 50 g of MgSO4).
Conclusion: In ELBW, infants antenatal exposure to MgSO4 is associate with a higher risk for PDA and this effect is dose related and more significant in the more mature infants (>26 weeks).
FC-18-004 Clinical presentation and outcome of neonatal renal vein thrombosis
J. Kucera1, J. Langer2, L. Veprekova3
1Institute for the Care of Mother and Child, Prague, Czech Republic; 2Children's Hospital of Charles University, Prague, Czech Republic; 3Central Haematology Laboratory, Charles University, Prague, Czech Republic
Objective: Assessment of incidence, risk factors, clinical course and long-term outcome of neonatal renal vein thrombosis (RVT).
Methods: Retrospective case analysis in tertiary centre for perinatal medicine (13 year period).
Results: We have diagnosed RVT in 9 newborns (incidence 28:100,000) in the period 1991–2004. Mean birth weight was 1604 g (620–3500), mean gestational age was 31 weeks (25–40) and sex ratio M:F was 8:1. Diagnosis was based on ultrasound scan performed after clinical and laboratory findings consistent with RVT appeared. Mean age of first symptoms was 18 days (1–58). Hematuria was present in all 9 patients whilst transient hypertension in 5 of them. Abdominal mass corresponding to enlarged kidney was palpable in 7 out of 9 patients. Thrombopenia accompanied all cases of RVT in our group. Clinical course was to same extent similar to neonatal sepsis. Right renal vein was affected in 5 and left renal vein in 4 patients. Thrombosis of inferior vena cava (IVC) was found in addition in two cases. Central venous line or umbilical venous catheter was used before RVT appeared in 5 neonates. Congenital thrombophilia was diagnosed in 4 patients. In one case RVT appeared after abdominal surgery. All patients were treated by anticoagulants. We did not observe severe acute renal failure as we fortunately did not have bilateral RVT in our group. Most of our patents were followed by pediatric hematologist and pediatric nephrologist. In al affected kidneys we observed reduction in size. Kidney function was reduced down to 0–33%. Two patients developed late hypertension which led to nephrectomy in one of them. In both patients with IVC thrombosis we could not demonstrate IVC recanalisation and surprisingly we did not see any specific symptoms so far.
Conclusion: RVT is a rare condition with high risk of long term renal consequences. Nearly one half of the patients was found to have hereditary prothrombotic anomaly.
FC-18-005 Minor neurological dysfunctions at age 5 years after very preterm birth: results of the epipage study
C. Arnaud1, L. Daubisse-Marliac1, V. Pierrat2, M. White-Koning1, C. Alberge3, H. Grandjean1
1INSERM U558/University P Sabatier, Faculte de Medecine, Toulouse, France; 2University Hospital, Service de Medecine Neonatale, Hopital Jeanne de F, Lille, France; 3University Hospital, Hopital des enfants, Toulouse, France
Objective: Minor neurological sequellae of very preterm birth such as impaired fine motor function, balance or coordination are rarely examined. Nevertheless, these minor neurological dysfunctions (MND) predict behavioural problems and learning difficulties at school age. We report the early predictive factors of MND at age 5 in a cohort of very preterm children.
Methods: EPIPAGE is a population-based cohort study including all infants born 22–32 weeks of gestation in nine French regions in 1997 and two control groups (full-term infants and children born at 33–34). MND were assessed using a simplified version of the Touwen evaluation. Two clinical subgroups were identified: simple and complex forms, with different consequences and associated factors. The type of impairment and their effect on behaviour and learning were described. Risk factors and early predictive factors were examined.
Results: We included 1221 very preterm children, 170 preterm (33–34) and 281 full-term children, all 5 years of age and without major neurodisabilities. Very preterm children were more likely than controls to have MND: 41% had a simple and 3% a complex MND vs. 28% (both simple and complex forms) in the 33–34 group and 22% for full-term controls. The children with MND have more behavioural problems and difficulties at school. Among very preterm children, major neonatal cerebral lesions, broncho-pulmonary dysplasia, postnatal corticosteroid exposure were associated with MND.
Conclusion: Very preterm children have a higher risk of MND at 5 years of age compared to term born children or less severe preterm children. Early screening is important in order to set up adequate care.
FC-18-006 Perinatal and neonatal complications associated with adverse neurodevelopmental outcome in extremely low birth weight infants
H. Slavikova, Z. Stranak, J. Melichar, P. Velebil, J. Feyereisl
Institute for the Care of Mother and Child, Prague, Czech Republic
Objectives: Increasing survival of ELBW infants raises a concern regarding the risks of adverse long-term outcome. The aim of the study was to assess the association of neurodevelopmental outcome with serious perinatal and neonatal complications.
Design: Prospective cohort study in tertiary perinatal centre.
Methods: One hundred and eighty-seven ELBW patients were analyzed (median BW 790 g, median GA 26.5 wks) and followed up at 2 years of corrected age using Bayley Scales of Infant Development II and neurosensory examination. Selected maternal and infant variables were abstracted from the medical records. Neonatal morbidity, the presense of visual and hearing impairment and cerebral palsy were assessed.
Results: Survival rate at discharge was 76%. Follow up was collected in 114 infants (86%). PVH-IVH ≥ III grade complicated with posthaemorrhagic hydrocephalus was found in 5.3% patients, PVL in 9.1% cases and ROP ≥ III grade in 23.5% infants up to discharge. Examination at 2 corrected age confirmed serious neurosensory impairment in 24% infants, moderate in 37% patients and mild impairment in 21%. Only 18% patients were classified as normal. Comparison of patients with serious neurosensoric imparment (SNI group) and normal neurodevelopment (NND group) has found statisticaly significant differences in: gestational age (25.3 wks SNI vs. 27.4 wks NND, p < 0.01), incidence of RDS (58% SNI vs. 42% NND, p < 0.05), frequency of patent ductus arteriosus (87% SNI vs. 13% NND, p < 0.0001), late-onset sepsis (74% SNI vs. 26% NND, p < 0.01) and retinopathy ≥ III grade (75% SNI vs. 25% NND).
Conclusions: The serious neurosensoric impairment is strongly associated not only with severe life threatening neurologic complications but also with less hazardous non-neurological diseases. Our results suggest that early treatment of patent ductus arteriosus and prevention of late onset sepsis are essential in improving neonatal outcome.
Supported by grant IGA MH CR NR/7841-3.
IS-04-001 Fetal programming: its relevance to postnatal nutrition
W. Hay
Neonatal Clinical Research Center and Perinatal Research Center, University of Colorado Health Sciences Center, Aurora, Colorado, USA
“Programming” has been defined by Lucas as a stimulus or insult that, when applied at a critical or sensitive stage in development, may result in a lifelong or lasting effect on the structure or function of the organism. For example: under nutrition in the fetus at critical stages permanently affects brain size, brain cell number, behavior, learning and memory; protein undernourished rat fetuses have long-term reductions in pancreatic cells and insulin secretion; overfeeding rat pups during suckling leads to adult hypercholesterolemia and hyperinsulinemia; high carbohydrate diet following weaning further increases enzymes that produce cholesterol and fat; overfeeding infants of many species leads to adult obesity; female offspring of diabetic mothers become diabetic in their own pregnancies, and so on into further generations.
Consequences of insufficient and then excess nutrition of preterm infants: Preterm infants often are born already growth-restricted and nearly all become growth restricted by term gestational age, despite efforts to provide sufficient nutrition. Furthermore, preterm infants that survive the neonatal period have a greater incidence of serious life-long complications including mental, visual and aural impairment, and cerebral palsy, and there now is compelling evidence that growth failure is a risk factor for the development of obesity, type 2 diabetes, and cardiovascular disease as adults (the “metabolic syndrome”). Efforts to improve nutrition of these infants have generally involved over feeding to induce catch-up growth. Often, however, such over fed infants tend to develop a higher incidence of the metabolic syndrome in later life.
Recommended approach to nutrition of the preterm infant: Postnatal nutrition should be started at birth, emphasizing intravenous and enteral amino acids and protein (3–4 g/kg/day between 24 and 32 weeks gestational age. Over nutrition of energy that induces a positive crossing of weight and weight-for-length centiles is not necessary. There may some advantage to ensuring intakes of docosahexaenoic acid, as preterm infants who are fed closer to normal in utero rates of this PUFA have higher visual acuity and improved Bayley mental development and MacArthur Communicative inventories. Improving early postnatal nutrition of preterm infants may help continue normal in utero growth rates and body compositions, thereby preventing postnatal growth restriction perceived need to produce catch up growth.
IS-04-003 Management of iugr fetus
G.P. Mandruzzato
Istituto per l'Infanzia, Burlo Garofolo, IRCCS, Trieste, Italy
Intrauterine growth restriction (IUGR) is defined as a fetus that fails to reach his potential growth. The causes of the reduced growth are many (maternal undernutrition, viral or parasitical infections, chromosome aberrations, fetal malformations, reduced maternal–fetal supply) but in about 60% of the cases IUGR is not a pathological condition but just indicates a so called “genetical small fetus”. The outcome can be adversely affected particularly if the cause of the IUGR is the reduction of nutrients and oxygen as well supply from the mother. The principal cause of reduced supply is represented by obliterative vasculopathy of the placenta that induces chronic fetal hypoxaemia (CFH). In order to improve the clinical outcome it is first necessary to recognize timely the restricted growth, what can be obtained mainly by ultrasound biometry. The target should be not to assess the estimated fetal weight but to detect the deviation from the expected curve of growth, being any single fetus the control of himself. After recognition of IUGR the second fundamental step (after excluding fetal abnormalities) should be the assessment of the level of the fetal oxygenation in order to identify the fetuses affected by CFH (65% of the cases) from those that are unaffected. The method of choice is represented by Doppler investigation on umbilical arteries that indicates the reduction of blood supply while Doppler assessment on fetal vessels indicates the adaptation or the decompensation of the fetus.
By monitoring fetal oxygenation the characteristics of the clinical management can be optimized and the outcome improved.
IS-04-008 Treating the patent ductus arteriosus in the preterm infant – just how much can we achieve?
P.W. Fowlie1, B. Van Overmeire2
1Neonatal Unit, Ninewells Hospital and Medical School, Dundee, Scotland; 2Department of Neonatology, Antwerp University Hospital, Belgium
A patent ductus arteriosus (PDA) is essential for fetal well-being. In term infants this vessel closes spontaneously within the first 48 hours. However, in infants born preterm the ductus arteriosus may remain patent for much longer and is associated with clinical morbidity – an increased risk of death, chronic lung disease and intraventricular haemorrhage – as well as other adverse health service outcomes – prolonged ventilation, longer lengths of stay and requirement for surgery. It is not unreasonable therefore to explore whether certain interventions might close the PDA and thereby improve outcomes.
A number of strategies for closing the PDA in preterm infants have been proposed – prophylaxis of high risk infants with cyclooxygenase inhibitors (indometacin/ibuprofen), treatment of asymptomatic or symptomatic infants using medical interventions (fluid restriction, diuretic therapy, cyclooxygenase inhibitors) and/or surgery. Mortality data relating to certain treatment strategies are reproduced below from the Cochrane Library Citation[1]. Data relating to other outcomes including neurodevelopmental outcome and “adverse” outcomes will also be presented. See .
The chance of survival is not improved by any of these interventions. There are very few data available that examine longer term neurological outcome. Health professionals and parents are therefore left to weigh the benefits of improved outcomes that are arguably less important against the potential for a degree of “harm” that might be associated with these interventions.
IS-04-010 Recent perinatal data in the czech republic
P. Velebil
WHO Collaborating Center, Institute for the Care of Mother and Child, Prague, Czech Republic
Objective: The purpose of the study is to document the advances as well as remaining problems of the system of perinatal care using available national perinatal data.
Methods: The nationwide perinatal data collected through the national perinatal surveillance system were used to evaluate the trends in the number of deliveries, multiple gestations, modes of deliveries, including caesarean sections, perinatal mortality and severe maternal morbidity. The results of perinatal care were confronted with changes of demographic conditions in the Czech Republic.
Results: The total perinatal mortality has reached a very low level (below 5/1000). The number of multiple deliveries and the frequency of caesarean sections has been increasing during recent years.
Conclusions: Perinatal mortality in the Czech Republic is one of the lowest in the developed world while the number of low birth-weight newborns is increasing and the population of pregnant women is getting older. The number of multiple gestations is increasing and the related perinatal mortality is 2–3 times higher than among singletons. Despite these negative factors the improved level of perinatal care compensates for their influence and preserves excellent perinatal results.
IS-04-013 Perinatology in russia
A. Mikhailov
Medical Faculty of St. Petersburg State University, Maternity Clinic No 11, Lesnozavodskaya 4, St. Petersburg, Russia
During the last years the birth rate in Russia increased after a deep loss in 90ths. In 2003 officially registered pregnancies resulted in term delivery in 92.1%, preterm delivery in 3.5% (all together 1 427 thousand births); late abortions between 22–27 completed weeks of pregnancy in 1%, and spontaneous abortions before 22 weeks in 3.4%. Calculated from 28 week of gestation and 1000 gr. perinatal mortality rate (PM) in Russian Federation decreased from 17.6% in 1991 to 10.6% in 2004. The same time stillbirth and early neonatal death rates decreased from 8.7 and 8.9 to 5.8 and 4.9 promiles correspondently. A huge investments in and improvements of neonatal intensive care probably played a main role in the PM positive dynamics. This supported by calculations of unofficial “PM” from 500 grams that in 1999–2003 that for example in St. Petersburg decreased more then 89% in compare with decreasing on 66% in official PM from 1000 grams. During the same period a negative tendency was registered – relative increasing of term pregnancy in PM structure that reached 46%. The main causes of PM are asphyxia, respiratory distress syndrome, infections, inborn defects and birth trauma. The cesarean section rate slightly and continuously increased and in 2003 reached the level of 15.9%. From the other hand the rate of vaginal operative delivery was unchanged for a long time on very low level – forceps and vacuum-extraction were used in 0.22% and 0.04% correspondently that probably explain the relatively high PM and morbidity connected with asphyxia and birth trauma in term pregnancy.
Implementation of “baby-friendly” principles and continues caregiver's teams training based on internationally approved medical care protocols could be a way for improvement of Perinatal care.
IS-04-014 A collaborative initiative to improve maternal and newborn health in south eastern european countries
M. Merialdi1, O.D. Saugstad2, A. Bacci3, M. Haralanova4
1Department of Reproductive Health and Research, World Health Organization, Geneva, Switzerland; 2Department of Pediatric Research, Rikshospitalet University Hospital, University of Oslo, Oslo, Norway; 3Making Pregnancy Safer, WHO Regional Office for Europe, Copenhagen, Denmark; 4SEE Health Network, Strategic Country Support Programme, Division of Country Support, WHO Regional Office for Europe, Copenhagen, Denmark
Each year 4 million newborns and more than 500,000 women die for causes related to pregnancy and childbirth. 99% of those deaths occur in low income countries and therefore this represents one of the largest health inequities of our time.
In Europe levels of maternal and neonatal mortality differ substantially across countries with different socio economic and health care conditions. Maternal mortality ratio ranges from 210 deaths per 100,000 live births in Kazakhstan to 5–4/100,000 live births in western European countries. Neonatal mortality rate ranges from 27 and 32 deaths per 1000 live births in Kazakhstan and in Uzbekistan, to 3/1000 in Italy and Slovenia. Significant variations are observed also within South Eastern European (SEE) countries with maternal mortality ratios and neonatal mortality varying from 36/100,000 and 16/1000 respectively in the Republic of Moldova to 10/100,000 and 5/1000 in Croatia.
Reduction in maternal mortality has been set as a priority among the UN Millennium Development Goals 2015 as well as the reduction in under 5 child mortality rate, of which newborn mortality represents a very large proportion (38%).
WHO, Norway and the SEE countries have endorsed a new initiative aimed at strengthening the health systems in SEE countries to improve maternal and neonatal health.
During the inception phase the project will:
Establish a working group of experts.
Prepare country profiles on the situation of maternal and newborn health in the SEE region.
Agree on a regional project proposal.
Prepare a draft Decision for implementation to be submitted for signing during the 13th Meeting of the SEE Health Network in June 2006.
IS-04-016 Monozygosity – the obstetrical problem
I. Blickstein
Dept. of Obstetrics and Gynecology, Rehovot and the Hadassah-Hebrew University School of Medicine, Israel
The prevalence of monozygotic (MZ) pregnancies decreased significantly because of the increasing numbers of predominantly dizygotic iatrogenic twin gestations. At the same time, however, the absolute numbers of MZ twins increased because all methods of infertility treatment are associated with an increased zygotic splitting rate. Moreover, assisted conceptions seem to increase the prevalence of bichorionic triplets, which consist of a singleton and a monochorionic (MC) twin pair.
The zygote destined to develop into a singleton but instead undergoes splitting into MZ twins represents a serious reproductive anomaly. It is thus no wonder that both the MZ twins and their placenta (especially of MC twins) are associated with increased risk of anomalies. This construct gives rise to serious perinatal problems which manifest as increased risk of structural anomalies, problems related to the anomalous placenta and the vascular connections (such as growth restriction, TTTS, and TRAP sequence), increased risk of double fetal inflammatory response, and specific—MZ-related anomalies—such as conjoined twins.
IS-04-022 Feeding the preterm infant – the effect of functional food
C. Costalos
Department of Neonatal Medicine, Alexandra Regional General Hospital, Athens, Greece
In preterm infants, particularly those cared in an intensive care setting, an abnormal pattern of bowel colonization develops, when compared with that in healthy full-term infants, with lack in particular of lactic acid producing bacteria. This could be due to late introduction of milk (particularly breast milk) and extensive use of antibiotics. The resulting abnormal pattern of colonization can create a reservoir of antibiotic resistant bacteria which could contribute to the pathogenesis of necrotizing enterocolitis and sepsis. Therefore the establishment of a balanced microflora in these high risk infants might protect them from untoward effects. Modulation of intestinal flora can be achieved by adding probiotics which are live bacteria that colonize the gut and provide a health benefit to the host, or prebiotics which are nondigestible food components in the form of lacto or fructo-oligosacharides which promote the growth of bifidobacteria. Despite extensive studies on the use of prebiotics and probiotics in older children and adults there is very little literature on their use in preterm infants. From the few studies available they appear to be safe and some improve food tolerance and prevent constipation. There are reports also of reduced incidence of necrotizing enterocolitis and atopic disease following their administration. There are however many questions to be answered regarding the timing of their administration, finding the ideal probiotic that combines different properties, testing the possibility of combining pre and probiotics and adjusting the dosage and frequency of administration. Finally long term studies are needed in order to assess their long term effects on the health of these tiny infants.
IS-04-026 Are we discharging very preterm infants in a suboptimal nutrtional state?
W. Hay
Neonatal Clinical Research Center and Perinatal Research Center, University of Colorado Health Sciences Center, Aurora, Colorado, USA
Goal for nutrition of preterm infants: The only nationally published recommendation in the USA for providing comprehensive nutrition to the preterm neonate from birth to the time of discharge is to mimic the growth rate of the normal fetus of the same gestational age (American Academy of Pediatrics Committee on the Fetus and Newborn). Implicit in this recommendation is that growth of the preterm infant should reflect increases in weight, length, and head circumference of the normally growing fetus. Most evaluations of growth of preterm infants, however, have only considered weight gain and not body composition. Furthermore, there are no guidelines by the AAP as to how such growth should be achieved in preterm infants, and there are no data in the literature to support or refute this recommendation.
Status of growth of preterm infants: In contrast to this recommendation, a number of studies have shown that contemporary feeding practices result in significant growth failure in the preterm infant. The most often cited report is that by Ehrenkranz and colleagues, who recently published growth measurements of preterm infants from a large multi-center cohort trial from the National Institutes of Child Health and Human Development Neonatal Research Network. These authors found that most infants born between 24 and 29 weeks gestation did not achieve the median birth weight of the reference fetus of same postconceptional age by the time of discharge. The reference growth parameters used in this study represented postnatal observational data. Carlson and Ziegler further showed that mean growth rate for a population of very preterm infants from one institution progressively lagged behind intrauterine growth rates derived from serial ultrasound measurements.
Conclusions: Regardless of the means of estimating in utero growth of the normally growing human fetus, postnatal growth failure is universal and significant. Recent observations indicate that rapid catch up growth, particularly the positive crossing of weight for age and weight for length growth centiles, might have long term detrimental outcomes of increased risk of obesity, insulin resistance, diabetes, and cardiovascular disease. Thus, improved nutrition of preterm infants much earlier in their postnatal course, to prevent growth restriction of this vulnerable population of infants, is indicated.
IS-04-32 Recommendations for the prevention of RSV infection
E. Domenech, P. Fuster, J. Fernandez, C. Villafruela, J. Mesa
Hospital Universitario de Canarias, Ofra s/n La Cuesta, La Laguna, Spain
Respiratory syncytial virus (RSV) is the main cause of lower respiratory tract infection, especially bronchiolitis and pneumonia, in children of <2 years. There are several studies that provide evidences that severe RSV bronchiolitis in early infancy is a strong factor of risk for the occurrence of reccurrent wheezing or asthma. Premature infants with BPD present higher rates of hospitalization (13–18%), and increased disease severity (mortality of 3.5%). RSV hospitalization in patients with BDP is associated with increased health service utilisation and costs in the first two years. Hygienic measures and RSV monoclonal antibodies (palivizumab) have been found useful in decreasing rates of RSV hospitalization in these patients. Hygienic measures: Educational programs on RSV infection and hygienic barriers are recommended, aimed at parents and health workers. In the home, preventive measures include avoiding exposure to cigarette smoke and contagious environments. Specially important is hand-washing, particularly during periods of contact with anyone presenting respiratory infection or at high risk of exposure. Disposable tissues should be used. Palivizumab: Guidelines for their administration include: Strongly recommended for premature babies ≤286 weeks gestation, or born between 290–320 weeks gestation and age <6 months at start of RSV season or discharged along it, or treated for BDP during last 6 months (oxygen, bronchodilators, diuretics or corticoids) or by severe congenital heart disease. The latter two groups could receive prophylaxis for two RSV seasons. Since in our setting the RSV season usually begins in late October/November, prophylaxis should be initiated in mid-October and continued once a month until the end of the epidemic period (mid-February, 5 intramuscular doses of 15 mg/kg). With the use of palivizumab, hospitalization rates of premature infants with BPD has reduced to 5.6%.
IS-04-034 Pre- and postnatal infections and the role of host defense mechanisms in preterm and term infants
C.P. Speer
University Children's Hospital, Wurzburg, Germany
Polymorphonuclear neutrophils constitute the primary line of defense in the cellular immune system. In addition, the innate immune system present at birth plays a crucial role in front line host defense since it has been identified as a collection of factors, – such as cell-bound Toll-like receptors (TLRs) and mannose-binding lectin (MBL), – which effectively mediate recognition of a great variety of microbes and microbial products. Intact functions of neutrophils and the innate immune systems seem of utmost importance for the newborn which is devoid of any protection against microorganisms by products of the adaptive immunity, apart from transplacentally transferred IgG-derived from its mother. In general, newborns have an increased risk for systemic infections, and very immature preterm infants are especially prone to developing nosocomial bloodstream infections which clearly have been associated with increased morbidity and mortality. It has convincingly been shown that the marrow neutrophil storage pool is deficient in newborns and preterm infants. As a consequence of a quantitative deficiency neutropenia may ensue during the course of systemic infection. Moreover, neonatal neutrophils have a functional defect in adherence, deformability and chemotaxis. These abnormalities would be expected to result in slow influx of neutrophils at sites of microbial invasion or inflammation and predispose the newborn to mucocutaneous infections and pneumonia. The possible importance of “intrapartum priming” on neonatal neutrophil function by horioamnionitis or by various postnatal events is far from clear. Basal mRNA and protein expression of TLRs in the neonate was reported to be equivalent to adults, however, activation by LPS and other ligands was reduced. Thus, abnormal neutrophil function combined with other defects in host defense such as immunoregulatory dysfunctions, impaired macrophage activation by γ-interferon and deficient opsonizing activity could predispose newborns and especially preterm infants to localized bacterial infections that rapidly become systemic.
IS-04-037 Use and abuse of antibiotics in the neonatal intensive care unit
T. Krediet
Dept. of Neonatology, Wilhelmina Children's Hospital, University Medical Center, Utrecht, The Netherlands
Antibiotics are the most frequently prescribed drugs in neonatal intensive care units. In our unit almost all admitted infants are treated with antibiotics at any time during admission. The incidence of proven infection, however, is much lower (early onset sepsis 2%, late-onset sepsis 15%). These data suggest a huge overtreatment of neonates with antibiotics. With the increasing threat of emerging multi-resistant microorganisms this borderless use of antibiotics is a major problem in neonatal intensive care. Strict indication to initiate antibiotic treatment is the occurrence of clinical signs of infection and positive culture results. The occurrence of risk factors for infection is another indication for treatment with antibiotics. However, the identification of infants at risk is difficult and interpretation of risk factors is often dependent on individual judgement. Laboratory parameters with high positive predictive values may be helpful to identify patients with infection. On the other hand, laboratory parameters with high negative predictive values are important to exclude infection and may be helpful in the decision to discontinue antibiotic treatment.
The choice of antibiotics used for treatment is determined by the time of onset of infection and dependent on the most frequently isolated microorganisms in early or in late-onset sepsis, and their antibiotic resistance patterns. Moreover, local circulation of multi-resistant strains may play a role in the decision on which antibiotics to use. Therefore screening for such strains and monitoring their resistance patterns is considered to be important, although there is also evidence that the emergence and increased circulation of multi-resistant Gram-negative microorganisms in the neonatal unit is not associated with an increased incidence of sepsis caused by these organisms.
In order to decrease the threat of multi-resistant Gram-positive microorganisms causing sepsis, it is strongly advised to minimize the use of vancomycin in the treatment of late-onset sepsis caused by coagulase-negative staphylococci, the predominant nosocomial infection in neonatal intensive care units. It has been shown that oxacillin or first generation cephalosporins can be succesfully used to treat these infections.
To control antibiotic usage in neonatal intensive care units an operative infection control team including neonatologists with special interest in neonatal infections, pediatric infectious disease specialists, medical microbiologists and hospital hygiene specialists is necessary and this team should have regular meetings with the medical and nursing staff attending the neonatal intensive care unit.
Posters
P-01-001 Breech delivery in the obstetric department university clinic “sestre milosrdnice” in a ten-year period
V. Kosec, R. Herman, K. Kuna, I. Grbavac, I. Bolanca
University Hospital “Sestre milosrdnice”, Zagreb, Croatia
Aim: During the ten-year period analysis (1995–2004) of the experience with breech presentation delivery in the Clinic for Gynaecology and Obstetrics of the University Hospital “Sestre Milosrdnice”, the contribution to modern controversies regarding the method of delivery by sharing our own professional experience.
Material and Methods: We included 776 single-fetus breech presentation pregnancies from their 28th gestational week to term in our retrospective study in the period from 1995 to the year 2004. We compared the perinatal outcome between two groups; one that was delivered vaginally, and the other that was delivered by a Caesarean Section (CS). Perinatal mortality, Apgar scores at the 1st, 5th and 10th minute were also subject of analysis, as well as injuries during the delivery procedures and puerperal complications.
Results: Out of 776 breech presentation deliveries, 364 (47%) were delivered by the CS and 412 (53%) vaginally. Although low, the perinatal mortality is two times higher in the vaginal delivery group when compared to the CS delivery group (2.6‰ against 1.3‰). Apgar scores are significantly lower during the first minute in the vaginal delivery group, but the scores during the 5th and 10th minute do not differ significantly. The clavicle, humerus and cranial fractures were only registered in vaginal deliveries, and none occurred in the CS operations. We had no serious maternal complications in the puerperal period except a statistically significant increase in number of transfusions in the operative group.
Conclusion: On the basis of our extensive experience, we believe that the CS operative delivery in breech presentation term pregnancy is a better solution in comparison to vaginal delivery.
P-01-002 Maternal obesity and adverse labour outcome
A. Shah1, L. Kenny2, J. Sands3
1St. Mary's Hospital, Manchester, UK; 2Academic Unit of O & G, Manchester, UK; 3North West Perinatal Survey Unit, Manchester, UK
Objective: To investigate the association between maternal body mass index (BMI) and the risk of Caesarean section.
Methods: A population-based observation study at University of Manchester. The study sample was drawn from the North Western Perinatal Survey, a population based database comprising a total of 53,250 deliveries in the North Western Region between January 2004 and December 2005. Primigravid women with a singleton pregnancy and cephalic presentation at 37 weeks or more of gestation with accurate information regarding BMI at booking were included in the study (n = 6790). The population was classified according to BMI as underweight (BMI < 20 kg/m2), normal weight (BMI 20–24.9 kg/m2), overweight (BMI 25–29.9 kg/m2) and obese (BMI 30 (kg/m2). Main outcome measures were Incidence of Caesarean section and fetal macrosomia (birth weight > 4500 g).
Results: Maternal obesity (BMI (30 kg/m2) was associated with a significant increase in the incidence of Caesarean section, particularly unplanned emergency Caesarean section, compared with women with BMI < 29.9 kg/m2 (odds ratio = 1.75, 95% confidence interval [CI]: 1.50–2.05). Infants born to obese women were more than twice as likely to be macrosomic compared with infants born to women with BMI < 29.9 kg/m2 (odds ratio = 2.15, 95% CI: 1.79–2.57).
Conclusion: Our analysis confirms that there is a strong association between maternal obesity and an unplanned term Caesarean delivery. Obese women are at increased risk of intra- and post-operative complications following Caesarean delivery. This study highlights the need for interventions to reduce the incidence of obesity in young women.
P-01-003 Urinary and fecal incontinence in the postpartum – preliminary study
A. Henriques1, A.V. Lourenc1, T. Rodrigues2, L. Nicolau2, B. Nobre1, L.M. Graca1
1Dept. of Obstetrics, Gynecology and Reproductive Medicine, Santa Maria Hospital, Lisbon, Portugal; 2Biomathematic Laboratory, University of Lisbon Medical School, Lisbon, Portugal
Objectives: 1) To estimate the incidence of stress and urge urinary incontinence (SUI and UUI) and fecal incontinence (FI) symptoms in the immediate postpartum of singleton pregnancies in our Department. 2) To identify if any type of delivery is significantly associated with postpartum urinary and fecal incontinence. 3) To look for a possible correlation between birth weight and urinary symptoms in the immediate postpartum.
Methods: From April to November 2005, 1850 singleton deliveries occurred in our department. Puerperal women voluntarily (n = 878) filled out a symptom questionnaire concerning bladder (Kings Health Questionnaire) and bowel function. Statistic analysis with SPSS software included: Fisher exact test, χ2 test and exploratory multivariate analysis.
Results: 26.7% reported SUI symptoms. These complaints were more prevalent, in forceps, vacuum extraction, normal delivery, in labor C-section and C-section before labor group, in decreasing order. SUI symptoms are associated most often with forceps delivery, and less with C-section before labor (p = 0.041). 38.8% had UUI symptoms, being more frequent in vacuum extraction, forceps, in labor C-section, normal delivery and C-section before labor group, in decreasing order. Birth weight did not correlate with any of type of incontinence. Sample size is still short to discuss FI.
Conclusions: This preliminary study will continue with detailed subgroup analysis. For the present we can say that our results are concordant with the literature.
P-01-004 Postpartal deep-vein thrombosis with underlying agenesis of the inferior vena cava
M. Ilijic1, M. Krpan2, Lj. Banfic3, M. Ivanisevic1, N. Ljubas1, J. Djelmis1
1School of Medicine, Department of Ob./Gyn., Zagreb, Croatia; 2Clinic for Pulmonary Diseases Jordanovac, Zagreb, Croatia; 3University Clinical Center, Clinic for Cardiovascular Diseases, Zagreb, Croatia
Introduction: Hereditary thrombophilia, prolonged immobilization, malignancy, trauma, infection pregnancy and use of oral contraceptives are common factors that predispose to deep vein thrombosis in female population less than 40 years of age. Agenesis of the inferior vena cava is an extremely rare vascular defect resulting from aberrant development of the venous system during embryogenesis. Some authors have suggested it to be the additional, independent risk factor for venous thrombosis especially in young people with no other known risk factors.
Case Report: We would like to present a case of a pregnant woman with history of multiple pregnancy failures, ordered with prolonged bed rest, whose pregnancy was complicated with preeclampsia and intrauterine growth retardation. Furthermore, she underwent a Caesarean section and developed urinary infection. Postpartal period was further complicated with complete thrombosis of the right superficial femoral vein with proximal extension of the thrombus. All the risk factors mentioned above mislead as at first in reaching the diagnosis of this rare anomaly. To our knowledge, our case is the first to report postpartal deep vein thrombosis, with underlying anomaly of the inferior vena cava and successful pregnancy.
Conclusion: Even in pregnant patients carrying multiple risks, diagnosed with proximal thrombosis, underlying malformations of venous system should be considered.
P-01-005 Placenta previa accreta – usefulness of ultrasonographic examination in pre-delivery management
M. Verner, M. Meixnerova, J. Feyereisl, L. Krofta, P. Krepelka, V. Hejda
Institute for Care of the Mother and Child, Prague, Czech Republic
Objective: The aim of our study was to show the efficacy of ultrasonographic examination in the prenatal diagnosis of placental pathology and disorders of placentation.
Methods: Case report.
Results: We present the case of a patient with placenta previa accreta in the second pregnancy after delivery by caesarean section. The abnormal localization and the abnormally deep invasion of the placenta into myometrium was diagnosed in the second trimestr. The early identification of this condition allowed us to adequately prepare for caesarean delivery. This is a significant factor in preventing maternal mortality and serious maternal morbidity in the group of patients with abnormal placental localization and myometrial invasion.
Conclusion: The incidence of placenta accreta has increased 10-fold in the past 50 years and now occurs with frequency of 1 per 2,500 deliveries. The major risk factors are maternal age and the number of previous caesarean sections. Both risk factors are rising in the population of pregnant women. It is very probable, that we can expect to diagnose this pathological situation more often. Placenta previa accreta is a condition with high morbidity and it is one of the most common causes of serious maternal postpartum hemorrhage. The early diagnosis of this condition allows us to adequately manage pregnancy and to plan delivery so as to minimize negative consequences. Today the most common diagnostic utility is ultrasound especially with complementary color Doppler examination in the case of abnormal placentation. In unclarified situations MRI is indicated.
P-01-006 Mode of delivery and method of monitoring labour in fetuses with prenatally diagnosed arrhythmia
M. Brejchova, T. Binder, J. Horak, R. Vlk
Clinic for Obstetrics and Gynecology, University Hospital Motol, Prague, Czech Republic
Objective: To evaluate the outcome of peripartum management in fetuses with arrhythmia diagnosed prenatally and treated in utero.
Methods: We evaluated a group of 15 pregnant women with prenatally diagnosed fetal cardiac arrhythmia. Of these: 11 cases of fetal tachycardia were treated according to Utrecht protocol (7 with prepartum total or partial conversion to sinus rhythm achieved, 4 with persisting tachycardia) 4 cases of fetal bradycardia due to an AV block.
A planned caesarean section was performed in 3 cases – 1 case with persisting tachycardia and progressive fetal hydrops, 2 cases with breech presentation of fetus. In the rest of studied women, we primarily chose the vaginal mode of delivery.
In 4 patients with fetal tachycardia and all patients with fetal bradycardia, valid intrapartum monitoring using CTG was impossible, these cases were monitored by fetal pulse oximetry.
Results: In 7 cases diagnosed with fetal tachycardia vaginal delivery took place without complications, of these in 4 cases monitoring was performed only with FPO. In 1 case, using FPO on the basis of decreased O2 saturation imminent fetal hypoxia was diagnosed and indicated termination of pregnancy by caesarean section. Vaginal delivery without complications took place in all 4 cases with fetal bradycardia. Evaluation of neonatal status and blood gas after delivery fully correlated with the FPO monitoring.
Conclusions: Vaginal delivery with monitoring by fetal pulse oximetry in our studied group appears to be sufficiently safe. Fetal pulse oximetry provides valid fetal monitoring.
P-01-007 Predictive factors for successful induction of labour
E. Kasikova, P. Krepelka, L. Krofta, P. Darebny, J. Feyereisl
Institute for Care of Mother and Child, Prague, Czech Republic
Introduction: Induction of labour is carried out in approximately 20% of pregnancies. However, approximately 20% of women having induction of labour end up having a Cesarean delivery. The traditional method of predicting whether an induced labour will be successful vaginal delivery is based on the preinduction ‘favouribility’ of the cervix as assessed by the Bishop score. However, this assessment is subjective and several studies have shown a poor predictive value for predicting the chances of successful labour induction have been investigated recently, it is a transvaginal sonography of the uterine cervix.
Aims: To study cervical clinical data and ultrasound parameters for predicting the mode of delivery following medically indicated induction of labour in term patient.
Methods: The study was conducted prospectively in women who required medically indicated induction of labour. Inclusion criteria were singleton pregnancy, gestational age over 37 weeks of amenorea, cephalic presentation and intact fetal membranes. The Bishop score and its components, parity, cervical ultrasound parameters and gestational ultrasound (presentation of the head, posterior angle of cervix, weight of fetus). These parameters were analysed in order to determine the most predictive factors for vaginal delivery following induction of labour.
Results: Of the 172 women included in the study, in 57 (33%) the pregnancies were terminated by caesarean section. Multivariate analysis of the standard deviation using General Linear Model was used for statistical evaluation. The level of significance was 0.004. There is a statistical significant difference between the groups (group of vaginal delivery and group of caesarean section) in the Bishop score, cervicometry and parity.
Conclusions: The lenght of the cervix, measured by transvaginal sonography, Bishop score as well as parity are predictors for vaginal delivery following induction of labour.
P-01-008 The outcome of multiple pregnancies compared to the method of delivery
V. Miketic, S. Raspopovic, I. Djukic
Dep. of Gyn. and Obs., Clin. Centre of Montenegro, Krusevac bb, Podgorica, Yugoslavia
Objective: To compare the pregnancy outcome between vaginal and SC delivery in multiple pregnancies.
Methods: Retrospective study is analyzed the method and outcome of delivery in multiple pregnancies during the period 1996–2005.
Results: During the abovementioned time period the total number of 27,192 deliveries had happened, out of which 475 were multiple pregnancies (1.74%). Out of total number of multiple pregnancies, there were 461 twin, 13 triplet and 1 quadriplet pregnancies. The total number of newborns delivered during multiple pregnancies was 965. By the SC was delivered 181 VS. 294 by vaginal delivery (38.1% vs. 61.9%), 47.15% multiple pregnancies were terminated before 37th weeks gestation. 21% newborns was treated in NICU. Total mortality rate was 4.9% (SC 2.1% vs. 2.8% vaginal delivery). 95.5% newborns with lethal outcome were from pregnancy between 28–30 gestatational weeks.
Conclusions: There was no significant difference in perinatal outcome compared to the method of delivery, in our study it's gestational age depended.
P-01-009 Deliveries of women with multiple gestations
B. Colakovic, V. Colakovic Popovic, I. Djukic, O. Colakovic, S. Crnogorac
Klinicki centar Crne Gore, Ljubljanska bb, Podgorica, Yugoslavia
Aim: Perceiving: frequency of multiple gestations delivery, delivery completion and perinatal mortality in two periods of time and comparison of obtained data.
Work Method: We have compared data on deliveries of women with multiple gestations in Clinical Center of Montenegro in Podgorica in the period 1977–1983 with the period of time at about 20 years later (2000–2004).
Results: See . In the first period (1977–1983) out of 19,450 deliveries, there were 223 or 1.14% with multiple gestations. Frequency of twins is 1:88 deliveries and of triplets 1:9725 deliveries.
In the second period (2000–2004) 13,962 deliveries, 272 or 1.94% were with multiple gestations. Twins were born in 1:54 deliveries, and triplets 1:1074 deliveries.
Perinatal mortality in Montenegro in the period 1977–1983 was between 17 and 14 per mille, and in the period 2000–2004 between 11 and 10 per mille.
Conclusions: Second period compared to first one:
frequency of twins is by 40% higher, and triplets by 9 times;
frequency of caesarean deliveries is by 4–5.5 higher;
perinatal mortality is by 15% higher, and early neonatal mortality (0–6 days) is higher by 28%.
P-01-010 Multifactorial causes for negative perinatal outcome after vacuum assisted deliveries
D. Tutunaru1, R. Vladareanu1, M. Petrache2, M.C. Dumitrascu3, A. Veduta1
1Elias Emergency Hospital, Marasti, Bucharest, Romania; 2Polizu Obstetrics Gynecology Hospital, Polizu, Bucharest, Romania; 3Universitary Emergency Hospital, Splaiul Independentei, Bucharest, Romania
Aim: To investigate the hypothesis that perinatal outcome after vacuum assisted delivery (VAD) is strongly influenced by obstetrician's experience and skills.
Methods: Retrospective, multicenter, case-control study. We compared obstetrical practice before and during VAD on new-borns with good outcome (control group) compared with those with poor outcome (study group). Cases were recruited from three large hospitals from Bucharest, between May 2003 and December 2005. Number of vacuum applying attempts, need for CS or forceps because of vacuum applying failure, Apgar scores, cardiotocograph (CTG) patterns, shoulder dystocia, cephalhematomas, intracranial hemorrhage, seizures, respiratory detress and number of deaths, have all been accounted.
Results: In the control group (n = 144) there was a correct conduct of the second stage of labor (CTG recordings, pushing, placement of the cup, etc.) and the number of low Apgar scores, shoulder dystocia, cephalhematoma was very low, whereas in the case group (n = 43) we discovered abnormalities regarding CTG pattern, delayed decision to shift to CS or to apply forceps, multiple vacuum attempts, incorrect cup appliance, delivery failure using vacuum, neonatal bruises (due to excessive pushing) and seizures (hypoxia), etc. In the control group the training level of practitioners was very high compared to that of the second group (where the residents comprised the largest part).
Conclusion: Obstetrician experience in vacuum assisted delivery is of paramount importance upon perinatal outcome, not only regarding the skills (proper application and knowledge to pull) but also the timing of taking the decision whether is appropriate to use vaginal delivery vs. CS, for safe delivery.
P-01-011 Ruptures of the scar and multiple caesarean sections
G. Relic1, M. Bogavac2
1Medical School in Pristina, Department of Obstetrics and Gynecology, BB, Priština, Serbia; 2Clinical Center Novi Sad, Department of Obstetrics and Gynecology, Novi Sad, Serbia
Aim: To investigate whether the increased number of caesarean sections increases the incidence of incomplete and complete ruptures of the scar.
Material and Methods: The authors investigated 2474 women with repeated caesarean sections (SC), hospitalized at The Department of Obstetrics and Gynaecology in Prishtina. The 2nd caesarean section was performed in 2041 women, the 3rd in 343, the 4th in 74, and the 5th in 16 women. Condition of the scar, i.e. incomplete (in case of perimetritis) or complete (when the integrity of the total uterine wall has been disturbed) has been estimated by a direct examination of the uterus during the procedure of caesarean section.
Results: The complete rupture of the scar occurred in 0.10% women following the 1st caesarean section and 0.05% patients following the 2nd caesarean section. There were no complete ruptures of the scar following the 3rd and 4th caesarean section. The recorded differences were not statistically significant. The incomplete rupture of the scar occurred in 0.53% of the women following the 1st caesarean section and 0.34% patients following the 2nd caesarean section. 1.17% of patients suffered from incomplete rupture of the uterus following the 3rd caesarean section and 1.35% following the 4th caesarean section. All recorded differences were not statistically significant.
Conclusion: Increased number of caesarean sections has not been followed by statistically significant incidence of incomplete and complete ruptures of the scar.
P-01-012 Does the number of early postoperative complications follow the increase of the rate OF caesarean sections?
G. Relic1, M. Bogavac2
1Medical School in Pristina, Department of Obstetrics and Gynecology, BB, Priština, Serbia; 2Clinical Center Novi Sad, Department of Obstetrics and Gynecology, Novi Sad, Serbia
Aim: To estimate whether the number of early postoperative complications follows the increase in the rate of caesarean sections.
Material and Methods: The incidence of the mentioned complications was investigated, comparing the 2nd and 3rd caesarean section and 4th and 5th caesarean section.
Results: Endometris occurred in 2.25% of women following the 2nd caesarean section, 2.33% following the 3rd caesarean section, 8.11% following the 4th caesarean section and 6.25% following the 5th caesarean section. Superficial wound dehiscence occurred in 3.38% patients following the 2nd caesarean section, 2.62% following the 3rd caesarean section, 2.70% following the 4th caesarean section and 6.25% following the 5th caesarean section. The complete wound dehiscence occurred in 0.93% patients following the 2nd caesarean section, 0.87% following the 3rd caesarean section, whereas there were no complete wound dehiscences following the 4th and 5th caesarean section. Peritonitis occurred in 0.88% patients following the 2nd caesarean section, 0.58% following the 3rd caesarean section, whereas there were no wound infections following the 4th and 5th caesarean section. Ileus occurred in 0.49% patients following the 2nd caesarean section and in 0.87% following the 3rd caesarean section, whereas it was not recorded following the 4th and 5th caesarean section. Hysterectomia totalis occurred in 0.93% patients following the 2nd caesarean section, 0.87% following the 3rd caesarean section, whereas there were no total hysetrectomyies performed following the 4th and 5th caesarean section. Sepsis occurred in 0.05% patients following the 2nd caesarean section, 0.58% following caesarean section, whereas there were sepsis recorded following the 3rd, 4th and 5th caesarean section.
Conclusion: Increase in the number of caesarean sections does not result in statistically significant increase in the number of postoperative complications.
P-01-013 Caesarean section deliveries: indications and risks for the newborn
M. Christodoulaki, M. Kalloniatou, G. Tsoukalas, S. Blazaki, A. Kanitsakis, A. Kotta, E. Xidaki, I. Tsoukalas, G. Daskalakis
General Hospital of Chania, Mournies, Chania, Greece
Background: There is a rising rate of caesarean deliveries in recent years.
Aim: To examine the indications of caesarean section in our hospital and the risks for the newborn of caesarean section.
Methods: An analysis was conducted of the medical records of 1031 women who had caesarean deliveries and the medical records of their infants during the period 2003–2005.
Results: During the study period there were 1031 caesarean deliveries and 1045 infants were born. The mothers of 712 (68.13%) newborns were Greek and 313 were aliens.
The main indications for caesarean section were: previous caesarean section (46%), failure to progress (13%), cephalopelvic disproportion (12%), maternal medical conditions (diabetes, hypertension, preeclampsia-eclampsia, others) (10%), breech presentation (6.4%), fetal distress (4.4%), placenta previa or abruption (2.6%), abnormal presentations (2%), multiple gestation (1.4%) and others.
Five hundred and sixty-two newborns delivered by caesarean section were males (54.5%).
Ninety-two newborns (9.8%), of gestational age ≥ 35 weeks, presented transient tachypnea of the newborn (42 admitted to neonatal intensive care unit) and 4 presented perinatal asphyxia.
Five hundred and twenty-five (50.2%) neonates were breast fed, 228 (21.8%) were formula fed and 292 (27.9%) were fed both formula and breast milk.
Conclusions: Previous caesarean section was the most common indication. Although caesarean deliveries have become safer over the past century they are not without significant risks for the newborn.
P-01-014 Early maternal and neonatal consequences of instrumental deliveries
E. Cardoso, N. Clode, L.M. Graca
Department of Obstetrics, Gynecology and Reproductive Medicine, Hospital Santa Maria, Lisbon, Portugal
Objectives: To evaluate maternal and neonatal early consequences of forceps and vacuum assisted deliveries in anterior or posterior vertex presentations.
Methods: All instrumental deliveries (Simpson forceps or Kiwi vacuum) in singleton term pregnancies (≥37 weeks) in anterior or posterior vertex presentation that occurred between June 2004 and December 2005 were reviewed. Maternal demographics, delivery characteristics, maternal outcome (episiotomy extension, perineal or cervical lacerations) and neonatal outcome (instrumental marks and bruising, molding, scalp lacerations, cephalohematoma, Apgar scores and need for neonatal intensive care unit admission) were evaluated, comparing vacuum to forceps assisted delivery. For statistical analysis t-Student, χ2, Fischer exact test and exploratory multivariated analysis, were performed.
Results: In 257 cases (128 vacuum assisted and 129 forceps) the data in the revised charts allowed the analysis. There were no differences concerning analgesia type, operator skill, fetal presentation, and newborn weight. Rates of higher stage application (p < 0.01) and use in primipara (p < 0.5) were greater in vacuum assisted deliveries. Episiotomy extension (p < 0.1) and third grade perineal laceration (p < 0.3) were more frequent with forceps use. Major maternal sequelae (third degree laceration and cervical laceration) were globally low (4%). No major neonatal sequelae were found. 119 (46%) newborns had marks, bruising, caput succedaneum or molding; these minor findings were more frequent in vacuum assisted deliveries (p < 0.1).
Conclusions: In our experience instrumental delivery in anterior or posterior vertex presentation seems to be safe for the mother and the neonate although forceps delivery is associated with a higher rate of maternal perineal trauma and vacuum delivery with minor neonatal sequelae.
P-01-015 Postnatal thromboprophylaxis. How good are we?
B. Singhania, S. Bollapragada, F. Mackenzie, P. Owen
Princess Royal Maternity Hospital, Glasgow Royal Infirmary, Glasgow, UK
Objective: To assess the compliance of a large maternity unit in administering appropriate postnatal thromboprophylaxis.
Methods: Case notes of all deliveries for the month of December 2005 (Total = 373, SVD = 226, Instrumental = 37, Elective caesarean section = 44, Emergency caesarean section = 66) were reviewed for the risk of VTE and thromboprophylaxis. The unit's protocol on postnatal thromboprophylaxis provided the audit standard.
Results: 1) Overall 38.3% (143 of 373) women were assessed to be medium or high risk by the auditing team and required thromboprophylaxis. 2) The correct documented risk assessment was noted in only 19.3% (72 of 373). The risk factors most commonly overlooked were obesity and maternal age. 3) Of those requiring thromboprophylaxis, only 12% (3 of 25) of the women having a SVD, 23.8% (5 of 21) of those having an instrumental delivery, 54.8% (17 of 31) of those having an elective caesarean section and 15.2% (10 of 66) of those having an emergency caesarean section were documented to have received adequate thromboprophylaxis. 4) 75% (75 of 100) of women in the high risk group did not receive thromboembolic deterrent stockings. 5) The correct dose, duration and timing of first dose of LMWH was given in only 50.3% (72 of 143) of women in the medium or high risk group.
Conclusions: There was a significant failure to implement the correct thromboprophylaxis measures. There is a need to improve the awareness amongst health care professionals about the need to correctly assess the risk for VTE and administer appropriate thromboprophylaxis. We have already implemented measures for this in our unit and plan to reaudit in March 2006.
P-01-016 Pelvic floor morbidity after instrumental delivery – the use of 4D ultrasound in the evaluation of pelvic organ prolapse
L. Krofta, M. Otcenasek
Institute for the Care of Mother and Child, Prague, Czech Republic
Objective: Vaginal childbirth is a risk factor for female pelvic organ prolapse and stress urinary incontinence. Transperineal, 2D ultrasonography can be used for the assessment of female pelvic floor organ morphology. The rapid development of three- and four-dimensional technology may allow dynamic assessment of pelvic floor anatomy. We intended to define the incidence of major trauma to the musculus levator ani (pars pubococcygea) after instrumental delivery.
Methods: The assessment included a clinical examination and 4D introital ultrasound. 58 primigravidas were seen 12 to 38 weeks after instrumental vaginal delivery (Forceps Kjelland).
Results: Of the 58 women, levator avulsion was diagnosed in 45 (78%) patients. Avulsion was bilateral in 14 cases, on the right side in 20 cases, and on the left in 11 cases. Among those with levator avulsion, there was an association with pelvic organ prolapse and worsened stress incontinence postpartum.
Conclusion: Instrumental delivery can cause morphological alteration visible on 4D translabial ultrasound. Avulsion of the levator ani muscle from the pelvic wall occurred in approximately 80% of all women delivered instrumentally.
P-01-017 Intracraneal hemorrhage in full term newborn infants
J.R. Castro-Conde, C. Villafruela-Alvarez, E. Domenech-Martinez, C. Gonzalez-Campo, A. Mendez-Perez, A.A. Hernandez-Borges
Servicio de Neonatología, Hospital Universitario de Canarias, Ofra s/n, La Laguna, Spain
Objective: To describe incidence, risk factors and major types of neonatal intracranial hemorrhage (ICH) in full term neonates in our unit.
Patients and methods: We analyzed the records of all full term newborns diagnosed of ICH between January 2000 and December 2005. We studied the clinical findings, ICH types, risk factors, treatment and prognosis of every case. TC was employed in all cases, and RMI in a third of them.
Results: We found 18 full term neonates with ICH. Five of them suffered ICH in two locations, resulting in 23 types of ICH in the whole sample. Eleven infants (61.1%) born in our hospital, while six (35.3%) born out. Six hemorrhages (26.1%) were intraventricular; 5 were primary subarachnoids (21.7%); 4 were epidurals (17.4%); 3 were intraparenchymals (13%); 3 were intracerebellars (13%); and 2 were subdurals (8.7%). Eleven infants (61.1%) born after forceps (n = 7; 38.9%) or vacuum extraction (n = 4; 22.2%), four infants (22.22%) after a spontaneous non traumatic labor, and three (16.7%) were born by caesarean. Clinical findings included: 6 cephalohematomas (33.3%), 4 cases with seizures (22.2%), 3 with irritability (16.7%), 3 infants were hypotonic and stuporous (16.7%), 1 had apnea and hypertonia, and 7 cases (38.9%) were asymptomatic. Only 3 infants need surgical treatment, and one infant died. Two infants suffered epileptic disorders, but all survivals showed favorable neurodevelopment.
Conclusions: ICH may occur in full term newborns without obstetrical risk factors. Furthermore, in many cases the ICH does not produce significant clinical signs or these are subtle. Therefore, it is possible an infradiagnosis of the ICH in these infants.
P-01-018 Serum s100b levels and thyroid function in neonates with perinatal asphyxia
G. Triantafyllidis1, M. Theodoraki1, A. Konstantinidi1, G. Kafalidis1, S. Tsalavoutas2, I. Labadaridis1
1NICU, General Hospital of Nikea, Piraeus, Greece; 2Endocrinology Lab of General Hospital of Nikea, Piraeus, Greece
Introduction/Aim: S100B is a member of a multigenic family of calcium-modulated, low molecular weight proteins, expressed in the CNS. Increased serum S100B levels have been associated with perinatal asphyxia, which also triggers alterations in the levels of several hormones. The aim of the present study was to determine serum S100B levels and thyroid function indices (T4, T3, TSH) in neonates with perinatal asphyxia.
Patients and Methods: The study group was composed of 16 full term newborns with a GA ≥ 37 weeks and history of perinatal asphyxia. All of them demonstrated fetal distress, had Apgar scores at 1 min < 4 and at 5 min < 7, required vigorous resuscitation and were intubated in the delivery room. 16 normally delivered term newborns served as the control group.
Serum S100B and thyroid hormones were measured within 48 hours from delivery.
Results: Serum S100B levels in the asphyxiated neonates were found to be significantly higher [median 5.5 μg/l (2.6–16.0)] than in the control neonates [1.6 μg/l (1.1–2.4)] (Mann – Whitney test; p = 0.005). Additionally, lower thyroid hormones levels [T4 = 9 μg/dl ± 2.3; T3 = 84 ng/dl (62–104); TSH = 6.19 μU/ml (2.9–8.9)] were observed in asphyxiated newborns than those reported in the literature for nonasphyxiated neonates.
Conclusion: Thyroid function is depressed, suggesting central hypothyroidism secondary to asphyxia. Furthermore, serum S100B levels are significantly elevated in asphyxiated newborns probably reflecting CNS damage due to asphyxia. The prognostic significance of the above alterations is under investigation.
P-01-019 Association between lactate concentration in amniotic fluid (AF) and dysfunctional labour
E. Wiberg-Itzel, H. Pettersson, S. Cnattingius, L. Nordström
Karolinska Institute, Stockholm, Sweden
Labour dystocia is a common obstetrical problem and main indication for operative intervention during parturition. Inefficient long lasting uterine activity during labour might lead to anaerobic metabolism in the uterine muscle with a progressive lactate acidosis. A possible source of lactate in AF could be the myometrium.
Objective: There is an association between lactate concentration in AF and dystocic labour.
Methods: 53 women attending labour ward at Soder Hospital, Stockholm, Sweden. All had a singleton fetus in cephalic presentation; gestation ≥ 34 weeks; cervical dilatation ≥ 4 cm; ruptured membranes; regular painful contractions and no sign of fetal distress. They all had an intra uterine catheter inserted. 5 μl AF was collected from the catheter for lactate analysis every 30 minutes. In each case a mean lactate concentration was calculated from all samplings. A receiver operator characteristic curve (ROC) was constructed to determine best “cut off” lactate concentration to distinguish between dysfunctional labour or spontaneously vaginal delivery.
Results: The median value of lactate in AF during labour for the whole group was 9.7 mmol/l. Among 30 women operatively delivered due to dystocia the median lactate value was 10.2 mmol/l (range 8.2–15. 8), while in the 23 with spontaneous delivery the corresponding values were 8.9 mmol/l (6.8–11.4) (p < 0.001).
25 of the women had a mean lactate value ≥ 9.8 mmol/l and 22/25 (88%) had an operative delivery caused by dystocia. 20 of the women had a lactate value ≤ 9.3 mmol/l, 15/20 (75%) had a spontaneously vaginal delivery. Eight of the women had a lactate concentration in AF between 9.3–9.5 mmol/l, 5/8 had a spontaneously vaginal delivery.
Conclusions: High lactate concentration in AF (≥9.8 mmol/l) is associated with labour dystocia. See .
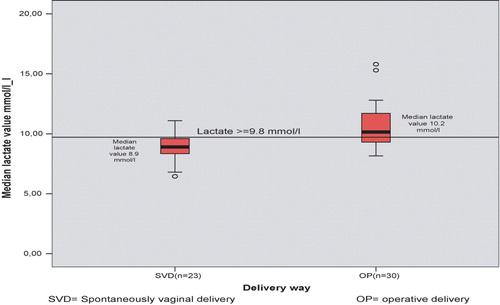
P-01-020 Caesarean section and perinatal morbidity and mortality
S. Petakovic, D. Malobabic, S. Arbanas, B. Mitrovic, O. Miladinovic
Health Center Sremska Mitrovica, Department of Gynecology, Obstetrics, and Neonatology, Stari Sor 65, Sremska Mitrovica, Serbia
Introduction: In the ongoing discussion on the controversy on the relative increase of the number of caesarean sections, the dilemma frequently arises if this also has an effect on reducing perinatal morbidity and mortality.
Goal: To establish the effect on caesarean section on perinatal morbidity and mortality.
Materials and methos: We was analyzed data on the total number of parturitions and caesarean sections, gestation age, and body weight of neonates, the Apgar score, perinatal morbidity and mortality of neonates.
Results: In the the ten year period, with a relatively constant number of patruritions of 1362–1699 (mean 1518), there was an increase of the percentage of caesarean section from 6.96%–18.13% (mean 12.73%). There were also 16 twin pregnancies. In 1933 caesarean sections, 1949 neonates were born. Most neonates were born in gestation week 38–40 (94.46%), with a body weight of 3000–3999 grams (64.92%). 98 (5.03%) caesarean sections were done in cases of premature neonates. Apgar score 8–10 was recorded in 63.62%, 4–7 in 32.22%, and 3–1 in 3.90% of neonates. Among types of neonatal morbidity, the most frequent were asphyxia (14.52%) and hiperbilirubinemia (2.77%). Most frequent causes of early neonatal death after caesarean section were RDS and asphyxia with aspiration. Mortality due to caesarean section was 0.33‰, and early neonatal mortality 1.24‰. In relation to the total number of births, perinatal mortality for babies born by caesarean section was 1.57‰, corrected 0.65‰. Total perinatal mortality for babies born during the same period is 12.64‰, corrected 7.27‰.
Conclusion: Intensive prepartum monitoring, a timely and correct decision pertaining to ending the parturition by caesarean section, accompanied by modern intensive care of neonates, resulted in reducing perinatal morbidity and mortality.
P-02-001 Development of growth curves for the population of pakistan
S. Munim, I. Azam, S. Malik, N. Ahmad
The Aga Khan University Hospital, Karachi, Pakistan
Objective: The main aim of this study is to develop antenatal growth curves that can be used as a reference in our population.
Methodology: It is a Prospective study conducted at The Aga Khan University Hospital, Karachi between October 2004 and December 2005. A cohort of 627 women was recruited and followed up longitudinally. Pregnant women were from two hospitals in Karachi.
Women with singleton pregnancy and gestational age confirmed by ultrasound were included in this study. Those with multifetal gestation and with any medical disorder were excluded.
Variables like age, Parity, Height, weight and ethnicity were all included in this study. Two or Three additional scans were performed between 16–37 weeks of gestation apart from the anomaly scan. Head circumference, abdominal circumference and Femur length were measured by trained operators. Post natal outcome was measured by birth weight and mode of delivery. In addition gender was also noted.
All data was entered in a database file and analyzed by SPSS statistical package.
Results: Growth curves were constructed based on the measurements of head circumference, abdominal circumference and femur length.
P-02-002 Proportions of neuroactive 3alpha- and 3beta-pregnanolone isomers are different in non-pregnant women and in pregnancy
A. Parizek1, M. Hill2, A. Paskova1, H. Havlikova2, L. Kancheva2
1Department of Gynecology and Obstetrics, 1st Medical Faculty, Charles University, Prague, Czech Republic; 2Institute of Endocrinology, Prague, Czech Republic
Pregnanolone isomers (PI) with a hydroxy-group in the 3alpha-position, allopregnanolone (3alpha-hydroxy-5alpha-pregnan-20-one, P3a5a) and pregnanolone (the 5beta- epimer, P3a5b), are are the most efficient endogenous analgesics operating via allosteric modulation of GABA(A) receptors. However, the steroids could be readily converted in oxido-reductive pathway to their 3beta-epimers exerting an opposite effect.
To estimate, whether the ratio of 3alpha- to 3beta-PI differs in various physiological situations in women of fertile age, the PI allopregnanolone (P3a5a), isopregnanolone (P3b5a), pregnanolone (P3a5b) and epipregnanolone (P3b5b) and their polar conjugates were measured in the serum of women in follicular (F, n = 15) and luteal phase (L, n = 16) and in maternal (M, n = 8) and umbilical serum (U, n = 8) at labor using GC-MS. The data were treated by multiway ANOVA followed by Fisher's LSD multiple comparisons.
In 5alpha-PI, the ratio of 3alpha to 3beta epimer (R3ab_5a) did not differ among the groups F, L and M but it was lower in U (p < 0.01). The ratio in 5beta-PI did not differ among the groups F, L and U but showed markedly higher value in M (p < 0.0001). The ratio for 5beta-isomers was significantly higher in pregnancy (p < 0.001). The findings could be of interest concerning the pregnancy-stabilizing role of 3alpha-pregnanolone isomers.
P-02-003 Preeclampsia complicating early pregnancy period in a case of partial hydatidiform mole
M. Cerna1, M. Korbel1, Z. Niznanska1, A. Havalda1, M. Redecha1, L. Danihel2, J. Vojtassak3, V. Repiska3
11st Department of Obstetrics and Gynaecology, Comenius University Medical School, Bratislava, Slovak Republic; 2Institute of Pathological Anatomy, Comenius University Medical School, Bratislava, Slovak Republic; 3Institute of Medical Biology and Genetics, Comenius University Medical School, Bratislava, Slovak Republic
Objective: A rare case of preeclampsia in early pregnancy period in partial hydatidiform mole is presented.
Methods: A case report.
Results: Symptoms of preeclampsia started in the first half of pregnancy in 24 year-old gravida 1. The blood pressure 110/60 mmHg at the first visit in 8th week rose slowly to 135/65 mmHg at 13 weeks of gestation. On ultrasound scan fetal CRL corresponded to 12 weeks of gestational age, NT&NB was normal, placenta morphology was not described. At 17 weeks of gestation blood pressure rose up to 145/80 mmHg elevated AFP in maternal serum and amniotic fluid over 2 MoM were detected. On ultrasound scan thick placenta and 2 weeks' fetal growth retardation were found. At 19 weeks of gestation oedema and lower abdominal pain occured, blood pressure rose up to 155/95 mmHg under magnesium sulfate control, urine dipstick protein 3+, moderate anaemia, thyroid dysfunction, and high level of hCG were detected. Ultrasound diagnosis of partial hydatidiform mole with bilateral ovarian multiple cysts, oligohydramnios, and 4 weeks' IUGR of fetus was performed. 69,XXX karyotype from amniotic fluid was obtained. Blood pressure rose up to 160/100 mmHg at the day of pregnancy termination. One week after evacuation blood pressure was 120/80 mmHg, and urine dipstick protein 1+. The histological examination confirmed the diagnosis of a partial hydatidiform mole. Karyotype 69,XXX from placental tissue and fetal muscle cells was obtained. Using DNA analysis, the paternal origin of the partial mole was confirmed. Two months after evacuation the patient was free of disease (normal blood pressure, negative hCG, no proteinuria, normal sonographic scan on uterus and ovaries).
Conclusion: Development of preeclampsia in 1st half of pregnancy should prompt a comprehensive workup to exclude possible molar pregnancy. In our case the abnormal levels of AFP & hCG, thick placenta with partial hydropic changes, oligohydramnios, IUGR prior 20 weeks of gestation and ovarian cysts on the ultrasound scan lead to the diagnosis of partial hydatidiform mole.
P-02-004 Antiphospholipid syndrome and pregnancy outcome
M. Antic1, M. Cvetkovic2, A. Ljubic2, J. Stamenkovic2, D. Bratic2
1Clinical centre “Dr D. Misovic”, Belgrade, Serbia; 2Institute of Gynaecology and Obstetrics KCS Belgrade, Belgrade, Serbia
Objective: Antiphospholipid syndrome is defined as a autoimmune disorder characterised by the presence of antiphospholipid antibodies, recurrent arterial and venous thrombosis and infertility. This syndrome is one of the most common causes of hypercoagulability in the general population. The antiphospholipid syndrome have recived considerable attention because of their association with a number of serious clinical disorders, including arterial and venous thromboembolism, acute ischemic encephalopathy (TIA, stroke), coronary artery disease, myocardial infarction in young persons by cosing thrombosis in the coronary arteries, renal syndromes cosed by acute thrombosis at level of capillaries, arterioles, and venules, spontaneous thrombosis in pulmonary vassels, thrombocytopenia, recurent pregnancy loss and serious complications in pregnancy. Pregnancy itself is notably a hypercoagulable state and interaction with an condition such is thrombophilia might caused the severity condition such as pre-eclampsia, venous trombosis and thromboembolism, placental abruption, HELLP syndrome.
Methods: A longitudinal, prospective, observational study was set in department of high risk pregnancy, Institut of Gynaecology and Obstetrics, Clinical centre of Serbia, Belgrade, during 2002–2005. Study obtained 30 pregnant women with diagnosis of antiphospholipid syndrome. Criteria for diagnosis of antiphospholipid syndrome was at least one clinical criterion (unexplained death of one or more morphologically normal fetuses after the 10th week of gestation, or three or more unexplained spontaneous abortions before the 10th week of gestation) and one laboratory criterion (anticardiolipin IgG or IgM antibodies, or lupus anticoagulant antibodies present in high levels in the blood). Combination Fraxarin plus low-dose asprin administered since the viable pregnancy was confirmed.
Results: Complications during the pregnancy included 3 placental abruption, 2 thrombocytopenia, 1 veno-us thrombosis, 1 HELLP Syndrome, 2 preeclampsia, 8 pregnancy induced hypertension. Three of them have a spontaneus abortion, one have a intrauterine fetal death in 28th week of gestation, and 26 of them had a succesfull outcome.
18 of them have a Caesarian section and 9 have a vaginal delivery.
Conclusions: The live birth rate of women with antiphospholipid syndrome without therapy is low as 10%. Combination of fraxarin and low-dose aspirin treatment, the live birth rate increases to 70–80%. There is still an excessive frequency of maternal and\or fetal complications, indicating the necessity of a better calibration of the dosage, and timing of administration of treatment.
Keywords: Antiphospholipid syndrome, pregnancy outcome
— Cancelled
P-02-006 Vascular endothelial growth factor expression in complicated pregnancies
D. Borras1, N. Ruiz2, I. Alonso3, C. Simon3, A. Pellicer2, A. Perales1
1Hospital Universitario la FE, Valencia, Spain; 2Hospital Universitario Dr Peset, Valencia, Spain; 3IVI, Valencia, Spain
Objective: The VEGF (vascular endothelial growth factor) ligands and receptors are crucial regulators of angiogenesis. Soluble vascular endothelial growth factor receptor 1 (sFlt-1) wich antagonizes VEGF has been implicated in the pathophysiology of abnormal angiogenesis. The purpose of this study is to compare the expression of VEGF complex from normal pregnancies with pregnancies with putative abnormal placentation: preeclampsia or single umbilical artery (SUA).
Methods: This prospective study included 45 healthy pregnants women, 41 with preeclampsia and 13 with SUA. Maternal plasma samples were collected at 2nd and 3rd trimester, also before delivery. At birth, umbilical artery and vein plasma was obtained to measure VEGF system (free VEGF, VEGF soluble receptor Flt-1, total VEGF). A p < 0.05 was considered significant.
Results: In preeclamptic pregnancies, sFlt-1(maternal, fetal artery and vein) is higher than in healthy pregnancies (442.56 ± 34.47 vs. 254.61 ± 21.03, 237.07 ± 56.24 vs. 75.58 ± 9.28, 242.45 ± 71.21 vs. 86.25 ± 13.85) respectively p < 0.001. No differences were found in Free and Total VEGF. In contrast SUA sFlt-1 was not different than normal pregnancies (maternal and fetal), whereas SUA pregnancies plasma free VEGF (maternal, artery and vein) is lower than the normal ones (56.23 ± 8.5 vs. 113.87 ± 6.8, 41.22 ± 8.9 vs. 128.49 ± 8.56, 37.53 ± 7.62 vs. 128.21 ± 8.4) p < 0.001 respectively.
Conclusions: This data suggest that the increase in sFlt-1 in Preeclampsia could mediate the impaired placentation and in SUA pregnancies the decrease in free VEGF reflected a decreased placental vasculogenesis.
P-02-007 Somatic parameters in relationship to cord blood leptin concentration of newborns from nondiabetic and diabetic mothers in pomeranian region
J. Wojculewicz1, H. Jasiel-Wojculewicz2, P. Krygier1, J. Szczapa1
1Neonatal Department Medical University, Gdansk, Poland; 2Department of Hypertension and Diabetology Medical University, Gdansk, Poland
Leptin is one of the most important hormone regulating body mass and energy usage. Its concentration increases in response to prolongated hyperinsulinaemia. In newborns, leptin level is stricltly connected with birth weight. In adults high leptin concentration occurs in obese subjects.
Aim: To estimate leptin concentration in umbilical cord blood in newborns born between 01.01.04–30.06.05 in Neonatal Department Medical University of Gdańsk from healthy and diabetic mothers.
Objective: The cohort of 59 newborns and their diabetic mothers (group 1) and 123 newborns and their healthy mothers was analysed.
Methods: Leptin concentration and antropometric measurements were taken in newborns. BMI was estimated in all women in the end of pregnancy.
Results: There were no significant differences between leptin concentration in newborns from both groups (14.9 + 11.7 vs. 13.7 ng/ml + 9.6). In macrosomic newborns (≥4000 g) from the first group (n = 16) the average leptin level was 20 ng/ml + 14.8. In the second group this value was 21.0 ng/ml ± 12.8 (NS).There was no significant differences between the average body mass and length at the birthtime (3617.2 + 549.3 i 3514.6 g + 462.9 and 54.2 + 3.3 i 54.8 cm + 2.7). Taking into consideration children from the first group we stated that the leptin level significantly differed between newborns delivered by mothers with diabetes t1 (before pregnancy) (N = 21) and with gestational diabetes (N = 38) (19.1 + 15.7 vs. 12.3 ng/ml ± 8.0). There were no differences in body mass. The average BMI in diabetic mothers was 30.4 + 4.5 and was significantly higher than in healthy women 27.1 + 3.2.
Conclusions: There was no differences in leptin concentration, body mass and length in both groups of newborns. We confirmed the difference in leptin level according to duration of diabetes in mothers. Basing on this conclusions we suggest that newborns' leptin concentration depends not only on their birth weight and body fat.
P-02-008 AB0 fetomaternal compatibility: risk for massive fetomaternal transplacental hemorrhage
Z. Zizka1, P. Calda1, T. Fait1, L. Haakova2, J.E. Jirasek2
1Department of Obstetrics and Gynecology, 1st Faculty of Medicine, Charles University, Prague, Czech Republic; 2Institute for the Care of the Mother and Child (UPMD), Prague, Czech Republic
Objective: Massive fetomaternal transplacental hemorrhage endangers the fetus (newborn) by massive anemization. A large transfer of blood is common in the 3rd trimester. The cytotrophoblast disappears, the syncytiotrophoblast becomes thinner and the vessels in the terminal villi come into intimate contact with the maternal blood in the intervillous space. Our aim was to determine whether AB0 compatibility puts the fetus at greater risk of severe fetomaternal hemorrhage.
Methods: We evaluated eight cases of severe fetomaternal transfusion during a 4-year period. For diagnosis we used the classic Kleihauer-Betke test and for quantification modern flow cytometry method. Further, we studied the blood group compatibility between the fetus and mother and the perinatal outcome.
Results: The incidence of adverse outcomes following transplacental hemorrhage was 75% (6 of 8). There were two perinatal deaths and four infants were affected with post-hypoxic damage. In 7 of the 8 cases there was AB0 compatibility between the fetus and the mother. One case of incompatibility was mild and had a good perinatal outcome.
Conclusions: On the basis of our results, we presume that the risk of severe fetomaternal hemorrhage is significantly decreased in the case of AB0 incompatibility between the fetus and mother. During contact of fetal and maternal blood at the level of placental microcirculation there is immediate agglutination with closure of pathological connections. Due to the very poor perinatal outcome, in the case of a single severe anemization of the fetus we recommend considering resuscitation in utero by intrauterine transfusion.
P-02-009 First trimester papp-a is a predictor of adverse pregnancy outcome
L. Krofta, I. Kucerova, H. Stefanovicova, S. Baresova
Institute for the Care of the Mother and Child, Prague, Czech Republic
Objective: Previous studies have shown an association between low first trimester PAPP-A and development of pregnancy complications. The aim of this study was to evaluate association between low levels of PAPP-A with the adverse pregnancy outcome.
Methods: The study included singelton pregnancies who underwent combined first trimester screening using PAPP-A, free beta hCG and nuchal translucency at 11–13+6 weeks gestation. Patients with chromosome abberations were excluded. The incidence of adverse pregnancy outcomes: a) fetal growth restriction, b) pregnancy induced hypertension, c) intrauterine fetal demise, d) placenta abruption, e) spontaneous miscarriage, f) pretarm labour were evaluated according to PAPP-A MoM levels.
Results: During the study period 1392 patients undervent combined first trimester screening. Pregnancy outcome was available for 1297 (93.2) women. Of these 18 had chromosomal aberations and 16 structural deviations. Of the remaining 1263 patiens pregnancy complicationsn were observed in 116 (9.2%). Patiens with PAPP-A ≤ 0.25 MoM had significantly higher rates of fetal growth restriction (p = −.044), pregnancy induced hypertension (p = −.005) and intrauterine fetal demise (p = −.0001).
Conclusion: Materna serum PAPP-A at 11–13+6 is significantly lower in adverse pregnancy outcomes.
This study was supported by the internal Grant Agency of the Ministry of Health of the Czech Republic.
P-02-010 The assessment of selected plasma free amino acids in preeclampsia
A. Haratym-Maj1, M.B. Wawrzycka2, B. Wawrzycki3
1Institute of Agricultural Medicine, Dept. of Pathology, Lublin, Poland; 2State Gynaecological and Obstetric Hospital, Maternal Unit, Lublin, Poland; 3School of Medicine, Lublin, Poland
Introduction: Many recent studies suggest that endothelium-dependent vascular relaxation is markedly impaired in preeclampsia, and a decreased nitric oxide NO bioavailability seems to be a central mechanism for this endothelial dysfunction. The amino acid arginine has been identified as precursor for NO synthesis. It was shown that reduced arginine availability may limit NO production. Even in the absence of extracellular L-arginine, the endothelium can resynthesize this amino acid from L-citrulline. L-glutamine is structurally similar to L-citrulline thus it is speculated that L-glutamine can inhibit L-citrulline transport in endothelial cells.
Aim: To compare plasma free amino acids levels between healthy pregnant women and those with preeclampsia.
Materials and Methods: The mean plasma levels of glutamine, arginine, and citrulline and ratio of L-citrulline to L-arginine, which reflects NO production was measured in maternal plasma samples from 20 pregnancies between 36 and 40 weeks gestation and compared with those found in matched samples. Plasma amino acids measurements were performed using ion exchange chromatography on an Ingos AA400 amino acid analyzer. Results are expressed as mean ± SEM. Values of P < 0.05 were considered to be statistically significant.
Results: The mean plasma level of L-glutamine was significantly higher in pregnant women with preeclampsia compared to healthy pregnant women. No significant changes were observed in L-citrulline levels and the ratio of L-citrulline to L-arginine, which reflects NO production, were slightly lower in women with preeclampsia than in controls. Sera from women with preeclampsia had higher L-arginine concentrations compared with healthy pregnant controls.
Conclusions: L-Glutamine may play a regulatory role in the biosynthesis of NO by its influence on availability of arginine for NOS.
P-02-011 Idiopathic non-immune hydrops fetalis – case report
I. Kucerova, J. Kucera, V. Cunat, L. Krofta
Institute for the Care of Mother and Child, Prague, Czech Republic
Background: Nonimmune hydrops fetalis is characterized by abnormal fluid accumulation in two or more fetal serous compartments together with generalized soft tissue edema without any identifiable circulating antibody to red cell antigens. Etiology is unknown in 20% of cases.
Case Report: 28 year old gravida I para I was referred to our institution in 31th week of gestation. Ultrasound examination was made on request. Fetal biometry corresponded to one week younger pregnancy. Extreme fetal cardiomegaly with tricuspidal regurgiation (CTI 0.6), pericardial effusion and ascites were observed. Doppler parameters (PSV MCA) were suggestive of severe fetal anemia. No other abnormalities were found. Amount of amniotic fluid was normal. Admission with subsequent cordocentesis and fetal transfusion was offered to the family. Induction of fetal lung maturity was initiated by steroids. Pregnancy was terminated by acute cesarian section indicated by reason of fetal hypoxia detected by CTG. Male newborn was delivered with Apgar score 5-4-6 and normal umbilical cord acid base analysis. Ventilatory support with extremely high setting was needed to maintain normal blood gases during first hours of life. Circulatory support by catecholamines and volume administration was required during first days of life. Ventilation was adversely influenced by ascites. Echocardiography revealed extreme cardiomegaly which resolved during three weeks. Severe fetal anemia was confirmed postnatally. No underlying reason for severe fetal anemia was found during subsequent laboratory testing. Baby recovered without having further severe complications. No developmental abnormalities were found during follow-up so far.
Conclusion: Non-imunne hydrops is a severe condition associated with high neonatal mortality and morbidity. Long term prognosis is influenced by underlying etiology and gestational age at the time of hydrops onset.
P-02-012 Prospective study of 24 hour blood pressure behavior in second and third trimester of uncomplicated and complicated by hypertension pregnancy
P. Korszun, G.H. Breborowicz
Department of Perinatology and Gynecology, University School of Medical Sciences, Polna, Poznan, Poland
Objective: This prospective study was to describe of circadian pattern of non-invasive ambulatory monitored blood pressure during the second and third trimester of pregnancy in clinically healthy women and in pregnant women who developed gestational hypertension.
Methods: The 24 h monitorings were performed in 372 pregnant women. In 215 of them gestational hypertension was diagnosed. All patients were divided to 5 equal 4 weeks periods groups between 21 and 40 week due to gestational age. During this investigation systolic and diastolic blood pressure, mean arterial blood pressure and maternal heart rate were measured. The 24 h BP monitorings were divided in to two periods, daytime (6:00 a.m. to 11 p.m.) and nighttime (11:00 p.m. to 6:00 a.m.). The mean diastolic and systolic daytime BP, mean systolic and diastolic nighttime BP, day/night BP ratio and SD were calculated for each group of patients. The distributions of these parameters were then statistically compared with normal reference values and for these two groups (normotensive and hypertensive) according to gestational time.
Results: We found significantly higher systolic (Mean SBP) and diastolic (Mean DBP) BP in day and nighttime in patient with hypertension. The MAP significantly increased in both day and nighttime as well, if compared to normotensive pregnant women. There were no significant differences of HR in case of gestational age.
Conclusion: Standardized 24-hour BP monitoring during pregnancy allows quantitative and qualitative evaluations of the hypertensive status.
Keywords: Pregnancy, hypertension, blood pressure (BP), mean arterial pressure (MAP), 24 hour ambulatory blood pressure monitoring (ABPM)
P-02-013 White coat effect and hypertension in pregnant women
P. Korszun, G.H. Breborowicz
Department of Perinatology and Gynecology, University School of Medical Sciences, Polna, Poznan, Poland
Objective: The aim of the study was to determine the prevalence of white coat effect among hypertensive pregnant women. Management was based upon standard sphygmomanometric recordings and 24 hours ambulatory blood pressure monitoring (ABPM).
Methods: Prospective experimental studies assessing the presence of a white coat effect. Population – 152 hypertensive pregnant women in the second half of their pregnancy admitted to hospital for management of their hypertensive disorders. Routine sphygmomanometric blood pressures were recorded by midwives in the ward and awake blood pressure recordings were averaged. These blood pressures were compared with average awake blood pressures recorded by 24 hours ambulatory blood pressure monitor (ABPM) (Accutracker Medilog Dx). White coat hypertension was defined as an average sphygmomanometer blood pressure ≥140 mmHg systolic and/or ≥90 mmHg diastolic with awake ABPM average blood pressure within the normal range for ABPM-derived blood pressures in pregnancy, according to gestation. White coat effect was the difference between average sphygmomanometer blood pressure and average awake ABPM-derived blood pressure. The clinical management was based upon routine sphygmomanometer recordings and to ABPM data. Main outcome measures – prevalence of white coat effect; with ≥20 mmHg systolic and/or ≥10 mmHg diastolic.
Results: Systolic white coat effect ≥20 mmHg was found in 19% and 16% had diastolic white coat effect ≥10 mmHg (P < 0.05). There were differences in maternal or fetal outcomes between women pregnancy induced hypertension and with a white coat effect.
Conclusions: White coat effect frequently occurs in mildly hypertensive pregnant women. Application of ABPM to identify a white coat effect in women presenting with hypertension in the second half of pregnancy is very useful diagnostic method.
P-02-014 Fetal fibronectin in cervico-vaginal secretion: could it be used as a predictive marker for labor induction success?
M. Theodora, N. Papantoniou, G. Daskalakis, A. Antsaklis
Maternal Fetal Medicine Unit, Athens, Greece
Objective: To determine whether the presence of fetal fibronectin in cervico-vaginal secretions at the time of induction of labor could be used as a predictive marker of successful induction of labor.
Material and Methodology: Cervicovaginal secretions were tested for presence of fetal febronectin prior to induction of labor, in 67 women with singleton term and post term pregnancies who were admitted in our unit from August 2004 until December 2005.
Results: The mean age of the examined women was 27.8 years (16–42 years). 74.2% of them were nulliparas. The overall caesarean rate was 27.3%. The mean gestational age was 40 + 2 (38–42). In 83.3% these cases cervix was unfavourable (BC ≤ 5).
Fetal fibronectin was detected in the cervico-vaginal secretion in 41 (62.1%) cases.
In 76% of the cases cervix was unfavorable (BC < 5).
In cases with positive fetal fibronectin vaginal delivery was achieved within 24 hour in 83%. The difference between the negative fFN group and the positive fFN group delivering vaginally was statistically significant (p = 0.01).
In 62% of fFN positive cases vaginal labor commenced within 6 hours after vaginal insertion of one prostaglandin pessary. In 10 cases a second pessary was needed and four cases had delivered by caesarean section. Oxytocin augmentation was need in 9 cases (21%) with positive fFN and vaginal delivery.
In the negative fetal fibronectin group vaginal delivery was achieved in 56%. In three cases labor commence after using one prostaglandin pessary. Twenty one (21) women (80%) needed a second pessary and 11 of them had caesarean section. Oxytocin augmentation was needed in 50% of negative fetal fibronectin group women who delivered vaginally.
Conclusion: The presence of fetal fibronectin seems to be a predictive marker for shorter and easier labor induction in our study. Moreover the presence of fFN in all cases with bishop scores <5 was predictive for successful labor induction.
P-02-015 Ultrasound biometry and iugr in risk population
S. Raspopovic, V. Miketic, A. Haliti
Department of Gynecology and Obstetrics, Clinical Centre of Montenegro, Krusevac bb, Podgorica, Yugoslavia
Objective: The purpose of this study was to evaluate sonographic biometry parameters – biparietal diameter (BPD) and abdominal circumference (AC) in determination of intrauterine growth restriction (IUGR) in a female population with chronic diseases – risk population.
Methods: Two groups of pregnant women analyzed: a) experimental N = 50 (chronic diseases present – pregnancy induced hypertension (PIH), heart and kidney diseases), and b) control group N = 50 from healthy population. Both groups underwent ultrasound measurements of biometry parameters (BPD, AC) beginning from 20th week of gestation (GW).
Results: IUGR was detected in 47 (84%) pregnant women from experimental group and in 6 (12%) from control group. There were no significant difference in socio-economic status, parity and age of all pregnant women. Hypertension and proteinuria were found in 66% and oedema in 78% women from experimental group. There were no significant difference in BPD and AC measurements in experimental and control group (p > 0.05) but AC values were higher in control group. As AC was the most sensitive parameter for IUGR detection with lower values (−10%) in experimental group, beginning from 24–26 GW. Differences in BPD measurement in experimental and control group are evident later, from 30–32 GW. Significant differences (p < 0.001) in BPD and AC measurements compared to GW were estimated, especially AC values.
Conclusion: IUGR is a consequence of a lot of different diseases, every each with its own patophysiology, with significant negative influence to perinatal morbidity and mortality. Determinating risk population and intensive surveilance of these pregnancies is very important. There is no answer about correlation between prenatal and childhood growth, and influence of IUGR on postnatal development. The mystery of reproductive biology is IUGR genesis.
P-02-016 Ultrasound and biochemical second trimester screening – prediction of iugr and other obstetric complications
D. Smetanova, E. Kulovany, D. Stejskal
Institute of Medical Genetics GENNET, Prague, Czech Republic
Introduction: Elevated levels of maternal serum alpha-fetoprotein (MS-AFP) in the second trimester indicate fetal abdominal wall defects (AWD) or neural tube defects (NTD). It is known that other obstetric complications like threatened abortion, premature labor, preeclampsia, IUGR, placental abruption or SIDS are associated with this finding as well. One of the reasons of MSAFP elevation is the malfunction of the fetoplacental unit caused by placental vasculopathies due to inherited or acquired maternal trombophilia.
Material and Methods: 121 patients with MS-AFP values more than 2.5 multiples of median (MoM) were examined between 1.1.2005–31.12. 2005. If morphological anomalies and multiple gestation were excluded by ultrasound scan, trombophilic mutations (Factor V Leiden – FVL, Factor II – FII and MTHFR 677 and MTHFR 1298), homocysteinemia and antiphospholipid antibodies were assessed. Uterine arteries blood flows were evaluated at 16–18 week of gestation and at 20–22 week of gestation scans. If the pulsatility index was more than 1.6, blood flow in umbilical arteries was evaluated at 20–22 week scan. Then in four week interval till 32nd week ultrasound scan evaluating amniotic fluid volume, placental and fetal circulation (PI in umbilical artery (UA), ductus venosus (DV) and medial cerebral artery (MCA)) were evaluated. Blood pressure and urine sample was examined as well.
Results: Trombophilic mutations (FVL or FII) were found in 8.5%, IUGR in 7%, preeclampsia in 1.5% and premature labor in 1.5% cases with elevated MS AFP in the second trimester. Low birth weight infants were delivered in 2.5% of cases.
Conclusion: Potential or clinical obstetric complications were found at 20% pregnancies with elevated MS-AFP. Early detection of these complications could contribute to the improvement of perinatological results.
P-02-017 Ultrasound finding of ovarian cystic formation in pregnancy – should we really not to follow up? A Case report
M. Hrehorcak, H. Robova, R. Vlk, M.G. Halaska, L. Rob
Obstetrics and Gynecology Dpt., 2nd Medical Faculty, Charles University, Prague, Czech Republic
Ultrasound finding of cystic mass in pregnancy is quite a common finding. Studies showed that association with malignant disease is extremely rare. There is ongoing discussion about the need to follow up the patients with accidental finding.
A case report of rare malignant endodermal sinus tumor diagnosed in early pregnancy is reported. 34 G3P2 presented to her gynecologist at 10th week of pregnancy, cystic formation was seen on ultrasound with negative tumor markers. Only routine follow up was recommended. Triple test in 16th week showed elevated levels of MS-AFP (13 856 IU/L).The patient was send to our referral prenatal diagnosis clinic due to test positivity. Normal fetal anatomy was found, but irregular multilocular cystic mass on the left side measuring 13 × 10 cm with central solid part was diagnosed. RI 0.56, PI 0.66. High levels of MS-AFP suggested malignant germ cell tumor of the ovary. Patient underwent laparotomy at 21w4d. Frozen section showed malignant tissue. Infracolic omentectomy and adnexectomy was performed. Final histopathological classification was malignant pure yolk sac tumor of the ovary. Four courses of chemotherapy were administered and delivery was planned at 34w 4d. Cesarean section with staging was performed (peritoneal washing, paraaortal and pelvic lymphadenectomy, hysterectomy and contralateral salp ingoophorectomy). Infant weighting 1980 g was delivered, AS: 7–8–9. No signs of spread on histology. Another 3 courses of chemotherapy were administered. Newborn required C-PAP for 3 days; anemia requiring blood transfusion was diagnosed (hgb 128 g/l). Pediatric, neurological and laboratory findings were normal in 1st and 2nd year.
Careful attention should be paid to the final decision about the follow up of the pregnant patient with irregular finding on the ovaries during routine scans. Although malignant disease is a rare event; other consideration (such as appearance of the tumor, and possibly the biochemical markers) should be taken into account.
P-02-018 Cardiac anomalies as a perinatal issue within tuzla canton region (BiH)
E. Nevacinovic, Z. Fatusic, F. Skokic, I. Serak, G. Bogdanovic, G. Grgic
UKC Tuzla OB/GYN Clinic, Trnovac bb, Tuzla, Bosnia and Herzegovina
Cardiac anomalies currently represent a big issue in perinatal medicine.
Objective: To show frequency of congenital cardiac anomalies at material available within the Clinic for gynecology and obstetrics in Tuzla in period from 1.1.1996 to 31.12.2003.
Methods: Through retrospective study during eight year period, frequency of congenital cardiac anomalies has been tested, as well as types of certain anomalies, and quality of antenatal protection and age of mothers who delivered babies with congenital anomalies. Obtained results have been processed by standard descriptive statistic methods.
Results: Within the analysed period from 1.1.1996 to 31.12.2003, 647 newborns have been delivered with some of congenital anomalies, of which 143 with congenital cardiac anomalies, so that the incidence rate of these anomalies is 1:289 and prevalence 3.45/1000 of liveborns. We have registered the most often septum ventriculi defect at 26.6% newborns, followed by septum atria defect at 23.7% newborns, while other found cardiac anomalies were much more seldom. Average age of mothers who delivered newborns with congenital cardiac anomalies is 30.4 ± 7.15 and is close to the age of mothers in tested group. Antenatal protection is insufficient, over 20% of mothers who delivered newborns with congenital cardiac anomalies did not have a single control during the pregnancy, while optimal number of examinations in tested group was done by only 8% of them.
Conclusion: Prevalence of congenital cardiac anomalies is similar to the prevalence rate in Croatia, although lower in comparison with other EUROCAT member countries, which might be explained by better registration and diagnostic in developed European countries, as well as still insufficiently developed antenatal protection.
Keywords: Congenital cardiac anomalies, incidence rate, antenatal protection
P-02-019 THE Role of risk factors in gestational diabetes screening
I. Spalova2, D. Bartaskova1, R. Vetesnikova-Koubova1
1Motol Hospital, Prague, Czech Republic; 22nd Medical Faculty, Charles University, Prague, Czech Republic
Introduction: An estimated 2–3% of all pregnancies in our population are complicated by gestational diabetes (GDM). Controversies still exist regarding screening, clinical management and infant outcomes.
Objective: Study design: In our study we retrospectively analysed: 1) the influence of risk factors on GDM screening, and 2) the influence of GDM screening on fetal outcome.
Results: There were 1022 pregnant women enrolled in the study. Only 482 (48%) of them were screened for GDM. But according to the recommendations of the U.S. Preventive Services Task Force 84% of women were at risk. There was no relation found between GDM and screening and risk factors. In the subgroup of women with a positive family history of DM (493 women, 48%) only 259 (52%) were screened. In some women there was a cumulation of risk factors. But even women with 3 risk factors (75 women, 7% of the whole group) were not screened more carefully. There were 12 babies (1.17%) born with perinatal complications directly linked with diabetes in pregnancy. Only two of these babies were born to women with a previously diagnosed GDM. This is a statistically relevant difference.
Conclusions: In our study population only about half of the pregnant women were screened. There was no relation between GDM screening and risk factors. Most of the infants (10/12) with perinatal complications were from not screened pregnancies.
P-02-020 Type-1 diabetes mellitus and prenatal midtrimester screening results
M. Ivanisevic, J. Delmis, D. Bljajic, N. Ljubas, D. Koraljka
Department of OB/GYN, Zagreb, Croatia
Objective: The results of studies in type-1 diabetes mellitus pregnant patients (type-1 DM) for mid-trimester distribution of serum multiple of the median (MoM) concentrations of alpha-fetoprotein (AFP), unconjugated estriol (uE3) and human chorionic gonadothropin (hCG) are often conflicting.
Aim: This study investigated the relationship between type-1 DM and maternal serum levels of AFP, uE3, and hCG.
Study Design: The serum markers AFP, uE3 and hCG during second trimester in 25 pregnant women with uncomplicated and well controlled type-1 DM have been compared with 327 healthy controls.
Methods: Competitive radio immunochemical procedures (2nd trimester Amerlax-M, Ortho Clinical Diagnostics, USA) were used. Serum markers were expressed as MoM concentration derived from the control samples, corrected for maternal weight. Gestational age was calculated by the last menstrual period (LMP) and verified by ultrasound not later than 10 weeks after LMP. Regression functions were used for adjustment of serum levels for weight. Mann Whitney test was used to calculate the statistical significance between two studied groups.
Results: Mean maternal weight in controls was 68.25 ± 10.31 kg, and in type-1DM group 72.16 ± 13.12 kg (p = 0.3). There were no significant differences in the distribution of hCG, AFP and uE3 between these two cohorts. All three markers AFP, uE3 and hCG levels in well controlled type-1 DM pregnant patients were lower but not statistical significant when compared to the healthy controls (). All pregnancies had favourable perinatal outcome.
Table I. MoM and mean ± SD values of hCG, AFP and uE3 after adjustment for maternal weight in all type-1 DM pregnat patients and controls.
Conclusions: In centres which offer appropirate medical facilities to their type-1 DM pregnant patients and reach optimal preconceptional and during pregnancy blood glucose surveillance, general adjustment of AFP, uE3 and hCG except for weight are no longer necessary.
P-02-021 Blood glucose profile comparison between gestational diabetes and pregnants with abnormal glucose challenge test
A. Kafkasli1, S.A. Cikim2, E. Selcuk3, Z. Yucel1, Y. Ustun1
1Inonu University School of Medicine Department of Obstetrics and Gynecology, Malatya, Turkey; 2Inonu University School of Medicine, Department of Internal Medicine, Division of Endocrinology and Metabolism, Malatya, Turkey; 3Inonu University School of Medicine, Department of Family Medicine, Malatya, Turkey
Objective: The aim of this study is to compare the blood glucose profile and glucose intolerance in pregnants with abnormal glucose challenge test (AGCT) with gestational diabetics (GD).
Methods: Eighteen pregnant women with AGCT and 22 GD were enrolled into the study. A 50-g glucose challenge test was performed between 24–28 weeks of gestation. Gestational diabetes was diagnosed by 2-step approach using Carpenter-Coustan criteria. The women were evaluated for insulin resistance by using HOMA, QUICKI and ISOGTT equations. Blood glucose profile was evaluated by detecting fasting, pre-postprandial (3 times/day) and midnight capillary blood glucose levels.
Results: Maternal age (30.5 ± 4.4, 29.3 ± 4.6 respectively), parity and the pre-pregnancy BMI were similar in pregnants with AGCT and GD. The rate of pregnant women with high fasting and morning postprandial blood glucose levels were similar. In addition; the blood glucose levels were comparable in patients with high glucose values detected by daily profile in both groups. Also HOMA, QUICKI, ISOGTT values were similar in both of the groups as well.
Conclusions: Blood glucose levels were similarly high in AGCT group with GD by daily glucose profile. We may speculate that pregnant women with AGCT have similar glucose intolerance with GD and, have to be managed like gestational diabetics.
P-02-022 Quality of antenatal care under the assessment surveys of technology implementation in moldovan maternities during 2003 and 2004
P. Stratulat1, V. Berdaga2, A. Curteanu1, T. Caraush1
1Mother@Child HealthCare Institute, Chisinau, Moldova; 2UNICEF Representative Office in the Republic of Moldova, Chisinau, Moldova
Objective: Under the Quality Perinatal Services Promotion Program (2003–2007) there have been conducted two surveys aimed at assessing the quality of interventions in pregnancy, delivery and postnatal care in 16 Moldovan maternities.
Methods: Both studies were performed by two multidisciplinary teams, which had evaluated each maternity during a 2-day period. Data processing was realized using 12 questionnaires, recommended by WHO. The data on the technologies applied in antenatal care are based on the interviews with 199 mothers.
Results: The supervision of the physiologic pregnancy by the family doctors was higher in 2004 (77%) than in 2003 (49%). The 2004 women's interview revealed that the average number of visits to the family doctor was 7.5 in 2004. The share of women whose pregnancy was registered at an early stage in 2004 was higher (69%) than in 2003 (57.05%). The distribution of the “Medical Perinatal Card” among pregnant women (85%), the share of women who took it with them at the maternity (67%) and the level of its completion (56.4%) were higher in 2004 than in 2003. At the same time, in 2004 the gravidogram was filled out in fewer cards (28.3%) than in 2003 (46%). Comparing the rate of iron supplements intake (62% vs. 38%) and folic acid intake (23.2% vs. 13.6%) we notice that in 2004 these indicators were higher than in 2003. In spite of this, the length of iron supplements intake by pregnant women wasn't enough. 46.4% of respondents were aware of the danger signs in 2003 and 69% in 2004. As for women's awareness of appropriate actions in case of danger signs, 48% of women answered they will address to the contact person; 16% – will call the hot line, and 52% will come immediately to the health facility.
Conclusions: The antenatal care indicators have improved thanks to the continuous training of the primary health staff, introduction of certain interventions in the Single Package of Health Insurance, provision of enough perinatal cards. The drawbacks are related to the pregnancy counseling, short period of iron supplements intake, and low use of gravidogram.
P-03-001 Expression of oct-4, vimentin (vim), alkaline phosphatase (ALP) and CD29 in/on amniocytes from second-trimester amniocentesis
D. Stejskal1, J. Mucskova2, P. Trefil2
1Institute of Medical Genetics GENNET, Prague, Czech Republic; 2BIOPHARM, Research Institute of Biopharmacy and Veterinary Drugs, a.s., Jilove, Jilove u Prahy, Czech Republic
Objectives: To verify presence of “mesenchymal” stem cells (AFMSCs) antigens in/on amniocytes obtained from second-trimester amniocentesis.
Methods: After short term incubation in culture media, amniocytes were labeled intracellularly by anti OCT-4 monoclonal antibody using Cytofix/Cytoperm. Other surface antigens were labeled by standard procedures. Expression of investigated antigens in/on amniocytes was ascertained by flow cytometry.
Results: Intracellular expression of Oct-4 antigen was found in 76% of amniocytes. Double positive Oct-4/CD29+ expression was found at 37% amniocytes. CD29+/ALP+ and VIM+/ALP+ subpopulations were found at 21.5% respective 23% amniocytes. Our findings further support concept of second trimester amniotic fluid as a promising source of fetal stem cells for therapeutic purposes.
P-03-002 Is age alone still an indication for invasive prenatal diagnosis?
I. Dhaifalah, J. Santavy
Department of Medical Genetics and Fetal Medicine, Palacky University Hospital, Olomouc, Czech Republic
Objective: To investigate the effectivity of first trimester screening (FTS), age and other factors as an indication for invasive testing for prenatal diagnosis of aneuploidy.
Methods: A retrospective analysis of indications for invasive procedures and their effectivity in the group of women who underwent the (FTS) in our centre from 12/2004 to 9/2005. Women were offered the combined screening program by ultrasound and biochemical markers. Women with risk more than 1:300 for chromosome 21, 18 or 13 trisomies, or those over the age of 35 years which is still an indication for invasive tests in the Czech Republic were offered genetic counseling and invasive testing. Chorionic villous sampling (CVS) or amniocentesis was then performed.
Results: Of the 1700 women who underwent FTS, 291 were over 35 years old and only 24 of them had a risk higher than 1:300. Detection rate of trisomy 21, 18 and 13 were 100%, (16 cases) with false positive rate of 4.6%. In the whole screened population 79 had a risk more than 1:300. The total number of invasive tests was 150. Amniocentesis was performed in 88 cases, 27 of them were done on the basis of screening with 3 aneuploidies detected. 36 amniocenteses were done for age and 25 for other indications. All had normal karyotype. 62 CVS were performed, in 52 CVS based on screening 13 aneuploidies were detected. In 5 cases for age and 5 others for family history the karyotype was normal.
Conclusions: Altogether 79 invasive procedures based on screening detected all 16 aneuploidies. Remaining 71 invasive tests (n = 41) for age and (n = 30) for other indications had a completely normal karyotype.
P-03-003 A prenatally diagnosed and postnatally confirmed case of with saldino-noonan syndrome
M.A. Guven1, S. Ceylaner2, M. Uzel3, A. Coskun1, G. Ceylaner2
1Kahramanmaras Sutcu Imam University, Dept. of Obstetrics and Gynecology, Kahramanmaras, Turkey; 2Zekai Tahir Burak Women's Health Education and Research Hospital, Dept. of Genetics, Ankara, Turkey; 3Kahramanmaras Sutcu Imam University, Dept. of Orthopedic Surgery, Kahramanmaras, Turkey
Objective: To present a prenatally diagnosed and postnatally confirmed case with Saldino-Noonan syndrome which is a member of lethal skeletal dysplasias called Short-Rib-Polydactly-Syndromes group.
Methods: Prenatal ultrasound and postnatal findings in a 28 year-old woman at 38 weeks of gestation are depicted.
Results: Prenatal ultrasound demonstrated depressed nasal bridge, short extremities, narrow thorax and short ribs, postaxial polydactyly, micromelia, deficient vertebral ossification and small ilia suggesting the diagnosis of a member of Short-Rib-Polydactly-Syndrome Type 1 ().
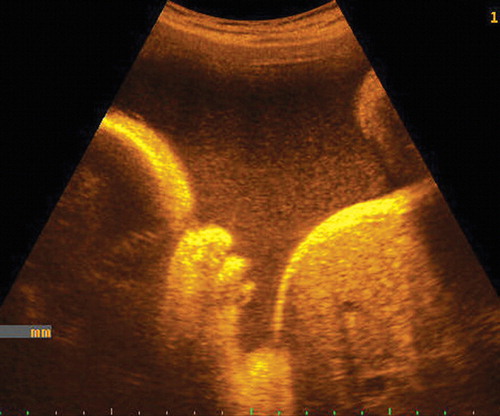
The fetus was delivered vaginally at 39 + 3 weeks after spontaneous onset of labour and weighed 3300 g. Postnatal phenotypic appearance confirmed the prenatal findings ( and ). Further, radiologic survey demonstrated short horizontal ribs, metaphyseal V shaped defects of long bones, trident and V shaped iliac corpora. Ossification was defective in the calvaria, vertebrae, pelvis, and bones of the hands and feet. Additionally, abnormal ossifications of the heels were seen.


Death from respiratory insufficiency secondary to pulmonary hypoplasia occured within the first few hours after birth.
Conclusion: Although there are very few prenatally diagnosed reports of this syndrome in the literature, our aim was to show the possibility of diagnosing Short-rib-Polydactly type 1 prenatally.
P-03-004 Expectations and pregnancy termination intentions in case of a fetus abnormality detection in a second trimester level ii ultrasound scan
A. Athanasiadis1, P. Polichronou1, K. Pantazis1, E. Asimakopoulos1, F. Tzevelekis1, T. Mikos1, K. Dampala1, I. Mpontis1
11st Department of Obstetrics & Gynaecology, Periferiaki Odos, Thessaloniki, Greece; 2Center of Prenatal Medicine, Agias Sophias, Thessaloniki, Greece
Objective: To investigate the thoughts, expectations and feelings of women presenting for second trimester Level II ultrasound scan.
Methods: We interviewed three hundred women, presenting consecutively for Second trimester level II ultrasound scan, using a self-completed questionnaire. The analysis was carried out using the SPSS program.
Results: The mean age of women was 31.2 years and the mean gestational age 21W (55% primigravidae). Detection of anatomical dysplasias (79.3%), assessment of fetal sex (51.7%) and detection of chromosomal abnormalities (68.3%) were the most common indications. The commonest patient expectations from the procedure were relief from anxiety (86%), detection of anatomical dysplasias (79%). In our population, in case of a fetal abnormality detection, 171/227 (75%) would opt for termination of pregnancy, 56/227 (24.7%) would decline while 60.5% of those declining, would do so for clearly personal reasons. There was significant difference between women declining and excepting a termination, regarding age (29.1 ± 3.6 vs. 31.86 ± 4.2 respectively, p < 0.001). One fourth (73/300) of the participants haven't yet decided if and under which circumstances they might terminate a pregnancy. 2/8 (25%) of those declining a termination due to mental retardation would indeed terminate a pregnancy in case of an obvious dysplasia. 137/219 (62.5%) estimated the scan's accuracy >70%.
Discussion: Women must be informed of the benefits and limitations of the examination before they underwent an ultrasound scan. In case of a fetus abnormality detection the consultation must be delicate but also prompt because of the large percentage of the patients denying a termination and because of the severalty of the fetus abnormality evaluation.
Keywords: Level II ultrasound scan, pregnancy, anxiety, prenatal diagnosis, fetus abnormality
P-03-005 Improvements in management of pregnancies at risk of x-linked diseases
G.C. Di Renzo, E. Picchiassi, G. Coata, L. Pennacchi, A. Fanetti, M. Centra
Dept. of Obstet. and Gynecology, Centre of Perinatal and Reproductive Medicine, University of Perugia, Perugia, Italy
Objective: The free fetal DNA present in maternal blood during pregnancy could be the tool for an early non invasive prenatal fetal gender determination: this fact might have great implication in the management of pregnant women carrying X-linked genetic disorders. Many authors have demonstrated the feasibility of the detection of Y-specific sequences in maternal blood since early gestation and showed that the sensitivity can reach 100% by using real time PCR. The aim of this study was to verify the sensitivity, specificity and predictive value of a new test for determination of fetal gender using PCR technology and maternal blood at first trimester of gestation.
Methods: 100 pregnant women between 10 and 12 weeks of pregnancy have been enrolled. Before blood sampling, written informed consent was obtained. After blood samples centrifugation, plasma DNA extraction was performed by using QIAamp Blood DNA minikit. The extracted DNA was analysed by real time PCR using TaqMan probes and primers specific for SRY gene.
Results: At the present, all samples tested have given results concordant with those obtained from ultrasonographic examination performed after 12 weeks of gestation. Therefore, these preliminary results show that this approach has a high sensitivity and specificity for fetal gender determination. The study will be completed when the babies will be born.
Conclusions: If these preliminary results will be confirmed, this approach could be used in clinical routine as prenatal diagnosis of fetal gender at first trimester of gestation. This prenatal genetic test performed in a non invasive way offers the advantage to know the fetal gender without any risks for the fetus and the mother and its performance in early gestation gives time to proceed with further investigations by using conventional invasive procedures.
P-03-006 Fetal brain mri findings in two cases of pyruvate dehydrogenase deficiency
E. Tsekoura1, C. Panousopoulou1, H. Michelakakis3, G.K. Brown2, M. Anagnostakou1
1B' NICU ‘Agia Sofia’ Children's Hospital, Thivon and Mikras Asias, Athens, Greece; 2Genetics Unit, Department of Biochemistry University of Oxford, Oxford, UK; 3Department Enzymology and Cellular Function-Institute of Child Health, ‘Agia Sofia’ Children's Hosp., Thivon and Mikras Asias, Athens, Greece
Background: Pyruvate dehydrogenase deficiency (PDHD) is one of the most common neurodegenerative inborn errors of metabolism. Symptoms start usually in infancy or in later childhood, but it may be present at birth. We present the fetal MRI findings in two cases diagnosed soon after birth.
Case 1: Female infant born at 37 weeks GA presented at birth with metabolic lactic acidosis, generalized seizures and dysmorphic features. Laboratory tests revealed increased levels of serum and CSF lactate, serum pyruvate, and serum ammonia. Diagnosis of PDHD was confirmed by low PDH activity in fibroblasts (0.1 nmol/mg protein/min, normal range 0.7–1.1) and sequencing of the E1 alpha gene mutation (base substitution G > A in exon 9). Fetal brain ultrasound and MRI at 25 weeks GA revealed ventricular dilatation, corpus calossum dysgenesis, and intraventricular diaphragms with cystic formations.
Case 2: Female infant born at 37 weeks GA presented at birth with generalized hypotonia. Investigations for inborn errors of metabolism revealed low PDH activity subunit gene mutation in a heterozygous female with 50% of cells expressing the mutant X chromosome. This was confirmed with monoclonal antibodies to E1 alpha and E2 subunits. Fetal brain MRI at 32 weeks GA revealed mild ventricular dilation and asymmetry, dilated third ventricle and intraventricular diaphragms with an isolated cystic formation in the frontal horns.
Conclusions: Both cases presented antenatally with abnormal fetal brain MRI findings. Fetal brain MRI could bring new insights in the early diagnosis of PDHD disorders.
P-03-007 Molybdenum cofactor deficiency in a neonate
T. Siahanidou1, H. Michelakakis2, C. Jacobs3, N. Verhoeven3, C. Acquaviva4, H. Mandyla1
1Neonatal Unit, First Department of Pediatrics, Athens University Medical School, Thivon & Levadias, Athens, Greece; 2Institute of Child Health, “Aghia Sophia” Children's Hospital, Thivon & Levadias, Athens, Greece; 3Metabolic Unit, Department of Clinical Chemistry, VU University Medical Center, Amsterdam, The Netherlands; 4Pediatric Biochemistry, Debrousse Hospital, Lyon, France
Molybdenum cofactor deficiency is a rare neurodegenerative inherited autosomal recessive disorder resulting in a lack of the activity of several oxidases, including sulfite oxidase. Clinical and brain imaging features of the neonatal form of the disease may resemble those of perinatal asphyxia. We report the case of a fullterm, male neonate, with molybdenum cofactor deficiency, who presented with high-pitch crying, poor feeding reflex and tremor immediately after birth; refractory convulsions occurred on day 3 of life. Electroencephalogram appeared asymmetrical and demonstrated a burst-suppression pattern. Brain MRI findings were suggestive of ischemic brain injury. Sulfite test in urine was grossly abnormal. Further urine analysis revealed excessive quantities of L-sulfocysteine and xanthine, while uric acid concentration was low. Plasma levels of L-sulphocysteine were increased, whereas uric acid was undetectable. Sulfite oxidase activity was absent in cultured skin fibroblasts. The early onset of symptoms in our patient and the lack of any effective treatment make the prognosis poor; however, prenatal diagnosis is possible in next gestations. We emphasize that molybdenum cofactor deficiency, as well as isolated sulfite oxidase deficiency, should be included in the differential diagnosis of unexplained neonatal seizures, especially in the presence of hypoxic-ischemic changes on neuroimaging studies.
P-03-008 Neonate with perinatal hypophosphatasia
V. Tsikrika, K. Gaitana, M. Goudesidou, A. Antonouli, E. Apazidou, E. Papadimitriou
University Hospital of Larissa, Mezourlo, Larissa, Greece
Hypophosphatasia is a rare inborn error of bone metabolism that in most cases is inherited as an autosomal recessive trait. It is characterized by decreased activity of the tissue non-specific alkaline phosphatase isoenzyme (TNSALP) and by great variability in its clinical expression. We describe the case of a premature boy with the perinatal form of the disease who was born after a 30 weeks uneventful pregnancy with a birth weight of 1450 g. On first clinical examination the bones of the cranium were unpalpable and the X-ray examination of the skull depicted no mineralization of the cranium bones. An abnormal mineralization of the long bones metaphyses was also depicted. The serum alkaline phosphatase of the baby was very low, 15 IU/L, and a low serum alkaline phosphatase was also found in both his asymptomatic parents. Now at the age of 18 months the most serious problem of the patient is respiratory insufficiency that needs mechanical ventilation. Diagnosis was confirmed by mutation analysis of the alkaline phosphatase gene. The patient was found to be a heterogygote for two mutations, the S164L mutation of paternal origin and the Y268X mutation of maternal origin. The father of the baby is Greek and the mother Italian from Trieste. Prenatal examination of the next child of the family revealed that he was an heterogygote for the maternal origin mutation only. This baby was also born prematurely after a 31 weeks gestation and his phenotype was normal.
P-03-009 The levels of serum free amino acids: L-Glutamine, L-Arginine, L-Citrulline, In women with intrauterine growth retardation
M. Wawrzycka1, A. Haratym-Maj2, B. Wawrzycki3
1State Gynaecological and Obstetric Hospital, Maternal Unit, Lublin, Poland; 2Institute of Agricultural Medicine, Dept. of Pathology, Lublin, Poland; 3School of Medicine, Lublin, Poland
Objective: It has been suggested that decreased nitric oxide (NO) production from endothelial cells is implicated in the pathophysiology of intrauterine growth retardation (IUGR). NO and L-citrulline are synthesized from amino acid L-arginine by NO synthase. In vitro study indicates that glutamine can limit arginine availability for NO production by inhibiting recycling of citrulline to arginine.The aim of this study was to compare maternal free amino acids levels between normal pregnancies and those with IUGR, in order to determine whether pregnancies with IUGR have lower nitric oxide synthesis.
Materials and Methods: The mean plasma levels of glutamine, arginine and citrulline and ratio of L-citrulline to L-arginine, which reflects NO production was measured in maternal venous plasma samples from 20 pregnancies between 37 and 39 weeks gestation and compared with those found in matched samples of women with uncomplicated pregnancy. IUGR was estimated by ultrasound examinations. Plasma amino acids measurements were performed using ion exchange chromatography on an Ingos AA400 amino acid analyzer. Results are expressed as mean ± SEM. Values of P < 0.05 were considered to be statistically significant.
Results: Our results show that concentration of glutamine was significantly increased in the plasma of patients with pregnancy complicated by IUGR. There were no significant differences in plasma concentrations of citrulline and arginine between the two study groups. Cit/Arg ratio showed a trend to decreased in pregnancy associated with IUGR.
Conclusions: Our results confirm previous observations that decreased nitric oxide production may be important in the pathophysiology of intrauterine growth retardation.
P-03-010 Prenatal diagnosis and its importance in treatment of the anomalies of gastrointestinal tract (git) in neonatal intensive care units, with the special insight into the anomalies of diaphragm – diaphragm hernia
R. Rudanovic1, S. Raspopovic2, D. Dakic1, M. Rudanovic1, Z. Micovic1, A. Bajmak2, D. Suhih1, A. Begovic1, M. Perosevic1, S. Zekovic3
1Children's Clinic, Krusevac BB, Podgorica, Yugoslavia; 2Clinical Center, Krusevac BB, Podgorica, Yugoslavia; 3Sanicard, Krusevac, Podgorica, Yugoslavia
Introduction: First clinical descriptions of GIT were given in XVII century and they are attributed to the names of Durstone and Macenzy. X-ray diagnosis and utilisation of contrast agents have recently provided for earlier detection of inherent failures, so that, thanks to prenatal diagnosis, modern neonatal intensive care and cure, and modern anestesis and surgery technique as well, the survival percentage of those patients is now nearly 100%.
Objective: Importance of early detection of (echography, amniocentosis, genetic counselling and prenatal therapy and laboratory diagnosis) anomalies of GIT and anomalies of diaphragm – impact onto adequate treatment and final outcome.
Method: Prospectous monitoring for four year period (2001–2005) of the frequency of the above mentioned anomalies at newborn children cured in Neonatology Centre.
Results for the above mentioned period: Total 2980 newborn children were under the cure. Total 50% of those children with the anomalies had joint anomalies, out of which 25% jeopardized life of patients and required urgent surgery intervention. According to our data, 21% out of total number of all anomalies refers to GIT anomalies. Half of those are anorectal anomalies, congenital anomalies, anomalies of heart and big blood arteries make 20%, urinary tract anomalies 10%, CNS anomalies 4%, while remaining 45% refers to other anomalies (respiratory tract, chromosomopathies, etc). Esolagus atresia in sample amounts to 5.7%, diaphragm hernia 0.5%, i.e. 1 in 1000 babies born alive or 1 in 1000 babies born dead.
In total sample, prematurus were 1.8 temporarius (hypotrophicus 4.4%).
Conclusion: Survival in the group of children with diaphragmal hernia is 96%, specifically in the group of children with highest percentage of prenatally determined diagnosis.
All the children were at mechanical ventilation and surgical treatment was made within 24 hours upon reception.
P-03-011 Arthrogryposis multiplex congenita: Report of 3 cases
B. Dane, M. Yayla, C. Dane
Haseki Education & Research Hospital, Department of Gynecology & Obstetrics, Division of Perinatology, Millet Caddesi, Istanbul, Turkey
Introduction: The term ‘arthrogryposis multiplex congenita’ (AMC) refers to multiple joint contractures present at birth. AMC is not a specific disorder but is the consequence of neurologic, muscular, connective tissue, and skeletal abnormalities or intrauterine crowding, which may lead to limitation of fetal joint mobility and the development of contractures.
Cases: We present 3 cases of AMC with different findings. The diagnosis was based on an abnormal fetal movement profile, in association with an abnormal position of the fetal limbs. The ultrasound features related to the “lack of movement” were: limb abnormalities (multiple contractures, clenched hands, clubbed feet), scalp edema, growth retardation, short umbilical cord, polyhydramnios, pulmonary hypoplasia, hypertelorism, camptodactyly, and micrognatia.
Discussion: The prognosis for AMC is related to the specific etiology. In some cases, the disease is lethal, and death occurs shortly after birth. Termination of pregnancy can be offered before viability. Confirmation of diagnosis after birth is important for genetic counselling.
P-03-012 An acardiac twining presented as placental mass
B. Dane, M. Yayla, C. Dane, F. Aksoy
Haseki Education & Research Hospital, Department of Gynecology & Obstetrics, Division of Perinatology, Millet Caddesi, Istanbul, Turkey
Introduction: Acardiac twinning is the most extreme form of twin–twin transfusion syndrome occurring in monzygotic twin pregnancies with monochorionic placentation. Data suggest a 50% mortality rate in the “pump” twin when the pregnancy is managed expectantly. The distribution of anomalies has led to the classification of four different morphologic types of acardiac twinning. ‘Acardius amorphous' is the fetus, which has no recognizable human form. We present a case of acardius amorphous, which was considered as a singleton gestation associated with an intraamniotic tumor.
Case: The case was referred at 18 weeks' gestation because of abnormal triple test. Serial ultrasound scans revealed a growing oval mass around the placenta (from 2 cm to 7 cm). Color Doppler flow mapping demonstrated arterial flow. Genetic amniocentesis revealed a normal karyotype. Tocolytic agents and therapeutic amniocentesis are used to tread preterm labor associated with hydramnios. At term there was no arterial flow in the mass and amniotic fluid volume was normal. Pathological examination showed a monochorionic monoamniotic placenta and an acardiac amorphous twin containing rudimentary tissues inside the body.
Discussion: Cessation of flow to the acardiac twin in our case was associated with a relative reduction in size, amnion volume and an uncomplicated neonatal course for the pump twin. It is likely that many such cases were never accurately diagnosed, resulting in the birth of a healthy infant and a small acardiac twin that could be missed among placental tissues. Postnatal examination of the placenta by suspected cases will show the real fetal/neonatal mortality rate of acardiac twinning.
P-03-013 Arnold-chiari malformation – spina bifida – case report
A. Haliti, V. Miketic
Department of Gynecology and Obstetrics Clinical Centre of Montenegro, Krusevac bb, Podgorica, Yugoslavia
Neural tube malformations involving the spinal cord and vertebral arches are referred to as spina bifida, with severe types of spina bifida involving protrusion of the spinal cord and/or meninges through a defect in the vertebral arch. Depending on the level of the lesion, interruption of the spinal cord at the site of the spina bifida defect causes paralysis of the legs, incontinence of urine and feces, anesthesia of the skin, and abnormalities of the hips, knees, and feet. Prenataly, neural tube defect is detectable on longitudinal ultrasound scanning by the loss of skin continuity. In a transverse view, a spina bifida appears as a U-shaped vertebra. Spina bifida is associated with the Arnold-Chiari malformation in 90–95% of instances. The cerebellar vermis, fourth ventricle and medulla are displaced caudally. Two characteristic sonographic signs of the Arnold – Chiari malformation are described – the “lemon” and “banana” signs.
Case Report: A 29-year-old G2P1, was examined by ultrasound at 29 weeks of gestation. There was no family history of congenital anomalies. The patient's antepartum course had been unremarkable. Ultrasound evaluation revealed a single fetus with biometry measurements compatible with 28/29 weeks of gestation. Morphological evaluation of the fetus revealed signs of spina bifida and Arnold Chiari malformation. The patient delivered a newborn at 39 weeks – postpartal analysis confirmed the ultrasound diagnosis.
P-03-014 Prenatal suspicion of crouzon syndrome
A. Torres, M. Perez, A. Hernandez, M. Mestre, M.D. Gomez, J.M. Lailla
University Hospital Sant Joan de Deu, Barcelona, Spain
Introduction: Crouzon syndrome is an autosomal dominant syndromic craiosynostosis characterized by premature closure of cranial sutures, exophtalmus, and midface hypoplasia. It is caused by multiple mutations in the fibroblast growth factor receptor 2 (FGFR2). The aim of this discuss are the clinical, radiographic features and management of the problems.
Case: A 33 years old multigravida woman without any antecedents comes to our medical center to get a pregnancy control.
The couple request an amniocentesis because the husband was been treated with chemotherapy for leukaemia two years ago. The result of the prove did not present any cromosomopathy.
The morphologic ultrasonography was realized at week 21. A little ventriculomegaly (10 mm) was found. For this reason multiples ultrasounds controls and a nuclear magnetic resonance were practiced and the only important anomaly that we found was polyhidramnios and light angular vertebras.
In the 35th pregnancy week she went in labour to hospital. We practiced an spontaneous vaginal delivery and after that neonatologists made an detailed exploration. They observed dysmorphic features, hydrocephalus newborn and choanal stenosis. All the tests suggested that the child may suffer the crouzon syndrome.
Discussion: The frequency of Crouzon syndrome is approximately 1 case in 25,000 childbirths. Although the transmission can be by autosomal dominant, the 30%–60% of the cases are from parents without family history. It is necessary to make a diferential diagnosis with similar cranioencephalics characteristics like Carpenter, Apert, Pfeiffer and others.
It is important to suspect the diagnosis antenatally because the adequate treatment should begin at the same moment of the birth.
P-03-015 Gastroschisis – mode of delivery
R. Vlk1, M. Hrehorcak1, I. Spalova1, M. Rygl2, J. Horak1, M.G. Halaska1, M. Cerny3
1University Hospital Motol, Department of Obstetrics and Gynecology, Prague, Czech Republic; 2University Hospital Motol, Department of Pediatric Surgery, Prague, Czech Republic; 3University Hospital Motol, Department of ObGyn, Neonatology Unit, Prague, Czech Republic
Objective: Gastroschisis is a typical paraumbilical defect of the abdominal wall. The optimal delivery mode for infants with gastroschisis remains controversial. Authors compared the obstetrical outcomes of infants born vaginally or by caesarean section.
Methods: We reviewed 21 cases of infants with gastroschisis delivered at the University Hospital Motol, Prague between 2000 and 2005. Data were collected retrospectively by a review of records from the prenatal diagnosis unit, maternal, pediatric and surgery records. We excluded those cases of gastroschisis with aneuploidy or other lethal congenital anomalies (2 cases). Assessment included patient demographics, complications of labor, mean induction time by vaginally mode, respiratory distress of newborns, mortality, method of closure, number of surgeries, parenteral nutrition days, time to full feeding, and length of stay.
Results: Nineteen patients were studied, 10 were delivered by vaginal route and 9 by caesarean section. No difference was found between the vaginal and operative groups for perinatal complications, method of closure, number of surgeries, parenteral nutrition requirement, and length of hospitalisation. Trauma to the intestine was described in one fetus that was delivered by caesarean section. One newborn died few days after surgery for sepsis.
Conclusions: The routine use of caesarean section for infants with gastroschisis is not supported by our results since comparable outcomes were observed using either mode of delivery. Caesarean section could be a necessary intervention for fetal distress.
Supported by grant VZ FNM 00000064203/6202.
P-03-016 Drainage of isolated fetal renal cyst: a case report
L. Assis, A. Cohen, I. Martins, L. Martins, J. Correia
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
In utero expansion of renal cysts disturbs the nephrogenesis and may contribute to the abnormal development of the fetal kidneys. The authors report a case of a 23 week foetus who has been diagnosed a large cystic mass (26 × 45 mm) of the right kidney on a routine scan. There were no other morphologic abnormalities. A conservative approach was the initial option. At 29th week the cyst had grown up to 84 × 75 × 55 mm with signs of parenchymal compression. An ultrasound-guided drainage procedure was undertaken with aspiration of 120 cc of clear fluid. A cycle of betamethasone (12 + 12 mg IM) had been previously administrated and tocolityc therapy (transdermic gliceryl trinitrate) was prescribed 30 minutes before the intervention. No procedure-related complications occurred. Residual cyst dimensions were 10x10mm. Eutocic delivery of a male baby weighting 2980 g occurred at 37th week. No other abnormalities were apparent on clinical examination. One year follow up will be available by the time of presentation.
P-03-017 Campomelic dysplasia: A case report
C.L. Ciobanu1, G. Cristescu2, C. Anastasiu2, M. Moga2
1Obstetrics and Gynecology University Hospital, Brasov, Romania; 2Transilvania University, Brasov, Romania
Campomelic dysplasia is a congenital disorder characterized by development of abnormal curvature of the long bones, particularly from lower extremities, together with other skeletal and extraskeletal defects. The authors presents the case of a 26-year old diabetic woman without proper clinical folow-up of the pregnancy, who delivered a plurimalformated fetus which was prior diagnosed with campomelic dysplasia. The fetus died after 30 days due to respiratory failure and presented also malformations associated with sex reversal.
P-03-018 Idiopathic thrombocytopenic purpura in pregnancy: Clinical experience with maternal and neonatal outcome
S.J. Shin, S.H. Kang, S.S. Shim, S.H. Jung, S.W. Chang
Pocheon CHA University Pundang Hospital, Sungnam, South Korea
Idiopathic thrombocytopenic purpura (ITP) frequently occurs in young women. Consequently, clinicians often treat pregnant women who have a diagnosis or a history of ITP.
Aim: To be a help for development of clinical guidelines of obstetric ITP patients and infants. We observed 19 pregnant women with ITP from March 1996 through March 2005. Nineteen pregnant women with ITP gave birth to twenty two babies. Ten of the cases were diagnosed with ITP before pregnancy and twelve during pregnancy. During pregnancy, thirteen pregnant women received corticosteroid treatment, three high-dose immunoglobulin therapies. At the time of delivery, six pregnant women received high-dose immunoglobulin therapies and seventeen platelet transfusion. Ten deliveries were by vaginal route and twelve were by caesarean section. There were no obstetric complications. Four infants were born with platelet counts below the 150,000/μl. No infant showed any clinical signs of hemorrhage and there were no neonatal complications.
Conclusion: We found that mothers with ITP can successfully deliver healthy infants and that though maternal and fetal bleeding can occur such complications are uncommon.
P-03-019 Non-invasive fetal rhd and rhce genotyping from maternal plasma in alloimmunized pregnancies
M. Cerny1, K. Vesela2, K. Nekovarova3, R. Vlk4, I. Spalova4, R. Gerychova5, A. Hakenova6, Z. Rosenbaumova7, R. Schrollova8, P. Calda3, I. Hromadnikova2
1Neonatology Dept., 2nd Medical Faculty, Charles University Hospital Motol, Prague, Czech Republic; 2Cell Biology Laboratory, 2nd Medical Faculty, Charles University Hospital Motol, Prague, Czech Republic; 3Dept. of Obstetrics and Gynaecology, 1st Medical Faculty, Charles University, Prague, Czech Republic; 4Dept. of Obstetrics and Gyneacology, Charles University Hospital Motol, Prague, Czech Republic; 5Dept. of Obstetrics and Gynaecology, University Hospital Brno, Brno, Czech Republic; 6Dept. of Transfusion Medicine, University Thomayer's Hospital, Prague, Czech Republic; 7Dept. of Obstetrics and Gynaecology, Masaryk Hospital, Usti n/L, Czech Republic; 8Blood Bank, Charles University Hospital Motol, Prague, Czech Republic
Objective: In this prospective study, we assessed the feasibility of non-invasive fetal RHD and RHCE genotyping from maternal plasma samples of anti-D, anti-C, anti-c and anti-E alloimmunized pregnant women at risk of haemolytic disease of the newborn.
Methods: We analysed DNA extracted from maternal plasma samples in 150 pregnant women within 6th and 40th week of pregnancy by using real-time PCR and primers and probes targeted toward RHD (exon 7 and exon 10) and RHCE (intron 2, exon 2 and exon 5) genes. We correlated the results with serological analysis of cord blood.
Results: The sensitivity and the specificity of the assays reached 99–100%. We were able to detect paternally-inherited alleles from 6th week of pregnancy, however we have usually performed the assays from 10th week of pregnancy.
Conclusion: Detection of the presence of RHD gene, the C/c and/or E alleles of RHCE gene in maternal plasma samples is highly accurate and we implemented it into clinical diagnostic algorithm for pregnancies at risk for haemolytic disease of the newborn. The absence of RHD gene, the C/c and/or E alleles of RHCE gene in the current pregnancy excludes the risk of haemolytic disease of the newborn caused by anti-D, anti-C, anti-c and/or anti-E alloantibodies and brings the possibility to avoid invasive fetal-blood sampling.
This project was supported by MZO 00064203 and MSM 0021620806.
P-03-020 Rh hemolytic disease of the fetus and newborn in montenegro
S. Raicevic1, R. Rudanovic2, G. Rasovic3, S. Babovic1, A. Haliti1
1Clinic for Gynecology and Obstetrics, Clinical Centre of Montenegro, Krusevac b.b., Podgorica, Yugoslavia; 2IBD-Clinical Centre of Montenegro, Krusevac b.b., Podgorica, Yugoslavia; 3CT-Clinical Centre of Montenegro, Krusevac b.b., Podgorica, Yugoslavia
Objective: To determinate the meaning of Rh hemolytic disease of newborn in causing perinatal morbidity and mortality of newborn in Montenegro.
Material and Methods: With prospective method pregnancies of Rh negative women were followed in period 2000–2004, titer of antibodies were determinating and US parameters were followed. The outcome of this pregnancies was analyzed, way of delivery and appearance of HDN in neonatal period.
Results: There were 13,962 deliveries, while HBN at Rh incopathibilia is marked at 50 pregnancies (0.36%). Rh(D) incopatibilia was present in 42 cases (0.30%). Rh(c) incopathibilia in 3, Rh(e) incopathibilia in in 1, Rh(E) incopathibilia in 2 and Rh(C) incopathibilia in 2 pregnancies. US finding of fetal hydrops at two pregnancies, at 3 pregnant women hydramnion and at 3 pregnant women placenta with a look of “smash glass”. Pregnancies were interrupted in two Rh(D) incopathibile pregnancies, at which titre of antibodies was > 256 (512) in enzyme environment and US finding of fetal hydrops. Six pregnancies were finished before time and a rest at time. Hiperbillirubinemia at newborns was treated with phototherapy in42 cases, approximately five days, with Phenobarbital almost at all newborns. EST was given at 21 newborns and transfusion at 10 and REST at 4 neonates.
Conclusion: With good implementation of imunoprofilacsis of Rh0(D)-sensibilisation, usage of ABO and Rh0(D)-compatibil transfusions, frequence of Rh0(D)-antitbodies, thereby Rh0(D)-isoimunisation is in permanent decreasing. Beside that, HDN caused by Rh incopatibility still represent mean perinatal and neonatal problem.
P-03-021 Comorbidity in feto-fetal transfusion
J. Arnaez Solis, C. Ortiz-Villajos, L. Albert, L. Aybar, A. Alarabe, L. Sanchez de Leon
Mostoles Hospital, Madrid, Spain
Objective: To describe the comorbiditiy in the twin-twin transfusion syndrome in a 2nd level hospital during a one year period in 6 patients from a total of 2020 live.
Methods: Retrospective study with review of the clinical records of live newborns during 2005.
Results: From the three monochorial diamniotic twin gestations with twin-twin transfusion syndrome, there were five live newborns, four of them by vaginal delivery. One fetus died a few hours before the delivery despite normal findings in tests taken two days before. All newborns were preterm between 31 and 35 weeks of gestation. In one case with, a fetoscopic laser photocoagulation was performed at 22 weeks with progressive hydrocephalia afterwards in both twins until delivery. At birth, a weight difference of 25 to 30% between each pair of twins was detected. The recipient twins did not need partial exchange transfusion and only one of the donors needed blood transfusion. Other complications that developed were: renal failure (one of them required peritoneal dialysis and veno-venous hemofiltration), hypertrophic cardiomyopathy with hypertension due to the hypervolemic status, coagulopathy and thrombocytopenia; necrotizing enterocolitis.
Among the neurological complications there was a patient with craneofacial assimetry with seizures and grade I intraventricular hemorrhage; another with microcephalia and prosencephalia on magnetic resonance imaging and his twin brother developed progressive non communicating hydrocephalia in relation to fetus intraventricular haemorrhage.
Conclusions: 1) The twin-twin transfusion syndrome has a high morbimortality occasionally with severe neurological complications and intrauterine death. 2) Severe neurological complications were observed in the only case in which a fetoscopic laser photocoagulation was performed though not related with the technique but with a hyper/hypovolemic status.
P-03-022 Herpesvirus 6 vertical transmission with fulminant neonatal sepsis
J. Arnaez Solis, L. Aybar, M.J. Mestre, L. Albert, J.C. Tejedor, L. Sanchez de Leon, P. Puyol
Mostoles Hospital, Madrid, Spain
Objective: We report a case of human herpesvirus 6 (HHV-6) infection in a preterm newborn with evolution to death. The importance of HHV-6 as a pathogen in the neonatal period is unknown althoug the vertical transmission has been described together with the presence of the virus in the umbilical cord as well as in the genital tract.
Methods: Retrospective study with review of clinical records.
Results: Antecedents. A 24 year-old mother with cocaine abuse; 4 abortions. Negative TORCH serology; fetal ultrasound: oligoamnios and ascitis at 33 weeks of gestation. Meconium stained amniotic fluid. The baby was born at 34 + 6 weeks gestation by emergency caesarean section. Apgar 1/5/10 = 0/2/5. Resuscitation with intubation and drugs. Cord blood pH: 6.82. Birth weight: 1550 g. He was admitted at NICU and broad spectrum antibiotics were iniciated. Physical examination: hepatosplenomegaly. His general status deteriorated with DIC, refractory hypoxemia and hemodynamic failure, dying at 6th day of age. Blood culture was sterile.
The pathology findings were cholestatic hepatitis, interstitial pneumonitis without cytomegalovirus inclusions and multiple microhaemorrhages; the placenta showed chorioamnionitis. Liver and lung tissues cultures: negative for fungi, bacteria and virus. The HHV6 DNA was detected by PCR in lung and liver samples. Maternal serology showed a recent infection to HHV-6 with positive IgM.
Conclusions: 1) The pathology findings, maternal serology data and clinical evolution in the newborn are consistent with HHV-6 as the ethiology agent causing the death in this patient. 2) Although the role of HHV-6 in the neonatal period is unknown, a severe infection with fatal evolution may occur as in our case.
P-04-001 Caesarean section as a result of unsuccessful labor induction
S. Plesinac, D. Plecas, I. Babovic
Institute of Gynecology and Obstetrics Clinical center of Serbia, Belgrade, Serbia
Introduction: Induction of labor has always been a challenge for obstetricians.
Aim: To show the incidence of caesarean section during unsuccessfull labor inductions in 2004 at Institute of Gynecology and Obstetrics Clinical Center of Serbia.
Materials and Methods: The patients were divided in three groups. Group I included 81 patients whose labor was inducted with PGE1. Group II 210 patients where we used PGE2 and group III 44 patients where we used oxytocin.
Results: The most frequent indication for induction was prologed pregnancy (50%) and hypertension in pregnancy (11%). The average duration of labor was 8.6 hours in group I, 5.9 hours in group II and 10.4 hours in groupIII. Neonatal peripartal asphyxia was detected in 36% of newborns in group III, 8.6% in group I and 3.8% in group II. The incidence of caesarean sections was 13.5% in group I, 0.9% in group II and 87% in group III.
Conclusion: PGE2 still remains the most releable way of labor induction.
P-04-002 Impact of operative vaginal delivery on umbilical arterial pH
A. Puertas, M.E. Lopez-Moreno, M.D. Ruiz-Leon, S. Manzanares, M. Navarro, J.A. Miranda
Obstetrics and Gynecology Dpt. Virgen de las Nieves University Hospital, Granada, Spain
Objective: To assess differences in neonatal outcome based on arterial pH at birth by different operative delivery procedure (spatulas, forceps or vacuum extractor) and the influence of different indications on this outcome.
Methods: Retrospective study of clinical records of vaginal instrumental deliveries attended at Virgen de las Nieves University Hospital in Granada in a 2-year period (2003 y 2004). 6327 deliveries were analyzed and all selected study variables recorded (umbilical artery pH at birth, mode of vaginal and instrumental delivery and indication for obstetric procedure). 4942 women underwent spontaneous vaginal delivery, 472 forceps, 599 spatulas and 287 vacuum extractor.
Results:
Multiple comparison of arterial pH at birth show significative differences between all groups excluding forceps vs. vacuum.
Conclusions: Operative vaginal delivery led to newborns with a lower umbilical pH value than spontaneously delivered. Thierry spatulas deliveries showed the lesser decrease. These differences may be due to operative delivery indication because indication for spatulas was more frequently shortening of 2nd stage of labor, meanwhile were more uncommonly used in prolonged 2nd stage of labor and more uncommonly than forceps in potential fetal compromise.
P-04-003 Operative vacuum assisted deliveries – perinatal outcome in 453 cases
Z. Aleksov1, Lj. Ristic2, U. Radivojevic1, B. Milanovic1, Z. Puzigaca1, R. Nikolic1, V. Ivanovski1
1Clinic for Human reproduction, Mother and Child Health Care Institute, Belgrade, Serbia; 2Clinic for Gynecology and Obstetrics, Pristina, Serbia
Objective: To evaluate the risk of neonatal adverse outcomes in vacuum assisted (VA) singleton deliveries.
Methods: We conducted a prospective study that included 453 VA deliveries, during the period from 1996–1997 at Clinic for Gynecology and Obstetrics, Pristina.
Results: 310 deliveries (first group) were performed using 1–2 tractions and the duration of calotte application up to 5 minutes (68.5%). In 118 cases (second group) 3–4, tractions were used with the duration of calotte application of 10 minutes (26%), while in eight deliveries (third group) more than five tractions were needed and the duration of the calotte, application was greater than 10 minutes. Vacuum extraction failure was noted in 7 (1.5%) cases. In the first group 289 (93.2%) babies were born healthy, while in 21 cases (6.8%) different morbidity was noticed. In the second group there were 44 healthy babies (37.3%), and 74 (62.7%) with different morbidity. In the third group all newborns 18 (100%) suffered from different VA deliveries complications while nine children (50%) died. Severe asphyxia perinatalis and intracranial hemorrhages were seen in all mortality cases.
Conclusion: Inadequate technique of VA delivery and disregard of the three-traction rule leads to high perinatal morbidity and mortality rates.
P-04-004 Cefazolin vs. ceftriaxone for antibiotic prophylaxis in elective caesarean section
Z. Grujic1, M. Bogavac1, I. Grujic2, Lj. Milasinovic1
1Clinical Center Novi Sad, Department of Obstetrics and Gynecology, Novi Sad, Serbia; 2Health Center “Veljko Vlahovic” Vrbas, Serbia and Montenegro
Aims: Single dose preoperative administration of antibiotics is sufficient to prevent intra and postoperative infections in the parturients with no high risk for the development of infection.
Material and Methods: A prospective investigation comprised 36 healthy pregnant women at term planned for elective caesarean section vs. 8 non-pregnant women planned for gynaecological surgery. The 1st group of 18 pregnant women and 4 non-pregnant women were preoperatively administered ceftriaxone in a dose of 2 g, i.v., 10 minutes before the planned surgery. The 2nd group of 18 pregnant women and 4 non-pregnant women were preoperatively administered cefazolin in a dose of 2 g, i.v., 10 minutes before the planned surgery.
Results: The mean concentrations of antibiotics in the patients following the elective caesarean section were as follows: cefazolin-44.80 μg/l vs. ceftriaxone-22.75 μg/l. Six hours later, the concentration of antibiotic decreased: cefazolin-24.87 μg/l vs. ceftriaxone-13.23 μg/l which was still over the MIC for sensitive bacteria. The mean concentrations of antibiotics following gynaecological surgery in non-pregnant patients were as follows: cefazolin-30.06 μg/l vs. ceftriaxone-12.03 μg/l. Six hours later, the concentration of antibiotic decreased: cefazolin-17.39 μg/l vs. ceftriaxone-5.7 μg/l. The concentration of cefazolin was still over the MIC for sensitive bacteria. The mean concentrations of the administered antibiotics in umbilical cord were high (cefazolin-35.14 μg/l vs. ceftriaxone-29.02 μg/l) and in amnioticfluid were low (cefazolin-6.8 μg/l vs. ceftriaxone-1.58 μg/l).
Conclusions: It is most optimal to administer a single-dose of the 1st generation cephalosporins-cefazolin-immediately following the clamping of the umbilical cord as well as in preoperative preparation in gynaecological operations.
P-04-005 Management of delivery of type-1 diabetic mother
M. Ivanisevic, J. Djelmis, D. Bljajic, N. Ljubas
Department of OB/GYN, Zagreb, Croatia
Patients and Methods: In ten years period (1995–2004) 396 pregnant patients with type-1 DM were delivered. The aim of the study was to analyze the mode of delivery, perinatal outcome in relation to gestational weeks, complications of diabetes mellitus and complications of pregnancy.
Results: 396 type-1 diabetic patients delivered 398 new born children (2 pregnancies with twins). 309 pregnant type-1 patients were without diabetic complications, 29 pregnant patients with non proliferative retinopathy, 23 patients with proliferative retinopathy, 5 patients with peripheral neuropathy and 30 patients with clinically manifest nephropathy. Premature labour occurred in 81 out of 396 deliveries (21.5%) of type-1 diabetic women. Among premature delivered patients the rate of elective preterm delivery was 16.6% what is explained with increased incidence of other complications of pregnancy like fetal in compromise (n = 35; 43.2%) and super-imposed pre eclampsia (n = 31; 38.3%). In 15 (18.5%) out of 81 prematurely delivered pregnant diabetic patients pregnancy was terminated earlier than 37 week of gestation because of contractions. The incidence of respiratory distress syndrome in premature new born children was 14.8% (n = 12). There were 93 (23.6%) spontaneous vaginal deliveries, 7 (1.8%) deliveries finished by VE, and by caesarean section delivered 296 (74.7%) type-1 diabetic patients. There were 23 (5.8%) SGA newborns, 269 (67.6%) AGA newborns, and 106 (26.6%) LGA newborns. Perinatal mortality was 3.3% (n = 13; 8 stillbirth and 5 neonatal death). Congenital malformations occurred in 10 (2.5%) newborns: one child with Potter’ syndrome, 6 children with congenital heart malformation, one child with prosencephaly, and two children with multiple malformations. Four children with congenital malformations died in early neonatal period.
Conclusion: The type-1 diabetic pregnant patients must be considered a high risk obstetric patients and delivered in the unit that can provide experienced obstetric care, continuous fetal monitoring, and neonatal intensive care.
P-04-006 Periodontal diseases and risk of preterm birth: immunological correlations
G.C. Di Renzo1, G. Coata1, A. Conversini2, L. Pennacchi1, A. Fanetti1, S. Pagano2, P. D'Errico2
1Dept. of Obstet. and Gynecology, Centre of Perinatal and Reproductive Medicine, University of Perugia, Perugia, Italy; 2Section of Odontostomatology, University of Perugia, Perugia, Italy
Objective: Periodontal disease (PD) and chronic oral infection, occurring in 5–40% of pregnant women, have been associated with several systemic conditions and adverse pregnancy outcome such as premature delivery and low birth weight.
In PD, anaerobic gram negative bacteria seems to trigger host-immune response causing activation of local and systemic pro-inflammatory mediators which could activate production of prostaglandins and metalloproteases (MMPs) that degradate collagen fibers of cervix.
The aim of this study is to determine if an association exists between fetal and maternal immune inflammatory response to oral pathogens supporting a role for maternal periodontal disease as an additional infectious risk for adverse pregnancy outcome.
Methods: Patients: Ten pregnant women at high risk for preterm birth (under tocolytic therapy) and 10 pregnant women with physiological pregnancy were enrolled between 23–32 weeks of gestation. Exclusion criteria were: pregnants using FANS, steroids and tetracyclines or affected by diseases as diabetes mellitus, hypertension and immunological diseases which may influence MMPs levels and pro-inflammatory mediators.
Materials and Methods: Gingival crevicular fluids (GCF), cervical-vaginal fluids and peripheral blood samples were collected from each patient and concentrations of MMPs, IL-6, IL-8, IL-1b, TNF-a and C-reactive protein were measured by using enzyme-linked immunosorbent assay. Besides, all GCF and cervicovaginal samples were analysed for anaerobic, aerobic and other common microorganisms.
Results and Conclusions: Preliminary results support an association between PD and immunological activation in patients with threatened preterm labour.
P-04-007 Mode of delivery and perinatal outcomes in women with heart disease
M. Korbel, Z. Niznanska, M. Redecha, A. Havalda
1st Department of Obstetrics & Gynaecology Schoool of Medicine Comenius University, Bratislava, Slovak Republic
Objective: Maternal heart disease complicates 0.3% of pregnancies in Slovak Republic. Pregnancy in women with heart disease is associated with significant maternal and neonatal complications. An analysis of perinatal outcome of women with heart disease delivering during the 18 year period was performed.
Methods: This study enrolled 379 pregnancies in women with heart disease receiving care in the 1st Department of Obstetrics and Gynaecology in Bratislava from January 1986 to October 2003. Retrospective analysis was submitted on mode of delivery and pregnancy outcomes in three time periods (from 1986 to 1990, from 1991 to 1996, and from 1997 to 2003).
Results: During study period there were 17 833 deliveries in our department, among them 379 (2.12%) deliveries of women with heart disease (in three time periods 1.9%, 2.9% and 1.7% respectively). Out of them 46% were congenital heart malformation, 12% acquired rheumatic lesions, and 42% miscellaneous heart lesions. Frequency of Caesarean section was 35%, forceps/ventouse delivery 5%, and normal vaginal delivery 60% during the whole study period. Caesarean section frequency in three time periods was 37%, 33%, and 36% respectively. Obstetrics indication for Caesarean delivery was in 52% and cardiological in 47%. The percentage of cardiological indication for Caesarean delivery in three time periods was 45%, 37%, and 67% respectively. Maternal mortality rate was 260/100,000. All pregnancies resulted in a live birth, 3.7% of them were premature, and 2.6% of babies were small-for-gestational-age. The recurrence rate of congenital heart disease in babies of mothers with congenital heart disease was 5.2%.
Conclusion: Specialized medical care enrolling pre-pregnancy counselling, early diagnosis, assessment and good cooperation between cardiologist and obstetrician, continuous surveillance during pregnancy, delivery and puerperium resulted in excellent perinatal outcomes and minimized risk of complications.
P-04-008 Neonatal neurological morbidity associated with uterine rupture
A. Garcia-Alix, M. Martinez Biarge, F. Cabanas, A.M. Sanchez Torres, F. Garcia Benasach, J. Quero
La Paz University Hospital, Madrid, Spain
Objective: Uterine rupture (UR) is a sentinel hypoxic event that can cause brain damage in a previously healthy fetus. However, nothing is known about the risk of hypoxic-ischemic encephalopathy related to uterine rupture. The aim of our study was to examine neurological morbidity associated with uterine rupture during labour and to compare it with the morbidity associated with a nonreassuring fetal status (NRFS).
Methods: This is a retrospective cohort study. We analysed all cases of term infants delivered after a symptomatic uterine rupture occurring at our hospital from January 1998 to September 2004, and compared them with a randomly selected group of infants born by operative delivery because of an abnormal (non-reassuring) fetal heart rate pattern.
Results: Prevalence of uterine rupture was 0.058%. Of 35 identified cases, 21 were included and compared with 63 controls. Maternal and infant general characteristics were similar between both groups. Perinatal morbidity was significantly higher in the uterine rupture group. Babies delivered after an uterine rupture had lower 1-minute and 5-minute Apgar scores, lower umbilical pH, and requiered more advanced resuscitation than infants in control group. Of the 35 cases with UR, seven (33%) had hypoxic-ischemic encephalopathy, compared with 5% in NRFS group (P < 0.01, RR 3.7). Among RU newborns, 4 (19%) had moderate or severe encephalopathy; all of them had also multisystem dysfunction and an adverse outcome: one infant died at 3 days of age, the remaining 3 infants showed marked neurological disability (cerebral palsy, mental retardation, developmental delay). No infant in the nonreassuring fetal status group showed moderate or severe encephalopathy.
Conclusions: Our results provide strong support to the fact that uterine rupture is a considerable sentinel hypoxic event which involves a high rate of early and late neurological morbidity.
P-04-009 Postpartum infection complications after obstetric operations in slovenia
B. Sajina Stritar
University Medical Centre, Department of Ob/Gyn, Perinatology unit, Ljubljana, Slovenia
Objectives: The important risk factors for postpartum maternal infection are obstetric operations. According to literature antibiotic prophylaxis in risk groups reduces postpartum infections complications. If the level of post-operative infection morbidity is lower than 10% without a policy of antibiotic prophylaxis, the antibiotic prophylaxis is not recommended.
Methods: We analysed the postpartum period in women who gave birth in Slovenia from 1997 to 1999. The data was collected from National Perinatal Informational System (NPIS).
Results: In 3 years (1997–1999) there were 52,990 deliveries in Slovenia. In 1559 cases (2.9%) the vacuum extraction or forceps were done. In that period there were 5159 (9.7%) caesarean deliveries in Slovenia, among them 3424 elective (6.4%) and 1735 urgent (3.3%). Postpartum infection (wound infection, endometritis, sepsis, tromboflebitis, other infection) and post operative fever were most common in the group with urgent than in the group with elective caesarean delivery. After operative vaginal delivery postpartum infection is more often than after spontaneous vaginal delivery. In the breech presentation the postpartum infection complications are more often than after vertex presentations. There were no statistical significant differences among groups. In all groups the infection complications were less than 10%.
Conclusions: In Slovenia infectious complications followed less than 10% of operative delivery. The routine administration of prophylactic antibiotic in women undergoing operative delivery in Slovenia is not necessary.
Keywords: Obstetric operations, infection, antibiotic prophylaxis
P-04-010 “Exit” Procedure (ex-utero intrapartum treatment): management of upper airway congenital malformations
A. Linde, M. Ortiz, F. Castillo, E. Carreras, J. Sanchez-de-Toledo, J.L. Peiro
Vall d'Hebron Hospital, Barcelona, Spain
Objective: Case report about 2 newborns with obstructive congenital malformations of upper airway managed with ex-utero intrapartum treatment (EXIT).
Method: To perform the EXIT technique caesarean section and uterine-fetal relaxation are needed. They allow the maintenance of placental oxygenation support to the fetus while the fetal head and neck can be exposed and intubation can be attempted. If intubation is not feasible, tracheostomy or mass resection must be made by the surgery team. Fetal monitoring includes continuous pulse oxymetry and ultrasound examination of umbilical cord blood flow.
Results: Case 1: Prenatal diagnosis of nasal-oro-hypopharyngeal teratoma with severe polyhydramnios. Tracheostomy was made with EXIT technique. Definitive treatment was made at 6th day of life without complications. Case 2: Prenatal diagnosis of cervical teratoma with tracheal and carotid deviation. During EXIT technique we proceeded to partial mass resection allowing us to intubate the patient. Definitive exeresis was made after delivery.
Conclusions: EXIT technique is a safe procedure that improves prognosis of cervical masses with upper airway obstruction. Multidiscyplinary management including obstetricians, paediatric surgeons, neonatologists, and anestesiologists is the key to the successful outcome of this procedure.
P-04-011 Small for gestational age neonates, delivered by caesarean section – morbidity analise
M. Skender, M. Raicevic Pavlovic, J. Lapcevic, S. Tasic
Clinical-hospital center Zemun-Belgrade, Belgrade, Serbia
Aim: To investigate a relationship between small for gestational age (SGA) neonate morbidity (Mb) and delivery mode. The prospective study included 54 SGA neonates (body mass below 10th percentile) delivered by Cesarean section (SC) (group A), 54 SGA neonates delivered vaginally (group B) and 54 AGA (body mass between 10th and 90th percentile) neonates delivered by CS (group C). Of 12,324 livebirths 4.97% were SGA Among them, 8.82% were delivered by SC: 20 by elective SC, 22 by SC after unsuccessfully induction of vaginal delivery and 12 by emergent SC. Groups A and B, except at delivery mode, significantly differed at: mothers age (28.89 vs. 25.15, p < 0.01), number of hypertensive pregnancies (17 vs. 7, p < 0.05), imminent fetal asphyxia (22 vs. 2, p < 0.01), intrapartal asphyxia (23 vs. l, p < 0.01), pulmonary deseaces (18 vs. 7, p < 0.05) and neurologic disturbances (21 vs. 6, p < 0.01). Groups A and C, except at body measures, significantly differed at: imminent fetal asphyxia (22 vs. 6, p < 0.01) and intrapartal asphyxia (23 vs. 4, p < 0.0l). There was no statistical difference between investigated groups at the other risk factors and neonatal Mb. SGA infants, delivered by elective SC had significantly lower intrapartal asphyxia rate than SGA infants delivered by SC after unsuccessfully induction of vaginal delivery (1 vs. 10, p < 0.05) and significantly lower rate of pulmonary deceases (4 vs. 8, p < 0.05), intrapartal asphyxia (1 vs. 12, p < 0.01) and neurologic disturbances (1 vs. 7, p < 0.01) than SGA infants delivered by emergent SC.
Conclusions: 1) that SGA neonates with imminent or incipient fetal asphyxia are more frequently delivered by emergent SC and have significantly higher Mb due to chronic intrauterine suffering and prematurity than SGA neonates, delivered vaginally or AGA neonates delivered by SC, and 2) that prenatal diagnostic, planning the adequate delivery mode and intensive neonatal care contribute to better perinatal and late outcome of SGA infants.
P-04-012 Subgaleal haemorrhage, prevalence and morbidity
J. Arnaez Solis, A. Garcia-Alix, C. Cudillero, M. Martinez-Biarge, J. Quero
Pediatric University Hospital La Paz, Madrid, Spain
Objective: To establish the prevalence of Subgaleal Haemorrhage (SGH) in a third level hospital, and to examine neonatal morbidity associated with this extracranial haemorrhage.
Methods: Medical records, radiological and neuroimaging studies of all patients diagnosed of SGH from January 2000 to January 2006 were reviewed.
Results: Prevalence of SGH was 0.02%. Of the 12 identified patients, one had an eutocic delivery. 3 were born by caesarean section, and 8 by operative vaginal delivery. Five (42%) had skull linear or depressed fracture, 2 of them had intracranial hemorrhage: 1 subdural with frontal cerebral contusion and one intraventricular. Four of the 12 patients (33%) were admitted in NICU due to hypovolemic shock requiring volume expansion and/or vasoactive drugs. These four patients developed coagulopathy, anemization and renal failure within 24 hours after admission. Hyperbilirubinemia due to over-production and cholestasis was observed in two cases. All four patients presented lethargy or stupor on the first neurological examination, and all but one showed a complete recovery. The most severe case developed bilirubin related encephalopathy and required exchange transfusion. One patient had seizures. None of them had hypoxic-ischemic brain injury. The remaining 8 cases did not have any complications and were admitted for clinical observation and/or treatment of other minor conditions.
Conclusions: SGH is rare extracranial hemorrhage, and it is not always associated with operative delivery. Skull fractures and more serious intracranial bleeding should be investigated in these patients. The high incidence of considerable extraneural morbidity warrants a vigorous approach.
P-04-013 Postoperative myometrial defects and increased fetomaternal morbidity
E. Kucera1, J. Feyereisl1, L. Krofta1, P. Krepelka1, V. Hejda1
1Institute for the Care of the Mother and Child, Prague, Czech Republic; 2Institute for Postgraduate Medical Education, Prague, Czech Republic
Objective: Increased fetomaternal morbidity and mortality are potential risks after different operations of the uterus. Caesarean section as well as modern endoscopic operations can cause an uterine scar which subsequent abnormal placentation.
Design: Case report.
Setting: Institute for the Care of the Mother and Child, Podolské nábřeží 157, Prague 4, 147,00.
Case: We present detailed analysis of typical case reports of pathological placentation after CS and hysteroscopic intrauterine surgery. The first case represents a 24-year-old infertile nullipara with a previous history of hysteroscopic uterine septum resection conceived 2 years after surgery. She experienced several episodes of vaginal bleeding between the 11th and 16th week of intrauterine pregnancy. Clinical and sonographic evaluation diagnosed abnormal placentation in the uterine fundus. Immediate surgical intervention with termination of pregnancy and resection of the afflicted area was indicated. The second case represents a 32-year-old woman with a history of CS. Termination of pregnancy was indicated in the 12th week of present gestation. Heavy bleeding with blood loss about 1700 ml occured during this procedure. TAH was indicated and prooved pathological nidation in the scar after CS.
Conclusion: Pregnancies after some types of intrauterine surgery (septum resection, endometrial ablation) are high risk. Pathological placentation after CS creates a specific group of patients threatened with severe hemorrhage. We recommend intensive prenatal care with immediate surgical intervention when complications occur.
P-05-001 Spontaneous abortions treated at the department of gynecology and obstetrics of the health center sremska mitrovica from 1987 to 2004
B. Divic, S. Arbanas
Health center, Sremska Mitrovica, Serbia
Aim: To investigate whether there could be any increase in the incidence of spontaneous abortions according to the worsening living conditions as a consequence of the civil war and economic crisis in Serbia.
Materials and Methods: We observed the situation in the region of Srem with a population of 370,000 inhabitants and an average of 1500 deliveties per year. Whole number of spontaneous abortions was divided into two groups. First group comprised abortions between 1987 and 1995. There were 1775 women treated under diagnose of spontaneous abortion. In the same period we calculated that it was 12.14% of all pregnancies which were diagnosed in our health center. We had 408 missed abortions and 1,368 miscarriages in the same period. Between 1996 and 2004 number of spontaneous abortions rised to 2197 cases, 15.17% of all diagnosed pregnancies in our region. Abortions were divided as follows: 646 missed abortions and 1551 miscarriages. In both periods the majority of women was between 21 to 35 years of age. The number of missed abortions was analyzed according to the age of women and gestational age. We did the same with the number of miscarriages.
Results: The authors noticed a significant rise in the number of spontaneous abortions during the period from 1996 to 2004 which was statistically documented. The increase is significant in the group of missed abortions and miscarriages as well.
Conclusions: It was a post war period of economic crisis and a time of transition which was late in Serbia comparing the surrounding countries.
P-05-002 Preterm labor therapy – are tocolytics always necessary?
V. Mandic Markovic, Z. Mikovic, D. Pavlovic, R. Vugdelic, M. Stankovic
Ob./Gyn. Clinic “Narodni front”, Belgrade, Serbia
Aim: To establish if tocolytics are indicated in the cases of imminent preterm delivery with the presence of regular uterine activity and minimal changes in cervical length and/or dilatation.
Methodology: A clinical randomized prospective trial included 60 patients gestational age 26 to 32 weeks with preterm labor. Preterm labor was diagnosed in the presence of regular uterine activity (4/1 h). The cervical effacement was <80% and dilatation <2 cm. 30 received 48 h intravenous beta-mimetic therapy; while in the other 30 placebo was administrated in the same time interval. We registered: maternal age, parity, history of preterm delivery, infection, cessation of uterine activity after 24 h, change in the cervical effacement (>10%) or dilatation (>1 cm), need for the another tocolytic therapy; gestational age, neonatal weight and Apgar scoor at delivery.
Results: There were no significant difference between the groups in maternal age, parity, history of preterm delivery and infection. The cessation in uterine activity was registered in 27 (90%) patients in group 1, while in 25 (83.33%) patients in group 2; change in the cervical effacement or dilatation was found in 5 (16.67%) patients in group 1, while in 17 (23.33%) in group 2. Intravenous tocolytic therapy was repeated in 2 (6.67%) patients in group 1, while in 4 (13.33%) patients in group 2. There were no significant differences between the groups in gestational age, neonatal weight or Apgar scoor at delivery.
Conclusion: Tocolytic therapy in the management of preterm labor should be administrated with great caution, only in the cases with the presence of uterine activity and adequate change in cervical effacement (>80%) and/or dilatation (>2 cm).
P-05-003 Presence of bacterial and fungal infection and their significance in preterm delivery
M. Bogavac1, Z. Grujic1, A. Mitreski2, G. Relic3, A. Nikolic1, Lj. Milasinovic1
1Clinical Center Novi Sad, Department of Obstetrics and Gynecology, Novi Sad, Serbia; 2Private Gynecological/Obstetrical Clinic “Minerva”, Novi Sad, Serbia; 3Medical School in Pristina, Department of Obstetrics and Gynecology, Priština, Serbia
Aim: To investigate the presence of bacteria and fungi in the patients with preterm delivery.
Material and methods: A group of 53 patients (preterm delivery, investigated group) has been selected by random choice in which the delivery occurred between the 24th and 36th WG relative to the 63 patients delivered in term (control group).
Results: The presence of bacterial infection has been investigated at the level of genitourinary tract. It was recorded in 21 (39.6%) patients with preterm and 7 (11.1%) patients with term deliveries. The incidence of bacterial infection was significantly increased (p < 0.001) in the group of patients with preterm delivery relative to the term ones. The fungal infection was recorded in 3 (5.7%) cases in the vagina and in 3 (5.7%) patients in the cervix in the group of preterm deliveries whereas the term delivery patients presented with 2 (3.2%) cases of fungal infection in the vagina 2 (3.2%) cases of fungal infection in the cervix. Fungal infection was recorded in a small number of patients which has been explained by the preventive administration of vaginal suppositories containing antimicrobial effect (MacMyror, Polyginax) either in the scope of antibiotic therapy or separately.
Conclusion: The analysis of bacterial infection of genitourinary tract revealed a significantly increased presence of bacteria (p < 0.001) in the patients with preterm deliveries relative to the patients delivered in term which is suggesting that there is a need for bacteriologic investigations during pregnancy in the risk groups of patients with previous spontaneous abortions and preterm deliveries, and in cases of the symptoms of genitourinary infections presented during pregnancy.
P-05-004 Early neonatal sepsis and pre-term rupture of amnion
F. Skokic
University Medical Centre Tuzla, Clinic for Gynaecology and Obstetrics, Tuzla, Bosnia and Herzegovina
Early neonatal sepsis is an acute system disease at the age of 0–7 days. The incidence ranges from 1 to 10 per 1000 living newborns. Risk factor for the occurrence of the disease is pre-term rupture of amnion, where the time period from the rupture of amnion to the delivery is latent period.
Objective: To present the incidence of early neonatal sepsis in pre-term rupture of amnion and compare it with the latent period, gestation age, birth weight and the outcome.
Examinees and Methods: Early neonatal sepsis incidence in pre-term rupture of amnion was followed over the period of two years in two groups of newborns with different length of latent period.
Results: 8925 newborns were born in the period of the study. 41 of them (0.45% 0 had early neonatal sepsis. 23 (56.09%) of them had a latent period shorter than 24 hours, and in 18 (43.91%) newborns the latent period exceeded 24 hours c2 = 8.97, p = 0.0027). The incidence of early neonatal sepsis in pre-term rupture of amnion is 5.75%. Pre-term babies were predominant in both groups compared to newborns born at term or after. Statistically significant difference in the occurrence of early neonatal sepsis compared to the latent period was found only in pre-terms (c2 = 29.18, p < 0.0001), whereas this difference is not statistically significant for children born at term or after (c2 = 10.55, p = 0.0051). In both examined groups, the number of newborns with low body weight was larger. Out of 41 newborns with early neonatal sepsis, 12 died (29.26%): 11 pre-terms and one born at term.
Conclusion: The incidence of early neonatal sepsis is 5.77% in newborns with pre-term rupture of amnion. It is more frequent in the group of newborns with shorter latent period, shorter gestation and lower birth weight.
Keywords: Early neonatal sepsis, pre-term rupture of amnion
P-05-005 Perinatal outcomes in immigrant women
M. Lopez-Vilchez, I. Martin Ibanez, L. Ymbert Pelleja, A. Mur Sierra
Hospital Universitari del Mar, Barcelona, Spain
Objectives: To describe the characteristics of immigrant women's newborn in our area, and to compare them with those of native pregnant women's.
Methods: All newborn attended in the Neonatology Section of Hospital del Mar in Barcelona, Spain, in 2003 and 2004 are included (n = 2735). Data was prospectively collected in a database. Pregnant immigrant women were classified in 6 regions (Eastern Europe, rest of Europe, Africa, Asia, Latin America and others). 12 diagnosis were defined and compared between native newborn and those of immigrant origin, calculating their relative risk.
Results: There were 1296 native newborn (47.8%) and 1416 of immigrant origin (52.2%). Immigrant women had a higher rate of HBsAg infection (2.0% vs. 1.0%) and lower of VHC (0.8% vs. 2.0%; p < 0.01). There was only one HIV-positive pregnant immigrant woman, in front of 14 Spanish (p < 0.01), and drug use was lower in the immigrant group (0.4% vs. 4.0%; p < 0.01). Immigrant newborn had a lower rate of prematurity (6.0% vs. 7.6%) and of low birthweight (2.3% vs. 4.6%; p < 0.01). There were no significant differences in the rate of respiratory distress nor fetal acidosis. The incidence of neonatal infection risk was higher in immigrant newborn (49.9% vs. 40.6%; p < 0.01).
Conclusions: Immigrant mothers'newborn have in our area better perinatal outcomes than native newborn, being the most frequent complications secondary to an inadequate prenatal care.
P-05-006 Prediction of preterm birth by transvaginal ultrasound assessment of cervical length in an unselected population
A. Veduta, R. Vladareanu, D. Tutunaru, R. Bohiltea, B. Alexandru
Elias Emergency Hospital, Marasti, Bucharest, Romania
Objective: To study the utility of the sonographic evaluation of cervical length in predicting preterm delivery (PTD), in women with low background risk.
Large studies established that shortened cervix is predictive of PTD, in women at risk, but studies in unselected populations are still missing.
Material and Methods: This is a prospective analytical study of 89 primiparas with singleton pregnancies (an unselected group with uniform, average risk of PTD). We assessed the cervical length for each patient, by transvaginal sonography, at 2-week intervals between 27 and 36 weeks of gestation (27 + 0 to 35 + 6).
We stratified the patients, on basis of the sonography evaluation results, in: patients who never scored less then 30 mm; patients who scored less than 30 mm at least once but never less than 15 mm; and patients who scored less than 15 mm at least once. We analyzed the incidence of PTD in the three subgroups.
Qualitative differences between subgroups were tested using chi2 test; p values less than 0.05 were considered significant.
Results and Conclusions: 43 of the 89 patients never scored less then 30 mm, and there was 1 preterm delivery in this subgroup; 26 patients scored less than 30 mm at least once but never less than 15 mm, and there was 1 preterm delivery in this subgroup; 20 patients scored less than 15 mm at least once and there were 3 preterm deliveries in this subgroup.
The frequency of PTD was significantly higher in the subgroup of patients who scored less than 15 mm at least once than in the subgroup of patients who never scored less then 30 mm (p < 0.05).
P-05-007 Can cervical length predict preterm delivery in women with threatened preterm labor?
R. Vladareanu, A. Veduta, D. Tutunaru, A. Filipescu, M. Zvanca, B. Alexandru
Elias Emergency Hospital, Bucharest, Romania
Objective: To study if sonographic measurement of the cervical length helps to distinguish between true and false preterm labor and to predict if preterm delivery will occur within 72 hours, in women presenting with threatened preterm labor.
Diagnosis of incipient preterm labor on clinical basis is not accurate. Recent studies showed that cervical length was the only significant independent predictor of immediate delivery.
Material and Methods: This is a prospective clinical series of 91 patients presenting with threatened preterm labor and intact membranes, before 35 weeks of gestation. Mean gestational age was 31 weeks ± 2 (25 + 0 to 34 + 6). Patients over 35 weeks of gestation, as well as patients with ruptured membranes and those presenting in active labor were excluded. We assessed the cervical length, by transvaginal ultrasound, in this series. The assessment was not disclosed and not taken into account in the subsequent management of the patients. Univariate logistic regression analysis was used to assess the association between delivery within 72 hours and cervical length and other maternal parameters.
Results: 19 of the 91 patients delivered within 72 hours. 2 of these 19 patients had the cervical length over 15 mm, and the rest of 17 patients had the cervical length of less than 15 mm. 55% of the patients with cervical length under 15 mm and only 3.3% of the patients with cervical length over 15 mm delivered within 72 hours. There was no significant association between delivery within 72 hours and the following parameters: maternal age, maternal BMI, vaginal bleeding, tocolytics use.
Conclusion: In univariate analysis, cervical length was the only significant predictor of delivery within 72 hours.
P-05-008 Multifactorial approach of patients with high risk of repetitive cervical insufficiency and immature birth
C. Roos2, A. Merien2, B. Arabin1
1Department of Perinatology Isala Clinics, Zwolle, The Netherlands; 2Clara Angela Foundation, Witten, Germany
Objective: Although cerclage has not been proven to reduce preterm birth in large populations, it may be effective in selected patients with a history of cervical insufficiency and/or changes of the cervix shown by transvaginal sonography (TVS). Early opening of the internal os and multiple pregnancy impair the outcome even after cerclage. We here report on our approach and the course of pregnancy in mothers who all had already lost two previous babies due to a history of repetitive immature birth in the second trimester (20–24 weeks).
Methods: The 3 patients were treated with vaginal cerclage (Shirodkar) at 12 weeks of gestation but presented with cervical shortening (CL < 1 cm !) and severe funneling within 4 weeks after the operation. Therefore, a cerclage pessary was placed “on top” to relieve pressure on the sutures. In addition, the patients were treated with progesterone and tocolysis, if they presented with conractions and metronidazol in case of bacterial vaginosis.
Results: Prolongation of pregnancy up to viability was achieved in all patients. The gestational age at birth was 33 weeks (PPROM), 36 weeks (acceptance of labor) and 37 weeks (elective induction). The birth weights were 1550 g, 2740 g and 2810 g respectively.
Conclusion: In patients with a poor history and early opening of the internal os a polypragmatic approach seems to be justified even though there will never be clear evidence for the combination of several mechanical and pharmaceutical therapies.
P-05-009 Could the ultrasonographic study of the cervix predict preterm delivery in low risk population?
E. Scazzocchio, A. Munoz, M. Echevarria, M.A. Rodriguez, P. Prats, M. Torrents, B. Serra, J.M. Carrera
Institut Universitari Dexeus, Barcelona, Spain
Objective: To assess the value of cervical length (CL) measurement by transvaginal ultrasound in low risk (LR) pregnancies for predicting spontaneous preterm delivery (PD).
Methods: A prospective observational study was carried out from 2000 to 2005 involving 7604 subjects with singleton pregnancies at LR for preterm delivery. The cervix was evaluated at 18–22 weeks of gestation. Cervical parameters included were CL and presence of funneling.
Results: Mean maternal age was 33 (DS 3.9) (29.5% > 35 years). Nulliparous women were 59.4%. The incidence of PD < 28 weeks <34 weeks and <37 weeks were 0.2%, 0.8%, 4.2% respectively. Women with PD had shorter median cervical lengths than those with term deliveries (). The effectiveness of cervical length and funneling to predict PD <34 weeks is shown in . A cervical length <28 mm, which corresponded to the 2.5th centile, occurred in 5.3%, 8.5%, 8.8% and 15.4% of those with PD <37, <34, <32 and < 28 weeks, respectively. Logistic regression Analysis identified LC <28 mm (OR: 5.3 CI (2.1–13.5)) as the only factor associated to risk of PD, excluding the presence of funneling.
Conclusions: The current data suggest that the value of cervical length assessment in our low-risk population is limited. The low sensitivity of CL to predict PD might increase adding and combining biochemical markers to predict PD as fibronectin test.
P-05-010 Biochemical and sonographic diagnosis in preterm delivery
M. Brik, M. Marin, C. Rizo, V. Maiques, A. Perales
Hospital Universitario La FE, Valencia, Spain
Objective: The performance of phIGFBP-1 has been poorly assessed in diagnosis of spontaneous preterm delivery. To date, no studies have been done combining the cervical length and phIGFBP-1. The aim of this study was to examine the diagnostic performance of ultrasonographic measurement of the cervical length and IGFBP-1 ph for premature delivery prediction.
Methods: 174 patients, complaining uterine contractions and with intact amniotic sac, between 24-35 weeks gestational age, were studied. Ultrasound examination of the cervical length and cervical IGFBP-1ph were performed. Outcome variables were the occurrence of preterm delivery within 48 hours, 7 days, and 14 days of admission, delivery ≤32 and ≤35 weeks, as well as the admission-to-delivery interval.
Results: The prevalence of preterm delivery ≤35 weeks was 19.2%, and ≤32 weeks was 5.4%. Cervical phIGFBP-1 frequency was 71.1% for negative test, and 28.9% for positive test, whereas cervical length <15 mm was 6.4%, and ≥30 mm was 75.6%. The presence of a positive ph IGFBP-1 is useful for prediction of preterm delivery before 32 and 35 weeks (+LHR = 2.5, CI: 1.48-4.47, and 2.1, CI: 1.26-3.49, respectively). Also, when decreasing cervical length, the admission-to-delivery interval was shorter (p < 0.05). When combined both test (phIGFBP-1 and cervical length) for the prediction of spontaneous preterm (Kaplan-Meier), the median interval time was shorter when both were positive as compared to only one positive tests or both negative, but CI were overlaped.
Conclusions: Both tests are useful for prediction of spontaneous preterm delivery. When combining them, their diagnostic improvements remain to be shown.
P-05-011 Immunoprophylaxis failure in infants borned from e antigen negative-precore mutant chronic HBV infected mothers
I. Elefsiniotis2, M. Papadakis1, G. Vlahos1, G. Daskalakis1, K. Barbati3, A. Antsaklis1
1First Department of Gynecology, University of Athens, Athens, Greece; 2Depatrment of Internal Medicine, Hippokration Hospital, Athens, Greece; 3Department of Pathology, Red Gross Hospital, Athens, Greece
Objective: Transplacental transmission of HBV is the major cause of immunoprophylaxis failure in infants born from chronic HBV infected mothers. The aim of our study was to prospectively evaluate the possibility of transplacental transmission of HBV infection from viremic HBeAg(−) chronic HBV infected pregnant women, who exhibit the precore HBV mutation (mt 1896), to their infants.
Patients: Twenty-three HBeAg(−)/AntiHBe(+) chronic HBV infected pregnant women with detectable viral load at week 28 of gestation and at labour (HBV-DNA positive, Amplicor, Roche) and their infants were serologically (HBsAg, HBeAg, Anti-HBe, Anti-HBc, Anti-HBs) and virologically (serum HBV-DNA) evaluated. Cord blood samples were also evaluated for the presence of viremia and HBV-DNA extraction was done from placenta tissue specimens. Sequencing of the precore region of the HBV genome was done in the HBV-DNA positive samples. Moreover immunohistochemistry of the placenta for HBsAg and HBcAg was done using the Envision HRP immunohistochemical method.
Results: HBsAg, HBeAg, Anti-HBs and HBV-DNA was not detected in none of 23 infant serum samples evaluated whereas Anti-HBe and Anti-HBc was detected in all of them at labor (before the immunoprophylaxis schedule). All cord blood samples were HBV-DNA negative and HBV-DNA was not extracted in any of 23-placenta tissue evaluated. None of 23-placenta tissue evaluated for HBsAg and HBcAg was positive. Passive-active immunoprophylaxis failure was not observed in any of the 23 infants evaluated.
Conclusion: HBV infection is not transmitted via the transplacental route in infants from viremic HBeAg-negative chronic HBV infected mothers with the precore mutation, resulting possibly in the extremely low rates of immunoprophylaxis failure observed in our country.
P-05-012 Hepatic function in a mother with diabetes mellitus
K. Kornacka, J. Tolloczko, J. Seliga
Warsaw Medical University, Department of Neonatology, Warsaw, Poland
Diabetes Mellitus in pregnancy and its complications in the neonate still remain an ongoing and challenging question in perinatology. In the past years several pathologies of the neonatal period were discovered such as; congenital diseases, hypoglycemia, hypoxia, respiratory disorders, and hyperbilirubinemia. Adequate carbohydrate metabolism reduces the risk of maternal and fetal complications.
Aim: To establish if there are any differences im hepatic function depending on pregnancy outcome (PGDM (pre gestational diabetis mellitus) or GDM (gestational diabetes mellitus) vs. physiological pregnancy) These children have a higher risk of hyperbilirubinemia which is due to hepatic prematurity and policytemia. Enzymatic dysfunction and policytemia is mainly caused by intrauterine hypoxemia due to insufficient carbohydrate metabolism and delay of hepatic maturation caused by hyperinsulinemia.
The research included 116 neonates (82 IDM and 34 healthy neonates). The average gestational age in the study and control group was >37 Hbd. All the neonates were in good clinical condition and were fed with breast milk.
On the third day of life blood samples were taken from all the neonates. We marked the levels of cholesterol, LDH, ALP, GGTP, bilirubin, biblical acid, and morphology.
There were no significant differences among the study groups. This leads us to a conclusion that adequate carbohydrate metabolism in a mother with diabetes mellitus in pregnancy allows sufficient physiological metabolic adaptation of the neonate.
P-05-013 Recurrent vulvovaginal candidiasis in pregnancy
M. Pacemski1, V. Atanasov2, V. Jovanov2, L. Zarova3
1Medical Center, Berovo, Macedonia; 2Medical Center, Delcevo, Macedonia; 3Institution for Health Protection, Kocani, Macedonia
Vaginal candidiasis is a common and frequently distressing infection in pregnancy. The hormonal mileau of the vagina during pregnancy undoubtedly enhances Candida colonisation and serves as a risk factor for symptomatic expression.
Objective: To assess the percentage of recurrent candida infection in pregnant women vagina.
Methods: From January to December 2005 cultures were taken from vagina of all 256 pregnant women in our units, which was at the first prenatal visit between 8–17 weeks' gestation. All specimens were cultured on plates containing Sabouraud dextrosa agar with 2% glucose.
Results: In our study, 256 pregnant women were investigated for Candida infection of the vagina. Clinical diagnosis, confirmed by culture, showed that 110 (43%) were treated for 6 days with clotrimasol (topical treatment). Treatment was considered as well accepted by all patients, and as well succesful in 220 (86%). According to our studies, treatment with topical drugs resulted in symptomatic cure and negative culture conversion in 86% of patients at the end of initial treatment. However Candida reappeared in the vagina after several weeks in 26 (24.2%) of initially cured cases, and some of them were again symptomatic. A small proportion of women 8 (7.4%) experienced three or more episodes of recurrent symptomatic vulvovaginal candidiasis.
Conclusion: Approximately 24% of pregnant women with vulvovaginal candidiasis get recurrent infection inspite of the adequate therapy.
P-05-014 Vaginal micro-flora – a perinatal risk factor?
M. Veleminsky1, P. Sak2
1Hospital Ceske Budejovice a.s., Ceske Budejovice, Czech Republic; 2The Faculty of Health and Social Studies, South Bohemian University, Ceske Budejovice, Czech Republic
Objective: To study the vaginal micro-flora of pregnant women at 24–42 weeks of gestation to determine whether the presence of specific micro-organisms is significantly associated with preterm birth, premature rupture of the membranes (PROM), preterm premature rupture of the membranes (pPROM) and other specific perinatal problems.
Methods: A prospective study of the vaginal micro-flora of 150 women between 24–42 weeks of gestation was performed. Three groups were compared: women with pPROM and/or preterm birth (less than 37 weeks), women with PROM (37 weeks and more) and women with birth at term without PROM. Microbiological assessment included cultures for aerobic and anaerobic bacteria, yeasts, Mycoplasma hominis, Ureaplasma urealyticum and Chlamydia trachomatis. Parasitological assessment and microscopy were performed.
Results: Prevalence of specific micro-organisms is described. At this time only not significant association between vaginal micro-flora and perinatal outcome were found.
Conclusions: Although strong association between vaginal micro-flora and perinatal outcome is described, we haven't found any significant yet. The study will be continued.
P-05-015 Bacterial vaginosis in pregnancy: Screening and epidemiology
M. Pacemski1, I. Samardziski2, V. Atanasov3, V. Jovanov3, L. Zarova4
1Medical Center, Berovo, Macedonia; 2Clinic of Gynecology and Obstetrics, Skopje, Macedonia; 3Medical Center, Delcevo, Macedonia; 4Institution for Health Protection, Kocani, Macedonia
Background: Bacterial Vaginosis (BV) is an important risk factor in pregnant women for premature rupture of membranes and preterm delivery. BV is detected in 9–28% of pregnant women and is often asymptomatic. Antibiotic treatment can be useful in prevention of preterm delivery or can contribute to the prolongation of pregnancy. We performed a cost-effectioeness analysis of screening and treatment for BV in early pregnancy.
Objective: The main aim of this prospective study was to determine the percentage of pregnant women with BV and single frequence of each microorganism.
Methods: We prospectively evaluated 256 pregnant women in our units during the period from January to December 2005. Vaginal and cervical swabs for bacterial culture and Gram stain were taken at the first prenatal visit between 8–17 weeks' gestation.
Results: Culture-proven BV was detected in 55 of 256 pregnant women (21.5%). The Following bacteria have been identified: streptococcus agalactiae in 5 (1.9%) of all patients, streptococcus viridans in 4 (1.6%), staphilococcus sp. in 9 (3.5%), enterococcus in 13 (5.1%), escherichia colli in 8 (3.1%), mycoplasma hominis in 13 (5.1%) and ureaplasma urealiticim in 29 (11.3%).
Conclusion: Our results have shown that bacterial vaginosis is highly present at pregnant women. The most common bacteria are enterococcus and ureaplasma urealiticum. As BV is associated with increased rates of preterm delivery there is a need for detailed microbiological monitoring of all pregnant women at early pregnancy.
P-05-016 Influence of pregnant screening cultures on the yielding of cord blood cultures
J.R. Cervilla, J.R. Fernandez Lorenzo, M. Lojo Rodriguez, J.M. Fraga
Hospital Clinico Universitario, Santiago de Compostela, Spain
Objective: Cord blood cultures (CBC) are done when there are sepsis-risk factors pre or intrapartum (corioamnionitis, maternal fever, prolonged rupture of membranes, low birth weight or resuscitation need among others. Besides Group B Streptococcus (GBS) is a leading cause of sepsis in livebirths (LB). Our aim had beeen to assess the yielding of CBC done and GBS found in CBC since 1998 through 2004.
Methods: To all LB born through these years, the yielding of CBC and positive-GBS CBC found were assessed. These data were compared between 1998 through 2001 (period 1) and from 2002 through 2004 (period 2) because pregnant women screening for vaginal/rectal GBS started at 2001 in our hospital.
Results: Overall CBC-positive rate was 2.4/1000 LB (41 out of 16.934). Between period 1 and 2, the CBC bacterial yielding rose from 1.2/1000 LB to 3.8/1000 LB (p < 0.05). The GBS-positive CBC rate was a median of 1.6/1000 LB during the entire period (1998–2004), and also rose from 1.0 to 2.4/1000 LB (p < 0.05). Mean rate of CBC done was 39.6/1000 LB and ranged from 27.9/1000 LB to 55.1/1000 LB between the two periods.
Conclusions: There were significant increments in either the yielding of positive-CBC found (152%) and GBS-positive CBC (120%) between the periods 1 and 2. These findings may be related to the raised rate of CBC/1000 LB done (98.2%) – which are made when high-risk infection factors exist – due to the increased awareness of the staff medical in charge.
P-05-017 Perinatal group B streptococcal disease – past and present
F. Ribeiro, A.P. Pereira, C. Silverio, F. Palma, C. Matos
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objective: To compare the incidence of perinatal group B streptococcal (GBS) disease during the years 2000 (before the implementation of the universal prenatal screening and intrapartum prophylaxis) and 2004 (after the implementation).
Methods: We searched for newborns with an infection risk and made a retrospective comparative study of the mother and newborn's clinical data in the years 2000 and 2004. We considered: maternal data, personal and obstetric history, pregnancy complications, prenatal screening, gestational age at birth, intrapartum prophylaxis, hours of rupture membranes, delivery data, neonatal morbidity and mortality.
Results: In the year 2004 there was 1 case of neonatal sepsis, confirmed with hemoculture. In the year 2000 we found 13 cases of neonatal sepsis: ten had positive hemoculture (group 1) and 3 had clinical and laboratorial sepsis with positive antigenuria but negative hemoculture (group 2). In group 1 we found a woman with GBS bacteriuria during the current pregnancy, 2 preterm delivery and 2 amniotic membrane rupture >24 hours. In group 2 we found 1 preterm delivery (planned caesarean delivery) and 1 case of intrapartum fever. Universal prenatal screening and intrapartum prophylaxis were not correctly made in groups 1 and 2.
Conclusions: Universal prenatal screening strategy based on combined vaginal and rectal cultures collected at 35–37 weeks' gestation from all pregnant women and recommended regimens for intrapartum antimicrobial prophylaxis for perinatal GBS disease prevention are effective in the prevention of perinatal GBS disease and neonatal morbidity and mortality associated.
P-05-018 Early onset candidiasis in premature twins: Case report
M. Goudesidou, E. Apazidou, V. Tsikrika, K. Gaitana, A. Antonouli, E. Papadimitriou
University Hospital of Larissa, Larissa, Greece
Background: Fungal infections (FI) are frequent and major cause of late onset septicemia in very low-birth-weight neonates. Early onset disease and especially congenital candidiasis remain rare. We present the cases of preterm twins with early onset FI.
Reports: Extremely low-birth-weight (ELBW) twins were born after 25 weeks of gestation by vaginal delivery. Their mother was colonized with fungi during pregnancy and presented leucocytosis and elevated ESR perinatally. Both neonates had a widespread erythematous burn-like dermatitis, severe pulmonary disease, pronounced leucopenia, neutropenia and thrombocytopenia as well as persistent hyperglycemia. They were managed by mechanical ventilation and broad spectrum antibiotics with no improvement. Both neonates died, twin A on 2nd day of life and twin B on 3rd day. Blood cultures were sterile but fungi were isolated in very high titles from umbilical catheter tips after death.
Discussion: Early onset candidiasis (EOC) is transmitted vertically, during the passage of the neonate through the infected vagina of the mother and appears between 2nd–7th day of life. ELBW infants with GA < 27 w consist the most vulnerable population and present with burn-like dermatitis and invasive pulmonary disease with fulminant course, as did the twins. Risk factors for our patients included maternal vaginal colonization, vaginal delivery and extreme prematurity. In our cases blood cultures were sterile, as is the case in 67% of EOC, and diagnosis was confirmed by isolation of fungi in otherwise sterile sites such as umbilical catheter tips. Antifungal therapy was not instituted since diagnosis was delayed and both neonates died.
Conclusion: EOC should be included in differential diagnosis of early onset sepsis in ELBW neonates, considering maternal history, severe clinical picture and the characteristic dermatitis and prompt systemic therapy should be instituted if outcome is to be improved.
P-05-019 Group B streptococcus prevalence in diabetic pregnant women
D. Tutunaru, R. Vladareanu, S. Constantinescu, A. Veduta, F.D. Lebit
Elias Emergency Hospital, Bucharest, Romania
Aim: To investigate the influence of maternal diabetes on the prevalence of group B streptococcus during pregnancy.
Methods: Prospective, nonrandomized, group controlled study. Inclusion criteria: In the study group were recruited 47 pregnant women with both pregestational and gestational diabetes mellitus, who were matched by age, parity and gestational age with 144 pregnant women normal carbohydrate tolerance. Exclusion criteria: PROM and STD. Culture specimens for group B streptococcus were obtained in 36th week of gestation from the vaginal fornix and from cervical external ostium. Two-tailed unpaired Student t test, Mann-Whitney U test, and chi2 test were used. Multiple logistic regression analyses were performed to evaluate the independent influence of maternal diabetes on the prevalence of group B streptococcus positive culture.
Results: Study group showed a higher prevalence compared to control group (47.3% vs. 19.5%). The colonization rate of group B streptococcus in pregestational diabetic women was 57.8% compared to patients with gestational diabetes, where it was 32.1% (P = .05).
Conclusion: Glucose intolerance seems to be a serious risk factor for group B streptococcus colonization in pregnancy.
P-05-020 Complications of perinatal infection
A. Mitreski1, M. Bogavac2
1Unit of Obstetrics and Gynecology “Minerva”, Novi Sad, Serbia and Montenegro; 2Clinical Centre, Department of Obstetrics and Gynecology, Novi Sad, Serbia and Montenegro
Aim: To evaluate incidence of complications of pregnancy during present infection in the vagina.
Material and Methods: During last two years in our private practice we followed up 364 pregnancies. All patients were screened for presence vaginal infection by vaginal, cervical and special smears for different microorganisms. We also performed testing on TORCH, adeno, coxackie, influenza and parvo B19 viruses, evaluation of WBC and CRP. Pregnancies were followed up by ultrasound.
Results: Among followed pregnancies we registered in 56 (15.38%) patients presence of vaginal infection, in 22 (6.04%) different respiratory infections, in 27 (7.41%) TORCH findings were positive and in 23 (6.32%) infection of urinary system was found. In total, various form of infection was detected in 118 (32.42%) patients. In this subgroup of patients incindence of pregnancy complications was as following: 43 cases of imminent premature labour (only 9 (7.63%) delivered before 37th week of pregnancy), 3 cases of premature rupture of membranes, one followed by intrauterine fetal death. In one patient after viral infection during early second trimester hydrocephalus was detected. In few other patients we detected isolated congenital anomalies, without genetic disorder (acrania, shortening of tibulo-fibular complex with anomaly of the foot, oesophageal atresia, facial cleft, abdominal cyst). Incindence of fetal congenital anomalies was 1.83%.
Conclusion: Present perinatal infection can cause different complications of pregnancy, such as miscarriage, premature rupture of membranes, premature labour, intrauterine growth retardation, intrauterine fetal death, or be involved in genesis of congenital anomalies. Adequate treatment includes administration of antibiotics and other medications, depending on the complication infection had provoked.
P-05-021 Neonatal mortality in very low birth weight premature newborns with the antecedent of clinical chorioamnionitis
S. Salcedo, F. Castillo, C. Ruiz, J. Sanchez de Toledo, L. Cabero
Hospital Materno-Infantil Vall d'Hebron, Barcelona, Spain
Objective: To analyze the neonatal consequences and mortality of our premature patients with the antecedent of clinical maternal chorioamnionitis (CoAm) when the prenatal administration of steroids and postnatal administration of surfactant are routinely practices in our hospital.
Methods: We analyzed the data of 599 newborn patients of <35 weeks gestational age (GA) and ≤1500 g birth weight (BW) attended in our hospital between 1.01.99 and 30.6.02. Median of GA: 29 weeks (range: 23–34); median of BW: 1080 g (range 310–1490). In 123 patients (21%) the antecedent of CoAm was present. In 529/599 patients (88.3%) prenatal maturation with betamethasone was induced.
Results: The mortality rate in the whole population was 93/599 (15.5%); 66/472 (14%) patients died in the group without the antecedent of CoAm and 27/123 (22%) patients died in the group with this antecedent. The mortality rate in the group of ≤27 weeks GA was 39.7% in the patients with CoAm vs. 31.7% in the patients without CoAm. No mortality was observed in the group of 55 patients with the antecedent of CoAm and >27 weeks gestational age vs. 27 deaths (7, 5%) in 360 patients without the antecedent of CoAm and >27 weeks GA (p < 0.001).
Conclusions: It is possible that the antecedent of clinical maternal CoAm may be associated with better survival rate in very low birth weight premature babies (GA > 27 weeks) as has been recently described in the literature in the case of histological chorioamnionitis (Dempsey E et al. Am J Perinatol 2005).
P-05-022 Carriage of group B streptococci in Swedish parturients: A national study of obstetric and bacteriological characteristics
S. Hakansson
Department of Pediatrics, University Hospital, Umea, Sweden
Background: There is a need to delineate the impact of perinatal GBS morbidity, and to determine Swedish guidelines for prevention of early onset GBS (EOGBS) disease.
Aim: 1) To investigate GBS carriage in parturients and to study characteristics of pregnancy and parturition in relation to vaginal/rectal GBS-colonisation, 2) determine transfer rate of GBS to the infant, and 3) to map serotype distribution in GBS isolates.
Method: A population-based sample of 1579 women fulfilled the protocol. A swab from vagina/rectum was obtained before birth, and one for detection of surface colonization was obtained from the infant soon after birth. A data form pertaining to pregnancy and delivery was completed. Bacterial samples were processed in one lab using selective, enrichment media. All GBS isolates were serotyped.
Results: GBS carriage rate was 25.3%. It was not increased in urban areas, nor influenced by maternal age or smoking. In women with parity ≥3, an increased proportion was GBS-positive (OR 1.7; 1.1–2.7). GBS in urine during pregnancy predicted an increased risk for GBS colonisation at parturition (OR 2.5; 1.5–4.2). The occurrence of obstetric risk factors was: ROM ≥ 18 h = 14%; preterm birth = 6.5%; temp during labour ≥38°C = 4.2%.
In GBS-positive women the infant colonisation rate was 56%, and 3.6% in infants of those who were GBS-negative. The infant colonisation rate was not influenced by the duration of ROM. A total of 596 GBS-isolates the distribution of serotypes was: Ia = 11%; Ib = 13%; II = 15%; III = 24%; IV = 16%; V = 18%; VI = 0.4%; VII = 0.7%; VIII = 0%, NT = 2.2%.
Conclusion: The prevalence of GBS-carriage among women and the infant transfer rate, was in the higher interval of figures previously reported. Notably, the prevalence of serotype Ia was comparatively low, whereas serotype IV was more frequent. Mothers, who were GBS-negative with a GBS-positive infant, probably had a falsely negative test. The corrected colonisation rate in parturients would therefore be around 30%.
Balancing the benefits and potential risks of an increased use of intrapartum antibiotics, the design of an appropriate national prevention strategy should consider the total burden of EOGBS disease, and be based on data regarding prevalence of GBS-carriage, infant colonisation rate, and obstetric risk factors.
P-05-023 Neonatal morbidity in very low birth weight premature newborns with the antecedent of clinical chorioamnionitis
A. Fina, S. Salcedo, F. Castillo, C. Ribes, J. Sanchez de Toledo
Hospital Materno-Infantil Vall d'Hebron, Barcelona, Spain
Objective: To analyze the morbidity of our premature patients and the neonatal consequences of chorioamnionitis (CoAm) when the prenatal administration of steroids and postnatal administration of surfactant are routinely practices in our hospital.
Methods: We analyzed the data of 599 newborn patients of <35 weeks gestational age (GA) and ≤1500 g birth weight (BW) attended in our hospital between 1.01.99 and 30.6.02. Median of GA: 29 weeks (range: 23–34); median of BW: 1080 g (range 310–1490). In 123 patients (21%) the antecedent of CoAm was present. In 529/599 patients (88.3%) prenatal maturation with betamethasone was induced.
Results: The antecedent of CoAm increases the risk of arterial hypotension during the first 72 hours of life (44% vs. 31.7%), patent ductus arteriosus (30.6% vs. 22%), intraventricular haemorrhage (37.4% vs. 25.6%), periventricular leukomalacia (17% vs. 11.5%), necrotizing enterocolitis (16.2% vs. 12.8%) and increases the indication of high frequency ventilation (22% vs. 10.4%), nitric oxide (12.2% vs. 6.6%), administration of surfactant (48% vs. 33%), administration of two or more doses of surfactant (20.3% vs. 13%), and dependency of oxygen at 36 weeks postmenstrual age (28.1% vs. 19.3%). All these differences are statistically significant.
Conclusions: The infectious and inflammatory consequences (transplacental passage of inflammatory mediators) of clinical maternal chorioamnionitis may adversely affect the neonatal adaptation of premature babies under 35 weeks gestational age.
P-05-024 Toxoplasma gondii seroconversion during the pregnancy in a university clinic from eastern part of Turkey
K. Dogan1, A. Kafkasli1, M. Atanbay2, L. Karaoglu3
1Inonu University School of Medicine Department of Obstetrics and Gynecology, Malatya, Turkey; 2Inonu University School of Medicine Department of Parasitology, Malatya, Turkey; 3Inonu University School of Medicine Department of Public Health, Malatya, Turkey
Objective: We aimed to evaluate the Toxoplasma Gondii seroconversion in each trimester of the pregnancy.
Methods: Pregnant women in the first trimester attempted to Inonu University Obstetrics Clinic and pregnant women in the third trimester of pregnancy attempted to the emergency room from April, 2004 to October, 2005 were recruited. Blood samples were drawn from 153 pregnant women at every trimester and from 159 pregnant women at their 3 trimester of pregnancy for serological testing. Toxoplasma gondii specific IgM and IgG were analyzed by Enzyme-linked Immunosorbent Assay (ELISA) and Indirect Fluorescent Antibody Test (IFAT). Cord blood samples were collected immediately after delivery and Toxoplasma gondii specific IgM and IgG were evaluated with the same serological tests.
Results: Mean maternal age was 28.1 ± 5.2 (16–42) years. Toxoplasma gondii specific IgM was not detected in any of the patients. Specific IgG was positive in 35.9% of the pregnants in each trimester. Also, the rate of IgG positivity was 37.5% in the third trimester of the pregnancy who were attempted to the emergency room. IgG seropositivity was significantly correlated with raw meat consumption and the soil exposure (p = 0.001 and p = 0.003 respectively).
All 312 cord blood samples were also seronegative for IgM. Parallel to maternal IgG seropositivity, the rate of IgG seropositivity was 37.5% in the cord blood samples.
Conclusion: A large amount of pregnant women are susceptible to toxoplasmosis in this part of Turkey. Prevention of congenital toxoplasmosis can be achieved by antenatal education.
P-06-001 Congenital heart anomalies in macrosomic newborns with prenatal immune system activation
I. Stojkovic-Eferica1, S. Sljivic1, M. Stojanovic1, B. Miljkovic1, B. Bjelakovic2
1Gynecology and Obstetric Clinic, Nis, Serbia; 2Clinic of Pediatrics, Nis, Serbia
Objective: The aim of this study was to show a possible connection between fetal/neonatal macrosomia, high frequency of congenital heart anomalies, accompagned by many others early neonatal problems and presence of a great number of different problems during pregnancy, apart from maternal glucose metabolism disorders. Also, to show disturbances in some immunological, hematological and biochemical parameters within this group of newborns.
Methods: Prospective study included 30 term newborns with birth weight up to p90 (3850g), from complicated pregnancies. Clinical examination was done during early neonatal period. Following laboratory parameters were analyzed: blood cells count, nitro-blue-tetrasolium test of peripheral blood phagocytes (NBT), serum immunoglobuline levels, glycemia, lactat-dehydrogenase (LDH) and creatine-phosphokinase (CPK) serum activities. Ultrasound examination of heart was performed. Statistical analyses: arithmetic mean and statistical significance have been used.
Results: All mothers had multiple and diverse problems during pregnancy and the most frequent were infections (93%), whereas only one of them had gestational diabetes. Different heart anomalies were discovered in even 53.3%, interventricular heart septum fibroses and thickening in 46.6%. All newborns had a lot of the others early neonatal problems. Laboratory findings showed: increased total IgM level at birth, increased absolute number of neutrophyles and monocytes, as well as, absolute number of NBT positive cells, increased serum activities of CPK and LDH (in 86.6% and 53.3% of cases respectively), transient hypoglycemia in 87.5%.
Conclusions: Increased total serum IgM level, exchanged evaluated immunological and hematological parameters indicated prenatal activation of fetal immune system. Maternal infection during pregnancy was the most frequent trigger of cytokines network disturbances at the level of feto-placental unit, with increased production of inflammatory cytokines and free radicals in developing tissues. These events may lead to alterated organogenesis and inadequate function of developing tissues. Increased iflammatory cytokines also could cause increased production of IGF 1 in fetal tissues, witch lead to fetal macrosomia in absence of maternal hyperglicemia and fetal hyperinsulinism.
P-06-002 The influence of hyperglycemia on ICAM-1 (CD54) and PECAM-1 (CD31) expression in human umbilical vein endothelial cells
M. Szczepanski1, M. Kamianowska1, M. Pietruczuk2, K. Wnuczko1, S. Wolczynski3
1Department of Neonatology, Bialystok, Poland; 2Department of Haematological Diagnostics, Bialystok, Poland; 3Department of Gynaecological Endocrinology, Bialystok, Poland
Background/Aims: Hyperglycaemia is a recognized primary factor responsible for endothelial dysfunction and microcirculatory changes in diabetic patients. There exist many reasons to claim that high glucose concentrations, influence on cellular expression of adhesion molecules, thereby mediating in endothelial interaction of leucocytes. In the present study, we examined effects of high glucose concentrations on ICAM-1 and PECAM-1 expression in human umbilical vein endothelial cells.
Methods: Human umbilical vein endothelial cells were cultured in a standard medium (M 199); the culture cells were incubated for 48 hours with a different concentration of glucose (5.55 mmol/l, 11.1 mmol/l, 22.2 mmol/l). Expression levels of ICAM-1 and PECAM-1 in the HUVEC were quantified by flow cytometry.
Results: In the control culture cells (5.55 mmol/l of glucose) expression of ICAM-1 and PECAM-1 amounted to 20.9 ± 0.4 and 28.4 ± 0.6 respectively. In the conditions of hyperglycaemia (11.1 and 22.2 mmol/l) expression increased to 26.2 ± 3.3 and 44.8 ± 5.2 for ICAM-1 and to 29.6 ± 4.0 and 47.2 ± 4.8 PECAM-1 respectively and the differences were statistically significant (p < 0.05).
Conclusions: High glucose concentration increases ICAM-1 and PECAM-1 expression in human umbilical vein endothelial cells.
P-06-003 Neurological disorders in newborns and immune response
S. Sljivic1, I. Stojkovic-Eferica1, M. Stojanovic1, Lj. Brankovic2, R. Milicevic2, Lj. Mrkaic1, Z. Milosevic1
1Gynecology and Obstetric Clinic, Nis, Serbia; 2Clinic of Pediatrics, Nis, Serbia
Objective: Inflammatory mediators play important roles in normal central nervous system development and in the response of the brain to diverse forms of injury. Prenatal brain injures and alteration in the primitive reflex activity are closely associated with intrauterine infections and inflammatory response.
The aim of this study is to point out prenatal activation of the immune system in newborns with neurological dysfunctions, following hematological, immunological and biochemical parameters.
Methods: Thirty-nine newborns with altered sceletal muscle tonus and primitive reflex activity have been monitored. Physical and neurologic examination, ultrasound examination of central nervous system in newborns as well as mother's case-history have been practised. The following laboratory parameters have been analyzed: red and white blood cell count, hemoglobin and hematocrit level, peripheral blood smears, nitro-blue-tetrasolium test (NBT), serum immunoglobulin levels, lactate dehydrogenase, creatin phosphocinase (CPK).
Results: Ultrasound examination of central nervous system showed intracranial hemorrhage, periventricular leucomalation, cystes plexus chorioidei, cystes subependimalis, while in 10% the findings were normal. The results of laboratory examination have shown: increased absolute number of monocytes, neutrophyles and increased absolute number of NBT positive cells, increased level of immunoglobuline M and increased activity of CPK in the serum. In most of the cases, mothers suffered from acute and chronic disorders during or before the actual pregnancy.
Conclusions: The analyzed laboratory parameters, observed at birth, indicated activation of the immune system and prenatal microenvironment alteration, as well as pathophysiological background of altered skeletal muscle tonus of these newborns. The prevention of proinflammatory cytokine formation, at this stage, can interrupt the proinflammatory cascade and might limit the extent of irreversible injury of neonatal brain and other tissues.
P-06-004 Serum 3-Nitrotyrosine is elevated in neonates who develop infection
B. Fisarkova1, R. Vytasek3, M. Vizek2
1Department of neonatology, Faculty Hospital Motol, Prague, Czech Republic; 2Department of Pathophysiology, 2nd Medical Faculty, Charles University, Prague, Czech Republic; 3Department of Physiology, 2nd Medical Faculty, Charles University, Prague, Czech Republic
Objective: Oxidative stress is believed to play a key role in pathogenesis of specific diseases of prematurity – i.e. bronchopulmonary dysplasia, retinopathy of prematurity, periventricular leukomalacia. Appropriate marker of oxidative stress is still missing. One of a possible candidates is also 3-nitrotyrosine (3NTYR) formed by vivid reaction of NO and O2. The aim of our study was to determine 3NTYR concentration in serum samples from preterm neonates, to correlate them with their morbidity and to compare them with 3NTYR concentrations in full-terms.
Patients and Methods: Serial serum samples had been collected from 90 neonates (40 samples from umbilical cord blood, 120 from venous blood). We divided neonates into two groups – full-terms (64 neonates) and preterms (26 neonates). Data about their acute and chronic morbidity were collected. We used ELISA method with sensitive monoclonal antibodies developed in our laboratory to measure 3NTYR in serum.
Results: We found that in full-term and otherwise healthy neonates, 3NTYR concentration decreased during the first week, whereas in preterms did not change. We didn't find any relationship between concentration of 3NTYR and FiO2 in ventilated neonates. There was a significant increase in 3NTYR concentration in neonates with clinically and laboratory proved infection.
Conclusion: Concentration of 3NTYR in full-term neonates changed during few days, so dynamic of 3NTYR production and degradation in organism is probably much faster than it is believed. In neonates 3NTYR seems to be a marker of oxidative stress caused by inflammation rather than that caused by hyperoxia.
P-06-005 Twins developing arterial thrombosis in the early neonatal period: An elusive diagnosis?
P.Q. Le1, M. Alexander1, A. Messaaoui2, L. Dewulf2, J. Goedseels1, A.B. Johansson2, A. Ferster2
1Hopitaux Iris Sud Universite Libre de Bruxelles, Brussels, Belgium; 2Hopital Universitaire Des Enfants Reine Fabiola Universite Libre de Bruxelles, Brussels, Belgium
The protein C system consists of proteins C and S which are natural anticoagulants that regulate the cascade of coagulation. Their deficiency leads to a high risk of thrombotic events, particularly in veins but also in arteries.
We report the clinical cases of a pair of non identical twins. They were born at 37 weeks, after an uneventful pregnancy, in a level II maternity unit. Apgar scores were normal. Both developed the same clinical symptoms with different severity, early in the neonatal period. For the first, it was observed within minutes after birth that one leg was intensely cyanotic. A diagnosis of popliteal artery thrombosis in the right leg was suspected, and confirmed by Doppler Ultrasound. The other had distal necrosis of the second and third toe some hours after birth. The first one received fresh frozen plasma, and they were both transferred to the childrens' hospital where they received fibrinolytic treatment. Afterwards, both were given low molecular weight heparin at therapeutic doses. Screening for thrombophilia markers was normal in the parents and in one of the boys. However, the protein S was low in the second boy. Clinical evolution at discharge was good for both. It is planned to further monitor thrombophilia markers of the twins at a later date.
The present case raises different questions about diagnosis and treatment of protein S deficiency. Indeed, there is no consensus on the normal value of protein S in the newborns, and on the other hand, there are no guidelines for prophylactic treatment in this disorder, in term of which drugs to use and how long to use them.
P-06-006 Lower levels of macrophage migration inhibitory factor (MIF) in tracheobronchial aspirate fluid (TAF) of VLBW with intrauterine systemic inflammation
W. Thomas1, S. Seidenspinner1, N. Kawczynska-Leda2, B.W. Kramer1, M. Chmielnicka-Kopaczyk3, A. Marx4, M. Szymankiewicz2, J. Gadzinowski2, C.P. Speer1
1University Children's Hospital, Wurzburg, Germany; 2Department of Neonatology, University of Medical Sciences, Poznan, Poland; 3Department of Pathology, University of Medical Sciences, Poznan, Poland; 4Department of Pathology, University of Wurzburg, Wurzburg, Germany
Objective: MIF is a proinflammatory cytokine produced by a variety of cells, including macrophages and the respiratory epithelium, and a pivotal mediator of the innate immune system. The objective of this study was to evaluate whether intrauterine inflammation might affect MIF concentrations in airways of VLBW infants.
Methods: TAF was obtained three times per day on day 1, 3, 5 and 7 of life from ventilated VLBW infants. Specimens were centrifuged and the supernatants stored at −80°C. Supernatants of one day were pooled and the MIF concentrations were measured by ELISA. The secretory component for IgA (SC) was used as reference protein. Placental tissue, membranes and umbilical cords of the VLBW infants were examined microscopically in order to distinguish three groups: chorioamnionitis, funisitis and control without inflammation.
Results: TAF of 35 infants (16 males) was examined. The mean gestational ages and birthweights (standard deviation) were 28.1 weeks (1.2) and 1073 g (189) for 13 controls, 26.8 (2.1) and 1089 (263) for 14 infants with funisitis and 26.6 (1.9) and 820 (197) for 8 infants with chorioamnionitis [p < 0.05 for birthweight].
Median values of MIF [ng/μg SC].
MIF on day 1 was lowest in the funisitis group [p < 0.01]. In the chorioamnionitis group it stayed relatively high on days 3–7 [p < 0.05; except control on day 3].
Conclusions: Our data suggest that intrauterine systemic inflammation of the fetus reflected by funisitis is associated with reduced concentrations of MIF in the airways of VLBW infants in the initial phase of postnatal life. Since MIF has a crucial role in innate host defense decreased concentrations of the mediator in TAF might predispose preterm infants for increased susceptibility to pulmonary infection which could rapidly become systemic.
P-06-007 Potential role of procalcitonin in the diagnosis of chorioamnionitis – preliminary report
J. Semberova, Z. Hodkova, Z. Stranak
Institute for the Care of Mother and Child, Prague, Czech Republic
Objectives: Procalcitonin (PCT) appears to be a highly sensitive and specific marker of the infectious stimuli. Chorioamnionitis (CA) is a severe infection responsible not only for premature birth but also for many severe neonatal diseases. The aim of the study was to investigate the role of PCT in the detection of CA.
Design and Setting: Comparative match-control study in tertiary perinatal centre.
Material and Methods: A prospective histological study of 45 placentas was performed. The serum levels of PCT, CRP (C-reactive protein) and total leukocyte count were measured in mother serum at the same time as short as possible before delivery (up to 2 hrs).
Results: Histological chorioamnionitis was positive in 11 cases (24%). Comparison of chorioamnionitis group (CA + ) and chorioamnionitis negative group (CA−) confirmed no statisticaly significant differences between both groups in gestational age, premature rupture of membrane duration, mode of delivery and obstetric history. We have found no statistically significant differences in PCT levels, CRP concentration and total leukocyte count.
Conclusions: These results suggest that PCT measurement might not be successful in the early detection of chorioamnionitis, but more data are necessary to establish this hypothesis.
Supported by grant IGA MH CR NR 7855-3.
P-06-008 What is the use of PCT, NPT, hCRP AND SAA in the diagnosis of neonatal infections?
D. Chovancova1, V. Parrak2, I. Hartmannova1, L. Divinec1, M. Majdan2, M. Skrakova3, L. Pejhovska1, M. Mistrik3, D. Fuchs4
1Neonatal Clinic of M. Rusnak Slovac Health University, Bratislava, Slovak Republic; 2Department of Clinical Biochemistry University Hospital, Bratislava, Slovak Republic; 3Department of Hematology and Transfusiology University Hospital, Bratislava, Slovak Republic; 4Biochemistry and Medical Chemistry University of Innsbruck, Innsbruck, Austria
Objective: During inflammation the production of procalcitonin (PCT), neopterin (NPT), C-reactive protein (hCRP-high sensitive) and serum amyloid A (SAA) are induced. The aim of the study was to compare these parameters in neonates who were suspected for bacterial infection and define their significance for the diagnosis of infection.
Methods: From January 2000 to December 2004 data of 150 newborns (25–42 g.w., birth weight 640–4400 g) treated in the Clinic of Neonatology of M. Rusnak suspected for infection were analyzed including PCT, NPT, SAA and hCRP. PCT was detected by quantitative immunochemiluminiscence (normal range < 0.5 ng/ml), NPT by ELISA (normal levels <15 nmol/l) – both by B.R.A.H.M.S. Diagnostica Germany, measurement of hCRP and SAA by nephelometry from DadeBehring Austria. All the parameters were checked in the umbilical blood of 104 healthy term neonates.
Results: PCT in infected neonates exceeded reference range of 2 ng/ml, with peak levels of 131.27 ng/ml. Concentrations of PCT in sepsis were greater than 10 ng/ml. PCT values fall more rapidly than hCRP. High increase of SAA (529.0 mg/l) together with increased NPT (28.8 nmol/l were detected in neonates with infection especially at the onset of infection.
Conclusions: PCT and SAA could in combination with hCRP be useful in diagnosis of infection and evaluation of antibiotic treatment.
P-06-009 Comparative study of two quantitative determination methods of C-reactive protein in blood
H. Chatziioannidis, P. Karagianni, G. Mitsiakos, C. Tsakalidis, D.G. Goulis, N. Nikolaidis
2nd NICU, Aristotle University of Thessaloniki, “Papageorgiou” Hospital, Greece
Background: The turbidometric (TUR) method of C-reactive protein (CRP) measurement is characterized by extent practicality, as it can be carried out in the Unit, with a very small blood quantity (20 μl vs. 1 ml) receiving the results quickly (2.5 min).
Objective: The aim of this project was the comparison of TUR method of CRP measurement with that of nephelometry (NEP).
Methods: The study included 163 samples of complete blood from 79 neonates treated in our Unit. CRP was measured in 97 samples of blood as routine (65 neonates, Group A) and in 66 samples of blood at neonates with clinical picture suspicious of infection (43 nurslings, Group B). The CRP TUR determination was performed by the technique Quick Read System, while the NEP with Beckman's company nephelometer.
Results: A statistically important difference was noted between the CRP levels in TUR and NEP methods (18.7 ± 22.6 mg/1 opposite 14.9 ± 20.7 mg/1 respectively p < 0.001). TUR and NEP methods were found in strong positive correlation (r2 = 0.945, p < 0.001). In Bland-Altman analysis a CRP over-estimate was noted with TUR method vs. the NEP, in prices up to 40 mg/1. With threshold 11 mg/1 the sensitivity and specificity of TUR method was 93% and 55%, respectively in relation to positive blood culture.
Conclusions: Fast CRP determination with TUR method appears to be reliable too, as it is characterized by high sensitivity and negative prognostic value.
P-06-010 ESBL-positive strains of klebsiella pneumoniae collected in the NICU
L. Kantor, M. Kesselova, M. Kolar, P. Sauer, D. Koukalova, J. Petrzelova, I. Vagnerova, I. Kohnova, K. Urbanek
Faculty of Medicine, Palacky University, Olomouc, Czech Republic
Objective: One of the problems of contemporary medicine is an increasing number of bacterial strains with hazardous phenotypes of resistance. This is also true for neonatal units where nosocomial infections caused by multiresistant bacteria pose a serious threat to newborns. The feared bacterial pathogens include Klebsiella pneumoniae strains producing AmpA Extended-Spectrum Beta-Lactamases. The study focused on the molecular biology characteristics of ESBL-positive strains of K. pneumoniae collected in the Neonatal Unit of the Teaching Hospital in Olomouc (NICU).
Materials and Methods: Clinical material from newborns hospitalized in the NICU was used to isolate and determine K. pneumoniae strains by standard identification procedures. Their susceptibility to antibiotics was tested using a dilution micromethod. A Double-Disk Synergy Test was used for phenotype determination of ESBL production. The bla gene coding ESBL production was demonstrated by PCR. Molecular biology characteristics of ESBL-positive strains utilized the genomic DNA isolation, XbaI restrictase digestion and PFGE differentiation. The acquired restriction maps of individual isolates were compared using the GelCompare software and their relationship was determined. The selection pressure of antimicrobial agents was assessed according to the absolute number of defined daily doses of individual antibiotics.
Results: During the monitored period, 112 K. pneumoniae strains were isolated in total. In 22 of them (19.6%), the TEM-type ESBL production was determined. ESBL-positive strains were only observed in upper respiratory tract and rectal swabs collected from newborns with no signs of infection. The molecular biology analysis showed that 21 ESBL-positive strains had an identical restriction profile, i.e. they were very likely to be identical.
Conclusion: The results presented above suggest that ESBL-positive strains of K. pneumoniae occurred in the NICU due to clonal and horizontal spread.
P-06-011 epidemiology of neonatal septicemia at a NICU. A comparative two period study (1996–2000 & 2001–2005)
G. Kafalidis1, M. Theodoraki1, G. Triantafyllidis1, E. Kapsabelli1, M. Savala2, I. Labadaridis1
1NICU, General Hospital of Nikea, Piraeus, Greece; 2Microbiology Department, General Hospital of Nikea, Piraeus, Greece
Background: Neonatal septicemias (NSs) occur frequently in neonatal intensive care units (NICUs) and are associated with substantial morbidity and mortality.
Objective: To describe the epidemiologic profile of NS at a NICU in two consecutive time periods.
Methods: A retrospective study of all cases with positive blood cultures during two time periods was performed.
Results: A total of 1504 neonates were admitted during the 1st period of whom 925 (61.5%) were term and 579 (38.5%) preterm. Out of 1530 neonates of the 2nd period 782 (51.2%) were term and 748 (48.8%) preterm. The positive blood cultures were 139 and 118 respectively.
a) There was a reduction on the incidence rate of septicemia from 9.2 to 7.2 per 100 admissions in our Unit.
b) An increased prevalence in the occurrence of septicemia among neonates of larger BW (>1500 g) was recorded (38.8% vs. 47.5%) along with a higher incidence of early-onset sepsis in the 2nd period (11.5% vs. 22.5%).
c) Insignificant (p > 0.05) differences were found in the overall frequencies of gram (+) and gram (−) bacteria between the two periods but an increase in the rate of fungal infections were recorded (2.2% vs. 5.9%).
Gram-positive bacteria were the most commonly isolated germs (52.3%), with coagulase-negative Staphylococus (36.4%) being the main pathogen and Group B Streptococcus remaining stable (1.4% vs. 1.7%). The frequencies of incriminating gram (−) bacteria significantly changed over the 10 yr span.
Conclusions: NS represent an important and frequent problem in neonates. Knowledge of the incidence of NSs allows the targeting and implementation of preventive strategies for reducing morbidity and mortality related to NS in an NICU.
P-06-012 Neonatal ureaplasma urealyticum respiratory colonization and bronchopulmonary dysplasia in very low birth weight infants
M. Arroyo, J. Perapoch, R. Bartolome, I. Benitez, S. Fina, S. Salcedo
Vall d'Hebron Hospital, Barcelona, Spain
Objectives: To determine the prevalence of Ureaplasma urealyticum (Uu) respiratory colonization in preterm newborns with birth weight below 1500 g, and the relationship between Uu colonization and the development of bronchopulmonary dysplasia (BPD) and atypical BPD forms.
Methods: From 115 preterm newborns born in a single hospital between February 1994–January 1996 and October 1999–May 2000, 101 surviving beyond 36 weeks of postmenstrual age were included in the study. Cultures from pharyngeal frotis and tracheal aspirates were weekly performed within the first 28 days of life. Variables that might influence on the development of BPD were collected prospectively. Univariate and multivariate analysis were performed using the SPSS statistical package.
Results: Nineteen patients (18.8%) developed BPD, 11 the typical and 8 the atypical form. The rate of global Uu colonization was 30.7%. Factors associated with typical BPD were low gestational age (OR: 0.20) and low birth weight (OR: 0.95). Factors associated with atypical BPD were, beside those two factors, chorioamnionitis (OR: 5.16), persistence of arteriosus ductus (PAD) (OR: 8.18) and Uu colonization (OR: 19.09). Cesarian section delivery was associated with lower incidence of atypical BPD (OR: 0.15). Multivariate analysis, however, disclosed PAD and Uu colonization as the only independent predictors of atypical BPD.
Conclusions: Preterm newborns developing typical and atypical BPD are different. PAD and Uu colonization are independently associated to the development of atypical BPD.
P-06-013 Serial C-reactive protein and sonography contribution to the management of a necrotizing enterocolitis outbreak
A. Zuasnabar1, I. Anquela1, V. Garriga2, B. Balsera1, V. Perez1, M. Abad1, M. Catala1
1Neonatal Unit, General Hospital Granollers, Granollers, Spain; 2Diagnostic Imaging, General Hospital Granollers, Granollers, Spain
Objective: To evaluate the contribution of serial CRP and abdominal US in diagnosis, staging and management of NEC during an outbreak in our neonatal unit.
Methods: 7 neonates (Case 1–7) were diagnosed of NEC (October 2005-January 2006): GA 32 weeks (30–36), BW 1.435 g (865–1820), M/F: 6/1, prenatal steroids 3/7, age onset 6.4 days (2–11). Enrollment criteria: 1) Clinical signs, blood chemistry, cultures and abdominal radiographs (7/7). 2) Serial CRP (7/7). 3. Serial color doppler US (5/7). Staging: IA (C6-7), IB (C2), IIB (C5), IIIA (C3-4), IIIB (C1). Management: feeding withholding, antibiotics, systemic stabilization, peritoneal drainage, surgery. According to a) Serial CRP: peak level 48 h and normalization. b) Serial US: pneumatosis intestinalis, portal venous gas, peristalsis, ascites, free air. Absence of bowel wall perfusion or thinning were indicative of necrosis. c. Progression of clinical signs and radiology.
Results: Stage I: M-CRP < 1 mg/dl (0–48 h). Rx: intestinal dilation. US (2/3) normal. Feedings restarted. Stage II: M-CRP 7.7–2.2 mg/dl (0–48 h). Rx: intestinal dilation. US no pneumatosis or portal gas. Feedings restarted after CRP normalization. Stage III: M-CRP 0.9–16.6 mg/dl (0–48 h). Rx: pneumatosis (3/3), portal gas (C2), free air (C1). US (C2-3): pneumatosis, portal gas, ascites. No bowel wall ischemic compromise. Outcome: C1 dead 4 h later. C2 transferred: intestinal resection 36 h later. C3 transferred: immediate peritoneal drainage, no surgery.
Conclusions: Serial CRP and abdominal US monitoring are useful in diagnosis and staging of neonatal NEC. Color doppler US findings permit a less aggressive and prompt intervention in relation to better staging. Normal wall thickness and perfusion are valuable information.
P-06-014 Analysis of causative organism and choice of antibiotics according to the onset of neonatal sepsis
Y.Y. Choi, J.S. Sung, S.H. Kim
Chonnam University Hospital, Gwangju, South Korea
Objective: The incidence of neonatal sepsis is still not decreased because of increased invasive procedure associated with high risk neonates. We analyze the causative organisms and its antibiotic sensitivity according to the onset of neonatal sepsis.
Methods: 83 patients with neonatal sepsis who admitted to NICU from Jan. 2000 and Dec. 2004 were enrolled. Isolating organisms from blood culture, gestational age, birth weight, sex, risk factors, clinical manifestations and antibiotic sensitivity were collected.
Results: The incidence of neonatal sepsis was 1.7% and male to female ratio was 1:1.3. Neonatal sepsis was more prevalent in premature and low birth weight infant (P < 0.05). Coagulase negative Staphylococcus was most common and then Candida, S. aureus, etc. All Candida species caused the late onset disease. Gram positive organisms were sensitive to VM, teicoplanin and CM. Gram negative were sensitive to ciprofloxacin and imipenem.
Conclusions: Most common organisms were Coagulase negative Staphylo, Candida and S. aureus. The first choice of antibiotics was combination of the 3rd generation cephalosporin and clindamycin in early-onset, the 3rd generation cephalosporin and glycopeptide in late-onset. If there is no response to antibiotic treatment, the use of antifungal agent should be considered.
P-06-015 Early onset serratia marcescens infection: A case report
P. Saik1, L. Suvari2, A. Konks1, E. Saik2
1Department of Neonatology, West-Tallinn Central Hospital, Women's Clinic, Tallinn, Estonia; 2Department of Neonatology, Tallinn Children's Hospital, Tallinn, Estonia
Objective: Serratia marcescens is a rare bacterial agent which causes the early onset meningitis with brain abscesses and sepsis.
Methods: We present a case of neonatal meningitis and sepsis in twin sisters caused due to S. marcescens.
Results: The term (GA 38 weeks) twin girls were born from elective caesarean section, both of them had SGA (I girl birth weight 2105 g, II girl – 2135 g) and in good condition. In the first day of life the emergency problem did not occur.
<48 hour of life the first twin girls had symptoms: hyperthermia, irritability, high-pitched cry, pale, feeding disturbance. Her laboratory values indicated for increased WBC (27.7 × 109 cells/l), CRP (79.6 mg/l), low platelet counts. The cerebrospinal fluid leukocyte count was 4020 × 106/l. The antibacterial therapy was commenced with penicillin, gentamicin, cefotaxime. When the blood and CSF culture for Serratia marcescens became available, penicillin was stopped. On Day 7 the brain ultrasound multiple abscesses with average size 9–24 mm in the frontal, periventricular and occipital area were seen and the same picture on the cerebral CT scan. The antibacterial therapy was changed to meropenem was continued for 4 weeks.
The second twin girl became ill 52 hour of life with symptoms hyperthermia and irritability, her laboratory values: CRP 53 mg/l, platelet count 129 × 109 cells/l. Blood culture was positive for S. marcescens, CSF was normal and sterile. The antibacterial therapy was penicillin, gentamicin and tazocin.
Conclusions: Those patients represent a rare case of early onset Serratia marcescens meningitis with brain abscesses and sepsis in newborn twins what was successfully treated.
P-06-016 Neonatal sepsis from flavobacterium meningosepticum
A. Fotiou1, P. Salvanos1, F. Lazaraki2, G. Liosis1, G. Saroglou2, H. Salvanos1
1Neonatal Unit, Elena Venizelou Perinatal Center, Athens, Greece; 2Microbiology Department, Elena Venizelou Perinatal Center, Athens, Greece
Introduction: Flavobacterium meningosepticum is a nonmotile, oxidative, Gram (−) bacillus incriminated as a cause of serious infections in newborns, most commonly meningitis.
We present a full-term newborn boy of 3670 g, born by normal delivery that was transferred from the nursery to the NICU on the 2nd day of life due to cyanosis. Maternal history was clear.
At admission the baby was floppy, non reactive, pallid and cyanotic. Vital signs: SatO2 = 95%, grunting, HR = 145 bts/min, BP = 46/18 mmHg, Mean Pr = 26 mmHg.
Laboratory Results: Hypoglycemia (17 mg/dl), Blood Gas: metabolic acidosis with elevated lactic acid (150 mg/dl) which deteriorated gradually. Full blood count, CRP, SGOT and SGPT were unremarkable. PT = 59.7′′ aPTT = 102.8′′ INR = 5.23 Fibrinogen = 95 mg%. CSF results: WBC 15/mm3, gluc = 8 mg/dl, protein 40 mg/dl. CXR, ECHO and U/S of upper and lower abdomen showed no pathologic results. Blood, CSF culture and amino acid blood test were taken.
Management: Management of shock (IV fluids and Dopamine), administration of antibiotics (Ampicilline, Gentamicine and Cefotaxime) and respiratory support (initially n-CPAP and then SIMV). Peritoneal dialysis was used to deal with the acute renal failure and blood and FFP transfusions to treat the DIC.
Despite the intensive treatment, death occurred 19 hours after admission.
24 h after death, the blood and the CSF culture detected Gram-negative bacillus Flavobacterium meningosepticum, resistant to all antibiotics tested except Vancomycine. Mother's vaginal secretion culture was negative. Environmental cultures from water taps, suction devices, sinks, faucets, antiseptic solutions, thermometers storage solutions from the delivery room and the nursery were negative.
Comments: This case is reported for the rarity and the multi resistibility of Flavobacterium meningosepticum.
P-06-017 Neonatal sepsis by herpes simplex virus (HSV) with fatal outcome in three cases
J. Arnaez Solis, M.A. Caballero, M. Navarro, E. Valverde, J.I. Rodriguez, J. Perez, J. Quero
Pediatric University Hospital La Paz, Madrid, Spain
Objective: To describe the clinical peculiarities of three newborn infants who died due to a sepsis by HSV along the year 2005 in a 3rd level hospital with 10,350 live borns this year. This represents a much higher incidence than that previously diagnosed in clinical or necropsy studies in our centre.
Methods: Retrospective study with review of the clinical records.
Results: The three neonates were born at term, one of them by caesarean section. One of the mothers had a probable herpetic genital lesion. Clinical signs started before 7 days of age in all three cases (two of them at 3rd day). All of them showed fever. Initial investigations showed leukocytosis in two patients though none of them had elevated immature forms. Treatment with ampicillin and gentamicin was started at admission in two cases, and cefotaxime added 48 hours later due to clinical worsening status. No oral or vesicular skin lesions were noted and bacterial cultures were negative in all of them. The first case had an episode of sudden gastrointestinal bleeding the 5th day of admission and died due to hypovolemic shock; no HSV infection was suspected. Another patient died, on the 14th day, due to a necrotizing pneumonitis in spite of starting acyclovir the 6th day of admission. The last patient developed a fulminant hepatic failure with fatal outcome; acyclovir was started four hours before death. The three neonates had coagulopathy and hypertransaminasemia. Postmortem findings revealed disseminated HSV infection, and positive immunoperoxidase staining for HSV. Cerebrospinal fluid PCR for HSV was negative in the two cases analyzed but it was positive for HSV type I in the blood of one of the two.
Conclusions: 1) The persistance of fever in spite of antibiotics, hypertransaminasemia and coagulopathy, were common findings. 2) Viral etiology should be investigated and VHS treatment with acyclovir considered if signs of infection persist, bacterial cultures are sterile and/or there is no response to broad-spectrum antibiotics even in the absence of obstetric antecedents, or vesicular skin lesions.
P-06-018 Neonatal plasmodium vivax malaria
J. Arnaez Solis1, S. Aguilera2, O. Busto2, J. Gomez3, J.P. Lopez4, R. Mendoza3
1Pediatric University Hospital La Paz, Madrid, Spain; 2Navarra University Hospital, Pamplona, Spain; 3Gregorio Maranon University Hospital, Madrid, Spain; 4Jacaltenango General Hospital, Jacaltenango, Huehuetenango, Guatemala
Objective: To describe a case of neonatal paludism probably acquired by vertical transmission during the last week of gestation. The newborn had a negative thick blood smear at birth.
Methods: Retrospective study with review of the clinical records.
Results: A 19-day old neonate was taken at the hospital emergency department after 12 hours of fever. Physical examination showed jaundice and hepatosplenomegaly. Laboratory workup was notable only for hemoglobin (11.4 g/dl), immature forms with normal white cell count and positive thick blood smear for Plasmodium vivax. He was treated with chloroquine and primaquine.
The mother, aged 28 years, was not controlled during her pregnancy. She sought care at the emergency department because of fever and jaundice four days before the delivery. On physical examination jaundice and stertors were observed; therefore, treatment with cephtriaxone, aerosoltherapy and intravenous hydratation was initiated. The laboratory tests showed normal white cell count but with high proportion of inmature forms and hemoglobin of 12.2 g/dl. She had fever during her stay and a thick blood smear done the 4th day after admission was positive for Plasmodium vivax. A caesarean was performed shortly thereafter due to worsening of clinical status. After the caesarean, she started treatment with choloroquine and primaquine. The patient's brother, aged 3 years old, was also admitted with the diagnosis of Plasmodium vivax paludism. The newborn, at term, had normal laboratory tests and the thick blood smear was negative 24 hours after birth, and was sent home three days later.
Conclusions: A negative result in the malaria tests performed at a newborn with high suspicion of vertical transmission does not exclude a malaria diagnosis and clinical signs, like fever or jaundice, have to be observed in order to repeat the tests if necessary.
P-06-019 Correlation between the sensitivity of microbial species derived from haemocultures of neonates from NICU and antibacterial treatment
P. Stratulat, A. Curteanu, L. Crivceanski, A. Maguliciac
Mother and Child Healthcare Research Institute, Chisinau, Moldova
Aim: To assess the sensitivity of the microbial germs derived from haemocultures of neonates to the most frequently used antibiotics in the NICU.
Methods: During the period of 2002–2004, we observed 614 neonates: 383 infants from the maternity NICU and 231 babies from the NICU for premature neonates having birth weight under 1500 g. The sensitivity of the microbial species derived from haemocultures was tested to penicillin, cephalosporin, aminoglycoside, and fluroquinolone antibiotics, representatives of erythromycin and chloramphenicol, etc. One haemoculture sample was taken at admission and another one 48–72 hours after admission.
Results: Out of the 614 neonates hospitalized in both units, 198 (30.78%) infants were born at term, and 416 (69.22%) – prematurely. In the NICU the following diagnostic, therapeutic interventions and care were provided: intubation – 98 (15.9%); exsanguinotransfusion – 18 (2.9%); catheterization of the umbilical vein – 177 (28.8%); intra-venous infusions – 478 (77.8%); feeding by nasal-gastric tubes – 215 (35%); parenteral feeding – 92 (14.9%) children. The blood in the neonates from both units was contaminated mostly by coagulase-negative staphylococci and Gram-negative organisms (Baccilus, Enterococcus, Ent. aglomerans, Kl. pneumoniae, E. coli, etc). The germs depicted in the haemoculture of the neonates from the maternity NICU were most sensitive to: ciprofloxacin, erythromycin, oxacillin, cefazolin, netilmicin, ampicillin, gentamicin, while those obtained from the infants from NICU for premature infants having the birth weight less than 1500 g were sensitive to ciprofloxacin, cefotaxime, gentamicin, medicamicin, and ceftriaxone.
Conclusions: Considering that the cultivated microbial species showed low sensitivity to ampicillin and gentamicin, and high sensitivity to ciprofloxacin and cefazolin (in both units), I–III generation cephalosporin antibiotics, medicamicin (macropen) and to netilmicin followed by gentamicin, the antibacterial treatment in the infants hospitalized in NICU shall be prescribed based on the antibioticogram results.
P-06-020 Neonatal group B streptococcal disease in northern part of Estonia
E. Saik1, P. Andresson2, K. Margus2, P. Saik3
1Department of Neonatology, Tallinn Children's Hospital, Tallinn, Estonia; 2Department of Delivery, East-Tallinn Central Hospital, Women's Clinic, Tallinn, Estonia; 3Department of Neonatology, West-Tallinn Central Hospital, Women's Clinic, Tallinn, Estonia
Background: Streptococcus agalactiae or group B streptococcus (GBS) is the most frequent cause of serious bacterial sepsis.
Objectives: No summarized data existed on neonatal GBS infection incidence in Estonia before GBS prevention program was initiated in the Northern part of Estonia in 2000. This study was initiated with the aim to establish the incidence of neonatal GBS disease in newborns, as well as to assess its risk factors and clinical features.
Methods: We analyzed retrospectively the neonatal cases of GBS disease in different hospitals of Tallinn over the period of 1.1.2000 to 31.12.2005.
Results: 53 cases were reported: 26 cases of invasive disease, incidence of 0.6/1000 live births, 27 cases of probable GBS infection, incidence of 1.2/1000. 96% of the neonates had early-onset disease (EOGBS). The mortality rates were 3.7%.
84% had perinatal risk factors; maternal GBS colonization/bacteriuria 74%, 21% of the mothers had premature rupture of membranes, 26% of the mothers were febrile. Predominant clinical symptoms were the following: respiratory 75%, cardiovascular 32% and neurological 37%. Laboratory findings: 91% had significantly elevated CRP, 26 neonates had culture-verified GBS septicaemia/meningitis, deep ear swab (<6 hour of life) was positive in 33 cases, 17% had pneumonia.
Conclusions: The incidence of invasive neonatal GBS disease in North Estonia is 0.6 cases per 1000 live births, which is relatively low. 96% of the cases had EOGBS. Respiratory symptoms are early clinical signs of EOGBS (75%), elevated CRP is the dominant laboratory marker for invasive GBS.
P-06-021 The most common causes of the neonatal sepsis
B. Vasiljevic1, O. Antonovic1, S. Maglajlic-Djukic2, M. Gojnic1, A. Glisic1
1Institute of Gynecology and Obstetrics – Clinical Centre of Serbia, Department of Neonatology, Belgrade, Serbia; 2University Children's Hospital, Belgrade, Serbia
Background: Neonatal sepsis is one of the most common causes of neonatal morbidity and mortality.
Objective: To investigate the most common organisms causing neonatal sepsis in our area and to assess appropriate empiric antibiotic therapy.
Methods: In our retrospective study all infants who were born in our Institute in 2002 were included. We were investigating the organisms causing early-onset sepsis (EOS) and late-onset sepsis (LOS) and antibiotic resistance these pathogens.
Results: Gram-negative organisms were the most frequent causes of EOS where Gram-positive organisms were responsible for the majority of LOS. Gram-negative pathogens (E. coli 40% and Klebsiella 40%) were the most common causes of EOS. Gram-positive pathogens (especially CONS 45%) were the most common causes of LOS. Ampicillin-resistance (80%) were very high degree in EOS, moderate degree resistance to amikacin (15%) and low degree resistance to cephalosporins (3%). Cephalosporins-resistance (66%) were significant in LOS, where were low resistance to combine therapy with carbapenems and vancomycin (9%).
Conclusion: Gram-negative organisms are the most common causes of neonatal sepsis and also a major causes of mortality. Incidence of antibiotic resistance continues are increasing, especially ampicillin-resistace in EOS and cephalosporins-resistance in LOS. Local monitoring of bacterial epidemiology and antibiotic resistance is crucial to determine appropriate initial antibiotic therapy.
Keywords: Early-onset neonatal sepsis, late-onset neonatal sepsis, Gram-negative pathogens, Gram-positive pathogens, antibiotic resistance
P-06-022 The analysis of development of 34 newborn children with body weight of less then 750 g
K. Kornacka, A.T. Kolodziejska
Neonatal Department of Warsaw Medical University, Warsaw, Poland
This report shows the analysis of development of 34 newborn children with body weight of less then 750 g. They were analyzed regarding to the physical development (body weight, body length, head perimeter), psycho-movement development, frequency of appearance of perturbation CNS, respiratory system diseases, eyes and ear perturbations.
It is concluded, that physical development, as well as psycho-movement development of newborn children with weight equal or less than 750 g during their first months of living is not regular. Their body growth and body weight is smaller, as well as head perimeter. Development of movement skills is delayed for 2 months in relation to “rectified age” and the norm is reached in most cases after about 24–30 months of living. It is also verified that the care of that children should refer to the recognition of the development problems as soon as possible and to the initiation of the prophylactic and therapeutic actions.
P-06-023 Pharmacokinetcs (PK) and pharmacodynamics (PD) modelling in the NICU (the pregraduate education practise)
P. Pokorna1, O. Cerna1, J. Martinkova2, J. Chladek2, V. Vobruba1, V. Kredba1, P. Srnsky1, M. Sadlo1, F. Perlik3, J. van den Anker4
11st Faculty of Medicine of the Charles University and General University Hospital Prague, Prague, Czech Republic; 2Department of Pharmacology, Faculty of Medicine of the Charles University Hradec Kralove, Hradec Kralove, Czech Republic; 3Department of Pharmacology, Faculty of Medicine of the Charles University Prague, Prague, Czech Republic; 4Division of Pediatric Clinical Pharmacology, Children's National Medical, Medical Centre, Washington, Netherlands Antilles
Aim: The use of PK/PD models to optimize the use of antibacterial and analgesic drugs in the NICU will be discussed. For this goal case reports will be presented.
Methods: Case report 1 – A woman, whose pregnancy was complicated by maternal fever for which she was treated with a single dose of i.v. 2 g ampicillin intrapartum, delivered a female fullterm neonate with normal Apgar scores at 1.5 and 10 minute. After birth, the neonate developed respiratory failure and was intubated and mechanically ventilated. Neonatal septicaemia was suspected and treated with broad spectrum of antibiotics. Problem of PK/PD modelling of antibacterial agents (aminoglykosides) will be presented. Case 2 will present the difficulties of assessing pain in term neonates and will show an analytical simulation of PK/PD of the use of tramadol. Multicenter efforts (6 nurseries) in objectively measuring pain will be shown. Cases 3–4 will be used to demonstrate the use of Therapeutic Drug Monitoring of aminoglycosides in the NICU using population pharmacokinetics (computer program MW-Pharm) as a possible toll for individualized aminoglycoside dosing after the first dose of gentamicin.
Results: The responses to a lot of the Quiz-questions.
Conclusions: PK/PD modeling of antibacterial and analgesic agent is needed at the NICU but currently still has a lot of difficulties due to an increased PK and PD variability of neonates.
The Development Project was supported by Ministry of Education RP 406/1/e/P.
P-07-001 Maternal obesity and risk of stillbirth and neonatal death
A. Shah1, L. Kenny2, J. Sands3
1St. Mary's Hospital, Manchester, UK; 2Academic Unit of O & G, Manchester, UK; 3North West Perinatal Survey Unit, Manchester, UK
Objective: To investigate the association between maternal body mass index (BMI) at booking and the risk of stillbirth and neonatal death.
Methods: A population-based observation study at the University of Manchester. The study sample was drawn from the North Western Perinatal Survey, a population based database comprising total of 53,250 deliveries in the North Western Region between January 2004 and December 2004. Total of 30,167 (181 stillbirths and 78 neonatal deaths) singleton pregnancies with accurate information regarding height and weight recorded at the booking visit were included. The population was classified according to BMI as underweight (BMI < 20 kg/m2), normal weight (BMI 20–24.9 kg/m2), overweight (BMI 25–29.9 kg/m2) and obese (BMI 30 kg/m2). Main outcome measures were still birth and neonatal death.
Results: Maternal obesity (BMI (30 kg/m2) was associated with a nearly two-fold increase in the incidence of neonatal death compared with women with BMI < 29.9 kg/m2 (odds ratio = 1.66, 95% confidence interval [CI]: 1.0–2.75). There was a slight but non-significant increase in the incidence of stillbirth in obese women compared with women with BMI < 29.9 kg/m2 (odds ratio = 1.13, 95% CI: 0.79–1.62).
Conclusion: Maternal obesity increases the risk of stillbirth and of neonatal death. This study, to our knowledge the largest in Europe, highlights the association between maternal obesity and adverse fetal outcome and emphasizes the need for public interventions to prevent or reduce obesity in young women.
P-07-002 Protective effects of erythropoietin against ethanol-induced apoptotic neurodegeneration and oxidative stress in the developing C57BL/6 mouse brain
A. Kumral1, K. Tugyan2, S. Gonenc3, K. Genc4, S. Genc4, U. Sonmez2, O. Yilmaz5, N. Duman1, N. Uysal3, H. Ozkan1
1Dokuz Eylul University, Department of Pediatrics, Izmir, Turkey; 2Dokuz Eylul University, Department of Histology, Izmir, Turkey; 3Dokuz Eylul University, Department of Physiology, Izmir, Turkey; 4Dokuz Eylul University, Learning Resources Center Research Laboratory, Izmir, Turkey; 5Dokuz Eylul University, Animal Research Center, Izmir, Turkey
Objective: The developing central nervous system is extremely sensitive to ethanol, with well-defined temporal periods of vulnerability. Recent studies have shown that administration of ethanol to infant rats during the synaptogenesis period triggers extensive apoptotic neurodegeneration throughout many regions of the developing brain. Furthermore, acute ethanol administration produces lipid peroxidation in the brain as an indicator of oxidative stress. In recent years, it has been shown that erythropoietin (EPO) has a critical role in the development, maintenance, protection, and repair of the nervous system. In the present study, we investigated the effect of EPO against ethanol-induced neurodegeneration and oxidative stress in the developing C57BL/6 mouse brain.
Methods: Seven-day-old C57BL/6 mice were divided into three groups: control group, saline-treated group, EPO-treated group. Ethanol was administered to mice at a dosage of 2.5 g/kg for two times with a 2-h interval. Recombinant human EPO (rhEPO) was given 1000 U/kg. Twenty-four hours after the first dose of ethanol, all the animals were killed.
Neuronal cell death, apoptosis, thiobarbituric acid substance (TBARS) levels, superoxide dismutase (SOD), and glutathione peroxidase (Gpx) enzymes activities were evaluated.
Results: Histopathological evaluation demonstrated that EPO significantly diminished apoptosis in the cerebellum, prefrontal cortex, and hippocampus and also spared hippocampal CA1, CA2, and CA3 neurons. Simultaneous administration of EPO along with ethanol attenuated the lipid peroxidation process and restored the levels of antioxidants.
Conclusions: Regarding the wide use of erythropoietin in premature newborns, this agent may be potentially beneficial in treating ethanol-induced brain injury in the perinatal period.
P-07-003 Psychosocial aspects of mothers with high sodium levels in their breast milk and severe dehydration in their newborns: A case-control study
A. Ozbek1, A. Kumral2, T. Guvenir1, F.V. Tas1, N. Duman2, H. Ozkan2
1Department of Child Psychiatry, Izmir, Turkey; 2Department of Pediatrics, Izmir, Turkey
Background: Hypernatremic dehydration in newborns associated with high sodium concentrations in breast milk is a rare condition with severe morbidity and mortality. Elevated sodium concentrations in breast milk are accepted to be a manifestation of unsuccessful lactation. It is commonly associated with failure to establish the normal decrease in breast milk sodium concentration. In addition to biological reasons, maternal stressors were also held responsible for problems in lactation. This research aimed to evaluate the psychosocial aspects of mothers with no known biological reasons to account for the high sodium concentrations in their breast milk and associated hypernatremic dehydration in their newborns.
Method: Mothers of 21 exclusively breast fed term infants, admitting to the hospital between December 2002–August 2005 for hypernatremic dehydration and associated high sodium concentrations in the breast milk were included. The control group composed of mothers of 43 healthy term infants, with expected levels of sodium in the breast milk. The assessment of each mother included a semi-structured interview covering sociodemographic characteristics of the mothers, gestational history and maternal attitudes towards breastfeeding. Edinburg Postpartum Depression Inventory, State and Trait Anxiety Scales were administered to assess maternal depression and anxiety.
Results: Mean (SD) ages of the mothers with high and expected levels of sodium in their breast milk were 28.9 (4.5) years and 29.0 (4.4) years, respectively. There were statistically significant differences between the mothers with high sodium levels in their breast milk and the control group in the aspects of; suffering from a previous psychiatric illness (57.1% vs. 18.6%, p = 0.003), perception of the pregnancy as untimely (52.4% vs. 20.9%, p = 0.010), unplanned pregnancy (52.4% vs. 20.9%, p = 0.020) and perceiving herself as ineligible to be a mother (19.0% vs. 4.7%, p = 0.017). Significantly higher number of these mothers stated that they have experienced various stressful life events during the pregnancy (57.1% vs. 20.9%, p = 0.005). They also had higher state anxiety scores as compared to controls (Mean (SD) 42.2 (11.1) vs. 35.5 (10.5), p = 0.031).
Conclusion: This study demonstrates that mothers with elevated levels of sodium in their breast milk present more adverse psychosocial characteristics and higher levels of state anxiety compared to those with expected levels of sodium achieving successful lactation. These findings might also indicate that psychosocial factors have an important role in high sodium concentrations in breast milk.
P-07-004 Screening for celiac disease among post delivery women: Relation with low birth weight
G. Solis Sanchez, A. Rodriguez Fernandez, C. Blanco Cristobal, E. Fernandez Rodriguez, A. Suarez Gonzalez, F.J. Roman Llorente
Hospital de Cabuenes, Gijon, Spain
Objective: To calculate prevalence rate of undiagnosed celiac disease in north of Spain among post delivery woman, with or without low birth weight newborns.
Methods: Case-control prospective study. Personal interview and serologic determination of transglutaminase antibodies post delivery.
Cases: Mothers of newborns under 2500 g birthweight. Controls: Mothers of newborns over 2500 g birthweight. Sample size: 1103 mothers (577 cases and 526 controls). Number of newborns: 1195 (465 pre term, 730 term).
Results: Mothers mean age: 31.1 years. Origin: 92.7% native and 7.3% foreigner. Pathologic history: 38.5% (dermatology 15.3%, respiratory 8.3%, endocrinology 3.7%, neurology 2.9%, haematology 2.9%, gastroenterology 2.3%, …). Related celiac diseases: iron-deficiency/anaemia 12.7%, thyroid disease 2.4%, type I diabetes 0.5%, hypertransaminasemia 2.4%. Celiac clinical symptoms: diarrhea 3.3%, constipation 14.4%, recurrent abdominal pain 3%, emesis 1.3%. Celiac familiar history: 2%. No significative associations between related diseases or clinical symptoms among study groups. Four of 1103 mothers had serologic and biopsy confirmed celiac disease (Prevalence global rate: 0.36% or 1/275). Two of them were from case group (0.34%) and two from control group (0.38%). Seven women were IgA defficiency with IgG transglutaminase antibodies negative.
Conclusion: Celiac disease post delivery prevalence rate is 0.36% in north of Spain. We did not found statistic differences among mothers of under or over 2500 g newborns birthweight (Grant PI021422 from Fondo Investigación Sanitaria of ISCIII, Spain).
P-07-005 Weight gain in twin gestation: Does it make the difference?
A.C. Gomes Julio, A. Cordeiro, E. Dias, H.T. Simoes
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objective: To study the effect of weight gain per week on twin pregnancy outcome, in women with a normal pregravid body mass index (BMI).
Methods: We analysed 452 twin pregnancies in surveillance program, from January 1996 to December 2005, in Alfredo da Costa Maternity. We considered women with a normal pregravid BMI (20–29.9 kg/m2) and established two groups according to maternal weight gain per week (less than 0.55 kg/week vs. more or equal than 0.55 kg/week). Maternal age, parity, gestational age at delivery, mode of delivery, birth weight of the newborn and maternal complications of pregnancy (hypertensive disorders and gestational diabetes) were evaluated for each group. Pearson χ2 test and independent samples T-test were used for statistical analysis (SPSS 10.0, Inc.).
Results: The mean maternal age was 30 years (15–48; SD 4.7) and 54.1% of women were nulliparas. Mean weight gain was 16.6 kg (2–35; SD 5.9). Women with greater gains delivered heavier babies (2422 ± 465 g vs. 2283 ± 480 g, p < 0.01). However there was no difference in frequency of very low birth weight (VLBW, less than 1500g) or preterm delivery (before 34 weeks). Cesarean section was the most frequent mode of delivery in both groups (without differences between them). Hypertensive disorders were more prevalent in women with greater weight gains (p < 0.05).
Conclusions: We confirmed the association between maternal weight gain during gestation and newborn birth weight in twin pregnancies. Despite normal pregravid BMI, women with excessive weight gain are more likely to develop hypertensive disorders.
P-07-006 Effect of early pregnancy body mass index and gestational weight gain on newborn size
E. Farri-Kostopoulou, M. Deli-Stavropoulou, D. Dimitropoulou-Tagalaki, A. Moustogianni, I. Koulouras
General Hospital “St. Andrew”, Patras, Greece
Objective: The purpose of our study was to evaluate the effect of early pregnancy Body Mass Index (BMI = kg/m2) and pregnancy weight gain on infant birth weight.
Methods: We studied 512 healthy women with singleton uncomplicated term pregnancies and their infants. Data were recorded and analyzed using t-test and multiple regression analysis. Early pregnancy BMI was calculated from weight and height at 1st visit within 4–6 weeks postconception. Pregnancy weight gain was estimated from 1st weight and last weight before delivery. Based on BMI women were classified into three groups: I: Low BMI (LBMI ≤ 19.9), II: Normal BMI (NBMI = 20–24.9) and III: High BMI (HBMI ≥ 25).
Results: Our group distribution was: LBMI 90 (17.6%) women, NBMI 299 (58.4%) and HBMI 123 (24.0%). Vaginally delivered 403 (78.7%) and by C/S 99 (21.3%). Mean pregnancy weight gain was 13.4 ± 5.1 kg and interestingly there was no statistically significant difference between the groups. Women of LBMI were younger compared to NBMI (p = 0.05) and HBMI (p = 0.10) and had fewer previous children compared to NBMI (p = 0.09) and HBMI (p = 0.01). In the total sample positive correlation was found between birth weight and both pregnancy weight gain (r = 0.14, p = 0.00) and early pregnancy BMI (r = 0.17, p = 0.00). Group Analysis showed positive correlation between birth weight and weight gain only for NBMI (r = 0.16, p = 0.01) and HBMI (r = 0.18, p = 0.05), while positive correlation between birth weight and BMI existed only for NBMI (r = 0.16, p = 0.01). Finally LBMI mothers had lower birth weight infants compared to NBMI (p = 0.00) and HBMI (p = 0.00).
Conclusions: We found positive correlation between gestational weight gain and birth weight for women of NBMI and HBMI group, while BMI has a positive correlation with birth weight only for NBMI. The lower infant birth weight of LBMI mothers, despite a similar pregnancy weight gain in all groups, indicates that low early pregnancy BMI is a strong indicator of newborn size.
P-07-007 Cord blood leptin concentration in the aspects of the growing symmetry and somatic parameters of newborns from pomeranian regions
J. Wojculewicz, P. Kryger, J. Szczapa
Neonatal Department Medical University, Gdansk, Poland
Aim: Estimation of the leptin level in the umbilical cord blood in newborns born in Medical University of Gdansk in connection to their somatic parameters.
Objective: A cohort of 301 newborns was examined. We analysed their leptin concentration in the umbilical cord blood, antropometric measurements were also taken.
Methods: Samples of the umbilical cord blood were collected after birth and leptin concentration was analysed by standard RIA method.
Result: We stated significantly lower leptin level in prematures comparing to mature children. Taken birth weight into account, as a nutritional state criterium we affirm that the lowest leptin concentration was observed in <3000 g group. The highest level was observed in >4000 g group. Significantly higher leptin level was observed in female children. There were no differences in P.I. between premature and mature newborns. P.I. was significantly higher in male newborns.
Conclusions: Cord blood leptin level is directly proportional to gestational age and birth weight. It is greater in female newborns. See .
Table I. Leptine concentration in cord blood depending on the antropometric parameters of examined newborns cohort.
P-07-008 Growing symmetry and somatic parameters in relationship to cord blood leptin concentration of newborns born by normotensive and hypertensive mothers
J. Wojculewicz1, H. Jasiel-Wojculewicz2, P. Krygier1, J. Szczapa1
1Neonatal Department Medical University, Gdansk, Poland; 2Department of Hypertension and Diabetology, Gdansk, Poland
Aim: To estimate leptin concentration in umbilical cord blood in newborns born in Medical University in Gdańsk by hypertensive and normotensive mothers. In this group hypertension was induced by pregnancy. Objective: The cohort of 29 children and their hypertensive mothers (group 1) and 31 children delivered by healthy women (group2) was analysed.
Methods: Leptin concentration and antropometric measurements were taken. BMI was measured in all women.
Result: Significantly lower leptin blood concentration was estimated in group 1 (). These newborns had significantly lower weight and length at birthtime. There was no difference in PI between two groups. The average BMI value in hypertensive mothers was 32.98 ± 6.65 and was significantly higher than the same parameter taken from healthy women (28.09 ± 2.89). Complicated neonatal period was observed in 37.9% newborns. Only 19.4% newborns from the second group demonstrated such problems.
Conclusions: Newborns born from hypertensive mothers were lighter and shorter. Complications after birth were frequently observed in this group. Connection between leptin concentration in umbilical cord blood and birth weight was confirmed.
Table II. Leptine concentration in cord blood and the antropometric parameters of examined newborns' cohort.
P-07-009 Cord blood leptin levels in appropriately grown newborns
E. Farri-Kostopoulou1, G. Raptis2, A. Muzaki2
1“St. Andrew” General Hospital, Patras, Greece; 2Medical School, University of Patras, Patras, Greece
Leptin is a 16 kDa hormone encoded by the ob gene that regulates body weight and energy expenditure.
Aim: To evaluate leptin concentrations in cord blood of normal AGA (appropriate for gestational age, >35 wks) infants and its association with different parameters.
Methods: Leptin levels were measured by ELISA in cord blood sera of 289 AGA neonates born in our Maternity Unit. Descriptive data of mothers and neonates were collected and recorded. For statistical analyses the SPSS v.12 statistical package was used. And for correlation the Pearson correlation (one-tailed).
Results: In our 289 AGA newborns mean GA was 39.1 ± 1.2 wks, BWt = 3167 ± 304.3 g, Lt = 50.4 ± 1.9 cm, and HC = 34.1 ± 1.0 cm. Analysis by gender (F/M = 155/134) showed significant differences in all somatometric parameters with boys being larger (wt: 3235.9 ± 272.5 vs. 3107.5 ± 318.4, p = 0.001, Ht: 50.7 ± 1.0 vs. 50.2 ± 1.8, p = 0.001, HC: 34.4 ± 1.0 vs. 33.9 ± 1.0, p = 0.056). Descriptive statistics of mothers showed: mean age 26.7 ± 5.2 y, ht 163.1 ± 6.4 cm, wt 61.5 ± 11.56 kg, pregnancy weight gain 13.6 ± 5.0 kg, BMI (kg/m2) 23.1 ± 3.9. Mean serum leptin levels for the total group was 14.45 ± 16.7 ng/ml. Analysis of leptin levels by gender showed that female AGA newborns had significantly higher leptin levels than male AGA newborns (F/M = 16.2 ± 21.5/12.3 ± 8.0, p = 0.0360), while boys had significantly higher BWt than girls (p = 0.001). A positive correlation was found between leptin levels and GA for the whole group (r = 0.15, p = 0.005) and for boys (r = 0.15, p = 0.038) and girls (r = 0.16, p = 0.018) separately. There was no correlation between leptin and BWt or maternal BMI, but we found a negative correlation of leptin levels and pregnancy weight gain only for boys (r = −0.16, p = 0.032).
Conclusions: This data suggest that GA rather than birth weight influences leptin levels in healthy near term and term AGA neonates.
P-07-010 Reactivity of cord blood mononuclear cells against diabetogeneic autoantigens assessment as a tool in type 1 diabetes prediction
M. Cerny1, K. Bohmova3, I. Spalova2, P. Pithova4, P. Mendlova3, Z. Vrabelova3, D. Chudoba5, R. Brabec1, P. Zoban1, K. Stechova6
1Department of Neonatology, Prague, Czech Republic; 2Department of Obstetrics and Gynaecology, Prague, Czech Republic; 3Department of Paediatrics, Prague, Czech Republic; 4Department of Internal Medicine, Prague, Czech Republic; 5Department of Molecular Genetics, Prague, Czech Republic; 6Department of Paediatrics, 2nd Medical Faculty of Charles University and University Hospital Motol, Prague, Czech Republic
Objective: In type 1 diabetes (T1D) pathogenesis autoreactive T cells play the most important role and the immune response is regarded to be Th1 polarised. The aim of our study was to analyse cytokine production of cord blood mononuclear cells after stimulation with known diabetogeneic autoantigens by protein microarray analysis.
Methods: We examined production of typical Th1 (IL-2, IFN-γ, TNF-β), Th2 (IL-4, -5, -13) and Th3 cytokines (IL-10, TGF-β1) after stimulation with diabetogeneic autoantigens: GAD65 amino acids (a.a.) 247–279, a.a. 509–528, a.a. 524–543; hsp 277 a.a. 277–300, proinsulin a.a. 9–23, IA-2/R2 a.a. 853–872. Tested objects: 8 newborns with positive family history of T1D (marked as “relatives”, 6/8 infants of mothers suffering from T1D, 2/8 infants of fathers treated for T1D), all of them were well babies (average GA = 38 weeks). As a control 6 newborns with negative family history of T1D were examined (marked “controls”).
Results: In “relatives” group we observed higher basal levels of IL-2 (p = 0.05), IFN-γ (border p = 0.06) and TGF-β1 (p = 0.04). Controls had higher basal level of IL-6 (p = 0.04). After specific stimulation relatives had more intensive response in IL-2 (p = 0.05). Controls after specific stimulation produced rather Th3/2 cytokines as IL-10 (p = 0.04) and IL-13 (p = 0.02). The most stimulatory autoantigens were proinsulin and tyrosin phosphatase derived peptides.
Conclusion: Cytokine production (basal as well as poststimulatory) differs between “relatives” and control groups. “More risky” type of response was present within “relatives” group. This approach seems to be useful in T1D prediction, however, this observation needs verification in larger newborn cohort.
Supported by grant No. MZO 00064203.
P-07-011 Perinatal risk factors of IUGR
B. Milisavljevic1, N. Prekajski2, Lj. Dobric3
1Health Center, Subotica, Serbia; 2Institute of Neonatology, Beograd, Serbia; 3Ginekology Clinic, Novi Sad, Serbia
Background: Regulation of fetal growth is multi factor and complex. The purpose of this study was to identify maternal characteristics associated with IUGR to determine the prevalence of IUGR in full-term infants.
Materials and Methods: Prospective research was taken place at Neonatal Department in Health Center Subotica, in period of January to December 1999. Investigated group was 50 infants whose birth weight was below the 10-nth percentile according to local standards, and the control group was 30 infants with birth weight from 25-nth to 75-nth percentile.
Twelve parameters was examined in mothers: maternal age, parity, parents' occupation, marriage status, height, weight gain during pregnancy, BMI, illnesses during pregnancy, anemia, height blood pressure, smoking during pregnancy.
Analytic statistic methods we used were S-test and Pearson test.
Results: We found that maternal age, parity, parents' occupation don't have individual significant prediction on nutrition condition on infant at delivery, but mothers age over 26 were significant different in infants with IUGR (p < 0.025). IUGR infants had statistically significant difference (p < 0.005) mothers with height less than 170 cm and weight gain during pregnancy over 85 kg. Low BMI is a good predictor but his interaction with other risk factors is more significant.
Percent of mothers wit Milanese during pregnancy, anemia, systolic blood pressure lower than 110 mmHg and higher than 130 mmHg, dystolic lower than 70 mmHg and higher than 90 mmHg. Were statistically different in group with IUGR (p < 0.10).
Conclusion: We conclude that increased awareness of maternal age over 26, lower pre-pregnancy height, weight gain during pregnancy, illnesses with anemia, height blood pressure, included history of smoking during pregnancy, is critical to identifying infants at risk for IUGR.
P-07-012 Perinatal growth and associated risk to develop retinopathy of prematurity
K. Allegaert1, S. Vanhaesebrouck1, A. Debeer1, I. Casteels2, R. Devlieger1, C. Vanhole1
1Division of Mother and Child, University Hospital Gasthuisberg, Leuven, Belgium; 2Department of Ophthalmology, University Hospital, Leuven, Belgium
Introduction: Pre- and postnatal growth restriction are reported in literature to be risk factors to develop retinopathy of prematurity (ROP). We focussed on pre- and postnatal growth characteristics in a population of LBW survivors (<1500 g) in an attempt to discriminate between these growth related risk factors.
Methods: Clinical characteristics (birth weight, gestational age, intrauterine growth restriction and 50% increase from birth weight at day 42 (yes/no) in LBW infants were retrospectively collected. Clinical characteristics in survivors who developed major ROP (grade 3) during later stay were compared with neonates without major ROP.
Results: Observations on 157 survivors with a median birth weight 1060 (400–1500) g and a median gestational age 28 (24–36) weeks were available. 52/157 (33%) had growth restriction (<10th percentile) at birth and 25/141 (18%) had postnatal growth restriction (50% weight increase on day 42). During neonatal stay, ROP (any grade) was documented in 56/157 (36%) of which 29/157 (18%) ROP grade 3. Growth restriction at birth was a risk factor to develop grade 3 ROP (RR 1.9, 95% CI 1.04–3.4) while postnatal growth restriction (RR 1.2, 95% CI 0.5–2.9) was not associated with an increased risk to develop major ROP.
Conclusions: Growth restriction at birth is a risk factor to develop major ROP during later neonatal stay in LBW infants while insufficient (50% increase in birth weight) postnatal weight gain in the first 6 weeks of life can not be used as an indicator of increased risk to develop major ROP. We hereby confirm an earlier reported case-control observation Citation[1].
P-07-013 Is preeclampsia a risk factor for suboptimal neurodevelopmental outcome in growth restricted fetuses?
E. Eixarch, E. Meler, A. Iraola, F. Figueras, M. Palacio, B. Puerto, E. Gratacos
Department of Obstetrics and Gynaecology, Hospital Clinic, Barcelona, Spain
Objective: Describe and compare the perinatal and psychomotor outcome of fetuses with a neonatal weight below the 10th centile regarding the presence of preeclampsia.
Methods: From November 2002 to November 2003, data were collected from fetuses born beyond 24-gestational weeks with estimated fetal weight below the 10th percentile and with normal cerebro-umbilical ratio. Fetuses were stratified according to the presence preeclampsia defined by proteinuria >300 mg/24 and a blood pressure >140/90. We prospectively performed a neurological evaluation at 2 years of age. For that purpose, we used the 24-month Age-Stage Questionary® (ASQ®). In order to adjust for neonatal birth centile and gestational age at delivery a linear regression was performed for each ASQ dimension.
Results: See .
Regression analysis showed that after adjusting for neonatal birth centile and gestational age at delivery, the existence of preeclampsia resulted in a mean decrease of 2.5 (p = 0.78) points of communication centile, 3 (p = 0.65) of gross motor centile, 16 (p = 0.04) of fine motor centil, 13 (p = 0.1) of problem solving centile and 10 (0.2) of personal-social centile.
Conclusion: The growth restricticted fetuses with preeclampsia showed a worrse perinatal outcome with earlier delivery, more frequent caesarean section and, the most important, high percentage of significant neonatal morbidity. These fetuses have worse psychomotor outcome in five developmental areas with statistically differences in fine motor dimension.
P-07-014 Retinal detachment after laser photocoangulation for retinopathy of prematurity in AGA and SGA infants
G. Niktari, F. Anatolitou, G. Polalis, G. Spyropoylos, H. Pantazatoy, M. Xanthou
Agia Sophia Children's Hospital, Athens, Greece
Background: Infants born SGA (birth weight < 10th percentile for gestational age) have been reported to be at increased risk of developing sight-threatening ROP.
Objective: To compare the prevalence of retinal detachment after laser photocoangulation administration for infants with threshold retinopathy of prematurity (ROP 3) between SGA and AGA (birth weight >10th percentile for gestational age) infants.
Methods: Sixty-one neonates (33 boys and 28 girls), mean birth weight: 933.7 g, range: 600–1650 g and mean gestational age: 26.7 weeks, range 23–31 that were administered laser photocoangulation for ROP 3 during the years 2003–2005, were studied. Twenty-seven of those infants were admitted to this tetriary referral neonatal unit exclusively for this reason. Nine infants were SGA and 52 were AGA.
Results: Retinal detachment occurred to 3 infants. Two of those were SGA. The percentage of retinal detachment was 22.2% in SGA and 1.9% in AGA infants (p < 0.05).
Conclusions: SGA infants had an increased risk of developing retinal detachment after laser photocoangulation administration in comparison to AGA infants.
P-07-015 Effect of smoking during pregnancy on newborns
G. Bogdanovic1, Z. Fatusic1, Z. Zigic2, S. Ramic2, G. Grgic1
1UKC OB/GIN Clinic, Tuzla, Bosnia and Herzegovina; 2UKC, Tuzla, Bosnia and Herzegovina
Objective: To assess the effect of tobacco consumption during pregnancy on anthropometric characteristics of newborns.
Methods: The prospective research was made at Clinic for Gynaecology and Obstetrics, University Clinical Centre Tuzla. The investigated group consisted of 300 newborns whose mothers smoked more than 15 cigarettes per day during pregnancy. The control group had 300 newborns of not smoking mothers. Four parameters were examined: 1) length; 2) birth weight; 3) head circumference, and 4) chest circumference.
Results: There is a statistically significant difference in anthropometric characteristics between two groups. Birth weight in investigated group was below 2500 g in 52% (N = 136) and 12% (N = 36) in control group. Anthropometric characteristics of investigated group were less than control group: birth weight average for 411.96 g, length average for 1.41 cm, head circumference average for 1.99 cm and chest circumference average for 2.02 cm.
Conclusion: Smoking during pregnancy has deleterious effect on newborns anthropometric characteristics.
P-07-016 Clinical recommendations of buprenorphine use in pregnancy
B. Vavrinkova, T. Binder
2nd Medical School of Charles University, Prague, Czech Republic
There is a lack of adequately controlled prospective studies of the use of buprenorphine in pregnancy to establish the safety of the use of the medication. In rare circumstances, discontinuation of buprenorphine treatment may pose a greater risk to mother and baby than continuing. Practitioners managing pregnant women with buprenorphine during pregnancy should consult with an addiction medicine specialist to discuss management during pregnancy. Dose reductions are advised against during pregnancy. Withdrawal symptoms should be avoided as much as possible as they may cause considerable distress to the foetus. If the doctor managing the patient decides with the patient to do so, the 2nd trimester is considered to be the least harmful period for an adverse obstetric event.
Third trimester monitoring is strongly recommend for all pregnant opiate dependent patients. This may include the following: an ultrasound at 32 to 34 weeks gestation is suggested to look at foetal growth, and cardiotocograph monitoring is suggested weekly from 35 weeks gestation to monitor fetal well-being.
Induction of labour may occur depending on the obstetric circumstances with routine methods including prostaglandin jelly, artificial rupture of membranes, oxytocin. All techniques for monitoring during labour are recommended.
Buprenorphine is a partial opiate agonist at the μ-opiate receptor with low intrinsic activity, high receptor affinity and slow rates of dissociation. Management of analgesia using other opiates such as pethidine, morphine – is therefore not effective for women maintained on buprenorphine as full opioid agonists will be ‘blocked’ by buprenorphine. Alternative approaches are required. These include: Non-pharmacological – showering, massage, mobilisation, TENS, nitrous oxide inhalation, epidural anaesthesia, pudendal block for low instrumental delivery, local anaesthetic infiltration for episiotomy.
P-07-017 Pregnancy outcome in obese and morbidly obese gestational diabetic women
Y. Yogev, R. Chen, A. Ben-Haroush, M. Hod
Department of Obstetrics and Gynecology, Rabin Medical Center, Beilinson Campus, Petah Tiqwa, Israel
Objective: We sought to determine if pregnancy outcome differs between obese and morbidly obese GDM patients.
Methods: Obesity was defined as BMI > 30 and <35 kg/m2; morbidly obese was defined as BMI ≥ 35 kg/m2. Well-controlled mean blood glucose was defined as <105 mg/dl. Adverse outcome included metabolic complications, macrosomia (>4000 g), NICU admission, respiratory support and caesarean section.
Results: 1) 760 obese (BMI 32.4 ± 1.6 kg/m2) and 559 morbidly obese (BMI 42.6 ± 2.2 kg/m2) women were compared. 2) Weight gain during pregnancy was significantly higher among morbidly obese patients (13.2 ± 4.1 vs. 10.2 ± 3.1 kg, p < 0.004). No difference was found in maternal age, OGTT results, gestational age at delivery and birth weight. 3) Insulin treatment was initiated for 62% of the obese and 72% of the morbidly obese women (p < 0.002). 4) Similar levels of glycemic control were found between the groups, 109 ± 19 (obese) and 108 ± 18 (morbidly obese). Moreover, comparable rates of women achieved the desired level of glycemic control (63% vs. 61%, respectively). 5) Similar rates of caesarean section, fetal macrosomia, shoulder dystocia and metabolic complications were noted.
Conclusions: Pregnancy outcome is compromised regardless of the level of obesity in GDM.
P-07-018 Is there a difference in the glycemic profile of non-diabetic women with positive/negative glucose challenge test screening (GCT) results?
R. Chen, C. Sagiroglu, Y. Yogev, A. Ben-Haroush, M. Hod
Department of Obstetrics and Gynecology, Rabin Medical Center, Beilinson Campus, Petah Tiqwa, Israel
Objective: It has been suggested that the elevated glucose challenge test (GCT) by itself reflects glucose intolerance during pregnancy. We sought to evaluate the glycemic profile characteristics in relation to GCT results in non-diabetic pregnant women.
Method: 52 non-diabetic gravid subjects were evaluated, of them 26 had positive 1-h 50 g GCT results (>130 mg/dl). All subjects in both groups had normal OGTT by the Carpenter/Coustan criteria. Daily glycemic profile was evaluated using the Continuous Glucose Monitoring System (CGMS). CGMS measures glucose levels every 5 minutes for 72 consecutive hours for a total of 288 measurements daily. During the study period, all women were requested to refrain from any lifestyle modification or dietary restrictions. For quality control, CGM data were compared to self-monitoring blood glucose performed in this timeframe by the women 6–8 times/daily.
Results: 1) Overall, 39,123 glucose determinations were obtained with an average of 752 ± 29/patient. 2) The correlation coefficient (r) between the glucose measurements by the sensor and meter was 0.93 ± 0.04, and the reliability coefficient was 0.88. 3) No difference was found in maternal age (28.2 ± 4.1 vs. 29.0 ± 3.1) and gestational age at evaluation (29.2 ± 2.1 vs. 29.5 ± 2.8 weeks, p = 0.3). 4) Subjects with a positive GCT had higher rates of obesity (BMI > 30 kg/m2) compared to women with negative GCT results (47% vs. 19%, p = 0.001) 5) Similar glycemic profiles (p = 0.23) were found for both screening glucose threshold groups (mean blood glucose, fasting value, 1-h and 2-h postprandial glucose value ().
Conclusions: In non diabetic subjects, elevated GCT by itself is not a marker for glucose intolerance.
P-07-019 Second trimester serum homocysteine levels and uterine arteries RI values as predictors of perinatal outcome
V. Stoykova1, V. Mazneikova1, V. Dimitrova1, St. Ivanov1, Zh. Karagiozova1, A. Tzoncheva2
1University Maternity Hospital “Majchin dom”, Sofia, Bulgaria; 2University Hospital “Aleksandrovska”, Sofia, Bulgaria
Objective: We hypothesized that second trimester Doppler evaluation of uterine arteries (UA) as well as serum homocysteine (Hcy) could be used as a screening test for determination of pregnant women at risk of adverse perinatal outcome later in pregnancy.
Methods: Sixty-three pregnant women at a mean age of 30 ± 5.03 were enrolled in a prospective study between 08.2004 and 11.2005. All women were between 18 and 24 weeks of gestation. UA Doppler US was performed to all patients. Serum Hcy levels were evaluated in fasting blood samples.
Results: Twelve (19.05%) women had an adverse perinatal outcome. Of them 10 (15.9%) developed preeclampsia. Four of them delivered before 34 weeks of gestation. There were 5 (7.94%) cases of IUGR, 2 (3.18%) intrauterine deaths and 1 (1.59%) placental abruption. The mean Hcy of the 12 women with adverse perinatal outcome was 7.17 ± 2.68 (mol/l, while in all others it was 5.54 ± 1.9 μmol/l (p < 0.05). The specificity for the Hcy higher than the 50th percentile was 81%, 56%, 62% and 77% respectively. The calculated relative risk (RR) for adverse outcome was 5.43. In 29 (46.3%) of the patients the mean RI was higher than the 50th percentile for the corresponding gestational age (specificity 82%, 50%, 47% and 87% respectively). The calculated RR was 3.55. When elevated Hcy was added to high mean RI, the RR was 3.9.
Conclusion: Doppler screening of the UA between 18 and 24 weeks of gestation identifies most women who subsequently develop serious pregnancy complications. Hcy level alone is also a good predictor of adverse perinatal outcome, but its supplementation to the Doppler US results doesn't significantly improve its prognostic value.
P-07-020 Subcutaneous fat necrosis of newborn children
R. Rudanovic1, D. Dakic1, M. Rudanovic1, Lj. Globarovic1, A. Begovic1, S. Zekovic2, P. Rakocevic3, M. Perosevic1
1Children's Clinic, Podgorica, Yugoslavia; 2Sanicard, Podgorica, Yugoslavia; 3Military Health Center, Podgorica, Yugoslavia
Objective: Subcutaneous fat necrosis is a rare disease which occurs in the first week of life and it is often a consequence of complications appearing during delivery (fetal distress and delivery trauma). Literature gives very small amount of data about this issue. The greatest study has been elaborated in Canada, which covered 11 patients followed up in 6 year period. Clinical diagnosis is identified on the basis of local findings and histopatologic examination (biopsy of skin sample).
Objective is to show clinical indicators and DDG scleredem of the newborn child and subcutaneous fat necrosis.
Methods: Three newborn children teated in Neonatal Center are described for two year period (2004/2005).
Results: All three infants had almost identical clinical findings. At the skin of back, in the supraclavicular and infraclavicular areas, as well as above two elbows there were dominant solid round tumeractions, intensively bright red in color, somewhere even blue. Histologic findings indicate to necrosis of fat tissue of infiltrative mononuclear cell with giant cell formation around focus of fat necrosis. Breaks in the needle shape are detected inside adipocites, but not inside macrolagocits. One mother had gestal diabetes, while all tested women had a fetus water of green color, and amnion water with meconium. We identified diagnosis on the basis of clinical findings, course of the disease, histologic findings (skin biopsy) and patognamonic findings of lab. hypercalcemia in the fourth and fifth week.
Delivery of one infant with fetal distress ended in Ceasarian Section, while the other two children were born thorugh vaginal delivery and final vacuum procedure. All tested persons had disease in duration of six weeks, and the outcome was good for all of them.
With respect to laboratory parameters, serum amilasys is moderately higher; hypoglicemia was maintained in the first week after reception; trombocitopenia was present before fat necrosis started and it was only temporary, so that it was deemed as sepsis; hypercalcemia was developed in third week; hypocalcemia was present in first week. As per data from literature, pathogenesis of hypercalcemia includes higher levels of prostaglandin E (22) and parathpromon.
Conclusion: Fetal distress and delivery trauma were present at all three patients. DDG in relation to SN is possible to be made according to time of occurrence, clinical picture, course, therapeutical treatment and outcome. All three patients had hypercalcemia.
P-07-021 Splanchnic circulation in healthy newborns during the first 3 days of life
K. Matasova, M. Zibolen, H. Kolarovszka, D. Murgas, M. Dragula
Faculty Hospital Martin, Martin, Slovak Republic
Background: The splanchnic circulation accounts for 20% of cardiac output, and at times it may contain one-third of the blood volume. Postnatal age is one of the factors affecting splanchnic blood flow patterns in infants.
Objective: The aim of the study was to evaluate coeliac axis (CA) blood flow and superior mesenteric artery (SMA) blood flow in healthy newborns by means of Doppler ultrasonography in connection with postnatal age.
Materials and Methods: Sixteen healthy newborn infants with gestational age of more than 37 weeks and uncomplicated postnatal adaptation were examined at the age of 2.5, 24 and 70 hours. SMA resistive index (RI) and CA RI, as an estimate of perfusion, were assessed.
Results: The SMA RI was significantly higher than the CA RI in all performed measurements (p < 0.01; r = 0.96). Resistive index decreased during the first 3 days in both vessels: CA RI 0.76 ± 0.11 vs. 0.66 ± 0.06, p < 0.01 (r = −0.51); SMA RI 0.93 ± 0.08 vs. 0.78 ± 0.05, p < 0.001 (r = −0.72). The most marked RI changes in both vessels were observed between measurements 1 (2.5 hours of life) and 2 (24 hours of life): CA RI 0.76 ± 0.11 vs. 0.61 ±0.01, p < 0.001; SMA RI 0.93 ± 0.08 vs. 0.77 ± 0.07, p < 0.001.
Conclusion: Ultrasound measurements in neonates suggest that superior mesenteric artery perfusion, as measured by resistive index, is significantly lower compared with coeliac axis perfusion. The perfusion of both measured vessels improves in the early postnatal period.
P-08-001 Growth and composition of the intestinal microbiota of infants fed an infant formula with added galacto- and fructo-oligosaccharides
C. Costalos1, M. Apostolou1, A. Kapiki1, E. Papathoma1, J. Wells2, P. Scholtens3, J. Knol3
1Alexandra Hospital, Department of Neonatal Medicine, Athens, Greece; 2Numico BV, WTC Schiphol, Schiphol, The Netherlands; 3Numico Research BV, Wageningen, The Netherlands
Objective: The aim of the study was to investigate the growth and intestinal microbiota composition of infants fed a starting formula containing 0.4 g/100 ml galacto- and fructo-oligosaccharides (GOS/FOS), in a ratio of 9:1.
Methods: The study was a double-blind, randomised, placebo-controlled clinical trial in which formula-fed infants aged <14 days were included in a 13 week intervention period. Infants received a starting formula with GOS/FOS, or a control starting formula. Weight, length, head circumference, mid upper arm circumference and skinfold thickness data were recorded during regular visits to the paediatrician (n = 130; enrolment, weeks 6 and 13). Faecal samples were collected by the parents (n = 121; enrolment and week 6), and analyzed by fluorescent in situ hybridization. Statistical analyses were carried out with Mann-Whitney U tests.
Results: The infants in both groups demonstrated normal growth. No significant differences between the groups were observed for faecal pH, or the faecal percentage of bifidobacteria. A significantly lower faecal percentage of clostridia bacteria was observed in the GOS/FOS group compared to the control group (p = 0.042).
Conclusions: The addition of 0.4 g/100 ml GOS/FOS to a starting formula does not affect the growth of healthy infants and results in a lower percentage of faecal clostridia bacteria.
P-08-002 Nutrition support and growth in preterm infants
N. Prekajski1, M. Rankovic1, A. Minic1, S. Simic1, V. Marinkovic1, B. Milisavljevic2
1Institute for Neonatology, Belgrade, Yugoslavia; 2Medical Center, Subotica, Yugoslavia
Objective: Evaluation and comparation of the efficasy of nutritional management organized by using fortified human milk in promotion of growth in preterm infants.
Methods: We conducted a study included 55 preterm infants gestation age up to 36 weeks of gestation, on enteral nutrition with fortify breast milk. Group A included 25 infants fed with breast milk plus powdered fortifier (Nestlé), and group B included 30 infants fed with breast milk plus domestic special premature formula (Preimpamil). Both kind of fortification have been prepared as 5% mixture. Total volume intake was in range from 70 ml/kg/day at the first day of life, up to 170–200ml/kg/day at the tenth day of life. We evaluated: initial birth weight loss (%), days for achieving birth weight, weight gain (g/kg/day), mean volume intake (ml/kg/day), caloric (kcal/kg/day) and protein (g/kg/day) intake during the first month of life.
Results: Among base line characteristics of the groups, such as, birth weight and gestation age, we found no statistically significant difference. Comparing group A to group B in initial loss in BW (9.3 ± 2.2 to 7.2 ± 1.89), days for achieving BW (15 ± 6.3 to 12.4 ± 5.34) and weight gain (13.6 ± 3.69 to 22.8 ± 5.79) we find no st. significant difference. Also, there was no st. significant difference between group in analyzing volume intake (184 ± 15.8 to 186 ± 18), protein intake (3.1 ± 0.43 to 3.63 ± 0.19), and caloric intake (138 ± 15.2 to 127 ± 16.3).
Conclusions: Fortification of breast milk potentially optimized caloric and protein intake in preterm infants. This study showed similarity between study groups in initial loss in birth weight, days for achieving BW, in weight gain, volume, protein and caloric intake, whether fortification was with powdered fortifier (Nestlé) or domestic special premature formula (Preimpamil).
P-08-003 Early nutrition and later outcomes in VLBW infants
F. Were, N. Bwibo
University of Nairobi, Nairobi, Kenya
Objectives: To evaluate the association between early feeding regimens with post discharge morbidity, mortality and functional disability in VLBW infants during the first two years.
Methods: One hundred and seventy-five VLBW infants without visible congenital anomalies who survived the neonatal period were recruited over a consecutive period of 1 year and followed up to gestation corrected age of 2 years. Neonatal nutritional history, early growth parameters, post discharge re hospitalization/mortality and neurological assessment (using the functional disability assessment tool described by Saigal and Rosenbaun) were determined at 2 years.
Results: Of the 175 infants recruited 5.6% were lost to follow up while 25.7% died before completion of study. The group's mean birth weight and gestation were 1.4 (1.0) kg and 32.4 (2.3) weeks respectively while 36.6% had intrauterine growth retardation. Early feeding regimens were as follows; Preterm Fomula (PF), in 20% of the infants, Breast Milk alone (BM) in 43% while 33% had Mixed Feeds (MF). The infants fed on PF had better neonatal weight gain; median 17.5 (2.5) than those on MF or BM who grew at 15.0 (2.0) and 12.0 (3.9) g/kg/day respectively (P < 0.001). The PF fed infants also had a higher median weight at the expected time of normal birth 2.4 (1.9) kg than those on either MF, 2.3 (1.4) or BM, 2.1 (1.7); P < 0.001. Infants fed on BM were more likely to be rehospitalized than those on MF (P < 0.001, RR 2.01, 95% CI 1.38–2.91) or PF (P < 0.001, RR 2.23, 95% CI 1.35–3.68). They (BM) also developed more neurological disabilities (P = 0.020, RR 2.04, 95% CI 1.10–3.78) compared to those on PF or MF. Only 18% of infants fed on PF died compared to 30 and 27% of those on exclusive BM and MF feeds respectively (not statistically significant).
Conclusion: Nutritionally enhanced enteral feeds may reduce post discharge morbidity and improve neurological outcomes at 2 years in VLBW infants.
P-08-004 Ghrelin levels in neonates of diabetic mothers (NDM)
K. Fotiou1, O. Kastanidou2, E. Thanopoulou2, M. Skouroliakou2, G. Liossis1
1Neonatal Unit, Elena Venizelou Perinatal Center, Athens, Greece; 2Dept. of Science of Nutrition and Dietetics, Harokopio University, Athens, Greece
Objective: The determination of ghrelin levels, that regulates the metabolism and growth in NDM premature and full term neonates and to assess its correlation with anthropometric and biochemical parameters.
Methods: Ghrelin levels of 70 neonates (21 preterm and 49 term) born in our hospital, were assessed by the radioimmunoassay method (Linco Research kit).
Results: The premature NDM had higher ghrelin levels compared with term ones (414.25 ± 235.82 vs. 689.87 ± 684.11 pg/ml, p < 0.019). Our results showed also, a sexual dimorphism, with mean ghrelin concentration higher in females (411.57 pg/ml) than males (386.87 pg/ml), but this difference didn't reach the limits of statistical significance. Ghrelin levels of the total NDM (premature-terms) showed negative correlation with their anthropometric measurements. Ghrelin also showed negative correlation with anthropometric indices inside the subgroups. The assessment of correlation between ghrelin and biochemical parameters, showed a negative relation with serum glucose levels in all NDM. On the contrary, ghrelin showed a positive correlation with the total HDL and LDL cholesterol but only in the premature ones.
Conclusion: 1) The observed higher ghrelin levels in premature NDMs, probably, is due to the fact that intra-uterine hyperinsulinemic environment does not influence the need of premature NDMs for growth. 2) The reverse relation between ghrelin and blood glucose levels can be explained with the excitation of appetite by ghrelin that maintains sufficient levels of blood glucose and respectively protects from hypoglycaemia. 3) The positive correlation of ghrelin with the lipidaimic molecules, in the team of premature, can be explained by the decreased oxidation of lipids that ghrelin causes, known as “alimentary partition”.
P-08-005 Serum adiponectin levels in preterm infants
T. Siahanidou1, H. Mandyla1, G.P. Papassotiriou2, I. Papassotiriou2, G. Chrousos1
1First Department of Pediatrics, Athens University Medical School, Thivon & Levadias, Athens, Greece; 2Department of Clinical Biochemistry, “Aghia Sophia” Children's Hospital, Thivon & Levadias, Athens, Greece
Objective: To determine the circulating concentrations of adiponectin in preterm infants, compare these levels to those obtained in fullterm infants and examine the possible associations of adiponectin with anthropometric parameters, caloric intake, weight gain and the serum levels of leptin and insulin.
Methods: Serum adiponectin was determined by RIA, leptin by ELISA and insulin by chemiluminescence immunoassay in 62 preterm infants (gestational age 32.0 ± 2.1 weeks) at discharge (40.9 ± 14.8 days of life) and 15 fullterm infants of a comparable postnatal age. All infants were fed with the same commercial formula, but in 9 preterm infants the formula contained added LCPUFAs (arachidonic and docosahexaenoic acid).
Results: Adiponectin concentrations were significantly lower in preterm (41 ± 15 μg/ml) than term infants (53 ± 16 μg/ml, p < 0.01). In preterm infants, adiponectin levels correlated positively with birthweight and birthweight z-score (p = 0.01), body weight z-score at discharge (p = 0.01), weight gain (p = 0.05) and feeding with a formula containing LCPUFAs (p = 0.02), but not with gestational age, gender, body length, head circumference, caloric intake and circulating levels of leptin or insulin. In multiple regression analyses, birthweight z-score, body weight z-score at discharge, weight gain and feeding with a formula containing LCPUFAs were independent predictors of adiponectin concentrations. In fullterm infants, no significant correlation was found between adiponectin levels and any of the variables studied.
Conclusions: Circulating concentrations of adiponectin are lower in preterm than term infants probably as a result of decreased adiposity. Adiponectin may have a role on the growth of preterm infants. Whether the relation between adiponectin concentrations and dietary PUFAs suggests that dietary supplemention with LCPUFAs has an impact on the risk for the later development of insulin resistance remains to be elucidated.
P-08-006 The analysis of the birth weight, birth length and body mass index of term neonates hospitalized at the children's clinic NIS in the 5-year period
R. Mileusnic Milenovic, D. Djordjevic, L.J. Saranac, M. Novak, L.J. Pejcic, S. Zivanovic
Children's Clinic, Clinical Center Nis, Nis, Serbia
Objective: The analysis of the birth weight (BW), birth length (BL) and BMI of term neonates and the analysis of the same parameters small (SGA) and large (LGA) for gestational age babies.
Methods: Retrospective analysis of medical documentation of 436 term neonates hospitalized at the Children's clinic in Nis, between 1.1.2002 and 31.12.2005. BW, BL, and BMI of all hospitalized neonates were analysed. To calculate the Z-score for BW, BL and BMI, The EuroGrowth program was used.
Results: One Way ANOVA test showed differences between 2001–2005 related only to the length of the neonates (p < 0.05). The average length value in 2001 (Student t-test) was smaller in relation to 2004 (p < 0.05), as well as in 2003 and 2005 (p < 0.01). The average value of Z-score of the body weight is lower in 2001 in respect to the year 2003 (p < 0.05). There is a difference in average weight, also in the average weight Z-score in 2001 as related to 2003 (p < 0.05). The complete presence of LGA neonates is significantly bigger than SGA (chi square test, p < 0.001). With SGA babies the most present are SGA babies with small weight, and with LGA babies those with big length. There is an obvious positive trend of LGA babies percentage, specifically LGA babies with big length and LGA with big both length and weight. There is a negative trend in the SGA babies percentage, mostly of small weight, than of small weight and length, as well as of small length, but that was less evident. For BMI no statistically relevant differences were observed.
Conclusions: The causes of the LGA babies positive trend are not clear enough, although it may be possible that one of them is a higher total number of thus born babies in a population. This is also indicated by the positive trend in the increase in the length of all hospitalised babies. The possible causes of the SGA babies negative trend are in the improvement of the prenatal diagnostic process and therapy.
P-08-007 The effect of nutritional habits on maternal-neonatal lipid and lipoprotein serum levels in three different ethnic groups
K. Schulpis1, S. Gavrili2, G. Vlachos3, C. Costalos2, A. Antsaklis3, K. Danelatou2, I. Papasotiriou4
1Institute of Child Health, Athens, Greece; 2Neonatology Department, “Alexandra” Hospital, Athens, Greece; 3First Department of Obstetrics and Gynecology, Athens University, Medical School, Athens, Greece; 4Department of Clinical Biochemistry, “Aghia Sophia” Children's Hospital, Athens, Greece
Aim: To investigate the effect of nutritional and religious factors on lipid profiles and the potential atherogenic risk in mothers and newborns.
Subjects and Methods: Lipids and lipoproteins were determined in 7 d dietetic diary of 9134 mothers (Greeks N = 3118, Albanians N = 3050, Muslim Asians N = 2966), in their sera and in the cord blood of their newborns with routine methods.
Results: Monunsaturated fat intake was similar among the groups. Total fat, saturated fat and cholesterol intakes were significantly lower in Muslims than those in Albanians and Greeks. Statistically significant low lipid and lipoprotein concentrations (Chol 5.09 ± 0.85 mmol/l, Tg 2.38 ± 0.58 mmol/l, LDL-C 2.90 ± 0.78 mmol/l, VLDL-C 0.32 ± 0.11 mmol/l p < 0.001) were measured in the Muslim Asian mothers and in their newborns. Higher levels of the mentioned biochemical parameters were found in Greek (Chol 5.20 ± 0.98 mmol/L, Tg 2.37 ± 0.62 mmol/l, LDL-C 3.40 ± 0.85 mmol/l, VLDL-C 0.48 ± 0.13 mmol/l) and Albanian mothers (Chol 7.1 ±0.78 mmol/l, Tg 2.55 ± 0.60 mmol/l, LDL-C 4.1 ± 0.88mmol/l, VLDL-C 0.52 ± 0.13 mmol/l) and in their newborns. The highest HDL-C levels were observed in the Asian Muslim mothers (HDL-C 1.60 ± 0.31mmol/l, vs. 1.4 ± 0.39 mmol/l in Greeks and 1.31 ± 0.39 mmol/l in Albanians p < 0.001).
Conclusion: The normal lipid profile in Greeks and the high in Albanians may be due to their nutritional habits and their socio-economic status. The lower blood lipid levels in the Muslim Asian mothers reflect religious, nutritional socio or even genetic differences. Cholesterol education programme and selective screening of infants and mothers with high cholesterol and/or LDL-C levels should be planned in Greece, as a preventive measure.
Keywords: Lipids, Lipoproteins, newborns, Greeks, Albanians, Muslim Asians
P-08-008 Allergic colitis in neonatal period
M. Benedit, I. Llana, M.T. Garcia Alvaro, M.C. Cantisano, A. Lopez Escobar, P. Touza, I. Romero
Hospital Madrid Torrelodones, Madrid, Spain
Introduction: Allergic colitis is an illness with an increasing prevalence in our population. It can occur within hours of birth, and therefore it should be considered in any members in whom rectal bleeding occurs. The true prevalence of allergic colitis is known.
Methods: We performed a retrospective study of all the patients diagnosed of hemorrhagic colitis developing in the neonatal period from January 205 to January 2006.
Results: Five patients were diagnosed of allergic colitis. The mean age at the onset of symptoms was 10 days (range 8 hours–28 days).
All of them except one were moderate preterm and had all received cow's milk formula in at least twice. In all five cases, eosinophilia was found. Only one patient underwent flexible sigmoidoscopy which confirmed the diagnosis.
In four of the five patients only elemental formula resolved the rectal bleeding. All infants are being followed up by gastroenterologist with favourable outcome.
Conclusion: Allergic colitis during the neonatal period life is an increasing pathology and should be considered together with enterocolitis necrotizing in the differential diagnosis of rectal bleeding. Sometimes an elemental formula is needed.
P-08-009 Docosahexaenoic acid status of breastfeeding mothers can be improved by low dose supplementation during pregnancy and lactation
R.L. Bergmann1, E. Haschke-Becher2, K.E. Bergmann1, J.W. Dudenhausen1
1Charite University Hospitals, Dept. of Obstetrics, Berlin, Germany; 2University of Lausanne, Dept. of Biochemistry, Epalinges, Switzerland
Aim: To investigate the effect of a low dose of docosahexaenoic acid (DHA, 22:6 n-3) in a daily supplement for pregnant and lactating mothers on the DHA concentration in red blood cell (RBC) phospholipids 3 months after delivery.
Methods: At 22 weeks of pregnancy, 144 mothers were enrolled to a randomized controlled double blind clinical trial on the daily intake of one of three supplements up to 37 weeks, and voluntarily up to 3 months after delivery. The first supplement contained minerals, and vitamins (Min/Vit), the second additionally contained a prebiotic (Prebio), and the third additionally 0.2 g DHA from fish oil (LCPUFA). Questionnaires and product consumption measurements verified compliance. At 3 months, venous blood samples were obtained from 89 mothers. The samples were analysed by gas-liquid chromatography. Treatment differences were estimated in the intention to treat (ITT) and per protocol (PP) data set by ANCOVA, correcting for the baseline measurement of the mother at week 22 (p-values adjusted for multiple tests).
Results: 3 months after delivery the concentrations of DHA-RBC (% of fatty acids) had decreased, exept for the LCPUFA-group. The DHA-RBC concentrations in the ITT data set were 5.05 (±1.53) compared to 5.17 (±2.09), and to 6.48 (±1.78) in the Min/Vit-, Prebio-, and LCPUFA-group, respectively. The treatment effect was significant in the LCPUFA-group compared to the Min/Vit- and to the Prebio-group utilizing the ITT data set (p = 0.0143 and 0.0164, resp.), as well as the PP data set (p = 0.0123 and 0.0126, resp.). Similar effects could be observed for eicosapentaenoic acid, but no statistical difference between groups was found for arachidonic acid.
Summary: Maternal low dose DHA-supplements in pregnancy and during lactation influenced the DHA-concentration in the lipids of their RBC up to 3 months after delivery, and prevented a decrease during lactation.
P-08-010 Intermediate metabolism in association with the amino acid profile during the third trimester of normal pregnancy and diet-controlled gestational DIAB
K.I. Pappa1, M. Theodora1, G. Vlachos1, M. Roubelaki2, A. Angelidou2, A. Aantsaklis1
11st Department of Obstetrics and Gynaecology, University of Athens School of Medicine, Athens, Greece; 2Foundations for Biomedical Research of the Academy of Athens (IIBEAA) and Laboratory of Biology, Athens, Greece; 3Department of Hygiene and Epidemiology, University of Athens, School of Medicine, Athens, Greece
Objectives: In the present study, we investigated the levels of fasting maternal plasma amino acids in normal pregnant women and compared them to those in gestational diabetes controlled by diet only. Also we delineated the alterations occurring in intermediate metabolic pathways.
Materials and Methods: 46 (64.7%) pregnant women with uncomplicated pregnancy (NP group) and 25 (35.2%) women with gestational diabetes mellitus (GDM group) between 30th and 33rd gestational week, participated in the study. Fasting maternal plasma carnitine (total, free and acyl-carnitine), (BOH), (FFA), glycosylated hemoglobin (HbA1c) and 21 amino acids were assayed.
Results: Fasting carnitine esters (AC) exhibited lower levels in the GDM group (P = 0.03) while total carnitine (TC) showed no significant difference between the two groups (P = 0.52). Higher levels of fasting β-hydroxybutyrate (BOH) and free fatty acids (FFA) (P < 0.001 and 0.02 respectively) were observed in the GDM group. No significant difference was found for the most of the 21 amino acids studied while only methionine, glycine, alanine, citrulline, and ornithine levels were found at significantly higher levels in the NP group (P = 0.03, P < 0.001, P = 0.01, P < 0.001, and P < 0.001 respectively).
Conclusion: These data imply that in gestational diabetes, ketogenic amino acids and the branched chain amino acids (BCAA) are released at low rates from skeletal muscle in contrast to normal pregnancy and are mostly catabolized in the liver than in peripheral tissues. β-hydroxybutyrate occupies a central role in the regulation of glucose homeostasis and amino acid metabolism and since gluconeogenesis is less effective, peripheral utilization of ketone bodies from ketogenic amino acids and FFA becomes the main energy source in gestational diabetes.
P-08-011 Nutritional status of pregnant women in the greek population
M. Skouroliakou1, C. Fodor1, G. Petrakos2, G. Tsoukalos2, Ch. Karkanis2, P. Panagopoulos2
1Dietology and Nutrition Department, “Harokopio” University of Athens, Athens, Greece; 2Department of Obstetrics and Gynecology, “Tzaneio” General Hospital of Pireaus, Athens, Greece
Objective: The aim of this study was to investigate both the nutritional status of Greek women during pregnancy and their need for supplement intake.
Results: The total mean calorie intake of the subjects was 1940 ± 618 Κcal/day, while the mean percentage intake/day of carbohydrates, protein and fats was 44.6%, 17.9% and 37.4% respectively. Folic acid, vitamin E and iron intake from food was observed to be very low. In contrast, intake of vitamins A, B1, B2, B12, C and phosphorus was significantly higher than recommended. 57% of the population reported taking nutritional supplements, with a predominance of iron, calcium, folic acid and magnesium.
Conclusion: The pregnant women, who participated in the study, seemed to adhere to a diet characterized by low total energy intake. Daily carbohydrate intake was low, while fat intake was observed to be much higher than the recommended value. Also excessive consumption of iron supplements and inadequate fibre intake was noted.
P-08-012 Multicentric program for the assessment of the risk for the development of pre-eclampsia and intrauterine growth restriction by a two stage uterine artery doppler in low-risk mediterranean population
E. Llurba1, E. Carreras1, E. Gratacos1, M. Juan2, J. Astor3, A. Vives4, S. Rodriguez4, E. Hermosilla1, P. Millan1, B. Garcia-Vadecasas1, T. Roig1, F. Crispi1, L. Cabero1
Obstetrics and Gynecology Department, 1Vall d'Hebron Hospital, Barcelona, Spain; 2Son Llatzer Hospital, Mallorca; 3Granollers Hospital, Spain; 4Terrasa Hospital, Spain
Objectives: To estimate the value of screening for pre-eclampsia and fetal growth restriction (IUGR) by performing color Doppler assessment of uternie arteries (UtA) at 20 and 24 weeks' gestation in an unselected Mediterranean population.
Methods: A prospective multicentre observational study including 6420 consecutive singleton pregnancies undergoing routine morphologic scan at 20 weeks gestation between June 2002 and June 2005. The left and right UtA were examined by color pulsed Doppler abdominally. The mean pulsatility Index (PI) and the presence of bilateral protodiastolic notching were recorded. Reference values for the mean PI at 20 weeks' gestation were calculated. Pregnancies were followed for the development of pre-eclampsia, IUGR, placental abruption and stillbirth. The sensitivity and predictive values of mean UtA-PI > 95th centile and the presence of bilateral notching in the prediction of these pregnancies complications were calculated.
Results: A mean PI of 1.55 was 95th centile of our population. A total of 6132 women were finally included, increased PI or/and bilateral Notches were present in 13.6%, only in 54% of them UtA Doppler persisted abnormal at 24 weeks gestation, a 5.8% of total population evaluated. The sensitivity of increased PI or/and bilateral notches at 24 weeks gestation was 33.4% for preeclampsia, 21.4% for isolated IUGR, and 75% for pre-eclampsia associated to IUGR. UtA Doppler at 24 weeks gestation identified almost the 20% of the population at risk of severe complications due to placental insufficience.
Conclusions: A two-stage color Doppler screening program identified most women who subsecuently developed serius complications of impaired placentation. The implementation of this screening test is limited by the lack of efective preventive measures on the population selected.
P-08-013 Atherogenic lipoprotein subfraction profile in preeclamptic women with and without high triglycerides: different pathophysiological subsets in preeclampsia
E. Llurba1, E. Gratacos1, E. Casals2, J. Delgado1, I. Mercader3, F. Crispi1, P. Martin-Gallan2, C. Dominguez2, L. Cabero1
1Fetal Medicine Unit, Department of Obstetrics, 2Biochemistry and Molecular Biology Center, Hospital Vall d'Hebron, Universitat Autonoma de Barcelona, 3Department of Biochemistry, Hospital Clinic i Provincial, Universitat de Barcelona, Barcelona, Spain
Objective: Abnormal lipid metabolism has been proposed as a pathogenic factor of preeclampsia, but it is unclear whether it is a constant feature in all preeclamptic patients. We evaluated whether triglyceride levels distinguish a subgroup of preeclamptic women with an atherogenic lipid profile from those with normal lipid metabolism.
Design: Prospective study including 34 women with preeclampsia and 23 healthy pregnant women. Preeclamptic women were further subclassified into normal-triglyceride (<250 mg/dl) and high-triglyceride (≥250 mg/dl) groups, on the basis of the 90th percentile in our population.
Setting: The departments of obstetrics and gynaecology at a university teaching hospital.
Methods: Low-density lipoproteins (LDL) were ultracentrifuged and separated into four subfractions, and lipid distribution in the subfractions was analyzed in all study groups. Vascular cell-adhesion molecule-1 (VCAM-1) was also measured as a marker of endothelial dysfunction.
Main Outcome Measures: Atherogenic lipoprotein subfractions profile in preeclamptic patients depending on triglyceride levels.
Results: Sixteen women with preeclampsia had high triglycerides (47% vs. 13% in controls, p < 0.001). This subgroup showed a significant shift in lipid distribution, mainly triglycerides, towards the small-dense LDL subfractions. However, preeclamptic patients in the normal-triglyceride subgroup showed LDL subfraction lipid distribution similar to that of healthy pregnancies. VCAM-1 levels were significantly elevated in preeclamptic patients in comparison to controls regardless of triglyceride levels.
Conclusion: Atherosclerosis-like changes in lipid metabolism are exclusive of a subset of preeclamptic patients with high triglyceride levels. These findings support the concept of heterogenic pathogenic lines in preeclampsia and the use of subclassifications in pathophysiologic research on the condition.
P-08-014 Gender and parity specific reference charts for fetal size in low risk singleton pregnancies at the start of the third trimester
P. De Reu1, L. Smits4, H. Oosterbaan5, R. Snijders3, J. Nijhuis2
1V.C.M.B., Boxtel, The Netherlands; 2Dep. of Obstetrics, Maastricht University, Maastricht, The Netherlands; 3F.M.F. Netherlands, Rotterdam, The Netherlands; 4Dep. of Epidemiology, Maastricht University, Maastricht, The Netherlands; 5Dep. of Obstet. & Gynecol., J.B.Z., Hertogenbosch, The Netherlands
Objectives: To determine fetal growth of uncomplicated singleton pregnancies in a low risk population at the beginning of the third trimester and to assess the influence of fetal gender and maternal parity.
Setting: Dutch primary care midwifery practice.
Study Design: Data from 3641 singleton pregnancies that were seen at a primary care midwifery centre in the Netherlands were analised retrospectively. Parameters used for analysis were fetal abdominal circumference (AC), fetal head circumference (HC), gestational age, fetal gender and maternal parity. Regression analysis was applied to describe changes in AC and HC with gestational age. Means and standard deviations in the present population were compared to commonly used reference charts in the Netherlands. Multiple regression analysis was applied to examine whether gender and parity should be taken into account.
Results: Between the 27th and the 33rd week of pregnancy the fetal AC and HC increased significantly with gestation (AC r2 = 0.3652, p < 0.0001; HC r2 = 0.3301, p < 0.0001). Compared to the original standard curves our means and standard deviations were smaller for the most part (at 30 + 0 weeks AC mean = 258 mm, SD = 13 mm; HC mean = 281 mm, SD =14 mm). Moreover, fetal gender was a significant determinant for both AC and HC (p < 0.0001 and p < 0.0001 respectively). Parity contributed significantly to AC only (p < 0.0049).
Conclusion: Data from the present study confirm that boys and girls differ in size already at the start of the third trimester; with boys having significantly larger HC's and AC's than girls. Comparison of prenatal size of first and subsequently born children demonstrated that there is a significant difference in AC but not in HC. The use of both gender and parity specific fetal growth charts might improve the detection of fetal growth abnormalities in early third trimester.
P-09-001 3/4D Ultrasound babygram, clinical necessity or commercial scan
P. Rozpravka1, M. Rozpravka2, A. Ostro1, A. Gresova1, S. Toporcerova1, L. Rosocha1
1Safaric's University and FN L. Pasteur, Kosice, Slovak Republic; 2Private Gynae Centre GSLC, Prague, Czech Republic
Objective: Adopt 3D imaging and improve its utilization in obstetrics. Discuss standards of ultrasound experts scanning and commercial applications of this foetal imaging. To understand the principles of three-dimensional ultrasound – 3D-ultrasound and real time 3D or 4D ultrasound. Compare ultrasonic protocol for screening of congenital abnormalities to commercial 3/4D-scanning value.
Methods: Clinical experiences from application of this imaging modality in comparison with 2D ultrasound.
Results: Three-dimensional ultrasound 3D allowing the acquisition of a volume and display of any plane within volume regardless of with orientation. Surface rendering of the volume image is also possible with post-processing display. Surface rendering is a process by with the surface of an area interest is displayed, not only sectional slices. It is possible rotate image in various directions. Post-processing modes enhance diagnostic capabilities and optimalization of image for commercial use. Demonstration of foetal defects is advantageous for 3/4D ultrasound and giving more precisious information in very early gestational age – Sonoembryology. Volume measurement is another important clinical application.
Main Conclusion: Focussing on 3/4D imaging in obstetrics and demonstrate the role of this technology in the field of foetal imaging and controversies of commercial 3/4D ultrasound scanning and its possible legal consequences. Perspective of this modality is to be used as an adjunct to standard 2D ultrasound techniques in the advanced ultrasound centres for congenital abnormalities screening and in commercial ultrasound centres for 3/4D-Babygram. The demands on sonographer qualification and experiences in commercial ultrasound centres are not established.
P-09-002 Case report: Prenatal diagnosis of gastroschisis with 3D/4D representation
P. Prats, E. Scazzochio, S. Baulies, M. Torrents, A. Munoz, M. Echevarria, M.A. Rodriguez, B. Serra
Institut Universitari Dexeus, Barcelona, Spain
Introduction: Gastroschisis is a paraumbilical defect involving all the layers of the abdominal wall, with evisceration of abdominal organs, usually the small bowel, on occasion large bowel and stomach. Prevalence ranges from 0.94–4.72/10,000 live births. Several reports are mentioning an increased incidence in the last decades probably due to multifactorial causes. The prevalence is also age-related and is higher in mothers younger then 24 years old, with the highest incidence in teenage mothers. Smoking, inadequate prenatal care and substance abuse seems to be risk factors for fetal gastroschisis. Males are more affected.
Case Report: An 18-year-old woman was referred to our centre for prenatal sonography for abdominal wall defect. Examination revealed an 18 week gestation with an abdominal wall defect located to the right of the umbilicus with bowel loops floating in the amniotic fluid, consistent with a right-sided gastroschisis. The abdominal wall defect was 12 mm. No associated anomalies were found. Karyotype 46XY. Ultrasound follow up was made at 23, 30, 33 and 35 weeks', with 2D and 3-4D sonogrophy. A caesarean section was prematurely performed at 35 weeks +2 days because of the presence of edema in the eviscerated and dilated bowel. The baby's weight was 2500 g. The surgery was performed 2 days after delivery. Surgeons returned the bowel in the abdominal cavity in two days and delayed the closure of the abdominal defect. Bowel stenosis after reintroduction was detected requiring a by-pass intervention. Now the baby is well and with a normal growth.
P-09-003 Prenatal diagnosis of absent pulmonary valve – one center experience
J. Hajdu, A. Beke, B. Pete, A. Harmath, Z. Papp
Semmelweis University, Budapest, Hungary
Objectives: To assess in a population of 10 fetuses diagnosed with absent polmonary valve the incidence of associated cardiac extracardiac and chromosomal anomalies and the outcome of pregnancies.
Method: Retrospective analysis of data of prenatally diagnosed absent pulmonary valve cases between January 1, 1993 and December 31, 2005. The diagnosis was controlled with autopsy or postnatal examinations. The time of the prenatal diagnosis, indications, connected cardiac extracardiac and chromosomal anomalies were studied.
Results: Absent pulmonary valve was diagnosed in 10 pregnancies. The mean gestational age at the time of the diagnosis was 23 weeks. In 7 cases the pregnancy was terminated. Among 3 live born infants 2 died in neonatal age. It was an isolated malformation at 2 fetuses, at 4 fetuses tetralogy of Fallot and absent ductus arteriosus Botalli, at 1 fetus absent aortic valve, at 1 fetus common atrium, at 1 fetus tricuspid valve dysplasia and at 1fetus absent ductus arteriosus Botalli were diagnosed. Extracardiac malformations associated with cardiac abnormality at 3 fetuses. The indication for fetal echocardiography was positive family history in 3 cases, abnormal four chamber view in 4 cases, thoracal cyst in 3 cases. In three cases where the family history was positive the chromosomal analysis was normal at parents and at fetuses too.
Conclusion: The absent pulmonary valve is a severe malformation and the prognosis is poor. The correct early prenatal diagnosis is possible. In our 3 cases autosomal recessive inheritance is possible.
P-09-004 Long term follow-up of children with serious arrhythmia diagnosed during fetal life
H. Bouza1, M. Koumenidou1, N. Eleftherakis2, D. Karatsoli2, M. Xanthou1, V. Thanopoulos2
1B Nicu “Aghia Sophia” Children's Hospital, Athens, Greece; 2Department of Cardiology “Aghia Sophia” Children's Hospital, Athens, Greece
Objective: Aim of the present study is to examine the long term follow-up of children with serious arrhythmia diagnosed during fetal life.
Methods: We examined four children, three male and one female with fetal arrhythmia presented the past four years in our hospital. Fetal arrhythmia was diagnosed by 2D and Doppler echocardiography. After their delivery they were hospitalized in our NICU and arrhythmia was confirmed by 12-lead Electrocardiogram (ECG) and treated. They were also checked for structural congenital heart disease by 2D and Doppler Echocardiogram. Follow-up was done by 24-hour Holter monitoring every three months. Mean follow-up time was 22.3 ± 8.3 months. Gestational duration was 37 ± 3 weeks and body weight at birth was 2640 ± 550 g.
Results: One child with fetal tachycardia was found in NICU to have accessory pathway mediated atrioventricular reentrant tachycardia with Wolff-Parkinson-White syndrome obvious in resting ECG as concluded after treatment. Intravenous Amiodarone was used for conversion to sinus rhythm and chronic treatment included flecainide and propranolol. The other child with fetal tachycardia was found to have atrial flutter and was electrically cardioverted to normal sinus rhythm as the arrhythmia was refractory to any medical treatment. The third child with fetal bradycardia was found to have corrected transposition of the great arteries and complete atrioventricular block and was permanently paced four months after birth. The fourth child was found to have Long QT syndrome with second degree atrioventricular block 2:1 and died suddenly three months after birth. The first two children were free of arrhythmia and symptoms during follow-up.
Conclusions: Serious fetal have good prognosis under appropriate medical treatment except for Long QT syndrome with bradycardia.
P-09-005 Preoperative treatment of neonates with transposition of the great arteries in neonatal intensive care units of our hospital
N. Eleftherakis2, H. Bouza1, M. Koumenidou1, M. Xanthou1, V. Thanopoulos2
1B Nicu “Aghia Sophia” Children's Hospital, Athens, Greece; 2Department of Cardiology “Aghia Sophia” Children's Hospital, Athens, Greece
Objective: Aim of the present study is to describe the treatment of neonates with TGA before their arterial switch operation.
Methods: We studied 53 neonates, 39/53 (73.58%) male and 14/53 (26.41%) female with TGA admitted in our hospital from January 2002 until December 2004. Gestational Duration was 38.4 ± 2.9 weeks and body weight at birth was 3140 ±970 g. Duration of hospitalization was 8–30 (21.6 ± 3.7) days. We examined the above mentioned neonates concerning their medical and invasive treatment with cardiac catheterization and their preoperative outcome.
Results: Establishment of diagnosis of TGA by echocardiogram performed within two hours after admission. All neonates were treated with intravenous prostaglandin 0.025–0.075 μg/kg/min and dopamine 8 μg/kg/min started on admission and kept for 3–10 days after admission. Cardiac catheterization and atrial septostomy was performed in 52/53 (98.11%) neonates 2–24 hours after admission. Preoperative mortality was 4/53 (7.55%) due to septicemia 2/4 (50%), prematurity with serious extracardiac problems 1/4 (25%) and refractory pulmonary hypertension 1/4 (25%).
Conclusions: Preoperative treatment of neonates with TGA includes intravenous prostaglandin and dopamine and elective atrial septostomy. Main cause of mortality during this period is septicemia.
P-09-006 Seasonal variation of full term births of neonates with serious congenital heart disease (CHD) needing intensive care immediately after birth
M. Koumenidou1, N. Eleftherakis2, H. Bouza1, M. Xanthou1, V. Thanopoulos2
1B Nicu “Aghia Sophia” Children's Hospital, Athens, Greece; 2Cardiology Department “Aghia Sophia” Children's Hospital, Athens, Greece
Objective: Purpose of the present study is to examine if there is seasonal variation in full term births of neonates with serious structural CHD.
Methods: We studied 206 full-term neonates, 116/206 (56.31%) male and 90/206 (43.69%) female with CHD admitted to our Neonatal Intensive Care Units from January 2002 until December 2004. Neonates with nonidiopathic cardiomyopathies, cardiac tumors and arrhythmias were not included. Statistical analysis was done using the χ2 test.
Results: Neonates included in the study had the following CHD: Trnsposition of the Great Arteries 51/206, Large Ventricular Septal Defect 28/206, Coarctation of the Aorta 30/206, Pulmonary Atresia 11/206, Critical Pulmonary Stenosis 10/206, Single Ventricle 7/206, Total Anomalous Pulmonary Vein Drainage 9/206, Tetralogy of Fallot 10/206, Tricuspid Atresia 7/206, Complete Common Atrioventricular Canal 7/206, Serious or Critical Aortic Stenosis12/206, Hypoplastic Left Heart Syndrome 8/206, Aortic Arch Interruption 6/206, Double Outlet Right Ventricle 6/206, Truncus Arteriosus 4/206. They were born as follows: January 21/206, February 16/206, March 17/206, April 17/206, May 12/206, June 11/206, July 21/206, August 22/206, September 17/206, October 21/206, November 17/206, December 14/206. The dissimilarity in monthly variation of births was not significant (p = 0.67).
Conclusions: There is no seasonal variation in full term births of neonates with serious structural CHD.
P-09-007 Fetal rhabdomyoma – Case report
I. Djukic, V. Miketic
Department of Gynecology and Obstetrics, Clinical Centre of Montenegro, Podgorica, Yugoslavia
Congenital tumors of the heart are extremely rare, their incidence is estimated at 0.1/1000 live births. The most common is rhabdomyoma which has an incidence three times that of theratoma or myxoma. Rhabdomyoma indicates fetal tuberous sclerosis up to 78% of cases, with the majority resulting from new mutations.
The echocardiografic diagnosis is based on finding one or more hiperechogenic masses within heart. They can produce mechanical obstruction to ventricular inflow and outflow with subsequent congestive heart failure (hydrops). An arrhythmia is often present (both brady and tachyarrhythmia's). Cardiomegaly is also a frequent finding.
Case Report: A 26-year-old woman G-2, P-1 was referred to a routine obstetrical ultrasound. Sonographic evaluation of the fetus revealed symmetrical biometric measurements of the fetal head, abdomen and long bones consistent with an estimated gestational age of 29 weeks. Cross-sectional evaluation of the fetal thorax revealed cardiomegaly as well as a large homogeneous, solid, echogenic mass. The sonographic appearance and location of the mass were consistent with the diagnosis of a cardiac rhabdomyoma. Because of the tumor size and bad prognosis, termination of pregnancy offered and obtained. HP analysis confirmed the ultrasound diagnosis.
P-09-008 Management of fetal tachycardia – experience of a Portuguese center
I. Silva, M. Almeida, A. Nordeste, G. Mimoso, E. Castela, J. Mesquita
Maternidade Bissaya-Barreto, Coimbra, Portugal
Objective: Fetal tachycardia is associated with high mortality due to progression to ventricular dysfunction and hydrops fetalis. Anti-arrhythmic therapy can be given to the mother and digoxin is the most frequently used first-line drug for fetal tachycardia.
Methods: In this study we analysed all fetuses with sustained tachycardia, diagnosed in an Obstetric Tertiary Unit with 3100 delivers/year, since 1991. They were all monitored with fetal echocardiograms and digoxin was the drug used for in utero therapy.
Results: We found 24 cases of fetal tachycardia in about 46,000 deliveries (incidence of 0.5‰) diagnosed between 24–37 weeks of gestation. In 11 cases (45.8%) the rhythm reverted spontaneously during pregnancy (between 26–33 weeks). Three babies were delivered at the time of diagnosis, all were at term and not complicated by ventricular dysfunction. Ten cases (41.7%) were submitted to treatment with digoxin in utero and 6 cases reverted to sinusal rhythm. Four fetuses were delivered urgently in tachycardia during digoxin therapy (failure rate 30%) but reversion occurred in post-natal period. The average gestational age of delivery was 37 weeks and eight babies were preterm. Eight babies needed cardiovascular therapy after birth. The babies with hydrops or rhythm disturbance at birth were followed by a paediatric cardiologist team.
Conclusions: This study shows the efficacy and safety of the treatment of fetal tachycardia with digoxin in fetus in the third trimester, even when hydrops is present. Because of possible maternal and fetal side effects, therapy with digoxin should be monitored by a multidisciplinary team with ultrasound and clinical specialist.
P-09-009 Increase nuchal translucency in the first trimester a marker for congenital nephrotic syndrome
B. Orive1, J. Elorz2, P. Morales1
1Hospital Txagorritxu, Vitoria, Spain; 2Hospital Cruces, Bilbao, Spain
Objective: Increased nuchal translucency thickness at 10–14 weeks of gestation has been associated with heart defects, structural abnormalities and genetic and chromosomal anomalies. Congenital Nephrotic Syndrome Finnish Type is an autosomal recessive condition with prevalence of about 1 in 8000 in Finland; but it is very rare in non-Finnish couples. We report a case of Congenital Nephrotic Syndrome of the Finnish Type, a rare cause of renal failure in infants, presented with increased nuchal translucency at the 13 week prenatal scan.
Case Report: A 29 year-old woman, referred to our hospital for amniocentesis because of enhanced nuchal translucency observed at the routine 13 week scan (4.7 mm). Karyotype was 46 XX and prenatal ultrasonography did no disclose any other anomaly. Kidneys and amniotic fluid volume appeared normal. At 36 week of gestation a normal female who weigh 1900 g with generalized edema was born. The placenta had a relevant edema and a weight of 900 g (47% of the fetal weight). There was severe proteinuria (protein/creatinine ratio 32), and severe hypoalbuminemia (0.9 g/l). An open renal biopsy, accomplished at 6 months showed dilated cystic proximal convoluted tubules. Immunofluorescence staining for inmunoglobulins and complement was negative. The changes were consistent with the diagnosis of Congenital Nephrotic Syndrome Finnish Type. The newborn was treated with albumin infusions, diuretics and nutritional support by the use of gastrostomy, L-tyrosine and GH, ACE inhibitors and platelet aggregation inhibitor agents were given. She developed a progressive renal failure and a successful renal transplant was performed at 3 years.
Conclusions: The finding of the present report suggests that Congenital Nephrotic Syndrome can present in the first trimester of pregnancy with increased nuchal translucency.
P-09-010 Prenatal diagnosis of cantrell's syndrome with lemon sign in the second trimester
C. Dane, M. Yayla, B. Dane
Haseki Education & Research Hospital, Department of Gynecology & Obstetrics, Division of Perinatology, Istanbul, Turkey
Pentalogy of Cantrell is a rare syndrome that is composed of a midline, supraumbilical abdominal wall defect, a defect of the lower sternum, a deficiency of the anterior diaphragm, a defect in the diaphragmatic pericardium and congenital intracardiac defects. This results from the developmental failure of a segment of the lateral mesoderm at around 14 to 18 days of embryonic life.
We present a case of pentalogy of Cantrell in which 20 gestational weeks. The fetus has showing omphalocele, thoraco-lumbar spina bifida, hydrocephalus, lemon sign and ectopia cordis and confirmed as a pentalogy of Cantrell (variant form) postnatal.
In this article we discussed Cantrell's pentalogy with the literature findings. Ectopia cordis associated with an omphalocele on prenatal ultrasonography is highly suggestive of pentalogy of Cantrell. The prognosis depends on kinds and severity of the associated intracardiac defect.
P-09-011 The significance of antenatal diagnosis of single umbilical artery
M. Khalil
Security Forces Hospital, Riyadh, Saudi Arabia
Objective: A prospective study to determine the frequency, nature and sonographic detection of structural anomalies in fetuses with single umbilical artery.
Methods: During the period from August 2002–June 2005 all cases of fetal single umbilical artery in a routine obstetric population at Security Forces Hospital, KSA were studied. Targeted sonograms and perinatal follow up were obtained.
Results: One hundred thirty-two cases of single umbilical artery were diagnosed on the basis of initial sonograms, 98 fetuses, 74.2% thought to have isolated single umbilical arteries, and 34, 25.8% had nonisolated single umbilical arteries, 6 out of 132 were subsequently shown to have 3-vessels cord. Among the 12,868 cases with three normal cord vessels by prenatal ultrasonogram, 13 infant confirmed to have single umbilical artery. So, the sensitivity, specificity, positive predictive value and negative predictive value of prenatal ultrasonographic diagnosis of single umbilical artery were 90.6%, 99.9%, 95.4% and 99.8% respectively. Out of the 34 nonisolated single umbilical artery, aneuploidy was present in 4 (11.7%) fetuses, however an apparently isolated single umbilical artery was never associated with an abnormal karyotype.
Conclusion: Color Doppler evaluation of the intrapelvic umbilical arteries is recommended to avoid a false-positive diagnosis of single umbilical artery. The finding of an apparently isolated single umbilical artery did not appear to increase the risk of aneuploidy.
P-09-012 Prenatal diagnosis of myoblastoma granulare: A case report
A. Novakov Mikic1, A. Kiralj2, K. Koprivsek3, M. Kacansk4
1Department of Obstetrics and Gynaecology, Novi Sad, Serbia; 2Department of Maxilofacial Surgery, Novi Sad, Serbia; 3Institute of Magnetic Resonance, Sremska Kamenica, Serbia; 4Institute of Pathology and Hystology, Novi Sad, Serbia
Objective: Presenting a case of prenatal diagnosis of a tumor protruding from oral cavity diagnosed at 28 weeks' gestation.
Methods: After the diagnosis of oral cavity tumor at 2D ultrasound was done, a 3D scan was performed which confirmed the diagnosis and revealed the peduncle at the upper border of maxilla. A detailed scan has been performed and no additional anomalies were seen. Magnetic resonance examination was organized which confirmed the diagnosis and the site of the tumor. Karyotype was previously done, and a normal female karyotype was found.
Results: Regular 3-week scans were arranged to follow the growth of the tumor as well as the state of the amniotic fluid. No tumor growth was seen, and the amniotic fluid volume was normal until the gestation of 39 weeks when a caesarean section was scheduled, due to fear that during a vaginal birth a disruption of tumor might have take place. Maxilofacial surgeon was present during an uneventful Cesarean section and a complete surgical excision was done immediately after the baby was extracted and umbilical cord ligated. The pathohystological diagnosis was Myoblastoma granulare. The female newborn was developing normally and at 5 months of age no traces of the scarring at the place of the tumor are seen.
Conclusion: In cases of prenatal diagnosis of oral cavity tumors, where a development of polyhydramnios can be expected as well as difficulties with feeding and breathing after birth, it is important to make a plan for adequate follow-up and a prompt surgical treatment immediately after birth.
P-09-013 Fetal arrhythmia – premature atrial contractions
K. Liska1, Z. Zizka2
1Department of Neonatology, General Faculty Hospital, Charles University, Prague, Czech Republic; 2Department of Obstetrics and Gynecology, General Faculty Hospital, Charles University, Prague, Czech Republic
Aim: Premature atrial contractions (PACs) are the most common cause of an irregular fetal heart rhythm. The aim of our study was to evaluate PACs during pregnancy for the potential risk of changing to severe forms of fetal arrhythmia such as supraventricular tachycardia (SVT) or atrial flutter that can lead to cardiac failure and fetal hydrops.
Study Design: Prospective study. We evaluated 102 fetuses with PACs detected by fetal echocardiography. In PACs, a detailed examination of the heart anatomy was performed to exclude congenital heart malformations. The fetal heart rate was analyzed by M-mode echocardiography every 2–3 weeks until delivery.
Results: We evaluated 102 cases of PACs. The median of detection was 31 gestational weeks (range 18–41 g.w.), PACs frequency – median 8 per minute (range 2–40/min), ventricular rate – median 132 per minute (range 80–152/min). 51% of PACs resolved spontaneously during pregnancy. 3 cases with a slow ventricular rate of 80–100/min in blocked atrial bigeminy were diagnosed, no neonate was hypoxic after delivery. No neonate with PACs had a congenital heart defect. We did not find a change of PACs to any severe form of fetal arrhythmia during pregnancy, only 1 neonate had a short episode of SVT after delivery.
Conclusions: PACs usually occur in fetuses with a normal heart anatomy, they are benign in nature and some of them resolve spontaneously during pregnancy or early in the postnatal period. The prognosis for the fetus and newborn is very good. In PACs detected prenatally, we recommend only to monitor the fetal heart rate by M-mode every 2–3 weeks. A slow ventricular rate due to blocked ectopic beats is not an indication for termination of pregnancy or caesarean section.
P-09-014 Cordocentesis of 198 cases in a university clinic of turkey during a 7-year period
T. Sener1, H.M. Tanir1, B. Durak2, M. Kaya1, T. Oge1, E. Tepeli2, S. Artan2
1Department of Obstetrics and Gynecology, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey; 2Department of Medical Genetics, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey
Methods: From January 1998 to November 2005, 198 pregnancies ranging from 20 to 23 weeks of gestation were undergone cordocentesis. The procedure was performed by a single experienced physician and performed under the guidance of real-time, 2D ultrasonography (Toshiba Sonolayer SSA-250 A), using 20–22 gauge needle. Either free loop of the cord or mostly the region of the cord entry into the placenta were chosen. All samples were immediately sent to the genetic laboratory and were observed with regard to early procedure-related complications such as fetal bradycardia or bleeeding into the amniotic cavity.
Results: Indications of cordocentesis were as follows: presence of fetal anomaly (37.9%), late referral of cases with triple test results (27.8%), intrauterine fetal growth restriction (6.1%), maternal anxiety (0.5%), abnormal amniocentesis results (6.1%), non-immune hydrops fetalis (3.0%), advanced maternal age >35 (10.6%). Of 75 fetuses with fetal anomaly on ultrasonography, only 8% (n: 6) revealed karyotype abnormalities. None of the cases with non-immune hydrops fetalis and maternal anxiety showed chromosomal aberrations. Of 55 cases with late referral, in whom triple test results were suspicious for the presence of aneuploidy, 3 (5.5%) cases had chromosomal aberrations.
Of 198 cases, 15 (7.5%) had chromosomal anomalies based on karyotype analysis, most of which were terminated due to trisomy 21 (40%). Two cases had normal karyotype. Cordocentesis of whom were performed due to the presence of fetal anomaly on ultrasonographic scan. However, all of these cases were terminated due to gross structural cardiac and cranial anomalies. With regard to procedure-related complications, hemorrhage from the umbilical cord (n: 13, 6.6%) and fetal bradycardia (n: 15, 7.6%) were detected. Fetal loss rate due to procedure itself was found to be 1/198.
Conclusions: In 29 (14.6%) cases, cordocentesis lead to procedure-related complications. Fetal loss rate in a 7-year period of FUBS was 1/198 in our institution. Every institution having prenatal diagnosis unit should document their own data on a periodical basis, which enable clinicians to compare their data, ameliorate their techniques as to give better care to patients in a less invasive way.
P-09-015 Evaluation of 894 amniocentesis in a 7-year period in a university hospital of mid-anatolian region of Turkey
T. Sener1, H.M. Tanir1, B. Durak2, M. Kaya1, T. Oge1, E. Egeli2, S. Artan2
1Department of Obstetrics and Gynecology, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey; 2Department of Medical Genetics, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey
Objective: We aimed to document our data regarding the evaluation of our amniocentesis cases in a single, university-based institution, which would lead us to better evaluate the patients.
Methods: From January 1998 to November 2005, a total number of 894 cases were undergone amniocentesis by two experienced clinicians. Gestational age distributions, indications, karyotype analysis and complications of the procedure were documented retrospectively. Amniocenteses were performed under the guidance of real-time, 2D ultrasonography (Toshiba Sonolayer SSA-250 A). All amniocenteses were performed by means of free-hand technique.
Results: Triple test results (n: 343) and advanced maternal age (n: 286) constituted the majority of procedure indications, 32% and 38.4% respectively. Maternal anxiety (4.9%), suspicious ultrasonography findings (7.3%), history of chromosomally abnormal infant (3.5%) were other amnicentesis indications. Of 894 amniocentesis, 21 (2.3%) casaes had chromosomal abnormalities, most of whose pregnancies (66.6%) were terminated due to autosomal trisomies such as trisomy 21 and 18. In only 2.1% (n: 19) of cases, a culture failure was seen. Most of the cases (95.6%), karyotype analyses were normal. With regard to intraoperative complications of amniocentesis, double-needle entry was present in 10 (1.1%) of cases. In 14 (1.5%) cases, bleeding into amniotic cavity was observed. Transplacental needle passage was observed in 271 (30.3%) of cases. No maternal morbidity like infection or organ laserations were observed. Fetal complications included 5 cases with amniotic fluid drainage and 5 fetal loss following the procedure. Fetal loss rate was 0.6% (5/894). All fetal losses were within 3 weeks following the procedure (median: 15 days).
Conclusions: During a 7-year retrospective cohort in a single university institution, 2.1% cases had complications related to amniocentesis per se. Those above-mentioned data would definitely lead us to better evaluate our cases with great vigilance to the real indication of the procedure, avoiding procedure-related fetal and maternal morbidities.
P-09-016 Non-immune hydrops fetalis due to meconium peritonitis: A case report
H.M. Tanir1, T. Sener1, N. Tekin2, A. Karatas1, Z. Karatas2, B. Tokar3
1Department of Obstetrics and Gynecology, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey; 2Department of Pediatrics, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey; 3Department of Pediatric Surgery, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey
Objective: This case report aims to present an infrequent cause of non-immune hydrops fetalis, meconium peritonitis, definitive diagnosis of which could only be possible postpartum.
Methods: A 25 years-old women (G:3P:1A:1) at 30 weeks of gestation was referred to the clinic due to the presence of premature uterine contractions. In previous visits, we noticed the history of fetal ascites and polyhydramnios. Having excluded any infectious etiology leading preterm labor, we initiated a parenteral beta mimetic tocolytic therapy together with bethametazone Prior to drug use, her vaginal examination revealed 3 cm cervical dilatation and 40% cervical effacement without any amniotic fluid drainage. Initial detailed ultrasonography, fetal echocardiography and laboratory evaluation confirmed the findings but failed to demonstrate any specific cause during the antenatal stay. Cordocentesis showed a female 46 XX karyotype. She spontaneously gave birth to a 2730 g, female infant with distended abdomen 7 day after her admission.
Results: Following a nasogastric drainage for 48 hours postpartum and rectal irrigation with saline solution, no meconium passage was observed. Due to her progressive deterioration in the clinical condition and lack of meconium passage for 72 hours, a laparotomy was contemplated. Laparotomy findings revealed fibrotic, conglomerated intestinal loops with brownish-green peritoneal exudate. Having aspirated the exudate, a mesothelial defect was found in conjunct with perforated intestinal segment of 15 cm in longitudinal axis at jejuno-ileal segment. This perforated region was completely resected. Her postoperative course was dismal. At 18th day postpartum, during her nursing by her mother, she was suddenly deteriorated and her respirations became irregular. She was then put on endotracheal intubation. She died 5 days following the intubation.
Conclusions: The fetal prognosis of non-immune hydrops fetalis depends on its specific cause. In most of cases, definitive diagnosis can not be made antenatally. Menonium peritonitis is rare cause of NIHF and has dismal neonatal prognosis. In addition to the underlying cause, the impact of premature delivery may further deteriorate the neonatal clinical course.
P-09-017 Chorionic villus sampling (CVS) of 68 cases: A retrospective analysis
T. Sener1, H.M. Tanir1, B. Durak2, M. Kaya1, T. Oge1, E. Tepeli2, S. Artan2
1Department of Obstetrics and Gynecology, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey; 2Department of Medical Genetics, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey
Objective: Through this study, we aimed to analyze our CVS data in our institution with regard to its indications, results and complications in a 7-year period.
Methods: From January 1998 to November 2005, 68 pregnancies ranging from 12 to 14 weeks of pregnancy were undergone CVS. The procedure was performed by a single experienced physician and performed under the guidance of real-time, two-dimensional ultrasonography (Toshiba Sonolayer SSA-250 A), using 18–20 gauge needle.
Results: Indications of CVS were as follows: nuchal thickness ≥95 percentile (19.1%), high risk conferred by first trimester combined test (27.9%), maternal age ≥35 (10.3%), pathologic ultrasonography findings (13.2%), maternal anxiety (4.4%), history of chromosomally abnormal infant (11.8%). Of 68 CVS cases, 4 (5.9%) had abnormal fetal karyotype analysis. Of 13 fetuses with increased nuchal translucency, 15.4% (n: 2) fetuses revealed karyotype abnormalities. None of the cases with high-risk combined test results, advance maternal age or historical risk factors showed fetal chromosomal anomalies. Two cases were terminated due to trisomy 21 based on CVS results. In other two cases, karyotype analysis showed balanced translocation 46XX t(15;19) and 46 XY t(9;10), respectively. None of the cases revelaed confined placental mosaicism. There was no fetal loss detected during this period.
Conclusions: CVS results in our hands revealed no procedure-related fetal loss rate. The result of this study encouraged us to perform more CVS to ensure pregnant women in an earlier gestational age about her fetus chromosomal set up.
P-09-018 Central nervous system (CNS) anomalies: 5 years' experience
H.M. Tanir, T. Sener, E. Ozalp, H. Ilgin
Department of Obstetrics and Gynecology, Eskisehir Osmangazi University School of Medicine, Eskisehir, Turkey
Objective: The aim of this study to retrospectively document the CNS anomalies during a 5 year period at a university hospital in mid-anatolian region of Turkey.
Methods: From January 2000 to November 2005, CNS anomalies were retrieved from hospital records. Patient's characteristics, gestational week at time of detection, anomaly type, mode of delivery and neonatal outcomes were retrospectively analyzed.
Results: Of 2789 deliveries in 5-year period, 17 CNS anomalies were detected, showing an incidence of 1/164. The percentage of referred cases was 47% (8/17). Mean gestational age of cases was 26.5 ± 1.2 years (20–40 years). Cases were composed of 4 meningocele, 1 anencephaly, 1 Meckel-Gruber syndrome, 5 meningomyelocele, 1 myeloschisis, 1 encephalocele, 3 isolated bilateral ventriculomegaly, 1 sacrococcygeal teratoma. Out of 4 cases with meningomyelocele, 2 cases were offered immediate postoperative neurosurgery. In latter cases, however, parents denied any surgical procedure. Two cases were undergone ventriculo-peritoneal shunt and their postoperative courses were uneventful. Intrauterine and intrapartum fetal demise were seen in one and 7 cases, respectively. The former was the one with occipital encephalocele detected at 27 weeks of gestation. Pregnancy termination was performed in 8 cases (47%), mean gestational age of whom at termination was 24.3 ± 2.1 weeks. Mean age of cases delivered by caesarean section was 39.1 ± 1.1 weeks. One case with sacrococcygeal teratoma was surgically corrected postpartum without any neurologic deficit.
Conclusions: Our series has shown that the incidence of CNS anomalies was 1/164. Early detection and appropritae perinatal follow-up of CNS anomalies may decrease the perinatal mortality rate and may lead to a more favorable delivery time that would be appropriate for optimal neurosurgical approach.
P-09-019 The clinical analysis of umbilical cord stricture and intrauterine fetal death in Korea
J.Y. Hwang, D.H. Lee, J.S. Cho
Kangwon National University, Chunchon, South Korea
Objective: To evaluate the clinical significance of umbilical cord stricture and intrauterine fetal death in Korea.
Methods: A retrospective study was conducted by searching our clinical database and KSOG database collected from January 1980 to April 2005. We found 6 cases of cord stricture in Korea. But we analyzed the clinical features of 5 cases because 1 case information was insufficient.
Results: The gestational period at fetal death in uterus ranged from 30th to 39th weeks, the mean gestational age was 33 ± 4.2 weeks. The mean birth weight was 1376 ± 867 gm. The cord length at delivery ranged from 26cm to 82cm weeks, the mean cord length was 63.2 ± 23.3 mm. This mean cord length was longer than that of normal cord study in Korea. The mean placenta weight/fetal weight ratio was 33.3 ± 16.3%. The mean cord stricture diameter/normal cord diameter ratio at delivery was 9.5 ± 9.2%. Of 5 cases, 4 cases had fibrosis in umbilical cord stricture site (80%) and 4 fetus were small for gestational age.
Conclusion: These data know that the cord length of umbilical cord stricture associated with fetal death was longer than that of normal cord study. The common pathologic finding was fibrosis and common clinical finding was small for gestational age.
P-09-020 Iron-deficiency anemia – proper timing for suplementation therapy
N. Sulovic, O. Kontic-Vucinic, N. Radunovic, M. Mitrovic, I. Pilic
IGA KCS, Belgrade, Serbia
Aim: Does and how much iron (Fe) supplementation depends on timing of beginning of therapy.
Material and Methods: 70 pregnant women were divided into two groups; each consisted of 35 anemic patients, diagnosed in first, and mid or late second trimester. All patients were treated with 120mg of elementary Fe. We used feritin and hemoglobin levels as control parameters.
Results: Feritin and hemoglobin levels were controlled 5 times during pregnancy at first and 3 times at second group:
We've found statistically significant differences between groups (df 2; 203 for p < 0.001).
All patients from the first group were delivered in term, while 3 pregnancies from second group were terminated between 31 and 35 weeks of gestation.
Hematological status of neonates was evaluated on day one postpartum:
First group: Hb 166.40 (SD 4.71), feritin 176.89 (SD 3.31).
Second group: Hb 157.8 (SD 7.9), feritin 166.7 (SD 24.2).
We found no statistically significant difference.
Conclusion: Mild and moderate forms of anemia demand supplementation therapy. Oral supplementation should be reserved for them. Effects of therapy are better if starts in early stage of gestation, although they don't influence on hematological status of neonates.
P-09-021 The index of placental lateralization in fetuses with idiopathic growth restriction
N. Karadzov-Orlic, Z. Mikovic, M. Marinkovic, B. Damnjanovic-Pazin
Ob./Gyn. Clinic “Narodni front”, Belgrade, Serbia
Objective: The purpose of this study was to evaluate the index of placental lateralization (IPL) and its correlation with parameters of fetal growth restriction.
Study Design: We prospectively analyzed 210 singleton pregnancies with idiopathic fetal growth restriction in a third-trimester. Central localization of placenta was found in none of the pregnancies. The localization of placenta was determined by using two imaginary planes: a frontal plane – which crosses uterus borders and separates uterus into a right and a left half; and a horizontal plane – which is orthogonal to previous one, and separates uterus into equal superior and inferior halves. IPL is defined as a sum of the largest placental segments in both planes, expressed in percentages. Severe placental lateralization was defined as IPL > 100 and moderate one as IPL < 100. IPL was correlated with Pourcelot index of non-placental uterine arteries, AFI index, birth weight and Apgar score at 5 minutes.
Results: In the group with IPL > 100 (mean IPL = 124.6 ±20.0, N = 75), flow velocity waveform in non-placental uterine artery was 0.66 ± 0.06; AFI 43.1 ± 13.1; birth weight 1783.7 ± 423.2 g and the 5-minute Apgar score 7.54 ± 0.7. Pregnancies were terminated in 34.92 ± 0.52 weeks of gestation and 46.1% of them with section Cesarean. IPL was shown positive correlation with Pourcelot index of non-placental uterine artery (r = 0.40, p = 0.0014), and negative correlation with AFI (r = −0.41, p = 0.001), birth weight (r = −0.36, p = 0.004) and the 5-minute Apgar score (r = −0.31, p = 0.016).
Conclusion: These findings suggest that the index of placental lateralization correlates with prenatal parametric ultrasonographic indices and neonatal outcome.
P-09-022 Campomelic dysplasia syndrome in newborn: Case report
E. Gulczynska, E. Lerch, B. Pawlowska, M. Kesiak, A. Grodzicka, J. Gadzinowski
Research Institute of Polish Mother's Memorial Hospital, Lodz, Poland
Campomelic dysplasia syndrome (CD) is a rare genetic disorder with prevalence estimated to range between 0.05–2:10,000 births. The gene responsible for the condition is SOX9 (SRY-related HMG – box gene) and is on 17q24-q25. The inheritance is autosomal dominant. About 75% of reported 46 XY patients exhibit sex reversal with completely female phenotype: the external and internal genitals are female.
Characteristic features are skeletal hypoplasias and anomalies affecting the face, head, scapulae, spine, pelvis and upper and lower limbs. The limbs are short with anterior bowing of the legs, often with pretibial skin dimples. Others extraskeletal anomalies involve the central nervous system, cardiovascular system, genitourinary system. Mental development is also abnormal. It is usually lethal in early infancy.
Diagnosis can be established by ultrasonography as early as 18 weeks of gestation.
CD should be differentiated between osteogenesis imperfecta type I and II, hypophosphasia, thanatophoric dysplasa, mesomelic dysplasia.
Authors describe a male newborn with Campomelic Dysplasia Syndrome who was born in Polish Mother's Memorial Hospital Research Institute. The baby was born by caesarean section at 36 weeks of GA with birth weight 2300g, Apgar score 6 at first minute of life. Congenital anomalies were found prenatally at 25 GA and osteogenesis imperfecta was suspected. The newborn had all characteristic features of CD syndrome and diagnosis was confirmed after radiological examinations.
P-10-001 Changes in circulating levels of corticotropin-releasing hormone, cortisol and beta-endorphines during invasive diagnostic procedures
O. Kontic-Vucinic, N. Radunovic, N. Sulovic, I. Pilic, M. Mitrovic
IGA KCS, Belgrade, Serbia
Aim: To determine whether fetal blood sampling is associated with changes in fetal and maternal circulating corticotropin-releasing hormone (CRH), beta-endorphins (BE) and cortisol concentrations.
Material and Methodology: A cross-sectional analysis was undertaken of pair fetal and maternal serum CRH, BE and cortisol, obtained between 18 and 40 weeks of gestation. All 81 pregnancies were singleton gestations. A total of 104 paired maternal and fetal samples were available for study. For comparison with maternal CRH, BE and cortisol levels, venous blood was obtained from 26 nonpregnant female. In order to compare fetal CRH, BE and cortisol with postnatal levels, blood was obtained from 24 neonates within 12 hours after spontaneous vaginal delivery (38–40 gestational weeks).
Results and Conclusion: Fetal CRH concentrations were significantly higher than neonatal values (p = 0.02) and nonpregnant adult values (p < 0.0001), but were significantly lower than maternal values (p < 0.001). Maternal CRH concentrations were significantly greater than that of nonpregnant controls (p < 0.0001). Maternal CRH concentrations also correlate with fetal cortisol (r = 0.41; p = 0.0002), and maternal cortisol (r = 0.28; p = 0.01). Fetal cortisol levels were significantly lower than maternal (p < 0.0001), neonatal (p = 0.0001) and nonpregnant adult values (p < 0.0001). In contrast, maternal cortisol values were significantly higher then of nonpregnant adults (p < 0.0001). Fetal blood sampling were associated with significant increases in BE release. It seems that fetus itself is the primary source of elevated circulating BE levels.
P-10-002 Outcome of post-term pregnancies
V. Astover1, A. Siller2, A. Ormisson3
1Children's Clinic, Tartu University Hospital, Tartu, Estonia; 2Women's Clinic, Tartu University Hospital, Tartu, Estonia; 3Dept. of Pediatrics, University of Tartu, Tartu, Estonia
Objective: To study the perinatal outcome of the post-term pregnancies.
Methods: Case reports of 207 mothers with prolonged pregnancy and their newborns were studied retrospectively during the years 2004–2005 in Tartu University Women's Clinic. The outcomes of post-term pregnancies were compared to the outcome of term pregnancies during the same time period.
Results: Post-term infants (PTI) (n = 207) occurred in 5.2% of all newborns with the gestational age ≥37 weeks (n = 4011). The labour induction was used in 56% in PTI group, which resulted in caesarean delivery in ¼ and vaginal delivery in ¾ cases. The caesarean section rate was significantly higher in PTI group than in term infants' (TI) group (20.8% vs. 14.7%, p = 0.0223, OR 1.52, 95% CI: 1.048–2.169). The birth asphyxia was higher presented in PTI group (8.7% vs. 4.4%, p = 0.0078, OR 2.05, 95% CI: 1.159–3.426). The newborns in PTI group were twice frequently macrosomic than in TI group (22.2% vs. 9%, p = 0.0001, OR 2.9, 95% CI 1.998–4.119). Birth trauma occurred significantly more often in PTI group (6.3% vs. 2.3%, OR 2.8, 95% CI: 1.430–3.042). There were no differencies in intrauterine growth retardation, shoulder dystocia, perinatal deaths and maternal and neonatal infections between two groups.
Conclusion: The outcome of post-term pregnancies resulted in significantly higher rate of caesarean birth, asphyxia, fetal macrosomia and birth trauma. Post-term pregnancies remain an obstetrical risk group.
P-10-003 Left isomerism – a case report
G. Borges, P. Veca, J.P. Marques, A. Melo, L.M. Graca
Santa Maria Hospital, Lisbon, Portugal
Background: Heterotaxy syndromes are very rare and expressed as right isomerism (bilateral right-sidedness) or left isomerism (bilateral left-sidedness). Usually, they are associated with visceral and cardiac abnormalities.
Clinical Report: We report a case of a fetus with a situs ambiguous, diagnosed in the second-trimester scan (21 weeks).The scan showed the stomach in the right side without other malformation, and the fetal echocardiographic examination detected the azygos continuation of the interrupted inferior caval vein. A normal baby was delivered at 41 weeks. In the postnatal period it was diagnosed a left isomerism in an otherwise healthy baby. The stomach was in the right side, there where two spleens on the right side, the liver was in midline and the inferior caval vein was interrupted.
Comments: Left isomerism or polysplenia syndrome is the rarest of the heterotaxy syndromes, being found in 1:40,000 live births.
P-10-004 Use of misoprostol for second trimester pregnancy termination with a live fetus
S. Santo, N. Clode, L.M. Graca
Hospital Santa Maria, Lisbon, Portugal
Objective: To evaluate the efficacy and safety of misoprostol in second trimester pregnancy termination.
Methods: Data concerning second trimester pregnancy termination (14–26 wks) with a live fetus using vaginal misoprostol over a three year period were reviewed. Failed induction was considered when pregnancy termination was not achieved after two trials of misoprostol (400 μg every 6 hours for 48 h) with 24 h interval. Median time to delivery and misoprostol dose were determined. Maternal outcomes – fever, postpartum hemorrhage, uterine rupture and placental retention – were evaluated.
Results: Eighty eight women were included. The median gestational age was 18.7 weeks. The indications for pregnancy termination were: fetal anomalies (66 cases – 75%), premature rupture of membranes (14 cases – 16%) and maternal disease (8 cases – 9%). Failed induction occurred in 11 cases (12.5%).
The median time to achieve delivery was 19 hours (2–76), the median number of misoprostol administrations was 2 (1–6). There were no major complications. Forty one cases (53.2%) were submitted to uterine curettage; 14 had placental retention.
Conclusion: Misoprostol in the used regimen appears to be an efficient method in second trimester pregnancy termination with an optimal safety profile.
P-10-005 Emergency cervical cerclage – a single centre experience
G. Daskalakis, N. Papantoniou, S. Mesogitis, K. Lambrinopoulos, M. Theodora, V. Koumbis, A. Antsaklis
Athens University, Athens, Greece
Objective: To evaluate the efficacy of emergency cerclage in cases with dilated cervix and protruding fetal membranes, in a group of women considered low-risk for preterm delivery by their obstetric history.
Methods: All cases of cervical dilatation and bulging membranes were detected through a transvaginal ultrasonographic screening for preterm delivery between 18 and 26 weeks (wks), during a six-year study period. 29 women underwent an emergency cervical cerclage and composed the “cerclage group”, while 17 others refused and formed the “bed rest group”. All patients were given antibiotics and prophylactic tocolysis.
Results: The mean prolongation of pregnancy (8.8 wks) and the mean birth weight (2101 g) after cerclage placement differed significantly from those of the “bed rest group” (3.1 wks and 739 g, respectively). 25 of the 29 pregnancies in the “cerclage group” ended in live birth, compared to 7 of the 17 pregnancies in the “bed rest group” (p = 0.001) (RR 0.33, 95% CI: 0.11–0.98). Neonatal survival was 96% in the “cerclage group” and 57.1% in the “bed rest group” (p = 0.025) (RR 0.09, 95% CI: 0.01–0.76). The preterm delivery rate <32 wks was 31% and 94.1% in the “cerclage” and the “bed rest group” respectively (p < 0.001) (RR 0.33, 95% CI: 0.19–0.57), while the admission to NICU was 28 and 85.7% in the two groups respectively, (p = 0.01) (RR 0.33, 95% CI: 0.16–0.66).
Conclusions: Emergency cervical cerclage can be safely accomplished in women with dilated cervix and bulging membranes. It can reduce preterm delivery before 32 wks and improve neonatal survival compared to the bed rest.
P-10-006 Placental pathology in women with gestational diabetes
G. Daskalakis, S. Marinopoulos, V. Krielesi, A. Papananagiotou, N. Papantoniou, S. Mesogitis, K. Lambrinopoulos, A. Antsaklis
Athens University, Athens, Greece
Objective: The aim of this study was to test this hypothesis by investigating various macroscopic and microscopic features of the placenta in pregnancies complicated by gestational diabetes, compared to non-diabetic pregnancies.
Methods: Forty singleton pregnancies complicated by gestational diabetes were recruited at the time of diagnosis between 28 and 35 weeks of gestation and compared to forty consecutive normal pregnancies (control group). Only women with insulin-dependent gestational diabetes were included. Exclusion criteria were the presence of hypertension, pre-eclampsia, intra-uterine growth retardation (birth weight <10th percentile) or major congenital fetal malformations. Representative specimens were taken from the cord, the cord insertion, placental membranes and full thickness of macroscopically normal placenta and from abnormal areas.
Results: Significantly higher placental weights (C = 668 ± 168 g; GDM = 734 ± 185 g; P < 0.01) and significantly lower fetal/placental weight ratios (C = 4.52 ± 0.76; GDM = 4.13 ± 0.82; P < 0.05) were found in pregnancies complicated by gestational diabetes compared to normal pregnancies. The presence of degenerative lesions such as fibrinoid necrosis and placenta calcifications was apparent, mainly in the diabetes group. Vascular lesions, like vessel infarctions, mural thrombosis and chorangiosis, were presented in the same distribution. These findings along with villous immaturity were significantly increased in the placentas of women with diabetes compared with controls.
Conclusions: Infants of diabetic women may be protected against hypoxemia because of a relative high placental weight corresponding for an increased exchange surface. The question, if an interaction exists between placental pathological changes and fetal vascular function, early during life in uterus, seems to be of substantial base.
P-10-007 Ultrasound examination of the cervix and preterm labour. Current status
G. Daskalakis, A. Antsaklis
Athens University, Athens, Greece
Many studies dealing with the ultrasonographic evaluation of the cervix during the course of pregnancy have suggested that cervical changes may detect or exclude the risk of preterm delivery. A clear relationship has been established between decreased cervical length and the risk of spontaneous preterm delivery. The technique for the evaluation of the cervix has been standardized and the transvaginal ultrasonography is considered to be superior than the transabdominal or the transperineal approach. In symptomatic patients, it can reliably diagnose those who are in true preterm labour, reducing the false-positive results. Moreover, it has been proved useful as a screening method for preterm labour in both low and high-risk women, as well as in multiple pregnancies. It has also been used in women with preterm premature rupture of membranes. In these cases a correlation between cervical length and the latency period has been reported. The main disadvantage of the method is its low sensitivity and positive predictive value in a low-risk population, because of the low prevalence of preterm delivery. Therefore the cut-off value for the cervical length should be carefully selected in order to achieve an acceptable sensitivity and specificity. The type of intervention following the identification of a short cervix needs also further evaluation. Although there are studies which showed that cervical cerclage leads to an increase in cervical length, preventing preterm deliver, there are others that concluded that this type of intervention may not be of any benefit. Prospective randomized trials evaluating cervical cerclage must be performed in high-risk patients detected by transvaginal sonographic screening, in order to confirm a potential benefit.
P-10-008 Presentation of a 5 year experience on function of outpatients clinic of amniocentisis in OB/GYN department of general hospital Chania, Greece
M. Kalloniatou, C. Christodoulaki, D. Gentsidis, M. Christodoulaki, M. Kampanieris, K. Stamou, G. Daskalakis, A. Tsopelas
General Hospital of Chania, Chania, Greece
The study concerns the time interval 2000–2005. During this period 450 amniocentisis were performed.
Indications: Elective in women under 35, for D typing, for sickle-cell syndrome, in diagnosis of fetal cytomegalovirus infection, in diagnosis of fetal toxoplasmosis infection, positive prenatal screening tests: PAPPA, A – Tests, or sonographic screening for minor abnormalities such as choroid plexus cysts, thickened nuchal fold mild hydronephrosis and positive family history of cystic fibrosis, family history for fetal abnormalities.
Side Effects: amniotic fluid leakage in 5 women (2 of the fetus were aborted), in 1 woman cell culture failure.
Results: 2 Down syndromes, 2 beta thalassemia, 1 Turner syndrome, 9–15 de novo translocation (t9;15) q31; q26, 13–4 de novo translocation del 13; 14 p11; q11.
P-10-009 Comparison of fetal cerebral pathology diagnosis by magnetic resonance and ultrasound
S. Ferrero, S. Cabre, N. Porta, M.D. Gomez, A. Vela, A. Diaz, J.M. Lailla
Hospital Sant Joan de Deu, Esplugues de Llobregat, Spain
Objective: To evaluate the diagnosis capability of ultrasound (US) with MR in fetal brain pathology study.
Material and Methods: In 45 months, 35 MR were required for the evaluation of fetal brain. The US examination was performed at a mean pregnancy age of 28 and MR at 31 weeks.
Results: In 34.82% of cases (12/35) US diagnosis was similar to MR and postnatal follow-up. The mean pathology in this group was ventriculomegaly: 58.33% (7/12). MR exploration was more accurate in 51.4% of the cases (18/35). In this group ventriculomegaly represents 61%, midline deffects 22% and posterior fossa pathology 11.11%. We also compared ultrasound and MR findings by pathologies: for ventriculomegaly, 75% of cases the results of US; for hydrocephaly, MR was more accurate in 50% and similar as US in 37%; for agenesis of the corpus callosum, both explorations were different in 60% and MR more accurate in 40%; in posterior fossa disorders, the results were similar in 80% for MR and US. The posnatal follow-up was possible in 71% of the cases (25/35): the evolution was good in 44% (all of them appropriate diagnosed prenatally); 7 cases required surgery for mielomeningocoele or ventriculomegaly (all diagnosed prenatally) and 2 death cases for severe hydrocephaly, one of them was rejected by MR.
Discussion: Ultrasound performed by experimented explorer is the elective exploration in cases of fetal brain anomalies. In case of uncertain diagnosis, MR is indicated as complementary tool. In our experience, US is very accurate for severe ventriculomegaly, while MR is useful for rejecting light ventriculomegalies and in the diagnosis of associated brain pathology.
P-10-010 First trimester miscarriages – ultrasonographic and cytogenetic findings
U. Radivojevic, Z. Puzigaca, B. Milanovic, Z. Aleksov, R. Nikolic, M. Scekic, S. Grkovic
Clinic for Human Reproduction, Mother and Child Health Care Institute, Belgrade, Serbia
Objective: First trimester miscarriages are complicating 15 to 20% of pregnancies. They are the leading cause of gynecology emergencies. Chromosome abnormalities can cause 50–60% of pregnancy losses. We conducted a retrospective study to present the proportions of incomplete and missed miscarriage or an anembryonic pregnancies, ultrasonographicaly diagnosed in 343 women with spontaneous miscarriage. We also present the cytogenetic findings in chorionic villi samples of 49 miscarriages.
Methods: Transvaginal or transabdominal ultrasonography was used at the first visit to identify those women with an incomplete miscarriage (IM), defined as the presence of heterogeneous products of conception within the uterus and distinguishable from a missed miscarriage (MM) or an anembryonic pregnancy (AP). Subjects were offered the choice of surgical evacuation of the uterus under general anesthesia or expectant management with a follow-up visits. All IM patients wished an immediate termination of pregnancy. MM and AP patients were advised to terminate pregnancy after 2–4 successive follow up visits. Cytogenetic analysis was performed in 15 cases of AP and 34 cases of MM.
Results: Out of 343 patients, IM was diagnosed in 70 cases (20.4%), MM in 176 (51.3%) and AP in 97 (28.3%) patients. Karyotype was obtained in 15 AP and was normal in 10 cases. Out of 34 MM karyotypes, chromosomal abnormalities were found in 22 cases (81.5%). Nine IM, 8 AP and 32 MM had previous obstetric history of first trimester miscarriages.
Conclusion: Missed miscarriage was the cause of 51.3% of first trimester pregnancy losses in the study, and the highest frequency of abnormal karyotypes was found in this group.
P-10-011 Osteogenesis imperfecta – prenatal diagnosis: Case report
B. Milanovic1, Z. Puzigaca1, U. Radivojevic1, V. Milanovic2, R. Nikolic1, Z. Aleksov1, D. Smolovic1, S. Grkovic1
1Clinic for Human Reproduction, Mother and Child Health Care Institute, Belgrade, Serbia; 2Clinical Center “Dr Dragisa Misovic”, Belgrade, Serbia
Objective: Osteogenesis imperfecta (OI) is a genetic disorder characterized by bones that brakes easily, often from little or no apparent cause. This condition originate from a mutation in one of the two genes responsible for making Type I collagen. The incidence is 0.4:10,000 live births and affect both sexes. Most cases of osteogenesis imperfecta are caused by a dominant genetic defect. Some children with OI inherited the disorder from a parent, but the genetic defect can occur as a spontaneous mutation. Although symptoms may vary, generally they are used to classify the four forms of OI each of witch represents the severity of condition. Here we present the case of prenatally diagnosed osteogenesis imperfecta by ultrasonography in 29 week of pregnancy.
Methods: A 16-year-old primigravida, in 29 weeks of pregnancy was refered to our Clinic for Human Reproduction, for ultrasonographic examination. Previous examination raised the suspicion of structural anomalies of the fetus.
Results: The BPD measurements were consistent with the 28 week gestational age. The skull was remarkable for its decreased echogenicity, a sign associated with decreased mineralization. The limb bones of lower extremities were extremely short. The long bones were very poorly echogenic and appeared bowed, but no evidence of fracture was recognized. The spine and thorax were morphologically normal.
Conclusion: The complete findings and a vital postnatal prognosis were explained to parents. Parents requested eugenic termination of pregnancy.
P-10-012 Spina bifida with arnold-chiari malformation: Case report
Z. Puzigaca, B. Milanovic, U. Radivojevic, Z. Aleksov, R. Nikolic, R. Pantovic, D. Smolovic, S. Grkovic
Clinic for Human Reproduction, Mother and Child Helath Care Institute, Belgrade, Serbia
Objective: We present the case of spina bifida with Arnold-Chiari malformation diagnosed by prenatal ultrasonography.
Methods: A 29 year old primigravida, was refered to our Clinic in the 20 week of gestation for an ultrasonografic examination.
Results: Ultrasound evaluation revealed a single fetus in the cefalic presentation with biometry measurements compatible with 19/20 weeks of gestation. Sonographic evaluation of the fetus revealed a U – shaped vertebra defect in the level of the lumbosacral spine in a transverse view and two characteristic sonographic signs of the Arnold Chiari malformation – the “lemon” and “banana” sings. After consultation with parents, the pregnancy was terminated. Autopsy results confirmed the ultrasonogpahic findings and failed to show other fetal anomalies.
Discussion: Prenataly, spina bifida is detectable on longitudinal and transversal scanning. Depending on the level of the lesion, interruption of the spinal cord at the site of the spina bifida defect causes paralysis of the legs, incontinence of urine and feces, anesthesia of the skin, and abnormalities of the hips, knees, and feet. Spina bifida is associated with the Arnold-Chiari malformation in 90–95% of instances. The cerebellar vermis, fourth ventricle and medulla are displaced caudally. The ultrasonographic findings and a vital postnatal prognosis were explained to parents, who requested eugenic termination of pregnancy.
P-10-013 Congenital diaphragmatic hernia – a case report
R. Carvalho, J. Pauleta, G. Borges, M. Castro, P. Veca, J.P. Marques, M.A. Melo, L.M. Graca
Hospital de Santa Maria, Lisbon, Portugal
Background: Congenital diaphragmatic hernia occurs in approximately 1 of 2200 births and is associated with a high degree of morbidity and mortality. Prenatal diagnosis occurs in approximately 50% of cases.
Case Report: A 30-year-old pregnant patient, G1, pregnancy after ICSI. At the 13 week ultrasound a nuchal translucency of 3.7 mm was seen. Fetal caryotype was normal (46 XX). Left CDH was diagnosed at 21 weeks. The fetal echocardiographic examination was normal except an accentuated right mediastinum deviation. A low lung/head circumference ratio (0.39) was seen at 32 weeks. Elective caesarean section took place at 38 weeks 2940 g, AI = 9/9. Twenty-four hours after birth she has submitted to paediatric surgery with correction of Bochdalek left hernia with several complications after, sepsis at day 24 and pulmonary hypertension among others. The baby was discharged 4 months later clinically well.
Conclusion: This case demonstrate the importance of antenatal diagnosis of this disease that permit programmed attendance to the neonate that needs surgery and differentiated care after birth to permit survive.
P-10-014 Predictive value of uterine arteries doppler in third trimester pregnancies complicated with low fetal weight and/or pregnancy hypertension
M.D. Gomez Roig, J. Sabria, C. Valls, N. Porta, S. Ferrero, S. Gimenez, A. Vela, J.M. Lailla
Sant Joan de Deu University Hospital, Barcelona, Spain
Objective: Evaluate the prediction of uterine arteries Doppler in perinatal results in pregnancies complicated with low fetal weight and/or hypertension, compared with umbilical artery Doppler.
Material and Methods: Longitudinal, prospective and non-interventionist study of 105 singleton pregnancies during the third trimester. 65 controls and 40 cases (2 intrauterine growth retardation (IUGR), 8 preeclampsies, 1 IUGR + preeclampsia, 5 hypertensive disease of pregnancy (HDP) without proteinuria, and 14 small fetus for gestational age (SGA). In all of them, the umbilical artery PI, the mean PI and the presence/absence of bilateral uterine arteries notches were evaluated.
Results: Significant differences (p < 0.001) in uterine and umbilical arteries PI were found between pregnancies with normal and adverse perinatal results.
These differences in the uterine arteries permit us to discriminate between IUGR and SGA and also between preeclampsies and HDP without proteinuria. The umbilical artery PI shows significant differences between IUGR and SGA, but not between preeclampsies and HDP without proteinuria. Furthermore, the uterine arteries mean PI sensibility and specificity is higher than the umbilical artery PI in the detection of IUGR or preeclampsia.
Conclusions: The uterine arteries Doppler study can provide higher predictive value of adverse perinatal results and better detection of IUGR and preeclampsia than the umbilical artery study, probably because of the earlier presence of an alteration in the uterine flow than in the umbilical one.
P-10-015 Antenatally diagnosed unilateral ureteropelvic junction obstruction: Does surgery improve renal function?
B. Orive1, J. Elorz2, J. Jimenez3, A. Villanueva3, A. Mari1, J. Cortes4
1Hospital Txagorritxu, Vitoria, Spain; 2Hospital Cruces, Bilbao, Spain; 3CH Donostia, San Sebastian, Spain; 4Hospital Santiago, Vitoria, Spain
Objective: Prenatal ultrasound allows the early detection of urinary tract abnormalities, especially patients with pelviureteric junction obstruction. The aim of the present study was to evaluate the renal function before and after Anderson-Hynes pyeloplasty in children diagnosed of congenital unilateral ureteropelvic junction obstruction.
Methods: We retrospectively reviewed 31 patients with hydronephrosis, antenatally detected and postnatally confirmed, to be due to unilateral ureteropelvic junction obstruction: 14 (54.8%) females and 17 (45.2%) males. All the patients had an obstructive pattern in the diuretic renography (MAG 3). Indications for surgery were: initially poor differential function (<40%) in 16 patients (51%), deterioration in differential function or step-up dilatation on the ultrasonographic examination during follow-up in 15 patients (49%). The median age for surgery was 0.75 years, interquartile range 0.33 and 2 years. Paired Wilcoxon and T test for non parametric and parametric data were used for statistical analysis.
Results: Surgery normalized renographic obstructive pattern in all patients. There were no statistical differences between renal function before and after pyeloplasty: median and interquartile range, 40% (33–47%) and 45% (39–49%) respectively, p 0.11. Analysis of patients with late surgery showed a significative statistical improvement: 47.07% (3.65) and 48.45% (3.25) (mean and SD pre and post surgery), Cohen's d 0.4; p < 0.01.
Conclusions: Our patients with initial split renal poor function, undergoing early pyeloplasty did not benefit significantly from it, perhaps reflecting irreversible antenatal damage. Patients with moderate affectation showed a statistical significative, although meaningful, amelioration.
P-10-016 Jejunal atresia – prenatal ultrasound diagnosis
A. Henriques, M.A. Melo, J. Marques, P. Veca, G. Borges, L.M. Graca
Santa Maria Hospital, Lisbon, Portugal
Background: Antenatal diagnosis is seldom done before 24 weeks gestation. Typical findings are: small bowel internal diameter > 7mm, several dilated loops of fluid-filled intestine with peristalsis, and third trimester polyhydramnios. Treatment is always surgical. Prognosis depends on the site and extension of the atresia, associated anomalies and complications. Jejunal atresia has a less favorable prognosis than distal obstructions. 18–36% of the fetuses with intestinal dilatation distal to duodenum have cystic fibrosis.
Clinical Case: We report a case of jejunal atresia diagnosed in a prenatal ultrasonogram. At 31 weeks gestation, fetal bowel dilatation with visible peristalsis was diagnosed, persisting throughout pregnancy. Polyhydramnios was evident only at 37 weeks. The newborn had a type III jejunal atresia in the context of cystic fibrosis. The infant is now 5 months old, and is still hospitalized in Paediatric Surgery Department. She had been submitted to 4 surgical interventions, and maintains total parenteric nutrition.
Comments: In this case, antenatal diagnosis allowed taking adequate measures to treat the neonate, improving its outcome.
P-10-017 A maternal death related to misoprostol overdose
A. Henriques1, A.V. Lourenco1, A. Ribeirinho1, H. Ferreira1, C. Palos2, L.M. Graca1
1Dept. of Obstetrics, Gynecology and Reproductive Medicine, Santa Maria Hospital, Lisbon, Portugal; 2Dept. of Intensive Care Medicine, Santa Maria Hospital, Lisbon, Portugal
Background: Misoprostol is an important drug in obstetrical and gynaecologic practice because of its uterotonic and cervical-ripening actions. The side effects are dose-related, normally transitory and well tolerated. However, the toxic dosage in humans has not been determined and there is no specific antidote.
Clinical Case: A 16-year-old girl developed a severe upper gastrointestinal bleeding after self-medication (12 mg misoprostol orally) with abortive intention. The patient had multi-organ-failure with severe hemodynamic instability and reveled acute abdomen signs. Emergency laparotomy showed gastric and esophageal necrosis with purulent peritoneal liquid. After several episodes of cardiac arrest, and despite reanimation efforts, the patient died.
Comment: Temporal relationship strongly suggests misoprostol was responsible for this fatal case. As far as we know this is the first fatal case that relates gastrointestinal bleeding with misoprostol overdose.
P-10-018 A prenatally diagnosed case of sirenomelia with polydactly and vestigial tail
M.A. Guven1, M. Uzel2, S. Ceylaner3, H. Karabiber4, A. Coskun1, A.H. Bayazit5
1Department of Obstetrics and Gynecology, Kahramanmaras Sutcu Imam University, Kahramanmaras, Turkey; 2Department of Orthopedic Surgery, Kahramanmaras Sutcu Imam University, Kahramanmaras, Turkey; 3Department of Genetics, Zekai Tahir Burak Women's Health Education and Research Hospital, Ankara, Turkey; 4Department of Pediatrics, Kahramanmaras Sutcu Imam University, Kahramanmaras, Turkey; 5Department of Obstetrics and Gynecology, Kahramanmaras Goverment Maternity Hospital, Kahramanmaras, Turkey
Objective: To present a prenatally diagnosed case with sirenomelia, vestigial tail and polydactyly.
Methods: Prenatal ultrasound and postnatal findings in a 30 year-old woman at 16 weeks of gestation with dichorionic twins.
Results: Prenatal ultrasound demonstrated fusion of the lower limbs with normal femurs, tibias and fibulas, and normal vertebras in one of the twins, suggesting the diagnosis of sirenomelia. After extensive counseling, the parents opted to continue the pregnancy. The twins were delivered vaginally at 35 weeks after spontaneous onset of labour. The abnormal twin weighed 1800 g. Postnatal examination revealed unseparated lower limbs with extreme retroversion, bilateral pes equinus, unilateral postaxial polydactyly, a vestigial tail on sacral region and large, wide-big penis, anal atresia. Further, radiologic survey showed united lower extremities without bony fusion and small, united, horizontal iliac wings and abnormally inverted V shape of pubic arms and symphysis pubis. The newborn died after 24 hours due to the complications related with anogenital atresia.
Conclusion: There is only one previous report of sirenomelia with vestigial tail in the literature. However, large, wide-big penis and polydactyly have not been reported before in association with this anomaly.
P-10-019 Trisomy 22: A case report
B. Dane, M. Yayla, C. Dane
Haseki Education & Research Hospital, Department of Obstetrics & Gynecology, Division of Perinatology, Istanbul, Turkey
Introduction: Trisomy 22 is a rare chromosomal defect, occurring with an estimated incidence of 1 per 30,000 to 50,000 live-born neonates. However, it represents one of the most common chromosomal abnormalities found in early spontaneous abortion. Prenatal diagnosis of trisomy 22 in the second and third trimesters is unusual.
Case Report: A 37-year-old woman, gravida 2, para 1, was refereed for a sonographic examination at a gestational age of 14. Nuchal thickening of 4 mm, talipes, and an atrioventricular septal defect were noted. Amniocentesis was performed uneventfully after two weeks. Chromosome analysis showed a 47, XX, + 22 karyotype. The pregnancy was terminated at 19 weeks' gestation. The following abnormalities were evident by postmortem examination: A short neck, mild skin edema, conical face shape, hypertelorism, micrognathia, and bilateral talipes.
Discussion: Second-trimester sonography provides valuable clues for the prenatal diagnosis of several chromosomal disorders, including trisomy 22. Well-known features associated with this condition include fetal growth restriction in association with structural anomalies involving mainly the heart, face, kidneys, and gastrointestinal tract. Most of these anomalies can be readily detected prenatally. Anomalies of the neck and skin were commonly reported, and because nuchal translucency was one of the predominant traits, it appears to be a reliable sonographic marker for this aneuploidy.
P-10-020 Prenatal diagnosis of methylmalonic and glutaric aciduria type II from amniotic fluid
S. Grkovic1, R. Nikolic2, Z. Puzigaca2, U. Radivojevic2, B. Milanovic2, Z. Aleksov2, M. Djordjevic1, D. Smolovic2
1Mother and Child Health Care Institute “Dr Vukan Cupic”, Department of Paediatric, Belgrade, Serbia; 2Clinic for Human Reproduction, Mother and Child Helath Care Institute “Dr Vukan Cupic”, Belgrade, Serbia
Objective: Prenatal diagnosis for some organic acidemias is well established and known to be reliable but for some disorders there is less experience and the prenatal diagnosis may be experimental. Amniocentesis is safer procedure than CVS and gives both amniotic fluid for analysis of diagnostic metabolites and amniocytes that can be cultured for an enzyme diagnosis assay and molecular investigations. This fluid contains small amounts of organic acids produced by the fetal kidneys so careful analysis of the amniotic fluid can be used for prenatal diagnosis of organic acidemias.
Methods: In our laboratory we have done two prenatal diagnosis in pregnancy at risk for methylmalonic acidemia (MMA) and for glutaric aciduria II (GA II) based on quantitation of specific organic acids in amniotic fluid. Method for organic acids in amniotic fluid was capillary gas chromatography (GC) with internal standard for accurate quantitation.
Results: In case of pregnancy at risk for MMA analysis of organic acids were normal which means that we do not detect a methylmalonic acid in amniotic fluid, the pregnancy was allowed to continue and the mother was delivered of a normal healthy male baby. In case of pregnancy at risk for GA II profile of specific organic acids were also normal, the pregnancy was allowed to continue and the mother was delivered of a normal healthy female baby.
Conclusion: In general use of direct biochemical analysis for prenatal diagnosis of organic acidemias, particularly methylmalonic and glutaric aciduria type II, appears reliable and may be used as the primary diagnostic method.
P-10-021 Delivery and neonatal outcomes of pregnancies beyond 40 weeks of gestation
Y. Engin-Ustun, Y. Ustun, A. Kafkaslı, H. Aladag
Inonu University School of Medicine, Department of Gynecology and Obstetrics, Malatya, Turkey
Objective: The purpose of the study was to determine whether delivery and neonatal outcomes change beyond 40 weeks of gestation.
Methods: From January 1, 2005, through December, 2005, 242 consecutive women presenting at 40 weeks' gestation or more who were candidates for labor were reviewed. Patient age, parity, gestational ages was recorded. Delivery outcomes and perinatal complications were main outcomes. Cesarean delivery rates were calculated for patients at 40 (n = 139), 41 (n = 83) and 42 (n = 20) weeks and were compared with rates for patients who had spontaneous labor.
Results: Mode of delivery was similar in three groups (p = 0.86). Umbilical cord pH (p = 0.39) and neonatal intensive care unit admission (p = 0.27) were similar in all groups.
Conclusion: In our study group, mode of delivery and neonatal outcome did not differ with increasing gestational age.
— Cancelled
P-11-002 Actual management of pregnancies at risk for fetal anemia
M. Lubusky1, M. Prochazka1, J. Santavy2, I. Mickova2, L. Kantor3
1Department of Obstetrics and Gynecology, University Hospital, Olomouc, Czech Republic; 2Department of Medical Genetics and Fetal Medicine, University Hospital, Olomouc, Czech Republic; 3Neonatology Department, University Hospital, Olomouc, Czech Republic
Objective: To evaluate the utilisation measurements of peak systolic velocities in the middle cerebral artery (MCA-PSV) to predict the degree of fetal anemia.
Methods: In 81 pregnancies at risk for fetal anemia MCA-PSV had been assessed and fetal blood sampling for measurement of hemoglobin concentration was obtained subsequently, either by cordocentesis or at delivery. The values of MCA-PSV and hemoglobin concentration were expressed as multiples of median (MoM). Anemia was defined as mild (hemoglobin < 0.84 MoM for a given gestational age, moderate (hemoglobin < 0.65 MoM), and severe (hemoglobin < 0.55 MoM).
Results: 313 examinations were performed at 17–38 weeks' gestation. An MCA-PSV >1.5 MoM detected 100% of severly anemic fetuses with a hemoglobin concentration <0.65 MoM that required invasive intervention. In 27 cases a cordocentesis was performed and intrauterine blood transfusion was given alternatively. Remaining fetuses did not require invasive intrauterine intervention and no or mild haemolytic anemia and hyperbilirubinemia were diagnosed after delivery. Overall sensitivity to detect moderate to severe anemia (hemoglobin < 0.65 MoM for a given gestational age) was 100%. Specificity was 92%, positive predictive value was 60% and negative predictive value was 100%. One false positive case was identified after 35 weeks.
At least one cordocentesis with intrauterine blood transfusion was required by only 24% of all fetuses at risk for fetal anemia. The other fetuses 76% (34/45) didn't require intrauterine transfusion.
Conclusion: Middle cerebral artery peak systolic velocity is a highly sensitive non-invasive means for determining the degree of fetal anemia and implementation of MCA-PSV into management of pregnancies at risk for fetal anemia enable to reduce the number of invasive procedures.
Supported by the study of Medical Faculty of Palacký University Olomouc “Safety of Ultrasound in Medicine”.
P-11-003 Fetal enterolithiasis: Prenatal sonographic and MRI diagnosis in two cases of urorectal septum malformation (URSM) sequence
M. Lubusky1, M. Prochazka1, I. Dhaifallah2, D. Horak3, M. Geierova4, J. Santavy2
1Department of Obstetrics and Gynecology, University Hospital, Olomouc, Czech Republic; 2Department of Medical Genetics and Fetal Medicine, University Hospital, Olomouc, Czech Republic; 3Department of Radiology, University Hospital, Olomouc, Czech Republic; 4Department of Pathology, University Hospital, Olomouc, Czech Republic
Objectives: Enterolithiasis (multiple calcifications of intraluminal meconium) is a rare, prenatal ultrasonographic finding. In this study, our aim was to evaluate the prenatal diagnostic features and discuss the management of the patients.
Methods: The data of two cases of prenatally diagnosed fetal enterolithiasis were collected from ultrasound, magnetic resonance imaging and neonatal or postnatal autopsy records.
Results: Malformations in two cases (both males) with partial and complete urorectal septum malformation (URSM) sequence were described. The absence of anal opening and presence of a fistula between the urinary and gastrointestinal tract were common findings. These features were considered as primary malformations contributing to the formation of enterolithiasis. Secondary anomalies (urinary and gastrointestinal system malformations, pulmonary hypoplasia, genital and other coexisting anomalies) were evalutated.
Conclusion: The prenatal detection of enterolithiasis carries a poor prognosis. Most of the previously reported cases were invariably associated with major fetal malformations of the urinary and gastrointestinal tract. It is a warning sign for large bowel obstruction with or without enterourinary fistula. Threrefore, adequate gastrointestinal and urologic studies must be undertaken after birth for final diagnosis. There is a high mortality rate in the reported cases, mostly attributed to associated anomalies, and all survivors required neonatal surgery. It is important to differentiate the partial from the full URSM sequence because the prognosis in the partial URSM sequence is generally good, with long-term survival common.
Supported by the study of Medical Faculty of Palacký University Olomouc “Safety of Ultrasound in Medicine”.
P-11-004 Cervical incarceration and radial nerve entrapment neuropathy
P. Vanhaesebrouck, A. Zecic, T. Bovyn, C. Vander Linden, K. Smets, C. De Praeter, H. Verhelst, P. Defoort
Ghent University Hospital, Ghent, Belgium
Background: Isolated radial nerve palsy is a rare condition in neonates. Since an association with prolonged labour was described, it has been hypothesized that intrauterine nerve compression should play a causal role. Prolonged intra-cervical incarceration with compressive impediment of the radial nerve is proposed here as the cause of this congenital neuropathy.
Case Report: A G1P0-mother was transferred to our obstetric unit because of PROM and oligo-hydramnios at 32 weeks' gestation. The male infant was born 2 weeks later by spontaneous vaginal delivery. There was no cord entanglement, neither amniotic bands. Apgar scores were 3 and 8. Birthweight was 2120 g. A huge localized edema was seen involving the infants' head, as well as his right shoulder up to the mid-humerus. He was intubated because of obstructive pharyngeal edema. Right wrist drop was detected at birth. There was normal ipsilateral elbow extension, as well as wrist and finger flexion. However, wrist and finger extension was absent. Triceps reflex was preserved. Sensory loss over the dorsum of the hand was also present. Thumb abduction could not be elicited by Moro reflex. Any fracture or diaphragm paralysis was excluded by X-ray. Electromyography (EMG) demonstrated absent sensory and motor responses of the right radial nerve and absence of voluntary motor units on needle examination of the right radial forearm muscles. These findings were consistent with acute denervation due to a peripheral axonal injury distal to the triceps muscle branch of the radial nerve.
Discussion: Preservation of triceps strength and sensory loss isolated to the dorsum of the hand were indicative of selective radial neuropathy at the spiral groove, as confirmed by EMG. Radial nerve compression by encircling pressure is strongly suggested by the circular ridge at mid-humerus. To the exclusion of cord entanglement, we assume that only intracervical incarceration of the infant's head and right upper arm could explain the ring-shaped constriction around the infant's upper part of the body with retrograde soft tissue swelling and ensuing radial nerve entrapment.
Conclusion: Peripheral nerve palsies in the newborn are not always traumatic in origin and can be acquired prenatally by uterocervical incarceration. Differential diagnosis with lower brachial plexus injury is important, the latter resulting in weakness of wrist and finger flexors, whereas radial nerve injury results in absence of their extension. At variance with a poor outcome in many cases of Klumpke's palsy a good prognosis is anticipated in the propositus.
P-11-005 Induction of ovulation with two different gonadotropin preparations
M. Petronijevic1, D. Petronijevic2, M. Pokrajac3, G. Ivanovic4, D. Ivanovic4, S. Vrzic-Petronijevic1, B. Miljkovic3, V. Boskovic4
1Institute for Gynaecology and Obstetrics, Clinical Center Serbia, Belgrade, Serbia; 2Pharmaceutical Institution Belgrade, Belgrade, Serbia; 3Institute for Pharmacokinetics, Faculty of Pharmacy, Belgrade, Serbia; 4Specialist Gynaecology and Obstetrics Clinic “Ivanovic”, Belgrade, Serbia
Objective: Pharmacokinetic evaluation of two different gonadotropin preparations.
Method: Patients, divided in group A and B received menotropin and FSH high purity from 2nd–3rd day of cycle, once daily. Serum levels of FSH, LH and E2 were measured and monitored.
Result: Mean Steady State concentration (CSS) – CSSFSH in group A and B were 18mIJ/ml and 15 mIJ/ml, respectively. CSSLH in group A and B were 1.6 mIJ/ml and 1.5mIJ/ml, respectively. CSSE2 in group A and B were 1100 pg/ml and 1300 pg/ml, respectively. Average oocyte number was: group A-8.92, group B-10.88, respectively.
Conclusion: Measuring FSH, LH and E2 serum levels showed no significant differences in efficasy of the used preparations. Pharmacokinetic parameters obtained from the monitoring FSH, LH and E2 serum levels show that the steady state was reached after 4th–5th day of therapy. Small differences in hormonal levels, although of no significance, indicated that the steady state was reached with certainty and maintained from 8th–9th day of therapy.
P-11-006 First trimester nuchal translucency screening for fetal down's syndrome in clinic for human reproduction: Preliminary findings
B. Milanovic, U. Radivojevic, Z. Puzigaca, Z. Aleksov, R. Nikolic, S. Grkovic
Clinic for Human Reproduction, Mother and Child Health Care Institute “Dr Vukan Cupic”, Belgrade, Serbia
Objectives: We are presenting preliminary results of the nuchal translucency (NT)-screening program performed in Clinic for Human Reproduction.
Methods: This study included 195 pregnant women attending our Clinic between April 2005 and July 2005. The mean maternal age was 33.8 years (range 19–45 years), 101 (51, 79%) women were 35 years old or more. Ultrasound scan was performed at 11 to 13 + 6 weeks. Crown rump length of fetuses was 45–84 mm. NT measurement was performed by five ultrasonographers according to Fetal Medicine Foundation (FMF) guideline, following strict methodological criteria. Scans were performed using transabdominal ultrasound in mid-sagital plane, with the fetus occupying at least 75% of the image. Calliper measurements were corrected to 0.1 mm. Care was taken to visualize clearly the fetal skin and amniotic membrane. The maximum thickness of subcutaneous translucency between the skin and soft tissue overlying the cervical spine was measured several times, and the largest measurement was taken into account. Fetal karyotyping was performed in cases of advanced maternal age (woman 35 years old or more), positive family history of aneuploidy, and when the measured NT was over 3 mm.
Results: NT was over 3 mm in four fetuses (2.5%). The consecutive values of NT measurements in four cases were 5 mm; 3 mm; 3 mm and 6 mm. At the present, two Down's syndrome were confirmed genetically.
Conclusion: Most of the fetuses were found to be anatomically normal on first trimester ultrasound scan. NT is an important sonographic marker to detect chromosomal defects. In fetuses with normal kariotype, the finding of increased NT demands a continuous sonographic follow up.
P-11-007 Elevated maternal serum alpha-fetoprotein and human chorionic gonadotropin levels in prediction of pregnancy outcome
M. Marinkovic, Z. Mikovic, N. Karadzov, B. Damnjanovic
Obstetrics and Gynecology Clinic “Narodni front”, Belgrade, Serbia
Objective: The study was undertaken to determine wether the elevated maternal serum alpha-fetoprotein (MSAFP) and/or human chorionic gonadotropin (hCG) levels in early second trimester of pregnancy in women with no previous medical complications can predict adverse pregnancy outcome.
Methods: The study group consisted of 72 patients with elevated MSAFP and/or hCG levels >2.0 MoM. Using ultrasound examinations and invasive prenatal diagnostics procedures the accurate date was established, the presence of multiple gestations and structurale or chromosomal abnormalities was excluded. All patients were without previous medical complications. Control group was formed of 119 patients with normal levels of those specific serum markers. The incidences of various pregnancy outcomes were evaluated according to the serum marker levels devided in 3 groups (elevated MSAFP, elevated hCG and elevated both MSAFP and hCG) in comparing with control group.
Results: In group with increased hCG levels significantly more often occured pregnancy-induced hypertension with or without preeclampsia, intrauterine growth restriction (IUGR) and gestational diabetes. Perinatal outcome is associated with lower birth weight and higher rate of fetal distress. Incresed MSAFP levels were found to be significantly associated with IUGR and preterm delivery and in perinatal outcome lower is gestational age, birth weight and 5′ Apgar score and higher incidence of fetal distress. In group with elevated both MSAFP and hCG (>4.0 MoM) there were high significant association with preeclampsia with severe IUGR and preterm termination of pregnancy by caesarian section and thus highly significans of all parameters of perinatal outcome. Inspite of low a prior risk 74.6% patients developed different obstetrics outcome.
Conclusion: Unexplained elevated MSAFP and/or hCG are significant in prediction of most pregnancy complications. In these pregnancies increased prenatal surveillance is important for early detection of complications and prevention of adverse perinatal outcome.
P-11-008 Nucleotides in fibroblasts for prenatal diagnosis of inherited deficiencies of purine de novo biosynthesis
M. Prochazka1, L. Zidkova2, J. Tomkova2, A. Janostakova2, D. Friedecky2, T. Adam2
1Department of Obstetrics and Gynecology University Hospital and Palacky University, Olomouc, Czech Republic; 2Laboratory for Inherited Metabolic Disorders, Dept. Clinniversity Hospital and Palacky University, Olomouc, Czech Republic
Objective: They are two enzyme deficiencies in purine de novo synthesis (PDNS) identified in human so far – adenylosuccinate lyase and AICA ribosiduria (Marie S, et al. 2004). The aim of this work was to determine whether nucleotide analysis in cultured skin fibroblasts (CSF) can be used for prenatal detection of inherited defects of PDNS.
Methods: Analysis of intracellular nucleotides in CSF was accomplished by capillary electrophoresis. Separations were performed in fused silica capillary using running buffer 40 mmol/l citrate – gama-aminobutyric acid (pH 4.4) with 0.8 mmol/l cetyltrimethylammonium bromide.
Fibroblasts were from stillbirths in various stages of gestation and were cultured using standard protocols and in purine deficient media to stimulate PDNS. Special attention was paid on optimisation culture and cell-harvesting conditions. We analyzed 24 CSF apparently purine disease free samples individuals. We also analyzed cultured Chinese hamster ovarial (CHO) cells defective in purine de novo synthesis in order to model the disorders and CSF from patient with adenylosuccinate lyase deficiency.
Results: We estimated reference values for nucleotides in CSF. In enzyme deficient CSF and CHO cells accumulation of specific nucleotides – substrates of defective enzymatic reaction was observed allowing distinguishing it from normal cell lines.
Conclusions: Analysis of intracellular nucleotides in CSF can be potentially used for prenatal diagnosing of PDNS defects.
This work was supported by grant IGA NR/7796-3 and NR/8578-3.
P-11-009 Prenatal diagnosis in multiple gestations following selective reduction
M. Theodora, I. Tsiaousi, N. Papantonioy, G. Daskalakis, S. Mesogitis, A. Antsaklis
Fetal Medicine Unit, 1st Department of Obstetrics and Gynecology, University of Athens, ‘Alexandra’, Athens, Gre
Objective: To determine whether the type and the timing of prenatal diagnosis procedures have any effect on the outcome of multiple pregnancies subjected to embryo reduction.
Material and Methods: We studied 428 multiple gestations in total. Fifty-six were subjected to amniocentesis 5–6 weeks after selective fetocide (group A). In 46, selective fetocide due to anomaly was preformed after prenatal diagnosis [amniocentesis-group B or chorionic villi sampling-group C]. We studied the maternal age, number of fetuses prior to and after reduction, the chorionicity, the gestational age at delivery and the perinatal mortality.
Results: In cases where amniocentesis was preformed after reduction the miscarriage rate was 8.9%, which is not different from the miscarriage rate in multiple pregnancies subjected to fetal reduction. The mean gestational age in delivery was 34 weeks in group A and 35 + 3 days in total.
In cases in which selective fetocide due to anomaly was preformed after prenatal diagnosis procedure the miscarriage rate was 8.5% in group C and 10% in group B. The mean gestational age at delivery was 33 weeks in both group B and C.
Conclusions: There is no deference in pregnancy outcomes regarding if selective reduction was done in the first or second trimester. There is no difference if selective reduction was preformed prior to the prenatal diagnosis. We suggest that CVS should be preformed in pregnancies with genetic burden. Nevertheless the decision on the time of the selective reduction and the type of prenatal diagnosis procedure should be individualized.
P-11-010 Reference range for fetal nasal bone length at 11–13 + 6 weeks gestation in a greek population
P. Benardis, M. Theodora, A. Pilalis, R. Antsaklis, K. Bassagianis, A. Souka, A. Antsaklis
Fetal Medicine Unit, 1st Department of Obstetrics and Gynecology, University of Athens, ‘Alexandra’, Athens, Gre
Introduction: The aim of this study was to provide a reference range for the length of the fetal nasal bone at 11–13+6 weeks gestation in a Greek population.
Material and Methods: A reference range of fetal nasal bone length was established from cross-sectional data on 750 consecutive singleton pregnancies scanned at 11–13+6 weeks gestation (CRL = 45–84 mm) as part of their routine nuchal translucency scan.
Results: Nasal bone length measurements increased as a function of gestational age showing a linear relationship. Using standard statistical methods a graph for fetal nasal bone length measurements as a function of gestational age was obtained and mean, 95% confidence intervals and 5th and 95th percentile were estimated.
Conclusions: These reference ranges of a Greek population may prove to be useful in prenatal screening and diagnosis of syndromes known to be associated with nasal hypoplasia (e.g. Down's syndrome).
P-11-011 Comparison of increased uterine artery pulsatility index and bilateral notches at the second trimester in screening for preeclampsia and fetal growth
A. Pilalis, A. Souka, M. Theodora, P. Antsaklis, N. Papantonioy, S. Mesogitis, G. Daskalakis, A. Antsaklis
1st Department of Obstetrics and Gynecology, Alexandra Maternity Hospital, University of Athens, Athens, Gre
Objective: To compare mean uterine artery PI ≥ 95th centile with bilateral notching in the prediction of pre-eclampsia (PET), small for gestational age fetuses (SGA) below the 5th and 10th centile and placental abruption.
Methods: 934 consecutive women underwent transvaginal scanning for uterine artery doppler examination at 22–23 weeks and the mean PI as well as the presence of a diastolic notch were recorded.
Results: Mean uterine artery PI was 1.06 and the 95th centile was 1.55. Bilateral notching was observed in 11.13% of our patients. The sensitivity of increased PI ≥ 95th centile for the prediction of PET, PET necessitating delivery ≤34 weeks, SGA ≤ 5th centile, SGA ≤ 5th centile necessitating delivery ≤34 weeks, SGA ≤ 10th centile and placental abruption was 67%, 80%, 23%, 100%, 12% and 33% respectively.
The respective sensitivities achieved by bilateral notching for the same outcomes were 67%, 80%, 38%, 100%, 30% and 50%.
Conclusions: The two screening methods had similar sensitivities for the studied outcome measures. They achieved the same sensitivity for PET, early onset severe PET and early onset severe SGA. Bilateral notches achieved higher sensitivities in the detection of SGA and placental abruption but at the cost of a double screen positive rate.
P-11-012 Screening for preeclampsia and small for gestational age fetuses at the 11–14 weeks scan using uterine artery dopplers
A. Pilalis, A. Souka, K. Bassagianis, J. Karamoyntzos, M. Theodora, N. Papantoniou, S. Mesogitis, A. Antsaklis
1st Department of Obstetrics and Gynecology, Alexandra Maternity Hospital, University of Athens, Athens, Gre
Objective: To assess the role of uterine artery Doppler at 11–14 weeks, in screening for preeclampsia (PET), small for gestational age (SGA) fetuses and placental abruption.
Methods: 1143 consecutive women presenting for routine examination at 11–14 weeks for nuchal translucency measurement, underwent transvaginal scanning for uterine artery doppler measurement. The mean PI was calculated and the presence of a diastolic notch was recorded.
Results: Six women miscarried before 24 weeks and in 14 cases the pregnancy was terminated for fetal pathology, leaving 1123 women for further analysis. Fourteen (1.25%) women developed preeclampsia, there were 45 fetuses with a birth-weight below the 5th centile (4%) and 115 below the 10th centile (10.2%). Placental abruption occurred in 9 women (0.8%). The mean, median and 95th centile of uterine artery PI were 1.71, 1.65 and 2.55 respectively. Bilateral notches were observed in 63.5% and a unilateral notch in 18.3% of cases. The sensitivity of uterine artery mean PI ≥ 95th centile was 21.4%, 33.3%, 17.8%, 100%, 9.6% and 44.4% for PET, early onset severe PET necessitating delivery before 34 weeks, SGA ≤ 5th centile, SGA ≤ 5th centile necessitating delivery before 34 weeks, SGA ≤ 10th centile and placental abruption respectively.
Conclusions: Abnormal dopplers at 11–14 weeks scan identified one third of women with severe early onset pre-eclampsia, all SGA ≤ 5th centile fetuses that were delivered at ≤34 weeks and 40% of cases with placental abruption. Notches were not found to be helpful as a screening tool in the first trimester due to the very high screen positive rate. Uterine artery doppler examination at the 11–14 weeks scan can identify a high risk population in which preventive or therapeutic interventions might be effective.
P-11-013 Screening for preeclampsia and fetal growth restriction bu uterine artery dopplers and PAPP-A and the 11–14 weeks scan
A. Pilalis, A. Souka, P. Benardis, P. Antsaklis, E. Anastasakis, N. Papantoniou, S. Mesogitis, G. Daskalakis, A. Antsaklis
1st Department of Obstetrics and Gynecology, Alexandra Maternity Hospital, University of Athens, Athens, Gre
Objective: To assess the role of uterine artery Doppler, maternal serum PAPP-A and their combination at 11–14 weeks, in screening for preeclampsia (PET) and small for gestational age (SGA) fetuses.
Methods: Prospective study of 873 consecutive women presenting for the routine 11–14 weeks ultrasound examination who underwent transvaginal scanning for uterine artery doppler measurement.
Results: The sensitivities of mean uterine artery PI ≥ 95th centile for the prediction of PET, early onset severe PET, SGA ≤ 5th centile and placental abruption were 23%, 33%%, 23% and 43%, respectively. The respective sensitivities for PAPP-A ≤ 10th centile were the same for PET (23%) and placental abruption (43%), decreased for early onset severe PET (17%), and increased for SGA ≤ 5th centile (34%), but for a double false positive rate of 10%. The combination of abnormal Dopplers and PAPP-A ≤ 10th centile increased marginally the detection rate for PET (31%) but improved substantially the sensitivity for SGA ≤ 5th centile (48%) and placental abruption (57%), at the expense of a false positive rate of about 13%. For a fixed screen positive rate of 5% the combination of abnormal Dopplers and low PAPP-A identifies almost one third of the cases with pre-eclampsia (31%) early onset severe pre-eclampsia (33%), fetuses with birthweight ≤ 5th (31%) centile and placental abruption cases (29%). Moreover, almost one in three of the screen positive women will develop one or more of these complications.
Conclusions: The combination of abnormal dopplers and PAPP-A ≤ 10th centile at the 11–14 weeks scan can detect approximately one third of women with preeclampsia and half of the fetuses with SGA ≤ 5th centile. For a fixed screen positive rate of 5% the combination achieves better results than either test alone.
P-11-014 Indications for fetal karyotyping – analysis of 3916 cases
A. Athanasiadis1, T. Mikos1, A. Karavida1, L. Florentin2, F. Tzevelekis1, E. Assimakopoulos1, A. Tantisis1, J. Bontis1
11st Department of Obstetrics & Gynecology, Aristotle University of Thessaloniki, Papageorghiou Gener, Thessaloniki, Greece; 2Centre of Molecular Biology and Cytogenetics AlphaLab, Athens, Attiki, Greece; 3Centre of Prenatal Diagnosis, Thessaloniki, Gre
Objective: To describe the use of the sonographic markers in the detection of karyotype abnormalities in the 2nd trimester.
Methods: Retrospective analysis of the indications and karyotype results from 132 chorionic villus sampling and 3784 2nd trimester amniocenteses that were performed from 2000 to 2005. The mean maternal age was 35.4 years (St. Dev. 4.35 years).
Results: The most frequent karyotyping indications were maternal age >35 years (2832/3916, 72.32%), positive 2nd trimester biochemical serum screening (312/3916, 7.97%), maternal request (205/3916, 5.23%), intracardiac echogenic focus (101/3916, 2.58%), and fetal abnormalities detected during the anomaly scan (81/3916, 2.07%). Other karyotyping indications were history of trisomy 21 fetus in previous pregnancy (2.08%), increased 1st trimester nuchal transulecency >2.5 mm (1.74%), increased 2nd trimester nuchal fold >6 mm (1.43%), renal pelvis dilatation (1.33%), echogenic bowel (0.74%), ventricular dilatation (0.49%). There were 87 (2.22%) fetuses with abnormal karyotype. There were found 59/87 (67.81%), 12/87 (13.79%) and 3/87 (3.44%) fetuses with trisomy 21, 18 and 13 respectively. Eleven of the trisomy 21 fetuses were diagnosed with chorionic villus sampling due to increased nuchal translucency. Amniocentesis indications in 48/59 trisomy 21 fetuses were increased maternal age (45.83%), increased nuchal fold in 2nd trimester scan (22.91), positive 2nd trimester biochemical screening (14.58%) and intracardiac echogenic focus (16.66%).
Conclusion: Increased maternal age and ultrasound markers offer good detection rates of trisomy 21 fetuses optimizing the use of 2nd trimester amniocentesis. Further studies are necessary in order to define the significance of the soft ultrasound markers in the detection of fetal karyotype abnormalities.
P-11-015 Sonographic and biochemical markers in 59 fetuses with trisomy 21
A. Athanasiadis1, A. Karavida1, T. Mikos1, L. Florentin2, E. Assimakopoulos1, F. Tzevelekis1, P. Polychronou1, P. Monastiriotis1, J. Bontis1
1Department of Obstetrics & Gynecology, Aristotle University of Thessaloniki, Thessaloniki, Greece; 2Centre of Molecular Biology and Cytogenetics AlphaLab, Athens, Attiki, Greece; 3Centre of Prenatal Diagnosis, Thessaloniki, Thessaloniki, Greece
Objective: To describe the most frequent sonographic findings in fetuses with trisomy 21.
Methods: 3916 genetic amniocentesis were performed in a single unit from 2000 to 2005. A total of 87/3916 (2.22%) fetuses with abnormal karyotypes were diagnosed. Retrospective analysis of the indications and the sonographic findings from 59/87 (67.81%) fetuses with trisomy 21. The mean maternal age was 35.71 years (St. Dev. 5.56 years).
Results: Eleven cases (11/59) of trisomy 21 were diagnosed after chorionic villus sampling in the 1st trimester. Increased nuchal translucency was found in each one of these cases (11/11, 100%), whereas there was a fetus with absent nasal bone (1/11, 9.09%). The rest 48/59 cases were diagnosed with amniocentesis after the 16th gestational week. Amniocentesis indications for this group were (a) maternal age >35 years (22/48, 45.83%), (b) increased nuchal fold (11/48, 22.91%), (c) intracardiac echogenic focus (8/48, 16.66%), (d) positive 2nd trimester biochemical serum screening (7/48, 14.58%), (e) major cardiac anomaly (2/48, 4.16%), (f) duodenal atresia (2/48, 4.16%), (g) renal pelvic dilatation (2/48, 4.16%), (h) ventricular septum defect (1/48, 2.08%), (i) atrial septum defect (1/48, 2.08%), (k) short femur (1/48, 2.08%). In 20.83% of the fetuses a single trisomy 21 sonographic marker was found (nuchal fold: 5 cases, echogenic focus: 3 cases, short femur: 1 case). Second trimester ultrasound scan did not reveal any abnormal finding in 25/48 (52.08%). In 22/25 cases amniocentesis was performed due to increased maternal age.
Conclusion: Although ultrasound holds a major role in the prenatal diagnosis of trisomy 21, there was no abnormal sonographic finding in approximately half of trisomy 21 fetuses, the amniocentesis being performed due to increased maternal age only. A single sonographic marker served as an amniocentesis indication in 1/5 of the abnormal karyotypes.
P-11-016 Intrapartum exposure to tobacco smoke: Is there a relevance to neonatal fibrinolysis and coagulation disturbances?
G. Mitsiakos1, G. Papaioannou2, E. Giougi1, P. Karagianni1, H. Chatziioannidis1, A. Karapiperidou2, N. Nikolaidis1
12nd NICU and Neonatology Department of Aristotle University of Thessaloniki, G.P.N. Papageorgiou, Thessaloniki, Greece; 2Hematology Department, G.P.N. Papageorgiou, Thessaloniki, Gre
Introduction: Maternal smoking during pregnancy is associated with a well-documented increase in perinatal morbidity and mortality rates in the newborns. The whole haemostatic system can be affected.
Objective: Investigation of possible alterations in coagulation profile and fibrinolysis of the newborn due to in utero exposure to tobacco smoke.
Subjects and Methods: The study included 36 neonates born between April 2005 and December 2005, who were declared healthy after physical examination. Infants with congenital coagulation disorders or maternal use of anticoagulants were excluded. Blood samples of 18 newborns of smoking (>10 cigarettes per day) and 18 newborns of nonsmoking mothers were obtained immediately after birth, before the administration of vitamin K. Values of prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastin time (aPTT) and fibrinogen were determined by synthetic substrate while tissue plasminogen activator (t-PA) and plasminogen activator inhibitor-1 (PAI-1) were determined by Elisa. The Mann-Whitney U test was used to compare the results of the 2 groups at the p < 0.05 level.
Results: Smoking mothers' group: The mean gestational age (G.A.) of the group was 36.73 ± 3.25 weeks and the mean birth weight (B.W.) 2534 ± 800 g. Seven infants were males. Mean coagulation values: PT: 16.5 ± 1.8 sec, aPTT: 50.1 ± 15.5 sec, INR: 1.35 ± 0.19, fibrinogen: 161.5 ±43.2 mg/dl, t-PA: 11.4 ± 3.6 ng/ml and PAI-1: 51.8 ±25.3 Av/ml.
Non smoking mothers' group: The mean was G.A. 36.27 ± 3.12 weeks and mean B.W. 2632 ± 689 g. Eight infants were males. Coagulation screen indicated: PT: 16.1 ± 1.9 sec, aPTT: 45.5 ± 8.7 sec, INR: 1.29 ± 0.20, fibrinogen: 165.1 ± 67.2 mg/dl, t-PA: 8.5 ± 3.8 ng/ml and PAI-1: 61 ± 32 Av/ml.
Between the 2 groups, there were no significant differences, neither in infants' characteristics nor in the values of the coagulation parameters (pN/S).
Conclusions: In pregnant women who smoke the activated coagulation process is not counterbalanced by an increase in fibrinolysis, as is the case in the nonsmoking ones. Nevertheless, the balance between coagulation and fibrinolysis in neonates is not influenced by maternal smoking. The study is ongoing using larger populations in order to obtain more accurate reference values.
P-11-017 Stan in clinical practice – the outcome of 2 years of regular use in the city of Varberg, Sweden
A.K. Welin1,2, H. Noren2, K.G. Rosen2
1Dept. of Obst. Gynec., Varberg Hospital and 2Perinatal Centre, Univ. of Gothenburg, Sweden
Objective: To monitor the introduction of the STAN-methodology in a district hospital.
Design: Retrospective study covering the total population of deliveries at term during 2004 and 2005.
Material and Methods: 1875 out of 3193 term pregnancies were monitored using the STAN® fetal heart monitor (Neoventa Medical, Moelndal, Sweden) and the associated clinical guidelines. Cord metabolic acidosis, neonatal outcome and rates of operative deliveries for fetal distress were assessed.
Results: provides a comparison with other STAN recent studies. Neonatal outcome showed a consistently low cord artery metabolic acidosis rate and the rate of Apgar scores <7 at 5 minutes was 0.5%, significantly lower then previously noted in Gothenburg during the 2nd year of STAN usage (OR 0.37; 0.18–0.73). ODFD and CS rates were lower as well, 6.9 vs. 10.3% (OR 0.65; 0.52–0.80) and 3.2 vs. 5.1% (OR 0.62; 0.45–0.84), respectively. The annual rate of STAN usage was also significantly higher (OR 2.35; 2.16–2.56).
Conclusion: High STAN usage provided an outcome equalling that noted in the Swedish RCT demonstrating the safe implementation of the STAN methodology in a non-academic unit.
P-11-018 Routine prenatal ultrasound screening for fetal abnormalities
C. Comas, G. Azumendi, I. Alonso, J.R. Herrero, M. Romero, J. Anderica
Gutenberg Center, Malaga, Spain
Objective: Result of routine obstetric ultrasound examination over a period of 2 years at the Prenatal Diagnosis Unit in Gutenberg Center is described.
Methods: An overall of 15703 consecutive routine prenatal scans were performed in our private Unit between January 2004 and December 2005. Scans were performed with Acuson Sequoia and Voluson 730 Expert. Maternal age ranged from 15 to 45 years (mean of 30). Gestational age ranged from 11 to 41 weeks (mean of 22). Main indications for referral were as follows: morphological scan (44%), previous suspected anomaly (37%) and sonographic marker (11%). An overall of 7% of cases were multiple pregnancies, including 9 cases of monochorionic twin pregnancies and 1 triplets. Post-natal follow-up confirming the diagnosis was obtained after delivery by phone interview.
Results: A total of 262 malformed fetuses were identified at abortion or delivery (1.67%). Fetal anomalies were diagnosed antenatally in 259 (98.9%) cases, with an overall follow-up of 40% of cases. Early prenatal diagnosis (before 22 weeks of gestation) was made in 167 cases (64%). Termination of pregnancy was decided in 13% of cases. Considering only the completed follow-up cases, fetal karyotyping diagnosed 7.8% autosomal trisomies and 3.4% sexual cromosomopathies. The most frequently diagnosed anomalies were urinary tract anomalies (17%), followed by heart anomalies (15%) and central nervous system anomalies and abdominal wall defects (8%). The final diagnosis was concordant in 97.1% of cases, with 3 overlooked cases at prenatal scan and 4 cases with a discordant diagnosis at follow-up.
Conclusions: Follow-up is needed, even in private activity, in order to have a quality control of the performance of our clinical practice.
P-11-019 The dynamics of cervical length measurements
M. Meijer-Hoogeveen, Ph. Stoutenbeek, G.H.A. Visser
Univeristy Hospital Utrecht, The Netherlands
Objective: The aim of this study was to visualize normal changes in the length of the cervix uteri during a 30 min. observation period.
Methods: Women who attented the outpatient clinic for a cervical length measurement were asked to participate in the study. A transvaginal ultrasound was performed in the supine position for 30 minutes continuously. The cervix was measured when changes were observed. The presence of contractions were recorded by tocography.
Results: Fourteen women with a gestational age between 23 and 38 weeks participated in the study. Five were nulliparous women, five of the 9 multips had a prevous preterm delivery. In the current pregnancy 10 women delivered at term and the others at 29, and 36 (n = 2) weeks, respectively. The recordings included one women who was admitted for threatened preterm labour, and had a cervical length between 11.3 and 16.7 mm with funneling.
The mean ultrasound-delivery interval was 53 days (range 10–108). The mean shortest cervical length measurement was 34.8 mm (range 11.3–51.1). Mean difference between the shortest and longest cevical length during the 30 minute recording (cervical variation) was 8.4 mm (range 1.5–15.6). During the observation period peristaltic movements of the bowel and fetal movements caused cervical changes, both shortening and lengthening of the cervical canal. No contractions were observed by tocography or reported by the women during the recording.
There was no correlation between the mean or shortest cervical length measurement and the cervical variation. Furthermore, there was no correlation between the cervical variation and gestational age at delivery.
Conclusions: The cervix uteri is a dynamic organ and its length varies with time. Contractions and bladder filling have been reported to shorten respectively lengthen the cervical canal. In this study we found dynamic changes in the cervix associated with fetal movements and peristaltic movements of the bowel. The mean cervical variation was 8.4 mm (range 1–16 mm) during the 30 minute recording period. This variation is clinically irrelevant in case of a long cervix, but may be relevant in case of a short cervix and threatened preterm labour.
P-11-020 Ultrasound diagnostics of fetal malformation in VMC podgorica
P. Rakocevic1, S. Vukcevic2
1Military Medical Center, Podgorica, Yugoslavia; 2Gynaecology Clinic – Clinical Centre, Podgorica, Yugoslavia
Introduction: Fetal malformation we can find in 2–4% of newborns. In 13% of children are the cause of death in first 15 years.
Objectives: Aim of this research is to identify pre-natal malformation will allowing the pregnancy with ultrasound diagnostics and to present our observation in connection with frequency, kind, and therapy of fetal malformations.
Methods: In prospective research of 5 years (1993–1997), carried out in the Department of Gynaecology of VMC Podgorica, we treated 829 nonselected pregnant women and 833 fetus. We performed ultrasound in the first trimester of pregnancy, 18th, 28–32nd and 36–40th week of gestation.
Results: For these period we detected prenatal 7 malformations or 0.83%. It were: two meningocoellae in 18th week of gestation, ended with miscarriage, one cyst of plecsus horioideus in 22nd week of gestation, also ended with miscarriage, one polycystic kidney in 27th week of gestation, baby born and operated in the 1st months of its life, one hidrouretheronephroses, baby born and operated in the 2nd month, two hydrocephalus, one of them in 24th week of gestation, concluded with miscarriage and one in 38th week of gestation, baby born but died after 10 days.
Out of total number of malformation 5 of them were CNS, two were malformations of urotract.
Conclusions: Ultrasound detection of fetal malformation is of great importance because it determine the way at pregnancy will be concluded.
P-11-021 Amniotic fluid adenosine deaminase and nitric oxide levels in uncomplicated pregnancies
A. Kafkasli1, A. Karabulut2, Y. Ustun1, H. Aladag1, R.T. Kıran2
1Inonu University School of Medicine Department of Obstetrics and Gynecology, Malatya, Turkey; 2Inonu University School of Medicine Department of Biochemistry, Malatya, Turkey
Objectives: The aim of this study is to evaluate the amniotic fluid adenosine deaminase (ADA) and nitric oxide (NO) levels in uncomplicated pregnancies.
Methods: ADA and NO levels were evaluated in 75 amniotic fluid samples from singleton uncomplicated pregnancies. Amniocentesis was performed for genetic analysis between 16–19 weeks of gestation. ADA and NO values were analyzed according to the gestational weeks.
Results: Distribution of the patients to the gestational weeks were as follows; 19 cases with 16 weeks, 18 cases with 17 weeks, 20 cases with 18 weeks and 18 cases with 19 weeks of gestation. Mean maternal age was 32.08 ± 6.1 (19–42) years. Mean ADA levels were 13.1 ± 7.9 IU/L, 15.0 ± 11.2 IU/L, 19.8 ± 16.3 IU/L and 19.7 IU/L in 16, 17, 18 and 19 week of gestation respectively. All the ADA values were comparable in each week of gestation. Similarly, amniotic fluid NO levels were comparable in all weeks. Mean NO levels were calculated as 52.3 ± 15.1 μmol/L, 54.1 ± 16.8 μmol/L and 51.2 ± 13.2 μmol/L, 51.8 ± 17.4 μmol/L in 16, 17, 18 and 19 weeks of gestation respectively.
Conclusion: ADA and NO levels during the placentation in normal pregnancies might be markers of inflammatory and endothelial response in normal pregnancies.
P-11-022 Evaluation of the blood pressure load in the diagnosis of hypertension in second and third trimester of pregnancy
P. Korszun, G.H. Breborowicz
Department of Perinatology and Gynecology, University School of Medical Sciences, Poznan, Poland
Objective: In this study, ambulatory blood pressure monitoring (ABPM) was estimated in 219 pregnant women in second and third trimester of pregnancy. In 123 women pregnancy hypertension were diagnosed. In 96 women normal physiological pregnancy were observed.
Methods: ABPM was carried out for one 24-h period during second half of pregnancy in the second trimester between weeks 21 and 24, and in the third trimester between weeks 29 and 33 and 37–40, in 96 normotensive pregnant women and 123 pregnant women with hypertension. On the basis of 24 hours ABPM, blood pressure load (BPL) in systolic (SBP), diastolic (DBP) and mean arterial pressure (MAP) in daytime and nighttime were evaluated.
Results: The incidence of hypertension was greater in hypertensive women than in control subjects. Hypertensive pregnant women showed higher systolic BPL, diastolic BPL and MAP in the second and third trimester compared with normotensive one. Women who developed pregnancy hypertension and preeclampsia in the second and third trimester showed significantly higher BPL profiles at night throughout gestation than those who remained in daytime and normotensive one.
Conclusions: Our study confirms the early increase of BPL in patients who will develop hypertension and suggests that nighttime systolic BPL in the second trimester is a useful predictor of PIH. 24ABPM may be useful in screening for PIH.
Keywords: Pregnancy, hypertension, blood pressure load (BPL), 24 hours ambulatory blood pressure monitory (ABPM)
P-12-001 Perinatal outcomes of pregnancies with borderline amniotic fluid index
I. Inegol Gumus1, A. Koktener2, N. Ozturk Turhan1
1Fatih University School of Medicine, Department of Obstetrics and Gynecology, Ankara, Turkey; 2Fatih University School of Medicine, Department of Radiology, Ankara, Turkey
Objective: Our aim was to determine whether a borderline amniotic fluid index observed during antepartum testing confers a significant risk of adverse perinatal outcome.
Methods: Between April 2001 and May 2005 uncomplicated gestations with a singleton non-anomalous fetus who underwent weekly monitoring of amniotic fluid index (AFI) until delivery and who gave birth at our hospital were identified for our study. Normal amniotic fluid volume and borderline amniotic fluid was defined as an amniotic fluid index of >10 and <24 cm and >5 and <10 cm retrospectively. The groups were compared on maternal datas, mode of delivery and perinatal outcomes as fetal distress, intrauterine growth restriction and meconium fluid.
Results: Total 90 cases were identified as borderline amniotic fluid and 277 cases as normal AFI. We observed significant increased incidences of admission of neonatal intensive care unit, pathologic doppler indices, intrauterine growth restriction and intrapartum fetal distress in borderline amniotic index group (p < 0.05).
Conclusions: A borderline amniotic fluid index observed in antepartum testing carries an increased risk of adverse perinatal outcomes. These patients should be followed up carefully with fetal monitoring during the antepartum and intrapartum period.
P-12-002 Influence of umbilical cord loops on fetal oxygen saturation
A. Puertas, S. Manzanares, M.E. Lopez-Moreno, T. Aguilar, M. Gonzalez-Salmeron, F. Montoya
Department of Obstetrics & Gynecology, “Virgen de las Nieves” University Hospital, Granada, Spain
Objective: To determine the influence of umbilical cord loops on fetal oxygen saturation (FSpO2), according to the association with fetal heart rate (FHR) variable decelerations.
Methods: Fetal oxygen saturation was monitored for two years (2.003 and 2.004) using Nellcor® 400 pulsioximetry system with FS-14B sensor, in two groups of pregnant women during active phase of labour. One of 263 women with a normal FHR pattern and another one with 270 women showing variable decelerations (VD). In all cases a FSpO2 monitoring of at least 70% of time was exigible. Mean value of FSpO2 was calculated for the time-lapse analyzed. After delivery, umbilical cord loops were observed, either around fetal neck, thorax or abdomen. Statistical method used analysis of variance and later subgroups comparison.
Results: 4 groups were observed.
Group 1: Normal FHR and no cord alteration (n: 214) FSpO2: 46.8 ± 7.6.
Group 2: Normal FHR and umbilical cord loop (n: 49) FSpO2: 46.2 ± 6.7.
Group 3: VD and no cord alteration (n: 188) FSpO2: 42.1 ± 6.7.
Group 4: VD and umbilical cord loop (n: 82) FSpO2: 41.2 ± 7.6.
Statistical differences were observed between groups (p < 0.001). Subgroups analysis found differences in comparisons 1 × 3, 1 × 4, 2 × 3 y 2 × 4.
Conclusions: The absence of statistical difference found in comparisons 1 × 2 y 3 × 4 allows us to affirm that factors leading to fetal heart rate variable decelerations are associated with a decrease in fetal oxygen saturation, independently of their association with a cord alteration.
P-12-003 Significance of ultrasound parameters and L/S ratio in prediction of perinatal outcome in term growth restricted neonates
I. Babovic, J. Opalic, S. Plesinac, M. Petronijevic, S. Vrzic, I. Jurisic, S. Vukajlovic, V. Ljubic, Z. Bogdanovic, D. Plecas
Institute of Gyn. and Obs., Clinical Center of Serbia, Belgrade, Serbia
Aim: To evaluate predictive value of sonographic parameters (biophysical profile or BPP and the cerebroplacetal or C/U ratio) and lecithin/sphingomyelin ratio or L/S ratio on perinatal morbidity in term growth restricted neonates (IUGR).
Materials and Methods: A retrospective study of 77 term (36–42 weeks of gestation) single-live born IUGR neonates (birth weight <10th percentile for gestational age) who were delivered by caesarean section during 2005 year in our Institute. We excluded fetuses with congenital malformations and intrauterine infections from the study.
Statistical Analysis: Sperman's, Hi-squared, Pearson's, Student's t-test, Fisher exact and Leven's tests.
Results: The most frequent early neonatal complications were perinatal asphyxia (57%), respiratory distress syndrome or RDS (19.4%) and intraventricular haemorrhagia (19.5%). The average birth weight was 2224 ± 533 g and the L/S ratio correlates with BW (r = 0.609; p < 0.05). Apgar-5 less than 7 had 11 (14.3%) neonates. There is significant positive correlation between BPP and AP-5 (r = 0.583; p < 0.05). Statistically significant negative correlation is found between asphyxia and BPP (r = −0.398; p = 0.000), C/U ratio (r = −0.379; p < 0.05) and L/S ratio (r = −0.272; p < 0.05). Increasing frequency of RDS is in statistically negative correlation with BPP (r = −0.0338; p = 0.003), C/U ratio (r = −0.269; p < 0.05) as well as with L/S ratio (r = −0.346; p < 0.05).
Conclusion: We found that the risk of perinatal asphyxia was higher in term IUGR neonates with lower BPP which was also important for prediction of RDS. The cerebroplacental ratio predicts well RDS, while L/S ratio predicts better asphyxia in term IUGR neonates.
P-12-004 Planned or urgent caesarean section and the perinatal outcome of term growth restricted neonates
I. Babovic, J. Opalic, S. Plesinac, M. Petronijevic, S. Vrzic, I. Jurisic, S. Vukajlovic, V. Ljubic, Z. Bogdanovic, D. Plecas
Institute of Gyn. and Obs., Clinical Center of Serbia, Belgrade, Serbia
Objective: The aim of the study was to evaluate early neonatal outcome of single-live born term (36–42 weeks of gestation) growth restricted neonates (birth weight at or less than 10th percentile for gestational age) according to elective or urgent caesarean section (CS).
Materials and Methods: Retrospectively, we compare the outcome of 38 single live-born term growth restricted neonates delivered by planned CS with 39 term IUGR neonates delivered by urgent CS during 2005 year in our Institute. Fetuses with congenital malformations and intrauterine infections were excluded from the study.
Statistical Analysis: Speraman's Rho-, Hi-squared tests and Student's t-test.
Results: There were 39 (50.6%) urgent and 38 (49.4%) planned caesarean sections in IUGR group. The average birth weight was statistically lower in planned CS group than in urgent CS group (2046 ± 551 g vs. 2397 ± 460 g; p = 0.003). Apgar score at 5th min. less than 7 was statistically more frequent in urgent CS group (23.7% vs. 5.1%; p = 0.024). Perinatal asphyxia was more frequent complication in planned than in urgent CS group (76.3% vs. 38.5%; p < 0.05). There is no difference in frequency of respiratory distress syndrome (RDS) between 2 groups (23.6% vs. 15.4%; p = 0.737; p > 0.05). The birth weight is in negative correlation to RDS in planned CS group (r = −0.359; p = 0.031). The cerebroplacental ratio is in statistically significant negative correlation to perinatal asphyxia in urgent CS group (r = −0.386; p = 0.015).
Conclusion: The degree of hypoxia in a term growth restricted neonates estimated by the cerebroplacental ratio (the C/U ratio) is indication for immediate preparation for urgent caesarean section. Those neonates delivered by planned caesarean section are at increase risk of low birth weight and respiratory distress syndrome.
P-12-005 Neurological development in low birth weight fetuses with pathologic doppler study in middle cerebral artery
A. Iraola, E. Eixarch, E. Meler, F. Figueras, M. Palacio, B. Puerto, E. Gratacos
Hospital Clinic, Barcelona, Spain
Objectives: To describe and compare the perinatal and 24-months psychomotor outcome in a group of fetuses with a neonatal weight below 10th percentil regarding middle cerebral artery pulsatility index (MCAPI).
Methods: Data were collected from 166 neonates born in our hospital from November 2002 to November 2003 with an estimated fetal weight below 10th percentile according to local standards, confirmed postnatally. We defined two groups: i) group A: fetuses with normal MCAPI, ii) group B: fetuses with MCAPI below 5th percentile. We prospectively performed a neurological evaluation at 24-months. We used the 24-month Age-Stage Questionary® (ASQ®) which addresses 5 dimensions: communication, gross motor, fine motor, problem solving and personal-social interaction.
The following variables were considered: neonatal weight (NNW), gestational age at birth (GA), neonatal weight percentile (NWP), caesarean delivery (CS), umbilical artery pH at delivery (UApH), significant neonatal morbidity (SNM), stay-length in the neonatal intensive care unit (LNUCI).
Results: shows our results. No mortality occurred.
Conclusion: Despite fetuses with a neonatal weight below 10th percentile and MCAPI below 5th percentile show similar perinatal outcome, psychomotor outcome at 24-months is worse in this group, albeit without reaching statistical significance. These data would make us consider IPACM as an indicator of fetuses at risk for suboptim neurological development.
P-12-006 Oxidative stress in diabetic pregnancy: Antioxidative enzymes activity and lipid peroxidation products
A. Nikolic1, A. Mikic-Novakov2, S. Stojic2, M. Bogavac2, Z. Grujic2, R. Djordjevic2
1Clinical Center Novi Sad, Institute of Laboratory Diagnostics, Novi Sad, Serbia; 2Clinical Center Novi Sad, Department of Obstetrics and Gynecology, Novi Sad, Serbia
Aim: To investigate the activity of some antioxidative enzymes and the intensity of lipid peroxidation in blood of pregnant women with Type 1 diabetes mellitus, healthy pregnant women and non-pregnant women.
Material and Methods: Ninety patients were divided into three groups: pregnant women with type 1 diabetes mellitus, healthy pregnant women and non-pregnant women. In pregnancy groups all parameters were followed in 1st, 2nd and 3rd trimester. Diabetic control was monitored by fasting blood glucose and glycosylated hemoglobin (HbA1c).The concentration of TBARS as a measure of lipid peroxidation, and activity of antioxidant enzymes: superoxide dismutase (Cu, Zn-SOD), glutathione peroxidase (GSH-Px) and catalase (CAT) were investigated in hemolysate of erythrocytes. SOD activity was assayed using the xanthine-xanthine oxidase system, CAT activity according to the method of Aebi, while GSH-Px activity was determined using the kits Randox-Ransel.
Results: Diabetic control monitored by fasting blood glucose and HBA1c was appropriate throughout the study. TBARS concentration increased significantly in pregnant women when compared with control group, as well as in pregnant diabetics compared with healthy pregnant women. The SOD activity was gradually increased in the group of normal pregnant women vs. non-pregnant group, but decreased significantly in the group of diabetic pregnant women. Catalase activity was significantly increased only in 3rd trimester diabetic pregnant women. The analysis of the ratio between prooxidant processes and antioxidant defense during normal pregnancy, pregnancy with diabetes and control, gives us an insight into the rising level of oxidant stress present in diabetic group.
Conclusion: Increased lipid peroxidation and reduced antioxidant status, despite good diabetic control, show that pregnant women are exposed to oxidative stress to a greater degree than controls.
P-12-007 Pregnancy after a previous gestation with an acute aortic dissection
C. Rodrigues, S. Santo, L. Pinto, C. Cardoso, L. Graca
Hospital Santa Maria, Lisboa, Portugal
Background: Acute aortic dissection is a rare life threatening complication of pregnancy. Cardiovascular and hormonal changes predispose to aortic dissection because of an increase of the shearing stress on the aortic wall. The most common predisposing factor during pregnancy is chronic hypertension. No further pregnancies in women who had acute aortic dissection have been reported.
Case Report: We describe a case of a 35-year-old pregnant woman with chronic hypertension, who in her previous gestation was submitted to an acute aortic dissection repair at 28 weeks of gestation, with a stent placement in the ascending aorta and a replacement of the aortic valve. Caesarean section was performed at the same operative procedure. MRI revealed a residual dissection in the proximal descending aorta. Three years later she became pregnant again. This pregnancy was uneventful. Normal blood pressure was obtained with 50 mg of atenolol daily. Subsequent MRI showed no progression of the residual dissection. She was admitted at the Cardiology Department with 29 weeks of gestation for close follow-up. An elective caesarean section was performed at 33 weeks after counseling with Cardiology. The patient delivered a 1520 g male infant with Apgar scores of 9 at 1 minute and 10 at 5 minutes. She refused tubal sterilization.
Comment: It is crucial to advise women with previous aortic dissection about the potential fetal and maternal risks in further pregnancies. In these cases a normal blood pressure and a close cardiologic and obstetrical follow-up are essential in order to obtain a favourable outcome.
P-12-008 Systemis lupus erythematosus and pregnancy
M. Centeno, C. Araujo, R. Carvalho, P. Goncalves, M. Tuna, L. Pinto, S. Capela, R. Figueira, A. Marques, C. Cardoso, L.M. Graca
Santa Maria Hospital, Lisboa, Portugal
Objective: To evaluate obstetrical and perinatal outcomes in pregnant women with systemic lupus erythematosus (SLE).
Methods: Retrospective study of 64 pregnancies (52 women) complicated with SLE, from January 1989 to December 2005.
Results: Average maternal age was 28 years. SLE diagnosis was made during pregnancy in 2 cases only. In most of the women the disease was in remission at the beginning of pregnancy and an exacerbation occurred in 2 of them. Obstetrical complications occurred in 12 cases. Hypertensive disorders were the most prevalent complication followed by gestacional diabetes and abruptio placentae. The mean gestacional age was 39 weeks. There were 11 cases (20%) of preterm deliveries, four of them being iatrogenic.
The main cause of neonatal morbidity was prematurity. There was one fetal death at 23 weeks (severe SLE with renal and central nervous system involvement) and one neonatal death (premature spontaneous delivery at 26 weeks).
During the puerperium period, two women experimented a significant exacerbation of SLE. There was no maternal mortality.
Conclusions: If adequately planned and conveniently survailled by a multidisciplinary team, pregnancy in women with SLE usually has a favourable outcome.
P-12-009 Maternal plasma homocysteine and uterine artery dopplers
M.A. Guven1, H. Ekerbicer2, M. Kilinc3, A. Coskun1, S. Karakus1, O. Ozdemir1
1Dept. of Obstetrics and Gynecology, Kahramanmaras Sutcu Imam University, Kahramanmaras, Turkey; 2Dept. of Public Health, Kahramanmaras Sutcu Imam University, Kahramanmaras, Turkey; 3Dept. of Biochemistry, Kahramanmaras Sutcu Imam University, Kahramanmaras, Turkey
Objective: Our aim was to investigate the possible association between maternal plasma homocysteine concentration and outcome of pregnancy with respect to the uterine artery Doppler measurements at two stage screening method.
Methods: This prospective study was conducted on healthy women undergoing screening for pre-eclampsia by uterine artery Doppler velocimetry measured at 20–22 and 24–26 weeks of gestation, respectively. Abnormal uterine artery blood flow was defined as average resistance index (RI) > 0.58 of both uterine arteries and/or uni- or bilateral early diastolic notch. Homocysteine (coefficient of variation, 4.1%), measurement was performed by two competitive immunoassay methods involving two steps at 20–22 and 24–26 weeks' gestation.
Results: In total, 60 women were recruited abnormal Doppler findings were found in 18 of 60 (30%) women at 20–22 weeks of gestation. The latter finding was reduced to 10% (6/60) at 24–26 weeks of gestation. Two of these women developed pre-eclampsia during the rest of pregnancy. There was no significant difference in the maternal plasma homocysteine level of women with abnormal Doppler findings when compared with controls at first and second visits (p > 0.05).
Conclusion: Mid-trimester maternal homocysteine concentration is not elevated in women with abnormal Doppler finding at two-stage screening method.
P-12-010 Cholestatic hepatosis in pregnency: Patient the 22nd week of pregnancy
M. Dolezal, K. Suchova, T. Binder, I. Spalova, R. Vlk, M. Cerny
Dept. of Obstetrics and Gynecology, 2nd Faculty of Medicine, FN Motol, Prague, Czech Repub
Objective: Twin pregnancy complicated by a severe form of cholestasis started in the 22nd week of pregnancy.
Methods: Patient referred to our outpatient prenatal unit from other hospital with laboratory values AST 11.55, ALT 16.90, ALP 3.39, GMT 0.58, bilirubin 12.0, bile acids 85. The patient was hospitalized at risk pregnancy unit with monitoring of the fetuses daily by CTG and weekly by ultrasound. Used therapy contained ursodeoxycholic acid 3 × 500mg p.o., S-adenosyl-L-metionin 2 × 500 mg i.v. for 14 days after 2 × 500 mg p.o. daily, cholestyramin 3 × daily 4 g p.o., dexamethason 4 doses per 6 mg i.m.
Results: The pregnancy was extended until the 32nd gestational week but despite of the intensive therapy the serum values of bile acids were under 20 μmol/l, which is considered as safe value for the fetuses. In the 32nd gestational week the parameters of hepatic transaminases raised again so the pregnancy was terminated by Caesarean section without any complications. Fetus A weighted 1770 g, fetus B 1720 g and Apgar score was 8-9-9 for both of them.
Conclusions: The modern forms of treatment of intrahepatic cholestasis in pregnancy allows us to prolong its duration but they didn't lead to suppression of the disorder especially in case of the severe form. Monitoring of the babies is essential and the termination of pregnancy has to be indicated in case of any health threats that occur or in case of sufficient fetal maturity.
P-12-011 Vascular endothelial growth factor expression and secretion, its relation to fetal hypoxia
A. Perales1, D. Borras1, N. Ruiz2, I. Alonso3, C. Simon3, A. Pellicer2
1Hospital Universitario La Fe, Valencia, Spain; 2Hospital Peset, Valencia, Spain; 3IVI, Valencia, Spain
Objective: To evaluate the role of the VEGF system in response to fetal hypoxia, and the possible use of maternal plasma levels as markers of fetal hypoxia.
Methods: Maternal plasma samples were collected from 98 pregnancies at 2nd and 3rd trimester, and also before delivery; concurrently flow velocimetry waveforms of uterine arteries (UA), umbilical artery (Umb.A) and mean cerebral artery (MCA) were recorded and Doppler indices measured. At birth, umbilical artery and vein plasma was obtained to measure VEGF complex (free VEGF, VEGF soluble receptor Flt-1 (sFlt-1), total VEGF); also umbilical blood gas analysis was performed. A p < 0.05 was considered significant.
Results: In pregnancy, maternal sFlt-1 is negatively associated with gestational age (r = −0.23, p < 0.01), and the newborn weight (r = −0.31, p < 0.001). Uterine artery waveform has a positive correlation with maternal sFlt-1 (r = 0.24 p < 0.01) whereas no association was observed with free or total VEGF. Fetal artery Free and Total VEGF significantly exceeded venous levels (115.86 ± 7.1 vs. 106.50 ± 6.2, 324.32 ± 37.51 vs. 180.70 ± 17.61) respectively, Umbilical artery sFlt-1 was associated positively with umbilical cord pCO2 artery and vein (r = 0.45, p < 0.001, r = 0.34, p < 0.01), and negatively with pH artery and vein (r = −0.46, p < 0.001, r = −0.54, p < 0.001). Umbilical cord gases were not associated with maternal VEGF complex.
Conclusions: These results indicate that lower levels of maternal sFlt-1 are linked with the normal fetal development. The Fetus may be a net VEGF producer in response to its respiratory demans. Maternal VEGF complex do not appear to be a marker of fetal hypoxia.
P-12-012 How does hormones changing and intrauterine transfusions affects level adrenocorticotropic, cortisol and β endorphin in blood anemic and nonanemic fetuses
J. Dukanac-Stamenkovic1, N. Radunovic1, M. Cvetkovic1, A. Ljubic1, M. Antic2, D. Bratic1
1Institute of Gynecology and Obstetrics, Belgrade, Serbia; 2Clinical Centre Dr Dragisa Misovic, Belgrade, Serbia
Aim: Evaluation of the effects of Rh alloimunisation and intrauterine transfusions on fetal stress hormone levels (adrenocorticotropic ACTH), cortisol and β endorphin) and in pregnancies with non-anemic fetuses.
Method: Umbillical cord samples were obtained immediately prior and after intrauterine transfusions in 50 anemic and 34 nonanemic fetuses. Samples were assessed for ACTH, cortisol and β endorphin.
Results: Concentrations β endorphin were higher after transfusions (p = 0.68, T = −0.4157, CL 95%), and levels of cortisol were higher before transfusions (p > 0.1, T = 0.227, CL 95%), and ACTH values remained unchanged after transfusions (p ≥ 0.1, CC = −0.046, CL 90%). Compared anemic and non anemic fetuses, β endorphin and ACTH (p < 0.05, CL 95%, p < 0.05, CL 95% respectively) were higher in anemic fetuses and cortisol values were lower in anemic fetuses (p < 0.05, CL 95%).
Conclusion: Compared with pretransfusions values, fetal β endorphin values were lower and this relative decrease in fetal β endorphin following by fetal transfusions, correlated with reduction in fetal stress followed by transfusions induced increases in blood oxygen contents. ACTH values remained unchanged after transfusions and this were result from immature H-H-A axis. Lower post transfusions values cortisol, suggested that a reduction in fetal stress followed by transfusions.
Fetal β endorphin and ACTH were higher in anemic fetuses and this suggested prolongated stress, compared values anemic and nonanemic fetuses. Cortisol levels were paradoxal lower in anemic fetuses in our results.
P-12-013 ST waveform of the fetal electrocardiogram during labour of the fetuses with presumed intrauterine growth retardation
L. Hruban1, P. Janku1, B. Kurecova1, J. Zahradnickova2
1Dept. of Gynecology and Obstetrics, Masaryk University, Brno, Czech Republic; 2Dept. of Neonatology, Masaryk University, Brno, Czech Republic
Objective: To test the hypothesis that analysis of the ST waveform of the fetal electrocardiogram – STAN improves the timely detection of incipient fetal hypoxia during labour of the fetuses with presumed intrauterine growth retardation.
Methods: A prospective study of 134 births in women with diagnosed intrauterine growth retardation of fetus who were monitored at our department from 2003 to 2005. They were randomly assigned monitoring with cardiotocography – CTG combined with STAN (Group A) and CTG combined with fetal pulse oxymetry – FpO2 (Group B) during labour. The following data were evaluated: number of operative deliveries for fetal distress, pH in umbilical artery after labour and Apgar score. Moreover, newborns'condition was evaluated by number of days spent at neonatal intensive care unit (NICU) or intermediate care unit and a total length of stay in hospital. Neonatal sepsis, hyperbilirubinemia and results of neurological examination were investigated, too. The results were compared and statistically evaluated.
Results: The difference between Apgar score in 1st minute shows statistical significance, favours Group A (p = 0.018, p < 0.05). The Other data revealed no statistically significant difference between Group A and Group B.
Conclusion: We did not prove better ability of STAN to identify intrapartal hypoxia of the fetus with assumed intrauterine growth retardation in comparison to CTG combined with FpO2.
The study was supported by Ministry of Health of Czech Republic IGA MZ ČR NH.
P-12-014 Massive fetomaternal hemorrhage: A serious pregnancy complication
R. Gerychova1, P. Janku1, E. Racanska1, D. Chocholackova2
1Department of Obstetrics and Gynecology, Medical Faculty, Masaryk University, Brno, Czech Republic; 2Department of Obstetrics and Gynecology Znojmo Hospital, Znojmo, Czech Republic
Background: Massive fetomaternal hemorrhage is an uncommon problem during late pregnancy that places the fetus at risk of severe morbidity and mortality. Rapid and massive fetomaternal hemorrhage may be a cause of perinatal hypoxic damage or finally fetus death. Early diagnose a symptoms at presentation and appropriate management may permit the fetus to escape serious injury.
Cases: Four cases of massive fetomaternal hemorrhage in the third trimestr of pregnancy diagnosed in our department during the year 2005. The incidence of adverse neonatal outcomes was 75% (3 of 4). There was two early neonatal death, one child has sever neurological handicap. Three women required emergency Caesarean section, one case was identified after vaginal forceps delivery.
Conclusions: reduced fetal movement, sudden maternal reaction (hypotension, tachycardia, dyspnoe, nausea, vomiting), pathological cardiotocography (sinusoid pattern, decreased variability), pathological sonography (Doppler, biophysical score) – special hematological tests for determination of fetal erythrocytes in the maternal blood should be ordered. According the results appropriate emergency Caesarean section or intraumbilical transfusion – may improve the neonatal outcomes.
P-12-015 Sonographic evaluation of cervical length prior to labor induction: A marker for labor induction success
M. Theodora, G. Daskalakis, N. Papantoniou, A. Pilalis, A. Antsaklis
1st Department of Obstetrics and Gynecology, University of Athens, Athens, Gre
Objective: To determine the best cut-off point for cervical length which could be used as a predictive marker of successful induction of labor.
Material and Methodology: Sonographical cervical assessment was undertaken prior to induction of labor, in 67 women with singleton term and post term pregnancies who were admitted in our unit from August 2004 until December 2005.
Results: The mean age of the examined women was 27.8 years (16–42 years). 74.2% of them were nulliparas. The overall caesarean rate was 27.3%. The mean gestational age was 40 + 2 (38–42). In 83.3% these cases cervix was unfavorable (BC ≤ 5).
Cervical length ranged from 10–49 mm (median 25 mm). In cases were the cervical length was ≤27 mm (59%) vaginal delivery was achieved within 24 hours of induction in 74%. In the group of cervical length ≤27 mm the caesarean section rate was 20.5%.
In the group with cervical length of ≤27 mm, labor was commenced after placing one pessary of prostaglandin in 20 cases (52%) and a second pessary was needed in 15 cases, five of which had caesarean section.
In the group with cervical length more than 27 mm, labor was commenced after placing one pessary in 7 cases (27%) whereas a second pessary was needed in 18 cases 9 of which delivered by caesarean section.
Conclusion: Transvaginal sonographic evaluation of cervical length has proved to be o useful marker for the prediction of successful labor induction and vaginal delivery within 24 hours. In our group, the best cut-off point for the prediction of successful induction was 27 mm. Moreover short cervical length predicts shorter and easier labor induction in our study.
P-12-016 Value of doppler blood flow assessment in the prognosis of recipient death in TTTS
M. Ropacka, W. Markwitz, G.H. Breborowicz
University of Medical Sciences, Poznan, Poland
Objective: To assess the predictive value of hemodynamic disturbances in the assessment of the recipient death in TTTS.
Materials and Methods: The study group included 27 recipients. This study evaluated following dysfunctional fetal heart parameters: 1) heart/thoracic index (CC/TC > 0.4 defined cardiomegaly); 2) shortening fraction of right ventricle (SF RV) < 25%; 3) enlargement of the right ventricle (RV) (greater than 95 percentile for the given gestational age); 4) the increase of the interventricular septum (IVS) thickness (>4 mm); 5) tricuspid (TV) or mitral valve (MV) regurgitation. The pulsatile flow in the UV, the presence of reversed flow in the DV, and PI values > 95 percentile in the UA and <95 percentile in the MCA were concerned as abnormal. Markers of hemodynamic disturbances with fetal or neonatal recipient death were correlated. Sensitivity, specificity, positive and negative predictive value, and odd ratio were calculated.
Results: The highest sensitivity was related to cardiomegaly (100%), increased IVS thickness (88.2%), enlargement of RV and pulsatile flow in the UV (82.3%). The highest positive predictive was associated with the presence of TV or MV regurgitation and abnormal SF RV (100%), the pulsatile flow in the UV (93.3%) and reversed flow in the DV (90.9%). The highest negative predictive value was related to echocardiographic parameters. The statistically significant OR was observed in cases of TV or MV regurgitation (87.0 [4.0–1871.4]), pulsatile flow in the UV (42.0 [3.8–469.4]), enlargement of RV (18.7 [2.6–136.5]), the reversed flow in the DV (12.9 [1.3–125.9]).
Conclusion: Fetal echocardiography and the analysis of venous blood flow in the UV and DV demonstrate the higher value in the prediction of fetal or neonatal recipient death in comparison to the assessment of blood flow in the UA and MCA.
Supported by KBN 2 PO5E03027.
P-12-017 Twin-twin transfusion syndrome
N. Amaral, S. Valadares, I. Martins, E. Dias, T. Simoes, A. Cohen, J. Correia
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objective: To review cases of twin-twin transfusion syndrome (TTTS) occurring in our hospital from 1994 to 2005, treatment options and their impact on pregnancy and child outcome.
Methods: TTTS was identified by ultrasonographic criteria (n = 38) and classified by Quintero score (Q). Under 26 wk (Q2 or higher), those who opted for treatment, were offered laser ablation, others were offered either expectant management or amniodrainage. We evaluate fetal and neonatal deaths, neonatal morbidity, gestational age at birth, birth weight, significant birth weight discordance and neurologic morbidity.
Results: 33 cases had complete data. 27 were diagnosed <26 wk of gestation and 6 after. 21/27 cases fulfilled treatment criteria: 16 had laser ablation, 3 amniodrainage, 2 expectant management. Of the 32 fetuses in the laser group, 20 (62.5%) survived (7 pairs and 6 co-twins) but 5 had neonatal death (NND). The overall survival rate was 46.9% (56.2% of women taking 1 baby home; 43.8% taking both). In the 13 pregnancies in which 1 fetus survived, labor had a median delay of 8 wk (SD 4.7), 9 delivered after 28wk. In the amniodrainage the delay to deliver was 4 wk with 2 pregnancies ending with 2 liveborn and 1 (Q4) with 2 NND. In the expectant management group there were 2 fetal deaths, 1 NND and 1 liveborn. The cases diagnosed >26wk were offered expectant management and delivery within 1 wk. At the end there were 5 SGA (1 NND). 3 cases had birth weight discordance (>25%) and all survived. Neurologic development is known for 20 cases (total survivors 31), only one had a minor disability.
Conclusions: Although mortality rate (fetal plus neonatal) is still high, laser ablation seems to be associated with higher survivors rate, later gestational age at delivery without major neurologic disability.
P-12-018 Is really monochorionic twins a high risk pregnancy?
F. Ribeiro, R. Lermann, N. Amaral, E. Dias, T. Simoes
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objective: We evaluated the morbidity and mortality of monochorionic (MC) vs. dichorionic (DC) twins followed at our hospital.
Methods: We identified MC twins amongst the 893 twin pregnancies followed and delivered at our hospital, between September 1994 and March 2005. We excluded twin births <24 weeks' gestation, and considered the maternal age and parity, mode of conception, maternal complications of the pregnancy, mode of delivery, gestational age at birth, birth weigh, birth weight discordance >25%, Apgar scores, major malformations, early neonatal mortality and major neonatal morbidity.
Results: We analyzed 193 MC diamniotic and 447 BC twin gestations. We found 5 (1.3%) intrauterine fetal deaths in MC twins and 5 (0.6%) in DC group. Gestacional age at delivery in MC vs. DC group was: 9.3% vs. 4.0% <32 wks, 46.1% vs. 29.5% 32–35 wks, 45% vs. 66.7% >36 wks. SGA (birth weight <P10 for twins) was more prevalent in DC twins (9.6% vs. 8.8%). Birth weight discordance (>25%) was higher in MC group (13.9% vs. 8.7%) and the ratio of SGA in birth weight pairs was also higher in this group (66.7% vs. 56.4%). Neonatal asphyxia (Apgar score <7 at 5′) was 2.1% in DC twins and 1.3% in MC. Perinatal morbidity is under evaluation.
Conclusions: There is a trend to preterm delivery and significant birth weight discordance in monochorionic twins. However SGA and neonatal asphyxia were more prevalent in dichorionic twins.
P-12-019 Assisted versus spontaneous twin pregnancy – different outcomes?
R. Lermann, R. Ribeiro, N. Amaral, E. Dias, T. Simoes
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objective: To evaluate spontaneous vs. iatrogenic twin pregnancies and their obstetrical and perinatal outcomes.
Methods: We evaluated retrospectively twin pregnancies that had their antepartum surveillance in our hospital between 1994 and 2004. We analysed maternal age, chorionicity, obstetrical and maternal complications, gestational age at birth, delivery data and perinatal outcomes.
Results: We followed 640 twin pregnancies: 525 (82%) spontaneous and 115 (18%) product of assisted reproductive technology. Monochorionocity was more prevalent in the spontaneous group (35% vs. 7.8%). There were 10 stillbirths in the spontaneous group (4 cases of TTTS) and no stillbirth in the iatrogenic group. Preterm delivery (<37 wks) occurred more frequently in the iatrogenic group (74.8% vs. 62.9%). We found 11.3% (26/230) SGA (birth weight < P10 for twins) liveborns in the iatrogenic group vs. 8.9% (94/1050) in the spontaneous group. Although birth weight discordance (>25%) was higher in the spontaneous group (11.1% vs. 6.9% in the iatrogenic group) the ratio of SGA in birth weight pairs was higher in the iatrogenic group (87.5% vs. 56.9%). Perinatal morbidity is under evaluation.
Conclusions: Assisted reproductive technology is associated with higher rate of preterm delivery, SGA and significant birth weight discordance. In spite of that there were less fetal deaths in the iatrogenic group.
P-12-020 Triplet pregnancies: Statistics
F. Rosario, B. Nogueira, P. Condeco, A. Lima, E. Dias, T. Simoes
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objectives: To evaluate maternal complications and perinatal results of triplet gestations.
Methods: Retrospective study of all triplet pregnancies that occurred in a 10-year period, with delivery at Maternidade Dr. Alfredo da Costa, and which were followed through on the Multiple Pregnancy Consultation. Several variables such as age, parity, obstetrical and clinical complications, admission during pregnancy, type of delivery and puerperal mobidity were studied in 48 pregnancies. The variables concerning newborns well-being were gestational age, weight, intrauterine growth restriction, fetal discrepancy, Apgar score and neonatal morbidity.
Results: Between 1994 and 2004, 833 multifetal gestation births occurred, of which 48 were triplets, representing 5.76% from the total of multiple pregnacies. The majority of these births occurred with maternal ages between 30–34 (45.8%), and 35–39 (37.5%). Of the 48 triplets pregnancies, 38 pregnant women were nuliparous (77.5%). The pregnancy was spontaneous in 16 women (32.6%); the remainder of pregnancies resulted from assisted reproduction techniques. The most common complication was preterm delivery (75.5%), and 44.8% of the cases needed hospitalization before delivery. Delivery was made trough a caesarian section in 97.9% of the cases with an average gestational age of 31.5 weeks. The average weight was 1755 g, with 30.8% weighing less than 1500 g, and 63.2% weighing between 1500 and 2499 g, for a total of 136 newborns.
Conclusion: The triplet pregnancies studied had a high rate of obstetrical complications and required a long period of maternal hospitalization. The vast majority of these pregnancies ended with a caesarian operation. Around 90% of new-borns survived without further complications.
P-13-001 Fryns syndrome: A case without diaphragmatic hernia
S. Heljic1, E. Saracevic1, S. Terzic1, M. Mackic2
1Pediatric Clinic of Clinical University Center Sarajevo, Sarajevo, Bosnia and Herzegovina; 2Institute for Human Genetics of Medical Faculty University of Sarajevo, Sarajevo, Bosnia and Herzegovina
Fryns syndrome is an extremely rare developmental disorder associated with deletion of long arm of chromosome 16. Characteristics of the Fryns syndrome are: craniofacial dysmorfism, diaphragmatic defects with lung hypoplasia, brain and urogenital abnormalities and other developmental disturbances. After the first description of syndrome in two stillborn sisters (1971), new reports appeared with descriptions included disorders which have not described previously. We described a case of female liveborn with deletion of long arm of chromosome 16. Our patient had a typical craniofacial dysmorfism, brain abnormalities (Dandy Walker malformation), cardiac defects (artial septal defect and persistent ductus arteriosus), renal hypoplasia, gastrointestinal problems, hypotonia and feeding difficulties. Our patient had no diaphragmatic hernia and he survived neonatal period with severe neurological impairment. Description of the new case of 16q deletion, due to rarity of the syndrome, makes the contribution in better recognition of various possible phenotype characteristics.
P-13-002 Simultaneous assessment of CYP2D6 and CYP3A4 ontogeny in early neonatal life
K. Allegaert1, A. Debeer1, R. Verbesselt2, M. Rayyan1, G. Naulaers1, J. de Hoon2
1Division of Mother and Child, University Hospital, Leuven, Belgium; 2Center for Clinical Pharmacology, University Hospital, Leuven, Belgium
Introduction: Total cytochrome (CYP) activity in the foetal liver is 30 to 60% of adult values but iso-enzyme specific ontogeny precludes the generalisation of a simple single developmental pattern for CYP activity, necessitating iso-enzyme specific assessment. Since both CYP2D6 and CYP3A4 are involved in tramadol disposition, tramadol disposition was used to simultaneously assess ontogeny of these iso-enzymes.
Methods: The contribution of tramadol (M), O-demethyl tramadol (M1, CYP2D6 mediated) and N-demethyl tramadol (M2, CYP3A4 mediated) to overall tramadol elimination and the log M1/M2 were assessed in 24 hours urine collections during continuous intravenous tramadol administration and correlations with perinatal characteristics [postnatal age (PNA), postmenstrual age (PMA)] were investigated Citation[1].
Results: Of the total amount of M administered in a 24 h interval, 34.5 (SD 6.1)% was retrieved in the urine as parent compound or metabolite in the first 24 hours in 25 neonates and young infants (PMA 25–53 weeks). This retrieval primarily consisted of M 79 (SD 18)%, M1 contributed 10 (SD 17)% and M2 3 (SD 3.4)%. Correlations of the contribution of M (r = −0.73), M1 (r = 0.68) and M2 (r = 0.4) to overall M elimination with increasing PMA were observed. Mean log M1/M2 was −0.01 (SD 1.98). Significant inverse correlations between the log M1/M2 ratio with increasing PMA (r = −0.68, 95% CI for r = −0.85 to −0.39, p = 0.0002) and PNA (r = −0.75, 95% CI for r = −0.88 to −0.49) were observed.
Conclusions: A progressive increase in phenotypic activity of both CYP2D6 and CYP3A4 were observed in the first months of life. Compared to developmental changes in CYP2D6 activity, maturational changes in CYP3A4 activity are relatively delayed and develop at a slower pace in the first months of life.
P-13-003 Experience in immigrant people cares in hospital materno-infantil vall d'Hebron in barcelona (HMIVH)
J. Almar, C. Abellan, N. Tokashiki, J. Sanchez de Toledo, S. Salcedo
Hospital Vall d'Hebron, Barcelona, Spain
Objectives: Analyse the incidence and origin of foreign pregnant attended in maternity unit of HMIVH and its impact on activity of neonatology unit.
Material, Methodology and Results: During 2004, 4335 births were attended from 4497 newborn children. From that figure, 996 correspond to foreign mothers with 1019 new-born children (23%), and 353 (35%) were ingresses in the several units of our unit. 106 newborn children (10.4%) came from 16 European countries (79.2% from outside the EU, 39.3% Romanian). 217 newborn children came from 10 African countries (77.4% Moroccan). 99 newborn children came from 11 Asian countries (63.6% from China) and 598 from 15 Latin American countries (46.1% Ecuadorian).
From the total hospitalised newborn children, 140 (40%) were in the hospitalisation unit and 213 (60%) in the observation unit of the maternity unit. 666 newborn children remained in their mother room.
Comments and Conclusions: Percentage of foreign mothers is growing in our society (23% of births). 13.74% of newborn children from foreign mothers ingresses in hospitalisation unit, while in the Spanish case it is 26.22%. We believe that this difference is due to the fact that the Spanish pregnant coming to our hospital is high risk in-patient.
We believe that it is important to include the position of a cultural mediator in the Neonatology Unit staff. It permits to integrate the foreign newborn families in the neonatal care activity.
P-13-004 Infertility in ancient times
M. Christodoulaki, G. Moschaki, G. Tsoukalas, P. Theoulakis, S. Blazaki, S. Fiotaki, A. Kotta, E. Xidaki, E. Kourmoulis, I. Tsoukalas
General Hospital of Chania, Chania, Greece
Aim: To analyze the opinion of physicians in ancient Greece about infertility in males and females and methods of treatment.
Method: Review of texts written from ancient Greece to Byzantine period.
Results: Causes of female infertility are: anatomical anomalies of uterus such as flexion or prolapse, obesity, disorders of menstruation, traumatic injuries of uterus, resulting from previous abortion or birth, bad health of mother, local or social mores that influence fertility.
From the other hand, causes of male infertility can be weakness of male member, luck of production of sperm or bad quality, slant of penis which makes difficult to the sperm to reach the uterus or asymmetry between the genital male organs and the length of uterus.
It is worth mentioning that the Byzantines gave big emphasis to the analysis of male infertility, especially to the eunuchs.
Concerning the therapy, Hippocrates suggested certain methods that facilitate the normal menstruation which he believed that played the most important role in fertility of the couple and the conception. Also, famous in that period was the use of holy herbages and seeds, ivy leaves in old wine, balsam and special conceptive drugs.
Conclusion: The existence of infertility in both sexes is confirmed even from ancient times. The physicians tried to comprehend the causes and to give an appropriate solution to this serious problem using all the means that had at their disposal.
P-13-005 Intestinal atresia in a newborn with cutis marmorata telangiectatica congenita
A. Zecic, M. Van Winckel, G. Mortier, K. Smets, P. Vanhaesebrouck
Gent University Hospital, Gent, Belgium
Background: Cutis marmorata telangiectatica congenita (CMTC) is a rare congenital disorder that can be segmental or generalized in distribution. The lesions manifest as a characteristic reticular vascular pattern which is accentuated by cold temperature or distress. More than one half of the patients with CMTC have additional extra-cutaneous associated congenital anomalies, including segmental overgrowth, cleft palate, glaucoma and mental retardation.
There are few reports of arterial disease in patients with CMTC. We report a newborn with CMTC and “apple peel” type intestinal atresia.
Case Report: The patient was diagnosed prenatally with intestinal obstruction. A baby boy was born at 35 weeks pregnancy by vacuum extraction. Extensive amount of bile-stained gastric fluid was present at birth. Physical examination revealed striking widespread erythematous reticulate cutaneous marking over the right side of the body and over the left leg and right leg hypertrophy. Surgery performed shortly after birth, revealed multiple intestinal atresia type “apple peel”. Resection of the atretic intestines resulted in a short bowel syndrome with 20 cm of ileum, ileocaecal valve and colon left in place. The patient required parenteral nutrition until the age of 13 months. The reticular capillary stain of his skin gradually faded, over the period of 18 months, although hypertrophy of the right leg remains obvious.
Discussion: CMTC is a relatively rare anomaly characterized by a congenital reticulate vascular capillary stain with a variable pattern. Disorders of large vessels are infrequent in the paediatric population. There are two reports of arterial disease in two patients with CMTC (stenosis of deep femoral artery in one case and iliac artery stenosis in the other). However, a 16 year old girl was described with mesenteric arterial malformations presenting with symptoms of mesenteric angina. Since atresias are thought to be most likely the result of a late intrauterine mesenteric vascular accident, we speculate on the existence of intrauterine mesenteric arterial malformations in patients with CMTC which can lead to multiple intestinal atresias.
Conclusion: In newborns with obvious CMTC and abdominal symptoms, the possible existence of intraabdominal arterial malformation should be considered.
P-13-006 Neonatal approachment to the problem of polycystic kidney disease
S. Stefanovic1, V. Stefanovic1, V. Stefanovic2
1Institute for Mother's and Children's Health Care, Medical Faculty, Novi Sad, Serbia; 2Medical Faculty, Novi Sad, Serbia
Introduction: By current convention, the term polycystic kidney disease (Ren polycisticus infantilis) is restricted to 2 conditions: autosomal recessive polycystic kidney disease (ARPKD) – known as infantile polycystic kidney disease – and autosomal dominant polycystic kidney disease (ADPKD) – sometimes called adult polycystic kidney disease. The abnormal gene for ARPKD has been localized in the short arm of chromosome 6. The frequency of ARPKD is one case in 6000 to 50,000 births. As it is a recessive disease, parents are unaffected. The reccurence risk is 25% in each pregnancy.
Aim: To point out the importance of prenatal and early neonatal diagnose of this kind of congenital abnormality in order to prevent severe consequences as neonatal sepsis in certain cases and to slow down the development of progressive renal insufficiency.
Material and Methods: We will review a neonatal history of a female newborn infant hospitalized in the neonatal department of Institute for mother's and children's healthcare in Novi Sad.
Case Report: L.K. was born on 29th February 2004. In spite of prenatal diagnosis of hydronephrosis bilateralis, parents brought her to ultrasound check in the second week of life as they they did not believe in diagnosis of kidney failure but neonatal jaundiced forced them to ask for doctor's advice.
Prenatal anamnaesis: II pregnancy/one artefitial abortus/of 29 year old women, she was working with metacril acid, anesthetics and other drugs till the beginning of the 8th month of pregnancy as a nurse in the field of dental medicine. During this pregnancy she was healthy except urinary tract infections, she frequently had urinary tract infections during her whole life. In 38th GS the ultrasound of fetus revealed bilateral hydropnephrosis and parents were sent for consultation to urologist. In mothers family was positive anamnesis towards kidney diseases – her sister and father had ultrasound findings of cystic kidney without health problems.
Perinatal anamnaesis: Delivery occurred in 40th GS, it was spontaneus, vaginal but oligohydroamnion was clearly notified. The baby was eutrophic for GS/body mass 3300 g, body length 49 cm, head circumference 34 cm, AS 9/10/.
Status presens: It is a female newborn, BM 3000 g BL 53.5 cm HC 35.5 cm, fat tissues is very thin, colour of skin is intensive yellow (verdin icterus) and although clinical and neurologic findings are normal for age, the child looks like a chronicly ill neonate patient.
Laboratory findings: WBC 12.32 G/L (nesegm 0.01 segm 0.57 eoz 0.03 lym 0.38), RBC 3.72 T/L, Hgb 118 g/l, Hct 37.8%, PL 500 G/l. K serum bilurubinaemia 193.5 μmol/l (conjugate bil 113.2 μmol/l e.g. over 60%), hepatic enzymes enlarged, urea 9.3 mmol/l, creatinine 152.5 μmol/l. Cl 118, Na 150, K 5.2, Ca 2.54, SO2 94%, pO2 9.86 kPa, pCO2 3.38kPa, pH 7.387, BE −8.1 mmol/l. CRP: pozitivan (24 mg/l). Urine: cloudy, pH 5, specific weight 1.010, proteins ++; sediment: 2–3 RBC, WBC, a lot of epithelial cells and bacteries. Urine culture: Escherichia coli > 100,000/ml. Hemoculture: negative.
Ultrasound scan: Bilateral enlargment of kidneys with a few cystic formations in both kidneys.
Therapy: Due to clinical and laboratory signs of neonatal infection, our patient was treated by antibiotics/Pentrexyl, Amikacyn iv/during 2 weeks. Clinical findings were improving fastly, our patient began to eat eagarly and to gain on weight, laboratory signs of neonatal infections as leukocytosis, positive C reactive protein, conjugated bilirubinaemia, enlargment of hepatic enzymes diminished. Urine culture was negative. Laboratory signs of renal insufficiency were recognized by nefrologist who recommended the ammount of infusion of G/S 5:1 and NaHCO3 day by day during the whole period of treatment.
Prognosis: The baby was dissmissed from neonatal department in good condition (weight 3450 g, length 55 cm, head circumference 36.5 cm) with the recommendation of regular and frequent checkings in nephrology department of our hospital.
Conclusion: Newborns with ARPKD should be carefully observed as soon as possible after delivery in order to check renal function and also to recognize and choose adequate treatment of urinary tract infection.
P-13-007 Neonatal haemolytic disease and psychomotor development in infancy
S. Stefanovic1, V. Stefanovic1, V. Stefanovic2
1Institute for Mother's and Children's Health Care, Medical Faculty, Novi Sad, Serbia; 2Medical Faculty, Novi Sad, Serbia
Introduction: In severe indirect hyperbilirubinaemia/above 360 μmol/l, free bilirubin entry into brain occurring toxic effects on brain cells. Kernicterus is a pathologic diagnosis and refers to yellow staining of the brain by bilirubin together with evidence of neuronal injury. Nowdays, kernikterus is a very rare complication of severe neonatal hyperbilirubianemia due to modern treatment of haemolytic disease/exasangvinotransfusion, intensive phototheraps, imunoglobulins etc. Yet we can clinically recognize children with severe neonatal jaundice if we do careful neurologic assessment in the first year of life although there is little evidence showing adverse neurologic outcome in healthy term neonates.
Aim: To notice if there is any significant differences in neurologic outcome during the first year of life in children with neonatal haemolytic disease treated with or without EST in accordance to American Paediatrics Academy protocol.
Material and Methods: Prospective clinical study was proceeded in 100 term neonates hospitalized due to haemolytic disease in neonatal department of Institute for mothers and children health care in Novi Sad, Serbia and Montenegro, period 1999–2004. They were divided in two groups: a) neonates treated with EST, and b) correlated control group neonates treated without EST. Neurological assesment was prepared in age of 6 weeks, 3, 6, 9 and 12 months. Psycho test/Brunett-Lazine – was done at age of 9 and 12 months. Results were statistically counted.
Results: Hypotonia was the most feequent patologic sign of motor development during the first year of life and it was found in over 50%. Hypertonia was not recognized in any case. Psychotest showed normal psychomotos development in all cases but at the bottom range/RQ 91.66 normal 90–125. There was no difference between a) and b) groups but there was statistically significant difference between boys and girls/90.16:93.16.
Conclusions: There is no evidence of pathologic psychomotor development during first year of life in infant with severe neonatal hyperbilirubinaemia wheather the treatment was by EST or not. Psychomotor development was in the range of the lowest normal level for age. Slight differences in psychomotor development were recognized in infants of different sex. There is a possibility that CNS in male neonates is more sensitive toward toxic effect of bilirubin.
P-13-008 The Wiedemann-Rautenstrauch (neonatal progeroid) syndrome: Report of two new cases
N. Tekin, M. Ayata, E.C. Dinleyici, M.A. Aksit
Eskisehir Osmangazi University, Medical Faculty Department of Neonatology, Eskisehir, Turkey
Objective: Wiedemann-Rautenstrauch syndrome (WRS), OMIM number: 264090, or neonatal progeroid syndrome, is a rare condition with poor prognosis, thought to be inherited in an autosomal recessive manner and characterized by premature aging appearance recognizable at birth. The diagnosis is made by identification of the characteristic clinical findings. We presented two new cases with this rare syndrome.
Case Reports: Both of two infants were born after a pregnancy complicated with intrauterin growth retardation. Dysmorphic features of our low birth weight patients included pseudohydrocephalus, a tiny face and mouth, prominent eyes, thin wrinkled skin, lipoatrophy and gluteal fat pads and thin ribs. Aged appearance was remarkable and suggestive of the Wiedemann-Rautenstrauch neonatal progeroid syndrome in the presence of other associated features.
Conclusion: The neonatal progeroid syndrome represents a complex of symptoms with unknown cause and pathogenesis. Herein we presented two new cases of Wiedemann-Rautenstrauch syndrome that was diagnosed just after birth. We reviewed the previous reports and discussed the differential diagnosis of this rare syndrome.
P-13-009 Dermatitis exfoliativa staphylococcica (SSSS) – case report
S. Prcic1, S. Stefanovic1, V. Stefanovic2, T. Panic2
1Institute for Mother's and Children's Health Care, Medical Faculty, Novi Sad, Serbia; 2Health Care Center, Novi Sad, Serbia; 3Healt Care Center, Novi Sad, Serbia
Introduction: Staphylococcal scalded skin syndrome (SSSS) occurs almost exclusively in infants and toddlers. Bullous lesions are caused by certain epidermal toxin-producing types of Staphylococcus aureus, group II, phage type 71. Gentle pressure on the skin causes the upper epidermis to slide off, leaving a denuded base (Nikolsky sign). When a Nikolsky sign is present, minimal shearing force produced by finger pressure will induce a skin slough or blister formation.
Most SSSS is associated with a primary cutaneous infection. However, the soluble toxin that causes the rash may be produced by an occult infection as osteomyelitis, septic arthritis, pneumonia, or meningitis.
Case Report: We present a patient in whom the first skin manifestation appears one day before hospitalisation. He had blisters with purulent contents on the right arm. The child was irritability, fever was not. The first child was born at term by first controlled pregnancy.
Status praesens: A six week old male newborn infant, eutrophic for age, physical examination and neurologic neonatologic examinations revealed healthy newborn infant except physical examination of skin. Dermatologic examination: Skin lesions were localised on the face and the scalp, right arm and perianogenital region, presented erythema and blistering. Nikolsky sign was present.
Laboratory Tests: WBC 16.99 g/l, CRP positive, bacteriologic test from skin lesions: E. coli and Staphylococcus aureus.
Treatment was systemic with parenteral antibiotic sensitivity of the cultured bacteria (Longaceph, Amikacin) and topical symptomatic therapy.
Ten days after treatment developed the generalised desquamation. Lesions responded well to topical Panthenol ung, reepithelization occurs within a week.
Conclusion: SSSS should be considered in any child who develops a generalized, tender erythema associated with a Nikolsky sign. Although SSSS is usually self-limited in healthy children, immunocompromised patients may develop complications related to their primary staphylococcal infection.
P-13-010 Psychomotor development during the first year of life in infants with perinatal hypoxia
V. Stefanovic1, S. Stefanovic2, V. Stejin3
1Health Care Center, Novi Sad, Serbia; 2Institute for Mother's and Children's Health Care, Medical Faculty, Novi Sad, Serbia; 3Institute for Mother's and Children's Health Care, Medical Faculty, Novi Sad, Serbia
Introduction: There are plenty of prenatal, perinatal and postnatal factors that can induce various kinds of brain lesion. The basic risk factor for brain development and function capacity of neurons is hypoxia. Hypoxic impact toward brain structures can be recognized: (1) during pregnancy – EPH gestosis or hypertension during pregnancy, preterm contractions of uterus, anatomic disorders of funiculi umbilici, severe anaemia, respiratory or cardiovascular disorders of pregnant woman; (2) during delivery – prolonged or induced delivery; (3) during the early neonatal period -severe hyperbilirubinaemia, birth injury, sepsis.
Aim: First signs of brain dysfunction can be recognized through careful neurological assessment of the newborn by the end of the early neonatal period. At that time, the newborn infant is at home due to early discharge from the hospital and only a nurse can notice if there are any problems in the infant's behaviour, but if she is not properly trained, that particular child may never obtain medical care. This is the reason why we wanted to choose newborns with signs of brain dysfunction at birth and to follow their psychomotor development during the first year of life in order to notice if there is a unique model of development in those cases.
Method: During a prospective clinical study (2001–2005) we followed the psychomotor development during the first year of life of 100 children who had perinatal hypoxia (Apgar score <7, US scan: hypoxia and/or oedema cerebri) and were hospitalized in the neonatal unit of our Institute. After their discharge from the hospital, they had regular medical check up by a neonatologist and a neurologist at the ages of 6 weeks, 3, 6, 9 and 12 months and a psychotest/Brunet-Lezine/at 9 and 12 months of age.
Results: At 3 months of age, the most common problem was hypotonia, dystonia was diagnosed in 12% of our patients, others were without neurological problem.
At 6 months of age the number of infants with hypotonia decreased but the number of infants with dystonia increased and for the first time in the study, we recognized spasticity in 6 infants.
At 9 months of age, hypotonia was observed in 22 cases, spasticity in 3 cases, others were without neurologic problems.
At 12 months of age, 10 children still had hypotonia, one child had a spastic motor development and the others were without neurological problems. Psychotest at 9 and at 12 months of age revealed normal results (QR 92).
Conclusion: Our results are optimistic due to the great plasticity of brain that is one of the unique possibilities of newborns and infants and due to careful neurologic assessment that detected patients for the early neurostimulation programme.
P-13-011 Follow-up of psychomotor development during the first year of life in neonates with birth injury
T. Panic1, S. Stefanovic2, V. Stejin2, V. Stefanovic1
1Health Care Center, Novi Sad, Serbia; 2Institute for Mother's and Children's Health Care, Medical Faculty, Novi Sad, Serbia
Birth injury is a very common problem in everyday neonatal practice. Sometimes it is recognized immediately after birth and those neonates are urgently transported to neonatal unites. In same cases these children are dismissed from delivery room as healthy infants but when consequences occur they come to neurologist as a problem.
Aim: To reveal psychomotor development in the first year of life in neonates with severe birth injury.
Material and Methodology: During 5 years (2000–2005) we made a follow up study of 60 neonates with severe birth injury (hypoxia perinatalis, kephalhaemathoma) AS less than 7 in the first minute of life. The diagnose was confirmed by clinical and neurological assessment and US of brain/intracranial haemorrhage, hypoxia cerebri, oedema cerebri. They were checked up by neonatologist and neurologist in certain age of life – 3, 6, 9, 12 months. Psycho test was done at 9 and 12 months/Brunnete-Lazine scale.
Results: 3 months old age-hypotonia in 52 cases, dystonia in 5 cases, healthy 3 cases 6 months of age-hypotonia in 40 cases, dystonia in 5 cases, spasticity in 2 cases 9 months of age-hypotonia in 35 cases, dystonia in 3 cases, spasticity in 1 case 12 months of age-hypotonia in 16 cases, spasticity in 1 case.
Psycho test: Score 92.
Conclusion: Good results are due to neurostimulation programme adviced on time, when first signs of psychomotor problems are seen but yet in the period of life when brain has the maximun plasticity.
P-13-012 Our experience considering fetal outcome using vaginal insert, 10 mg dinoprostone for cervical ripening in posterm pregnancies
M. Kalloniatou, C. Christodoulaki, M. Christodoulaki, M. Kampanieris, K. Stamou, D. Gentsidis, A. Tsopelas, G. Daskalakis
General Hospital of Chania, Chania, Greece
Objective: The purpose was to determine the impact of using vaginal insert, 10 mg dinoprostone on the perinatal outcome of patients admitted for induction of labor at posterm.
Study Design: Patients (n = 180) included in the study were those, who were admitted for induction of labor at 40–42 weeks of gestation, with unfavourable cervix intact membranes, NST reactive, normal U/S findings, no maternal pathology. n = 40 women underwent induction of labor using amniotomy, 32 women using oxytocin only and 18 women using vaginal insert of dinoprostone and then amiotomy.
Results: The four groups were similar regarding maternal age, gestational age, and birth weight. The number of caesarean deliveries due to fetal distress or failure of the myometriume to achieve synchronous contractions was significantly higher in the dinoprosone group. There was no significant difference among the four groups regarding the Apgar scores or neonatal admission in neonatal intensive care unit.
P-13-013 Evaluation of effectivity of interventional strategies in slovak neonatology
F. Bauer, G. Magyarova, K. Demova
Novorodenecka klinika SZU a TU, Nove Zamky, Slovak Republic
Objectives: Evaluation of effectivity of interventional strategies in Slovak Neonatology and Perinatology.
Methods: Retrospective analysis of newborn delivered in Slovakia in the years 1999–2003. Comparison of the results among various regions, states and years.
Results: VLBW infants: Main strategy in this group was concerned to intrauterine and postnatal centralization and displacement of the border of viability. Increasing of centralization to perinatal centres from 29% in the year 2000 to 75% in the year 2003 brought decreasing of mortality by 18%.
Perinatal asphyxia: After the realization of Resuscitation and Stabilization Project in Slovak Neonatology the rate of mortality for asphyxia was decreased from 17.8% (in 2002) to 13.5% (in 2003).
Congenital abnormalities (CA): There is an increasing tendency in the rate of mortality. Intrauterine detection of CA is only 13%.
Extension of priorities: The specific neonatal mortality in group 1500–1999 g is high (compare to CR more than three times higher: 21.4‰ in SR: 6‰ in CR) and has increasing tendency (0.6‰ in 1999 to 0.72‰ in 2003).
Conclusions: Interventional strategies were correctly realized in group VLBWI and perinatal asphyxia. Further improvement is possible by greater centralization and by innovation of equipments. Inappropriate i.u. detection of CA is a reason of nonimprovement in specific mortality. Interventional strategy in the group 1500–1999 g was oriented on prevention and treatment of i.u. and early infections and support of centralization.
P-13-014 Depression and anxiety after delivery
O. Giakoumaki1, L. Lili2, K. Vassilaki1, C. Tziachrista1, M. Skouroliakou2, G. Liossis2
1Neonatal Unit, Elena Venizelou Perinatal Center, Athens, Greece; 2Harokopio University, Dept. of Science of Nutrition and Dietetics, Athens, Greece
Objective: To study postpartum psychological distress in our population.
Design: Two hundred and fifty women born in our hospital participated in the study. They all were able to communicate in the Greek language. They were administered two questionnaires the Edinburgh Postnatal Depression Scale (EPDS) and the State-Trait Anxiety Inventory (STAI). They completed the questionnaires 2–3 days after their delivery and were re-evaluated at 3 months and 6 months postpartum.
Results: The findings indicate that a 14.5% of women scored high on the Edinburgh Postnatal Depression Scale (EPDS > 14), 2–3 days postpartum. The social factor that has a statistical significance in the maintenance of post-partum depression is the age of the mother as the mothers that have EPDS > 14 have the age of 29.3 ± 5.8 and those with EPDS <14 have the age of 31.6 ± 5.8, p < 0.008. Other factors does not seem to influence psychological distress. The findings indicated that a 22.9% of women experience state anxiety and a 22.9% trait anxiety, 2–3 days postpartum. There is a significant relationship between depression and anxiety. A 36.5% of women with high scores in the stait anxiety have high scores of depression, p = 0.000 and have five times the risk of depression OR = 4.5 (2.46–8.46). A 37.5% of women with high scores in the trait anxiety have high scores of depression, p = 0.000 and have five times the risk of depression OR = 5.37 (2.8–10.2).
Conclusion: Our results on the prevalence of postpartum depression are consistent with the literature. The anxiety level is high; however, there is a lack of research on the role of anxiety in the postpartum period. The high relationship between anxiety and depression suggests a strong influence between these two psychological factors.
P-13-015 Ten years use of the Nordic-Baltic perinatal death classification in Iceland
R. Bjarnadottir1, R. Geirsson1, G. Palsson2
1Department of Obstetrics and Gynaecology, National University Hospital, Reykjavik, Iceland; 2Department of Pediatrics, National University Hospital, Reykjavik, Iceland
Objective: To audit perinatal deaths in Iceland (≥22 weeks or 500 g) over a 10-year period using the Nordic-Baltic Perinatal Death Classification (N-BPDC). This classification consists of 12 groups based on the following variables: time of death in relation to admission and delivery, fetal malformation, gestational age, growth retardation and Apgar score at five minutes. By identifying major groups and areas for improvement the classification focuses on potential avoidability from a health service perspective.
Materials and Methods: All cases of perinatal death in Iceland 1994–2003 were found using the Icelandic Birth registry. Medical records were analysed for each case which was then grouped according to the Nordic-Baltic Perinatal Death Classification.
Results: In the 10-year study period there were 42,106 deliveries and 272 perinatal deaths. Of these 203 infants were stillborn (74.6%) and 69 (25.4%) early neonatal deaths. The cumulative perinatal motality rate (PNMR) was 6.4/1000 for all perinatal deaths (≥22 weeks/500 g) but 4.6/1000 using a cut off of ≥28 weeks/1000 g for stillborn infants. By far the largest N-BPDC group was group III: intrauterine deaths of non growth-retarded singletons ≥28 weeks; 30.9% of all perinatal deaths. The majority of early neonatal deaths were in group XII: early neonatal death before 28 completed weeks of gestation, 18% of all perinatal deaths and thus the next largest group. Group IV: intrauterine deaths before 28 weeks was 14.3% of total perinatal deaths. One-tenth of the perinatal deaths was due to fetal malformation (9.9%). Another one-tenth of the cases were classified as potentially avoidable groups; i.e. group II: intrauterine death of growth retarded singletons ≥ 28 weeks (8.1%) and group VI: intrapartum deaths ≥ weeks (1.8%).
Conclusion: The Nordic-Baltic Perinatal Death Classification is useful in perinatal audit as it may facilitate comparison between populations and periods.
P-13-016 Breast cancer associated with pregnancy
M.G. Halaska1, M. Komar1, K. Suchova1, H. Stankusova2, G. Chod1, P. Strnad1, L. Rob1, M. Hrehorcak1, T. Binder1, M. Cihar1
12nd Medical Faculty, Charles University, Prague, Czech Republic; 2Dept. of Radiotherapy and Oncology, Prague, Czech Repub
Objective: Breast cancer in pregnancy is becoming to be an important issue. Current incidency is 3 in 100,000 cases of pregnancy. The aim of our study is to follow women in whome a breast cancer was diagnosed during pregnancy or within a one year after the delivery.
Methods: Between the year 2003 and 2006 eight women were referred to our department, three with the diagnosis of breast cancer during pregnancy, five within 1 year after the delivery. A management was selected individually with respect to the age of pregnancy, the stage of the disease and to the decision of the women. The average age of the diagnosis, management, way of delivery, fetal outcome, maternal outcome were recorded.
Results: The average pregnancy age was 34.5 weeks. The management depended on gestational week of the carcinoma diagnosed. By all our pregnant patients we induced lung maturity, by 1 patient we initiated therapy with segmentectomy, followed by chemotherapy during pregnancy. All of pregnant patients delivered by caesarean section even if we tried to induce spontaneous labour. All of children were healthy, one newborn the rectal atresy was diagnosed and operated. Two of our patients are dead, one is unknown, rest of the patients are alive.
Conclusions: Breast cancer diagnosed during pregnancy is a special and rare situation, which needs to be managed individually as there is a lack of information about such patients.
P-13-017 The diabetic nephroúathy and pregnancy (two case reports)
K. Andelova
The Institute for the Care for Mother and Child, Prague, Czech Republic
The pregnancy outcome of two pregnant patient with type 1 diabetes (T1 diabetes). Duration of diabetes was in both cases 15 and l7 years. The first patient was 3l years old and had her third pregnancy. Her metabolic compensation was bad (glycosylated Hb above 8%) and the first trimester results showed proteinuria 2 g/24 hours, hypertension and normal renal function. She was informed about all risk factors, she strictly refused the early termination of pregnancy. Progression of proteinuria and hypertension, deterioration of kidney function massive oedemas, the signs of cardiac failure and IUGR were the reason for termination of pregnancy in 31th week of pregnancy. The patient is 9 months after delivery on waiting list for kidney and pancreas transplantation. The second patient was 27 years old and had her first pregnancy. Her metabolic compensation was good for a long time (glycosylated hemoglobin up to 5%). Before the pregnancy she was treated for hypertension and had proteinuria 4 g/24 hours with serum creatinine 14 Oumol/l. For high risk the pregnancy wasn't recommended to her. She became pregnant and she refused to terminate pregnancy. Further deterioration of renal function with extreme proteinuria (t15 g/24 hours) and serious hypertension led to the decision to terminate the pregnancy in 20th week. Ultrasound investigation showed the fetus of normal size and without congenital malformations. The pregnancy was terminated with caesarean section. Two months after delivery she had fixed proteinuria 2 g/24 hours and mild hypertension.
Conclusions: 1) The importance for finding more exact criteria for pregnancy recommendation. 2) The wide information for the patient and her family about all risk. 3) The closed cooperation among all stages of healthcare staff in support for the patient. 4) The offer of prolonged psychological support after pregnancy. 5) The educational programmes for patients directed to importance of planning pregnancies.
P-013-018 Selective reduction of multiple pregnacy in singleton: Medical and moral questions
I. Tsiaousi, M. Theodora, N. Papantoniou, S. Mesogitis, A. Antsaklis
Fetal Medicine Unit, 1st Department of Obstetrics and Gynecology, University of Athens, ‘Alexandra’, Athens, Gre
Introduction: We are nowadays facing a new challenge as due to social and financial reasons many couples desire reduction of multifetal pregnancies to singleton. What is the aspect of medical professionals? Is there enough evidence to support the reduction of twins and higher order multiple pregnancies in singleton?
Material and Methods: We studied 428 multiple gestations which were subjected to fetal reduction (control group). Twenty-four of these were reduced in singleton due to parental request without any medical reasons (group A) and forty-three were reduced to singleton due to anomaly of one fetus (group B).
We studied the maternal age, the order of multiples prior and after the reduction, the chorionic, the gestational age at delivery and the perinatal mortality.
Results: The miscarriage rate in group A was 4.1%, and it was less than the miscarriage rate (7.8%) in control group. The mean gestational age at delivery was 36 week (34 + 3 weeks in the control group) and there was no intrauterine or neonatal death. In group B the miscarriage rate was 4.76% and the mean gestational age at delivery was 33 weeks.
Conclusions: The pregnancy outcome, perinatal morbidity and mortality in singleton pregnancies were better but the number of cases is limited.
Whether the fetal reduction based on social and financial motives is moral or not is a question which answer reflects our society's ethics and lies beyond the scope of this study.
P-13-019 Limb-body wall complex: A case report
M. Petros1, O. Simetka1, D. Matura1, R. Curik2, P. Koliba1
1Department of Obstetrics and Gynaecology, University Hospital Ostrava, Czech Republic, 2Pathology Department, University Hospital Ostrava, Czech Republic
Background: Limb-body wall complex (LBWC) is a rare polymalformative syndrome. The diagnosis is based on the presence of at least two out of three of the following abnormalities: exencephaly/encephalocele with facial clefts, thoraco- and/or abdominoschisis and limb defects. There are several hypotheses about the pathogenesis: early amnion rupture – amniotic-band theory, vascular disruption theory, and concept of early embryonic dysgenesis. Two distinct phenotypes are described: “placento-cranial” and “placento-abdominal”. Prenatal diagnosis is based on serum alpha-fetoprotein measurement and ultrasonographic examination.
Case report: We are presenting a 32-year-old healthy pregnant woman, gravida 2 parity 1, with uneventful personal and family history, and without abuse of alcohol, nicotine or drugs. In her 1st pregnancy, she delivered spontaneously a full-term healthy girl of body weight 2700 g, conceived after in vitro fertilization due to anovulatory cycles. Current bichorionic biamniotic twin pregnancy with the same partner begun again after in vitro fertilization. Fetus A was diagnosed as LBWC by ultrasound at 13 weeks. Fetus B had no obvious abnormalities. The woman was hospitalized due to imminent abortion at 7 and 16 weeks of gestation. The mother was referred to our department because of preterm premature rupture of membranes at 25 weeks of gestation. Termination of pregnancy was postponed due to immaturity of healthy fetus B. Cesarean section was indicated for prolonged rupture of membranes and transverse lie of fetus B and performed at 30 weeks of gestation. Pathological examination of fetus A revealed the following multiple congenital malformations. Craniofacial defects: occipital encephalocele, deformations of nose, upper lip, left eyelid, facial cleft, thoraco-facial and dorso-occipital amniotic band, and synostosis of coronary suture. Thoraco-abdominoschisis: ectopic heart, liver, spleen, and bowel. Urogenital malformations: bilateral atresia of ostium ureteris, bilateral megaureter and hydronephrosis. Limb defects: absence of left hand, syndactyly, oligodactyly, club feet, arthrogryposis, rotation defects, and talipomanus. Further abnormalities: severe scoliosis, anal atresia, hypoplastic lungs, umbilical cord measured 5 cm in length and contained two vessels. External genitals were male.
Results: Male fetus A with body weight 710 g died intrapartaly. The autopsy confirmed LBWC. Fetus B was a healthy female with body weight 1360 g.
Conclusions: Limb-body wall complex is a rare fetal abnormality. The association of LBWC with in vitro fertilization techniques deserves further evaluation. Early diagnosis is essential and can improve prenatal management.
P-14-001 Perinatal asphyxia in ancient Greece
M. Christodoulaki, S. Blazaki, A. Kanitsakis, M. Kalloniatou, G. Moshaki, A. Tsopelas, G. Tsoukalas, G. Daskalakis, I. Tsoukalas
General Hospital of Chania, Chania, Greece
Aim: To record the opinions of Hippocrates about the causes and treatment of perinatal asphyxia.
Method: Review of texts of Hippocrates.
Results: The most common causes for perinatal asphyxia, according to Hippocrates are the following:
The bleeding during the parturition (separation of placenta).
The circumvolution of umbilical cord around the neck or the shoulder of fetus, as a result of his movements in the uterus.
The prolapse of the hand or the umbilical cord of the fetus through the vagina of the mother. In that case the compression of umbilical cord causes anoxia in the fetus. The abnormal protrusion of fetus (breech presentation).
The abnormal position intrauterus (transversal or oblique).
Some other cases as the inertia of uterus (absence of birth pangs), the acute birth, the premature rupture of the placenta, oligoidramnio, premature fetus or multiple gestation and congenital malformations of the fetus.
As far as it concerns the treatment of perinatal asphyxia, Hippocrates recommended the cut of the umbilical cord when the newborn is breathing, is moving, is sneezing or crying. If the neonate does not have the previous characteristics in a few minutes will be dead. Also he is the first doctor who recommended the tracheal intubation for resuscitation.
Conclusion: Most of the causes of perinatal asphyxia mentioned by Hippocrates continue to be valid up to the present day. Hippocrates was the first to support that neonates with perinatal asphyxia have increased mortality.
P-14-002 FiO2 delivered in resuscitation may be underestimated
M. Thio1, A. Martin-Ancel2, M. Iriondo2, E. Salguero2, J. Aguayo2, E. Buron2, J.R. Fernandez-Lorenzo2, J. Vinzo2, I. Izquierdo2, M. Garcia del Rio2, L. Paisan2
1Agrupacio Sanitaria Sant Joan de Deu-Clinic, Esplugues-Barcelona, Spain; 2Working Group in Neonatal Resuscitation, Spanish Society of Neonatology, Esplugues-Barcelona, Spain
Overadministration of oxygen during neonatal resuscitation may be harmful. It is traditionally assumed that FiO2 delivered by 5 l/min oxygen flow through a bag without a reservoir is around 0.4. This delivery system is reviewed.
Objective: To analize the FiO2 delivered experimentally through a self-inflating bag without reservoir. To know which oxygen flow gives a FiO2 of 0.4.
Method: Different oxygen flows were given through the bag described (Ambu®), to either open air or a neonatal lung device. A sensor was used to analize FiO2 delivered when bagging for a targeted tidal volume of 10–15 ml, measured through a pneumotachograph.
Results: When oxygen flow was 5 l/min, minimum FiO2 achieved was 0.6 in one minute and it was sustained. Only when oxygen flow was reduced to 1 l/min, the FiO2 delivered was 0.4. See .
Conclusion: We may give more oxygen than expected when bagging and infant with an oxygen flow of 5 l/min. We need to accurately know the delivered FiO2 as well as the optimal concentration of oxygen, to improve resuscitation skills. Widespread use of FiO2 mixers is advisable.
P-14-003 ELBW infants' resuscitation workshop by spanish society of neonatology
M. Iriondo1, M. Thio2, E. Salguero2, J. Aguayo2, E. Buron2, A. Martin-Ancel2, J.R. Fernandez-Lorenzo2, J. Vinzo2, I. Izquierdo2, M. Garcia del Rio2, L. Paisan2
1Agrupacio Sanitaria Sant Joan de Deu-Clinic, Esplugues-Barcelona, Spain; 2Working Group in Neonatal Resuscitation, Spanish Society of Neonatology, Esplugues-Barcelona, Spain
International guidelines establish different recomecommendations in the resuscitation of ELBW infants. Structured courses in which usual situations in the delivery room are reproduced, seem a good method to achieve skills in neonatal resuscitation (NR).
Aims: To discuss the content of the Workshop in extremely low birth weight (ELBW) infants resuscitation developed in Spain by the Working Group in Neonatal Resuscitation.
Materials and Methodology: Contents of theoretical and practical lessons are: Lesson 1: General aspects (Limit of viability, ethical aspects and control of temperature). Lesson 2: Initial ventilation strategies (Use of oxygen, positive-pressure ventilation, CPAP, PEEP, and ventilation devices). Lesson 3: ELBW infant resuscitation algorithm. Lesson 4: Medications, intravascular accesses, initial stabilization and transport to NICU. The length of the workshop is of 5 hours Theoretical lessons are given by instructors in NR to the whole group of attendants. Practice training represent > 60% of the course length. Student/teacher rate is ≤8/1. Total capacity is 32 students (4 groups of 8 students).
Results: One workshop of ELBW infants resuscitation has made in the last National Congress of Perinatal Medicine (Las Palmas, November 2005) and 32 professionals got the level of training required and received a certificate. ELBW infant resuscitation algorithm is showed.
Conclusion: This methodology allows the students to improve their skills, self-confidence and knowledge's in ELBW infant resuscitation according to Internatinal Guidelines.
P-14-004 Neonatal resuscitation training program offered by the spanish society of neonatology
E. Buron1, M. Iriondo2, J. Aguayo2, M. Thio2, A. Martin-Ancel2, E. Salguero2, J.R. Fernandez-Lorenzo2, J. Vinzo2, I. Izquierdo2, M. Garcia del Rio2, L. Paisan2
1Hospital Clinico de Valladolid, Valladolid, Spain; 2Working Group in Neonatal Resuscitation, Spanish Society of Neonatology, Esplugues-Barcelona, Spain
Professionals who take care of newborns at the delivery room (DR) must learn to identify infants with problems at birth and must be trained to perform an adequate neonatal resuscitation (NR). Courses with mannequins in which usual situations in the DR are reproduced seem a good method to achieve skills in NR.
Aims: Our objective is to show a training program in neonatal resuscitation (NR) developed in Spain since 2001 by the Working Group in Neonatal Resuscitation of the Spanish Society of Neonatology and to evaluate its implementation in our country.
Materials and Methodology: The program is structured to achieve increasing levels of knowledge in NR: initial steps, complete resuscitation (special situations), post-resuscitation stabilization and neonatal transport. A special course to form instructors in NR has also been developed. The different courses available are:
Course for qualification in initial NR;
Course for qualification in complete NR;
Course for qualification in stabilization and neonatal transport;
Workshop in extremely low birth weight (ELBW) infants resuscitation (new);
NR instructor course.
A certificate is handed in after a theoretical and practical evaluation.
Results: 1120 professionals in Spain have attended the NR course (146 initial and 974 complete), 28 the stabilization and neonatal transport course, 32 the ELBW infants Resuscitation Workshop and 65 the NR instructor course.
Conclusion: Continuous training of professionals involved in newborn resuscitation is a major goal to decrease the neonatal morbidity and mortality. Likewise, training in NR allows to spread the NR International Guidelines in different areas or countries.
P-14-005 Comparative dosing tolerance, clinical response and outcomes between lucinactant (Surfaxin®) and poractant (Curosurf®) in very low birthweight infa
J. Mazela1, J. Hajdu2, G. Liu1
1Discovery Laboratories, Warrington, USA; 2Semmelweis Egyetem Hospital, Budapest, Hungary
Background: In 2002, Semmelweis Egyetem Hospital NICU participated in a masked, multicenter, randomized, controlled, non-inferiority trial comparing the safety and effectiveness of Surfaxin® (lucinactant) a novel, peptide-containing synthetic surfactant with porcine-derived Curosurf® (poractant alpha), in the prevention of Respiratory Distress Syndrome (RDS) in premature neonates of 24 to <29 weeks estimated GA (600–1250 g BW). Our centre enrolled 40 of the 252 (15.9%) patients in the trial. Initial treatment was administered within the first 30 minutes of life at a dose of either Surfaxin at 175 mg/kg birth weight (5.8 ml/kg using a 30 mg/ml concentration of Surfaxin) or Curosurf 175 mg/kg birth weight (2.2 ml/kg using an 80 mg/ml concentration of Curosurf). From 6–48 hours after birth, neonates were retreated for FIO2 ≥ .30 up to 2 doses of either Surfaxin (175 mg/kg) or Curosurf (100 mg/kg per label), at least 6 hours apart. The results from the main study (STAR) have recently been published (Sinha S, et al. Pediatrics, 2005;115).
Method: As the volumes of the comparators are different, we investigated dosing tolerance during surfactant administration, the clinical response, and the study's primary endpoint (Alive without BPB at 28 days). We looked at the occurrence of significant oxygen desaturation (<85%) and bradycardia (<100 BPM) up to 2 h post drug administration. All doses were administered with positive pressure ventilation. Investigators were masked to treatment assignment.
Results: See .
Conclusion: Despite differences in dosing volume, our clinical findings demonstrated that dosing tolerance was similar for both surfactants. Additionally, synthetic, peptide-based Surfaxin and animal-derived Curosurf provided a comparable clinical response.
P-14-006 The effect of surfactant replacement therapy in the nearterm neonates with severe pulmonary disease
S.L. Lee, B.Y. Lee, J.Y. Kim, C.S. Kim, T.C. Kwon
Dongsan Medical Center, Keimyung University, Daegu, South Korea
Objective: We performed this study to investigate the effect of surfactant replacement therapy (SRT) in nearterm neonates who were required mechanical ventilatory care due to meconium aspiration pneumonia (MAP) or other severe pulmonary disease (PD) (severe pneumonias, hyaline membrane disease, others).
Methods: 48 patients, gestational period ≥36 weeks, who were admitted in NICU of Dongsan Medical Center, Keimyung University between July 1999 and June 2004 were enrolled. They were divided into two groups, either MAP group (15 cases) or PD group (33 cases). The differences in the pre-SRT oxygenation index (OI), duration of ventilatory care and oxygen therapy, and outcome (complications and survival rate) were analyzed using statistical method. The mean doses of surfactant (modified bovine surfactant, Newfacten, Yuhan Co., Korea) was 120 mg/kg.
Results: Between the two groups, mean pre-SRT OI was higher in MAP group (21.8 ± 3.2) than that of PD group (18.3 ± 4.5) but statistically not significant (P > 0.1), mean duration (days) of ventilatory care (4.9 vs. 5.5) and oxygen therapy (9.4 vs. 8.8) were similar distributions. Early complications (PPHN, pneumothorax) and survival rate were lower in MAP group (20% vs. 27.3%, and 86.7% vs. 100%, respectively), but clinically not significant (P > 0.1). Within PD group, earlier SRT (given before 12 hours of life) revealed significantly lower early complication rate than later SRT (given after 12 hours of life) (14.3% vs. 50%, p < 0.05).
Conclusion: Our experience suggested that SRT seems to be an effective therapy in nearterm neonates with severe pulmonary disease, and earlier SRT tends to reduce complications in PD group than later therapy.
P-14-007 Prophylactic administration of surfactant (Insure)
Ch. Tsakalidis, P. Karagianni, H. Chatziioannidis, N. Nikolaidis
2nd NICU Aristotle University of Thessaloniki, “Papageorgiou” Hospital, Gre
Introduction: The effectiveness of surfactant (SF) administration in the prevention and treatment of Respiratory Distress Syndrome (RDS) of premature neonates has been revealed by numerous studies. During the recent years scientists have focused on the study of the SF administration time, comparing the prophylactic administration of SF (once the neonate is born) and the transportation to N-CPAP (INSURE – intubation – surfactant – extubation), with the SF administration after the appearance of RDS.
Objective: The aim of this study was the examination of the role of the prophylactic SF administration in the treatment of RDS, the morbidity and the survival of premature neonates.
Patients and Methods: 20 premature neonates with Gestational Age (GA) between 25 and 32 weeks, to which SF was administrated in less than 20 minutes since the birth (200 mg/kg, natural porcine SF, Curosurf®) were studied. A second SF dose was necessary in 5 neonates after 12 hours due to the need for mechanical ventilation. Originally the clinical and radiological arrangement of RDS, the release time from intubation, the development of oxygenation estimation indexes were assessed and later the maximum concentration and duration of administrated oxygen, the duration of hospitalization and the complications.
Results: The average SF administration time was 12 minutes (0–20) and the average time under mechanical ventilation for the neonates that survived (n = 19/20) was 12.35 ± 22.85 hours (0–96). After release from intubation, N-CPAP or Hood was implied to the neonates. The oxygenation estimation indexes were satisfying (OI ≤ 3, A-aDO2 <150 mmHg, a/APO2 ≥ 0.5) once SF was administrated and further progress was made during the development of the study. In 6 hours since the prophylactic administration, radiological picture of RDS was noticed only in 3 neonates and was 1st–2nd degree. The average duration of oxygen administration was 15.18 ± 7.47 days (0–65), FiO2 on 6, 12 and 24 hours was between 21–50% (average: 25%) and maximum PIP was 16mmH2O. One neonate remained oxygen dependant on 28th day of life, whereas no neonate needed respiratory support on 36th week after conception. No neonate showed severe intraventricular hemorrhage (3rd–4th degree), periventricular leukomalacia or retinopathy of prematurity. One neonate died within the 1st day, he was a 25 w GA, twin, with intra-uterine sepsis.
Conclusions: The study proves that the prophylactic SF administration, following INSURE to neonates with GA ≤ 32 weeks improves the morbidity and reduces the appearance of complications. The duration under mechanical ventilation is very small, the needs for administrated oxygen are very small, the appearance of CLD is reduced and it only appears as “new type”. These special impressive results did not permit for ethical reasons, the elaboration of a double-blind study, however, they do agree with the studies mentioned in the International Literature.
P-14-008 High frequency jet ventilation improves gas exchange in extremely premature infants with evolving bronchopulmonary dysplasia
R. Plavka, M. Dokoupilova, L. Pazderova, P. Kopecky, V. Sebron, M. Zapadlo
Division of Neonatology, Department of Obstetrics and Gynecology, General Faculty Hospital and 1st Faculty of Medicine of Charles University in Prague, Czech Repub
Background: Extremely preterm infants often develop chronic lung disease (CLD) characterized by heterogeneous aeration, poorly supported, floppy airways and air trapping. High-frequency jet ventilation (HFJV) with high end-expiratory pressure (optimal lung volume strategy, OLVS) may improve airway patency, lead to better gas distribution, improve gas exchange and facilitate extubation.
Objective: To explore, in a pilot trial, the effect of HFJV on oxygenation, ventilation, and ease of extubation in preterm infants with evolving CLD and refractory respiratory failure (RRF).
Design/Methods: From 9/02 to 10/04 twelve episodes of RRF developed in 10 ventilated extremely immature infants with evolving CLD (10 on conventional and 2 on high-frequency oscillation). Chorioamnionitis was confirmed in all infants, patent ductus arteriosus was ligated in 5 patients and Ureaplasma urealyticum was cultured from trachea in 4 patients. HFJV (Life Pulse, Bunnell Inc.) with OLVS was initiated when oxygenation index (OI) > 10 or tidal volume (Vt) ł 7 ml/kg were required to maintain PaCO2 < 60 mmHg. Inspiratory time 0.02 and frequency 310–420/min were set initially with adjustment of pressure amplitude to keep PaCO2 45–55 mmHg. Ventilatory stabilization and weaning from mechanical ventilation with extubation to nasal CPAP were the goals of this approach. Gas exchange data were analyzed by ANOVA for repeated measures.
Results: Ten patients on 11 occasions of RRF were extubated to nasal CPAP successfully in a median of 15.5 days. Nine of ten patients survived (1 died of Cantrell's Pentalogy), all required supplemental O2 at 36 weeks. PaCO2 fell within 1 hour after the initiation of HFJV and OI decreased by 24 hours. Both remained significantly lower until successful extubation (p < 0.02).
Conclusion: Compared to conventional ventilation or HFOV, HFJV used with OLVS improves gas exchange and may facilitate weaning from MV in extremely immature infants with evolving CLD. These encouraging pilot data support a larger clinical trial.
Study was supported by the grant of IGA MZ ČR No. 8360-2/200.
P-14-009 Evaluation of risk factors in development of bronchopulmonary dysplasia in premature infants
A. Minic, N. Prekajski, T. Macut, M. Rankovic, M. Lukavac, I. Pejcic
Institute for Neonatology, Belgrade, Yugoslavia
Objective: Evaluation the influence of risk factors in development BPD in LBWI (BW < 1500 g), gestation age < 32 weeks.
Methods: Retrospective study included 37 infants, all imposed to the same risk factors, with BPD group of 18 infants who develop the disease, and control group with no BPD development. We examed: birth weight, gestation age, Apgar score in 1st and 5th minute, Silverman score, prenatal, postnatal risk factor and influence of resuscitation at birth. Prenatal risk factors included: duration of membrane rupture and chorioamnionitis and among postnatal factors: severity of RDS, surfactant therapy, PDA, sepsis, duration of mechanical ventilation and oxygen requirement. Statistical analysis was performed by t test, Chi square test, and sensitivity (Sn) and specificity (Sp).
Results: Comparing BPD group and control group, there was significant difference in birth weight and Apgar score at 1st minute (p < 0.01), and in gestation age and Silverman score (p > 0.05). For duration of membrane rupture sensitivity was 55.56% and specificity was 72.22%, and for chorioamnionitis Sn. was 60% and Sp. was 72.2%. There is st.significant difference for resuscitation at birth in BPD group (Chi square 0.94, p < 0.05).In postnatal risk factors, we found for sepsis Sn. was 11.11%, Sp. 78.95%; for PDA Sn. was 40%, Sp. 76.47%, and for surfactant therapy Sn. was 5.56%, Sp. 84.21%. We found st. significant difference for severity of RDS in developing BPD (p < 0.01). Comparing two group there was st. significant difference for BPD group in duration of mechanical ventilation and oxygen requirement (p < 0.01).
Conclusions: We showed with this study a great influence of chorioamnionitis, resuscitation at birth, severity of RDS, duration of mechanical ventilation and oxygen dependency in development of bronhopulmonary dysplasia.
P-14-010 Multiple pneumothoraces due to persistent pulmonary emphysema in a newborn
S. Ilia, M. Giannakaki, M. Koropouli, M. Theodoraki, V. Valari, E. Chatzakis, K. Chandanos, M. Philipidis
Neonatal Intensive Care Unit, Venizelion Hospital, Heraclion, Greece
Pulmonary interstitial emphysema (PIE) is a result of over-distention and rupture of alveoli shortly after birth and leads to entrapment of air into the interstitial tissues, where oxygen absorption is poor. PIE is more frequent in premature infants that require mechanical ventilation for severe lung disease, since underdeveloped lungs lack adequate compliance. The gas entrapped into the interstitium can disappear spontaneously or decompress into proximate spaces causing pneumothorax, pneumomediastinum, pneumopericardium, or subcutaneous emphysema. PIE normally resolves within 2 weeks. In the current literature, the incidence of the disease appears declined following the introduction of the exogenous surfactant as well as the availability of high frequency oscillatory ventilation (HFOV) implementation.
We report a case of a baby girl born at 30 weeks gestation by caesarian section because of oligohydramnios and weighing 2 kg. She was admitted to our unit shortly after birth due to severe respiratory distress needed ventilator support. Upon intubation, she developed pneumothorax that required chest tube insertion. Since then and for the next 9 weeks she suffered approximately 18 episodes of spontaneous pneumothorax and pneumomediastinum. Chest X-ray and CT scan findings revealed linear and cyst-like radiolucencies throughout the lung parenchyma along with small bilateral multiple pneumothoraces, a characteristic radiological appearance for PIE. The neonate was initially treated with conventional ventilation which was swapped to HFOV after neonate's deterioration. At 10 weeks of age there was an abrupt dramatic improvement of neonate's condition and no identifiable factor was associated with this response. We report this case to highlight the repeated episodes of pneumothoraces and the uncommonly prolonged period of the route of PIE.
P-14-011 Acute respiratory distress in a term infant: An unusual etiology
G. Delanghe1, I. Van Herreweghe1, R. Ciardelli1, E. Chevalier1, F. Mergan2, M. Spehl3, D. Haumont1
1Neonatal Unit, St-Pierre University Hospital, Brussels, Belgium; 2Paediatric Surgery Department, St-Pierre University Hospital, Brussels, Belgium; 3Paediatric Radiology Department, St-Pierre University Hospital, Brussels, Belgium
We report a case of a term newborn male, with a perfectly normal physical examination the first day of life. On day three, he presented increasing severe respiratory distress, requiring admission on the neonatal ward. Clinical and radiological diagnosis of right-sided tension pneumothorax was made and immediately treated with needle aspiration, followed by chest tube drainage.
A first attempt at discontinuing suction 36 hours later was unsuccessful. The immediate recurrence of a massive air leak impaired three more attempts to discontinue suction. Because of a clinical and radiological suspicion of an underlying pathology a second chest tube was placed in an anterior position.
A pulmonary CT scan, made with the two chest tubes in place, confirmed the presence of a cystic lesion corresponding either to a cystic adenomatoid congenital lung malformation or a bronchial atresia, situated in the antero-inferior segment of the left upper lobe. At three weeks of life, the large cystic lesion was surgically removed, resulting in complete remission of the respiratory symptoms and normalisation of the chest X-ray.
Pathological examination confirmed the diagnosis of congenital cystic adenomatoid malformation type I.
Conclusion: The recurrence of a spontaneous pneumothorax in a term infant despite adequate treatment suggests underlying congenital lung malformation.
P-14-012 Selective ventilation for severe unilateral pulmonary emphysema in premature infant – case report 1
L. Pazderova, R. Plavka
Division of Neonatology, Department of Obstetrics and Gynecology, General Faculty Hospital and 1st Faculty of Medicine of Charles University in Prague, Czech Repub
revere right-sided pulmonary emphysema (PE) developed in 34-wks old premature infant during the mechanical ventilation and after surfactant administration for respiratory distress syndrome (RDS). The infant was admitted to our NICU in 2 weeks of life for progression of unilateral PE and respiratory failure during conventional ventilation. A severe, right-side, acquired PE was primarily treated by the ride sided positioning and extubation from PSV-VG mode to low PEEP nCPAP. This treatment strategy failed after 3 days and high frequency jet ventilation (HFJV) with low-lung volume strategy did not improve the lung pathology. Hemodynamics was gradually compromised by severe hyperinflation of the right lung with left mediastinal-shift and the collapse of the left lung developed. Selective HFJV of the left lung with right bronchus obstruction was started.
This treatment strategy was divided to four stages. First stage (5 days), a period of “the sleeping lung”: selective intubation of right main bronchus without any artificial ventilatory support and right side positioning caused partial right-sided lung atelectasis and selective left-sided lung ventilation by HFJV was started. Second stage (1 day), a period of alveolar stabilization: Right lung was lavaged carefully by continuous infusion of diluted surfactant (Curosurf 5 mg/ml) repeatedly. Third stage (1 day), a period of “the waking up lung”: Spontaneous gradual aeration of the right lung was started by the opening endotracheal tube, and removing the body from the right side to supine position. Fourth stage, the period of the right lung recruitment with gas redistribution: Extubation to nasal CPAP with spontaneous breathing developed in symmetrical gas distribution in both lungs. Infant was discharged in 51 days of life without supplemental oxygen or any therapy for bronchopulmonary dysplasia.
Conclusion: Selective lung ventilation with two-endotracheal tubes technique (right bronchial obstruction and left lung HFJV) can be successful method in the treatment of severe unilateral PE especially when respiratory and circulatory failure is evolving. Complete resolution of PE with the normal redistribution of ventilation in both lungs is documented.
Study was supported by the grant of IGA MZ ČR No. 8360-2/200.
P-14-013 Selective hfov for primary atelectasis of right hypoplastic lung caused by vascular anomaly – case report 2
J. Burkertova, R. Plavka
Division of Neonatology, Department of Obstetrics and Gynecology, General Faculty Hospital and 1st Faculty of Medicine of Charles University in Prague, Czech Repub
Objective: To demonstrate successful treatment of primary right atelectatic lung by selective ventilation with two tubes technique in premature infant with hypoplastic rigth lung caused by vascular anomaly.
A 34 week premature newborn with primary atelectasis of the right lung was admitted to NICU for severe respiratory distress in 10 hours of life. Surfactant was administered and conventional ventilation was started in the II.level of neonatal care unit. Because the non-aeration of right hemithorax syndrome on repeated X rays had been found the infant was transported to our NICU.
After admission high-frequency oscillatory ventilation (HFOV) was started. Oxygenation and ventilation improved however chest X-ray still showed homogenous opacity of the whole right hemithorax. Bronchoscopy excluded agenesis of the right lung or severe right bronchial hypoplasia. The selective right and left sided HFOV by two tubes technique (first was inserted into the right main bronchus and the second into the trachea) was started. The right side administration of surfactant (Curosurf 100mg/kg) was given to the right atelectatic lung before the lung recruitment. The initial huge difference between ventilatory parameters on both HFO ventilators gradually diminished and oxygenation had been improving during the next 6 hour period of stabilization. Nonselective HFOV was continued and infant was extubated to nasal CPAP without oxygen need in the 4th day of life and from 9th day of life had been breathing without any ventilatory support and transferred back with recommendation of further examinations to discover primary cause of right lung hypoplasia.
Angiography of the pulmonary vessels in 4 months discovered the primary cause of right lung hypoplasia: Anomalous drainage of the left upper pulmonary vein into the hypoplastic right upper pulmonary vein and abnormal flow distribution of the right lung and sequestration of the right middle and lower pulmonary lobe were found.
Conclusion: Selective HFOV by two tubes technique can be the successful method of respiratory failure treatment when the biophysical profiles of both lungs are dramatically different.
P-14-014 Scimitar syndrome in the newborn: A case report
A. Melo Bento1, R. Cancella de Abreu1, O. Nascimento1, A. Marques Valido1, M.A. Sampaio2, M.P. Magalhaes2, J. Oliveira Santos3
1Maternidade Alfredo da Costa, Lisbon, Portugal; 2H. Cruz Vermelha Portuguesa, Lisbon, Portugal; 3H.D. Estefania, Lisbon, Portugal
Scimitar Syndrome is a relatively rare congenital disorder characterized by an association of cardiopulmonary abnormalities. Neonates have severe symptoms with worse prognosis. Diagnostic procedures are important in predicting the outcome and defining the best approach. Surgical intervention is not always indicated.
We report a case of a female child that born at 38 weeks and conceived by IVF. Pregnancy was uneventful, except for positive vaginal culture for GBS. Ampicillin was given prior to c-section. At about six hours of life she developed tachypnea, respiratory distress and was noted to have a systolic murmur. The initial chest X-ray suggested pneumonia at the right upper lobe. The newborn was transferred to our NICU and was managed with nCPAP, oxygen and antibiotics. Her blood culture was negative and she was on room air on day four.
As she persisted with diminished breath sounds on the right upper hemithorax and worsened tachypnea, a CT scan was performed, which revealed an absent right upper lobe eventually associated with vascular malformation. To confirm and demonstrate other associated abnormalities she also underwent bronchoscopy, scintigraphy and 3D ultra-fast CT scan, which revealed an abnormal right sided pulmonary venous drainage in the inferior vena cava, dextroposition of the heart, hypoplastic right pulmonary artery, anomalous systemic arterial supply to the right inferior lobe and an absent or extreme hypoplasic right upper lobar bronchus. She was diagnosed has having Scimitar Syndrome and the therapeutic approach was decided to be conservative.
She progressively worsened, developing severe respiratory insufficiency, pulmonary hypertension and heart failure. Her blood culture tested positive for Staphylococcus epidermidis. She was ventilated, failed to respond to iNO and died at the age of 1.5 months. The autopsy confirmed the diagnosis.
P-14-015 Monitoring of pulmonary status by pulse oxymetry in newborn with respiratory distress
G. Radoja, F. Skokic
UKC Gyn./Ob. Clinik, Tuzla, Bosnia and Herzegovina
Newborn with respiratory distress requires permanent monitoring of pulmonary status. The pulse oximetry is one of the non invasive monitoring techniques.
Objective: To examine the reliability of assessment of pulmonary status in newborn with respiratory distress by pulse oxymetry.
Material and Methods: 46 newborns with respiratory distress received in neonatal intensive cara were studied in a prospective study over the period of one year. Respiratory function was estimated on the basis of physical findings, cest X-ray, pulse oxymetry and capillary blood gases by micromethod Astrup.
Results: In 32 cases oxygen saturation by pulse oxymeter readings was in the range of 89–95%, pH 7.27–7.34, pCO2 6.0–6.5 kPa, pO2 6.8–9.0 kPa. In 5 cases oxygen saturation was 95–100%, pH 7.30–7.35, pCO2 5.5–6.3 kPa, pO2 8.9–9.4 kPa. In 9 cases oxygen saturation was 82–88%, pH 7.21–7.30, pCO2 6.4–7.4 kPa, pO2 4.6–5.6 kPa.
Conclusion: Oxygen saturation by pulse oximeter readings in the range of 89–95% is in good correlation with blood gases and provide good evaluation and adequate monitoring of pulmonary status. Higher or lower saturation by pulse oxymeter readings has to be combined with blood gases.
P-14-016 Protein S-100 As tissue-marker of hypoxic-ischemic encephalopathy after perinatal asphyxia in lambs
E. Hilario1, F. Goni-de-Cerio1, F.J. Alvarez2, A. Alvarez1, A. Caballero1, M.C. Rey-Santano2, N. Martinez-Lopez1, V.E. Mielgo2, A. Valls-i-Soler1
1School of Medicine, University of Basque Country, Bizkaia, Spain; 2Reserach Unit, Hospital of Cruces, Bizkaia, Spain
Objective: To evaluate the efficacy of protein S-100 (a biochemical marker) as tissue-marker of the brain damage after hypoxic-ischemic encephalopathy.
Methods: Fetal lambs of 124–133 days of developmental age (term: 145 days) were randomly assigned to three different experimental groups: one control and two hypoxic-ischemic groups (0 and 3 hour after hypoxic-ischemic injury). Injury was induced by partial occlusion of umbilical blood flow during 60 minutes. Brains were fixed by perfusion with paraformaldehyde and divided in different cerebral regions: frontal and parietal cortex, basal nuclei and hippocampus Citation[1]. These regions were disgregated and immunolabelled for astroglial protein S-100. Samples were analyzed by flow citometry and immunolabelled cell percentage was evaluated. Data were compared by one-factor ANOVA (p < 0.05).
Results: Hypoxic-ischemic group sacrificed after injury (0 h) did not show differences of astroglial protein S-100 levels in comparison to control one in studied brain regions (Parietal cortex: 58.4 ± 16.9% vs. 62.4 ± 9.3%; Frontal cortex: 51.2 ±15.7% vs. 59.2 ± 15.7%; Hippocampus: 42.1 ± 13.5% vs. 58.4 ± 5.4%; Striatum: 48.4 ± 20.2% vs. 54.6 ± 9.4%, respectively). However, in all brain regions, the astroglial protein S-100 levels were significantly decreased in the group sacrificed after 3 hours of hypoxic-ischemic injury in comparison to both previous groups (Parietal cortex: 11.5 ± 7.2%; Frontal cortex: 8.4 ± 1.6%; Hippocampus: 8.2 ± 7.5%; Striatum: 10.7 ± 4.5%).
Conclusion: Our results suggest that tissue levels of protein S-100 determined as early as 3h after hypoxic ischemic injury, could be used as marker of asphyctic event.
This work has been supported by University of the Basque Country (grants 1/UPV075.327-E-14885/2002 and 9/UPV00077.327-15330-2003).
P-14-017 Heart rate variability transition between the first and third day of life
L. Kantor
Faculty of Medicine, Palacky University, Olomouc, Czech Republic
Introduction: Heart rate variability (HRV) is commonly analyzed in adults, but only limited data are available for newborns. The methodology of HRV measurements in newborns is complicated by their non compliance.
Objectives: To devise a way of standard measurement of HRV that can be used in healthy and sick newborns. To determine physiological values of HRV in healthy term newborns. To observe any evolving changes of HRV in the first three days of life.
Methods: We measured HRV in 94 healthy term newborns in the first and third day of life. The average gestation was 40 weeks and average birth weight 3620 g. The infants were in the 3rd behavioral state according to Prechtl. We used neonatal version of VarioCardio TF4 (Sima Media s.r.o.) which enabled us to measure the R-R intervals with sensitivity of 1 ms. Three intervals of 300 heart beats each were measured in supination, orthostais and in supination again. The changes in the duration of the R-R intervals were evaluated with fast Fourier transform. Nonparametric Mann-Whitney test and Kruskal-Wallis test were used for statistical comparison of the groups.
Results: We established simple and accurate method of measuring HRV in neonates. There were large inter individual differences of HRV in our cohort. We showed that in first and third day of life reactivity of the autonomic system during the orthostatic maneuver is not significant. However there is a definite maturing of the autonomic system during the first three days of life. The HRV was higher in boys compared to girls in all measurements. The differences were more pronounced in the third day of life than in the first day.
P-14-018 Increased urine nitrite levels in newborns under phototherapy
I. Kilic, I. Cakaloz, S. Demir, G. Can
Pamukkale University, Faculty of Medicine, Denizli, Turkey
Objective: Nitric oxide (NO) is a potent endogenous vasodilator and is involved in cytotoxicity, neurotransmission, and immunological defense mechanisms. The aim of this study was to investigate the levels of urinary nitrite levels prior to phototherapy, during 24 hours phototherapy, and after discontinuation of treatment.
Methods: Term neonates with hyperbilirubinemia requiring phototherapy were included in the study. Urinary nitrite levels were measured before and after being on phototherapy for 6, 12, 24 hours and at the 4th hour after discontinuation of treatment by a Griess reagement. Heart rate values did not show significant changes during phototherapy.
Results: Twenty-five term newborns (mean gestational ages were 38.2 ± 0.7 weeks; mean birth weights were 3273 ± 415 g; postnatal age 4.6 ± 1.6 days) were included in the study. Urinary NO levels measured after 6 hours of phototherapy were significantly higher (33.0 ± 20.0 μmol/mmol creatinine) than the levels measured before phototherapy (26.7 ± 18.3 μmol/mmol creatinine; p < 0.05). The increase continued during the therapy. Urinary nitrite level was 58.3 ± 78.3 μmol/mmol creatinine at four after the phototherapy. Although urinary nitrite levels decreased at the 4th hour after the phototherapy, the decrease was not significant (p > 0.05). Mean heart rate values did not show significant changes during the phototherapy.
Conclusion: We have demonstrated that urinary nitrite excretion is significantly elevated in term infant during phototherapy. In conclusion, we suggest that circulatory functions should be carefully evaluated in preterm, septic or ill newborns during phototherapy.
P-14-019 Recording and evaluation of one year's data in recently established neonatal department
A. Charitou1, K. Maniati1, K. Souga1, E. Kolovou1, K. Tsantila1, E. Papadimitriou1, A. Gounaris2, M. Scouroliakou1
1Maternity Clinic Lito, Athens, Greece; 2University of Thessaly, Larisa, Greece
Objective: The present study aimed at reporting our experience on the use of newly developed software in order to evaluate the quality and efficiency of our standards of practice.
Methods: We developed a user friendly software in which we entered the following data for each neonate admitted in the neonatal department of LITO Maternity Hospital from 1/4/04 until 31/3/05: demographics, antenatal history, birth events, medical problems during hospitalization, length of stay, outcome on discharge and total cost of hospitalization. Statistical analysis of the above data was then performed.
Results: All users reported that data entry was quick and easy. Even personnel with minimal experience on the use of computers reported no difficulties in data entry.
During the study period there were 3846 births in the hospital and 499 neonates were admitted to the neonatal department. Bacterial infections occurred in 6% of all study babies. Intraventricular hemorrhage occurred in 4.3% and bronchopulmonary dysplasia in 14.3% of neonates with birth weight 1000–1500 g.
Perinatal mortality was 6.2% (stillbirths accounting for 4.1% e.g. 16 from 24 babies that died). Mean total hospitalization cost ranged from 310.4 ± 249.2 € for the neonates with birth weight > 2500 g admitted to level 1, to 6704.3 ± 4079.5 € for those with birth weight 1000–1500 g admitted to level 3.
Conclusions: The software helped to improve the accuracy and availability of information for our neonates. It has also helped to check the efficiency of our standards of practice. We conclude that the use of such software is especially useful for a neonatal department.
P-14-020 Convulsions in newborn infants–frequency and aetiology
M. Jonovic1, B. Miljkovic1, G. Jovanovic1, N. Stojanovic1, B. Jocic-Jakubi2, L. Dimitrijevic3, V. Antic1
1The Clinic for Gynecology and Obstetrition, Nis, Serbia; 2The Clinic for Mental Health and Child Neuropsychiatry, Nis, Serbia; 3The Clinic for Physical Medicine and Rehabilitation, Nis, Serbia
The neonatal convulsions are neurological disorders that can be identified as a dysfunction or important lesion of the central nervous system, associated with subsequent neurodevelopmental deficits. The frequency of convulsions in neonatal period is from 0.2 to 25%.
Objective: Examining the frequency and etiology of neonatal convulsions in morbidity of newborn infants.
Materials and Methods: We used a retrospective analysis of morbidity in newborn babies born in Clinic for Gynecology and Obstetrition in Nis, in the period 2002–2005. We analyzed: mother's health before and during the pregnancy, the way of completing delivery, Apgar score, biochemical analysis, clinical, neurological examine and neurosonographic examination.
Results: There were born 13299 babies during this period. We found convulsions in 41 babies (0.31%), of which there were 5 preterm. In most cases (53.7%) mothers suffered from acute and chronic disorders during or before the actual pregnancy.
The way of completing delivery: per vias naturalis-53.6%, SC-26.8%, VE-19.5%. Apgar score 0–3 was in 14.6%, 4–7 in 29.2% and the others had Apgar score 8–10. In 67.8% convulsions were present in male babies. The onset of convulsions in the first 24 hours of life was in the 31.7%, in the second day 21.9% and in the third 17.1%. Neurosonographic examination determined that 36.5% of children had intracranial hemorrhage, 9.8% periventricular leucomalation and 2.4% had cystic leucomalation. 7.3% of babies had infection and 17.1% metabolic disorders. One baby died.
Conclusion: Neonatal convulsions have an important role in morbidity of newborns. The most frequent cause of convulsions in our examination is intracranial hemorrhage and asphyxia.
P-14-021 Recovery of multiple brain abscesses caused by serratia marcescens in newborn age – case report
M. Fejes1, E. Borbas2, A. Papp3, Zs. Szekhelyi1, A. Szuts1
1PIC Borsod County Teaching Hosp., Miskolc, Hungary; 2Ped. Radiology Dept. County Teaching Hosp., Miskolc, Hungary; 3Neurosurg. Dept. County Teaching Hosp., Miskolc, Hungary
Objective: Multiple brain abscesses caused by Serratia marcescens is a rare disease in newborn infants. The lecture shows the development, case history and treatment of the disease.
Patient and Methods: A newborn baby boy presented polycythaemia and fever was admitted to the hospital in the first days of life. On the 11th day after admission convulsions occured and because of suspected intracranial abnormality or meningitis cranial CT was performed. On CT scans multiple abscesses were revealed and surgical therapy including drainage and ventricle shunt was done. During the treatment he had epileptic seizures frequently, but he became symptome free after the introduction of complex antiepileptic therapy. In one years age he was in a good physical condition but he has mild motoromental deficience.
Conclusion: Radiological imaging plays an important role in the diagnosis and the follow up of brain abscesses and also in the evaluation of its complications.
P-14-022 Leading perinatal and neonatal factors in relation to severe intraventricular haemorrhage in extremely low birth weight infants
P. Sanakova, Z. Stranak, J. Melichar, J. Kucera, P. Velebil, J. Feyereisl
Institute for the Care of Mother and Child, Prague, Czech Republic
Objectives: Intraventricular haemorrhage is severe complication of prematurity, and it is the main antecedent of cerebral palsy and neurodevelopmental delay in preterm infants. The purpose of our study was to evaluate the clinical factors associated with neonatal severe periventricular-intraventricular haemorrhage ≥ III. grade (PVH-IVH) in a cohort of extremely low birth weight infants and to establish different perinatal and neonatal risk factors.
Design: Prospective cohort study in tertiary perinatal centre.
Methods: Neonatal cranial ultrasound was performed in every neonate, using a standardized protocol for screening of cerebral damage. Select maternal and infant variables were abstracted from the medical records. 187 ELBW patients were enrolled to this analysis (median BW 790 g, median GA 26.5 wks) and followed up to discharge.
Results: Survival rate to discharge was 76%. Comparison of survival (S group) and non-survival patients (NS group) confirmed that PVH-IVH ≥ III. grade is one of the most common mortality factor (S: 5.3% vs. NS 50%, p < 0.0001). Analysis of perinatal/neonatal events acknowledged statistically significant differences in PVH-IVH group (A) and non PVH-IVH group (B) in: delivery in perinatal centre (A: 16% vs. B: 44%, p < 0.03), use of antenatal steroids (A: 7% vs. B: 37%, p < 0.0001), gestational age (A: 6% vs. B: 22%, p < 0.03), Apgar score at 5 and 10 minute (A: 6 resp. 7.1 vs. B: 7.3 resp. 7.9, p < 0.002, p < 0.0001), the severity of RDS (A: 3.4 vs. B: 1.9, p < 0.0001) and air-leak syndrome (A: 45% vs. B: 10%, p < 0.0005). In the other parameters no statistical differences were found.
Conclusions: The serious PVH-IVH is strongly associated with extremely low birth weight newborn mortality and morbidity. Potential reduction is available with restriction of preterm delivery, perinatal hypoxia and the respiratory distress severity and its complications. Delivery in tertiary perinatal centre is essential for decreasing severe PVH-IVH.
Supported by grant IGA MH CR NR/7841-3
P-15-001 Selecting neonates with congenital cytomegalovirus infection for ganciclovir therapy
K. Smets1, K. De Coen1, Ph. Jeannin2
1Ghent University Hospital, Gent, Belgium; 2Jan Palfijn Hospital, Gent, Belgium
Objective: To look for evidence based or scientific guidelines for selection of newborns with congenital cytomegalovirus infection that might benefit from treatment with ganciclovir.
Methods: Literature search involving the MEDLINE English-language database and the Cochrane Collaboration Library. Abstracts were reviewed to select pertinent articles dealing with ganciclovir therapy in neonates. References from selected articles as well as from reviews were screened for additional relevant articles.
Results: Eight case reports (15 patients in all), one descriptive uncontrolled study (9 patients), two randomized dose-comparative studies (54 patients in all) and one randomized controlled study (42 patients) were identified. Only the randomized controlled study showed a reduction of hearing deterioration in the treated group. Published predictors of hearing loss in congenitally CMV infected children should allow to identify candidates that might benefit from treatment. Asymptomatic children with higher CMV burden are more likely to have sensorineural hearing loss. In children with symptomatic congenital CMV infection, the presence of petechiae and intrauterine growth retardation are independently associated with the development of hearing loss.
Conclusions: Studies so far are promising, but of insufficient number to make evidence based recommendations about indications for treatment of congenital CMV. As such studies are very difficult to conduct, treatment of high risk infants may appear justified. There is literature data to help clinicians in selecting on a scientific basis a subgroup of infants that is at higher risk of hearing deterioration and therefore might benefit the most from ganciclovir therapy.
P-15-002 Neonatal necrotizing enterocolitis
R. Rudanovic, G. Markovic, D. Dakic, L. Globarevic, M. Rudanovic
Institute for Children Diseases, Podgorica, Yugoslavia
Background: Neonatal necrotizing enterocolitis (NEC) is acquired, severe disease of neonates. Incidence is 1–5% of all newborns hospitalized in neonatal Intensive Care Unit, with mortality rate 70%. Most of them are prematures. Etiology is still unknown, but hypoxia of intestinal tract is the main reason that leads to mucous and transmural necrosis of intestine. Risk factors for NEC include perinatal asphyxia, tromboembolism, polycytaemia, hypotension, imune system immaturity, milk allergy, IgA deficiency in adapted milk, direct invasion of germs (Clostridium perfrigens, E. coli, Klebsiella …). In premature children, symptoms appear in first two weeks (rarely two months). Termine newborns express symptoms during first day of life. In both of them, clinical manifestations always begin after first meal.
Case Presentation: We would like to present a male newborn, brought to our hospital in third day of life in very bad state: decreased level of conciousness, gray skin, dyspnoic, without spontaneous movements, weak reactivity. There is a small amount of pure content on nasogastric sonde. Thoracic cage appears short, because of extremely distended abdomen. This child is delivered at time by healthy mother. His birth weight is 4050 g, height 53 cm, AS 9/10. After two breast feedings, newborn gets high temperature, refuses meals, tahypnoic, tahycardic, abdomen extremely distended. We put him in isolete, on mechanic ventilation, took blood analysis, X-ray and US examinations and consulted child surgeon.
Conclusion: Necrotizing enterocolitis is still diagnostic and treatment challenge and problem.
P-15-003 Infection in preterm infants with nec – does it affect outcome?
M. Rankovic Janevski, N. Prekajski, A. Minic
Institute for Neonatology, Belgrade, Yugoslavia
Objective: To estimate the incidence of infection and it's impact on the outcome of preterm infants with necrotizing enterocolitis (NEC).
Method: Diagnosis of NEC was established by using Bell's modified classification. Risk factors for disease, morbidity structure and bacteriological findings were analysed, comparing to the primary outcome.
Results: NEC was diagnosed in 17 preterm infants, incidence 1.9%, divided in two groups: I (6) survivors and II (11) nonsurvivors. Values were expressed as range and mean ± SD. In I group body weight (BW) was 960–1700 g (1401 ± 293), gestational age (GA) 28–34 weeks (32 ± 2.6), Apgar score (AS) 2–4 (3.2 ± 0.9). In II group BW was 900–1600 g (1318 ± 267), GA 27–33 weeks (29.7 ± 1.4), AS 3–7 (4.5 ± 1.5), without differences between the groups. Risk factors: significant differences were found in the incidence of mechanical ventilation and thoracic drainage (p < 0.05), while incidence of umbilical catetherisation and gastric tube feeding showed no difference.
Morbidity structure: significant differences were found in the incidence of RDS and apnea (p < 0.05), and not for septicemia, asphyxia, anemia and DAP.
Bacteriological findings: blood, stool, and cerebrospinal fluid, tracheal aspirate and chest draine apex cultures showed no differences between the groups.
The incidence of positive cultures of the endotracheal tube apex was significantly higher in II group (p < 0.05), with Klebsiella Enterobacter most commonly identified.
Disscussion: Preterm infants in this study are VLBW, with perinatal asphyxia and high mortality rate. Nonsurvivors were all mechanically ventilated, and accompanying complications contributed to negative outcome.
Conclusion: This study did not confirm that systemic infection significantly affects the outcome of preterm babies with NEC. Risk factor analysis showed the impact of mechanical ventilation and accompanying infections.
P-15-004 Indoor air studies of fungi contamination at the neonatal departments in bialystok and kavala
C. Lukaszuk1, E. Krajewska-Kulak2, M. Szczepanski3, J. Szamatowicz4, H. Tsokantaridis5, A. Hatzopoulu6
1Department of General Nursing, Mycological Laboratory, Bialystok, Poland; 2Department of General Nursing, Mycological Laboratory, Bialystok, Poland; 3Department of Neonatology, Bialystok, Poland; 4Department of Neonatology, Bialystok, Poland; 5Department of Intensive Care Unit and Palliative Care, Kavala, Greece; 6Department of Intensive Care Unit and Palliative Care, Kavala, Greece
Background/Aims: The assessments of the indoor air and walls contamination of fungi at the different Neonatal Departments in Greece and Poland were made. The studies were carried out at the two Neonatal Departments in Kavala (Greece) and Białystok (Poland).
Methods: Materials for the tests were: the air samples (in front of the building and the selected rooms) and swabs from the walls. The air pollution was determined using SAS SUPER 100 (Pbi International). The microbial flora from walls was assessed using the Count-Tact applicator and the plate Count-Tact (BioMerieux). Fungi were identified using standard microbial procedures. Classification of isolated fungi was made with an accordance to the current procedures. Humidity and temperature were evaluated by a termohigrometer.
Results: The following fungal pathogens isolated from air were Candida albicans, Acremonium, Rhodotorula species, Penicillium species and Aspergillus species. Fungi type isolated from the walls of the tested departments were Candida albicans, Candida species, Penicillium species, Acremonium species, Aspergillus species, Epicoccum species, Rhodotorula species, and Cladosporium species.
Conclusions: The air and walls from the Neonatal Department in Kavala showed the higher number of fungi colonies compared with Białystok. The air of Neonatal Department in Kavala was characterized with larger variety of mycological flora. Significant differences in occurrence the mycological flora (in relation to the fungus type and its quantity) in dependence of the place isolation as well as location of the Department.
P-15-005 Systemic aspergillosis in the premature newborn – successful treatment by voriconazol and caspofungin in combination: case report
P. Svihovec, B. Zlatohlavkova, J. Burkertova, R. Plavka
Div. of Neonatology, Perinatological Centre of General Faculty Hospital, Charles University, Prague, Czech Republic
The case-report describes clinical course of the systemic aspergillosis in the premature newborn. This boy was borne in the 31st week of gestation (birth weight 1520 g). Mother's acute respiratory infection with progression into the serious absceding pleuropneumonia occurred just before the delivery.
Early neonatal period was complicated by serious RDS with pneumothorax with necessity of the transient chest drainage. RDS and pneumothorax resolved during the first 5 days of life. The clinical course was stable during the next 3 weeks. The clinical and laboratory signs of infection developed during the 4th week of life (elevation of the CRP, left shift in the white blood count, hepatosplenomegaly, hypotonia, enteral feeding intolerance and skin rash) with negative bacteriological examinations (blood culture, CSF, stool, urine), normal chest X-ray, and normal CT scan and ultrasound examination of the abdomen. Broad spectrum empiric antibiotic treatment (incl. fluconazol) lead only to partial, transient lowering of the inflammatory markers. Diagnosis of the systemic aspergillosis was suspected when the aspergillus antigen was positive in the blood and urine in the 6th week of life and confirmed by the positive mycological cultivation of the Aspergillus fumigatus in the urine sample and nasopharyngeal swab. (Mycological cultivations usually takes about 2–3 weeks.)
Intraveneous antimycotic treatment by the combination of the voriconazol (V-fend; Pfizer) and caspofungin (Cancidas; Merck) had been started when the aspergillus antigen was positive and lead to rapid resolution of the clinical signs of infection and normalization of the laboratory parameters. Three weeks intraveneous administration of voriconazol 5 mg/kg twice daily and caspofungin 1 mg/kg once daily) was followed by enteral course of the voriconazol monotherapy in the same dosage for the next 7 weeks. Mycological cultivation and aspergillus antigen examination were negative during the last week of the antimycotic treatment.
Conclusion: The combination of the voriconazol and caspofungin lead to the successful treatment of the systemic aspergillosis without serious adverse effects in this case. This antimycotic combination currently represents the effective therapeutic alternative, which could be reserved for severe mycotic infections in the neonatal period.
P-15-006 Voltage-gated calcium channels mediate hypoxic vasoconstriction in the human placenta
V. Jakoubek1, J. Bibova3, V. Hampl2
1Institute for the Care of Mother and Child, Prague, Czech Republic; 2Department of Physiology, Charles University in Prague, Second Medical School, Prague, Czech Republic; 3Cardiovascular Research Centre Prague, Prague, Czech Republic
Unlike all vascular beds with the exception of the pulmonary circulation, fetoplacental vessels respond to acute hypoxia with vasoconstriction. While this hypoxic fetoplacental vasoconstriction (HFPV) is considered essential in the pathogenesis of intrauterine growth retardation, its mechanism is largely unknown. Hypoxia inhibits potassium channels and thus causes depolarization in fetoplacental vascular smooth muscle. We propose that this hypoxia-induced depolarization leads to vasoconstriction by activating voltage-dependent calcium (Ca) channels and Ca influx. We compared HFPV between isolated perfused human cotyledons treated with an inhibitor of L-type channels, nifedipine, and preparations receiving only vehicle. While the solvent (diluted DMSO) had no inhibitory effect on HFPV, the hypoxic responses were completely abolished even by a relatively low dose of nifedipine (1 nM). We conclude that activation of L-type Ca channels is an essential part of HFPV. These data were already published in Placenta, 2005 Dec. 16.
— Cancelled
P-15-008 Neonatal outcome and related factors in pregnancies complicated with preeclampsia
B. Tekin, N. Tekin, E.C. Dinleyici, M.A. Aksit
Eskisehir Osmangazi University Medical Faculty, Eskisehir, Turkey
Objective: Hypertensive disorders of pregnancy are associated with increased risk of maternal-perinatal adverse outcome. The aim of the study was to determine the risk factors in predicting neonatal deaths of severe preeclamptic-eclamptic mothers at a tertiary university referral centre.
Methods: We analysed retrospectively all consecutive live-born infants of preeclamptic-eclamptic mothers from January 1, 2004 to December 31, 2005. This retrospective study covered 85 (26 term and 59 preterm) infants with a birth weight of 2009.9 ± 78.8 g and mean gestational age of 34.6 ± 0.35 weeks at delivery. A comparison was made between the surviving infants and death infants.
Results: Fourteen infants out of 85 were dead with a mean age of 11.9 ± 2.9 days(1–32 days). We found a significant difference in birth weight (1752 ± 202.5 vs. 2143.5 ± 84, p < 0.05), gestational age (31.8 ± 0.9 vs. 35.2 ± 0.3 p < 0.05), first minute Apgar (2.81 ± 0.76 vs. 6.02 ± 0.27 p < 0.001), and fifth minute Apgar score (5.18 ± 0.61 vs. 7.91 ± 0.19, p < 0.001 and base excess (−10.4 ± 1.8 vs. −6.7 ± 0.6, p < 0.05) between the two groups. Exitus time was correlated with first minute Apgar (r = 0.731, p < 0.05), and fifth minutes Apgar score (r = 0.656, p < 0.05) and serum AST levels (r = 0.672, p < 0.01). The newborn infants who died at early neonatal period had lower first minute Apgar score (1.33 ± 0.55 vs. 4.6 ± 1.1, p < 0.05) and higher serum AST levels (124.3 ± 19.5 vs. 50.1 ± 8.3, p < 0.05) than the infants who dead after 7 days of their lives.
Conclusion: Severe perinatal asphyxia is the major cause of deaths in infants of preeclamptic-eclamptic mothers in the early neonatal period. Early referrals to the tertiary centre will optimised the timing of deliveries and prevent further adverse effects of preeclampsia on fetus.
P-15-009 Low-dose doxapram infusion does not decrease cerebral blood flow in preterm infants
T. Yamazaki, H. Mizutani, M. Takeuchi, M. Kubota, M. Miyata
Fujita Health University School of Medicine, Kutsukake, Toyoake, Japan
Objective: The purpose of this study is to evaluate the effect of low-dose doxapram on cerebral blood flow in preterm infants using cerebral Doppler ultrasonography.
Methods: Eleven preterm infants with idiopathic apnea of prematurity unresponsive to aminophylline were included in the study. Doxapram was administered at a continuous infusion of 0.2 mg/kg/h. Their birth weights ranged from 830 g to 2504 g (median 1545 g), gestational ages from 25 to 35 weeks (median 31 weeks). Using Doppler ultrasonography, blood flow velocities and the resistance index (RI) and the pulsatility index (PI) were measured in the anterior cerebral artery. Measurements were performed at baseline, 30 minutes and 2 hours and 8 hours after the start of doxapram.
Results: There were no significant changes in maximal systolic blood flow velocity (Vmax), end-diastolic blood flow velocity (Vmin), resistance index and pulsatility index after the start of doxapram.
Conclusions: Doxapram is a respiratory stimulant used for the treatment of idiopathic apnea of prematurity, although it has been demonstrated that it can induce a transient decrease of cerebral blood flow after a 2.5 mg/kg body weight loading dose. From the results of our study, continuous infusion of low-dose doxapram did not reduce cerebral blood flow in preterm infants. In view of the cerebral blood perfusion, low-dose doxapram infusion may be a safety modality in treating idiopathic apnea of prematurity. Further studies including more infants would be necessary to draw any final conclusions.
P-15-010 Significance of cranial ultrasound in preterm infants at 40 weeks of postconceptional age for further development prognosis
E. Helwich, M. Rutkowska, K. Polak, Z. Kulakowska, M. Dzwonkowska
Institute of Mother and Child, Warsaw, Poland
Introduction: USG of brain done close to term (37–40 PCA) is believed to be an important parameter in the prognosis. A normal or slightly abnormal picture seems to indicate a positive prognosis for further development of VLBW infant.
Aim: To examine sensitivity of USG of VLBW infants performed at term (40 PCA) in predicting further development.
Material: 31 infants born ≤32 GA, treated in NICU between 1998 and 2001 and followed up to the corrected age of 2. All the infants were diagnosed with IVH grade 3 or 4 and/or PVL 2 or 3.
Method: USG was performed repeatedly for full assessment of evolution. USG at term was classified as normal, slightly abnormal (slightly enlarged ventricles, isolated PVL cavity) and abnormal (significant enlargement of ventricles, visible PVL).
Results: 6 infants with normal USG, 5 develop normally, 1 is doubtful. In the group of 10 infants with abnormal USG at 37–40 PCA, 7 were diagnosed with CP, 3 was assessed as doubtful. The greatest developmental differences were in the group of 15 infants with slightly abnormal USG. 9 of them developed normally, 4 was doubtful and in 2 cases was abnormal.
Conclusions: 1) Significantly distorted USG before discharge indicates bad prognosis for the child's development in most cases it was the result of IVH grade 4 and PVL grade 3. 2) Normalisation of USG in the weeks before discharge indicates no permanent lesion of CNS and is prognostic generally normal development on 2 years but they should be followed-up. 3) Stating the prognosis is most difficult among the children with slightly distorted USG and therefore it seems essential to add MRI exam. 4) Developmental prognosis in PVL grade 2 and IVH grade 4 with limited range may be positive.
P-15-011 Neurological examination of preterm infants at term age: Relation to gestational age
P. Karagianni, H. Chatziioannidis, M. Kyriakidu, C. Tsakalidis, G. Mitsiakos, M. Lithoxopoulou, N. Nikolaidis
2nd NICU Aristotle University of Thessaloniki, General Hospital “Papageorgiou”, Thessaloniki, Gre
Objective: The aim of this study was to establish: (1) the spectrum of neurologic findings at term age in preterm infants born between 26 and 36 weeks gestation (GA) who are considered healthy and without significant abnormality on cranial ultrasonograms. (2) If the findings in preterm infants differed, whether this was dependent on gestational age at birth, and (3) the differences in neurologic findings between preterm infants reaching at term age.
Methods: The Dubowitz neonatal neurologic examination was performed prospectively at term age in 31 low-risk preterm infants born between 26 and 36 weeks GA (2004–2005). Infants were subdivided in 2 groups according to their gestational age at birth. Group A consisted of 15 infants born between 26 and 31 weeks GA and group B consisted of 16 infants born between 32 and 36 GA. The categories of Tone, Tone Patterns and Reflexes were examined. Tone category consists of 10 items (posture, arm recoil, arm traction, leg recoil, leg traction, popliteal angle, head control 1, head control 2, head lag, ventral suspension). Tone Patterns Category consists of 5 items (flexor tone 1, flexor tone 2, leg extensor tone, neck extensor tone/sitting and, increased extensor tone/horizontal). Reflexes category consists of 5 items (suck/gag, palmar grasp, plantar grasp, placing, Moro reflex). The form consists of numbered columns, between 3 and 5 for each item. Each item was scored from the column 1,2,3,4 or 5 in which it fell. If an item fell between 2 columns, it was given the appropriate half score between the columns.
Results: The range of the scores was similar in the two gestational age groups for 4 of the 19 items assessing Tone, Tone Patterns and Reflexes. For the other 15 items the range of scores differed between the two groups. The median scores in the two groups, however, were similar for 18 of the 19 items. No statistical difference was found in the scores between the two groups (pNS, Mann Whitney U test).
Conclusions: The distribution of scores provides useful guidelines when a preterm infant is examined at term. The range of the scores was different between the two groups. The fact that the median scores were similar into 95% of the items examined shows that the effects of gestational age at birth were small. Therefore, it is suggested that there were no difference in neurological assessment between the two gestational groups of the preterm infants reaching at term.
P-15-012 Follow-up of extremely preterm infants (less than 25 weeks gestational age)
M.C. Cespedes, A. Fabregas, A. Linde, J. Perapoch, A. Fina
Department of Neonatology, Vall d'Hebron Hospital, Barcelona, Spain
Objectives: To study the morbidity of extremely low gestational age (GA) infants (under 25 weeks gestational age). Follow-up at 12 months of corrected age.
Methods: We included all the surviving children of less than 25 weeks GA discharged from a single hospital since the 1st of June of 1998. All the infants were evaluated at the corrected age of at least 12 months: 45 preterm infants (14 = GA 24 weeks, 31 = GA 25 weeks). Median birthweight was 690g (range 420–1100 g).
Results: Motor development: Normal 50% = GA 24 weeks, and 78.6% = GA 25 weeks; mild motor delay 33% = GA 24 weeks, and 14.2% = GA 25 weeks; cerebral palsy 16% = GA 24 weeks (2 children: 1 diplegia, and 1 spastic tetraplegia, both severe), and 7.1% = GA 25 weeks (2 children: 1 moderate and 1 severe).
Cognitive development: Normal 25% = GA 24 weeks, and 64.2% = GA 25 weeks; mild delay 50% = GA 24 weeks, and 28.5% = GA 25 weeks; moderate to severe delay 25% = GA 24 weeks, and 7.1% = GA 25 weeks.
Visual development: Normal vision 41.6% = GA 24 weeks, and 64.2% = GA 25 weeks; mild affection 41.6% = GA 24 weeks, and 32.1% = GA 25 weeks; severe affection 16.6% = GA 24 weeks, and 3.6% = GA 25 weeks.
Global impairment: GA 24 weeks: 0% free of disabilities, 58.3% mild sequelae, 16.6% moderate sequelae, and 25% severe sequelae. GA 25 weeks: 32.1% free, 53.6% mild, 7.1% moderate, and 7.1% severe sequelae.
Five children lost in follow-up (11%).
Conclusions: We conclude that our newborns at the limits of viability have a high risk of disabilities, although in most cases this is a mild impairment. Later childhood follow-up assessment is needed to evaluate the effects of extreme prematurity.
P-15-013 Hyperkaliemia and neonatal bartter syndrome: An unusual association
G. Romera1, C. Puente1, M. Riaza1, M. Espino2, L. Sanchez de Leon1
1Madrid-Monteprincipe Hospital, Madrid, Spain; 2Fundacion Hospital de Alcorcon, Madrid, Spain
Neonatal Bartter syndrome represents an unusual cause of pediatric tubulopathy. All disease variants follow autosomal recessive inheritance, and recently their genetical basis have been described. Grouped by the common definition of hereditary hypokaliemic tubulopathies, they are clinically characterized by the presence of renal hyponatremia, metabolic hypokaliemic alkalosis, hypochloremia and normotensive hyperrreninemic hyperaldosteronism, as well as for an increased renal wasting of sodium, chloride, potassium and calcium with nephrocalcinosis and a severe polyuria. The neonatal Bartter variant is frequently associated to the antecedents of polyhydramnios and premature delivery. As ethiopatogenic basis it's described an increased production of prostaglandin E2 that led to a disruption of chloride resorption in the ascending limb of the loop of Henle and a subsequent stimulation to the renin-aldosterone axis. In their treatment an appropriate fluid and ionic replacement according to the losses are highlighted as well as indomethacin use to reduce polyuria.
A case of neonatal onset is presented, with the polyhydramnios and prematurity obstetrics complications. In addition to the previously described clinical and analytic findings, an initial hyperkaliemia is highlighted, an uncommon finding but already reported and that it may induce to an erroneus diagnostic.
P-15-014 Two cases of rare metabolic errors in newborn infants: Congenital lactic acidosis: Alkaptonuria
A. Popescu1, T. Miculescu2, R. Nimigean1
1Department of Neonatology, “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania; 2Saint Agnes Hospital, Maryland, USA
Objective: We present two cases of newborn infants with rare metabolic errors (congenital lactic acidosis and alkaptonuria) in order to highlight the problems related to diagnosis and treatment.
Methods: The clinical and biochemical evaluation of the two newborns was used.
Results: The first case was a male infant, born on term, 2.750 g, Apgar score 9. Immediately after birth he presented polypnea, inter- and subcostal indrawing, grunt, restlessness, generalized hypotony and diminished reflexes. Biochemical examinations revealed metabolic acidosis, hyperammonemia, pyruvic acid = 1.78 mg/dl, elevated L/P ratio, normal blood sugar and ketonemia levels. The mass s Spectrometry confirmed catastrophic discharge of alpha-ketoglutarate. The infant was diagnosed with congenital lactic acidosis due to Pyruvate Carboxylase Deficiency Type B. In spite of being administered high doses of Na-bicarbonate, the newborn died at 11 days.
The second case was a female infant, the first-born to a woman who had three previous spontaneous miscarriages. The pregnancy was carried to term through treatment until the seventh month. The only clinical manifestation was the brown staining of diapers in contact with urine. The infant was diagnosed with alkaptonuria using high performance liquid chromatography which revealed high discharges of homogentisic acid in urine.
Conclusions: In the first case, the prognosis was poor due to the absence of efficient therapeutic means. In the second case, the vital prognosis was good, but there was the risk that ochronosis develop in the future. In both cases there was the risk of transmitting the disease to other descendents. Parents must be aware of this risk.
P-15-015 The results of surgically repaired congenital GIT malformations
T. Matejek1, Z. Kokstein1, J. Koudelka2, M. Kralova2
1Teaching Hospital, NICU, Hradec Kralove, Czech Republic; 2Teaching Hospital, Pediatric Surgery, Hradec Kralove, Czech Republic
We report on survival and mortality rate of surgically repaired intestinal atresia, intestinal stenosis, bowel malrotation and abdominal wall defects in tertiary perinatological center Hradec Kralove in years 1998–2005.
The results are comparable with those of other centers. We found zero mortality in newborn infants with isolated intestinal atresia (20 neonates) or intestinal stenosis (5 neonates) and in bowel malrotation (3 neonates). One from 13 newborn infants operated on for anal atresia died, but severe associated malformations were diagnosed (VACTER syndrome). Mortality of surgically repaired abdominal wall defects was also low. One death from 9 neonates operated on for gastroschisis and one death of 6 neonates operated on for omphalocele. Prematurity does not elevate mortality risk.
P-15-016 Ophthalmological neonatal diseases in ancient Greece and byzantine times
M. Christodoulaki, P. Theoulakis, A. Kanitsakis, G. Tsoukalas, G. Moschaki, D. Athanasopoulos, E. Xidaki, A. Kotta, I. Tsoukalas
General Hospital of Chania, Chania, Greece
Introduction: From the ancient times already Greeks worshiped several so called “ophthalmic” gods, such as Apollo, Athena, Poseidon and Aesculapius. The ophthalmic sufferings are being healed by three women Saints: Saint Kallistheni, Saint Makrina and Saint Paraskevi. Of great interest is the degree of knowledge ancient and byzantine physicians had in the field of Ophthalmology.
Aim: The inquest of the point of view ancient physicians had regarding ophthalmological diseases of the neonatal age.
Material/Method: Indexing of the works of ancient and Byzantine authors.
Results: The ancient physicians were aware of several anatomical elements of the human eye, attempted to interpret vision's function while knowing little of the physiology of the eye and instructed patients on everyday ophthalmic hygiene. They discovered neonates could be born with congenital blindness. They were also aware: a) of the danger of eye infection during labour and recommended chemoprophylaxis, b) of the existence of ophthalmia neonatorum which they healed with the use of medications originated from the plant and animal kingdom as well as with chemical drugs in various pharmaceutical forms (collyriums, ointments, powders etc). They believed in the existence of a direct correlation between ophthalmia and climatic conditions, c) of strabismus, d) of hypertelorism, e) of mydriasis and mysis, f) of anisocoria, a condition considered to be a bad prognostic factor, g) of subconjuctival haemorrhage (hyposphagma). h) Finally, they proceeded in a variety of operations and/or cauteries with the use of specific instruments.
Conclusion: The point of view ancient Greek physicians had regarding neonatal ophthalmological problems, based principally on observation but also on research, are not far away from our current knowledge.
P-15-017 Retinopathy of prematurity in low birth weight infants – six years of experience
E. Papamichael
Neonatal Intensive Care Unit, Archbishop Makarios III Hospital, Nicosia, Cyprus
Objective: Research evidence shows that low birth weight, early gestational age and the length of oxygen therapy are the major risk factors for ROP. The purpose of this study was to analyse ROP risk factors and ROP frequency in VLBW infants.
Methods: A retrospective analysis study of 563 VLBW (700–1500 g) infants born between 1999–2005 at the N.I.C.U. at Arch. Makarios III hospital was performed. A data base was constructed of all valid data extracted from the medical records. Chronic lung disease (CLD) was defined as oxygen requirement for more than 28 postnatal days. A low mean airway pressure (MAP) was used to maintain PaCO2 in the high normal range. A routine u/s brain was performed during the first week of life and repeated oftenly. Daily glucose intake was adjusted to maintain glucose levels of <130 mg/dl. The results of detailed ophthalmologic exams were available for each neonate.
Results: 157 neonates (27.88%) were diagnosed with ROP. ROP neonates were of lower gestational age and birth weight that neonates without ROP. ROP neonates required longer oxygen supplementation (CLD) than NON ROP: 157 (100%) vs. 95 (23.3%) (p < 0.0001); 19 (12.5%) ROP neonates were diagnosed with IVH in comparison to 20 (5%) in the NON ROP group (p < 0.0001). ROP frequency in neonates <1500 g was 27.88% for all stages (1–5) ROP stage 3–5 was 2.48%. Therapeutic procedure was done in all neonates (14) with ROP stage ≥ 3. 13 had photocoagulation and 1 cryotherapy. 3 of the neonates with photocoagulation died due the other cases.
Conclusion: Conservative respiratory therapy, low mean airway pressure, well controlled hyperglycemia, low incidence of IVH and CLD resulted in a low incidence and mild ROP in VLBW neonates at our institution.
P-15-018 Newborn hearing screening in a neonatal intensive care population
Th. Papadouri, E. Papamichael, Ch. Karaoli, A. Aspris, A. Hadjidemetriou
Arch. Makarios III Hospital, Nicosia, Cyprus
Objective: This prospective study reports on the prevalence and incidence of hearing impairment and associated risk factors for hearing disorders in a neonatal intensive care unit (NICU) population in Cyprus.
Methods: From March 2003 until December 2005 a hearing screening program was performed in 1369 neonates using the method of transitory evoked otoacoustic emissions (TEOAE). On those infants who failed the initial testing twice follow up testing was performed by using the brainstem evoked response audiometry (BERA).
Results: Of 1369 neonates who where admitted in NICU, 551 (40%) had additional risk factors for hearing loss as defined by the Joint Committee on Infant Hearing. 1169 infants successfully passed the initial hearing screening. Of the remaining 200 neonates, 124 tested false-positive (9%), 18 were lost to follow up and 52 are expected to be tested again. Hearing impairment of about 30 dB was confirmed in 3 children bilaterally and in 3 children unilaterally.
Conclusions: Hearing screening of our high-risk neonates revealed hearing disorders in 0.4% of infants, suggesting good quality perinatal care in this population. Significant risk factors for hearing loss in our population were low birth weight <1500 g, perinatal anoxia and prolonged mechanical ventilation. The method of TEOAE used as a hearing screening test has a sensitivity of 100% and a specifity of 91%.
P-15-019 The effects of neonatal dexamethasone and methylprednisolone on rat growth and neurodevelopment
I. Kilic, E. Dagdeviren, E. Kaya
Pamukkale University, Faculty of Medicine, Denizli, Turkey
Objective: Dexamethasone is commonly used to reduce the morbidity of chronic lung disease in premature infants. In this study, our aim is to evaluate the effects of same efficient dose of tapering dose of neonatal dexamethasone and methylprednisolone on rat growth and neurodevelopment.
Methods: The pups were randomly separated into three treatment groups on PD (postnatal day) 3. Group 1: dexamethasone group (n: 12) (received 0.5 mg/kg on PD 3, 0.25 mg/kg on PD 4, 0.125 mg/kg on PD 5, 0.05 mg/kg on PD 6 subcutaneously), Group 2: methylprednisolone group (n: 12) (received 2.6 mg/kg on PD 3, 1.3 mg/kg on PD 4, 0.650 mg/kg on PD 5, 0.325 mg/kg on PD 6), Group 3: control groups (n: 12) (normal saline injected). Weight was recorded on PD 3–6, 8, 14, and 22, length was recorded on PD 3, 7, 14, 21 for each group. Neurological responses and physical development were tested on PD 7, 14, 21.
Results: On PD 4–6, 8, 14, 22, the pups' weights of the dexamethasone and methylprednisolone groups were lower than those of the control group but the pups' weights in the dexamethasone group were the lowest (p < 0.05). The lengths of the pups of the dexamethasone group were significantly lower than those of the methylprednisolone group on PD 14 and 21. Dexamethasone treated animals exhibited a reduced total neurological score compared with the methylprednisolone and control groups on PD 7, 14, 21. Although methylprednisolone treated animals had lower total neurological score than that of the control group on PD 7 and PD 14 (p < 0.05), total neurological scores were not different in the methylprednisolone and control groups on PD 21.
Conclusion: Postnatal methylprednisolone treatment might be safer than dexamethasone treatment in newborns.
P-15-020 Administration of betamethasone before birth has no effect on the glomerular filtration rate at birth
K. Allegaert, V. Cossey, A. Debeer, R. Devlieger, C. Vanhole, H. Devlieger
Division of Mother and Child, University Hospital, Leuven, Belgium
Introduction: Dimitrou et al. recently reported on the impact of prenatal steroids on insensible water loss and on urine output Citation[1]. However, diuresis, glomerular filtration rate and tubular function all are different aspects of renal function. We therefore evaluated whether antenatal steroid administration had any impact on glomerular filtration rate (GFR) hereby using amikacin clearance at birth as marker of GFR Citation[2].
Methods: Clinical characteristics and amikacin pharmacokinetics were retrospectively collected in a cohort of preterm infants (n = 264, <31 weeks GA, day 1, on respiratory support, 1/1/2000–1/12/2005). Pharmacokinetics were calculated assuming a one-compartment model with instantaneous input and first order output in every individual neonate and were based on amikacin blood samples collected for therapeutic drug monitoring of amikacin collected before and following second administration. Results reported by median and range or incidence. Mann Whitney U test was used to compare amikacin clearance in infants either or not co-treated with betamethasone before birth (yes/no).
Results: In this cohort (mean birth weight 1077 (SD 337) g, median GA 28 (SD1.7) weeks), median amikacin clearance was 0.47 (0.09–2.33 ml/kg/min). 207/264 were treated with betamethasone before birth, but there was no significant difference in amikacin clearance (0.48, range 0.09–2.33 vs. 0.44, range 0.16–1.33 ml/kg/min, p = 0.15) between both groups.
Conclusions: In contrast to the impact on diuresis and fluid balance, prenatal steroid administration had no effect on the GFR at birth when amikacin clearance was used as marker of GFR.
P-15-021 Are neonatal outcomes influenced by the interval between exposure to betamethasone and delivery in very premature neonates?
J. Pauleta1, C. Rodrigues1, N. Clode1, C. Cifuentes2, A. Graca2
1Dept. of Obstetrics and Gynecology, Santa Maria University Hospital, Lisbon, Portugal; 2Dept. of Pediatrics, Santa Maria University Hospital, Lisbon, Portugal
Objective: The purpose of this study was to determine whether the interval between betamethasone administration and delivery influences neonatal outcomes in very premature neonates.
Methods: A retrospective chart review was performed of all deliveries between 24 and 31 weeks' gestation that occurred between January 2003 and September 2005 at our institution and in which at least one dose of betamethasone was administrated. The neonates were grouped in 3 groups: A – one dose administrated; B – complete course administrated ≤48 hours to delivery; C – complete course administrated >48 hours to delivery. Groups were reviewed concerning to incidence of respiratory distress syndrome (RDS), need of oxygen at 36 weeks and intraventricular haemorrhage (IVH). For statistical analyses (2, Fisher's exact test and multiple variance analysis (ANOVA) were used. Statistical significance was considered when p < 0.05.
Results: A total of 103 newborns were analysed. Forty-seven were multiples. Results are compared in .
Conclusion: Among very premature neonates the incidence of severe complications were apparently not associated nor to the existence of a complete course of betamethasone neither to the interval between the first administration and delivery.
P-15-022 The role of maternal L-Argi˙ni˙ne administration on skeletal muscles of newborn rats
B.A. Kilic1, C. Guven2, K. Kilinc3, I. Kilic1
1Pamukkale University, Faculty of Medicine, Denizli, Turkey; 2Ankara University, Faculty of Medicine, Ankara, Turkey; 3Hacettepe University, Faculty of Medicine, Ankara, Turkey
Objective: It has been presented by us that maternal NO inhibition by NG-nitro-L-Arginine (L-NNA) protects the newborns' skeletal muscles from hypoxic injury. However, it was also shown that the muscles were protected against ischemia-reperfusion injury by the precursor for the synthesis of NO, L-arginine (L-ARG). In this study; we aimed to investigate the role of maternal L-ARG administration in hypoxic skeletal muscle damage in newborns.
Methods: Four group of rats were used: control, hypoxic, L-ARG, and L-ARG + hypoxic groups. For the third and fourth groups, L-ARG was administered 100 mg/kg as a bolus intraperitoneally to the timed-pregnant rats on the last three days of pregnancy. Hypoxia was induced to newborn rats on the first day of life by breathing of a mixture of 8% oxygen and 92% nitrogen for 3 hours. All newborn rats were decapitated after the procedure of hypoxia and reoxygenation. The hind limb muscles were removed immediately.
Results: Lipid peroxidation levels in the muscles (TBARS nmol/g wet tissue) were 33.4 ± 2.3, 39.7 ± 3.4, 36.8 ± 2.7, and 35.6 ± 4.2 in control, hypoxic, L-ARG, and L-ARG +hypoxic groups respectively (p > 0.05). Hypoxic group has irregular muscle fibers with indefinite cell borders and smaller nuclei. L-ARG + hypoxic group was similar to control group histopathologically.
Conclusions: These data suggest that either maternal L-NNA or L-ARG administration acts as a protective agent in the pathogenesis of hypoxia-reoxygenation injuries of the skeletal muscle.
Midwives
FC-M-001 Associating obstetric interventions in labour with a cascade of interventions at birth
S. Tracy1, M. Tracy2, E. Sullivan1, Y.A. Wang1, D. Black1
1UNSW, Sydney, Australia; 2Nepean Hospital, Sydney, Australia
Objective: To determine the strength of the association between obstetric interventions in labour and operative intervention in birth amongst low risk women.
Design: A population based study.
Setting: Australia, 2000–2002.
Patients or Other Participants: Amongst all 753,859 women who gave birth in Australia during 2000–2002 there were 363,794 women who satisfied our low risk criteria: 20–34 years; no hypertension or diabetes; no gestational hypertension or gestational diabetes; live singleton cephalic-presenting infant of normal size born at term.
Intervention(s): Induction or augmentation of labour; epidural/caudal/spinal analgesia/anaesthesia.
Main Outcome Measure(s): Mode of birth: unassisted vaginal birth, instrumental birth or caesarean section after labour; stratified by parity, adjusted for maternal age, private health insurance status and Aboriginality.
Results: Amongst the 32.95% of primiparous low risk women who were offered an epidural and induction or augmentation during labour, 36.76% had an instrumental birth, and 33.51% had a caesarean section. Using multinomial logistic regression and after adjusting for maternal age, private health insurance status and Indigenous status, we found the odds of an instrumental birth were 8.34 times greater (AOR 8.34; 99% CI 7.93–8.76); and the odds of a caesarean section with labour were 52.30 times greater (AOR 52.30; 99% CI 47.67–57.38) than the odds of having either birth outcome where induction or augmentation and epidural had not been offered during labour. Amongst multiparous low risk women who had both an epidural and induction or augmentation in labour, the adjusted odds of an instrumental birth were 12.68 times greater (AOR 12.68; 99% CI 11.66–13.79); and the adjusted odds of a caesarean section with labour were 30.89 times greater (AOR 30.89; 99% CI 27.81–34.31) than the odds of these events when no interventions were offered in labour.
Conclusions: Induction and epidurals are associated with a significant cascade of operative interventions at birth. There is an urgent need for randomized clinical trial evidence of the extent of their implication in the rate of instrumental birth and rising caesarean section rates.
FC-M-002 Level of intrapartum intervention and midwives' intrapartum risk perception
M. Mead
University of Hertfordshire, Hatfield, UK
Objective: In the context of variations in the labour care of women suitable for midwifery led care, this study was undertaken to test the hypothesis that midwives working in higher intervention units would have a higher perception of risk for the labour of women suitable for midwifery led care than midwives working in lower intervention units.
Methods: A survey of UK midwives involved in intrapartum care in eleven maternity units, using standardised scenarios questionnaires, was used to investigate midwives' options for intrapartum interventions, their perceptions of intrapartum risk and the accuracy of these perceptions in the light of actual maternity outcomes.
Results: Midwives working in higher intervention units generally perceived intrapartum risks to be higher, but midwives generally underestimated the ability of women to progress normally and overestimated the advantages of technological interventions, in particular epidural analgesia.
Conclusions: Variations in intrapartum care cannot be solely explained by the characteristics of the women. The influence of the workplace culture plays a significant role in shaping midwives' perception of risk, but it seems even more likely that the medicalisation of childbirth has had an influence on midwives' appreciation of intrapartum risks.
Intervention rates for low risk births are often higher than recommended by research. The level of interventions varies across hospitals and higher rates are associated with higher perception of risk by midwives. Attention needs to be given to the influence the workplace plays in shaping midwives' perception of risk; and to the effect of organisational culture on intervention rates.
FC-M-003 Effects of breastfeeding on somatic complaints and SOC score of mothers
B. Borrmann, B. Schucking
Universitat Osnabruck, Osnabrueck, Germany
Objectives: The purpose of this study was to assess the short- and medium-term breastfeeding effects on somatic complaints of mothers and scores of their Sense of Coherence.
Methods: A prospective cohort study was performed with a base-line questionnaire at 1–5 days post partum, a follow-up questionnaire at 5–6 months, and a follow-up questionnaire at 18 months post partum. The sample consisted of 2 groups: the formula feeding group (n = 32) and the breastfeeding group (n = 98). For further analysis the breastfeeding group was divided into 3 subgroups: women who stopped breastfeeding within 5 months (n = 32), women who continued breastfeeding for more than 5 months but introduced complementary foods within this time (n = 39) and women who continued exclusive breastfeeding for more than 5 months (n = 27).
Results: Increase of somatic complaints within the first 5–6 months after delivery tended to be higher in the breastfeeding group. During the first 5 days after delivery 28.6% of the breastfeeding women reported sore nipples, at month 5–6 this proportion had raised to 34.8%. A large proportion (20.3%) of the breastfeeding women developed mastitis within 5 months after delivery. Women who continued breastfeeding and introduced complementary foods within 5–6 months post partum tended to have a worse subjective health status than the formula group and the two other breastfeeding groups. In the formula group the SOC-Score declined from 52.7 to 48.7. In the breastfeeding group the SOC-Score increased from 50.9 to 51.6. This indicates more problems with anxiety and depression in the formula group.
Conclusions: Besides wide spread health problems like exhaustion, haemorroids, painful perineum and backache, many breastfeeding women additionally have to deal with sore nipples and mastitis. On the other hand there is evidence that women can profit from breastfeeding in the sense of mastering a challenge, which is expressed in a higher SOC-Score comparing to formula feeding women.
FC-M-004 Out-of-Hospital birth in Germany
C.A. Loytved
University of Osnabrueck, Osnabruck, Germany
Aim: To describe the work of midwives in an out-of-hospital setting concerning pregnancy, birth and the post partum period and the outcome of mothers and their children.
Methods: In the descriptive study nearly 10,000 births are documented for the year 2004 in Germany. With the data given by 663 midwives we can show the outcome of the mother and the fetus depending on the risks in pregnancy and during birth. These data can be compared to the same data set in 2003.
Results: Although more and more risks have been documented for the pregnancy, the outcome for the children did not change. Of all births started out of hospital 91.1% of the newborn did not suffer from anything like transfer in a clinic, morbidity, reanimation or low Apgar score. 95% of all mothers had no uncomfort like transfer post partum or exceeded bleeding. Compared to former years risks have augmented but at the same time, the outcome further improved.
Conclusions: Data of out-of-hospital births document good quality of midwifery care. Concerning the documented risks for the pregnant women, the question rises, if the risk catalogues existing in Germany are valid to predict bad outcome.
FC-M-005 Can One-to-One midwifery care increase the normal birth rate?
P. Dorling1, J. Munro1, J. Freeman2, T. Oxley1
1Sheffield Teaching Hospitals NHS Trust, Sheffield, UK; 2Sheffield University, Sheffield, UK
Objective: Of 6000 women delivering in Sheffield annually approximately 4% are managed through the One-to-One midwifery scheme. In this model of care, each midwife has a defined caseload of women, providing continuity of care and carer throughout the antenatal, intrapartum and postnatal periods. This study investigated the effects of caseload midwifery on outcomes of labour and rates of breast-feeding in a non-selective population-based sample.
Methods: Between June 2002 and December 2004, 612 women had one-to-one midwifery care during pregnancy and the post-natal period compared to 14,332 controls receiving standard midwifery care. We conducted a retrospective analysis of patient records. Data were analysed using multiple regression techniques to adjust for confounders. The main outcome variables were mode of delivery, home birth rate, epidural rate, rate of breast-feeding on discharge.
Results: For the women receiving one-to-one care there was a higher rate of unassisted normal delivery (62.4% for standard care, 72.9% for one-to-one care; P < 0.01). Both elective and emergency caesarean section rates were lower for the women receiving one-to-one care (8.3% for standard care, 6.2% for one-to-one care; 14.3% for standard care, 10.3% for one-to-one care respectively). After adjusting for maternal age, parity, deprivation score and ethnic group there was evidence of a significant difference in the odds of an emergency section between the two groups, this being higher for women receiving standard care (odds ratio: 1.72, 95% CI 1.24 to 2.41). Additionally, the women in the one-to-one scheme had lower rates of epidural analgaesia, and higher rates of home birth and breastfeeding.
Conclusions: One-to-one midwifery offers real benefits for women during labour, with an increased likelihood of uncomplicated labour for the majority.
FC-M-006 Exploring a new concept of clinical midwifery care in Germany
N. Bauer, A. Kehrbach, F. Sayn-Wittgenstein
University of Applied Sciences, Faculty of Business Management and Social Sciences, Osnabrueck, Germany
Objectives: In Germany the majority of pregnant women give birth in a hospital. Less than 10% of all hospital births take place without any medical interventions. In 2003 the first midwife-led-care unit was set up in Germany to introduce a model of care that supports a birth process which is as low in disturbances and as resource-oriented as possible and in which very little or no medical interventions are needed. The major objectives of the study were to investigate what were the criteria of midwifery care from the point of view of those midwives who were employed in a hospital and to examine changes in midwifery care after the introduction of the midwife-led-care-unit.
Methods: The study was based on a qualitative design. Data were obtained using semi-structured interviews and focus groups discussions. A typical sample was obtained consisting of midwives of the study site (n = 12) who were working in a midwife-led-care-unit and of midwives of a comparison clinic without midwife-led-care-unit (n = 12). The first round of interviews took place in both clinics in spring 2004. The midwives in the midwife-led-care-unit were interviewed a second time one year later. Data were analyzed using content analysis.
Results: The study results underscore specific features of midwife-led-care which constitute a new concept of clinical midwifery care in Germany. Results relate to midwives' understanding of her competencies, origin of midwifery care, support and professional care concerning women's autonomy and self-control in the birth process among others. Aspects of health promotion as well as prevention were distinctively presented among midwives working in the midwife-led-care-unit.
FC-M-007 Prolonged labour – when and why? augmentation or prevention?
H. Kjaergaard1, A.K. Dykes2
1Juliane Marie Centre for Women and Children, Copenhagen University Hospital and Lund University, Copenhagen, Denmark; 2Lund University, Dept. of Health Sciences, Lund, Sweden
Background: Prolonged labour (dystocia) is usually treated by i.v. augmentation. The rate of this in primiparous is 41–59% Emergency caesarean section and vacuum extraction is seen almost four times more frequently among these. 60% of all caesarean deliveries in USA are related to dystocia.
Interventions with reference to dystocia may or may not be justified. We lack consistence in defining the length of normal labour and thus criteria for diagnosing dystocia. We need studies based upon longitudinal recording of labour and delivery, using validated measurement instruments and an operational definition of dystocia.
Design: A Danish prospective multi centre study on risk factors for dystocia is ongoing.
Overall aim: To identify risk factors associated with failure to progress in primiparous labour.
The study consists of 5 sub studies.
The hypotheses of the three quantitative studies focus on associations between failure to progress and:
Psychological factors;
Social and lifestyle factors;
Clinical and other factors during labour.
The aim of 2 substudies in a qualitative design: describe parents' and midwives' experience of deliveries with dystocia.
The workshop
Aim: To elucidate midwives' experiences of deliveries with failure to progress in primiparous, to discuss how failure to progress is defined, to discuss potential causes and risk factors for failure to progress, share experiences of potential prevention of dystocia.
Participants: The number of participants will depend on the interest and the facilities. The number should however not exceed 40–50 participants to make sure that everybody can benefit from the discussion.
Procedure: 45-min. introduction, 60 min. discussion in focusgroups. The introduction will focus on current scientific knowledge on the length of normal labour and risk factors for dystocia. The discussion will be introduced according to the aim of the workshop.
FC-M-008 Childbearing over 35 years: What implications for care?
M. Carolan
Victoria University, Melbourne, Australia
Older childbearing is an increasingly common trend in advanced industrial nations, and this trend has been steadily increasing for more than two decades. Older primiparae of today represent a new social phenomenon, with many women now mothering in the context of professional careers. These women often delay first parturition while in pursuit of educational or career opportunities.
Currently, much of the research literature relating to pregnancy in women >35 years focuses on medical risks of delayed childbearing, and within medical and nursing circles, there is a common perception of higher rates of maternal maladjustment and postnatal depression among this group of mothers.
In this study, a qualitative narrative approach has been utilized and a total of 22 first time mothers >35 have been interviewed over two junctures about their experiences of transition to motherhood. Consistent with expectations, high levels of anxiety were indeed reported in the early days of mothering, by this study's participants, particularly by the more professional women. However, despite a shaky start, these mothers ultimately proved themselves to be both resourceful and proactive, in terms of recruiting information to meet their needs, and in general, did not demonstrate the high levels of post-natal maladjustment or depression, commonly associated with this group.
The importance of this study is located in the opportunity it presents to develop an understanding of the experiences of maternity for contemporary older primiparae, and the identification of the specific needs of this group.
FC-M-011 Recruiting midwives for a multicentre cohort study
M.M. Gross1, C.H. Schwarz1, H. Hecker2
1Medical School Hannover, Department of Obstetrics, Gynaecology and Reproductive Medicine, Hannover, Germany; 2Medical School Hannover, Department of Biostatistics, Hannover, Germany
Background: Validity problems of cohort studies due to sample selection are widely recognized. A participation survey was conducted as part of a state-wide multicentre longitudinal study on processoriented care during the childbearing process (ProGeb-Study). The aim was to relate research attitudes of hospital based and independent midwives to their decision to participate in the ProGeb-Study.
Method: Irrespective of their participation status, all 96 hospital based midwifery teams, as well as independent midwives in Lower Saxony, Germany, were asked to complete a Likert scaled questionnaire.
Results: The overall response rate of all hospital based midwifery teams was 82.3% (n = 79). Participating units contributed with 48.1% (n = 38) and non participating units with 51.9% (n = 41). The group of independent midwives contributed with 17 survey forms. Midwives' opinions on research in general, and on the ProGeb-Study in particular, differed between the three groups. Eight of the ten Likert items showed significant results (Kruskal-Wallis; p < 0.05). In each case, the Cochran test revealed a trend from non-participating to participating centres and then on to independent participating midwives (p < 0.05). The independent participating midwives showed a significantly higher motivation to participate in the ProGeb-Study than hospital-based midwives in participating units. Participating midwives had fewer doubts about the practical impact of the study, considered the immense work-related writing demands less stressful. They could also deal with the high routine workload more easily than midwives in non-participating units could. Higher motivation was correlated with more interest in research on the birthing process.
Conclusion: Motivation is a major predictor for the participation of midwives in a multicentre cohort study. Unfavourable working conditions play a negative, but secondary role regarding participation.
FC-M-012 Prenatal midwifery care – possibilities and limits
B. Kosfeld
Pegasus – das Zentrum fur ganzheitliche Geburtshilfe, Fortbildungsakademie fur Hebammen e.V., Aachen, Germany
Telling a pregnant woman some procedure or medicine is necessary for the safety and health of her unborn baby, there is nothing she will say against it, she will offer no argument. The becoming mother is seldom aware that decisions are made over her pregnancy and she is rarely informed of the potential dangers to herself and her baby of each and every alteration, often so called preventive interferences or “improvements”, of the natural process.
The midwife is educated to believe, that normal pregnancy is loaded with unpredictable sensations. Accepting pregnancy and labour as a natural physiologic function is not a normal attitude any more. Medical equipment, originally designed for the detection of complications, is nowadays dominating the healthy pregnancy to get “accurate results”. Even so no drug has been proven not to affect the baby they are highly recommended without clear evidence data that indicates their necessaty. Even so every expert knows that drugs cross the placenta and that the fetus is physiologically and metabolically unprepared to cope with their pharmacological effects the prescription of drugs is normal in every pregnancy.
Prenatal midwifery care must be based on the knowledge that any interference can create a greater risk to the woman than the original problem it was intended to solve. Midwifes know, that pregnancy and birth is too important to be seen only as a medical process, but must create a reunion of mother and child. They look at medicine as an art and know, a healthy person never sees a doctor.
FC-M-013 We all have one aim
Z. Stromerova
Porodni dum U capa, o.p.s., Prague, Czech Republic
Objective: Mutual aim for all the care providers: safe care, healthy and content mothers, healthy and content newborns.
Methods: To reach the mentioned above aim the midwives and medical doctors may use different methods and practices. In some countries they argue and sometimes even fight. Medical doctors would often wish to command the midwives not realizing that midwifery profession is different profession from gynaecology. It is because midwives are expert in normal pregnancy and birth. They view a birth as a social event more than a critical health crises. They are supporting more than treating. They use their head, heart and hands more, than modern technology and drugs. They trust in wisdom of nature and midwifery knowledge.
Results: Although the medical doctors tend to look at midwifery work as not scientific, the midwives all over the world are still reaching the mutual aim pretty well. With little help of modern machines, but with empathetic, thoughtful heads, big hearts and caring hands.
Conclusion: There is more than one way that leads to the mutual aim. The more the professional groups will cooperate, the better results they would reach and the more content would the care providers and the clients be.
Keywords: Listening, understanding, respecting, open mind, attention, knowledge
FC-M-014 From fear to confidence
Z. Stromerova
Porodni dum U capa, o.p.s., Prague, Czech Republic
Objective: To become a knowledgeable, self-confident professional midwife, who is able to offer safe on her own responsibility, without medical supervision and without own fear.
Methods: Regarding the fact that the midwives in Czech Republic have been and still are educated mainly to work in the hospitals and under the supervision of medical doctors, it is no wonder, that they feel unsure to work independent, that very often they even fear their own profession. The only way to raise their self-confidence and loose fear is to get more knowledge about their own profession, about the roots of their own profession, about the course of natural birth. Traditional midwifery knowledge, which has almost died out in Czech Republic has to be transported from abroad. We organize course for midwives from practice, which focuses on social skills and complex community care provided by midwives.
Results: About 35 midwives have passed our course by now. They work or in community setting or in hospitals. They use and appreciate the gained knowledge in their daily work. They became more independent, more self-confident, better in protecting natural birth and less afraid of their own profession.
Conclusion: Lifelong education plays important role in life of every midwife. It is even more important in countries, where a specific part of midwifery education is missing or is very weak.
FC-M-015 Necessity of combining practice and theoretical learning in midwifery profession
B. Kosfeld
Pegasus – das Zentrum fur ganzheitliche Geburtshilfe, Fortbildungsakademie fur Hebammen e.V., Aachen, Germany
The midwifery education faces many problems nowadays. One major problem is the loss of experiencing normal unmedicalised pregnancy, birth and postnatal period in the educational setting – the hospital. The midwifery student is trained in the wrong enviroment. Being responsible for normal pregnancy, birth and the first postnatal year as a graduated midwife, there is hardly any knowledge in practice about these subjects after leaving school. This bad state of affairs leads to an identification problem in the midwife – what is her specific role, being no doctor, no nurse, no assistance? Filled with theory of “the normal way”, mixed by the practical experience of permanent danger in every situation around and during birth, the midwife is working between constant insecurity and fear until she finds “her” personal way to deal with all these contradictory information in her professional daily life, but the deep longing for the connecting of theory and practice in a sufficient way never ends. Looking at possible ways to fullfill this desire is the task.
FC-M-016 Midwives in primary care in Canada
B. Lynch
McMaster University, Hamilton, Ontario, Canada
In 1994 midwifery became a regulated health profession in Canada and midwives joined obstetricians and family physicians in providing maternity care in this country. Midwives are primary care providers for women through pregnancy and birth and we provide primary care to both the new mother and her infant for the first six weeks after birth. Midwives in Canada are regulated to attend women giving birth in hospital, in birthing centres and at home. However, we are currently facing an obstetric healthcare crisis in our country. Fewer medical students are choosing obstetrics as a specialty, and a large number of currently practicing obstetricians will be retiring in the next decade. Midwives are engaged in government reviews of the maternity care system. We are working together with physicians and nurses to explore collaborative primary care models in order to keep maternity care in local communities. As part of this process midwives are considering an expansion of our current scope of practice. This talk will review the Canadian model of midwifery and discuss the challenges facing the maternity care system in Canada today.
FC-M-017 Equality of access to midwifery care for the migrant population in Switzerland
P.V. Held
Swiss Federation of Midwives, Bern, Switzerland
Over 20% of the population in Switzerland are not Swiss. The health outcomes for this segment of the population are not as good as for the local population. There are many barriers to migrant families in accessing the health services, particularly also in the reproductive health sector. In 2002/2003 I undertook a postgraduate course in transcultural competencies in health care. The paper I then wrote looked at the ways in which the Swiss Federation of Midwives could initiate and participate in programmes to achieve equality of care for the migrant population of Switzerland and better access to midwifery care. The Swiss Federation of Midwives cooperated with IAMANEH (International Association for Maternal and Neonatal Health) and the Swiss Ministry of Health to initiate various activities which were coordinated by a national coordinating centre for reproductive health. I will give some short background information on the situation in Switzerland and report on the various activities undertaken.
FC-M-018 Screening of the compromised fetus: A randomised controlled trial of umbilical artery doppler ultrasound performed by midwives in the community
M. Spencer1, S. Shaw2, A. Barton3
1South Devon Healthcare NHS Trust, Torbay Hospital, Torquay, Devon, UK; 2School of Mathematics, University of Plymouth, Plymouth, UK; 3Penisula Research and Development Support Unit, Penisula Medical School, Plymouth, UK
Objective: The primary function of antenatal screening is the detection of fetal compromise in order that appropriate plan of care is implemented. In the UK this screening is largely conducted by midwives using well established abdominal examination and history taking techniques. Recently it has become possible to use Doppler scanning in the community to assess the umbilical artery blood flow. Monitoring blood flow could enable midwives to detect a fetus whose growth is compromised but is not standard practice. Our objective was therefore to assess the effectiveness of midwives using Doppler scanners in the community as a means to detect small for gestational age (SGA) babies.
Methods: This was a randomised controlled trial conducted by midwifery teams working in South Devon, UK. Women receiving antenatal care were randomised to receive Doppler ultrasound scanning as part of their antenatal care or conventional monitoring with no scan. A wide range of outcomes was monitored.
Results: 880 women were randomised to the two groups which were well balanced on prognostic factors. For most variables, including SGA babies and the earlier detection of SGA babies there was no difference between the groups. However, there was a statistically significantly smaller number of admissions to the special care baby unit (SCBU) among the babies born to the Doppler group. There was also a small non-significant tendency for fewer gestations of less than 37 weeks in the Doppler group.
Conclusion: The use of Doppler scanners by community midwives is feasible and easy and midwives performing umbilical artery Doppler appear to have the potential of reducing admissions to SCBU.
FC-M-019 Introduction to the midwifery-workshops in the XXth european congress of perinatal medicine
As the European Union Council Directive from as early as 1980 sets out the principles for the training of qualified midwives, we should see to that this directive and especially article 4 be implemented efficiently in the member states. This article states that midwives are at least entitled to take up and pursue activities such as family planning, monitoring the development of pregnancies, advise on necessary examinations in cases of pregnancies at risk, parenthood and childbirth preparation including advice on higiene and nutrition, assisting the mother during labour and monitoring the condition of the foetus, conducting spontaneous deliveries, recognizing signs of abnormality and taking necessary measures if a doctor is not available, examining the newborn baby, monitoring the mother in the postnatal period and advising her on intant care. Midwifery is a traditional highly respected profession in Europe. However, today the profession is threatened if not enough political commitment is found.
Pregnancy and birth are existentially important phases in life. Unfortunately, many phases of the female biography are medicalised as for example the pregnancy. Female health politics and midwives in particular have opposed a tendency to pathologize the female efficiently. More and more women want to experience pregnancy and childbirth as a natural process. Accordingly an increasing number of women wishes to give birth to their child without disturbance.
The change in the culture of midwivery care reflects different historical processes: sexual taboos, medical developments and ideologies, social restrictions as well as political situations. In the age of unlimited medical opportunities it is the midwife's task to support the woman, the child and the family together as a system. To ensure that pregnancies are wanted and deliveries are safe. Considering the confident relationship and the professional competence that characterize the midwifery work, one clearly realizes how significant and indispensable this profession is in the health system.
It is of special interest to exchange midwifery knowledge across the borders on an European level. Since one can observe often that worries and problems which arise in one's own country are shared by members of the profession in other countries. To collect and transport midwivery know-how numerous European and international contacts allow for a dynamic exchange of knowledge and abilities. We hope that in this meeting in this conference “XXth European Congress of Perinatal Medicine” we have plenty of possibilities to exchange the necessary knowledge.
As for example learn not to forget the anatomy and physiology in the work of midwives. Not to forget the necessary knowledge and practical part in our profession.
To explain the approach of education: how can midwives successfully continue their responsibilities by practicing the use of brain, heard and hands? In her daily experiences the midwife is confronted with problems of all kinds medical as well as social. Which pre-conditions have to be met by a midwife to grow into the profession of midwifery? Can the scientific and medical environment where the midwife usually learns lay the foundation for an overall approach towards obstetrics? How do modern midwives acknowledge their own identity? What kind of significance do science and academic titles bear? What is female work? In the time of this conference we should try to put all pieces together as the midwife nowadays has the problem how to develop the midwifery model of maternity care provision in the phase of pre-existing medical monopolize and all enveloping partnership models woman's skills, which are being lost because of lack of continuity in care.
The task is a pre-condition of the development of a professional of midwifery practice which knowledge has been obtained. Midwifery work up to now and which relevance appears for midwivery practice today. A new professional awareness can only be developed through personal commitment but that requires an investment in terms of time, money, energy and courage. The international comparison of health-care-system, in which midwifery-care is restricted to the delivery room or is of very low or no relevance at all, the extend of midwifery care stands in correlation to obstetric interventions.
We as midwives should develop holistic models of midwifery care ourselves and stop fullfilling only assistent work but keep the profession autonomous.
FC-M-020 The videofilm “Committed to midwifery”
R. Drejer
International Confederation of Midwives, Leeuwerikenlaan 10, Voorhout, The Netherlands
My name is Mrs Renske Drejer, I am a midwife in the Netherlands.
The videofilm I made is called “Committed to Midwifery”.
In a filmed filmed portrait midwives from Austria, Belgium, Croatia, Czech Republic, Germany, the Netherlands, Slovenia and Switserland, speak about their commitment to midwifery.
Although their jobs are in different settings, their spirit is the same as far as it is about the real commitment of the midwife in spite of differences in cultural, historical and political backround.
Being a member of the International Confederation of Midwives, I got the opportunity to meet and film these midwives. At the same time I do realise the importance of meeting midwives in the proper sense of the word in the international arena.
FC-M-021 Holistic midwifery education
V. Schmid
Scuola Elementale di Arte Ostetrica, Via Pier capponi 17, Florence, Italy
Midwive's education comes from the medical model of birth, but midwifery practice needs different tools. The school for continous education in Florence offers a new model and a new language for midwives, focused on salutogenesis (genesis of health), on physiology and neurophysiology, on scientific evidences and woman's evidences. In a student centred approach and trough active teaching and body experiencies the midwife teachers of the school help other midwives to find their strength and their knowledge back. The integration of scientific and empiric knowledge forms the art of midwifery. Midwives need strength and knowledge to break down with an old system of midwifery care and build up new services for women.
P-M-001 Sense of coherence and preterm births – a prospective study of hospitalized women with preterm labour
S. Roehl, B. Schuecking
University of Osnabrueck, Osnabrueck, Germany
Introduction and Question: Currently, 8% of births in Germany are Preterm Birth (PB) and the number is increasing. PB is a major health problem and a multifactorial process. Both medical and psychosocial conditions influence PB (internationally defined as birth before 37 weeks gestation).
35.5% of all German women with PB are diagnosed with preterm labour during their pregnancy, many of them are hospitalized. The sense of coherence (SOC) is a measurement of global orientation in live and might turn out to be an individual resource in the context of preterm birth.
This study addresses the following questions:
Is there a difference between health potential measured as SOC-scores of women with preterm birth and women with childbirth at term? Is there a correlation between the level of the SOC-score and the term of birth?
Design: The survey was conducted in 13 hospitals in three federal states of Germany. 203 pregnant women participated in this survey. All were in inpatient treatment because of preterm labour during pregnancy.
First data was collected during hospital treatment (t1). Further data was collected by means of telephonic interviews (mean value 18 weeks post partum (t2)).
The survey started in March 2003. The t1-survey was finished in October 2004. The survey included: time of medical treatment, diseases during pregnancy, socio-economic and demographic factors and occurrence of anxiety and depression.
Results: Women with preterm birth have prevalently a lower SOC-score. Distinctions indicate the mean value of the SOC-score (group with preterm birth = 47.07; group with childbirth at term = 49.59) in favour of women without preterm birth (t-test: ns. p = 0.059).
The logistic regression indicates a significant correlation between the SOC-score and the time of birth or the tendency towards preterm birth (r = 0.224; p = 0.015). This means: The higher the SOC-score, the higher the tendency towards childbirth at term.
P-M-002 The midwives' qualifications during the 2nd century P.C.
A. Kotta, E. Xidaki, M. Christodoulaki, G. Tsoukalas, E. Kourmoulis, I. Tsoukalas
General Hospital of Chania, Mournies, Chania, Greece
Aim: The study of midwives' qualifications during the 2nd century P.C.
Material/Method: Indexing of the book (Sorani Gynaeciorum Libri IV) by Soranus Ephesius (Obstetrician-Gynaecologist, 2nd century P.C.).
Results: According to Soranus, the midwife who would help during the labour had to be selected very carefully. She had to be psychologically, morally and physically gifted. She also had to be literate and have theoretical knowledge of her work. A midwife had to be characterized by wit, strong memory and diligence. She had to be decent since she was going to be trusted with the secrets of entire families. Her senses had to be in a good condition since she had to see and hear well when she was addressed questions. She had to be able to realise even with the sense of touch, be honest, healthy, calm and also sympathetic. A midwife had to be strong, stable, taciturn, not to be bribed, and not to believe in prejudices.
A proficient midwife is the one who achieves the goal of Medicine alone while an excellent midwife is the one who has not only practical skills but also theoretical knowledge and experience. She must be trained in all kinds of medical treatment. She should be able to give health instructions and observe the whole and the partial so that she will be in position to decide what the most effective treatment is. A midwife should also define the treatment in relation to the development of the illness and be able to justify thoroughly her selection of medicine. Soranus stresses that, according to the standards he sets, those midwives who are really excellent will realize that they have all the required qualifications while those who are new in this profession will find a model to follow. Moreover, when people are in need of a midwife, they will know which one is the best to send for.
Conclusions: Who can question the fact that the above mentioned properties reflect a midwife's qualifications in modern times too?
P-M-003 Influencing factors on health and well-being of obese women round childbirth
K. Makowsky, B. Schucking
University of Osnabrueck, Osnabrueck, Germany
Objectives: The prevalence of obesity has been rising continuously in the last decades and includes more and more children, adolescents and young adults (meanwhile 20.4% of people in industrialized countries are obese; WHO 2003). Therefore obesity is an increasing health problem in obstetrics as well. This study investigates selected personal and environmental factors which influence health and well-being of obese women during pregnancy, childbirth and child-bed.
Methods: Based on qualitative research methods (according to the methods developed by Witzel 1989 and Strauss & Corbin 1996), 10–12 obese women will be interviewed during childbed. First results will be validated and amplified by at least 30 standardized questionnaires (self-developed questionnaire about experience with pregnancy and child-birth, SOC-L9, WHO-5, FEV) following quantitative research methods. Furthermore 4–6 qualitative expert-interviews (Meuser & Nagel 1991) with experienced physicians and midwives will include fields of professional care practice as an example for environmental factors in addition.
Results: Literature shows that obesity is one of the most important risk-factors in obstetrics (Kautzky-Willer & Winzer 2002). Studies investigated several somatic complications influencing maternal-health during pregnancy, childbirth and child-bed. Furthermore social and psychological problems of living with obesity in general are described as well. Following the bio-psycho-social model, it is recommended apart from biological to integrate also psychological and social aspects in obstetrics.
Conclusions: The study focus' personal and environmental factors of obese woman round childbirth in relation to health and well-being. Thus it is expected to integrate biological, psychological and social consequences of obesity in pregnancy similarly. Moreover the outcomes can be used as starting points for evaluation of quality in obstetrical health care systems.
P-M-004 Institution of “Country delivery house St. Apolinair” – it's history and education of midwives
Z. Sibkova
General Faculty Hospital, Prague, Czech Republic
Objective: To show long history of midwifes' education in Bohemia especially in condition of the oldest and bigest delivery hospital house in Czech republic.
Methods: Review of literature and personal experiences.
Results: The history of formal education of midwifes and doctors start by 1783 in Czech and alemand language (Hynek Jan Ruth, Vlassky Hospital). This education has controled by Study order by 1804. The Delivery house St. Apolinair was founded in 1789. New building of this institution from famous architect Hlavka was opened in 1875. Maximally 4 months courses for midwifes were connected with Charles University. From 1891 it was divided and Scholl for midwifes start it's independent history as part of state education system. This school lost hospital department in 1922. From 1947 education was 2 years long and work on delivery room was a practice part of education. From 2004 the midwifes' education was shift from higher school to high school. Practice part for education continues in St. Apolinair.
Conclusion: Practice part of midwifes' education is historically joined with delivery house St. Apolinair. Length and forms of this education were changed but the most important part of it – practice skills – has roots in this institution for more than 200 years.
P-M-005 Obstetrical intervention rates and midwifery in Germany
C. Schwarz1, B. Schuecking2
1Institute of Social Medicine and Health Economics, University of Magdeburg, Magdeburg, Germany; 2University of Osnabrueck, Osnabrueck, Germany
Objective: Obstetrical intervention rates in Germany are among the highest of all European countries. Of the more than 700,000 women who give birth in Germany per annum 98.7% undergo births in hospital largely characterized by medical interventions.
Methods: 1) Retrospective secondary analysis of the Lower Saxony Perinatal Survey 1984–1999 containing more than 1 million births (70 000 births per year) with more than 150 items for every birth. 2) analysis of maternity care in the German health care system.
Results: 1) The statistical analysis demonstrates an increase in almost all obstetrical interventions over the time with a remarkable extend in the low risk group. Only very few women (6.7%) had no documented intervention. 2) The German health care system provides very good general conditions for midwives e.g. the German midwifery act (every birth has to be attended by a midwife), every midwife is allowed to practice as independent (self employed) midwife and is paid by the compulsory health insurance.
Conclusions: In spite of these favourable conditions specialist care is “normal” for both high risk and low risk pregnancies, the dominant care providers in Germany are obstetricians and in reality as care providers midwives play a marginal role. Under these circumstances it is difficult to “keep birth normal”.
P-M-006 Alternative approaches in midwifery
B. Finderle, S. Tomic, B. Lucic
Clinical Hospital Rijeka, Rijeka, Croatia
Objective: The purpose of this paper is to show alternative methods in midwifery practice at the Department of Obstetrics and Gynaecology, Clinical Hospital Rijeka.
Methods: We took into consideration all births on the chair and in water which have been performed since these methods were first introduced at our clinic. We also showed our experiences in application of gymnastics ball during the first stage of birth.
Results: The first birth in water took place on 25 February 2003 and there have been 275 such births since. The first birth on the chair was performed on 14 August 2005 and there have been 60 such births since, while the gymnastics ball has been used in our clinic since 17 July 2003.
Conclusions: All alternative methods that we have come to use more often in our Clinic proved to be extremely useful and effective for women, but also for the purpose of raising the midwifery in our country to a higher level because these methods give the midwives the opportunity to work and make the decisions independently. Alternative approaches to birth are a contribution to the humanization of the relation to women in birth, taking into consideration of their choice and to the positive experience of birth.
P-M-007 Doula in the context of health psychology
M. Holancova
Czech Doula's Association, Prague, Czech Republic
The paper draws on my bachelor's thesis “Experiencing labor with a doula” (FHS UK 2005, Health Psychology CP conducted by doc. Vaclav Brichacek, PhD).
It gives information about
Health psychology (holistic health, primary prevention, coping with stress, salutogenesis, social support, secure attachment etc.);
the perinatal period from psychological and psychosomatic point of view;
doula and her care in reflection of health psychology.
The empirical part of the thesis is formed by eight cases of primiparas and multiparas accompanied by a doula during birth. All the women consider the doula care as a great benefit.
A doula provides professional, nonmedical and continuous support at birth. She “mothers the mother” during pregnancy and the postpartum period as well. Doula care represents the continuity of childbirth support tradition.
Health psychology studies the impact of human behaviour on health. According to the WHO health definition, it considers health as a whole, with its physical, mental and social dimension. Health is not only the absence of disease, but also a feeling of well-being.
One of the main topics of this discipline is coping with stress. Among others, a doula helps the mother understand her current situation, releases her stress and pain by long-lasting support, comforting her, providing information, supporting her self-confidence etc.
From the health psychology point of view, doula care corresponds to promoting health in all of its dimensions (physical, mental and social). According to many international randomized studies, doula care at birth has a positive effect on its outcome. It contributes to primary prevention. No negative impact of doula care has been discovered.
Keywords: Doula, labor support, childbirth, health psychology, health
P-M-008 The impact of the environment on the birth physiology
E. Geisel
GfG German Association for Childbirth Education, Family Support and Women's Health, Germany
Is the birth process dependent of the environment? Unfamiliar clinical versus familiar comfortable environment.
Numerous studies show that, being alert and the use of stress management strategies for coping with unfamiliar situation trigger hormonal releases, more specifically the release of adrenalin. Adrenalin inhibits the release of the birth hormones. The synthesis of the birth hormones works at best under specific circumstances that will be explained.
A pre-requisite for keeping birth normal is to reduce the neo-cortical activity.