
Abstract
Stress and bullying create severe pressure on workplace health. Although the connection between quality management and health is beginning to be well established, the association to workplace stress and workplace bullying has not been previously studied. The purpose of the paper is to examine associations between quality management values, workplace health and workplace stress.
A questionnaire based on theory and previous research was constructed and delivered to a sample of Swedish secondary school teachers. The questionnaire included previously developed constructs of quality management values and workplace health. In addition, constructs measuring stress, demand, control and bullying were included. Correlation analyses and cluster analysis were carried out.
The findings confirm the connection between quality management and workplace health that previous research has identified. In addition, the results indicate that quality management can increase the level of control that the employees have over their work situation, thereby alleviating some of the effects of workplace stress. Furthermore, the results show an association between quality management and workplace bullying. Moreover, control but not demand was found to be related to workplace health. Four clusters of employees with different quality management, stress and health profiles were identified.
Introduction and purpose
Workplace health is problematic in the western world as well as globally and work-related health problems are estimated to result in an economic loss of 4–6 percent of most countries GDP (WHO, Citation2020). Despite advances in medical science, workplace health is not always as good as it ought to be. Increasing demands and down-sizing mean that fewer employees are expected to do more and more which contributes to stress and discontent (Brenner et al., Citation2014). A study on 21,000 European employees showed that 60% of all European employees have at least one health problem related to their work (Daubas-Letourneux & Thébaud-Mony, Citation2003). Stress is generally seen as a common contributor to this development.
In previous research, quality management has been shown to be related to workplace health (Bäckström et al., Citation2012; Lagrosen, Citation2006; Lagrosen et al., Citation2007; Lagrosen et al., Citation2010; Lagrosen et al., Citation2012). However, the associations between quality management and workplace stress have not yet been examined. Despite several searches in major databases, we have not been able to find any research study into this connection from any part of the world. Workplace bullying is another factor that contributes to workplace health problems as well as being a major work environment problem (Bowling & Beehr, Citation2006). Possible relationships between bullying in organisations and quality management are however also yet to be explored.
Consequently, the purpose of this paper is to examine associations between quality management values, workplace health and workplace stress. Workplace health in this case implies the employees’ mental and physical health situation.
The remainder of the paper is structured as follows. First, some theoretical contributions and previous research in the relevant areas, workplace health, stress, workplace bullying and quality management are briefly overviewed. Next, the methodology of the study is described. Subsequently, the findings are presented, elaborated and discussed. After that, some conclusions are drawn, and the implications for research and for practitioners are discussed. Finally, we conclude the paper by addressing the limitations and suggesting some avenues for further research.
Workplace health
Ill health at the workplace is a major social problem. In addition to affecting job performance it is, for instance, related to depression and work/family conflicts (Wang et al., Citation2010). In addition to costs for society and employers, it causes significant human suffering. In Sweden, after decreasing for some time, levels of sick-leave have increased again since 2011 and the total cost for the Swedish Social Insurance Agency was 40 billion SEK in 2019 (source: Statistics Sweden and the Swedish Social Insurance Agency). To this should be added the costs for employers and for the healthcare sector. The increasing levels of sick-leave may be an effect of decreased workplace health although sick-leave is influenced by many other factors such as unemployment levels, economic compensation etc. At the same time, there is a corresponding problem with presenteeism – that employees go to work even when they are ill.
Organisational (organisation, communication and management) or social (interaction with colleagues and managers) factors were the third most usual reason for work-related disease in Sweden in 2015 (The Swedish Work Environment Authority, Citation2016). For women, these factors accounted for 44% of the cases making them the most common cause. In addition, these cases increased by 83% between 2011 and 2015.
In response to these problems, workplace health programmes have become common, and research shows that they often have positive effects (Cancelliere et al., Citation2011). The scientific roots of health promotion can be found more in social and behavioural sciences than in medicine (Hanson, Citation2007). Health promotive interventions in organisations are usually of two different types:
Programmes which address the individual employees’ lifestyles with interventions aimed at e.g. smoking cessation, exercise, diet or stress management.
Organisational interventions targeting the organisational climate and the social work environment. For instance, this may concern how work is organised, the management style, how communication is taking place and the way in which people at the workplace interact with each other.
Research suggests that employers primarily focus on programmes intended to influence the individual employees’ lifestyles and less on organisational factors (Larsson, Citation2015) even though they are just as important as they impact workplace health (Arneson, Citation2006).
Stress
Stress is the most common cause of sick leave in Sweden (Source: The Swedish Social Insurance Agency), and stress is usually found in inappropriate organisational conditions. At the same time, work under good conditions can have a positive impact on our health. This may include support for health promotive activities, a health supporting work environment, including health activities in the business strategy and helping employees improving their lifestyle (Addley, Citation1999). Knowledge of how to create a health promotive work situation is thus valuable.
Studying work-related stress in organisations the Demand-Control-model (Karasek, Citation1979; Karasek & Theorell, Citation1990) is often used. This model depicts a broad spectrum of health-related work situations based on two factors:
Demands – the work-related difficulties that the employees need to cope with. This includes physical challenges as well as psycho-social aspects such as high workload, routine work, role conflicts and lacking leadership.
Control – the possibilities that the employee has to influence the demands. This concerns the opportunities to alter the work situation, to which extent the employees can use their competency as well as the options for competence development.
These factors combined give rise to four different work situations with related effects on health and well-being.
High-strain work is characterised by high demands and low control. This is the most critical combination. The psychological pressure in these cases often leads to fatigue, depression, anxiety and disease. Work on an industrial conveyor belt whose pace one cannot influence is a typical example of such a job. The result is often lack of satisfaction and high levels of sick-leave.
Passive work implies low demands and low control, which is sometimes seen in employments within cleaning, maintenance and security. In these occupations, employees seldom have the possibility to fully utilise their competency. The work is not challenging and therefore not satisfactory. The result may be low levels of motivation and morale.
Low-strain work results from the combination of low demands and high control and can be seen for instance in self-employed people in manual work. Since the strain is low, the risk for disease and health problems is less. However, possibilities for development are limited and thus the work often lacks stimulus.
Active work denotes those positions where both control and demand are high. These occupations are often challenging, interesting and stimulating. One example of this kind of work situation is the employments in academia. They imply less risk of health problems, but they still have their health challenges.
Social support is another aspect that profoundly influences the work situation and is thus often included or combined with the demand-control-model. Social support can protect against too demanding work situations and is consequently important for a well-functioning workplace. Social support is a subjective experience, and it only exists to the extent that the employees perceive it (House, Citation1981). Moreover, research has shown that the experienced level of social support is related to the incidence of cardiovascular disease and arteriosclerosis (Bernin, Citation2002).
Workplace bullying
Workplace bullying concerns repeated activities directed at someone for whom they are unwanted, relating to negative or aggressive psychological behaviour (Einarsen et al., Citation2011). Bullying at work has been found to be related to decreased well-being of individuals as well as organisations (Bowling & Beehr, Citation2006). Workplace bullying has also been shown to be clearly related to mental health problems, such as depression, and there are indications of associations to physical ailments for instance cardiovascular disease (Kivimäki et al., Citation2003). Moreover, victims of workplace bullying are themselves more likely to misbehave as a consequence of being bullied (Fida et al., Citation2018). Individual as well as environmental factors influence the occurrence of workplace bullying (Bowling & Beehr, Citation2006). Likewise, bullying often results from an interaction between antecedents such as power imbalances, motivating structures (e.g. internal competition) and triggering circumstances (e.g. changes in work group composition) (Salin, Citation2003). Autoethnography and cognitive adaptation in the form of meaning in life strategies (Pheko, Citation2018) and personal resilience (Jackson et al., Citation2007) have been found to be ways for the individual of coping with workplace bullying and reduce the vulnerability. Yet, the responsibility should really rest on the organisations and their leaders to avoid bullying taking place, and research has shown that ethical leadership by fostering justice at work can reduce the risk of workplace bullying across cultures (Ahmad, Citation2018).
Quality management and health
Quality management has gone from a focus on total quality management, TQM to a more mature emphasis on values, techniques and tools needed to build a quality culture (Dahlgaard-Park et al., Citation2013). Several authors hold the view that there are various levels of quality management (Dale, Citation1999; Dale & Lascelles, Citation1997; Lagrosen & Lagrosen, Citation2003). The levels are defined in slightly different ways. Our view is that three levels of increasing degree of profoundness can be distinguished (see ). The most superficial level contains numerous practical techniques and tools sometimes based on statistics. The second level consists of a number of more holistic models or systems (e.g. the award models and ISO 9000). The third level, which is most profound, is constituted of certain phenomena that different authors call values (Hardjono et al., Citation1997), principles (Dahlgaard et al., Citation1998), key elements (Dale, Citation1999) or cornerstones (Bergman & Klefsjö, Citation2010). They are deep-lying notions of how the organisation should function. Arguably, successful quality management requires these values (which we prefer to call them) to permeate the organisation and in fact they should be supported by even more fundamental core values such as trust and honesty (Dahlgaard-Park, Citation2012) (see ). The values that should be included vary among different authors. However, in our literature searches, we have found the following six to be most common.
Customer orientation
Leadership commitment
Participation of everybody
Business process focus.
Continuous improvements
Management by fact
Figure 1. The levels of quality management, QM.
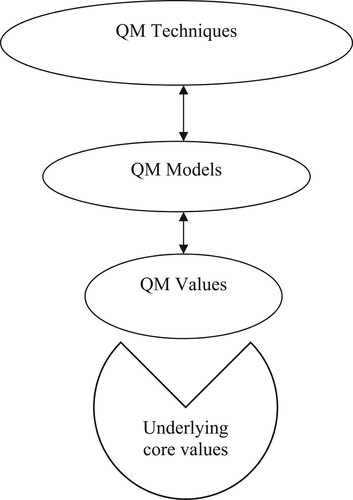
Research has shown that the values are effective for achieving well-functioning quality systems and performance in organisations of all types (Baird et al., Citation2011; Lagrosen & Lagrosen, Citation2005). Interestingly, a stream of research has identified associations between quality management and workplace health (Lagrosen, Citation2006). Particularly the values have been found to be connected with workplace health (Lagrosen et al., Citation2007) and mechanisms of this have been further explored (Lagrosen et al., Citation2010). The research shows that employees who experience that the values presented above are present in the organisation also have better self-reported health. Consequently, we will use the values in this study as a basis for examining the association quality management has with health, stress and bullying in the workplace.
Methodology
The study was directed towards upper secondary school teachers. The reason for this was that they are a large group of people with fairly uniform education, status and working conditions. There are also comprehensive official lists of the schools, which make it easy to reach the schools albeit not necessarily the teachers themselves. Thus, the research population included all upper secondary school teachers in Sweden. A web questionnaire was developed. The questionnaire contained several sections. One section measured the level to which the respondents felt that the quality management values were present in their schools. They contained constructs of the six values presented above consisting of three items each, as developed in previous research (e.g. Lagrosen & Lagrosen, Citation2014). The index regarding customer orientation had to be edited somewhat since the word customer is rarely used in schools. Instead, pupils are mentioned. In a similar fashion, workplace health was measured with an index consisting of three items that has been used in several previous studies and has proved to be reliable (Bäckström et al., Citation2012; Lagrosen et al., Citation2012; Lagrosen & Lagrosen, Citation2012). In addition, three-item indices were constructed for measuring the levels of demand and control. Moreover, as a control, we included a single item question about stress formulated ‘I often feel stressed at my work’. All these items were measured on a seven-level Likert type scale with the extremities ‘do not agree at all’ and ‘agree completely’. Finally, a question regarding bullying at their workplace was included.
From a list of all Swedish public upper secondary schools, 90 schools were randomly selected using the random number function in Excel. They were contacted via e-mail and asked to forward a link to the questionnaire to their teachers. A total of 311 responses were received. However, the number of employees of the schools is not available, which means that unfortunately the response rate is impossible to calculate. Please, see an elaborated discussion regarding the implications of this in the section ‘Limitations and suggestions for further research’ below. Of the respondents 183 identified as female, 127 as male and one as other. Regarding age, 23 respondents were younger than 20, 24 in their twenties, 62 in their thirties, 76 in their forties, 84 in their fifties and 42 in their sixties. In order to preserve maximum anonymity and since it was not related to the purpose no other demographic questions were asked.
The responses from the questionnaire were analysed with descriptive statistics, correlation analysis and cluster analysis.
Findings
The indices were examined with Cronbach’s alpha test for reliability. The descriptive data for the Likert type questions and indices are presented in .
Table 1. The descriptive statistics of the Likert scale indices and questions.
A Cronbach’s alpha score of .6 or more is generally considered to be reliable (Hair et al., Citation1998). Since all the indices exceed this level, we conclude that the reliability of the constructs is satisfactory.
As part of the purpose of the study was to check whether the quality management values were associated with workplace health, we calculated the associations between the quality management indices and the workplace health index. Moreover, the correlations between workplace health and the stress related indices demands and control as well as the single question regarding health, were measured. As a normal distribution of the variables could not be assumed Spearman’s Rho-test was used. The results are shown in .
Table 2. The correlation between workplace health and the quality management values and the stress variables.
As can be seen in the table, all the quality management values are highly significantly correlated with the health index. This confirms previous research findings that the quality management values are associated with better workplace health. The single question on stress was significantly, negatively correlated with workplace health while control had a significant positive relationship. On the other hand, the demands index was not related to workplace health in any significant way.
Next, we tested the associations between the stress-related factors, demands, control and feeling of stress, and the quality management values. The results are presented in .
Table 3. Correlation between the stress variables and the quality management values.
Here, the picture is somewhat more varied. All the quality management values are significantly correlated with control indicating that quality management increases the employees’ possibilities to handle the demands of work and control the work situation. The correlations are all rather high, over .5 all of them, which indicates that this is a prominent effect. Regarding demands, customer orientation and participation of everybody are significantly correlated, positively and negatively respectively, while the other values are not significantly correlated. This implies that customer orientation may make the work situation more demanding while participation of everybody has the opposite effect. However, the associations were fairly weak. Concerning the control question on stress, it is interesting to note that participation of everybody, process orientation and management by fact are negatively correlated with stress.
The responses to the question about bullying revealed that almost 88 percent of the respondents do not feel bullied at their workplace. However, about 11 percent occasionally experience bullying while less than 2 percent are often exposed to it. In order to examine whether the occurrence of bullying is related to the quality management values and to workplace health, we calculated Oneway ANOVA. The results are shown in .
Table 4. The associations between workplace bullying, quality management and workplace health.
Thus, we can see that bullying is related to lower workplace health, which highlights the importance of avoiding it. In this context, it is noteworthy that there are significant differences between those bullied and those not bullied in the mean value of all the quality management values. The difference between those bullied and those who are not is large for most values.
Finally, as we wanted to have a structured view of the participants, we carried out cluster analysis. K-means clustering (Hair et al., Citation1998) was chosen and several runs with different theoretically relevant numbers of clusters showed a solution with four clusters to be most informative. The results are presented in .
Table 5. The cluster analysis of the respondents.
The clusters were labelled and can be described as following:
The problematics. This group has the worst situation. Their health is not good and they do not experience the quality management values in their organisations. They have very low control while the demands are high and thus they are stressed.
The quality enjoyers. On the other hand, this is the group with the best situation. They experience the quality management values to a high degree and their health is good. Their level of control is high which means that although their demands are substantial, the stress level is not very high.
The unmotivated. In this group, the levels of stress and demands are quite low. Yet, their control is also low and they do not experience much of the quality management values. Thus, their health is not good.
The ambitious. This group has the highest levels of stress and demands. However, the control is also relatively high and they experience the quality management values to a reasonable degree. Consequently, their health is fairly good.
Discussion
The correlation analysis showed that the values participation of everybody, process orientation and management by fact are negatively correlated with stress. The explanation may be that these quality management values make organisations more efficient and well-functioning which decreases the stress levels.
In addition, it is interesting to note that the quality management values are highly correlated with control while their association with demands is more mixed. Actually, the value customer orientation seems to lead to a higher level of demands. This is not entirely surprising since satisfying the customers’ needs and wants requires a great amount of effort, not least for pupils in schools. On the other hand, the increased control that is associated with this (and the other) values appears to mitigate the effects on stress that these increased demands lead to. Thus, although customer orientation increases the demands, it does not seem to increase stress, probably due to the increased control.
In general, although there is a variation, at least some of the values seem to have an effect of decreasing the stress level among the employees. For the value process orientation, the reason probably is that it implies a better organised and well-functioning organisation, which is likely to have an effect of decreasing organisational stress. The foundation for the stress-reducing effect of participation of everybody is almost certainly its intimate connection to control.
There were significant differences in the perception of the quality management values between the teachers that were bullied and those who were not. This may indicate that quality management is a way of avoiding bullying at workplaces.
Comparing the results from the cluster analysis to the demand-control-model and its categories, we can note that the quality enjoyers and the ambitious are in the active work category which rhymes well with their higher level of workplace health despite high demands. This is also where it is most natural to find academic professions of this kind. In contrast, the unmotivated are in the passive work category with low demands and low control. This is not where teachers are normally expected to be and this may be a failure of their work situation possibly due to lacking leadership or underfunding. Going further, we find that the problematics are in the high strain work category with high demands and low control. Although this is more in line with what would be expected for teachers of today, it is the worst work environment situation and it is natural that it takes a toll on their health. Finally, it is noteworthy that none of the clusters is in the low-strain category which seems logical since this is not a category where employees in the educational professions are expected to be.
Conclusions and implications
The first conclusion that can be drawn from the study is that it confirms previous research findings that there is an association between quality management values and workplace health (e.g. Bäckström et al., Citation2012; Lagrosen, Citation2006; Lagrosen et al., Citation2010). This relationship was very clear in the study and it provides further evidence to the series of studies that have shown this connection. Research has shown that self-reported health corresponds with objective measures of morbidity (Nyberg et al., Citation2005). Therefore, it is reasonable to believe that an increase in self-reported health also leads to lower levels of sick-leave.
Secondly, some conclusions can be drawn regarding stress. The findings indicate that high control is associated with higher workplace health while the level of demands does not seem to have a significant influence on health. The correlation analysis indicated that the quality management values are correlated with control while the associations with demand were mixed. The final important conclusion is that the quality management values are associated with lower levels of workplace bullying. This is important since the study also shows that being exposed to bullying is related to lower workplace health.
The scientific implications of the study are firstly that it confirms the findings of previous research that quality management values (see ) are related to workplace health. With a large number of studies now having come to the same conclusions in different organisations and various settings, this is becoming close to an established fact. While the effects of quality management on workplace health had been studied earlier, the findings regarding workplace stress and bullying are novel and constitute the originality of this study. The beneficial effects of quality management on these adversities add to the scientific understanding of the usefulness of quality management, not only for improved products and processes, but also for employee well-being.
The practical implications for school managers, and possibly for other managers mainly lie in pointing out the value of creating a quality culture based on quality management values in the organisation. The cluster analysis clearly shows that with an established quality culture in which the fundamental values of quality management are lively, the well-being of the employees can be high despite demanding work situations. The finding that quality management can alleviate bullying should also inspire managers to implement it in order to avoid suffering for many employees.
Limitations and suggestions for further research
There are several limitations for the study. Secondary school teachers in Sweden were studied. We cannot know to what extent the findings are representative also for other industries or in other nations. Another reason for some caution is that the response rate was presumably low. In fact, we cannot calculate how high it was since we do not have any figures regarding the number of employees in the schools. According to statistics from the Swedish National Agency for Education, 34,476 people are working as teachers in the Swedish upper secondary school system which contains 1,329 school units. This means that the average school unit has approximately 26 employees. If this figure is used for calculation, the sample should include around 2,300 people. The response rate would then be about 13%. Nevertheless, this is just a crude approximation and the number is most likely lower since the schools that were approached often contain several units. There is definitely a possibility that there is a bias due to differences between the sample and the entire research population. Even so, a considerable number of secondary school teachers have participated in the study. In addition, the most important aspect of the study concerns associations between different variables and they should be less sensible to bias than the absolute figures. For instance, the proportion of teachers reporting that they have been bullied may be substantially distorted by differences in response rate among bullied and non-bullied respondents. Therefore, this study should not be used as a source for gauging the frequency of bullying in the Swedish upper secondary school system. However, there is much less reason to assume that the associations to health and quality management variables are different for bullied or non-bullied respondents and non-respondents respectively. Thus, the findings should be of substantial value even if the representativeness cannot be assured.
A further limitation is that subjective self-reporting is used for measuring health. However, it may be the most critical measure since the experience of health is what actually influences peoples’ lives (Bowling, Citation2005). In consequence, self-reported health has been found to correlate with objective, medicinal measures of health (Nyberg et al., Citation2005).
For further research, studies of the same factors in other organisations and other countries should be useful. While, the association between quality management and health is becoming rather well studied, the connections to workplace stress and bullying have not been studied earlier. Thus, studies with this aim would be particularly valuable. Moreover, qualitative studies examining the mechanics and the causes of the associations that have been found could enrich the knowledge with more in-depth understanding. Finally, among the components of quality management presented in , it is the quality management values that have been studied in this and previous studies. This is logical due to their basic nature and since they are often espoused by management. Nevertheless, it would be interesting to study the effects of the other components (tools, models and core values) on employee health.
Acknowledgement
The data that support the findings of this study are available on request from the corresponding author, [sl]. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Addley, K. (1999). Developing programmes to achieve a healthy society: Creating healthy workplaces in Northern Ireland. Occupational Medicine, 49(5), 325–330. https://doi.org/https://doi.org/10.1093/occmed/49.5.325
- Ahmad, S. (2018). Can ethical leadership inhibit workplace bullying across East and West: Exploring cross-cultural interactional justice as a mediating mechanism. European Management Journal, 36(2), 223–234. https://doi.org/https://doi.org/10.1016/j.emj.2018.01.003
- Arneson, H. (2006). Empowerment and health promotion in working life [Doctoral dissertation]. Linköping University.
- Bäckström, I., Eriksson, L., & Lagrosen, Y. (2012). A health-related quality management approach to evaluating health promotion activities. International Journal of Quality and Service Sciences, 4(1), 76–85. https://doi.org/https://doi.org/10.1108/17566691211219742
- Baird, K., Hu, K. J., & Reeve, R. (2011). The relationships between organizational culture, total quality management practices and operational performance. International Journal of Operations & Production Management, 31(7-8), 789–814. https://doi.org/https://doi.org/10.1108/01443571111144850
- Bergman, B., & Klefsjö, B. (2010). Quality from customer needs to customer satisfaction (3rd ed.). Studentlitteratur.
- Bernin, P. (2002). Managers’ working conditions - stress and health. Karolinska institutet.
- Bowling, A. (2005). Measuring Health - A review of quality of life measurement scales (3rd ed.). Open University Press.
- Bowling, N. A., & Beehr, T. A. (2006). Workplace harassment from the victim’s perspective: A theoretical model and meta-analysis. Journal of Applied Psychology, 91(5), 998–1012. https://doi.org/https://doi.org/10.1037/0021-9010.91.5.998
- Brenner, M. H., Andreeva, E., Theorell, T., Goldberg, M., Westerlund, H., Leineweber, C., … Bonnaud, S. (2014). Organizational downsizing and depressive symptoms in the European recession: The experience of workers in France, Hungary, Sweden and the United Kingdom. PLoS One, 9(5), e97063. https://doi.org/https://doi.org/10.1371/journal.pone.0097063
- Cancelliere, C., Cassidy, J. D., Ammendolia, C., & Coté, P. (2011). Are workplace health promotion programs effective at improving presenteeism in workers? A systematic review and best evidence synthesis of the literatur. BMC Public Health, 11(1), 395–406. https://doi.org/https://doi.org/10.1186/1471-2458-11-395
- Dahlgaard-Park, S. M. (2012). Core values - the entrance to human satisfaction and commitment. Total Quality Management & Business Excellence, 23(2), 125–140. https://doi.org/https://doi.org/10.1080/14783363.2012.655067
- Dahlgaard-Park, S. M., Chen, C.-K., Jang, J.-Y., & Dahlgaard, J. J. (2013). Diagnosing and prognosticating the quality movement - a review on the 25 years of quality literature (1987-2011). Total Quality Management & Business Excellence, 24(1-2), 1–18. https://doi.org/https://doi.org/10.1080/14783363.2012.756749
- Dahlgaard, J. J., Kristensen, K., & Kanji, G. K. (1998). Fundamentals of total quality management. Chapman & Hall.
- Dale, B. G. (1999). Managing quality (Vol. 3). Blackwell Publishers Ltd.
- Dale, B. G., & Lascelles, D. M. (1997). Total quality management adoption: Revisiting the levels. The TQM-Magazine, 9(6), 418–428. https://doi.org/https://doi.org/10.1108/09544789710186957
- Daubas-Letourneux, V., & Thébaud-Mony, A. (2003). Working organisation and health at work in the European Union. European Foundation for the Improvement of Living and Working Conditions.
- Einarsen, S., Hoel, H., Zapf, D., & Cooper, C. (2011). The concept of bullying and harassment at work: The European tradition. Taylor & Francis.
- Fida, R., Tramontano, C., Paciello, M., Guglielmetti, C., Gilardi, S., Probst, T. M., & Barbaranelli, C. (2018). ‘First do no harm’: The role of negative emotions and moral disengagement in understanding the relationship between workplace aggression and misbehavior. Frontiers in Psychology, 9(671), 1–17.
- Hair, J. F., Anderson, R. E., Tatham, R. L., & Black, C. B. (1998). Multivariate data Analysis (5th ed.). Prentice Hall Inc.
- Hanson, A. (2007). Workplace health promotion - a salutogenic approachHouse.
- Hardjono, T. W., ten Have, S., & ten Have, W. D. (1997). The european way to excellence. European Quality Publications.
- House, J. (1981). Work, stress and social support. Addison-Wesley.
- Jackson, D., Firtko, A., & Edenborough, M. (2007). Personal resilience as a strategy for surviving and thriving in the face of workplace adversity: A literature review. Journal of Advanced Nursing, 60(1), 1–9. https://doi.org/https://doi.org/10.1111/j.1365-2648.2007.04412.x
- Karasek, R. (1979). Job demands, job decision latitude and mental strain: Implications for job redesign. Administrative Science Quarterly, 24(2), 285–307. https://doi.org/https://doi.org/10.2307/2392498
- Karasek, R., & Theorell, T. (1990). Healthy work, stress, productivity, and the reconstruction of working life. Basic Books.
- Kivimäki, M., Virtanen, M., Vartia, M., Elovainio, M., Vahtera, J., & Keltikangas-Järvinen, L. (2003). Workplace bullying and the risk of cardiovascular disease and depression. Occupational and Environmental Medicine, 60(10), 779–783. https://doi.org/https://doi.org/10.1136/oem.60.10.779
- Lagrosen, Y. (2006). Values and practices of quality management - Health implications and organisational differences [Doctoral dissertation]. Chalmers University of Technology.
- Lagrosen, Y., Bäckström, I., & Lagrosen, S. (2007). Quality management and health - a double connection. International Journal of Quality and Reliability Management, 24(1), 49–61. https://doi.org/https://doi.org/10.1108/02656710710720321
- Lagrosen, Y., Bäckström, I., & Lagrosen, S. (2010). The relationship between quality management and health - exploring the underlying dimensions. International Journal of Productivity and Quality Management, 5(2), 109–123. https://doi.org/https://doi.org/10.1504/IJPQM.2010.030737
- Lagrosen, Y., Bäckström, I., & Wiklund, H. (2012). Approach for measuring health-related quality management. The TQM Journal, 24(1), 59–71. https://doi.org/https://doi.org/10.1108/17542731211191221
- Lagrosen, S., & Lagrosen, Y. (2003). Quality configurations - a contingency approach to quality management. International Journal of Quality and Reliability Management, 20(7), 759–773. https://doi.org/https://doi.org/10.1108/02656710310491203
- Lagrosen, S., & Lagrosen, Y. (2014). Work integrated learning for employee health in schools. International Journal of Quality and Service Sciences, 6(4), 387–398. https://doi.org/https://doi.org/10.1108/IJQSS-09-2012-0015
- Lagrosen, Y., & Lagrosen, S. (2005). The effects of quality management - a survey of Swedish quality professionals. International Journal of Operations and Production Management, 25(10), 940–952. https://doi.org/https://doi.org/10.1108/01443570510619464
- Lagrosen, Y., & Lagrosen, S. (2012). Organisational learning for school quality and health. International Journal of Educational Management, 26(7), 664–677.
- Larsson, R. (2015). Managing workplace health promotion in municipal organizations Doctoral dissertation Mälardalen University.
- Nyberg, A., Bernin, P., & Theorell, T. (2005). The impact of leadership on the health of subordinates. National Institute for Working Life.
- Pheko, M. M. (2018). Autoethnography and cognitive adaptation: Two powerful buffers against the negative consequences of workplace bullying and academic mobbing. International Journal of Qualitative Studies on Health and Well-Being, 13(1), 1459134. https://doi.org/https://doi.org/10.1080/17482631.2018.1459134
- Salin, D. (2003). Ways of explaining workplace bullying: A review of enabling, motivating and precipitating structures and processes in the work environment. Human Relations, 56(10), 1213–1232. https://doi.org/https://doi.org/10.1177/00187267035610003
- The Swedish Work Environment Authority. (2016). Arbetsmiljöstatistik Rapport 2016:1, Arbetsskador 2015, occupational accidents and work-related disease. The Swedish Work Environment Authority.
- Wang, J., Schmitz, N., Smailes, E., Sareen, J., & Patten, S. (2010). Workplace characteristics, depression, and health-related presenteeism in a general population sample. Journal of Occupational and Environmental Medicine, 52(8), 836–842. https://doi.org/https://doi.org/10.1097/JOM.0b013e3181ed3d80
- WHO. (2020). Protecting workers health. who.int/news-room/fact-sheets/detail/protecting-workers’-health.
Appendix 1
Workplace health and stress questionnaire
(Translated from Swedish. Please note that the questionnaire was online with a completely different layout, which is impossible to reproduce in text. The study was part of a larger research programme and so the questionnaire included additional questions not used in this study and thus not included below.)
Gender (female, male or other):
Age (seven categories starting with 19 y or younger and ending with 70 y or older):
To what extent do you agree with the following statements (measured on a seven level likert-type scale with the endpoints 1 = Do not agree at all, 7 = Agree completely):
I am proud of the quality of our activities.
We give our pupils the best possible education, given the resources we have.
I always do my best to support my colleagues in their work.
I can influence my work situation.
I can carry out my tasks in the way that suits me best.
I can influence decisions regarding my workplace as a whole.
My managers pay attention to my situation and support me.
My managers are actively and visibly engaged in the operations.
My managers are good examples regarding quality.
My workplace is organised around our most important activities regardless of formal positions and borders.
My tasks are devoted to the needs of the operations without unnecessary bureaucracy.
There is always someone who is responsible for each part of our operations.
My workplace has clear and measurable goals that are followed-up.
The decisions of my managers are based on facts.
I have good possibilities to measure and assess the results of my work.
At my workplace, creative ideas and suggestions are encouraged.
We always try to carry out our activities in the best possible way even if it means that we often need to reorganise and change our routines.
My workplace is characterised by continuous improvements.
The pace of work at my workplace is high.
I have difficulties not thinking of my work on my free time.
I feel high demands of performance in my work.
I can myself decide when and where to carry out my tasks.
I often feel stressed at my workplace.
Do you feel that you are bullied at your workplace (no, sometimes, often)?