
ABSTRACT
Introduction
Herpes zoster (HZ) or shingles occurs as a result of reactivation after a primary infection with varicella zoster virus (chickenpox). The burden of HZ in older adults in China is not well understood. We conducted a systematic literature review to understand the burden of disease related to HZ, its complications, and associated costs in China.
Areas covered
Using publications retrieved from Chinese and English literature databases, we described incidence and prevalence of HZ, occurrence of HZ-related complications, and costs associated with HZ in mainland China, Taiwan, and Hong Kong.
Expert opinion
The data, although limited, indicate that the burden of disease due to HZ is substantial in China, with incidence rates that are comparable to the rest of the world. Recently, an adjuvanted recombinant HZ vaccine was approved for use in China. Disease prevention is likely to reduce the burden of disease, with potentially significant economic benefits. However, understanding the public health impact of vaccination in China will require extensive baseline information about incidence, complication rates, and associated costs. This review gives an overview of available research, but also reveals existing gaps. Well-designed observational studies are needed to quantify the total burden of disease and potential impact of prevention through vaccination.
PLAIN LANGUAGE SUMMARY
What is the context?
Although Herpes zoster (shingles) is a common disease of older age, the burden of disease in China is not well described.
32% of the Chinese population is aged 50 years and Older and this proportion is increasing. As a result of the ageing population, the public burden associated with shingles is expected to increase over time.
What is new?
We accessed published studies in the English and Chinese language literature to explore available information describing shingles in China.
The incidence of shingles in Taiwan, Hong Kong and mainland China appears to be similar to other countries, although reliable population-based data are currently sparse in Hong Kong and mainland China.
What is the impact?
Data describing the disease burden due to shingles are currently heterogeneous throughout China. This review is a first step to determine those populations which could benefit most from shingles vaccination.
Preventing shingles through vaccination could benefit the individual as well as provide potentially significant economic benefits for the individual, the employer and the economy.
1. Introduction
The total population of China is more than 1.4 billion, and in 2019, residents aged 50 years and older were estimated to comprise approximately 32% of the population in China [Citation1]. The proportion of adults aged 50 years and over is increasing by 3–4% annually, posing significant social and economic challenges [Citation1,Citation2]. Herpes zoster (HZ or shingles) is a disease that is strongly linked to older age and is a consequence of viral reactivation after a primary infection with varicella zoster virus. Latent virions within sensory ganglia can re-activate when immune control fails, most commonly as a result of natural age-related declines in immunity (immune senescence) or immunosuppression due to any cause. HZ typically manifests as a painful vesicular rash with a dermatomal distribution. The most common complication is the persistence of neuropathic pain (post-herpetic neuralgia, [PHN]), which follows HZ. The risk of developing PHN increases with age and can affect more than 30% of those aged ≥80 years who develop HZ [Citation3]. PHN resolves in the majority of patients by approximately 1 year but can persist for up to 5 years or more in around 2% of patients [Citation3]. Other complications of HZ include ocular involvement with uveitis, secondary bacterial infections, motor deficiencies, disseminated HZ infection, encephalitis, and other neurological complications, and vasculopathies that can cause stroke or myocardial infarction [Citation4,Citation5].
Much of the data describing the disease burden due to HZ comes from database studies conducted outside of Asia [Citation6]. To our knowledge, systematic surveillance of HZ is not performed in China. Incidence rates of HZ from studies conducted in the United Kingdom, Europe, North America, Australia, Taiwan, and South Korea range from approximately 2 to 5 per 1000 person-years at age 40 years, increasingly from age 50 years, up to 10 per 1000 person-years, and up to 16 per 1000 person-years at age 85 years [Citation7]. The lifetime risk of developing HZ is 30% [Citation7]. The quantity and quality of studies describing the burden of HZ across Asian countries are highly variable [Citation8]. Some countries/regions are well represented, such as Korea, and Taiwan, whereas there are little data in the published English language literature describing HZ in mainland China [Citation8].
As the Chinese population age, the public health burden and associated costs due to HZ will increase over time. We conducted a systematic review of the literature to understand the burden associated with HZ and its complications, as well as the costs related to HZ in mainland China, including the off-shore territories of Hong Kong and Taiwan.
2. Methods
2.1. Objectives
The study objectives were to describe the incidence and prevalence of HZ in Chinese adults ≥18 years of age; to summarize the occurrence of complications due to HZ, such as PHN, ocular, neurological, cutaneous, or other HZ-related complications; to assess the risk of HZ in patients with other co-morbidities; and to evaluate healthcare resource use due to HZ and PHN by assessing direct medical costs and indirect costs to patients. Secondary objectives were to consider resource use in terms of medications and treatments.
2.2. Information sources and search strategy
English language (PubMed, EMBASE, EBSCO, Web of Science) and Chinese language (Cnki 知网, Wanfang Data 万方, and Weipu 维普) databases were searched for relevant literature published between 1 January 2000 and 10 April 2019. Specific queries for each study objective were undertaken using a combination of terms/synonyms for HZ, PHN, China, Hong Kong, Taiwan, incidence, incidence of complications, costs, and burden. The complete search strings are provided in Table S1, and the search strategy for each database in Table S2.
2.3. Selection process, data collection and quality control
We included articles in English or Chinese with information pertaining to the incidence or prevalence of HZ, HZ-associated complications, HZ-associated comorbidity, and costs. Articles that only described results in children, immunocompromised populations, or patients on immunosuppressive therapy were excluded. We also excluded review articles, letters, editorials, expert commentaries, clinical trials, and case reports. Retrieved articles and reviews were manually searched for additional references.
The titles and abstracts identified from each search strategy were screened for their relevance to the study objectives (). Full-text articles were assessed for eligibility and, if relevant, underwent data extraction into evidence tables. Information about the study design, the incidence, prevalence, or proportions of patients with HZ and HZ-related complications, as well as health-care resource utilization and direct and indirect costs, was captured. All relevant articles were included and all data extracted from Chinese articles were translated into English. Two reviewers screened titles, abstracts, full texts, and extracted data.
Figure 1. Article selection
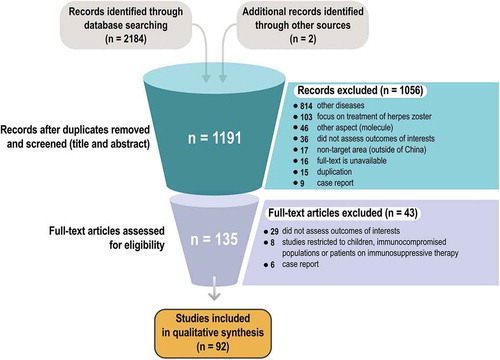
Few studies used a classical epidemiological design and most were descriptive follow-ups of a group of patients and were not suited for appraisal with existing checklists. Therefore, no quality assessment was performed and all studies identified in the search were included in the review. Where information was available, case ascertainment was described. Performing a meta-analysis was not the objective of this study due to the clinical diversity of the studies and heterogeneity of the data. Limitations of the studies are discussed in Section 5.
2.4. Evaluation of cost of disease
Costs associated with HZ disease/complication were reported as direct costs (medications, all medical services including outpatient visits, hospitalizations) and indirect costs (costs of transport, productivity loss of patient and/or family caregiver(s), nutrition, and other costs incurred associated with HZ but not included in the direct costs). Definitions vary across articles assessed.
3. Results
The search for articles yielded 2186 records from which 92 unique articles were identified for inclusion in this review (). Of these, 36 were published in Chinese and 56 in English. There were 46 studies conducted in mainland China, 42 in Taiwan, and 4 in Hong Kong.
Most studies conducted in mainland China were hospital-based case series, and several were large community surveys linked to the investigation of medical records and provided a broader picture of the HZ disease burden. All studies in Taiwan used data from the National Health Insurance Research Database (NHIRD) which captures all health-care administrative and claims data in the entire Taiwanese population of approximately 24 million. The database holds information on demography, inpatient, and outpatient services (physician services, drugs, imaging, and laboratory examinations), and procedures. Primary and secondary diagnoses are coded in the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) format. The four studies in Hong Kong encompassed a range of designs and data sources and included a cost-effectiveness analysis, and hospital-based case series.
3.1. HZ age-distribution, incidence, and prevalence
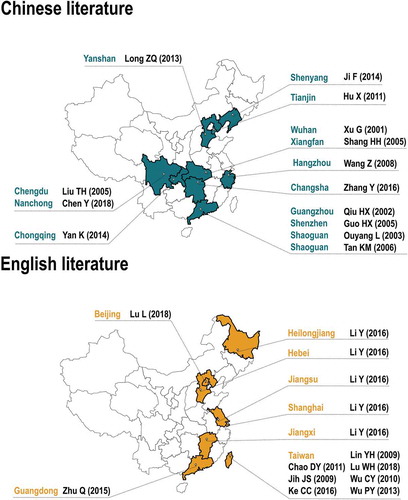
Eighteen studies reported on the occurrence of HZ in mainland China (14 written in Chinese, 4 in English) and 7 (all in English) provided information from Taiwan. The studies were conducted between 1995 and 2017 and together provided information from 11 out of 26 Chinese provinces and 4 Chinese municipalities ().
Figure 2. Distribution of studies published in Chinese and English literature across provinces in China
All 14 of the Chinese literature studies were hospital-based case series that provide the age-distribution of HZ cases according to varying age-group categories. A summary of the Chinese literature studies and the reference list is provided in Table S3. Case ascertainment methods were not reported in the majority of articles, and the studies encompassed wide age ranges. As a result, there was a wide heterogeneity in the results. The results reported that 56.02% to 79.7% of all HZ cases occurred in adults aged ≥50 years, and 38.75% to 66.22% occurred from the age of 60 years (Table S3).
HZ incidence rates were reported in 10 studies, and three reported the incidence of HZ in mainland China [Citation9–11] (). All three were community-based surveys that employed trained researchers to interview community members about the occurrence of an HZ episode in recent years. One study was conducted in Guangdong, one in Beijing, and another in a mix of rural and urban townships. One study reported the overall adjusted incidence of HZ to be 1.9 per 1000 population [Citation10]. Two studies showed an increasing incidence of self-reported HZ among individuals aged ≥50 years over time; from 4.1 per 1000 person-years in 2011 increasing to 5.8 in 2013 in one study [Citation9], and from 2.9 per 1000 population in 2010 increasing to 4.18 per 1000 population in 2012 in another [Citation11]. Both studies were subject to under-reporting as well as recall bias. One of the studies showed that HZ was more frequent in women than in men (3.95 versus 2.89 per 1000 population) and in urban versus rural settings (7.65 versus 2.06 per 1000 population) [Citation11].
Table 1. Incidence of Herpes zoster (HZ) in Taiwan and mainland China (English literature)
Seven studies reported HZ incidence in Taiwan and all used the NHIRD [Citation12–18]. These studies spanned the years 2000 to 2011 and differed in their objectives, study years, and methodology. The incidence of HZ in the general population between 2000 and 2008 ranged from 4.45 to 6.89 per 1000 person-years and increased over time [Citation12–16]. HZ was more frequent in women than men (5.09 versus 4.71 per 1000 person-years, 5.20 versus 4.72 per 1000 population) [Citation14,Citation17]. In six studies that provided incidence data by age group, HZ incidence was higher in older age [Citation13–18]. In 2008, the incidence of HZ per 1000 person-years was 12.81 in 65–74 year-olds, 13.52 in 75–84 year olds, and 12.41 in those aged ≥80 years [Citation15]. In the most recent study using data from 2005 to 2011, the incidence of HZ in Taiwan was 1.53 per 1000 person-years in persons aged less than 30 years, versus 9.53 per 1000 person-years in those aged >70 years [Citation18].
We did not identify any studies that reported the incidence of HZ in Hong Kong.
Two cross-sectional studies, both conducted in mainland China, reported on the prevalence of HZ [Citation9,Citation19]. In the first study, the prevalence of physician-diagnosed HZ among 36,170 adults from 40 years presenting to 24 hospitals across China over a 30- to 60-day period was 7.7% [Citation19]. The prevalence of HZ was 5.5% in 40–50 year olds, 7.1% in 51–59 year olds, 8.4% in 60–69 year olds, and 10.6% in those aged ≥70 years, and was similar in women (7.9%) and men (7.6%) [Citation19]. In the second study, a sample of 7149 individuals aged ≥50 years from 34 countries/districts of Guangdong province were surveyed [Citation9]. The estimated lifetime prevalence of self-reported HZ was 3.46% in ≥50 year-olds [Citation9]. The proportion of individuals who developed HZ was 2.93% in 50–59 year olds, 3.24% in 60–69 year olds, 3.42% in 70–79 year olds, and 6.40% in those aged ≥80 years, and was higher in women (3.94%) than in men (2.86%).
3.2. The risk of HZ in patients with other co-morbidities
There were 27 articles that evaluated the risk of developing HZ in persons with a range of underlying medical conditions, or who were taking steroids, androgen deprivation therapy, or statins. All the studies were conducted in Taiwan, using the NHIRD, compared HZ rates in the population of interest with rates in the general population. Three studies were case–control studies in which controls were matched on age and sex. The results expressed as ratios (hazard ratio [HR], odds ratio, or risk ratio) variably adjusted for a range of variables including age, sex, co-morbidities, and medication use are presented in . The tabulated data and list of references are provided in Table S4.
Figure 3. Adjusted ratios comparing the incidence of HZ in persons with a range of underlying co-morbidities compared to a comparator population. Only studies from Taiwan are shown. Tabulated data including adjusted variables, references are provided in Table S4
Persons with the highest risk of developing HZ were those who had undergone renal transplant (HR 8.46, 95% CI: 5.85–12.2) (). Markedly elevated risks were also observed in individuals undergoing peritoneal dialysis for treatment of chronic renal failure (HR: 3.61, 95% CI: 2.69–4.83) and individuals with autoimmune diseases including systemic lupus erythematosus, rheumatoid arthritis, dermatomyositis or polymyositis, Sjogren’s syndrome, and unspecified autoimmune diseases (range of HRs between 4.55 and 1.28).
Diabetes, malignancies, chronic kidney disease/uremia, chronic obstructive pulmonary disease, and peptic ulcer disease were all associated with a significantly higher risk of HZ than the general population in most studies (range of HRs: 1.17–8.46) [Citation13,Citation14,Citation18,Citation20–27]. The potential association was weaker in persons with depression, psychiatric disease, hyperlipidemia, hypertension, as well as those post-general anesthesia (range of HRs: 1.11–1.29) [Citation20,Citation25,Citation26,Citation28,Citation29]. Conversely, systemic steroid use in patients with psoriasis was associated with a significantly reduced risk of HZ (HR: 0.6, 95% CI: 0.44–0.81) [Citation30], as was radical prostatectomy and hormone therapy in patients with prostate cancer (HR: 0.60, 95% CI: 0.44–0.81) [Citation31].
3.3. Complications of HZ
3.3.1. Post-herpetic neuralgia
There were 39 studies that reported the occurrence of PHN after an episode of HZ. Of these, 27 were from mainland China, 9 were from Taiwan, and 3 were from Hong Kong. A total of 18 studies were written in Chinese and 21 in English. A summary of these studies and the full list of references are provided in Table S5.
The results of the studies were heterogeneous and the percentages of patients with HZ who developed PHN varied from very low (1.85%) [Citation32] to very high (80.2%) [Citation33]. The median percentage in the data from all three countries was 22% (interquartile range 10–37). PHN was defined by ICD codes, physician diagnosis, medical records, as pain persisting from between 30 and 180 days, as a pain score, and was unspecified in 6 articles (Table S5). There were no clear trends in PHN rates based on the PHN definition employed. In seven studies, where PHN was defined as pain lasting ≥30 days to >6 weeks duration, the percentage of patients who developed PHN varied from 15.2% to 46.43%. In eight studies, where the duration of pain was at least 90 days, PHN rates ranged from 4.6% to 57.81%. In one study where PHN was defined as pain lasting at least 180 days, the rate in adults aged ≥75 years was 80.2%. In four studies conducted in patients aged ≥50 years, the incidence of PHN ranged from 16.2% to 40.2%, although each study used a different PHN definition [Citation9,Citation11,Citation34,Citation35]. In seven studies of cohorts of adults aged at least 60 years, PHN incidence ranged from 2.4% to 80.2% [Citation15,Citation33,Citation36–40].
3.3.2. Other complications
Fourteen articles explored the percentage of patients with HZ, who developed complications other than PHN; eight from mainland China, four from Taiwan, and two from Hong Kong (). Eight studies were written in Chinese and six in English. Ophthalmic complications developed in 0.76% to 26.42% of patients with HZ, infections including pneumonia sepsis, and encephalitis/meningoencephalitis in 1.11% to 4.7%, and dermatological complications including cellulitis and other skin infections in 2.17% to 12.86% of patients. Neuralgic complications including motor nerve palsy, trigeminal neuralgia, or Ramsay Hunt syndrome, developed in 0.5% to 8.92% of patients. One study reported on post-herpetic stroke (1.26% of patients).
Table 2. The percentage of patients with herpes zoster (HZ) who developed complications (English and Chinese literature)
3.4. Economic burden of HZ
There were 17 studies that assessed the HZ-associated health-economic burden such as direct costs, indirect costs such as transport costs to seek medical care (). Of these, 13 were conducted in mainland China, two in Taiwan, and two in Hong Kong. Reported costs were standardized to 2019 consumer price index and currency rates and are also presented in United States dollars (USD) (1 Chinese Yuan [RMB] = 0.1448 USD and 1 euro = 1.1076 USD).
Table 3. Estimates of the cost of disease in patients with Herpes zoster (HZ) (English and Chinese literature)
3.4.1. Mainland China
There were 13 articles that reported the economic cost of HZ in mainland China [Citation41–52). Several studies were conducted to evaluate the costs associated with different treatment regimens, such as different anti-viral drugs or Western versus traditional Chinese medicines. Eleven studies were written in Chinese and two in English and all studies were reported in RMB.
Five studies investigated the cost-effectiveness of four antiviral drugs: acyclovir, valaciclovir, ribavirin, and ganciclovir for the treatment of HZ [Citation41–43]. The reported average treatment costs per patient with HZ, which included antiviral drugs, injection, hospitalization, examination, adjuvant drug therapy, wet wrap therapy (a traditional Chinese treatment), and nursing expenses, and ranged from RMB 421.2 to 1798.36. The costs associated with the administration of traditional Chinese medicine ranged from RMB 112.4 to 157.4 and the costs of Western treatments ranged from RMB 333.39 to 594.50 [Citation46,Citation50]. The cost of individual traditional Chinese treatments such as cotton-sheet moxibustion, acupuncture, tapping/cupping, and hot needle puncture ranged from RMB 221.76 to 254.52 [Citation49].
Two of the 13 articles were economic evaluations that studied the costs associated with different analgesics used in patients with PHN, including oxycodone-acetaminophen tablets (RMB 106.14 for 20 doses), ibuprofen sustained-release capsules (RMB 15.40), prednisone (RMB 470), hydrocortisone (RMB 690), and betamethasone (RMB 500) [Citation44,Citation48].
In the community survey conducted by Li Y et al. [Citation11], costs were recorded from inpatient and outpatient health-care records, receipts of payments for medical treatment, reimbursement records from the New Rural Co-financing Medical System and the Health-Care Insurance System, and through patient recall. Cost information included outpatient and inpatient expenses, ancillary drugs, transport costs to seek medical care, productivity loss for the patient and caregiver, and any other associated costs. The total mean cost of HZ among adults aged ≥50 years was RMB 840.6 per patient (range 0–30,002) [Citation11]. The mean cost was RMB 4502.4 for HZ-associated hospitalization, RMB 543.8 for outpatient services, and RMB 109.4 for other expenses. The total cost increased with the age, from mean RMB 674.07 in 50–59 year olds, peaking at RMB 1138.1 in 70–79 year olds. Mean costs increased over time and were higher in urban (RMB 891.61) than rural (RMB 802.97) areas. The mean cost of HZ was higher in patients who developed sequelae (e.g. PHN or dermatological complications) (RMB 1221.78), than patients who had uncomplicated disease (RMB 530.92).
A study conducted in Beijing [Citation51] used a questionnaire to survey 218 individuals who had experienced HZ. Approximately 90% of subjects were field surveyed and 10% by telephone survey. Subjects with HZ were identified from the dermatology or traditional Chinese medicine department from two tertiary hospitals, and two second-class hospitals. The reported mean cost of HZ was RMB 1614.47 per patient, made up of RMB 1270.44 in direct medical costs and RMB 344.03 in non-medical costs (transportation, nutrition, and other expenses). Medical costs included outpatient service charges (RMB 1091.54) and hospital charges (RMB 178.90). Non-medical costs included transport expenses (RMB 105.08) and nutrition and other expenses (RMB 238.95). Another study conducted in a rural township interviewed adults aged >50 years with a history of HZ and matched them to medical records [Citation52]. This study found that the average cost of HZ was RMB 286.02 among 51 outpatients and 1 inpatient [Citation52].
3.4.2. Taiwan
There were two studies that reported the costs associated with HZ in Taiwan [Citation14,Citation17] (). Both analyses used claims information from the NHIRD. Lin et al. [Citation17] demonstrated that total medical expenditure related to the treatment of HZ increased progressively over time in Taiwan, from USD 7.7 million in 2000 to USD 9.8 million in 2004, likely as a result of population aging. Direct costs increased with age, from approximately USD 30.8 per patient in children and adolescents to USD 204 per patient for those aged ≥80 years [Citation17]. Jih et al. [Citation14] reported that the cost of HZ was €53.30 per person for home care cases, and €1,224.70 for hospitalized cases.
3.4.3. Hong Kong
Two studies evaluated the costs of HZ in Hong Kong [Citation53,Citation54] (). Ming et al. [Citation53] reported direct costs associated with HZ hospitalization from two tertiary hospitals in Hong Kong. The mean total direct medical cost of all hospitalized HZ cases (n = 105) was USD 4883. The mean cost per patient who was immunocompromised was USD 9891 compared to USD 4049 per immunocompetent patient [Citation53].
You et al. [Citation54] performed a cost-effectiveness evaluation of HZ vaccination in Hong Kong using medical records from several outpatient clinics and two general hospitals. Indirect costs included productivity loss and loss of life-time earnings due to HZ-associated mortality by age and gender. Age- and gender-specific labor force participation and unemployment rate were used to multiply median monthly earnings. The median cost was USD 309 per outpatient case, USD 2887 for each case of hospitalized uncomplicated HZ and ranged from USD 1900 (secondary skin and soft tissue infection) to USD 26,269 (central nervous system infection) for per each hospitalized case with complications.
3.4.4. Duration of hospitalization
Eleven studies reporting the mean length of stay of patients hospitalized for HZ are summarized in Table S6. Eight studies were conducted in mainland China, and seven were written in Chinese. There was one article from Taiwan and two from Hong Kong.
The mean duration of hospitalization for patients with HZ ranged from 8.44 to 13.87 days in China and appeared to differ according to the treatment regimen, being the shortest in patients treated with valaciclovir (10.59 or 12.04 days in two studies, versus 11.37–13.19 days for other anti-virals) [Citation11,Citation42,Citation45,Citation52,Citation55–58]. The mean length of hospitalization was shorter in Taiwan (8.3 days, single study [Citation23]) and Hong Kong (range of 5 to 5.9 days in immunocompetent adults or adults without HZ-associated complications) [Citation53,Citation54]. Hospitalizations were longer in immunocompromised patients with HZ (mean 14.7 days), and in patients with severe complications (10 days for disseminated HZ, 11 days for Ramsay Hunt Syndrome and 43 days for central nervous system infections) [Citation53,Citation54].
4. Conclusions
To our knowledge, this is the first systematic literature review conducted among the Chinese population that accessed both English and Chinese databases for peer-reviewed publications. Despite the limitations in the data available, the results show some important trends. The incidence of HZ in mainland China, Taiwan, and Hong Kong is similar to the incidence reported in Western countries. The annual incidence rate of HZ has been reported to range from 3 to 5 per 1000 person-years, increasing to 6 to 8 per 1000 person-years from 60 years of age [Citation6]. In the studies reported here, the incidence of HZ was in the same range, from 2.9 to 5.8 per 1000 person-years in individuals aged ≥50 years in mainland China, and from 4.04 to 6.89 per 1000 person-years in all ages in Taiwan. As observed in other countries, the incidence of HZ tended to be higher in women than men, and there was evidence of an increase in HZ incidence over time [Citation6,Citation7]. The rate of PHN varied, which is consistent with previous reports finding that PHN incidence rates are affected by study design, age of the population being studied, and the definition used [Citation6]. The observed incidences of PHN are likely to be higher in studies conducted in hospital settings than in community-based or retrospective database studies, given that hospitalized patients with HZ may be more likely to have severe disease, or be older with underlying co-morbidities. The interpretation of community-based surveys is difficult given their propensity for under-reporting and recall bias. Differences in study setting and design will also impact estimates of other complications, as well as the costs associated with HZ. Some findings were unexpected, such as the observation in one study that the use of systemic steroids was strongly associated with a reduced risk of developing HZ [Citation30]. This finding is difficult to interpret given that patients with psoriasis were likely to be receiving other immune-modulating drugs that may have influenced the risk of developing HZ.
The economic burden of HZ varied widely across China, reflecting the differences in study setting, and also potentially health-care systems, treatment practices, and access to drugs and facilities. Traditional medicines and treatments are frequently used in the management of HZ in China, arguing in favor of considering them in economic analyses of the healthcare burden. As expected, costs increased markedly for patients who required hospitalization and for those who developed complicated disease.
China encompasses a vast territory with residents of different ethnicities, and provinces and areas such as Taiwan and Hong Kong have markedly different health-care infrastructures than much of the mainland China. The NHIRD in Taiwan provides a high-quality population-level data source that can provide detailed insights into disease epidemiology, treatment, and outcomes. By contrast, areas of rural China have been surveyed using trained investigators to interview community residents from door-to-door. The heterogeneity in data sources added to regional differences in healthcare infrastructure, and healthcare access is apparent in the wide variability in observed outcomes in the studies we reviewed.
The potential limitations of the systematic review methods include the use of several databases which potentially use different search methods with different logical operators, which could influence the number and completeness of hits obtained. Furthermore, we cannot exclude that publication bias occurred.
5. Expert opinion
The Chinese and English language literature reviewed here suggests that the patterns of HZ disease in China are similar to other parts of the world. Nevertheless, much of the disease burden due to HZ in China remains uncharted, with limited representation of many provinces and differences between rural and urban areas that require further exploration. Studies conducted in Taiwan made use of the NHIRD, a comprehensive country-wide database that is used extensively in epidemiological research in Taiwan. Very few studies have been conducted in Hong Kong and while there are a considerable number of publications from mainland China, the majority were descriptive hospital-based case series or community surveys that are limited by potential biases and are unable to provide reliable estimates of population incidence rates. There was very high variability in the reported estimates of HZ and PHN. This variability probably arises from a mixture of hospital-based and community-based studies, different definitions of PHN used across studies, and because different age-groups were included in each study, and increasing age is a major risk factor for PHN in patients with HZ [Citation59]. The highest reported PHN incidence of 80.2% in adults aged 75 years and over was probably a result of the study being conducted in an elderly, hospitalized population who might be expected to have severe or complicated disease [Citation33].
Extrapolation of data collected by Li et al. [Citation11] suggests that there are 1.563 million new HZ cases annually in mainland China, with an annual cost of more than 1.3 billion RMB (188 million USD). In the United States, Yawn et al. estimated 1 million new HZ cases each year accounting for annual costs of 1.1 billion USD [Citation60]. A review in Europe demonstrated the economic burden associated with HZ disease in five countries, Sweden, Germany, Italy, United Kingdom (UK), and France. Annual costs varied between approximately 51 million euros in Italy, to 271 million euros in the UK [Citation61]. However, these costs cannot be directly compared given the vast differences between the health-care systems in place in each country.
Recently, the National Medical Products Administration approved the use of adjuvanted recombinant zoster vaccine (RZV, Shingrix, GSK) in China for use in adults aged ≥50 years to prevent HZ in May 2019. In Phase 3 efficacy trials, RZV showed more than 90% efficacy in preventing HZ and PHN in adults aged ≥50 years, including those aged ≥80 years [Citation43,Citation44]. Widespread use of RZV could, therefore, have major impacts in reducing HZ and the common and debilitating complication of PHN in China. Disease prevention is likely to reduce work absenteeism and improve productivity, with potentially significant economic benefits for the individual, the employer, and the economy. However, understanding the public health impact of vaccination in China will require extensive baseline information about incidence, complication rates, and associated costs. While this information is available in Taiwan and to a lesser extent in Hong Kong, basic information about the disease burden and incidence of HZ and related diseases in mainland China is very limited, and because China has no established effective monitoring system for HZ, detailed epidemiological data cannot be provided in the short term.
The introduction of RZV into China is likely to face several hurdles, such as the expected opportunity cost, which means that HZ vaccine is likely not to be included in a broad national immunization program in the short term. However, targeted vaccination of vulnerable risk groups, such as persons with diabetes, could ensure that these groups benefit from HZ prevention. This systematic literature review is a first step toward mapping out which populations in China could be the primary targets for HZ vaccination. However, more local data are required before evidence-based recommendations on HZ vaccination policy can be made across China.
The combination of China’s large population and the provision of universal health care provides a unique opportunity to develop large databases that could be used to answer important questions about disease epidemiology, treatment, and outcome. The development of electronic record based ‘big data’ in China, which can provide population-based health and medical behavior information, is being actively pursued through government and academic initiatives. Even though significant challenges remain in terms of harmonization of data collection systems, such data will eventually make an enormous contribution to our understanding of disease [Citation45]. In the interim, identification of target groups likely to benefit most from HZ vaccination in China is needed, and well-designed observational studies are needed to quantify the impact of vaccination after its introduction. Additionally, knowledge, understanding, and attitudes of Chinese people toward HZ and HZ vaccination, and the role of traditional Chinese medicines in HZ treatment would also contribute valuable information to the approach to HZ management in China.
This systematic literature review provides a solid starting point for initial HZ vaccination policy review and points to existing knowledge gaps that warrant further investigation for future recommendations. The search in Chinese literature databases added substantially to the quantity of evidence we identified. We recommend that future systematic reviews of the literature give serious consideration to the inclusion of non-English data sources, regardless of the topic under investigation.
Article highlights
We searched English and Chinese databases in a systematic literature review of the burden of disease and costs associated with HZ in China.
The annual incidence of HZ ranged from 2.9 to 5.8 per 1000 person-years in individuals aged ≥50 years in mainland China, and from 4.04 to 6.89 per 1000 person-years in all ages in Taiwan, which is similar to incidence rates in other countries.
Traditional medicines and treatments are frequently used in the management of HZ in China, arguing in favor of considering them in economic analyses of the healthcare burden.
This systematic literature review provides a solid starting point for initial HZ vaccination policy review in China.
Declaration of interest
A Marijam, D Van Oorschot, D Saha, H Tang, J Diaz-Decaro, NJiang, Z Wu, Y He, and P Watson are employees of the GSK group of companies. A Marijam, D Saha, D Van Oorschot, and P Watson hold shares in the GSK group of companies. Y Feng reports personal fees from the GSK group of companies outside the submitted work. D Yin, X Xie, and Y Ren report no conflicts of interest.
Reviewer disclosures
A reviewer on this manuscript has disclosed that they received grants from Sanofi Pasteur MSD, GSK Biologicals SA, Pfizer, Sanofi Pasteur, MSD Italy, Emergent BioSolutions, and Seqirus for taking part to advisory boards, expert meetings, for acting as speaker and/or organizer of meetings/congresses and as principal investigator and chief of O.U. in RCTs. Peer reviewers on this manuscript have no other relevant financial or other relationships apart from those disclosed.
Supplemental Material
Download PDF (488.1 KB)Acknowledgments
The authors would like to thank Yanfei Yuan for his input and review. The authors would like to thank Business & Decision Life Sciences platform for editorial assistance, writing support, and manuscript coordination, on behalf of GSK. Maxime Bessières coordinated manuscript development and editorial support.
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
References
- World Data Atlas. Total population aged 50 and over years. [cited 2020 Feb 03]. Available from: https://knoema.com/atlas/China/topics/Demographics/Age/Population-aged-50-years.
- Fang EF, Scheibye-Knudsen M, Jahn HJ, et al., A research agenda for aging in China in the 21st century. Ageing Res Rev. 2015;24(Pt B):197–205.
- Watson PN. Postherpetic neuralgia. BMJ Clin Evid. 2010:0905.
- Johnson RW, M-J A-P, Bijl M, et al. Herpes zoster epidemiology, management, and disease and economic burden in Europe: a multidisciplinary perspective. Ther Adv Vaccines. 2015;3(4):109–120.
- Warren-Gash C. Herpes zoster: epidemiological links with stroke and myocardial infarction. J Infect Dis. 2018;218(suppl_2):S102–S106.
- Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4(6):e004833. Epub 2014/ 06/12.
- Yawn BP, Gilden D. The global epidemiology of herpes zoster. Neurology. 2013;81(10):928–930.
- Chen LK, Arai H, Chen LY, et al. Looking back to move forward: a twenty-year audit of herpes zoster in Asia-Pacific. BMC Infect Dis. 2017;17;(1):213.
- Zhu Q, Zheng H, Qu H, et al. Epidemiology of herpes zoster among adults aged 50 and above in Guangdong, China. Hum Vaccin Immunother. 2015;11(8):2113–2118. Epub 2015/ 05/29.
- Lu L, Suo L, Li J, et al. A retrospective survey on herpes zoster disease burden and characteristics in Beijing, China. Hum Vaccin Immunother. 2018;14(11):2632–2635. Epub 2018/ 07/31.
- Li Y, An ZJ, Yin DP, et al. Disease burden due to herpes zoster among population aged ≥50 years old in China: a community based retrospective survey. PLoS One. 2016;11(4):e0152660.
- Wu PY, Wu HD, Chou TC, et al. Varicella vaccination alters the chronological trends of herpes zoster and varicella. PLoS One. 2013;8(10):e77709. Epub 2013/11/10.
- Wu CY, Hu HY, Huang N, et al. Do the health-care workers gain protection against herpes zoster infection? A 6-year population-based study in Taiwan. J Dermatol. 2010;37(5):463–470. Epub 2010/ 06/12.
- Jih JS, Chen YJ, Lin MW, et al. Epidemiological features and costs of herpes zoster in Taiwan: a national study 2000 to 2006. Acta Derm Venereol. 2009;89(6):612–616. Epub 2009/ 12/10.
- Lu WH, Lin CW, Wang CY, et al. Epidemiology and long-term disease burden of herpes zoster and postherpetic neuralgia in Taiwan: a population-based, propensity score-matched cohort study. BMC Public Health. 2018;18(1):369. Epub 2018/ 03/21.
- Chao DY, Chien YZ, Yeh YP, et al. The incidence of varicella and herpes zoster in Taiwan during a period of increasing varicella vaccine coverage, 2000-2008. Epidemiol Infect. 2012;140(6):1131–1140. Epub 2011/ 09/13.
- Lin YH, Huang LM, Chang IS, et al. Disease burden and epidemiology of herpes zoster in pre-vaccine Taiwan. Vaccine. 2010;28(5):1217–1220. Epub 2009/ 12/01.
- Ke CC, Lai HC, Lin CH, et al. Increased risk of herpes zoster in diabetic patients comorbid with coronary artery disease and microvascular disorders: a population-based study in Taiwan. PLoS One. 2016;11(1):e0146750–e0146750.
- Yang F, Yu S, Fan B, et al. The epidemiology of herpes zoster and postherpetic neuralgia in China: Results from a cross-sectional study. Pain Ther. 2019;8:249-259.
- Liao TL, Lin CH, Chen HH, et al. Significant associations of neurological complications of herpes zoster with stroke in rheumatoid arthritis patients. J Am Heart Assoc. Epub 2017/ 07/21. 2017;6(7). doi:10.1161/JAHA.117.006304
- Lin SY, Liu JH, Lin CL, et al. A comparison of herpes zoster incidence across the spectrum of chronic kidney disease, dialysis and transplantation. Am J Nephrol. 2012;36(1):27–33.
- Wu MY, Hsu YH, Su CL, et al. Risk of herpes zoster in CKD: a matched-cohort study based on administrative data. Am J Kidney Dis. 2012;60(4):548–552. Epub 2012/ 05/12.
- Chen HH, Lin IC, Chen HJ, et al. Association of Herpes zoster and type 1 diabetes mellitus. PLoS One. 2016;11(5):e0155175–e0155175.
- Peng YH, Fang HY, Wu BR, et al. Adult asthma is associated with an increased risk of herpes zoster: a population-based cohort study. J Asthma. 2017;54(3):250–257. Epub 2016/ 07/14.
- Lai SW, Lin CL, Liao KF. Real-world database investigating the association between diabetes mellitus and herpes zoster in Taiwan. Medicine (Baltimore). 2019;98(18):e15463.
- Liao CH, Chang CS, Muo CH, et al. High prevalence of herpes zoster in patients with depression. J Clin Psychiatry. 2015;76(9):e1099–1104. Epub 2015/ 10/13.
- Chen JY, Cheng TJ, Chang CY, et al. Increased incidence of herpes zoster in adult patients with peptic ulcer disease: a population-based cohort study. Int J Epidemiol. 2013;42(6):1873–1881.
- Yang YW, Chen YH, Lin HW. Risk of herpes zoster among patients with psychiatric diseases: a population-based study. J Eur Acad Dermatol Venereol. 2011;25(4):447–453. Epub 2010/ 07/30.
- Chen YH, Rau RH, Keller JJ, et al. Possible effects of anaesthetic management on the 1 yr followed-up risk of herpes zoster after Caesarean deliveries. Br J Anaesth. 2012;108(2):278–282. Epub 2011/ 12/14.
- Tsai SY, Chen HJ, Lio CF, et al. Increased risk of herpes zoster in patients with psoriasis: a population-based retrospective cohort study. PLoS One. 2017;12(8):e0179447.
- Hsu CY, Chen PR, Chen HJ, et al. Association between radical prostatectomy and risk of herpes zoster. Eur J Clin Microbiol Infect Dis. 2017;36(2):337–342.
- 刘太华, 张忠奎, 许泽娟, et al. 带状疱疹临床流行病学分析. 西南军医. 2005;06:28–30.
- 龙竹青. 老年带状疱疹患者神经性疼痛并发症的相关危险因素. 中国医学创新. 2013;36:87–088.
- Li L, Wang H, Shen L, et al. Early application of salvia miltiorrhiza at huatuojiaji points reduces incidence of post-herpetic neuralgia. Int J Clin Exp Med. 2018;11(7):7216–7223.
- Tsai TF, Yao CA, Yu HS, et al. Herpes zoster-associated severity and duration of pain, health-related quality of life, and healthcare utilization in Taiwan: a prospective observational study. Int J Dermatol. 2015;54(5):529–536. Epub 2014/ 09/12.
- 孔宇虹, 李元文, 杨碧莲, et al. 带状疱疹后遗神经痛发病相关因素流行病学分析. 环球中医药. 2014;7(12):909–914.
- Zhai XY, Cheng RY, Kong LT, et al. A study on the connection between the incidence of postherpetic neuralgia and serum ionized calcium. Chin Med J. 2015;128(22):3106–3108. Epub 2015/ 11/27.
- 尚辉辉. 老年人带状疱疹临床特点分析. 人民军医. 2005;9:506–508.
- 邱海霞, 蔡小嫦, 王南. 老年带状疱疹78例临床特点分析. 暨南大学学报(自然科学与医学版). 2002;6:97–98.
- 陈燕, 丁小洁, 陈星, et al. 老年带状疱疹后遗神经痛的发病因素分析及预防. 老年医学与保健. 2018;24(5):494–496.
- 夏永江. 3种不同抗病毒药物治疗带状疱疹的药效经济学分析. 临床合理用药杂志. 2015;32:70–71.
- 徐志毅. 3种抗病毒药物治疗带状疱疹的药物经济学分析. 国际医药卫生导报. 2004;10(10):103–105.
- 杨嘉永. 阿昔洛韦与盐酸伐昔洛韦治疗带状疱疹的成本-效果分析. 海峡药学. 2005;17(2).
- 揭金阶. 氨酚羟考酮片与布洛芬缓释胶囊治疗带状疱疹后遗神经痛的疗效与药物经济学分析. 山西医药杂志. 2009;38(13):670.
- 李林泉. 不同抗病毒药物对带状疱疹的药效经济学研究. 国际病毒学杂志. 2015;22(1):58–62.
- 杨惠妮. 带状疱疹中西医学疾病特征及相关资料横断面研究 [硕士]. 广州中医药大学; 2010.
- 陈富超, 于琳, 李鹏, et al. 两种用药方案治疗带状疱疹的药物经济学评价. 中国医药. 2009;4(12):990–991.
- 隗祎, 吴惠琍, 秦立模. 三种糖皮质激素治疗带状疱疹神经痛的经济学评价. 复旦学报(医学版). 2004;31(1):78–80.
- Li XW, Yang YK, Xie XM, et al. Economic evaluation of treating herpes zoster with various methods of acupuncture and moxibustion. J Tradit Chin Med. 2012;32(1):125–128.
- 徐运安. 中西药不同方案治疗带状疱疹的成本_效果分析. China Pharm. 2005;16(1):37–38.
- 王红增, 吴明. 北京市西城区带状疱疹就诊患者直接经济负担研究. 国际病毒学杂志. 2017;24(4):242–247.
- 高士锐, 马玉杰, 孙兆丹, et al. 宁安市带状疱疹发病的回顾性调查. 中国公共卫生管理. 2017;33(3):308–309+315.
- Ming WK, Yu WY, Tsang OTY, et al. Economic analysis of herpes zoster in a hospital setting in Hong Kong. Acta Derm Venereol. 2019;99(6):616–617.
- You JHS, Ming WK, Lee CF, et al. Potential cost-effectiveness of adjuvanted herpes zoster subunit vaccine for older adults in Hong Kong. Vaccine. 2018;36(31):4610–4620. Epub 2018/ 07/01.
- 解放. 305例带状疱疹住院患者病例回顾性研究 [硕士]. 辽宁中医药大学; 2014.
- 王靓轩, 卢益萍. 75例带状疱疹患者临床回顾性分析. 现代中医药. 2018;38(2):57–59.
- 倪阳, 王甦平, 龚睿婕, et al. 带状疱疹的临床路径实施效果评价研究. J Shanghai Jiao Tong Univ Med Sci. 2014;34(5):736–740.
- 丁杨峰, 涂法钢, 易雪梅. 带状疱疹临床路径诊疗经济学分析. 中国麻风皮肤病杂志. 2014;30(2):99–101.
- Forbes HJ, Thomas SL, Smeeth L, et al. A systematic review and meta-analysis of risk factors for postherpetic neuralgia. Pain. 2016;157(1):30–54.
- Yawn BP, Itzler RF, Wollan PC, et al. Health care utilization and cost burden of herpes zoster in a community population. Mayo Clin Proc. 2009;84(9):787–794.
- Gater A, Uhart M, McCool R, et al. The humanistic, economic and societal burden of herpes zoster in Europe: a critical review. BMC Public Health. 2015;15:193.
- 严昆. 523例带状疱疹临床流行病学分析. 中国实用医药. 2014;9(35):81–82.
- 张源, 王青, 张腾. 带状疱疹202例临床分析. 中国社区医师. 2016;32(13):123+125.
- Chen D, Li H, Xie J, et al. Herpes zoster in patients with systemic lupus erythematosus: clinical features, complications and risk factors. Exp Ther Med. 2017;14(6):6222–6228. Epub 2017/ 12/30.
- 徐刚, 鄢素华, 黄玉玲. 带状疱疹并发症分析. 中国麻风皮肤病杂志. 2001;17(3):180–181.
- 钟婷婷, 罗茂, 许飏. 带状疱疹后脑卒中21例临床分析. 广东医学. 2016;37(19):2924–2926.
- 赵凤琴. 前额眼睑带状疱疹眼球并发症的分析. 中国眼耳鼻喉科杂志. 2006;6(3):185.
- Chen JY, Wang LK, Feng PH, et al. Risk of shingles in adults with primary Sjogren’s syndrome and treatments: a nationwide population-based cohort study. PLoS One. 2015;10(8):e0134930.
- Wang WY, Liu SH, Lin MY, et al. Initial presentation sites as predictors of herpes zoster complications: a nationwide cohort study. PLoS One. 2016;11(10):e0164019.
- Chan DYW, Edmunds WJ, Chan HL, et al. The changing epidemiology of varicella and herpes zoster in Hong Kong before universal varicella vaccination in 2014. Epidemiol Infect. 2018;146(6):723–734. Epub 2018/ 03/13.