
ABSTRACT
Child and adolescent psychology and psychiatry healthcare guidelines recommend a structured clinical assessment of conscience of juveniles displaying antisocial behaviour to substantiate the allocation of treatment or penal sanctions. The scientific literature on conscience development is accumulating, yet no widely accepted, integrative clinical instrument for assessment of conscience is available. Consequently, clinicians assess conscience, utilising their acquired knowledge and experience. Resulting in a largely intuitive process that varies vastly among professionals. This study aimed to gather and explicate the implicit knowledge of experienced clinicians on the assessment of adolescent conscience. Semi-structured interviews were conducted with seven clinical experts working in various Dutch (forensic) mental health organisations. Using a five-phase systematic and structured content analysis, the framework method was applied to explore the techniques and concepts used by clinical experts. The concepts they used grossly matched the concepts found in the literature. We identified three pivotal domains: empathic capacity, self-conscious emotions, and moral reasoning. Moreover, the data suggested to consider these domains expressing the overarching concept of self-image or identity. These results will enable the design of a clinically based, comprehensive instrument to improve the quality of the assessment of conscience in the context of child and adolescent forensic psychiatric healthcare.
KEYWORDS:
1. Introduction
In the field of child and adolescent (forensic) psychiatric and psychological healthcare, theoretical knowledge about the development of conscience in children and adolescents has grown substantially over the past decades (Frick et al., Citation2014; Goffin et al., Citation2020; Killen & Smetana, Citation2014; Verkade et al., Citation2020). In the psychological assessment of delinquent juveniles for the indication of (enforced) treatment interventions and advise about accountability in the judicial context, an assessment of conscience is warranted in many countries (e.g., for the Netherlands, see NIFP, Citation2020; Richtlijn Nederlands Jeugdinstituut, Citation2013). Moreover, current guidelines for the general psychiatric assessment of children and adolescents recommend the assessment of conscience, especially in the case of behavioural problems (Doreleijers et al., Citation2015; King, Citation1997). However, in daily clinical practice, clinicians are challenged with regard to the assessment of conscience because clinical instruments are sparse. As a consequence, clinicians base the assessment of conscience on the implicit knowledge that they have collected during years of training and daily practice. Therefore, the assessment remains a largely intuitive process that varies vastly among professionals (Hillege et al., Citation2018). The current project was conducted to analyse the concepts used in the assessment of conscience in adolescence in (forensic) mental healthcare. This paper describes the first step in the larger project of aiming at the development of an instrument for a structured clinical assessment. We explored the perspectives of clinical experts on the concepts and assessment of conscience by making their implicit knowledge explicit and accessible. By interviewing clinical experts, we examined their assessment methods and identified their underlying implicit theoretical constructs. Potentially, this clinical knowledge can be used in the construction of a new, clinically based instrument. Thereby, helping clinicians to profit from this expert knowledge and standardise the assessment of conscience.
1.1 Theoretical perspectives
We briefly outline the theoretical perspectives of conscience. In a review of scholar’s perspectives on conscience it is shown that over time different factors are centralised. For instance, Kohlberg’s (Citation1984, Citation1958) moral stage theory centralises the factor of moral cognitive reasoning. First, children start at a pre-moral level in which external consequences guide their action. Then, growing older, the child wants to adhere to conventions. Lastly, at the level of autonomous morality, internalised principles guide the child’s actions (Gibbs, Citation2019). In clinical assessment the level of maturation of moral reasoning can be assessed using the semi-structured interview Sociomoral Reflection Measure – Short (Brugman e.a., Gibbs et al., Citation1992). However, it challenges the clinician to identify reasons why adolescents often behave at a lower level than they have matured into (De Castro et al., Citation2012). The model of social adjustment helps to understand this gap (Dodge, Citation1980, Citation1985). Attributing negative intentions to others may cause one to display antisocial behaviour and therefore social information processing skills are considered important for the functioning of conscience (Crick & Dodge, Citation1994). Clinicians can/do also use the How I Think Questionnaire (Barriga et al., Citation2001; Nas et al., Citation2008) to assess cognitive distortions such as self-centring and blaming others.
Social psychology focuses on the factor empathy in the theory of conscience. Cuff et al. (Citation2016) proposed the following definition: ‘Empathy is an emotional response (affective), dependent upon the interaction between trait capacities and state influences. Empathic processes are automatically elicited but are also shaped by top-down control processes. The resulting emotion is similar to one’s perception (directly experienced or imagined) and understanding (cognitive empathy) of the stimulus emotion, with the recognition that the source of the emotion is not one’s own’ (p. 150). In a healthy functioning conscience, an empathic reaction to the suffering of another propels prosocial behaviour, such as voluntarily helping another person and withholding behaviour that hurts others (Hoffman, Citation1970, Citation2000). Empathy and externalising conduct problems are often negatively associated from childhood onward (Paz et al., Citation2021). In addition, a lack of affective empathy is considered a key characteristic of callous and unemotional psychopathic traits (Chabrol et al., Citation2011).
Exploring perspectives further, other theories of conscience have centralised moral emotions (Cole et al., Citation1992; Eisenberg et al., Citation1994). Social and evolutionary psychology maintain that moral emotions have a strong social function: they are assumed to promote pro-social behaviour and inhibit anti-social behaviour. In the psychoanalytic approach of conscience, emotions such as shame and guilt are experienced when inner norms and values are violated (Schalkwijk, Citation2015). The moral emotions are called self-conscious emotions, because they evaluate the self and conscience is associated with self-esteem and identity. Be that as it may, to assess conscience from this perspective, the clinician assesses the proneness to experience self-conscious emotions and how they are (not) guiding behaviour. The Thematic Apperception Test (Edner et al., Citation2020) is available for this approach.
Over time, more comprehensive theoretical frameworks have been developed that integrate two or more components from the aforementioned theoretical perspectives. For example, Thompson et al. (Citation2010) defined a guilty conscience and empathy as the primary concepts. Others provide the idea of conscience as a self-regulating system based on cognitive, behavioural, and emotional factors (Goffin et al., Citation2020). Recently, Schalkwijk proposed a model of conscience in which the domains of moral reasoning, the capacity for empathy, and the proneness to experience self-conscious emotions are integrated (Schalkwijk, Citation2015; Schalkwijk et al., Citation2014). Reframing psycho-dynamic theory, he argues that conscience is a psychic function that guards the self and self-esteem. It functions like the thermometer of an air conditioning system: it activates when the room temperature deviates from the pre-set temperature. In the same way, conscience comes out of its standby state when the habitual level of self-esteem is threatened. When the actual level exceeds the habitual level, pride is experienced, but when it descends to a lower level, shame, embarrassment, or guilt is experienced. The psychic input for the conscience activity is based on the capacity to be empathic, the level of moral development, and the proneness to experience self-conscious emotions. Therefore, to assess conscience, clinicians should collect information on the (dis)functioning of these three domains. Schalkwijk’s integrative model approximates the concept of conscience as a self-regulating system based on cognitive, behavioural, and emotional factors (Kochanska, Citation1991). However, to this moment no clinical instrument exists to assess this integrative model of conscience.
1.2 The current study
Without the availability of a clinical instrument that covers the integrative model of conscience, the clinical practice of assessing conscience remains a largely implicit process by the clinician (Le Sage, Citation2015; Schalkwijk, Citation2015). Consequently, there is variance in; the referral and tailoring of treatment and the advisal of criminal accountability for juveniles displaying misconduct. Therefore, analysis and dissemination of existing clinical experience is useful for improving the quality of assessment of conscience, but also an important stepping-stone for developing an integrative clinical instrument. Therefore, we set out to collect the knowledge of clinical experts, who, we assumed, would have integrated the rich knowledge of the existing literature into their daily practice. Furthermore, our aim was to make their implicit theory about conscience assessment explicit. More precisely, our aim was to identify (1) how the experts conceptualised adolescent conscience and (2) how they gathered information for conducting the assessment.
2. Method
2.1 Participants
To ensure a clinically based perspective on concepts and assessment of conscience, a basic set of criteria for the selection of participants was met: (a) to have spent a minimum of 10 years conducting psychological child and adolescent (forensic) assessment (b) to be actively engaged in the practice of clinical (forensic) child and adolescent psychiatry and psychology at the time of the study. To find eligible participants (‘clinical experts’), the Dutch Institute of Forensic Psychiatry and Psychology (NIFP) and Levvel, Academic Centre for Child and Adolescent (forensic) Psychiatry were approached. Experts were sampled through purposive sampling (Boeije, Citation2014) based on the pre-set criteria. Of the experts that were approached, all agreed to participate in the study (N = 7; male = 4, female = 3). The mean age of the experts was 51.76 years (range 42–64 years, SD = 11), and the mean years of working experience was 20 years (range 15–39, SD = 10). The sample consisted of clinical psychologists (n = 6) and a child and adolescent psychiatrist. All of them had experience in mental health services with forensic expertise (children aged 6–18), and four worked for the NIFP (adolescents aged 12–24).
2.2. Design and procedure
In this explorative study, we chose a methodology based on grounded theory, which addresses knowledge gained through a systematic analysis of data (Green & Thorogood, Citation2018). The study was approved by the ethical commission of the University of Amsterdam (project number: 2020-CDE-12228).
Between September and December 2019, seven experts were interviewed individually. Interviews were held at the experts’ place of choice in which privacy measures were taken. Semi-structured interviews were conducted by two members of the research group: a researcher/psychologist with training in qualitative research methods (JT) and an auditor, psychoanalyst, former forensic reporter, and extraordinary professor of conscience development (FS).
Prior to the study and based on the literature review, a topic list () was compiled, reviewed, and approved by other qualitative researchers. The main structure of the interview was for the expert to think back to their last assessment of conscience, allowing them to get into the topic (Boeije, Citation2014). Subsequently, the expert was asked to describe in-depth how the assessment was deployed, expounding on the methods and techniques used, and elaborating on the targeted concepts. The interview strategy chosen was an in-depth analysis in which the interviewer strives for clarification, elaboration, and motivation with a focus on grounding the answers in practice as much as possible (Green & Thorogood, Citation2018). The interviewer would only introduce subsequent topics if they had not been mentioned before. The interviews, 60–90 min in duration, were digitally audio-recorded and transcribed verbatim.
Table 1. Assessment of conscience development; topic list for semi-structured interviews with experts.
2.3 Analysis
The qualitative methodological approach used in this study was a framework analysis. This five-phase systematic and structured content analysis method includes data familiarisation, thematic analysis, indexing, charting, and mapping and interpretation (Green & Thorogood, Citation2018). First, the researcher became immersed in the data by listening and rereading the transcripts. In the next stage, the interviews were sorted by adding codes to the statements, exploring patterns, and actively grouping codes under a higher-level construct that pertained to the research question. This process made recurrent themes salient and provided the basis for a coding scheme (thematic analysis). The auditor (FS) reviewed the scheme for interpretive value and precision. Recommended changes were implemented, and codes were adopted and defined. The transcripts were imported into the computer program ATLAS-ti for qualitative analysis, where the coding scheme was systematically applied to the data (indexing). JT and FS coded all interviews independently and compared the results until a consensus was reached. When new themes emerged, new codes were formed or other codes merged, and through this process of abstraction and synthesis, a rudimentary thematic framework was constructed. After six interviews, no new themes emerged from the experts’ narratives, suggesting a saturation of the data (Boeije, Citation2014). The data were then rearranged according to thematic content (charting), facilitating an overview of the range of data across cases and under themes. In the final phase, the developing thematic framework and its potential new themes were discussed in the research group by means of constant comparison. Finally, the thematic framework was subjected to respondent validation. In the member-check meetings, the interviewed experts provided feedback. The feedback was used in the process of thematic framework development (mapping and interpretation). In the results section, an ordered presentation of the experts’ conceptual knowledge of conscience and their ways of seeking information to make a factual assessment is included.
3. Results
In this section, we present the identified conceptual domains of conscience in clinical practice and their methods for assessment. The clinical experts spoke extensively about empathic capacity. Therefore, empathic capacity was identified as the first domain and is presented most elaboratively. The second identified domain was self-conscious emotions; pride, shame, and guilt were correlated with empathic activity. The third domain identified from the data was moral reasoning. Conceptually, the clinical experts deemed self-conscious emotions to be important, but barely mentioned methods of assessing them, leaving this part less thoroughly described. Consequently, the domains of self-conscious emotions and moral reasoning are presented in less detail.
3.1 Domain I: empathic capacity
All of the clinical experts conceptually associated conscience with the capacity for empathy. Some maintained that with the description of the client’s capacity for empathy and the assessment of conscience would be mostly covered, while others assumed that empathy is only one of the constituents of conscience. The experts assumed that virtually everyone has the potential for empathy, but that it requires a sufficiently secure attachment with the caregiver for this capacity to mature. Provided it has matured, the capacity for empathy is always available, but the empathy experienced or showed is a phenomenon that manifests itself only temporarily. The quote of an expert illustrates how, like a switch, the empathic activity can be alternated in specific situations:
A mother told me, “I know he loves us and wants to do good, but when this switch is flicked, we cease to exist and we’re not taken into account anymore.”
Empathic activity is affected by factors such as substance use and trauma. The clinical experts who mainly report for justice purposes were more inclined to assess the absence of empathic activity (in crime situations), whereas experts who primarily worked as therapists were more inclined to observe and describe empathic activity anywhere it presented itself. For the collection of diagnostic information about empathic capacity, the clinical experts referred to clinical interviews, (play) observation, and testing.
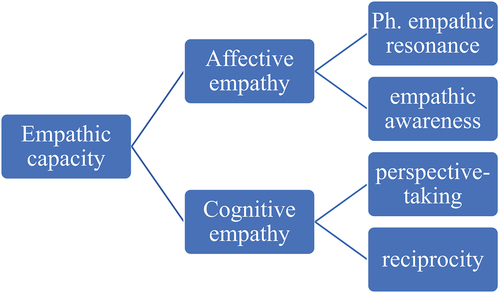
We found that all of the clinical experts differentiated between affective and cognitive empathy (; italics are used when the concept is part of the figure), as many theories of empathy have emphasised these separable components (Blair, Citation2005). Affective empathy was broken down into two practically useful concepts: physical empathic resonance and empathic awareness. Signs of physical empathic resonance are looked for in spontaneous reactions to unexpected situations in a shared experience. Is there some kind of visceral emotional reaction to, say, an accident in the conversation room or at play, or a loud noise outside, or does it go by unattended? Does the client describe discomfort in immoral situations, or does he/she appear to be (socially) imperturbable? In hetero-anamnesis, do parents describe that nothing seems to affect their child or that their child is easily emotionally affected by something outside themselves?
Figure 1. Clinically relevant concepts in the assessment of conscience: the domain of empathic capacity.
As an instrument, the experts used countertransference to estimate the empathic awareness of the client. For instance, when the client is asked to describe a situation of transgressive behaviour, does the story evoke feelings of compassion in the expert or does is leave the expert unaffected? This quote illustrates the incongruency of verbal and nonverbal signals of the client:
He told me something awful, while smiling.
The expert looks for congruent signs of compassion regarding the victim or towards the parents or siblings. Clinical experts considered affective empathy to be based on very early emotion regulation development, making it difficult to acquire later in life.
In addition, cognitive empathy was considered to have two practically useful concepts: perspective-taking and reciprocity. In perspective-taking, the expert describes the client’s ability to understand that their behaviour affects the well-being of others. Cues that suggest this ability are the point of view from which a situation is described. Is it solely from his/her own point of view or does it alternate with the minds of others? Clinical experts also use themselves as instruments to verify whether the client is considerate of the expert’s mind. If this is suggested, does the client use this information to fine-tune his/her own behaviour in a pro-social or anti-social manner, or does the client show rigidity? These signals provide information about the extent to which the client can understand that their behaviour affects the well-being of others. The ability to (adequately) display socially desirable behaviour is a characteristic of cognitive empathy.
In reciprocity, the expert describes the ability to convert cognitive empathy into taking account of the other person and to temporarily set aside personal needs. Indications show that the client adapts his/her own behaviour to the (possibly incompatible) needs of the other. Can the client temporarily negate his/her own needs in favour of the other and how does the client cope with there being no absolute justice in day-to-day experiences? For instance, can the client see the rules set by their parents as a sign of concern? This quote illustrates how the expert gathers information about the client’s obedience to (legitimate) authority:
I hear it in the way clients talk about school. A sign of a premature conscience is how easily they get offended when corrected by the teacher.
For example, when the client is only concerned with how the teachers’ correction devaluates his self-esteem. Conversely, when the expert observes that the client is motivated to take the other into account, even at the expense of oneself, an interplay of affective and cognitive empathy is suggested. The experts believed that in the case of suboptimal child-rearing conditions, cognitive empathy can be acquired later in life through active learning. It is considered an effective behaviour inhibitor when challenged in situations of seduction.
3.2 Domain II: self-conscious emotions
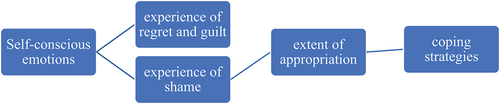
As briefly mentioned in the introduction to this section, most of the experts considered self-conscious emotions as a derivative of empathic activity. They spoke of pro-social emotions to which they attributed an inhibitory effect on antisocial behaviour and a facilitative effect on conscientious behaviour. The clinical experts explicitly mentioned regret, guilt, and shame as important to the assessment of conscience (). They look at the propensity to experience these self-conscious emotions in different contexts and towards different people and observe the extent to which self-conscious emotions are genuinely experienced and appropriated. In this endeavour, they are specifically aware of the coping strategies used.
Figure 2. Clinically relevant concepts in the assessment of conscience: the domain of self-conscious emotions.
3.2.1 Shame
A clinical expert is alerted to non-verbal cues of shame when the client is asked to talk about misconduct, such as looking away, lowering the eyes, or speaking softer. Making eye contact can be seen as an expression of a more integrated conscience, whereas defiant or provocative behaviour is presumed to be indicative of a lack of shame. In addition, the use of countertransference is used to estimate the extent to which emotions are heart-felt.
This quote illustrates that addressing the topic of shame can in itself be shame-inducing as it affects the (often vulnerable) self-image and identity of the client:
Of course, the client will deny that completely, it would be a sign of weakness, right? If you feel guilty. The same goes for shame, for they consider themselves not afraid of anything.
Therefore, it requires a tender approach to collect useful clinical information about regret, shame, and guilt. In the clinical interviews, some experts avoided the direct use of terms such as shame and guilt. Instead, more indirect methods were used, like in these illustrative phrases:
Can you think of something you have done that has disappointed your parents?’, ‘What would you never do, even if you’d get a thousand euro?’, and ‘Do you allow people to tease you?
Here the expert assumes that if the client is open about their bad conduct and their concomitant self-conscious emotions, their conscience might be more integrated. However, the expert is aware that clients have a limited vocabulary to express their inner world and help them find the right words for their emotions.
3.2.2 Regret and guilt
In forensic practice, the offender is usually advised to express regret and guilt. Some experts inquire directly about regret and guilt and carefully observe non-verbal information. Is the nonverbal information congruent with the verbal information? Is there an increase in physical tension? Are there signs of appropriation of expressed regret or guilt? Another important focus is to whom self-conscious emotion is experienced: is it in relation to the parents, peers, the victim, and/or the self?
In clinical assessment, the expert pays attention to the different styles of coping with self-conscious emotions. Knowledge of adaptive and maladaptive coping strategies is key to recognising the self-conscious emotions at play without directly observing them. Self-conscious emotions are often a response to a perceived humiliation. Coping strategies are activated to make these negative emotions manageable, like this quote illustrates:
… She had developed all kinds of strategies to not feel quite ashamed or guilty toward her family. To not feel like a failure.
For instance, excessive pride (overcompensation) can be interpreted by experts as a reversal of an intolerable self-conscious emotion such as guilt (or shame). Self-conscious emotion derivatives can be observed in adolescents, such as being alert to one’s behaviour; justifying it via the externalisation of accountability; rationalisation; inflated (narcissistic) self-esteem; a strong sense of justice; commanding respect through bold, insensitive behaviour; and violence. In addition, drug use can function as a pacifier for negative effects. Experts try to consider culture-based differences in the expressions of self-conscious emotions. For instance, cultures that admit moral trespassing are considered worse than denying one’s participation. They assume that there are differences in the utterances of feelings of regret, guilt, and shame among clients from various religious and cultural backgrounds.
3.3 Domain III: moral reasoning
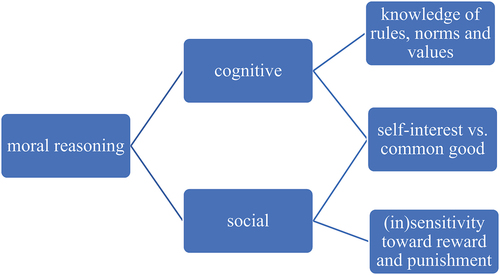
The third identified domain was moral reasoning. Clinical experts use concepts that predominantly contain more cognitive and social components of moral reasoning (). The cognitive perspective is primarily determined by Kohlberg’s cognitive theory. Social-oriented concepts are based on Gibbs’s theory of moral reasoning and social learning. First, the experts test the level of knowledge of rules and agreements, norms, and values by asking the client about his or her (general) ideas, focusing more on the effects of these ideas on their behaviour. This quote illustrates that moral reasoning is multi-layered:
Figure 3. Clinically relevant concepts in the assessment of conscience: the domain of moral reasoning.
The client told me that selling drugs is of no problem as people choose to do drugs themselves, but robbery he would never conduct.
This quote also shows that the expert is uncovering discrepancies in the client’s thoughts. Socially desirable/acceptable answers or behaviours are seen as the ability to apply moral knowledge in social situations. Second, personalised moral dilemmas are used to evaluate the extent to which the client can oversee the effects of his or her (mis)behaviour:
What would you do if you find 100€, and what do you think would happen if you’d take the money to the police station?
Here the expert tries to bring to light the point at which serving the common good is overtaken by self-interest. Usually, the client would say that he or she hands the found money over to the police. By taking the dilemma a step further, the expert examines the willingness to adhere to this behaviour if the conditions change. The expert is aware of signs that indicate whether the client’s motivation to adhere to moral conventions is extrinsically or intrinsically determined. Like adding to the following quote that no one is going to find out:
Suppose you find a bicycle with the keys still in the lock, what would you do?
Extrinsic-motivated adherence to rules is based on wanting to avoid punishment. Intrinsic motivation represents the internalisation of moral conventions that have become part of one’s identity. Or like the expert eloquently stated:
Is the client able not only to adhere to the letter but also to the spirit of the law?
In the assessment, the expert strives to evoke cognitive dissonance within the client, for instance, by being highly normative about the client’s conduct or confronting contradictions in the client’s story. Subsequently, the expert pays close attention to tension regulation and coping strategies while evaluating flexibility in moral reasoning. The expert is interested in moments when the client can refrain from misconduct, and the expert will work to collect information about extrinsic or intrinsic motivation.
… but her mother can leave her wallet unattended.
This quote illustrates that expert is aware that moral evaluation is affected by what the client considers to be an in- or outgroup. The expert therefore takes into account the indications of peer pressure and the client’s identification with certain sub-groups. Like the following quote illustrates:
Within the gang, codes of conduct are strictly enforced.
Experts evaluate the client’s behaviour to be morally foundational when, in principle, it serves society-welfare concerns. The central question is whether and at what point self-interest yields generally accepted norms and values. In addition, a higher level of moral reasoning is assumed when the client is able to conform to those in authority if needed.
From the perspective of social learning, the experts saw their clients’ sensitivity to social rewards and punishment as an important predictor of moral development. Indifference towards social acceptance or rejection is considered less favourable for the development of moral reasoning. With younger adolescents, during free-play, the expert can observe internalised norms and values. Does the client take into account the rules in a boxing game and does he or she stop at the (feigned) pain of the expert? Is the client able to wait for their turn and comply with the rules in a game of ‘4 in a row’? Open cheating can be seen as an indication of social indifference, poor mastery of impulses, or a failure to foresee the consequences of breaking the rules.
4. Discussion
The aim of the present study was to explore the perspectives of clinical experts in the assessment of conscience. We conducted semi-structured interviews which resulted in clinically relevant insights into pivotal concepts and techniques. Following the framework method, three separate and clinically relevant domains of conscience were identified: empathic capacity, proneness to experience and coping with self-conscious emotions, and moral reasoning. The results showed that the clinical experts connected and integrated different perspectives in the academic literature, and this practice is in concordance with the current comprehensive theoretical framework.
Most of the clinical methods the experts used revolved around the clinical interview, but free and structured play was also exercised. While observing, the expert is attentive to non-verbal information and is alert to incongruencies. The experts prefer indirect interviewing or letting the client speak spontaneously, while countertransference is scrutinised. Experts make use of methods to increase emotional pressure (cognitive dissonance); for instance, by being highly normative or confronting the client with inconsistencies in the narrative while closely observing their stress regulation, cognitive flexibility, and (mal)adaptive coping strategies. The use of standardised instruments that the clinicians mentioned was restricted to instruments for personality diagnostics.
In addition to Schalkwijk’s (Citation2015) comprehensive model of conscience, in which a specific domain bears no relative weight, clinicians consider empathic capacity as the most important domain. Two concepts of affective empathy were used: the ability to spontaneously feel another’s emotion (empathic resonance) and feeling what the other person feels after learning the story (empathic awareness). Cognitive empathy was defined by the ability to take another’s perspective (perspective taking) and behaving in accordance with what the person needs, despite one’s own needs (reciprocity). In the literature, empathic resonance is seen as a precursor to real affective empathy, as the characteristic of empathic contagion indicates that both persons experience the same emotion and are not differentiated. Using this concept in assessment suggests that the ability to control such an emotion is key to understanding the development of emotional empathy. In addition, in the literature (Cuff et al., Citation2016), reciprocity is not seen as an empathic activity, but rather as a capacity for interpersonal tuning.
The second identified domain was the proneness to experiencing self-conscious emotions and the way they were coped with. In clinical practice, concepts have different meanings than those in the research literature. For example, when diagnosing a behavioural disorder, clinicians gather information about the presence/absence of regret and guilt (following international diagnostic guidelines or the DSM-5). Regret is considered clinically meaningful, as it can cover a harsher-felt self-conscious emotion like shame. Clinicians consider shame as an important factor, although hardly any client will concede to experiencing shame. Clinicians find it difficult to assess the extent to which the client appropriates self-conscious emotions. Clinicians are more inclined to look for shame in interpersonal situations rather than focusing on intra-psychic shame, and they look for patterns of (inadequate) coping styles. Through the moral identity of the client, the clinician tries to determine the appropriation of shame and guilt (see below).
The third identified domain was moral reasoning. The clinically useful concepts are general knowledge of rules and norms, knowing where self-interest yields the common good, and sensitivity towards social learning. Despite the long tradition of cognitive moral stage theory, Kohlberg’s approach to moral reasoning is hardly mentioned. Instead, clinicians differentiate between intrinsically and extrinsically motivated moral reasoning. Based on the Equip-program (Gibbs, Citation2019), clinicians are confronted with multi-layered situations to find out when they yield their self-interest to the common good; for example, sketching moral dilemmas or looking for cognitive dissonance. Although we are not sure whether this is conceptually the best position, we have put obedience to authority in the realm of moral reasoning. Moral behaviour signals conscience activity; therefore, clinicians consider obedience to (legitimate) authority as an important factor in assessment. Juvenile misconduct can be seen as a cue of internal processes, such as self-centralisation, which leads to immoral behaviour.
How the specific personality of the client has an impact on the identified concepts of conscience is seen by clinicians as a result of a complex interaction of nature, as seen in amygdala reactivity, temperament, or impulsivity, and nurture, as seen in attachment style, parental sensitivity, or macro-contexts like social class. This was not the focus of our research, but the clinician keeps these factors in mind, as they may have an important influence and might lead to limitations in development.
In the integrative model, the function of conscience is considered a safeguard for one’s self-image and self-esteem (Schalkwijk, Citation2014, Citation2015). We were interested in whether the experts would associate empathy with self-image and self-esteem regulation, or rather see it as an isolated, trained skill. Clinicians tended to endeavour to assess conscience as part of the client’s personality, using personality diagnostics to assess this. However, only a few clinicians had assessed the domains of conscience in the service of the identity or self. Furthermore, it appeared that clinicians with a focus on DSM-diagnostics tended to describe developmental deficits, whereas clinicians with a focus on treatment tended to focus on positive developmental assets. Moreover, the results suggested that clinicians focused on empathy as a skill rather than focusing on what it means for the client to be an empathic person. However, in forensic practice, clinicians see that the client maintaining a criminal identity is important for assessment. In this way, clients are attributing criminal activities positively to their criminal identity, leaving the function of the conscience inactivated. This is well documented in the literature of criminology (De Jong, Citation2007) and is in line with Schalkwijk’s (Citation2015) integrative model: As long as self-esteem is not threatened, conscience remains on standby.
This study adds valuable clinical knowledge to the existing literature on the assessment of conscience in child and adolescent psychiatry and psychology. However, some limitations should be considered. First, choosing to conduct semi-structured interviews with clinical experts helped make their implicit knowledge explicit. However, this method may have resulted in the underreporting of self-conscious emotions. The clinical experts focus on adolescents’ externalising behaviour and therefore tend to collect more information on the social self. The self-conscious emotions are used to balance the private self. Of course, the social and private self are concepts that pertain to the overarching concept of self-image and identity. Had the youngsters been assessed for internalising problems (e.g., depression, social anxiety), the focus might have been more on the aspect of balancing self-esteem, the private self.
Second, even though a maximum diversity in participants was aimed at, the study relied on clinical experts who were ready to participate, resulting in coverage of clinical experts from the urban areas of the Netherlands. Despite this limitation, we believe that making this implicit knowledge communal provides an important insight into clinical practice. Hopefully, this will inspire other scientific practitioners to conduct their own studies and encourage us to combine these results.
The material further suggested that clinical experts working as forensic reporters for the judicial courts applied a deficit model, focusing on the lack of conscience of misconducting juveniles. The clinical experts working mainly as therapists, however, seemed to apply a developmental model and focused more on opportunities for change or further development. To determine whether these differences are solid, both groups would need to be studied in greater numbers. We recommend a study of these groups to determine how conscience is assessed in different domains.
The clinical experts stressed the absence of an integrative, clinically useful, structured instrument for the assessment of conscience, thus confirming our idea that such an instrument is missing. Most clinical experts admitted that diagnostics of conscience rely heavily on their clinical experience and little on conceptual knowledge. Therefore, they welcomed the design and construction of instruments for the assessment of conscience.
In conclusion, this study contributes to the improvement of the clinical assessment of conscience in child and adolescent psychiatry and psychology by making the implicit process of clinical experts’ conscience assessment explicit and accessible. Empathic activity, self-conscious emotions, and moral evaluations were identified as the main domains. These domains, along with the presented clinical methods, can guide future clinicians in what and how to address conscience assessment. This is an important step in making the process less intuitive and dependent on the clinician’s experience. The results will be of important input for the construction and development of an instrument for structured clinical assessment. Ultimately, supporting the clinician in the intricate process of assessing, allocating, and treating forensic juveniles and adolescents dealing with behavioural problems.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Barriga, A. Q., Morrison, E. M., Liau, A. K., & Gibbs, J. C. (2001). Moral cognition: Explaining the gender difference in antisocial behavior. Merrill-Palmer Quarterly, 47(4), 532–562. https://doi.org/10.1353/mpq.2001.0020
- Blair, R. J. R. (2005). Responding to the emotions of others: Dissociating forms of empathy through the study of typical and psychiatric populations. Consciousness and Cognition, 14(4), 698–718. https://doi.org/10.1016/j.concog.2005.06.004
- Boeije, H. (2014). Analyseren in kwalitatief onderzoek. Denken en doen. [Analysing in Qualitative research. Thinking and Doing.] (2nd ed.). Boom.
- Chabrol, H., Van Leeuwen, N., Rodgers, R. F., & Gibbs, J. C. (2011). Relations between self-serving cognitive distortions, psychopathic traits, and antisocial behavior in a non-clinical sample of adolescents. Personality and Individual Differences, 51(8), 887–892. https://doi.org/10.1016/j.paid.2011.07.008
- Cole, P., Barrett, K., & Zahn-Waxler, C. (1992). Emotion displays in two-year-olds during mishaps. Child Development, 63(2), 314–324. https://doi.org/10.2307/1131481
- Crick, N. R., & Dodge, K. A. (1994). A review and reformulation of social information processing mechanisms in children’s social adjustment. Psychological Bulletin, 115(1), 74–101. https://doi.org/10.1037/033-2909.115.1.74
- Cuff, B. M. P., Brown, S. J., Taylor, L., & Howat, D. J. (2016). Empathy: A review of the concept. Emotion Review, 8(2), 144–153. https://doi.org/10.1177/1754073914558466
- de Castro, B. O., Verhulp, E. E., & Runions, K. (2012). Rage and revenge: Highly aggressive boys’ explanations for their responses to ambiguous provocation. European Journal of Developmental Psychology, 9(3), 331–350. https://dspace.library.uu.nl/handle/1874/307790
- de Jong, J. D. (2007). Kapot moeilijk. Een etnografisch onderzoek naar opvallend delinquent groepsgedrag. Aksant.
- Dodge, K. A. (1980). Social cognition and children’s aggressive behavior. Child Development, 51(1), 162–170. https://doi.org/10.2307/1129603
- Dodge, K. A. (1985). A social information processing model of social competence in children. In Cognitive Perspectives on children’s social and behavioral development (1st ed., pp. 50). Psychology Press. https://doi.org/10.4324/9781315802343
- Doreleijers, T., Boer, F., Huisman, J., & de Haan, E. (2015). Leerboek psychiatrie kinderen en adolescenten (E. Doreleijers, T. Boer, F. Huisman, & J. de Haan, ed.; 3rd ed.). De Tijdstroom. https://research.vumc.nl/en/publications/leerboek-psychiatrie-kinderen-en-adolescenten
- Edner, B. J., Glaser, B. A., Calhoun, G. B., Dukes-Murray, H., Khan, Z., & Donaldson, K. (2020). Efficacy of the MMPI-A in detecting trauma among delinquent youth: Cross-validation of the Trauma scale for juvenile offenders (TSJO). Journal of Forensic Psychiatry and Psychology, 31(1), 1–16. https://doi.org/10.1080/14789949.2019.1657483
- Eisenberg, N., Fabes, R. A., Murphy, B., Karbon, M., Maszk, P., Smith, M., O’Boyle, C., & Suh, K. (1994). The relations of emotionality and regulation to dispositional and situational empathy-related responding. Journal of Personality and Social Psychology, 66(4), 776–797. https://doi.org/10.1037/0022-3514.66.4.776
- Frick, P. J., Ray, J. V., Thornton, L. C., & Kahn, R. E. (2014). Annual research review: A developmental psychopathology approach to understanding callous-unemotional traits in children and adolescents with serious conduct problems. Journal of Child Psychology and Psychiatry and Allied Disciplines, 55(6), 532–548. https://doi.org/10.1111/jcpp.12152
- Gibbs, J. C., Basinger, K. S., & Fuller, D. (1992). Moral maturity: Measuring the development of sociomoral reflection. Erlbaum.
- Gibbs, J. C. (2019). Moral development and reality: Beyond the theories of Kohlberg, Hoffman and Haidt (4th ed.). Oxford University Press.
- Goffin, K. C., Kochanska, G., & Yoon, J. E. (2020). Children’s theory of mind as a mechanism linking parents’ mind-mindedness in infancy with children’s conscience. Journal of Experimental Child Psychology, 193, 104784. https://doi.org/10.1016/j.jecp.2019.104784
- Green, J., & Thorogood, N. (2018). Qualitative methods for health research. SAGE.
- Hillege, S. L., van Domburgh, L., Mulder, E. A., Jansen, L. M. C., & Vermeiren, R. R. J. M. (2018). How do forensic clinicians decide? A Delphi Approach to identify domains commonly used in forensic juvenile treatment planning. International Journal of Offender Therapy and Comparative Criminology, 62(3), 591–608. https://doi.org/10.1177/0306624X16658724
- Hoffman, M. L. (1970). Carmichael’s handbook of child psychology. In P. Mussen (Ed.), Moral Development (Vol. 2, pp. 261–361). Wiley.
- Hoffman, M. L. (2000). Empathy and moral development: Implications for caring and justice. Cambridge University Press.
- Killen, M., & Smetana, J. G. (Eds.). (2014). Handbook of moral development (2nd ed.). Psychology Press. https://doi.org/10.1080/03057240.2015.1053738
- King, R. A. (1997). Practice parameters for the psychiatric assessment of children and adolescents. American Academy of Child and Adolescent Psychiatry. Journal of the American Academy of Child and Adolescent Psychiatry, 36(Suppl 10). https://doi.org/10.1097/00004583-199710001-00002
- Kochanska, G. (1991). Socialization and temperament in the development of guilt and conscience. Child Development, 62(6), 1379. https://doi.org/10.2307/1130813
- Kohlberg, L. (1958). The development of modes of moral thinking and choice in the years ten to sixteen. University of Chicago.
- Kohlberg, L. (1984). Essays on moral development: The psychology of moral development. Harper & Row.
- Le Sage, L. (2015). De gebrekkige gewetensontwikkeling in het jeugdstrafrecht. Implicaties voor de toerekening en behandeling. SWP.
- Nas, C. N., Brugman, D., & Koops, W. (2008). Measuring self-serving cognitive distortions with the “how I think” questionnaire. European Journal of Psychological Assessment, 24(3), 181–189. https://doi.org/10.1027/1015-5759.24.3.181
- NIFP. 2020. https://www.nifp.nl/actueel/nieuws/2022/04/20/richtlijn-ambulant-forensisch-psychologisch-onderzoek-geactualiseerd
- Paz, Y., Orlitsky, T., Roth-Hanania, R., Zahn-Waxler, C., & Davidov, M. (2021). Predicting externalizing behavior in toddlerhood from early individual differences in empathy. Journal of Child Psychology and Psychiatry and Allied Disciplines, 62(1), 66–74 doi:10.1111/jcpp.13247.
- Richtlijn Nederlands Jeugdinstituut. 2013. https://www.nji.nl/richtlijnen/richtlijn-oppositioneel-opstandige-stoornis-en-gedragsstoornis
- Schalkwijk, F., Stams, G. J., Stegge, H., Dekker, J., & Peen, J. (2014). The conscience as a regulatory function: Empathy, shame, pride, guilt, and moral orientation in delinquent adolescents. International Journal of Offender Therapy and Comparative Criminology, 60(6), 675–693. https://doi.org/10.1177/0306624X14561830
- Schalkwijk, F. (2015). The conscience and self-conscious emotions in adolescence. An integrative approach. Routledge.
- Thompson, R. A., & Newton, E. K. (2010). Emotion in early conscience. In W. F. A., & E. A. Lemerise (Eds.), Emotions, aggression, and morality in children: Bridging development and psychopathology (pp. 13–31). American Psychological Associatio.
- Verkade, M., Karsten, J., Koenraadt, F., & Schalkwijk, F. (2020). Conscience as a regulatory function: An integrative theory put to the test. International Journal of Offender Therapy and Comparative Criminology, 64(4), 375–395. https://doi.org/10.1177/0306624X19881918
