
Abstract
Objectives: To review literature on the use of manual and automatically switching multimemory devices by hearing aid and CI recipients, and to investigate if recipients appreciate and adequately use the ability to switch between programmes in various listening environments. Design: Literature was searched using PubMed, Embase and ISI/Web of Science. Additional studies were identified by screening reference and citation lists, and by contacting experts. Study sample: The search yielded 1109 records that were screened on title and abstract. This resulted in the full-text assessment of 37 articles. Results: Sixteen articles reported on the use of multiple programmes for various listening environments, three articles reported on the use of an automatic switching mode. All studies reported on hearing aid recipients only, no study with CI recipients fulfilled the selection criteria. Conclusions: Despite the high number of manual and automatically switching multimemory devices sold each year, there are remarkably few studies about the use of multiple programmes or automatic switching modes for various listening environments. No studies were found that examined the accuracy of the use of programmes for specific listening environments. An automatic switching device might be a solution if recipients are not able, or willing, to switch manually between programmes.
Introduction
Daily communication takes place in various situations. It has been well documented that in many listening conditions, speech recognition remains a challenge for recipients of a hearing aid or cochlear implant (CI). Not surprisingly, one of the frequently mentioned situations in which hearing aid recipients seek for hearing improvement is the situation in which speech has to be recognised in noise. A device that improves hearing only in specific situations can be expected to have low overall satisfaction ratings, because of the variety in listening environments a hearing-impaired listener experiences during a day (Kochkin Citation2007). Therefore, it is important for recipients of a hearing device that settings are optimally adapted, depending on the specific listening environment, to assure optimal speech recognition.
Current hearing devices allow users to either switch manually or automatically through multiple programmes for various listening environments. In clinical practice, hearing-impaired listeners are regularly fitted with these manual and/or automatically switching devices. These devices often have specific programmes with names each representing a specific listening environment (e.g. “speech in noise” and “music”) and the listener is counselled to use the programmes in these specific listening environments. Despite the fact that these devices are prescribed very often, little is known about the actual need for and use of these functionalities. Therefore, a scoping review was performed to identify the available evidence on the use and appreciation of manual and automatically switching devices.
In the past, analogue hearing aids were fitted with a gain-frequency response based on standard prescription rules. These standard rules were often used as a first fit, followed by individual adjustments. The resulting setting had to be used in every listening environment. Research, however, has shown that recipients can benefit from using different hearing aid settings in different listening environments. Van den Heuvel, Goverts, and Kapteyn (Citation1997) and Ricketts and Bentler (Citation1992) found better speech recognition if recipients had specific hearing aid programmes for listening in quiet and in noise.
Multimemory hearing aids were introduced that support multiple programmes for use in various listening environments (e.g. hearing in a restaurant or public place, enjoying music or using the phone). These devices allow the hearing aid user to choose between programmes with different settings for different listening environments. Programme settings used for different listening environments could include variations in overall gain, different frequency responses, directionality of microphones and noise suppression algorithms. In this scoping review, hearing aids that allow the user to switch between two microphone modes (directional or omnidirectional) are considered multimemory hearing aids as well. In the development of CI speech processors, a technological evolution similar as for hearing aids was observed. Directional and omnidirectional microphones were introduced, followed by multimemory speech processors. Thus, in both types of hearing devices, development resulted in the availability of various programme settings for various listening environments. In the current paper, the term “multimemory devices” is used to refer to all the devices that allow the user to switch manually between programmes. Often terms as “multiprogrammable” or “programmable” devices are used for the same type of devices. With a multimemory hearing device, the user can manually switch between the various programmes as the listening environment changes, either by pressing a button on the device or by using a remote control.
After the development of multimemory hearing aids, devices were introduced that are able to switch between settings based on acoustic scene analysis of the incoming sound. In these devices, the microphone input is analysed by extracting specific signal features, followed by determining the most likely listening environment. Finally, the identified scene is used to decide if and when the current programme has to be changed (Mauger et al. Citation2014). The aim of this device feature is to optimise settings in all listening environments and to minimise user interaction. Recent studies have shown that automatic scene classification and programme selection in CI speech processors can benefit their recipients [see Wolfe et al. (Citation2015) for an overview].
The current scoping review was limited to studies evaluating multimemory devices that allow the user to manually switch between discrete programmes for specific listening environments, and automatically switching devices that use a classifier to differentiate between specific listening environments and alter settings accordingly. The rationale for focussing on devices with specific programmes for specific listening environments is that patients are usually counselled to use a programme in a specific listening environment. The names of these programmes often represent a specific listening environment (e.g. “restaurant” or “music”). Based on current clinical practice, we started the literature search with several assumptions on the use of manual and automatically switching devices. First, we assume that a manual switching multimemory device has added value when the hearing device user is able to characterise listening environments adequately, select the most appropriate programme and that he or she is capable in using the switch button or remote control. However, as listening environments may change rapidly, it seems unrealistic to expect that a user switches manually for every change in listening environment. It is assumed that a specific setting for a specific listening environment (e.g. a programme with directional microphone for conversations in a restaurant) generally provides benefit in terms of speech recognition and listening effort compared to a programme that is not optimal for the same listening environment (e.g. a programme for listening to music). Thus, the possibility to manually switch between settings does not unequivocally guarantee the most optimal setting in each listening condition.
The added value of automatically switching devices is based on the assumption that all hearing device recipients prefer a specific setting in a particular listening environment (i.e. specific settings are fixed for a particular listening environment regardless of a person’s individual preferences). However, it is possible that the signal processing preferred by one individual in a specific environment might not be the preferred option for another individual in the same environment, or an individual might prefer different processing variants in the same acoustic environment, depending on his or her focus of attention in the given environment.
The research questions for the scoping review were:
For multimemory devices (manual switching): Do recipients of hearing aids or cochlear implants use different programmes in various listening environments? If so, do recipients value the possibility to switch between programmes, and do they use the correct programme that is designated for a specific listening environment?
For multimemory devices (manual switching): Which factors influence whether a recipient actually uses multiple programmes?
For automatically switching devices: Do hearing aid and CI recipients value a device that switches automatically between settings, depending on listening environment?
Methods
Scoping review design
The current scoping review follows the methodology for systematic scoping reviews developed by the Joanna Briggs Institute (JBI). Scoping studies are increasingly being used to review the available literature and identify possible gaps in the available evidence (Davis, Drey, and Gould Citation2009; Peters et al. Citation2015). The design of a scoping review differs from that of a systematic review in that it can address broader topics with many different study designs. A scoping review does generally not assess the quality of the included studies (Peters et al. Citation2015) and is less likely to address very specific research questions (Arksey and O'Malley Citation2005). Furthermore, a scoping review adds a narrative integration of the relevant evidence. For the purpose of the current review, it was important that the design allowed inclusion of studies whose primary aim was not related to answering one of our research questions. Therefore, the descriptive style of a scoping review was used to answer the research questions. Given the limited number of studies that met the inclusion criteria, the large differences in study designs and used procedures, the frequent use of subjective measures and differences in outcome measures in the included studies, it was not possible to pool the study findings.
Data sources
A review protocol was developed to search for evidence in various online sources. PubMed, Embase.com and ISI/Web of Science were searched by FDG and JCFK from inception up to 19 April 2016. The following terms were used (including synonyms and closely related words) as index terms or free-text words: “hearing aids” or “cochlear implants” and “multiple programmes” or “settings” or “(omni-)directional microphone” or “environmental or scene classification”. The full search strategy for each database can be found in the Supplemental Digital Content. This procedure yielded articles in English and German, which were all included for further selection.
Study selection
From the results of the search, duplicates were removed, after which titles and abstracts were screened for possible inclusion. The first two authors (FDG and EH) independently reviewed titles and abstracts of all records. Studies that clearly did not meet the inclusion criteria were excluded. Full text articles of the remaining records were assessed for eligibility using the selection criteria described below. An additional search was conducted to identify additional records by reviewing the reference and citation lists of the records already included.
A set of criteria, composed by two investigators (FDG and EH), was used for selection of articles. Inclusion criteria were (a) patient related studies concerning adult hearing aid or CI recipients; (b) studies describing the use of multiple programmes/microphone settings, with manual or automatic selection, in various listening environments; (c) studies describing the patients’ preference for and the appreciation of the use of one or more hearing device settings in various listening environments; (d) studies describing the patients preference for and appreciation of the use of a hearing device that automatically alters settings according to listening environments. Criteria (a) and (b) had to be met, combined with either (c) or (d). Studies including participants outside of the target age range (18 years and older) were excluded unless the mean age fell within the target age range, or the data could be split for separate analysis. Studies in which speech recognition measures were used to solely evaluate the effect of different settings (e.g. gain or fitting rules) on speech recognition were excluded.
Results and discussion
Study characteristics
After removing duplicates, the initial search yielded 1109 articles. Of these, 1072 articles were excluded based on title and abstract, leaving 37 articles for full review. Of these, 13 were included after reading the full-text article. An additional six articles were identified through reference and citation searching, resulting in a total of 19 studies that conformed to the inclusion criteria (). Fourteen of these articles were published in peer-reviewed journals and the remaining five articles were published in non-peer-reviewed journals. The study characteristics of the finally included articles are outlined in .
Figure 1. Study selection process.
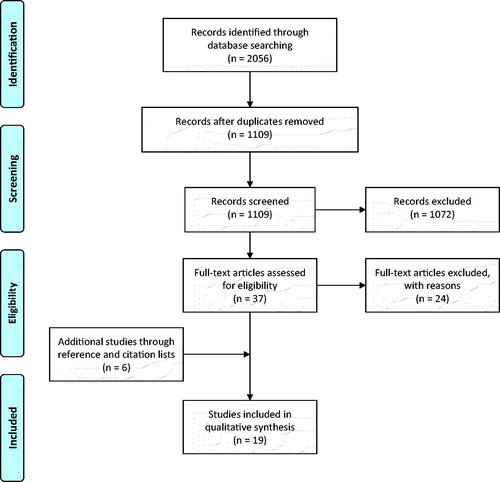
Table 1. Study characteristics.
Overall, 11 studies investigated whether patients use different programmes, depending on the listening environment (Banerjee Citation2011; Berninger and Nordstrom Citation1997; Goldstein, Shields, and Sandlin Citation1991; Keidser Citation1995; Keidser, Dillon, and Byrne Citation1996; Keidser et al. Citation1997, Citation2005; Kuk Citation1992; Ringdahl et al. Citation1990; Stelmachowicz, Lewis, and Carney Citation1994; Van den Heuvel, Goverts, and Kapteyn Citation1997). Five studies investigated the use of different microphone settings for different listening environments (Cord et al. Citation2002; Kuk Citation1996; Palmer, Bentler, and Mueller Citation2006; Ricketts, Henry, and Gnewikow Citation2003; Walden et al. Citation2004). Three studies investigated whether hearing aid recipients value a device that switches automatically between settings according to listening environments (Buechler Citation2001; Gabriel Citation2002; Olson, Ioannou, and Trine Citation2004). Note that all studies that fulfilled our selection criteria reported on recipients of hearing aids only. No studies were found evaluating the use of multiple programmes in recipients of a CI. The results of the included studies were all based on field and laboratorial tests during which subjects reported on the use of different programmes for different listening environments. The majority of the participants in these studies were experienced recipients of hearing aids (). Several studies included participants who already had experience with multiple programmes or were successful recipients of switchable microphones. The age of the participants and the severity of hearing loss varies within and across the included studies. Some additional characteristics of the hearing-impaired participants could be identified, such as “good speech discrimination abilities” and “good oral communication” (Goldstein, Shields, and Sandlin Citation1991; Ringdahl et al. Citation1990), or a very motivated group of hearing-impaired participants (van den Heuvel, Goverts, and Kapteyn Citation1997).
Question 1: for multimemory devices (manual switching): do recipients of hearing aids or cochlear implants use different programs in various listening environments? If so, do recipients value the possibility to switch between programs, and do they use the correct program that is designated for a specific listening environment?
The studies showed that there was no general preference for using different programmes. Some participants used and valued the option to have manual access to multiple programmes in various listening environments, while other hearing aid recipients did not use the option to manually switch between programmes. Stelmachowicz, Lewis and Carney (Citation1994) showed that recipients did not select different settings in five simulated environments. In a study by Keidser et al. (Citation1997), only five out of 27 participants used different settings in different listening environments. They also reported that no participant experienced benefit from more than two different settings. Banerjee (Citation2011) showed that the default setting was deemed acceptable by the hearing recipients for the majority of time. Berninger and Nordstrom (Citation1997) showed that the majority of their participants used all four programmes regularly. The main focus of their study was the repeatability of the recipients’ preference for a specific setting, i.e. the percentage of participants who selected the same programme as the best one (on individual basis). In demanding listening environments, this repeatability was high (75%), while it dropped to 40% in less demanding situations.
Studies showed mixed results on the use of different microphone modes (omnidirectional or directional) for specific listening environments (Cord et al. Citation2002; Kuk Citation1996; Palmer, Bentler, and Mueller Citation2006; Ricketts, Henry, and Gnewikow Citation2003; Walden et al. Citation2004). The majority of participants reported switching between microphone modes based on different listening environments. In contrast, however, subgroups of participants left the hearing aids in the default microphone mode (Cord et al. Citation2002; Kuk Citation1996), were not able to differentiate between different microphone modes (Palmer, Bentler, and Mueller Citation2006), or were equally divided in terms of preference between the omnidirectional and directional microphone mode (Palmer, Bentler, and Mueller Citation2006).
In conclusion, studies showed that some hearing aid recipients value the option of multiple programmes for various listening environments. However, little is known about the correct use of programmes designated for a specific listening environment. None of the studies examined whether participants used a certain programme in the correct listening environment (e.g. whether hearing aid recipients selected the noise programme in noisy environments).
Question 2: for multimemory devices (manual switching): which factors influence whether a recipient actually uses multiple programs?
Several factors seem to be important for the successful use of multimemory hearing aids. First, the hearing aid user needs to meet specific criteria. A set of guidelines was devised (Keidser et al. Citation2005) to specify which individuals are likely to actually use multimemory hearing aids. These guidelines indicate that subjects (1) must demonstrate motivation for better hearing in listening environments experienced on a regular basis, (2) must be able to understand, manage, and accept a multimemory hearing device and (3) must be fitted with hearing aid settings in the different programmes that are sufficiently different for the hearing aid user to tell them apart. These guidelines were evaluated in 48 hearing recipients and appeared to correctly identify the majority of the participants who actually used the multimemory hearing aid.
In addition to the characteristics of potential multimemory hearing aid recipients mentioned in the guidelines of Keidser et al. (Citation2005), several other factors could be identified through the included studies. First, recipients need to be able to classify the listening environment, must be willing to subsequently switch to different settings and recipients need to be physically capable of switching between programmes. In addition, the user needs to experience a clear benefit in switching between programmes (Cord et al. Citation2002; Kuk Citation1996). Recipients who perceive an advantage in switching between different microphone modes are more likely to switch than recipients who do not (Kuk Citation1996). No findings were reported about the ability of listeners to assess the listening environment correctly, except for the studies by Walden et al. (Citation2004) and Cord et al. (Citation2002). The data of these studies suggest that patients are able to assess the listening environment correctly and change the microphone mode accordingly. However, it is complicated to conclude about the listeners ability to specifically assess listening environments, due to a difference between listening environment (i.e. acoustic environment) and listening situation (i.e. focus of a hearing device user in an acoustic environment). For instance, a recipient might want to switch between listening to a distant speaker, or focus attention to someone sitting next to him. In this case, the listening environment has not changed; however, a change in settings might be required due to the change in listening situation.
Studies showed that patients tend to leave hearing aids in the default setting (Banerjee Citation2011; Cord et al. Citation2002; Van den Heuvel, Goverts, and Kapteyn Citation1997). This is often prompted by the fact that hearing health care professionals may instruct recipients to keep the hearing aids in the default setting, except when speech recognition is affected to such a degree that the settings of the hearing aid should be changed (e.g. in a listening environment with background noise). This may prevent recipients from switching to the most optimal setting when the environment changes. We think that counselling of hearing aid recipients is very important for the appreciation of a multimemory hearing aid use. Attention should be paid to explain the characteristics of the different programmes for specific listening environments. It is shown that patients do not understand, are not aware of, or have forgotten what the specific listening characteristics of an environment are in which programmed hearing aid settings provide substantial benefit (Cord et al. Citation2002). Therefore, a session could be added to the counselling process in which the recipient experiences examples of listening environments and is trained to choose the designated programme. An additional session might be needed after some time to determine whether the recipient is still using the features of the hearing device appropriately. Although this might be considered necessary for an optimal fitting procedure, it is questionable whether this is a realistic scenario for clinical practice. The possible negative effect of using a multimemory hearing aid while it is in a programme that is not designated for the specific listening environment was not discussed in any of the studies included in this review.
An important factor, also highlighted in the aforementioned guidelines, is that recipients have to find themselves in varying listening environments on a regular basis to experience benefit from a multimemory hearing aid (Keidser et al. Citation2005; Van den Heuvel, Goverts, and Kapteyn Citation1997). However, listening environments vary between individuals. Therefore, it might be important to fit a hearing aid with settings for those listening environments that are pointed out to be important by the individual wearer. Some patients might benefit from volume changes only and do not necessarily need multiple programmes (Banerjee Citation2011; Keidser et al. Citation1997; Stelmachowicz, Lewis, and Carney Citation1994). In a study in which recipients could alter both the volume and the settings, none of the participants who frequently used the volume control preferred different programmes for different listening environments (Keidser et al. Citation1997). Stelmachowicz, Lewis, and Carney (Citation1994) have argued that it is likely that the efficacy of a multimemory device is highly dependent upon the specific hearing aid characteristics programmed into each memory and how well these characteristics match the user’s needs in daily listening environments. Adapting hearing aid settings on an individual basis, however, is very time consuming, and does not guarantee the use of multiple memories in all hearing aid recipients (Stelmachowicz, Lewis, and Carney Citation1994).
In conclusion, a multitude of factors that may influence the (non-)use of multiple programmes, related to the hearing aid recipients as well as to counselling and fitting, could be identified through the included studies. However, the evidence is weak and based on relatively little and older hearing aid literature. It is evident that, because of this vast number of factors, not all hearing aid recipients value the option to manually switch between multiple programmes in different listening environments.
Question 3: for automatically switching devices: do hearing aid and CI recipients value a device that switches automatically between settings, depending on listening environment?
Three studies that described the use of an automatic switching mode (Buechler Citation2001; Gabriel Citation2002; Olson, Ioannou, and Trine Citation2004) concluded that this functionality was used with satisfaction by the majority (range 75–89%) of hearing aid recipients. Despite the usefulness, the automatic mode was shown to be unable to anticipate to individual preferences or correctly classify all acoustic environments (Buechler Citation2001). This might be due to the fact that an automatic switching device selects its settings mainly based on specific acoustical characteristics of the incoming sound (e.g. presence or absence of noise). Individuals, on the other hand, may choose settings based on these acoustical characteristics, but also on the specific listening situation.
The majority of subjects in the study by Gabriel (Citation2002) evaluated the automatic switching mode as being useful. The automatic switching mode was used for 70% of the time, a remote control to switch manually between programmes was used the rest of the time. Buechler (Citation2001) showed that in specific situations (e.g. in a group conversation, where one user prefers to focus on the speaker, while another hearing aid user wants to hear other speakers in the group as well), the option to manually choose the appropriate programme was preferred. However, the majority of subjects found the automatic switching mode useful, and only 20% of the subjects indicated that they would rather not use it. Olson, Ioannou, and Trine (Citation2004) reported that subjects supported the concept of an automatic switching mode, and the subjects indicated that the automatic mode switched to the preferred microphone mode (directional or omnidirectional) about 89% of the time, although the recipients had difficulty to choose between microphone modes in some environments (e.g. a restaurant environment).
The included studies have shown that an automatic switching device might be a good option for individuals who want to have a simple-to-use device, and for individuals who are not able to assess the listening environment adequately and alter the settings of hearing aids accordingly (Buechler Citation2001; Gabriel Citation2002; Olson, Ioannou, and Trine Citation2004). A manual switch would be preferable for individuals who prefer settings that deviate from the selection made by the automatic switching mode (Gabriel Citation2002). However, the studies are quite old and may therefore not reflect the possibilities of newer automatic switching hearing devices.
General discussion
Despite the high number of multimemory devices and automatically switching devices that is sold each year, this scoping review showed that the evidence for the use of these features, the appreciation of these features and the evidence for the appropriateness of the setting selection is remarkably low. It was recently stated that the hearing aid industry has been emphasising on development over research (Zeng Citation2015). A continuous market pressure to introduce new features often results in the introduction of technologies in an absence of compelling evidence to support the use of these features by the key stakeholders, the hearing aid recipients.
First, it is important to mention that the evidence is weak and based on relatively little and older literature. The number of studies identified through this search was low and the studies have several limitations. These limitations have impeded us to draw strong and consistent conclusions concerning the use and appreciation of manual and/or automatically switching devices. The lack of evidence is surprising, since manual and automatic switching devices are the current state of the art and fitted regularly to hearing-impaired patients. Some of the studies are decades old and report on technology that is different from the current technology used in hearing aids and cochlear implants. Thus, the results of these older studies may not reflect the possibilities of newer hearing devices, especially with automatic switching devices. Automatic switching devices have gone through various technical improvements over the last years, resulting in more powerful devices that can address more and more specific listening situations. The principle of manual switching between different programmes for various listening environments has not changed and is independent of technical improvements in hearing devices, since patients still have to be able to characterise the environment, select the most appropriate programme and switch between programmes.
Second, studies report that participants “benefit” from the use of a multimemory device if they use the feature to manually switch between programmes. However, it is not clear what exactly motivates a participant to use this feature: is he or she experiencing benefit in terms of increased speech recognition abilities when altering settings, or does a change in settings lead to more comfort in listening? As no studies elaborate on this issue, it is unclear which experience underlies the actual use of a multimemory device.
Third, the data on the use of multiple programmes are often subjective. The majority of studies use diaries or questionnaires in which recipients report details of the listening environments (i.e. type of environment, and signal and noise location), the used settings for the specific environment, and whether they altered the settings. The diaries and questionnaires thereby rely fully on, for instance, the ability of participants to distinguish between programmes, the participants’ analysis of the environment, judgment of sound quality and willingness to report every single listening environment. Whether the appropriate programme is used in each listening environment cannot be derived from these data. In contrast, the availability of data logging in a hearing device, as used in some studies (Banerjee Citation2011; Van den Heuvel, Goverts, and Kapteyn Citation1997), provides objective information on the hours of daily usage, relative amount of time each programme is used and volume changes. Kiessling et al. (Citation2007) state that subjects are able to provide a reliable estimation of their daily hearing aid use, as compared to the hearing aid use acquired with data logging. However, this study also found that the correlation between self-reported and logged device adjustments, such as programme changes, is considerably less strong. Data logging can offer an objective view of the use of multimemory hearing aids, next to the subjective information as used in the majority of the studies.
Fourth, in several studies (Banerjee Citation2011; Ringdahl et al. Citation1990), the participants had to select the preferred setting for a specific listening environment, also referred to as “forced choice by direct comparison”, even while the recipients did not necessarily have a preference for one setting over another. Although this method can be considered to be more reliable than retrospective interviews or questionnaires, it can lead to unreliable data since it cannot be verified that participants have tried multiple settings, or have compared their own hearing aid to the study hearing aid.
Fifth, some studies (Kuk Citation1992; Ringdahl et al. Citation1990) used a study design in which a new hearing aid was compared to the participant’s own hearing aid. This study method introduces bias, because new hearing aid technology is generally rated more positively than conventional technology (Bentler et al. Citation2003; Dawes, Powell, and Munro Citation2011). In addition, it is unclear whether subjects have followed the study instructions of Kuk (Citation1992) and Ringdahl et al. (Citation1990) and duly have tried multiple programmes in various listening environments, or have only compared their own hearing aid to the default setting of the study hearing aid.
A sixth limitation is that most studies pay little attention to continuation of the use of the features after completion of the study. It is plausible that subjects use multiple programmes during the study period, but stop using them once the study finishes. Kuk (Citation1992) used a follow-up period of 1 year to investigate the long-term use in 19 participants. He showed that the number of participants using multiple programmes increased from 9 to 11 during the follow-up period. This might indicate that participants need to acclimatise to the use of a multimemory hearing aid. The results of a study by Gatehouse (Citation1992) showed that it takes time, ideally 6–12 weeks, to experience the advantages of a new frequency response setting. In the studies discussed in the current article, the hearing aid experience of included participants ranged from no experience with hearing aids to extensive experience with hearing aids and even extensive experience with multimemory hearing aids. It goes without saying that new hearing aid recipients need time to familiarise themselves with hearing aids in general, let alone a multimemory hearing aid that requires them to analyse the listening environments and change the hearing aid settings accordingly.
Seventh, several studies (Goldstein, Shields, and Sandlin Citation1991; Keidser Citation1995; Stelmachowicz, Lewis, and Carney Citation1994) have investigated the use of a multimemory hearing aid in a laboratorial setting. Listening environments in daily life may change rapidly and are not comparable to situations in a sound-treated test booth. In addition, participants in a laboratorial setting might be more aware of the fact that they need to change programmes than when using a hearing aid in daily life. Punch, Robb, and Shovels (Citation1994), for instance, have shown that preferences of hearing aid recipients in laboratory sessions were only fair predictors of preferred hearing aid settings in the real world. However, test conditions that simulate the hearing aid wearer’s daily listening environments in a laboratorial setting might help to evaluate the candidacy for the use of multiple programmes for different listening environments.
Conclusions
This scoping review investigated the available evidence for the added value of manual and automatically switching devices for various listening environments by hearing aid and CI recipients. No studies were found that concerned CI recipients, so this review only reflects the results of studies in hearing aid recipients. It is unclear to what extent the results of studies with hearing aid recipients hold for CI recipients, who often have more severe hearing losses than hearing aid recipients. Nineteen studies were included in the review, from which 14 were published in peer-reviewed journals.
The scoping review shows that, despite the high number of multimemory devices and automatically switching devices that are sold each year, the evidence for use and appreciation of these features, and the evidence for the appropriateness of the setting selection is remarkably low. Although the evidence is weak, this review indicated that some hearing-impaired individuals use the possibilities of a multimemory hearing aid. No studies were found that objectively examined the accuracy of the use of specific programmes for specific listening environments by hearing aid recipients. Several characteristics of hearing aid recipients could be identified that possibly influence the use of a multimemory device: the hearing aid user must indicate a clear need for better hearing in various, often encountered, listening environments, must understand the use of a multimemory device, must be willing to change the settings and must be able to assess the listening environments. In addition, the programmes of the hearing device must be sufficiently different for the user to tell them apart, the user has to be aware of the different programmes, the user has to experience benefit from the various programmes in different listening environments and must be able to use either a switch button or remote control to change the settings. For those who are not able, or willing, to switch between programmes in different listening environments, an automatic switching device might be a good solution. For others, satisfying results with an automatic switching device can be obtained in combination with a manual switch.
The use of a scoping review allowed the inclusion of a broad range of literature to synthesise the available evidence and identify interesting topics for future research. Based on this scoping review, we recommend that future research should focus on gathering objective evidence concerning the use of multiple programmes for various listening environments by hearing aid and CI recipients. Data logging functionalities in modern hearing devices, hearing aids and CIs, could be useful to gain further insight in the listening environments encountered (Busch, Vanpoucke, and van Wieringen Citation2017), and in the programmes a user selects in these environments.
Declaration of interest
The authors declare no conflicts of interest.
Supplementary material available online
| Abbreviations | ||
| CI | = | Cochlear implant |
| HA | = | Hearing aid |
| SNHL | = | Sensorineural hearing loss |
Suplemental_content.docx
Download MS Word (12.8 KB)References
- Arksey, H., and L. O'Malley. 2005. “Scoping Studies: Towards a Methodological Framework.” International Journal of Social Research Methodology 8: 19–32.
- Banerjee, S. 2011. “Hearing Aids in the Real World: Use of Multimemory and Volume Controls.” Journal of the American Academy of Audiology 22: 359–374.
- Bentler, R. A., D. P. Niebuhr, T. A. Johnson, and G. A. Flamme. 2003. “Impact of Digital Labeling on Outcome Measures.” Ear and Hearing 24: 215–224.
- Berninger, E., and I. Nordstrom. 1997. “Multiple Memory Hearing Aid. Consistency of Program-Usage in Real-World Listening Situations.” Scandinavian Audiology 26: 252–256.
- Buechler, M. 2001. “How Good Are Automatic Program Selection Features?” Hearing Review 8: 50–55.
- Busch, T., F. Vanpoucke, and A. van Wieringen. 2017. “Auditory Environment Across the Life Span of Cochlear Implant Users: Insights From Data Logging.” Journal of Speech, Language, and Hearing Research 60: 1362–1377.
- Cord, M. T., R. K. Surr, B. E. Walden, and L. Olson. 2002. “Performance of Directional Microphone Hearing Aids in Everyday Life.” Journal of the American Academy of Audiology 13: 295–307.
- Davis, K., N. Drey, and D. Gould. 2009. “What Are Scoping Studies? A Review of the Nursing Literature.” International Journal of Nursing Studies 46: 1386–1400.
- Dawes, P., S. Powell, and K. J. Munro. 2011. “The Placebo Effect and the Influence of Participant Expectation on Hearing Aid Trials.” Ear and Hearing 32: 767–774.
- Gabriel, B. 2002. “Study Measures User Benefit of Two Modern Hearing Aid Features.” Hearing Journal 55: 46–50.
- Gatehouse, S. 1992. “The Time Course and Magnitude of Perceptual Acclimatization to Frequency Responses: Evidence from Monaural Fitting of Hearing Aids.” The Journal of the Acoustical Society of America 92: 1258–1268.
- Goldstein, D. P., A. R. Shields, and R. E. Sandlin. 1991. “A Multiple Memory, Digitally-Controlled Hearing Instrument.” Hearing Instruments 42: 18–21.
- Keidser, G. 1995. “The Relationship Between Listening Conditions and Alternative Amplification Schemes for Multiple Memory Hearing Aids.” Ear and Hearing 16: 575–586.
- Keidser, G., H. Dillon, and D. Byrne. 1996. “Guidelines for Fitting Multiple Memory Hearing Aids.” Journal of the American Academy of Audiology 7: 406–418.
- Keidser, G., H. S. Limareff, S. Simmons, C. Gul, Z. Hayes, C. Sawers, B. Thomas, K. Holland, and K. Korchek. 2005. “Clinical Evaluation of Australian Hearing's Guidelines for Fitting Multiple Memory Hearing Aids.” Australian and New Zealand Journal of Audiology 27: 51–68.
- Keidser, G., A. Pellegrino, A. Delifotis, J. Ridgway, and M. Clarke. 1997. “The Use of Different Frequency Response Characteristics in Everyday Environments.” Australian Journal of Audiology 19: 9–21.
- Kiessling, J., B. Brenner, J. Nelson, O. Dyrlund, and J. Groth. 2007. “Feldstudie zum Nutzungsverhalten von Hörgeräten: Datalogging versus Selbsteinschätzung.” Zeitschrift für Audiologie 46: 48–55.
- Kochkin, S. 2007. “Increasing Hearing Aid Adoption Through Multiple Environmental Listening Utility.” Hearing Journal 60: 28–31.
- Kuk, F. K. 1992. “Evaluation of the Efficacy of a Multimemory Hearing Aid.” Journal of the American Academy of Audiology 3: 338–348.
- Kuk, F. K. 1996. “Subjective Preference for Microphone Types in Daily Listening Environments.” Hearing Journal 49: 29–38.
- Mauger, S. J., C. D. Warren, M. R. Knight, M. Goorevich, and E. Nel. 2014. “Clinical Evaluation of the Nucleus® 6 Cochlear Implant System: Performance Improvements with SmartSound iQ.”International Journal of Audiology 53: 564–576.
- Olson, L., M. Ioannou, and T. D. Trine. 2004. “Appraising an Automatically Switching Directional System in the Real World.” Hearing Journal 57: 32–38.
- Palmer, C., R. Bentler, and H. G. Mueller. 2006. “Evaluation of a Second-Order Directional Microphone Hearing Aid: II. Self-Report Outcomes.” Journal of the American Academy of Audiology 17: 190–201.
- Peters, M. D. J., C. M. Godfrey, H. Khalil, P. McInerney, D. Parker, and C. B. Soares. 2015. “Guidance for Conducting Systematic Scoping Reviews.” International Journal of Evidence-Based Healthcare 13: 141–146.
- Punch, J. L., R. Robb, and A. H. Shovels. 1994. “Aided Listener Preferences in Laboratory Versus Real-World Environments.” Ear and Hearing 15: 50–61.
- Ricketts, T. A., and R. A. Bentler. 1992. “Comparison of Two Digitally Programmable Hearing Aids.” Journal of the American Academy of Audiology 3: 101–112.
- Ricketts, T., P. Henry, and D. Gnewikow. 2003. “Full Time Directional Versus User Selectable Microphone Modes in Hearing Aids.” Ear and Hearing 24: 424–439.
- Ringdahl, A., M. Eriksson-Mangold, B. Israelsson, A. Lindkvist, and S. Mangold. 1990. “Clinical Trials with a Programmable Hearing Aid Set for Various Listening Environments.” British Journal of Audiology 24: 235–242.
- Stelmachowicz, P. G., D. E. Lewis, and E. Carney. 1994. “Preferred Hearing-Aid Frequency Responses in Simulated Listening Environments.” Journal of Speech Language and Hearing Research 37: 712–719.
- Van den Heuvel, J., S. T. Goverts, and T. S. Kapteyn. 1997. “Evaluation of Fitting Rules with a Programmable Hearing Aid.” Audiology 36: 261–278.
- Walden, B. E., R. K. Surr, M. T. Cord, and O. Dyrlund. 2004. “Predicting Hearing Aid Microphone Preference in Everyday Listening.” Journal of the American Academy of Audiology 15: 365–396.
- Wolfe, J., S. Neumann, M. Marsh, E. Schafer, L. Lianos, J. Gilden, L. O’Neill, . 2015. “Benefits of Adaptive Signal Processing in a Commercially Available Cochlear Implant Sound Processor.” Otology & Neurotology 36: 1181–1190.
- Zeng, F. G. 2015. “Do or Die for Hearing Aid Industry.” Hearing Journal 68: 6.