
Abstract
Objective: Tinnitus is one of the most common somatic symptoms to affect humanity. Prevalence rates in adult populations range from 8.2 to 20.1%. Our aim was to understand the beliefs and interpretations of tinnitus and the experience of living with it.
Design: An in depth grounded theory interview study. Grounded theory is an inductive approach to developing theory.
Sample: Thirteen contrasting people with tinnitus who had sought help from clinical services in England.
Results: We identified that the thinking patterns that people held around their tinnitus impacted how they experienced it. A core category emerged from the data, “sense making”. Around “sense making” eight other themes operated. Results are discussed in relation to the literature on tinnitus acceptance and beliefs.
Conclusions: The aim of interventions is to foster understanding and enhance perceptions of control, which may minimise the emotional impact of tinnitus and reduce the perceived severity of consequences.
Background
Subjective tinnitus is often described as the experience of perceiving sound in the absence of corresponding external auditory or electrical stimulus (Milerová et al. Citation2013; McKenna et al. Citation2014). Tinnitus can occur with differing levels of severity, it may arise in conjunction with hearing loss (HL) and often no cause is found (Holmes and Padgham Citation2011). McKenna et al. (Citation2014) propose that tinnitus is one of the most common somatic symptoms to affect humanity. Prevalence rates in adult populations both overseas and in the UK agree broadly (ranging from 8.2 to 20.1%) and show an increase in the prevalence with age (Fabijanska et al. Citation1999; Nandahl et al. 2002 ; Shargorodsky, Curhan, and Farwell Citation2010; Dawes et al. Citation2014). Epidemiological data for severely distressing tinnitus (persistent tinnitus impacting most aspects of life quality) has been reported to be in the range of 1–3% and is also associated with increasing age (Davis and El Refaie Citation2000). In 2005, more than 13 million people in the United States and Western Europe sought medical advice for tinnitus (Vio and Holme Citation2005). A recent investigation into the incidence of tinnitus in England by Martinez et al. (Citation2015) again supported an increase in incidence with age and postulated that 324,000 new cases of tinnitus are expected to occur in England alone between 2012 and 2021, representing a potentially significant burden to the UK health system. Around 1 in 10 adults are thought to experience tinnitus and at least 32,000 people sought help in England in 2015 (Action on Hearing Loss factsheet, 2016). In the US, 25 million adults report permanent tinnitus with 16 million seeking help each year (http://hearinghealthfoundation.org/statistics). In light of compelling prevalence and incidence data along with effects on quality of life (Tyler and Baker Citation1983; Stouffer and Tyler Citation1990; Cima, Crombez, and Vlaeyen Citation2011; Negrila-Mezei, Enache, and Sarafoleanu Citation2011), effective management to reduce these associated effects is of significant global importance.
The characteristics, neuroanatomical correlates and treatment (Baguley et al. Citation2013) of tinnitus have received attention in the audiological literature. Yet understanding the process of why some people suffer whilst others do not is a key challenge in tinnitus research and clinical practice (Milerová et al. Citation2013; McKenna et al. Citation2014). Recently McKenna et al. (Citation2014) have taken these psychological correlates further by proposing a novel cognitive-behavioural model of tinnitus building on the work of Hallam, Rachman, and Hinchliffe (Citation1984). The model suggests that patients’ interpretations of tinnitus and subsequent changes in behaviour that ensue are given a central role in creating and sustaining distress and that a clearer understanding of the role of thoughts or conscious cognitive mechanisms involved would help improve treatment outcomes for patients (McKenna et al. Citation2014). As with complex chronic conditions, coping with tinnitus means living with an ‘invisible illness’ that can create challenges to credibility and stigma (Armentor Citation2017).
The majority of tinnitus research has utilised quantitative self-report measures in order to infer descriptive correlations and characteristics about tinnitus sufferers. Dauman and Erlandsson (Citation2012) warn that this could lead to a limited and biased model of tinnitus experience. There appears to be a paucity of qualitative studies involving tinnitus patients (Andersson and Edvinsson Citation2008; Adams, Verrier, and Walsh Citation2012; Dauman and Erlandsson Citation2012; Wheeler and Hopwood Citation2015; Dauman et al. Citation2017). These studies have used a variety of qualitative methodologies. Grounded theory has been an approach that has yielded crucial information about the mechanisms behind tinnitus distress and maintenance of symptoms. Andersson and Edvinsson (Citation2008) used grounded theory (GT) methods to obtain patient’s views about their tinnitus and treatment, the results of which never ventured past descriptive categories due to lack of theoretical data saturation. Adams, Verrier, and Walsh (Citation2012) identified the role of information in leading to a sense of empowerment with tinnitus. Dauman et al. (Citation2017) described the role of emotional content in tinnitus distress. A psychodynamic narrative approach to capture one patient’s experience of living with tinnitus was performed by Dauman and Erlandsson (Citation2012), while a short performance ethnography piece utilising poetry in order to presented reflections on the tinnitus experience (Wheeler and Hopwood Citation2015) and a pilot study (cited in Dauman and Erlandsson 2012) found that participants needed to grieve the loss of silence after tinnitus emergence.
Objective
A qualitative approach using grounded theory has the explanatory power to generate new theories yet also complement and strengthen existing theories about tinnitus (Andersson and Edvinsson Citation2008). Grounded theory is an inductive approach to data, which aims to identify a core concern in the participants' experience.
The study was reviewed by the proportionate review service of the National Research Ethics Service (Leeds East Research Ethics Committee reference 183770) and additional governance approvals were obtained from Great Western Hospital Swindon and Aston University (who sponsored the study).
Participants – selection
Thirteen participants were purposively sampled from a patient population who had been seen in clinical tinnitus clinics in the south west of England over an 18 month period. The sample was chosen for maximum variation (Sbaraini et al. Citation2011), relating to age, gender, occupational status, severity of tinnitus distress, duration of tinnitus and hearing loss. Participation was entirely voluntary and all participants were given pseudonyms to conceal identities. The participants are described here to illustrate the range of experience and life characteristics that will influence their description of living with tinnitus. This sample size is not intended to represent a statistically generalisable sample. Rather this sample includes the key variations that impact the experience of living with tinnitus and the thoughts that emerge as a result.
Data collection and analysis
Grounded theory enables the description and theorising of an adaption and change in response to a chronic health conditions (Tolley et al. Citation2016). It has been employed in related hearing conditions such as King–Kopetzky syndrome (Pryce Citation2003).
Semi-structured intensive interview
Interviewing was chosen to enable gathering of rich focussed data for developing abstract conceptual information (Dicicco-Bloom and Crabtree Citation2006; Charmaz Citation2014). Interviews were conducted face to face over 6 months. Each interview lasted approximately 60 min. These interviews were conducted by the authors (K. C. and H. P.). The second set of six interviews was used to check the emerging theory from the first set. This iterative refinement of theory provided further insights as to how the themes related and operated.
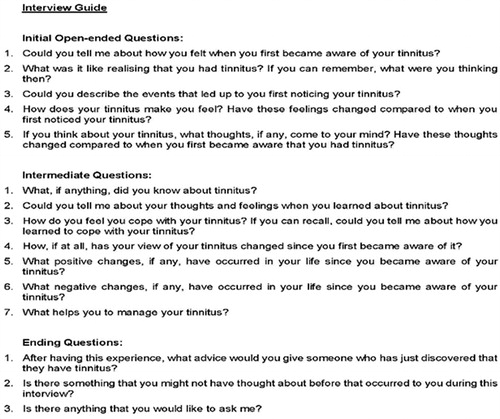
Interview questions were designed to be open and non-judgemental, and consisted of initial questions to initiate conversation, intermediate questions to investigate areas in more depth and closing questions to prevent an abrupt end (Charmaz Citation2014). (see ). Interviews were all conducted face to face in participants’ homes. The structure aims to guide and facilitate conversation in a flexible and fluid semi-structured format, yet allow for discovery of information that was of importance to participants (Gill et al. Citation2008). Interviews and analysis occurred in parallel and interview data informed the phrasing of questions and topics to explore.
Figure 1. Interview guide.
Analysis
All interviews were recorded and professionally transcribed. Charmaz (Citation2014) proposes that we are part of the world we study, data we collect and analyses we produce, we construct our grounded theories through our past and present involvements and interactions with people, perspectives and research practices. In this case, the researchers are audiologists and their personal perspectives informed their interpretation of participant’s descriptions of tinnitus. The participants had not seen the researchers as clinicians and met them as researchers only. In particular, the researchers were aware of the risk of framing descriptions of distress as clinical symptoms. The researchers discussed this perspective and reflected on any points during the interview where verbal or non-verbal communication might shape descriptions of thoughts or experiences as “symptoms”. This formed part of the iterative process of interview, analysis and reflection.
To begin conceptualisation (Charmaz Citation2014), pre-coding was employed to create familiarity with transcripts. This involved highlighting potentially significant quotes or passages for later attention. The first author coded all data and then presented un-coded transcripts to the second author for independent coding. Descriptive and initial coding was aligned between both authors. First-cycle coding methods involved initial coding, which employed micro-analysing transcripts line by line.
Second-cycle coding involved focus coding. Charmaz (Citation2014) describes this analytic process as a way of pinpointing and developing the most salient codes, putting aside ones that are not and then testing them against large batches of data. Abstract categories were created both from existing codes and based on the amount of data and codes across interviews that supported them. Connections between categories were then examined as an integrative basis for theory-building and for clarifying theoretical centrality (Charmaz Citation2014). Triangulation was achieved by both researchers separately coding data extracts and comparing the codes and interpretations together. There was consensus on most coded labels and where there was not the researchers discussed their interpretations and agreed a coded label.
As theoretical sampling progressed and participants were chosen according to the emerging theoretical direction (Elliott and Lazenbatt Citation2005), interview questions were subtly adjusted. Analysis appeared well saturated in that there were fewer novel or original descriptions of the tinnitus experience and each varied description fitted an existing category. A provisional theoretical explanation was found for the phenomenon being explored (Saldaña Citation2015).
To promote researcher reflexivity on the data corpus and as an additional code and category-generating method in itself, analytic memos were written throughout the research process. Memos were critical during the transition from first to second-cycle coding and became essential during theoretical coding for reflection on categorical relationships and emergent themes for theoretical direction.
Findings: losing silence, gaining acceptance
Pseudonymised participants
Carol a retired female in her 60s with normal hearing could recall vividly the emergence of her bilateral tinnitus as it came into her awareness following a road traffic accident in the mid-1980s. It became apparent that she had expected this perception to dissipate as her body healed; however, when this did not occur she was able to describe the exact time and place when she realised that this sound within her head was permanent. Carol had utilised her own coping behaviours centring on music based sound enrichment for the majority of her adult life in order to distract herself from her tinnitus.
Amanda, a self-employed female in her 30s with mild hearing loss in the left ear reported that she had experienced bilateral tinnitus for approximately 15 years and had trouble recalling a time when she was not aware of the percept. Initially, Amanda had attributed her tinnitus to noise exposure but explained that one day her tinnitus just did not stop; Amanda described this initial tinnitus as annoying but not enough to seek any medical help. She sought medical help 3 years ago when the loudness of her tinnitus increased, which she felt affected her ability to hear, this increase in tinnitus loudness was also accompanied with symptoms of hyperacusis (sensitivity to sound). Her tinnitus could also be exacerbated by loud sounds.
Keith, a retired male in his 60s with bilateral high frequency hearing loss, first become aware of his tinnitus in 2008. He described it as being constant and in both ears but more predominant in the right. Keith sought medical attention very quickly as initially he associated tinnitus emergence with a medication side-effect.
Sarah was a self-employed female in her 40s with bilateral hearing loss. She described her tinnitus as periodic in nature and having a different pitch and quality in each ear. Sarah had come to think of her tinnitus more fondly with time as she felt its emergence was a warning sign that she should take rest as her tinnitus was often accompanied by feelings of extreme tiredness.
Paul was a retired male in his 70s with bilateral moderate high-frequency hearing loss. He had first become aware of tinnitus at work. He described his tinnitus as being constant and centralised within his head. It was not until after retirement and a subsequent change in lifestyle that Paul saw his GP and mentioned that he had tinnitus as it was becoming more intrusive, which then led to a referral in to the Tinnitus Clinic.
Michael was a retired male in his 50s with mild bilateral hearing loss and described experiencing tinnitus periodically at first. His tinnitus became less periodic, louder and more intrusive over a period of 12 months which prompted him to seek help in 2013. Michael now describes his tinnitus as constant and bilateral but louder in the left ear.
Carl was a self-employed male in his 30s. He first became aware of unilateral left-sided tinnitus in 2014 for which he did seek prompt medical attention. Carl’s tinnitus seemed to be exacerbated by environmental noises and he also described symptoms of sensitivity to sounds.
Freya was a retired engineer in her 70s. She first noticed tinnitus approximately 10 years before but has only recently become troubled by the changing quality of the sound that she hears. She was a passionate musician and keen to ensure she can continue to take an active role in her various musical groups.
Nicola was in her 50s and has a role in the military. She noticed a single sided tinnitus for a few years. A second sound started and was causing her distress. She found that she struggled to communicate this to her partner and felt isolated.
Jenny was in her late 80s and lived with her son. She was not very bothered by the tinnitus that she heard in both ears, but was anxious that it should not progress or get worse. Jenny found it difficult to identify when tinnitus started.
Ben was in his 40s and had just started to notice a tinnitus sound. He was concerned about changes to his hearing and was undergoing investigations for this.
Phil was in his 50s and medically retired from work due to his poor health. He described a pragmatic approach to living with tinnitus day to day and in the context of his other health problems. His tinnitus was first diagnosed in 1995.
Barbara had a tinnitus that she found to be triggered by other high pitched noises. This troubled her during her musical past-times. She found the tinnitus becoming more noticeable over the last 2 years.
Rich contrasting interviews with 13 participants provided a detailed description of the process of thinking about tinnitus and its impact on symptom perception. Acceptance of tinnitus seems to be difficult and takes time to achieve, but if reached may represent an internalised form of self- control. Acceptance appears to reduce negative emotional thoughts relating to the perceived loss of silence and/or control that the tinnitus perception can symbolise. Nine unique themes were clustered around the process of thinking about and eventually accepting tinnitus, and what may hinder and or enable this process ().
Table 1. Table of major themes.
Theme 1: losing silence and a sense of control
Tinnitus emergence can be expressed as a loss of silence in some participant’s lives, an unwelcome intrusion into a once private space. “It intrudes on your … you know when you want a moment of quiet.” Amanda goes on to say that, “In a sense it is all that’s left.” (Amanda) The tinnitus becomes expressed using language indicating external control. “… yeah, I think I started to realise that…there was something else going on here, which was outside of my control.” (Amanda)
Theme 2: perceiving a sense of loss leads to negative emotional responses
The data suggest that emotional responses towards tinnitus are transient and vary depending on the perceived impact at a particular point in time or situational context e.g. “I've come to see it and unless it's waking me up in the night…I really don't mind it.” (Keith) Emotions related to tinnitus seem to exist on a spectrum and regardless of which, tinnitus is always expressed as being external to the self. “It’s annoying really, it really is annoying …it really is. I can’t stand it, so much so I feel like cutting my ear off.”(Jenny)
Negative emotions were elicited when perceiving loss, “I’d like to say frustrated but I think there’s something more than frustrated really … desperate sometimes … but all along that I know that there isn’t a lot that I can do about it and I have to put up with it but it’s not something that’s easy to put up with.”(Barbara)Positive emotions were elicited when perceiving gains, “I think it's looking after me.” (Nicola) Importantly, ambivalence towards the tinnitus percept was expressed in one participant where no loss of silence was perceived yet externalised control was still expressed; the tinnitus percept appeared fused with their autobiographical memory: “… it doesn’t annoy me or anything, you know make me grumpy because, [laughs] I’ve got this. Because I don’t know anything, how it was, I can’t remember when it was just … silence you know.” (Nicola). This suggests that a sense of loss must be consciously perceived in order for negative emotional responses to occur and that remembering the loss of silence may be much more easily perceived than loss of control.
Theme 3: valuing apparent control through the use of effective coping strategies
Participants appeared to use an array coping strategies. This may be devices such as hearing aids or pillow speakers. As one participant noted “… the hearing aids, if I don't wear them for a day … I will get rumbles. And it will start.”(Paul) It could also be behavioural strategies such as engaging in an active lifestyle, avoiding environments that exacerbate the tinnitus or distracting activities: “When you’re concentrating on something at work or whatever, gardening or whatever you’re doing, you don’t notice it because you’re focussing on something else.”(Sarah)
Seeking out and using coping strategies was associated with the language of internalised control e.g. “Yeah, but what I did do some years ago, actually prior to going to {Service}. I’d already gone down the route of getting a catalogue and getting a, a night-time masking device.” (Freya) Respite from or alteration of the tinnitus perception through effective coping strategies seems to provide participants with an apparent control. When discussing how much the night-time sound generator had helped to reduce tinnitus awareness commented, “Well, if I was to say it gives me control…. well, let’s say apparent control.”(Freya)
Control appears to have value in reducing negative emotional responses towards tinnitus, and is often enabled by new technologies and techniques. For instance some participants compared the difficulties they were having before then after hearing aids were fitted. They, describing the time preceding hearing aids as being “Really hard. And the tinnitus is more prevalent I think because it was there all the time.”(Paul) Having control can also promote tolerance towards situations: “Well I you know, I’ve just got to put up with it you know it, the days with these hearing aids are brilliant now, brilliant. But night times, well I haven’t really found, [laughs] an answer to it.”(Michael)
Theme 4: wanting ultimate control, the elusive off-switch
When participants express desire for an off-switch this suggests a desire for ultimate control: “I just want to have a switch to be able to just turn it off” (Sarah). Those experiencing less personal impact from tinnitus would just like not to have it. “No, it’s, [laughs] I’d like not to have it, but you know life isn’t it, get on with it.”(Carl) For others not having tinnitus represents a return to normality: “… But it would, or it would be nice if I just woke up one morning and it went” (Ben). Talking about the inability to switch tinnitus off appears intimately related to negative emotional responses: “… it’s a horrible noise and I wish it would go away” (Barbara), “… it’s because there isn’t a, an off-switch” (Keith)
Theme 5: articulating a condition that is difficult to explain
Difficulties finding words to describe what it’s like to have tinnitus appear influenced by its imperceptible nature, “… because you can’t, you can’t explain noise… to somebody else…”(Ben) It is also influenced by beliefs about other people’s reactions. “because it’s very personal, and it’s hard to share because in a way… who wants to hear about it?” (Jenny) It is also influenced by feeling unable to explain the condition appropriately. “I've been trying to explain my condition in a way that's, um, appropriate to other people.” (Ben)
Participants commented that the very act of being asked to talk about tinnitus can lead to increased tinnitus awareness, which reduced their wish to talk about it. “But if someone asks you about it, you notice it. So, in a sense I don’t talk about it a lot with [partner].” (Sarah)
The difficulties communicating what it is like to have tinnitus, although forming part of the tinnitus narrative, may logically impact upon sense-making and understanding mechanisms.
Theme 6: putting tinnitus into perspective
Participants describe upward and downward comparison with make sense of their own experience with tinnitus. For instance, one participant framed it in terms of what his father had to endure: “You, you have to try and deal with it well….my father’s generation, they had their things to deal with to do with wartime … in a way you feel guilty that you’ve got something that you’re worrying about which is pretty, you know…. it’s not massive and on the scale of thing. … you’ve got to put it in some sort of perspective.” (Carl)
When putting tinnitus into perspective, participants predominantly used comparison narratives, comparing tinnitus with other things or comparing themselves with other tinnitus sufferers in order to portray its subjective significance:
“Um. I Feel quite lucky ……And it's by no means the worst. Whereas when this guy, it was a troubling thing for him and I think it is troubling for a lot of people.”(Carl)
“Nobody knows somebody else’s pain … There was a lady on the television the other night, she had this terrible, terrible pain, she can’t live with it any more, something to do with her leg … she’s having her leg taken off. … It must be terrible that you’d do something as extreme as that.” (Ben)
Theme 7: achieving tinnitus acceptance
The data imply that achieving acceptance appears to be important for dealing with tinnitus successfully, living with it rather than battling against it. “Once I gave in and thought actually I can’t control it, that’s kind of when the battle, me and the tinnitus decided to call a truce.” (Paul)
“I think not to battle it … and just try and accept it really, because that’s the only thing you can do.”(Jenny) When tinnitus acceptance has been achieved participants gain a form of internalised control. “… I know I’ve got it and I’m not going to get rid of it…. but it’s okay … you’ve just got to get on the best you can with it.”(Srah) Acceptance does not appear to be fleeting like emotions. Instead, it represents the conscious choosing of a state of mind with which to regard tinnitus. This state of mine where it no longer has dominating negative emotional effects. “I don't welcome it, it's not particularly nice. But I don't see it as a bad thing and it doesn't stress me out in any way.” (Phil)
Theme 8: influencing perspectives and expectations
Importantly, it appears that perspectives, and hence expectations, about tinnitus are not fixed and can be changed by external influences. This cognitive alteration can be observed directly in the data, such as when one e.g. this participant described his change in perspective following interaction with an Audiologist. “And the audiologist did say to me then I think me and her had quite a long chat about it… it almost suddenly something just clicked and it was like right you know this is life long, and you’ve just got to deal with it and just get on with it and its not life threatening,” (Michael) Perspectives also appeared to change when patients were informed that their tinnitus may have had become more intense due to a decrease in hearing acuity. “You know when I said, “Oh the tinnitus is feeling more, more intense.”(Paul) And [Audiologist] would say, “Well that’s probably because you’re losing your hearing sensitivity … and it was that bit that I hadn’t twigged. And suddenly she said, so she said, “Hearing aids might help.” (Paul)
See for a linking diagram illustrating how these eight themes relate.
Figure 2. Linking diagram illustrating how the eight themes relate.
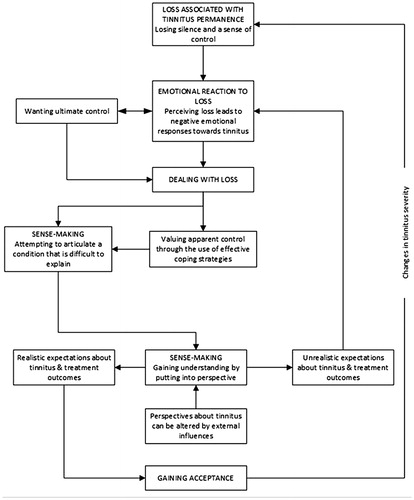
The core category – “sense making”
In these data, the core category that determines how these nine themes operate is “sense making”. This appears in every account and determines how the other themes operate in each individual account. This category denotes the process of rationalising the tinnitus and gaining understanding of the impact of the tinnitus. Where sense making leads to increased tinnitus acceptance, the result appears to be lower emotional reaction. Alternatively if sense making results in a sense of an on-going quest for ablation of the sound, the distress is maintained.
Discussion
This study models the way in which the way people think about their tinnitus impacts on their perception of it. It demonstrates how the process of acceptance occurs and is moderated. Acceptance, however, is not a permanent state and appears to be affected by external or internal influences e.g. an increase in tinnitus severity, which suggests the process maybe cyclical in nature.
Moreover, cognitions that allow participants to achieve acceptance tend to be associated with their expectations about tinnitus and treatment outcomes. Perspectives, and hence expectations, about tinnitus appear to be able to be modifiable via informational materials and/or discourse with others.
Tinnitus acceptance
This research resonates with and supports existing research on tinnitus and its acceptance. Psychological acceptance can be described as a process of actively taking in thoughts, memories, feelings and bodily sensations in a specific situation without having to pursue or alter them (Hayes, Strosahl, and Wilson Citation1999). Recent studies suggest correlations between positive effect of acceptance on tinnitus related distress and more recently, quality of life (Westin, Hayes, and Andersson Citation2008a, Citation2008b; Hesser et al. 2009, Citation2015; Riedl et al. Citation2015;). Furthermore, due to variable outcomes with of established tinnitus treatments (Martinez-Devesa et al. Citation2010), support from chronic pain research (Öst Citation2014) and tinnitus often being likened to chronic pain (Moller 2000), interest in Acceptance and Commitment Therapy (ACT) based interventions for the treatment of tinnitus have emerged and experimental studies of ACT have been shown to be successful (Hesser et al. 2012 ; Öst Citation2014). Hayes et al. (Citation1999) describe ACT as “… a psychological intervention based on modern behavioural psychology, including relational frame theory, that applies mindfulness and acceptance processes, and commitment and behaviour change processes, to the creation of psychological flexibility”.
Research shows that acceptance of tinnitus should not be seen as an end but a process of changing cognitive patterns referred to in these data as “sense making”. If thoughts are less aimed at control and more focussed on healthy living in spite of tinnitus, the impact of tinnitus is lowered. The importance of thinking patterns of this sort have been reported elsewhere (Westin, Hayes, and Andersson Citation2008a; Hesser et al. 2012, Citation2015). Interestingly, the process of acceptance as measured by acceptance based self-report measures appears to mediate treatment effects even in treatments believed to have different causal pathways underlying therapeutic change (Hesser et al. Citation2014; Moschen et al. Citation2015). Riedl et al. (Citation2015) explain this by hypothesising that acceptance may be influenced by psycho-education and other treatment elements (Adams, Verrier, and Walsh Citation2012). The results also suggest that acceptance may be influenced by non-treatment elements, e.g. following discourse with others, which is not referenced elsewhere in the literature. Recently, tinnitus acceptance and habituation have been related in terms of tinnitus adaptation, a recent low-quality cross-sectional study by Croft et al. (Citation2013) suggests that tinnitus acceptance may represent the cognitive response that precedes, underpins or facilitates the automatic perceptual/behavioural processing of tinnitus noise (i.e. tinnitus habituation), although this has yet to be tested empirically in a longitudinal study.
The process of putting tinnitus into perspective using comparisons and analogies bears similarities to rational-emotive behaviour therapy, which includes as a major component of treatment, the building of frustration tolerance, which amounts to increasing one’s acceptance of unpleasant elements of life (Ellis Citation2004). However, participants appear to be using this strategy unguided – perhaps this behaviour represents a logical cognitive process of sense-making or adjustment towards a chronic condition in order to move towards acceptance? A recent randomised controlled trial study has demonstrated that mindfulness approaches (which work on tolerance) has been more effective than relaxation control (Mckenna et al. Citation2017). Andersson and Edvinsson (Citation2008) also found that participants used comparisons in relation to how they identified with their tinnitus either positively or negatively. In a similar vein but focussed on models of adversarial growth, Davis and Morgan (Citation2008) used a cross-sectional study in patients with chronic tinnitus which highlighted a central role of meaning-making processes in pursuit of adaptation if a loss was perceived. Research to date suggests that acceptance has a unique role to play in tinnitus severity (Hesser, Bankestad, & Andersson Citation2015) and this study appears to lend support to this. Above all, this work builds on Dauman et al. (Citation2017) grounded theory analysis of cultivating a tolerance to frustration associated with tinnitus. This recognition of the active work and engagement of people experiencing tinnitus is becoming recognised. The process of sense making is an active part of building resilience and tolerance in tinnitus coping.
Beliefs about tinnitus
McKenna et al. (Citation2014) state that beliefs about tinnitus fuel negative thoughts and are based on experience of tinnitus in others or derive from general beliefs about health, the self, or the world. Unexpectedly, the results of this study appear to support these suppositions. McKenna et al. (Citation2014) speculate on whether beliefs about tinnitus need to be altered, this study tentatively suggests that they may need to be.
A key construct within the Common-Sense Model (CSM) of self-regulation of health and illness (Leventhal, Meyer, and Nerenz Citation1980), is the idea of illness representations or “lay” beliefs about illness. These representations are said to integrate with existing schemata, enabling individuals to make sense of their symptoms and guide coping actions (Hale, Treharne, and Kitas Citation2007). Coping actions are seen as mediators to outcomes (Hale, Treharne, and Kitas Citation2007), acceptance has been shown to mediate tinnitus distress (Westin, Hayes, and Andersson Citation2008a). Results from studies investigating tinnitus adjustment are in line with assumptions of the CSM – the way people think and feel about tinnitus and the way they cope with tinnitus are related to tinnitus adjustment (Budd and Pugh Citation1995; Reynolds, Gardner, and Lee Citation2004; Vollmann et al. Citation2012, Citation2014). The CSM makes no specific predictions about the role of and interaction with significant others but these can conceivably influence illness representations.
This work contributes to the understanding of how individuals integrate tinnitus into their lives. We have documented how thinking plays a part in self-management and build on the description by Audulv, Asplund, and Norbergh (Citation2012) and Dauman et al. (Citation2017).
Conclusions and clinical implications
Vollmann et al. (Citation2012) suggest that patients with chronic tinnitus may benefit from information provision and discussions about symptoms, timeline, possible treatments and likely consequences of tinnitus. The aim of interventions is to foster understanding and enhance perceptions of control, which may minimise the emotional impact of tinnitus and reduce the perceived severity of consequences. Understanding patients’ illness representations may help predict outcomes that are potentially alterable in a favourable way (Hale, Treharne, and Kitas Citation2007).
Acknowledgements
The authors would like to thank our participants.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Adams, J., E. Verrier, and M. Walsh. 2012. “Adults' Perceptions of Their Tinnitus and a Tinnitus Information Service.” Australian and New Zealand Journal of Audiology 32 (2): 83–94. http://hdl.handle.net/2328/37080
- Andersson, G., and E. Edvinsson. 2008. “Mixed Feelings about Living with Tinnitus: A Qualitative Study.” Audiological Medicine 6 (1): 48–54. doi:10.1080/16513860801899355
- Armentor, J. L. 2017. “Living with a Contested. Stigmatized Illness.” Qualitative Health Research 27 (4): 462–473. doi:10.1177/1049732315620160
- Audulv, Å., K. Asplund, and K. G. Norbergh. 2012. “The Integration of Chronic Illness Self-Management.” Qualitative Health Research 22 (3): 332–345. doi:10.1177/1049732311430497
- Baguley, D., G. Andersson, D. McFerran, and L. McKenna. 2013. Tinnitus: A Multidisciplinary Approach. 2nd ed. Chichester: Wiley.
- Budd, R. J., and R. Pugh. 1995. “The Relationship between Locus of Control, Tinnitus Severity, and Emotional Distress in a Group of Tinnitus Sufferers.” The Journal of Psychosomatic Research 39 (8): 1015–1018. doi:10.1016/0022-3999(95)00512-9
- Charmaz, K. 2014. Constructing Grounded Theory. 2nd ed. London: SAGE Publications Ltd.
- Cima, R. F., G. Crombez, and J. W. Vlaeyen. 2011. “Catastrophizing and Fear of Tinnitus Predict Quality of Life in Patients with Chronic Tinnitus.” Ear and Hearing 32 (5): 634–641. doi:10.1097/AUD.0b013e31821106dd
- Croft, C.,. R. F. Brown, E. B. Thorsteinsson, and W. Noble. 2013. “Is Tinnitus Acceptance the Same as Tinnitus Habituation?” The International Tinnitus Journal 18 (2): 143–148. https://www.researchgate.net/profile/Rhonda_Brown2/publication/273639185_Is_tinnitus_acceptance_the_same_as_tinnitus_habituation/links/5546d1280cf24107d3980914.pdf
- Dauman, N., and S. I. Erlandsson. 2012. “Learning from Tinnitus Patients' Narratives—A Case Study in the Psychodynamic Approach.” International Journal of Qualitative Studies on Health and Well-being 7 (1): 19540. doi:10.3402/qhw.v7i0.19540
- Dauman, N., S. I. Erlandsson, D. Albarracin, and R. Dauman. 2017. “Exploring Tinnitus-Induced Disablement by Persistent Frustration in Aging Individuals: A Grounded Theory Study.” Frontiers in Aging Neuroscience 9: 272. doi:10.3389/fnagi.2017.00272
- Davis, A., and A. El Refaie. 2000. Epidemiology of tinnitus. In: Tinnitus Handbook, edited by R. S. Tyler. San Diego, CA: Singular.
- Davis, C. G., and M. S. Morgan. 2008. “Finding Meaning, Perceiving Growth, and Acceptance of Tinnitus.” Rehabilitation Psychology 53 (2): 128. doi:10.1037/0090-5550.53.2.128
- Dawes, P., H. Fortnum, D. R. Moore, R. Emsley, P. Norman, K. Cruickshanks, A. Davis, et al. 2014. “Hearing in Middle Age: A Population Snapshot of 40- to 69-Year Olds in the United Kingdom.” Ear and Hearing 35 (3): e44. doi:10.1097/AUD.0000000000000010
- DiCicco-Bloom, B., and B. F. Crabtree. 2006. “The Qualitative Research Interview.” Medical Education 40 (4): 314–321. doi:10.1111/j.1365-2929.2006.02418.x
- Elliott, N., and A. Lazenbatt. 2005. “How to Recognise a 'quality' Grounded Theory Research Study.” The Australian Journal of Advanced Nursing 22 (3): 48–52. ISSN: 0813-0531
- Ellis, A. 2004. The Road to Tolerance: The Philosophy of Rational Emotive Behavior Therapy. Amherst, NY: Prometheus.
- Fabijanska, A., M. Rogowski, G. Bartnik, and H. Skarzynski. 1999. “Epidemiology of Tinnitus and Hyperacusis in Poland.” In Proceedings of the Sixth International Tinnitus Seminar, edited by J. Hazell. Cambridge, UK: The Tinnitus and Hyperacusis Centre. [Online] Available from: http://tinnitus.org/downloads/ [Accessed:11 April 2015].
- Gill, P., K. Stewart, E. Treasure, and B. Chadwick. 2008. “Methods of Data Collection in Qualitative Research: Interviews and Focus Groups.” British Dental Journal 204 (6): 291. doi:10.1038/bdj.2008.192
- Hale, E. D., G. J. Treharne, and G. D. Kitas. 2007. “The Common-Sense Model of Self-Regulation of Health and Illness: How Can We Use It to Understand and Respond to Our Patients' Needs?” Rheumatology 46 (6): 904–906. doi:10.1093/rheumatology/kem060
- Hayes, S. C., K. Strosahl, and K. G. Wilson. 1999. Acceptance and Commitment Therapy: Understanding and Treating Human Suffering. New York: Guilford.
- Hallam, R. S., S. Rachman, and R. Hinchliffe. 1984. “Psychological Aspects of Tinnitus.” In Contributions to Medical Psychology, edited by Rachman, S. Oxford: Pergamon.
- Hesser, H., Gustafsson, T., Lundén, C., Henrikson, O., Fattahi, K., Johnsson, E., Westin, V.Z., Carlbring, P., Mäki-Torkko, E., Kaldo, V. and Andersson, G., 2012. A randomized controlled trial of internet-delivered cognitive behavior therapy and acceptance and commitment therapy in the treatment of tinnitus. Journal of consulting and clinical psychology 80(4): p. 649. In: Journal of Consulting and Clinical Psychology, ISSN 0022–006X, E-ISSN 1939–2117, Vol. 80, no 4, p. 649–661.
- Hesser, H.,. E. Bankestad, and G. Andersson. 2015. “Acceptance of Tinnitus as an Independent Correlate of Tinnitus Severity.” Ear and Hearing 36 (4): e176–e182. doi:10.1097/AUD.0000000000000148
- Hesser, H.,. T. Gustafsson, C. Lunden, O. Henrikson, K. Fattahi, E. Johnsson, V. Zetterqvist Westin, H. Hesser, V. Z. Westin, and G. Andersson. 2014. “Acceptance as a Mediator in Internet-Delivered Acceptance and Commitment Therapy and Cognitive Behavior Therapy for Tinnitus.” Journal of Behavioral Medicine 37 (4): 756–767. doi:10.1007/s10865-013-9525-6
- Holmes, S., and N. D. Padgham. 2011. “Ringing in the Ears'': Narrative Review of Tinnitus and Its Impact.” Biological Research for Nursing 13 (1): 97–108. doi:10.1177/1099800410382290
- Leventhal, H., D. Meyer, and D. Nerenz. 1980. “The Common Sense Model of Illness Danger.” In Medical Psychology, edited by S. Rachman, 7–30. New York: Pergamon.
- Martinez, C., C. Wallenhorst, D. McFerran, and D. A. Hall. 2015. “Incidence Rates of Clinically Significant Tinnitus: 10-Year Trend from a Cohort Study in England.” Ear and Hearing 36 (3): e69. doi:10.1097/AUD.0000000000000121
- Martinez-Devesa, P., R. Perera, M. Theodoulou, and A. Waddell. 2010. “Cognitive Behavioural Therapy for Tinnitus.” The Cochrane Database of Systematic Reviews Sept 8 (9): CD005233. https://doi.org/http://www.hopefortinnitus.com/pdfs/Cochrane%20Review%20of%20CBT.pdf
- McKenna, L., E. M. Marks, C. A. Hallsworth, and R. Schaette. 2017. “Mindfulness-Based Cognitive Therapy as a Treatment for Chronic Tinnitus: A Randomized Controlled Trial.” Psychotherapy and Psychosomatics 86 (6): 351–361. doi:10.1159/000478267
- McKenna, L., L. Handscomb, D. J. Hoare, and D. A. Hall. 2014. “A Scientific Cognitive-Behavioral Model of Tinnitus: Novel Conceptualizations of Tinnitus Distress.” Frontiers in Neurology 5: 196. https://doi.org/10.3389/fneur.2014.00196
- Milerová, J., M. Anders, T. Dvořák, P. G. Sand, S. Königer, and B. Langguth. 2013. “The Influence of Psychological Factors on Tinnitus Severity.” General Hospital Psychiatry 35 (4): 412–416. doi:10.1016/j.genhosppsych.2013.02.008
- Moller, A. R. 2000. Similarities between Severe. Journal of the American Academy of Audiology 11(3): 115–124. https://audiology.org/sites/default/files/journal/JAAA_11_03_01.pdf
- Moschen, R., D. Riedl, A. Schmidt, M. Kumnig, H. R. Bliem, and G. Rumpold. 2015. “The Development of Acceptance of Chronic Tinnitus in the Course of a Cognitive-Behavioral Group Therapy.” Psychosomatic Medicine and Psychotherapy 61 (3): 238–246. https://doi.org/10.13109/zptm.2015.61.3.238
- Negrila-Mezei, A., R. Enache, and C. Sarafoleanu. 2011. “Tinnitus in Elderly Population: Clinic Correlations and Impact upon QoL.” Journal of Medicine and Life 4 (4): 412–416. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3227161/
- Öst, L. G. 2014. “The Efficacy of Acceptance and Commitment Therapy: An Updated Systematic Review and Meta-Analysis.” Behaviour Research and Therapy 61: 105–121. doi:10.1016/j.brat.2014.07.018
- Pryce, H. 2003. “Emotional Responses to King–Kopetzky Syndrome: A Qualitative Study.” Audiological Medicine 1 (4): 247–254. doi:10.1080/16513860310022381
- Riedl, D., G. Rumpold, A. Schmidt, P. G. Zorowka, H. R. Bliem, and R. Moschen. 2015. “The Influence of Tinnitus Acceptance on the Quality of Life and Psychological Distress in Patients with Chronic Tinnitus.” Noise and Health 17 (78): 374–381. https://dx.doi.org/10.4103%2F1463-1741.165068
- Reynolds, P., D. Gardner, and R. Lee. 2004. “Tinnitus and Psychological Morbidity: A Cross-Sectional Study to Investigate Psychological Morbidity in Tinnitus Patients and Its Relationship with Severity of Symptoms and Illness Perceptions.” Clinical Otolaryngology and Allied Sciences 29 (6): 628–634. doi:10.1111/j.1365-2273.2004.00879.x
- Saldaña, J. 2015. The Coding Manual for Qualitative Researchers. London: Sage.
- Sbaraini, A., S. M. Carter, R. W. Evans, and A. Blinkhorn. 2011. “How to Do a Grounded Theory Study: A Worked Example of a Study of Dental Practices.” BMC Medical Research Methodology 11 (1): 128. doi:10.1186/1471-2288-11-128
- Shargorodsky, J., G. C. Curhan, and W. R. Farwell. 2010. “Prevalence and Characteristics of Tinnitus among US Adults.” The American Journal of Medicine 123 (8): 711–718. doi:10.1016/j.amjmed.2010.02.015
- Stouffer, J. L., and R. S. Tyler. 1990. “Characterization of Tinnitus by Tinnitus Patients.” Journal of Speech and Hearing Disorders 55 (3): 439–453. doi: doi:10.1044/jshd.5503.439
- Tolley, E. E., P. R. Ulin, N. Mack, S. M. Succop, and E. T. Robinson. 2016. Qualitative Methods in Public Health: A Field Guide for Applied Research. San Francisco, CA: John Wiley & Sons.
- Tyler, R. S., and L. J. Baker. 1983. “Difficulties Experienced by Tinnitus Sufferers.” Journal of Speech and Hearing Disorders 48 (2): 150–154. doi: doi:10.1044/jshd.4802.150
- Vio, M. M., and R. H. Holme. 2005. “Hearing Loss and Tinnitus: 250 Million People and a US$10 Billion Potential Market.” Drug Discovery Today 10 (19): 1263–1265. https://pdfs.semanticscholar.org/e571/a4c63f6832484e03ddf23b741573b35b298f.pdf#page=4 doi:10.1016/S1359-6446(05)03594-4
- Vollmann, M., N. Kalkouskaya, B. Langguth, and M. Scharloo. 2012. “When the Ringing in the Ears Gets Unbearable: Illness Representations, Self-Instructions and Adjustment to Tinnitus.” The Journal of Psychosomatic Research 73 (2): 108–111. doi:10.1016/j.jpsychores.2012.04.009
- Vollmann, M., M. Scharloo, B. Langguth, N. Kalkouskaya, and C. Salewski. 2014. “Illness Representations as Mediators of the Relationship between Dispositional Optimism and Depression in Patients with Chronic Tinnitus: A Cross-Sectional Study.” Psychological Health 29 (1): 81–93. doi:10.1080/08870446.2013.828294
- Westin, V., S. C. Hayes, and G. Andersson. 2008. “Is It the Sound or Your Relationship to It? The Role of Acceptance in Predicting Tinnitus Impact.” Behaviour Research And Therapy 46 (12): 1259–1265. doi:10.1016/j.brat.2008.08.008
- Westin, V., R. Östergren, and G. Andersson. 2008. “The Effects of Acceptance versus Thought Suppression for Dealing with the Intrusiveness of Tinnitus.” The International Journal of Audiology 47 (Suppl 2): S112–S118. doi:10.1080/14992020802301688
- Wheeler, S. L., and A. G. Hopwood. 2015. “Tinnitus: A Deaf hearing Phenomenon.” Qualitative Inquiry 21 (2): 173–174. doi:10.1177/1077800414542700