
Abstract
This study aims to understand patterns in the social representation of hearing loss reported by adults across different countries and explore the impact of different demographic factors on response patterns. The study used a cross-sectional survey design. Data were collected using a free association task and analysed using qualitative content analysis, cluster analysis and chi-square analysis. The study sample included 404 adults (18 years and over) in the general population from four countries (India, Iran, Portugal and UK). The cluster analysis included 380 responses out of 404 (94.06%) and resulted in five clusters. The clusters were named: (1) individual aspects; (2) aetiology; (3) the surrounding society; (4) limitations and (5) exposed. Various demographic factors (age, occupation type, education and country) showed an association with different clusters, although country of origin seemed to be associated with most clusters. The study results suggest that how hearing loss is represented in adults in general population varies and is mainly related to country of origin. These findings strengthen the argument about cross-cultural differences in perception of hearing loss, which calls for a need to make necessary accommodations while developing public health strategies about hearing loss.
Introduction
Hearing impairment is one of the most common sensory impairments, especially among the elderly. According to the World Health Organisation (WHO) about 360 million people worldwide have disabling hearing loss (WHO Citation2017). In addition to difficulties in communicating, hearing impairment often causes psychological and social problems. Although the vast majority of these persons would be helped by hearing aids, most refrain from seeking professional help and undergoing audiological rehabilitation (Davis et al. Citation2007). Previous studies have shown that the willingness to seek help and to use hearing aids is affected by both external factors (e.g. health care organisation, the professionals’ knowledge and access to technology) and internal factors (e.g. demographic factors and coping strategies) (Knudsen et al. Citation2010). Also, a study on the influence of culture on help-seeking and hearing-aid uptake in the UK, Sweden, China and India (Zhao et al. Citation2015) suggests that society’s cultural norms, attitudes and views of aspects such as ageing and disability have a major impact on people’s behaviour and willingness to seek help and to use technical aids. Studies have shown that there are large differences between countries in terms of percentage of people with hearing loss who seek help and use hearing aids (for review see Strom Citation2013).
WHO highlights in the International Classification of Functioning, Disability and Health (ICF) that social norms as well as social and individual attitudes have great impact on people’s lives and actions (WHO Citation2001). This model provides a possibility to address different dimensions of functioning and disability (Leonardi et al. Citation2005). According to the model, health and disability are an interaction between aspects such as body structure, body function, activities, participation, environmental and personal factors. In general, environment may play an important role in people’s decision making. For example, people with various disabilities including hearing loss tend to be influenced by others in society (e.g. significant others, friends, colleagues and health professionals) in deciding whether to seek help, to pursue intervention and to make efforts to resolve their difficulties (Manchaiah, Stephens, and Meredith Citation2011). Preliminary studies during the development of the ICF core sets for hearing loss identified various factors related to society as important in relation to hearing loss (Granberg et al. Citation2014a, Citation2014b). However, research on societal factors is limited.
There are a quite a few studies on attitude towards people with hearing loss. These studies often include certain subgroups, e.g. significant others (Hallberg and Barrenäs Citation1993), co-workers (Hétu, Jones, and Getty Citation1993; Hétu, Getty, and Waridel Citation1994), teachers (Cox, Cooper, and McDade Citation1989) and class-mates (Stein, Gill, and Gans Citation2000). Attitudes among persons with a hearing loss have been studied with the Attitudes towards Loss of Hearing Questionnaire (ALHQ), further developed by Saunders et al. (Citation2005). The theory underpinning studies related to attitudes and ranking is most often Goffman’s theory of stigmatisation (Goffman Citation1968) and the attitude reflects cultural valuations and social meanings (Shakespeare Citation1994; Thomson Citation1997). However, an in-depth theoretical analysis is seldom conducted and research on attitudes is constrained, and does not grasp the broader perspective of these environmental factors.
A theory that has been developed in order to understand and explain not only a person’s worldview but also how it is related to behavioural aspects is the social representation theory. In this theory, the concept of attitude is addressed, and is here considered to be of a more individual character expressing a response to a stimulus, based on previous representations of the object (Carle et al. Citation2006). This view leads to the position that an attitude is a part of a representation and that our representations govern our attitudes (Germundsson Citation2015). The theory is about our everyday knowledge and offers a possibility to describe and explain the group’s beliefs about the world, built together with others through social interaction. The founder of the theory, the French social psychologist Serge Moscovici, defines social representations as a system of values, ideas and practices with a twofold function (Moscovici Citation1973, p. xiii). First, they enable people to orientate themselves in their material and social world and, second, they enable communication by providing individuals with a code for naming and classifying various aspects of their world (ibid.). Two influencing factors are highlighted in the theory: the historical context and the role of the mass media in modern society. Thus, representations can be seen as expressions of our contemporary culture with all its symbolic and iconic forms of expression (Chaib and Orfali Citation1995).
With this background, an interdisciplinary and international multi-centre research project that aimed to explore social representations of “hearing loss” and “hearing aids” in different countries was initiated (Manchaiah et al. Citation2015a, Citation2015b). Results from previous studies show that the social representations differ between the participating countries (India, Iran, Portugal and the UK). For example, participants in India reported more positive associations to “hearing loss” compared to participants from the other countries. Also, comparing data across countries suggested differences in the social representations of “hearing aids”. In Great Britain, for instance, participants had more frequent associations with appearance and design, whereas in Iran associations with disability and ageing were more prominent. However, the previous studies focused on common perceptions in general public across different countries, without addressing whether the perceptions of participants would vary based on their demographic characteristics. This study is part of the same research project in which further analysis was performed on the same data set with all four countries’ combined. Our aim is to discover whether individual demographics are associated with different representations of hearing loss.
Methods
Ethical considerations
Ethical approval was obtained for each country from local institutional ethical boards. These included: All India Institute of Speech and Hearing, Mysore, India; Department of Audiology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran; School of Allied Health Sciences, Polytechnic Institute of Porto, Porto, Portugal; and Research Ethics Committee, Anglia Ruskin University, Cambridge, UK.
Study design and participants
Participants were recruited using the snowball sampling methodology. In each country the researcher approached his or her colleagues and friends in the workplace (i.e. university), requesting them to take part in the study and also to help in recruiting more participants through their acquaintances. The study sample consisted of individuals with no particular knowledge on hearing loss, although it included a few elderly individuals with hearing difficulties. All those who were approached were given a study information sheet and had the opportunity to ask questions of the researcher. Those who agreed to participate completed the questionnaire, and return of the questionnaire was taken as consent. The study sample included 404 adults (aged 18 years and over) in general population from four countries (i.e. India, Iran, Portugal and UK). The mean age of the participants was 41 years. Half of the participants were men and half were women. Almost 60% were persons with tertiary education, and 46% had a non-manual profession (see ).
Table 1. Demographic details of participants.
Data collection
The data were collected using a questionnaire. One of the researchers (V. M.) coordinated the data collection with regular online meetings and email interactions to ensure that the method was consistently followed. The questionnaire required participants to report up to five words or phrases that immediately come to mind while thinking about hearing loss. 396 of the 404 respondents (98%) provided five words or phrases. Seven of the participants provided four associations and one person provided only two. The method is known as the free association task, which is frequently used to access the semantic content of social representation. This is a well-established method and has been used in several studies (Linton et al. Citation2013; Danermark et al. Citation2014). The object of representation (i.e. hearing loss) is used to prompt associations. Due to the spontaneous way in which these responses are elicited, they are considered less controlled; hence, they provide a better understanding of what constitutes the semantic universe of the term or subject being studied (Abric Citation1994). In addition, demographic information (i.e. age, gender, education, profession and family history of hearing loss) was also recorded.
The original version of the questionnaire was in English and was used in the UK. It was also translated into Kannada, Farsi and Portuguese. The translated versions were used in India, Iran and Portugal, respectively. It is important that the questionnaire should be conceptually valid across different languages to be able to use it in different countries. The well-accepted methods of forward and back-translation were incorporated (Beaton et al. Citation2000). The process aimed to achieve different language versions of the questionnaire that were conceptually equivalent in each of the target countries, and the focus was on cross-cultural and conceptual equivalence rather than on linguistic/literal. The process of translating involved: (a) forward translation; (b) expert back translation; (c) review and resolution of any discrepancies and (d) pre-testing with five participants each in different countries. The translation of the collected data from the local language to English was made by the researchers who collected the data in each country. Words and phrases were discussed and cross-checked before the categorisation process started.
The questionnaire did not contain any information that could identify the individual who completed the questionnaire. Data were shared with the researchers who were conducting the analysis, and assigned a case number.
Data analysis
For this article data from all four countries were combined, and analysed together in order to investigate differences based on demographic factors. First, the responses from free association task were analysed using qualitative content analysis (Graneheim and Lundman Citation2004). This step involved grouping of words and phrases that have the same meaning into categories. The data analysis from all countries was done mainly by one of the researchers (V. M.) and cross-checked by another researcher (P. G.). If the meaning of the words or phrases was not clear, or consensus was not reached, the researchers who collected and translated data in the respective countries were consulted.
Second, a cluster analysis was done with the Reinert algorithm (Reinert Citation1983, Citation1990; Ratinaud and Marchand Citation2012). This method is a hierarchical divisive clustering. The starting point is a 0/1 matrix which cross individuals in line and categories in column. A correspondence analysis (which is the equivalent of principal component analysis for categorical data) is made on this matrix, and coordinates of individuals on the first factor are used to split the matrix in two different groups. The created groups tend to share similar pattern of answers (which is translated by similar 0/1 line in sub-matrix). This operation is done on sub-matrix until the number of clusters provided as parameters is reached. The produced clusters are groups of individuals who tend to be homogeneous in their answers within each clusters, and heterogeneous between clusters. In these steps, only categories of free associations are used. The secondary variables (demographic details) are crossed with the clusters a posteriori. A chi-square analysis is carried out to explore whether any of the primary variables (main categories identified from content analysis) or the secondary variables (demographic details) had significant association with any of the clusters. The computation of these values follows the same logic as in the lexical analysis; the proportion of individuals with a particular category within the cluster is compared to the proportion of individuals with the category in the rest of the sample to determine which categories are over-represented in each cluster. Thus, the presence of a category in a cluster indicates a proportion of individuals in this category within the cluster significantly higher than the proportion found in the rest of the sample. The process summarises the specificities of the epistemological subjects outlined by clusters in a list of over-represented categories and demographic modalities. This analysis was performed using the Iramuteq software (R Development Core Team Citation2014; Ratinaud Citation2014).
Results
The content analysis resulted in 34 categories and the detailed results have been presented elsewhere (Manchaiah et al. Citation2015a). presents in alphabetical order the list of categories and the frequency of those categories (all countries put together). The most frequently occurring categories included: assessment and management, causes of hearing loss, communication difficulties, disability, hearing ability or disability, hearing instruments, negative mental state, others’ attitudes, and sound and acoustics of the environment.
Table 2. Percentage of categories reported in different countries (adapted from Manchaiah et al. Citation2015b) and the percentage of respondents mentioning each category.
Following the qualitative content analysis, the cluster analysis was performed to identify patterns within the dataset. The cluster analysis included 380 responses out of 404 (i.e. 94.06%) and resulted in five clusters as shown in the dendrogram (see ). The remaining 24 respondents (i.e. 5.94%) were discarded by the software as being too deviant from rest of the data (i.e. outliers). The cluster names are based on the main categories included in each cluster (see ). Two pairs of clusters, aetiology and individual aspects and also limitations and the surrounding society were fairly close based on the cluster analysis. However, the cluster exposed is connected to the first pair of clusters.
Figure 1. Cluster analysis of hearing loss social representation.
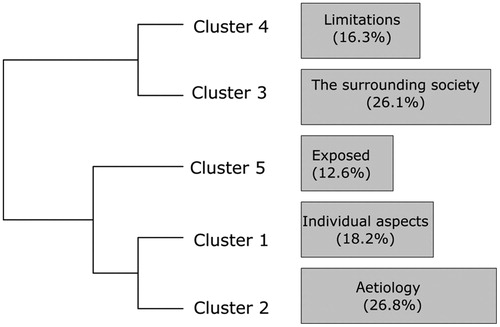
Table 3. Individual aspects (cluster 1).
Table 4. Aetiology (cluster 2).
Table 5. The surrounding society (cluster 3).
Table 6. Limitations (cluster 4).
Table 7. Exposed (cluster 5).
Cluster 1 – individual aspects
A total of 18.2% of the respondents (i.e. 69 out of 380) were assigned to the cluster individual aspects. In this cluster, the categories were mainly connected to individual characteristics and aspects. However, it should be noted that this cluster contains categories that could also be interpreted as being of a more environmental character. For instance the biggest category, alternative mode of communication, contains associations such as sign language and written/gestural mode of communication.
The respondents in this cluster were significantly more likely to report the categories: alternative modes of communication, hearing ability or disability, body structure, coping strategies, dependence on other senses, sound and acoustics of the environment and disability (see ). Chi-square analysis suggested that participants with secondary education (X2=11.6; p = 0.00065), no occupation (X2=6.70; p = 0.0008) and young adults (X2=4.49; p = 0.03341) appeared to be significantly more likely to be in this cluster. A p value of 0.05 was used for all significance interpretations.
Cluster 2 – aetiology
Cluster 2, named aetiology, contained 26.84% of the respondents (i.e. 102 out of 380). Most of the categories in this cluster have to do with body structure, i.e. biological aspects. It also contains the category hearing instruments – which could be interpreted as a tool for enhancing the body function.
The respondents in this cluster were significantly more likely to report the categories: causes of hearing loss, ageing, disability, body structure, voice and speech functions, hearing instruments, and assessment and management (see ). Chi-square analysis suggested that participants from Iran (X2=31.99; p ≤ 0.0001) are significantly more likely to be in this cluster. However, no other of the demographic variables appeared to be associated with inclusion in the cluster.
Cluster 3 – the surrounding society
Cluster 3, named the surrounding society, consisted of 26.1% of the respondents (i.e. 99 out of 380). The largest categories in this cluster (negative mental state, communication difficulties and others’ attitudes) contain associations where the respondents mention the relationship between persons with hearing loss and persons in the surrounding society. Also, environmental conditions such as activity limitations and education, employment and career issues are mentioned.
The respondents in this cluster were significantly more likely to report the categories: challenging, lifestyle and relationship changes, negative mental state, dependence on others, problem for others, communication difficulties, others’ attitudes, positive mental state, friends and family members, reduced ability, education, employment and career issues, and activity limitations (see ). Chi-square analysis suggested that participants from Portugal (X2=4.78; p = 0.02884), those with compulsory education (X2=8.77; p ≤ 0.0001), and older adults (X2=8.77; p = 0.00306) appeared to be significantly more likely to be in this cluster.
Cluster 4 – limitations
Cluster 4, named limitations, contained 16.32% (i.e. 62 out of 380) of the respondents. This cluster appears more closely connected to categories containing limiting aspects, such as negative mental state, isolation and activity limitations. The category sound and acoustics of the environment contains associations concerning sound and noise, or the absence of those. This category is also present in the individual aspects cluster. This is an example of how the categories can be interpreted somewhat differently; whether the respondents primarily think of sound as an (inevitable) part of the society or sound is more perceived as a factor affecting the individual.
The respondents in this cluster were significantly more likely to report the categories isolation, negative mental state, orientation, stress and exhaustion, attitude of the individual, sound and acoustics of the environment, and activity limitations (see ). Chi-square analysis suggested that participants from UK (X2=4.6; p = 0.03204) and those with tertiary education (X2=5.28; p = 0.02156) appeared to be significantly more likely to be in this cluster.
Cluster 5 – exposed
Cluster 5, named exposed, contained 12.63% (i.e. 48 out of 380) of the respondents. Most of the categories in this cluster concern the situation for persons with hearing loss, and that the individual is exposed and dependent on others. This is indicated by categories as need for support and not well understood. The cluster also suggests that respondents connect those categories to health condition and assessment and management, which in turn contains associations such as doctor, hearing test and treatment.
The respondents in this cluster were significantly more likely to report the categories health condition, need for support, social support, not well understood, assessment and management and others’ attitudes (see ). Chi-square analysis suggested that participants from India (X2=31.99; p ≤ 0.0001) and those with tertiary education (X2=113.98; p ≤ 0.0001) appeared to be significantly more likely to be in this cluster.
Discussion
This study explored the patterns in the social representation of hearing loss reported by adults in the general population in different countries, focusing on whether demographic characteristics are associated with different representations. The study indicates that only a few demographic factors are associated to the response patterns. These factors seem to play a minor role, which can be interpreted as the social representation being robust in relation to demographic factors. However, different levels of education are related to four clusters (1, 3, 4 and 5), different age is related to two clusters (1 and 3) and being unemployed is related to one cluster (1). Another finding is that country of origin is significantly associated to four clusters (2, 3, 4 and 5), which suggests cross-cultural differences in the perception of hearing loss.
The dendrogram (see ) suggest a split between clusters. The three clusters aetiology, individual aspects and exposed appear to be closer (forming a cluster group), whereas the remaining two clusters limitations and the surrounding environment appear to be grouped together (forming another cluster group). This split into cluster groups can be perceived and interpreted in the light of the biopsychosocial model of disability, a holistic approach that is the starting point for the ICF (WHO Citation2001). In this study, biological factors are the main focus in the clusters aetiology and individual aspects. Here we find the categories causes of hearing loss and ageing (in aetiology), and alternative modes of communication and hearing ability or disability (in individual aspects). In other words, in these clusters the respondents were significantly more likely to provide associations in those categories. In both those clusters we also find the categories body structure and disability. In addition, the cluster exposed also mainly focuses on biological aspects. This cluster contains categories such as health condition and assessment and management. However, in this cluster, which is more loosely connected to those focusing on biological aspects, we also find categories that can be assigned to social factors, as need for support, others’ attitudes and social support.
The other two clusters, i.e. the surrounding society and limitations, mainly focus on societal factors. For example, the categories negative mental state (in the surrounding society) and isolation and activity limitations (in limitations). Within these clusters the respondents think of the relation between persons with hearing loss and the world that surrounds them.
It is important to note that the clusters in these two groups are not mutually exclusive. For instance, the categories others’ attitudes and attitude of the individual are found in both groups. Moreover, it appears as if communicational factors form an ‘analytic bridge’ that spans between the biological and social factors. This bridge is found in the fact that categories containing communication aspects (e.g. alternative modes of communication and communication difficulties) are present in both groups of clusters. This indicates that communication is a key aspect of hearing loss and underlines the importance of addressing hearing issues with a holistic and biopsychosocial perspective (Manchaiah and Danermark Citation2017). This is further underlined by Granberg et al. (Citation2014a) who emphasis that: “Humans are typically communicating beings, and participation restriction in relation to communication is likely one of the most important restrictions for any human being. For persons with HL, this restriction is a highly recognised negative consequence of the health condition”.
The social representation theory states that the way we perceive our surrounding world, or our everyday knowledge of it, affects how we act. For instance, young people’s beliefs and attitudes towards hearing loss, noise, and hearing protector devices have a significant impact on their use of such devices as well as on their hearing status (Keppler, Dhooge, and Vinck Citation2015). Various societal factors (e.g. societal attitudes, social norms, practices and ideologies) are reported to influence the help-seeking and rehabilitation uptake in people with hearing loss (Granberg et al. Citation2014b, Citation2014c), although limited literature exists in this area. In this context, then, this insight shows that when it comes to addressing the problem of people not seeking help and low levels of hearing aids uptake it is important for rehabilitation personnel to address not only the individual (and biological aspects) but also psychological and social factors, including communication partners and societal attitudes.
Another finding is that respondents from the Asian countries (i.e. Iran and India) are more likely to be in first cluster group (biological) and respondents from the European countries are more likely to belong to second cluster group (social). This is somewhat surprising compared to previous cross-cultural studies by Hofstede, which found that European countries are more likely to be more individual (priority to individual needs and to self-care) and Asian countries are more collective (priority to group’s needs, to close friends and family) (Hofstede Citation2010). However, studies by Hofstede were mainly conducted on employees of software companies, whereas our data comes from the general population. Hence, further studies are needed to understand what factors result in cross-cultural similarities and differences in terms of perception of and attitude towards various disabilities including hearing loss.
The theory of social representations provides an opportunity to capture and interpret social differences regarding hearing loss that have to do with values (as well as beliefs, attitudes, ideas and views and the like) which play a significant role in shaping social policies regarding hearing loss. The interdisciplinary field of study known as Science and Technology Studies has shown that social policies regarding hearing loss may also be advanced through the values embedded in the design of materialities that range from “hearing instruments/aids” to the “sound and acoustics of the [built] environment” (Blume Citation2012). While we acknowledge that there are values that may be implicitly advanced through design, and that these implicit values may frequently be very significant, we here focus on explicitly expressed values. This focus further justifies our decision to rely on the social representation theory, which is tailored to the study of expressed values like the ones we sought to collect through our study. The results may be useful while developing, for instance, public health campaigns about hearing loss in prioritising what message may be given to which groups of individuals in terms of hearing disability.
The strength of this study is that it is an international multi-centre study and gives an opportunity to explore differences and similarities in how hearing loss is perceived in a cross-cultural perspective. However, the study has some limitations that should be considered. The sampling method used and the sample size may have resulted in some bias. We gathered the data in the local language and then translated before the analysis. This may have some bearing towards the categorisation of responses (Santos, Black, and Sandelowski Citation2015). Also, in the process of categorisation some element of subjectivity may have existed. We tried to overcome these obstacles through a translation process involving the researchers who collected the data, and a process where categorisation was made with consensus from two of the researchers.
Conclusions
This study explored the patterns in the social representation of hearing loss reported by adults in the general population in different countries. The cluster analysis resulted in five clusters, which were named: (1) individual aspects; (2) aetiology; (3) the surrounding society; (4) limitations and (5) exposed. The study indicates that demographic factors have relatively limited impact on the response patterns. However, various demographic factors (age, occupation type, education and country) showed associations with different clusters, although country of origin seemed to be associated with most clusters. The study results suggest that how hearing loss is represented in adults in the general population varies and is mainly related to country of origin. These findings strengthen the argument about cross-cultural differences in perception of hearing loss, which calls for a need to make necessary accommodations while developing public health strategies about hearing loss.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Abric, J. C. 1994. “Méthodologie de Recueil des Representations Sociales.” In Pratiques Socials et Représentations, edited by J.C. Abric, Paris: P.U.F.
- Beaton, D. E., C. Bombardier, F. Guillemin, and M. B. Ferraz. 2000. “Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures.” Spine 25 (24): 3186–3191. doi:10.1097/00007632-200012150-00014.
- Blume, S. 2012. “What Can the Study of Science and Technology Tell us About Disability?” In Routledge Handbook of Disability Studies, edited by N. Watson, A. Roulstone, and C. Thomas, London, NY: Routledge.
- Carle, J., B. Nilsson, J. L. Alvara, and A. Garrido. 2006. Socialpsykologi. Bakgrund, Teorier Och Perspektiv. Lund, Sweden: Studentlitteratur.
- Chaib, M., and B. Orfali. 1995. Sociala Representationer. Om Vardagsvetandets Sociala Fundament. Göteborg, Sweden: Daidalos.
- Cox, L. R., W. A. Cooper, and H. L. McDade. 1989. “Teachers´Perceptions of Adolescent Girls Who Wear Hearing Aids.” Language Speech and Hearing Services in Schools 20 (4): 372–380. doi:10.1044/0161-1461.2004.372.
- Davis, A., P. Smith, M. Ferguson, D. Stephens, and I. Gianopoulos. 2007. “Acceptability, Benefits and Costs of Early Screening of Hearing Disability: A Study of Potential Screening Tests and Models.” Health Technology Assessment 11 (42): 1–294. doi:10.3310/hta11420.
- Danermark, B., U. Englund, P. Germundsson, and P. Ratinaud. 2014. “French and Swedish Teachers’ Social Representations of Social Workers.” European Journal of Social Work 17 (4): 491. doi:10.1080/13691457.2013.829803.
- Germundsson, P., 2015. “Inclusive Education and Social Representations.” In Inclusive Education – Perspektiven und Entwicklungen im Internationalem Vergleich, edited by G. Hensen, and A. Beck, Landsberg, Germany: Beltz Juventa.
- Goffman, E. 1968. Stigma: Notes on the Management of Spoiled Identity. Harmondsworth, England: Penguin.
- Granberg, S., J. Dahlström, C. Möller, K. Kähäri, and B. Danermark. 2014a. “The ICF Core Sets for Hearing Loss: Researcher Perspective, Part I: Systematic Review of Outcome Measures Identified in Audiological Research.” International Journal of Audiology 53 (2): 65–76. doi:10.3109/14992027.2013.851799.
- Granberg, S., K. Möller, A. Skagerstrand, C. Möller, and B. Danermark. 2014b. “The ICF Core Sets for Hearing Loss: Researcher Perspective, Part II: Linking Outcome Measures to the International Classification of Functioning, Disability and Health (ICF).” International Journal of Audiology 53 (2): 77–87. doi:10.3109/14992027.2013.858279.
- Granberg, S., D. W. Swanepoel, U. Englund, C. Möller, and B. Danermark. 2014c. “The ICF Core Sets for Hearing Loss Project: International Expert Survey on Functioning and Disability of Adults with Hearing Loss Using the International Classification of Functioning, Disability, and Health (ICF).” International Journal of Audiology 53 (8):497–506. doi:10.3109/14992027.2014.900196.
- Graneheim, U. H., and B. Lundman. 2004. “Qualitative Content Analysis in Nursing Research: Concepts, Procedures and Measures to Achieve Trustworthiness.” Nurse Education Today 24 (2): 105–112. doi:10.1016/j.nedt.2003.10.001.
- Hallberg, L. M., and M. L. Barrenäs. 1993. “Living with a Male with Noise-induced Hearing Loss: Experiences from the Perspective of Spouses.” British Journal of Audiology 27 (4): 255–261. doi:10.3109/03005369309076702.
- Hétu, R., L. Jones, and L. Getty. 1993. “The Impact of Acquired Hearing Impairment on Intimate Relationships: Implications for Rehabilitation.” International Journal of Audiology 32 (6): 363–381. doi:10.3109/00206099309071867.
- Hétu, R., L. Getty, and S. Waridel. 1994. “Attitudes towards co-Workers Affected by Occupational Hearing Loss. II: Focus Groups Interviews.” British Journal of Audiology 28 (6): 313–325. doi:10.3109/03005369409077315.
- Hofstede, G. 2010. Cultures and Organizations: Software of the Mind. New York, NY: McGraw Hill.
- Keppler, H., I. Dhooge, and B. Vinck. 2015. “Hearing in Young Adults. Part I: The Effects of Attitudes and Beliefs toward Noise, Hearing Loss, and Hearing Protector Devices.” Noise and Health 17 (78): 237–244. doi:10.4103/1463-1741.165024.
- Knudsen, L. V., M. Oberg, C. Nielsen, G. Naylor, and S. E. Kramer. 2010. “Factors Influencing Help Seeking, Hearing Aid Uptake, Hearing Aid Use and Satisfaction with Hearing Aids: A Literature Review.” Trends in Amplification 14 (3): 127–154. doi:10.1177/1084713810385712.
- Leonardi, M., T. J. Steiner, A. T. Scher, and R. B. Lipton. 2005. “The Global Burden of Migraine: Measuring Disability in Headache Disorders with WHO’s Classification of Functioning, Disability and Health (ICF).” The Journal of Headache and Pain 6 (6): 429–440. doi:10.1007/s10194-005-0252-4.
- Linton, A. C., P. Germundsson, M. Heimann, and B. Danermark. 2013. “Teachers’ Social Representation of Students with Aspergers Diagnosis.” European Journal of Special Needs Education 28 (4): 392–412. doi:10.1080/08856257.2013.812404.
- Manchaiah, V. K., D. Stephens, and R. Meredith. 2011. “The Patient Journey of Adults with Hearing Impairment: The Patients’ Views.” Clinical Otolaryngology 36 (3): 227–234. doi:10.1111/j.1749-4486.2011.02320.x.
- Manchaiah, V., B. Danermark, T. Ahmadi, D. Tomé, K. Rajalakshmi, F. Zhao, Q. Li, and P. Germundsson. 2015a. “Social Representation of ‘Hearing Loss’: Cross-Cultural Exploratory Study in India, Iran, Portugal and United Kingdom.” Clinical Interventions in Aging 10: 1857–1872. doi:10.2147/CIA.S91076.
- Manchaiah, V., B. V. Danermark, T. Ahmadi, D. Tomé, K. Rajalakshmi, and P. Germundsson. 2015b. Social Representation of ‘Hearing Aids’: Cross-cultural Study in India, Iran, Portugal and United Kingdom. Clinical Interventions in Aging, 10: 1601–1615. doi:10.2147/CIA.S86108.
- Manchaiah, V, and B. Danermark, eds. 2017. The Experience of Hearing Loss: Journey through Aural Rehabilitation. Oxon, NY: Routledge.
- Moscovici, S. 1973. Foreword. In Health and Illness: A Social Psychological Analysis, edited by C. Herzlich, London, NY: Academic Press.
- R Development Core Team 2014. “A language and environment for statistical computing [Online].” Accessed 01 July. http://www.R-project.org
- Ratinaud, P. 2014. “IRaMuTeQ: Interface de R Pour Les Analyses Multidimensionnelles de Textes et de Questionnaires (Version 0.7 Alpha 2) [Windows, GNU/Linux, Mac OS X].” Consulté à L’adresse http://www.iramuteq.org.
- Ratinaud, P., and P. Marchand. 2012. “Improbable Search of a Homogenous Diversity: The Debate on National Identity.” Langages 187 (3): 93–107. doi:10.3917/lang.187.0093.
- Reinert, M. 1983. “Une Méthode de Classification Descendante Hiérarchique: Application à L’analyse Lexicale Par Contexte.” Les Cahiers de L’analyse Des Données VIII (2): 187–98. http://eudml.org/doc/88079.
- Reinert, M. 1990. “ALCESTE, Une Méthodologie D’analyse Des Données Textuelles et Une Application: Aurélia de G. de Nerval.” Bulletin de Méthodologie Sociologique 26 (1): 24–54. doi:10.1177/075910639002600103.
- Santos, H. P. O., A. M. Black, and M. Sandelowski. 2015. “Timing of Translation in Cross-Language Qualitative Research.” Qualitative Health Research 25 (1): 134–144. doi:10.1177/1049732314549603.
- Saunders, G. H., K. M. Cienkowski, A. Forsline, and S. Fausti. 2005. “Normative Data for the Attitudes towards Loss of Hearing Questionnaire.” Journal of the American Academy of Audiology 16 (9): 637–652. doi:10.3766/jaaa.16.9.2
- Shakespeare, T. 1994. “Cultural Representation of Disabled People: Dustbins for Disavowal.” Disability & Society 9 (3): 283–299. doi:10.1080/09687599466780341.
- Stein, R., K. Gill, and D. Gans. 2000. “Adolescent´s Attitudes toward Their Peers with Hearing Impairments.” Journal of Educational Audiology 8: 1–8. www.edaud.org/journal/2000/1-article-00.pdf.
- Strom, K. 2013. “Staff standpoint: Worldwide hearing aid sales.” Hearing Review. Accessed 20 March 2017. http://www.hearingreview.com/2013/05/staff-standpoint-worldwide-hearing-aid-sales/.
- Thomson, R. G. 1997. Extraordinary Bodies: Figuring Physical Disability in American Culture and Literature. New York, NY: Columbia University Press.
- WHO (World Health Organization). 2001. International Classification of Functioning, Disability and Health. Geneva: World Health Organization.
- WHO (World Health Organization). 2017. “Deafness and hearing loss.” Accessed 20 March 2017. http://www.who.int/mediacentre/factsheets/fs300/en
- Zhao, F., V. Manchaiah, St. L. Claire, B. Danermark, L. Jones, M. Brandreth, K. Rajalakshmi, and R. Goodwin. 2015. “Exploring the Influence of Culture on Hearing Help-Seeking and Hearing-Aid Uptake.” International Journal of Audiology 54 (7): 435–443. doi:10.3109/14992027.2015.1005848.