
Abstract
Objective: We conducted a retrospective review of medical records of tinnitus patients at a tertiary ENT clinic in Groningen, Netherlands. Our goal was to identify factors that differentiated the intermittent subgroup from the larger continuous group with chronic tinnitus.
Design: Tinnitus-related factors such as hearing loss, emotional aspects, and demographics were used to advance our understanding of the subgroups. We analysed the data using descriptive statistics and binomial logistic regression, supplemented by random forests classification.
Study sample: Patients presenting with tinnitus visiting the tinnitus clinic. We examined 1575 medical intake records obtained at a tertiary ENT hospital.
Results: Duration, total Tinnitus Handicap Inventory (THI), and THI Functional subscale scores differed significantly between the two groups. Increasing age and higher THI Emotional subscale scores were associated with an increased likelihood of intermittent tinnitus. Increases in duration, depressive scores and THI Functional and Catastrophic subscale scores, decreased the likelihood of intermittent tinnitus.
Conclusions: Results from this study dissociate the factors affecting those with intermittent and those with continuous tinnitus and point to potentially different mechanisms underlying the two conditions.
Introduction
Tinnitus is the perception of sound in the absence of an external source. It is a common and potentially debilitating condition. Similar to epidemiological surveys in other countries, a recent Dutch study estimated that the prevalence of tinnitus is 10% in the general population, of which 60% report having mild to moderate complaints and 40% have severe complaints (Maes et al. Citation2013). When severe, tinnitus is related to a profound reduction in the quality of life (Erlandsson and Hallberg Citation2000). The aetiology of tinnitus is largely unknown. However, a majority of tinnitus patients have some amount of hearing loss (Tan et al. Citation2013). A key hypothesis is that tinnitus is caused by maladaptive neural plasticity as a result of hearing loss (Shore, Roberts, and Langguth Citation2016). Clinical evidence suggests that, despite this common trait, tinnitus may not be homogeneous. Instead, the umbrella term tinnitus includes several subgroups. The neurophysiological underpinnings of these different types of tinnitus are currently unknown. Tinnitus can be categorised as continuous, intermittent or temporary. Both continuous and intermittent tinnitus are chronic conditions, whereas an acute episode of tinnitus that does not recur is considered to be temporary (Henry et al. Citation2016). In intermittent tinnitus, periods of presence and absence of the tinnitus alternate, and occur in a more or less periodic fashion (Humphriss, Hall, and Baguley Citation2016; Oiticica and Bittar Citation2015). This contrasts with patients who perceive tinnitus constantly.
Currently there is no established definition of intermittent tinnitus. Tinnitus tends to vary within an individual over the course of a day or over several days. Differences in pitch, loudness, sound quality and the bothersome nature of the sound are reported. In contrast, those with intermittent tinnitus report that at times they experience complete relief of their symptoms, i.e. that it is simply not perceived or is absent for a certain period of time.
The prevalence of intermittent tinnitus is not well described in the literature and estimates vary. A PubMed search [Search keywords: intermittent tinnitus and prevalence] produced nine English articles, of which three were about tinnitus as a symptom of other disorders and two were related to comorbid effects or interventions. Of the remaining five studies, one reported the prevalence of tinnitus in children (Humphriss et al. Citation2016) and the other four described adult populations. Of 100 veterans, 25% reported intermittent tinnitus compared to 42% reporting continuous tinnitus (Henry et al. Citation2016). Another study from Brazil reported that of individuals with tinnitus, 68% reported having intermittent tinnitus and 32% reported having continuous tinnitus (Oiticica and Bittar Citation2015). A study conducted at a Nigerian University Hospital showed that of the patients who reported tinnitus, 76% had intermittent tinnitus whereas 24% reported having continuous tinnitus (Sogebi Citation2013). Despite the large proportion of people with intermittent tinnitus, the characteristics of this population are not well described.
The limited and variable information about intermittent tinnitus makes treating it a challenge. Further, this subtype may offer a window into the possible mechanisms of tinnitus by the contrasting periods of “on” and “off” tinnitus. Greater knowledge of factors that mediate the switching on or off of the tinnitus periods in individuals with intermittent tinnitus may allow us to better understand the mechanisms that make tinnitus chronic. This, in turn, will help us understand the risk factors influencing the presence of tinnitus and potential protective factors present during a period the tinnitus is off. The non-specificity of current treatment methods is due to our incomplete understanding of the neural mechanisms of tinnitus. Better understanding of the risk factors associated with intermittent tinnitus and dissociating it from continuous tinnitus may lead to better treatment options for both groups.
The question about whether an individual’s tinnitus is intermittent or continuous is routinely asked in clinics. In this study, we investigated if there are consistent differences across the two categories with regard to perceptual characteristics, e.g. the presence of tinnitus, and emotional responses, e.g. the bothersomeness of the tinnitus.
Records maintained at a tertiary Ear, Nose and Throat (ENT) clinic in the northern Netherlands provided an excellent opportunity for investigating the intermittent subgroup and its distinguishing characteristics. At the University Medical Centre in Groningen, a tinnitus-specific consultation is set up and patients from all over the country attend the clinic. As a result, a large database has been developed over the last 10 years that contains a large array of tinnitus-related measurements, including a specific question on whether the tinnitus is continuous or intermittent. It is unlikely that the patients included have temporary tinnitus, due to the tertiary nature of the clinic and consequent time that has elapsed between the first visit to a physician and admittance to the tinnitus consultation. This database provided us with robust means to study the prevalence of intermittent tinnitus within the larger tinnitus population and to investigate the characteristics of this subgroup. Thus, the aim of the present study was to investigate the prevalence rate of intermittent tinnitus and to identify the risk factors associated with intermittent tinnitus compared to continuous tinnitus.
Materials and methods
A retrospective review was conducted on anonymized data collected during the tinnitus consultation at the ENT department of the University Medical Centre Groningen. Patients referred to this consultation had visited other health professionals first and needed a referral. In addition to this, they typically underwent a wait time of 6–12 weeks before being seen. The data were collected in the period between 2007 and 2015. During this tertiary consultation, medical information and data on physical and psychological well-being were collected. Patients were asked to complete several questionnaires during the initial visit. One of the questions asked was: “Is your tinnitus continuous or intermittent?” Patients who ticked the box “Intermittent” were classified as such in the database constructed for the purpose of this study. Of the 1575 patients who attended, 161 reported having symptoms of intermittent tinnitus while the remainder reported continuous tinnitus.
Procedure
The data included in our review were scores on the Tinnitus Handicap Inventory, scores on the Hospital Anxiety and Depression Scale, age, sex and hearing thresholds of the patients and the duration of their tinnitus. Patients with missing data on any of the aforementioned variables were excluded from the analysis. This resulted in a total of 1189 records, with 139 cases of intermittent tinnitus and 1050 cases of continuous tinnitus.
Statistical analysis
A Chi-Square test was performed to test the relationship between intermittence and reported fluctuations in tinnitus loudness. This was done to confirm that patients did not interpret intermittent to mean moderate fluctuations in loudness, but instead tinnitus the alternating between absent and present.
A two-sample Kolmogorov Smirnov test (MATLAB 2017b, (The MathWorks)) was used to investigate if the outcome values on the different variables originated from the same distribution for the two groups. The Kolmogorov Smirnov test returns a “D” statistic, a decision on the null-hypothesis (i.e. h-statistic) and a p-value on which it based the decision on the null-hypothesis that the data of the two groups were from the same continuous distribution.
The variables tested were divided over two principal groups: (a) factors relevant to the perception of the sound and epidemiological factors: duration, age, and the High Pure Tone Average index for the right and left ear separately, (b) factors related to the psychological reaction: THI Total, THI Functional (THI-F), Emotional (THI-E) and Catastrophic (THI-C) subscales, and HADS Anxiety (HADS-A) and Depression (HADS-D) subscales. The Kolmogorov Smirnov test does not provide information on the direction of any potential group differences between the distributions of values on the aforementioned outcome values; therefore, a regression model was used to examine any differences more carefully.
We used binary logistic regression to investigate if having either intermittent or continuous tinnitus could be predicted based on any of the variables included in the Kolmogorov Smirnov test, along with the categorical variable of sex. Bootstrapping was performed to estimate the sampling distribution of the regression coefficients. In order to run this regression analysis, up-sampling was used to equate the uneven sample sizes. Linear interpolation was conducted to generate new samples, while maintaining the range and standard deviation from the original database.
We used the method of random forest to classify a composite dataset generated by combining the original chronic-tinnitus and the original intermittent-tinnitus datasets. “Random forest” is a classification method that builds multiple uncorrelated decision trees and corrects for over fitting of data while allowing for unbalanced groups. The more votes a particular variable receives from the individual decision trees in terms of parsing the dataset, the greater its importance (see Supplementary Digital Content for more information).
Results
Descriptive statistics
In both the intermittent and continuous group, there were slightly more male than female patients (59% and 61% respectively), but this difference did not reach significance according to a Pearson Chi-Square test of independence (χ2(1)=1.070, p = 0.3).
Perceptual and epidemiological factors
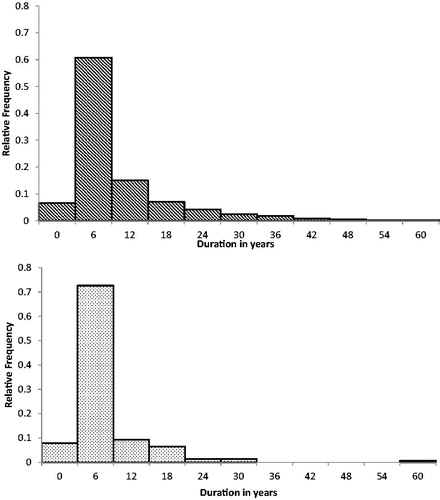
There was a statistically significant difference in the mean duration of tinnitus between the groups (p = 0.005 Independent-Samples Median Test or p < 0.001 Mann–Whitney U). Patients with intermittent tinnitus had on average a shorter duration since onset of having tinnitus than the continuous group (see ). The continuous group has greater frequency of durations over the modus of 6 years compared to the intermittent group. There was no statistically significant difference in hearing thresholds.
Figure 1. Distribution of duration for the continuous and intermittent tinnitus group.
Psychological factors
A Pairwise Mann–Whitney test showed that the intermittent tinnitus group had lower THI scores then the continuous group (p = 0.068) and lower HADS-D scores. However, HADS-A (p = 0.761) and HADS-D (p = 0.083) scores did not differ significantly. Disregarding the statistical significance, the mean difference on the HADS-D was not clinically relevant in any case, as it was only 0.43 points on a 42-point scale. For the THI subscales, a Mann-Whitney test showed that the difference between the two groups was mainly due to the THI-F (p = 0.003), with a difference of 3.2 points. There was no significant difference in mean scores on the THI-C (p = 0.133) or THI-E (p = 0.923) between the intermittent and continuous tinnitus groups; see .
Table 1. Demographics, questionnaire scores and tinnitus characteristics of patients in sample.
A Chi-Square test was performed to test the relationship between intermittence and reported fluctuations in tinnitus loudness. There was no association between intermittence and variable loudness reports, Chi-Square (1) = 2.249, p = 0.134. Seventy-one percent of patients in the continuous group reported varying loudness of their tinnitus versus 77% in the intermittent group. This makes it unlikely that intermittence was interpreted as variations in loudness, especially since the majority of patients in the continuous group reported fluctuations in loudness of their tinnitus at similar rates to those in the intermittent group.
The Kolmogorov Smirnov test indicated if the data of the two groups originated from the same population distribution. The results of the Kolmogorov Smirnov test were positive for tinnitus duration, total THI and THI-F (see ), indicating that the distributions of these factors were different for the two groups.
Table 2. Kolmogorov Smirnov test Decisions on Continuous and Intermittent Tinnitus coming from the same continuous population distribution.
To further understand the contribution of the different factors to the presence of intermittent and continuous tinnitus, we conducted a binary logistic regression analysis. The variables included in the logistic regression model were sex, age, duration, high Fletcher index scores right, high Fletcher index scores left, THI Functional scores, THI Emotional scores, THI catastrophic scores, HADS Depression scores and HADS Anxiety scores. A high Fletcher index score is the mean of the hearing thresholds at 1, 2 and 4 kHz of one participant, a clinical measure commonly used in the Netherlands. The model was statistically significant (χ2(10) = 217.295, p < 0.0001). The model explained 13.5% (Nagelkerke R2) of the variance in tinnitus type and correctly classified 63% of cases. The variables age, duration, THI subscale scores and HADS-D scores all contributed significantly to the model. Increase in age and in scores on THI-E were associated with an increased likelihood of intermittent tinnitus. Increases in duration, THI-F, and THI-C scores, and HADS-D scores were associated with a reduction in the likelihood of having intermittent tinnitus; see .
Table 3. Prediction of Intermittent vs Continuous Tinnitus based on Binary Logistic Regression.
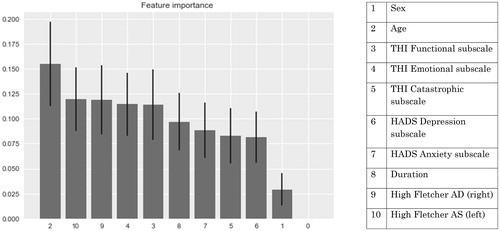
The random forest classification model was generated with the original intermittent data set (i.e. without the up-sampling). Classification accuracy and precision were 92% (see ). The model accuracy describes the proportion of correct classifications overall, i.e. the total number of correct predictions over the total number of observations. The model precision indicates the correct number of positive predictions out of the total number of positive predictions, i.e. how many intermittent predictions are correct from total number of intermittent predictions. The final model also ranked the relative importance of the variables that contributed to this classification, with age being ranked as the highest in terms of importance. The next four features were high Fletcher index scores left and right, THI-E, THI-F, and Duration; see . Except for the high Fletcher index scores, this echoed the findings from the logistic regression model.
Figure 2. Prediction accuracy of the random forest model (n = 100 trees).
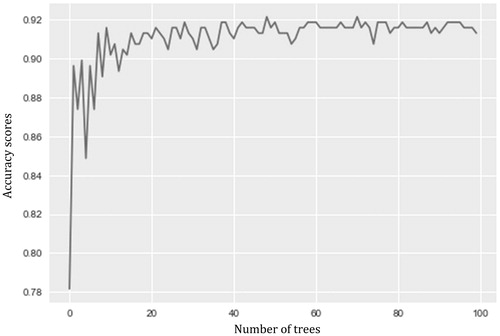
Figure 3. Feature importance for the random forest analysis.
Discussion
The main findings of our retrospective review were related to the differences in distribution and the significance of the factors affecting the intermittent and continuous tinnitus groups. The distribution of duration of tinnitus but not the hearing thresholds varied between the groups. The psychological reaction to the tinnitus differed between the groups and scores on the total THI and the THI-F differed significantly between the two groups. Increased duration, higher scores on the THI-F and THI-C and higher scores on the HADS-D were associated with a reduction in the likelihood of having intermittent tinnitus. The Random Forest model classified age, high Fletcher index, the THI-E, THI-F, and duration as the variables that differentiated best between continuous and intermittent tinnitus.
Prevalence of intermittent tinnitus
The prevalence of intermittent tinnitus in our sample was 10%. Prevalence rates of intermittent tinnitus have varied considerably in the reported literature. In a recent survey of the general population in Sao Paulo, Brazil, of those with tinnitus 68% reported intermittent tinnitus (defined as not being perceived daily), and 32% had continuous tinnitus (Oiticica and Bittar Citation2015). In the young adult age group, 85% presented with intermittent tinnitus compared to 59% in the older adult group, implying that intermittent tinnitus is more common in younger adults. In contrast, in a pilot study (Henry et al. Citation2016) the prevalence of intermittent tinnitus was 25% compared to 42% reporting continuous tinnitus, with the remaining participants not reporting tinnitus. The prevalence of intermittent tinnitus in our dataset is much lower than that of other studies. It must be noted that our dataset is based on a tertiary clinic and it might not be reflective of the general population. If intermittent tinnitus is less bothersome, for instance because it is infrequent, then a relatively small portion of people with intermittent tinnitus will approach our clinic.
Factors affecting the likelihood of intermittent tinnitus
As has been noted in the literature, hearing loss occurs with tinnitus in about 90% of cases (e.g. Hazell and Jastreboff Citation1990). In our study, hearing loss did not dissociate the two groups. Factors associated with intermittent rather than continuous tinnitus were a lower score on the THI-F, and a shorter duration of tinnitus. Based on the distribution of , duration of tinnitus mainly differentiates between the intermittent and the continuous group if the tinnitus duration is long (i.e. >6 years). A surprising finding is that there was no difference between groups in scores on the emotional subscale of the THI. It appears that having intermittent tinnitus is as emotionally disruptive as having continuous tinnitus, for those seeking care at the clinic. Scores on the different subscales of the THI had different associations with intermittent tinnitus – higher scores on the emotional subscale increased the likelihood whereas higher functional and catastrophic subscale scores decreased the likelihood. The THI total and THI-F scores were significantly lower for the intermittent group. Even though the emotional impact of intermittent tinnitus was as large as for continuous tinnitus, it did not appear to interfere with functionality as much. This might be explained by the “recovery” periods that occur for intermittent tinnitus. In intermittent tinnitus, individuals do not have to live with their tinnitus every day, but it occurs from time to time. This is in keeping with a recent study, where the tinnitus handicap scores, as measured by Tinnitus Functional Index, were significantly lower for an intermittent group than for a continuous group (Henry et al. Citation2016). Of the 100 adults included in this preliminary study of a tinnitus screener, 25% reported intermittent tinnitus, 42% reported continuous tinnitus and 33% reported no tinnitus symptoms. Henry et al. (Citation2016) did not report on scores for the various subscales of the TFI.
Of the perceptual factors, duration was the most significant; tinnitus perception may start with a fluctuating percept of tinnitus and progress to become stable and thus labelled continuous. For the psychological factors, the groups differed primarily on the THI-F score. The THI-F gives an indication of the impact the tinnitus has on daily life functioning, with the implication that intermittent tinnitus has a lower impact on daily functioning than continuous tinnitus.
It appears that fewer of those that have intermittent tinnitus seek help in a tertiary clinical setting, probably because intermittent tinnitus is generally less bothersome than continuous tinnitus. However, of those that suffer sufficiently to seek help in a tertiary clinic, it appears that the emotional burden of intermittent tinnitus is equal to that of people with continuous tinnitus. Intermittent tinnitus appears to interfere less with day to day functioning than continuous tinnitus; due to the periods of relief, when people are temporarily free from tinnitus. On the other hand, it could be argued that the presence of continuous tinnitus has a certainty to it, whereas some people find intermittent tinnitus a difficult condition to habituate to because of its irregularity. This uncertainty might increase feelings of anxiousness, depression, and worrying and feelings of frustration, as is reflected in the scores on the THI-E and the HADS-A. Taken together, the experienced burden on daily life functioning directly related to tinnitus in general might lead people to be persistent about seeking help. However, the secondary effect of the emotional burden of the tinnitus is not enough for people to seek out a tinnitus specific consultation, as reflected in the prevalence rates and data of our tertiary clinic. This warrants the modification of models of burden as applied to continuous tinnitus, where the focus is on emotional impact of tinnitus (McKenna et al. Citation2014). The distress caused by intermittent tinnitus alone is apparently not enough to motivate people to seek help. This implies that not the emotional distress but the functional impairment drives the need for medical help in tinnitus.
Possible models explaining intermittent tinnitus
There are not many studies of intermittent tinnitus and little is known about its possible mechanisms. Neurophysiological models offer several possible explanations for the occurrence of intermittent tinnitus, one of which focuses on a gating mechanism at the thalamic level allowing the tinnitus signal to reach the cortex and become a percept, and another one focuses on the conscious awareness of the percept.
Rauschecker et al. (Citation2010) alluded to this subject in their paper on limbic-auditory interactions in tinnitus. They proposed that in the event of a cochlear lesion, due to noise exposure or ageing, plastic reorganisation occurs. This reorganisation is involved in the generation of hyperactivity in the ascending auditory pathways. In a normal functioning limbic system, the hyperactivity is identified and a noise cancellation mechanism is employed to cancel it out. This cancelling out is hypothesised to occur by subtraction of the hyperactivity (i.e. the tinnitus signal) from the afferent signal via feedback to the inhibitory thalamic reticular nucleus. In an earlier paper, Jastreboff (Citation2000) had theorised that the deviating activity in the limbic system of tinnitus patients reflects the emotional reaction to tinnitus and is an indicator of the consequences of having tinnitus. In contrast, Rauschecker et al. argued that the role of the limbic system in tinnitus is an active one opposed to a reactive one. In their proposed circuit, the limbic and para-limbic structures around subcallosal areas act as a self-regulating gating mechanism that prevents the tinnitus signal from reaching the cortex. When a break-down of this gating system occurs, the tinnitus signal is perceived. Chronic tinnitus is explained by the constant depletion of serotonin, which causes excitotoxicity due to the constant firing of serotonergic neurons that have to signal that the tinnitus sound needs to be filtered out (Rauschecker, Leaver, and Mühlau Citation2010). Intermittent tinnitus can then be explained by hypothesising that serotonin levels fluctuate rather than being depleted.
Another explanation regarding the origin of intermittent tinnitus is that the percept only sometimes rises to the level of consciousness. Cognitive neuroscience literature has implicated global changes in connectivity of several brain regions, including sensory cortices, association cortices, and a posterior parietal hub, as sub-serving the conscious awareness of external stimuli, including sounds (Dehaene et al. Citation2014; Godwin, Barry, and Marois Citation2015). Extending this to the internally generated tinnitus sound, several candidate brain regions and networks may be involved. According to Vanneste and De Ridder (Citation2012), these candidate regions, including the auditory cortex (which may be necessary but not a sufficient conduit) and the supplementary motor area, are implicated in conscious perception of tinnitus. A possible mechanism is due to the binding of events into a single percept via synchronised gamma band activity (e.g. Joliot, Ribary, and Llinás Citation1994; Llinas et al. Citation1998), which becomes a conscious percept only when the salience or self-awareness network is simultaneously activated (De Ridder et al. Citation2011). Resting state functional connectivity studies of tinnitus have implicated the role of the default mode network and its nodes, principally the posterior cingulate and the precuneus as the other major players in conscious awareness of tinnitus (De Ridder et al. Citation2014; Husain, Carpenter-Thompson, and Schmidt Citation2014; Lanting et al. Citation2016). The default mode network is a network measurable with fMRI that is most active during rest and is deactivated during task-oriented behaviour (Raichle et al. Citation2001).
Because the current data are not cross-sectional, it is difficult to make any predictions on the evolution of intermittent tinnitus. Interesting is that whereas longer duration of tinnitus was classified as a factor that increased the likelihood of continuous tinnitus, increasing age was classified as a factor increasing the likelihood of intermittent tinnitus. Intermittent tinnitus appears to be related to a shorter duration of tinnitus, regardless of the age at which the tinnitus occurs. It could be that the difference in duration between intermittent and continuous tinnitus implies that tinnitus sometimes progresses from intermittent to continuous tinnitus. If this is the case, it has implications for treatment. On the one hand it will be important to intervene when the tinnitus is still perceived intermittently, systems might not have reorganised and the pathways have not yet reshaped into a dysfunctional state. On the other hand, as continuous tinnitus cannot yet be abolished, converting it to intermittent tinnitus may be something to strive for since this might increase the functionality of patients. Some neuromodulation techniques appear promising in this respect, as temporary decreases in the tinnitus percept and suffering are reported (Peter and Kleinjung Citation2019).
Caveats
It is largely unknown how the patients in the different studies referred to in this article defined “intermittent” tinnitus. One possible definition of intermittent tinnitus is that the tinnitus ceases to be perceived for hours or days at a time. Another definition is that the tinnitus loudness fluctuates while the internal sound is always perceived. This classification problem might be the cause of the large variation in prevalence reports and the difficulty in understanding the subgroups of tinnitus. In our study we did not find an association between self-reported fluctuations of the tinnitus loudness and self-reported classification of intermittent tinnitus. We therefore conclude that, in our dataset at least, intermittence is interpreted as fluctuating periods of presence and absence of the tinnitus percept. However, there is little information available on the classification of intermittence in the literature. Thus, a follow-up study may be helpful where patients are asked to rate not only the occurrence of the tinnitus itself but also the associated states, e.g. stress-levels, wakefulness and mood, to better understand the difference between intermittent and continuous tinnitus. With modern techniques available to us, such as mobile phone applications, we can now better investigate how individuals determine that they have continuous or intermittent tinnitus. As a follow-up step, neuroimaging techniques such as MRI scanners can help us identify what neurophysiological differences underlie this distinction.
Conclusions
Continuous tinnitus was more prevalent than intermittent tinnitus (90% versus 10%, respectively) for people attending at a tertiary tinnitus clinic. Those with intermittent tinnitus had shorter durations of tinnitus and lower tinnitus-related handicap scores, suggesting that continuous tinnitus leads to a more severe psychological reaction. Sex and hearing loss did not affect the likelihood of having continuous versus intermittent tinnitus. Although our analysis did not include longitudinal data, taking into account the variable of duration, the results can be interpreted as reflecting that some cases of tinnitus may begin as intermittent and progress into continuous after several years, regardless of the age of onset. Models of chronic tinnitus and those that seek to explain changes in tinnitus over time should take this finding into account. Intervention studies can also leverage the initial intermittent aspect, when present, of chronic tinnitus for better success of treatment.
Acknowledgments
The authors would like to thank Cris Lanting for his help in setting up the code for the random forest analysis. We would also like to thank Rosemarie Arnold for setting up and maintaining the database from which the data were drawn.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- De Ridder, D., A. B. Elgoyhen, R. Romo, and B. Langguth. 2011. “Phantom Percepts: Tinnitus and Pain as Persisting Aversive Memory Networks.” Proceedings of the National Academy of Sciences 108 (20): 8075–8080. doi:10.1073/pnas.1018466108.
- De Ridder, D., S. Vanneste, N. Weisz, A. Londero, W. Schlee, A. B. Elgoyhen, and B. Langguth. 2014. “An Integrative Model of Auditory Phantom Perception: Tinnitus as a Unified Percept of Interacting Separable Subnetworks.” Neuroscience and Biobehavioral Reviews 44: 16–32. doi:10.1016/j.neubiorev.2013.03.021.
- Dehaene, S., L. Charles, J. R. King, and S. Marti. 2014. “Toward a Computational Theory of Conscious Processing.” Current Opinion in Neurobiology 25: 76–84. doi:10.1016/j.conb.2013.12.005.
- Erlandsson, S. I., and L. R.-M. Hallberg. 2000. “Prediction of Quality of Life in Patients with Tinnitus.” British Journal of Audiology 34 (1): 11–19. doi:10.3109/03005364000000114.
- Godwin, D., R. L. Barry, and R. Marois. 2015. “Breakdown of the Brain’s Functional Network Modularity with Awareness.” Proceedings of the National Academy of Sciences 112 (12): 201414466. doi:10.1073/pnas.1414466112.
- Hazell, J. W., and P. J. Jastreboff. 1990. “Tinnitus. I: Auditory Mechanisms: A Model for Tinnitus and Hearing Impairment.” The Journal of Otolaryngology 19 (1): 1–5. http://www.ncbi.nlm.nih.gov/pubmed/2179573
- Henry, J. A., S. Griest, D. Austin, W. Helt, J. Gordon, E. Thielman, S. M. Theodoroff, et al. 2016. “Tinnitus Screener: Results from the First 100 Participants in an Epidemiology Study.” American Journal of Audiology 25 (2): 153–160. doi:10.1044/2016_AJA-15-0076.
- Humphriss, R., A. J. Hall, and D. M. Baguley. 2016. “Prevalence and Characteristics of Spontaneous Tinnitus in 11-Year-Old Children.” International Journal of Audiology 55 (3): 142–148. doi:10.3109/14992027.2015.1120890.
- Husain, F. T., J. R. Carpenter-Thompson, and S. A. Schmidt. 2014. “The Effect of Mild-to-Moderate Hearing Loss on Auditory and Emotion Processing Networks.” Frontiers in Systems Neuroscience 8: 1–13. doi:10.3389/fnsys.2014.00010.
- Jastreboff, P. J. 2000. Tinnitus habituation therapy (THT) and tinnitus retraining therapy (TRT). In Tinnitus Handbook, 357–376. San Diego: Singular Publishing Group.
- Joliot, M., U. Ribary, and R. Llinás. 1994. “Human Oscillatory Brain Activity near 40 Hz Coexists with Cognitive Temporal Binding.” Proceedings of the National Academy of Sciences of the United States of America 91 (24): 11748–11751. doi:10.1073/pnas.91.24.11748.
- Lanting, C., A. Woźniak, P. van Dijk, and D. R. M. Langers. 2016. “Tinnitus- and task-related differences in resting-state networks.” In Advances in Experimental Medicine and Biology. 894: 175–187. doi:10.1007/978-3-319-25474-6_19.
- Llinas, R., U. Ribary, D. Contreras, and C. Pedroarena. 1998. “The Neuronal Basis for Consciousness.” Philosophical Transactions of the Royal Society B: Biological Sciences 353 (1377): 1841–1849. doi:10.1098/rstb.1998.0336.
- Maes, I. H. L., R. F. F. Cima, J. W. Vlaeyen, L. J. C. Anteunis, and M. A. Joore. 2013. “Tinnitus: A Cost Study.” Ear and Hearing 34 (4): 508–514. doi:10.1097/AUD.0b013e31827d113a.
- McKenna, L., L. Handscomb, D. J. Hoare, and D. A. Hall. 2014. “A Scientific Cognitive-Behavioral Model of Tinnitus: Novel Conceptualizations of Tinnitus Distress.” Frontiers in Neurology 5: 196. doi:10.3389/fneur.2014.00196.
- Oiticica, J., and R. S. M. Bittar. 2015. “Tinnitus Prevalence in the City of São Paulo.” Brazilian Journal of Otorhinolaryngology 81 (2): 167–176. doi:10.1016/j.bjorl.2014.12.004.
- Peter, N., and T. Kleinjung. 2019. “Neuromodulation for Tinnitus Treatment: An Overview of Invasive and Non-Invasive Techniques.” Journal of Zhejiang University-SCIENCE B 20 (2): 116–130. doi:10.1631/jzus.B1700117.
- Raichle, M. E., A. M. MacLeod, A. Z. Snyder, W. J. Powers, D. A. Gusnard, and G. L. Shulman. 2001. “A Default Mode of Brain Function.” Proceedings of the National Academy of Sciences of the United States of America 98 (2): 676–682. doi:10.1073/pnas.98.2.676.
- Rauschecker, J. P., A. M. Leaver, and M. Mühlau. 2010. “Tuning out the Noise: limbic-Auditory Interactions in Tinnitus.” Neuron 66 (6): 819–826. doi:10.1016/j.neuron.2010.04.032.
- Shore, S. E., L. E. Roberts, and B. Langguth. 2016. “Maladaptive Plasticity in Tinnitus — Triggers, Mechanisms and Treatment.” Nature Reviews Neurology 12 (3): 150–160. doi:10.1038/nrneurol.2016.12.
- Sogebi, O. A. 2013. “Characterization of Tinnitus in Nigeria.” Auris Nasus Larynx 40 (4): 356–360. doi:10.1016/j.anl.2012.11.003.
- Tan, C. M., W. Lecluyse, D. McFerran, and R. Meddis. 2013. “Tinnitus and Patterns of Hearing Loss.” Journal of the Association for Research in Otolaryngology 14 (2): 275–282. doi:10.1007/s10162-013-0371-6.
- The MathWorks. 2017. MATLAB and Statistics Toolbox Release 2014b. Natick, Massachusetts, United States: The MathWorks, Inc. Retrieved from https://uk.mathworks.com/
- Vanneste, S., and D. De Ridder. 2012. “The Auditory and Non-Auditory Brain Areas Involved in Tinnitus. An Emergent Property of Multiple Parallel Overlapping Subnetworks.” Frontiers in Systems Neuroscience 6: 1–9. doi:10.3389/fnsys.2012.00031.