
Abstract
Objective
The purpose of this fit-testing study in the field was to systematically compare three Hearing Protection Device (HPD) fit-training methods and determine whether they differ in the acquisition of HPD fitting skill and resulting amount of earplug attenuation.
Design
Subjects were randomly assigned to receive HPD fit-training using one of three training methods: current, experiential HPD (eHPD), and integrated. Personal Attenuation Ratings (PARs) were acquired via HPD fit-testing and used to verify attenuations pre- and post-training.
Study Sample
US Marine training recruits (n = 341) identified via HPD fit-testing for remedial HPD fit-training and assigned to three cohorts.
Results
The post-training HPD fit-test passing rate differed by training method, with pass rates ranging from 50% (current) to nearly 92% (eHPD). The difference between group delta PAR values were significantly higher (>9 dB) in both the eHPD and integrated methods compared to the current method.
Conclusion
The HPD fit-training methods that teach “what right feels like” (eHPD and integrated) provided a greater number of trainees with the skill to achieve noise attenuation values required for impulse noise exposures encountered during basic training. The attenuation achieved by those methods was significantly greater than the current training method.
Introduction
Noise induced hearing injury (NIHI, i.e. hearing loss, tinnitus) is a work place injury that affects numerous Service Members (SMs) across all branches of service. During a sampled three year period, over 85,000 medical encounters for NIHI were documented among the US military population (Helfer et al. Citation2010). The increased risk of hearing loss among military SMs has been well documented throughout the literature (Abel Citation2008; Ahroon, Hill and Goodes Citation2011; Karch et al. Citation2016; Wells et al. Citation2015; Yong and Wang Citation2015). Although NIHIs are preventable, the U.S. Department of Veterans Affairs reported NIHIs hearing loss and tinnitus as the top two service-connected disabilities in Fiscal Year 2018 (Veterans Benefits Administration Citation2019).
The issuance of hearing protection devices (HPDs) is a common way to reduce the risk of NIHI at the individual level. In the U.S. military, in-ear HPDs (i.e. earplugs) are one of the most widely used hearing protector types. In fact, the amount of attenuation achieved by the user has been reported to be influenced by the properties of the HPD in addition to the skill of the user to fit the issued earplug (Tikka et al. Citation2017). Therefore fitting (to ensure proper size) and training the individual user are essential to ensure the SM is effectively protected from noise-induced hearing loss.
Ample evidence indicates that when properly fitted, earplugs are effective at attenuating noise (Federman and Duhon Citation2016; Pääkkönen et al. Citation2000). The amount of earplug attenuation (in dB) achieved by users in the real world has been reported to be associated with insertion depth, earplug shape and material, the anatomical characteristic of the ear/head, and fitting techniques (Berger Citation2013; Joseph et al. Citation2007; Murphy et al. Citation2011; Samelli et al. Citation2018; Tufts, Chen and Marshall Citation2013). For example, Tufts et al. (Citation2013) found that, the deeper a custom earplug is inserted, the greater the amount of achieved attenuation by the user. Similarly, Berger (Citation2013) reported that the amount of attenuation a foam earplug affords its user is influenced by both the depth of its insertion and its physical shape (e.g. tapered, cylindrical). Samelli et al. (Citation2018) reported higher PAR values when foam earplugs were used compared to that of pre-molded earplugs. In addition, Berger (Citation1996a) reported that less than 10% of employees likely have ear canals that vary in size, and to achieve proper fit, these persons would likely require use of two different sized earplugs.
Previous studies of military training recruits have reported a portion of the sampled population was unable to achieve the target attenuation with the issued standard earplug and required an alternate HPD (Federman and Duhon Citation2016; Pääkkönen et al. Citation2000). Specifically, utilising a field attenuation estimation system (FAES) to verify physical fit, i.e. by measuring the amount of attenuation) Federman and Duhon (Citation2016) found that, among a cohort of 320 USMC training recruits, 15% failed to achieve the minimum target attenuation when using a standard issued, one-size-fit-all foam earplug when fit by an expert. Once an alternate sized earplug was provided, all users were able to achieve at least the minimum target PAR value set at 25 dB. Pääkkönen et al. (Citation2000) reported among a sample of 95 military conscripts, approximately 9% were unable to achieve an attenuation that might reduce their risk for acquiring hearing loss. Considering the reported ear canal sizes range in diameter from 7 to 11 mm in the studied cohort, proper earplug sizing remains a factor impacting proper fit of an earplug even for one-size-fits-all options.
While proper HPD use may not be intuitive to users, training and instruction on proper fit and use in both individual and small group settings can positively influence both the amount of attenuation achieved and the amount of time the device is used (Joseph et al. Citation2007; Liu and Yang Citation2018; Murphy et al. Citation2011; Salmani Nodoushan et al. Citation2014; Toivonen et al. Citation2002; Tsukada and Sakakibara Citation2008; Williams Citation2004). HPD fit training can be delivered using photographic, infographic, written, video or multimedia technology either in group or one-on-one settings. Instruction techniques can also include a physical demonstration of proper fit with the instructor either fitting the HPD on themselves or on the user.
Previous research indicates that without training on the proper insertion techniques for the issued HPD, a user is likely to have difficulty obtaining the device’s advertised noise reduction rating (NRR) (Murphy et al. Citation2011). Joseph et al. (Citation2007) reported finding a statistically significant difference in the skill to don an earplug after training (both one-on-one and small group) was provided. When comparing instruction methods for proper insertion techniques delivered to inexperienced users, one-on-one verbal instructions provided by an expert resulted in greater achieved attenuation (up to 16 dB) than with manufacturer written/infographic instructions alone (Williams Citation2004). Gong et al. (Citation2019) reported that among noise-exposed workers, one-on-one instruction resulted in a difference (post-training minus pre-training PAR values) of 14 dB, which was stated to be statistically significant (p < 0.05). Toivonen et al. (Citation2002) reported that use of a 30-min group lecture with a supervised practice session (including one-on-one instruction if needed) achieved mean attenuation roughly 6–10 dB higher than a control group who did not receive training before HPD fit-testing. Similarly, Murphy et al. (Citation2011) reported that individualised expert instruction resulted in a greater amount of attenuation achieved by the user than either written manufacturer instruction or instructional video. Furthermore, Federman and Duhon (Citation2016) found a significant increase in mean attenuation among military training recruits after they received a short one-on-one fit-training during which an expert explained the fitting-process step-by-step while the recruit was fit with the HPD. This increase in attenuation from baseline was observed when the training recruit then self-fit the HPD immediately following the training session.
To assess the attenuation achieved by an HPD (and to determine the effectiveness of fit-training), an HPD user is fit-tested. Individual HPD fit-testing has been identified by the OSHA-NHCA-NIOSH Alliance and the US Department of Defense (DoD) as a “best practice” in hearing conservation programmes (OSHA Citation2008; U.S. Department of Defense Citation2019). HPD fit-testing is a method to measure earplug attenuation either subjectively or objectively depending on the test system. Use of test systems that are designed as a subjective psychoacoustic measure, user response and identified threshold can vary based on the listener’s state of arousal, background noise and masking effects from physiologic noise (Nélisse et al. Citation2015; Samelli et al. Citation2015). One method of fit-testing that is widely used to measure HPD attenuation in individuals is field-attenuation estimation system (FAES). FAES testing provides a single quantitative value called the personal attenuation rating (PAR). PAR reflects both the inherent attenuation properties of the HPD as well as the real-time user’s fit of that HPD. The PAR is the amount of attenuation attained by an HPD user and calculated by the FAES (Voix and Hager Citation2009).
When implemented in a HCP, HPD fit-testing can serve as a teaching tool, training and instruction aid, or verification measure. As a teaching tool, fit-testing can facilitate conversations concerning HPD attenuation, PAR values and their meaning, and proper fitting techniques (Smith, Monaco and Lusk Citation2014). Marshall et al. (Citation2016) recommended individual fit-testing in order to verify how well each and every dispensed earplug protects the user. Since achieved attenuation is influenced in part by the physical fit of the earplug in the ear, Hager (Citation2011) recommended the use of fit-testing to select the HPD. Federman and Duhon (Citation2016) provided proof-of-concept that fit-testing can be successfully used on a large scale (n = 320 USMC training recruits) as a verification tool after HCP training to quantifiably measure the amount of attenuation achieved by individuals after they have either fit themselves or been fit by an expert.
Visual inspection of the insertion of an earplug has been reported to be the “least accurate method” to assess the quality of HPD fit. This was reported first by Berger (Citation1996b), and most recently by the Council for Accreditation in Occupational Hearing Conservation (Suter Citation2007). Supporting evidence is lacking in the literature for the assumption that a visual inspection of HPD fit is a reliable indicator for attenuation achieved. Without verification of HPD attenuation, there is no method to determine that the issued HPD is adequately protecting individual recruits or SMs from hazardous noises commonly experienced in military training and combat environments.
The goal of this study was to systematically compare three HPD fit-training methods (current, eHPD, and integrated). Specifically, this study was designed to investigate whether these three HPD fit-training methods alter USMC training recruits’ ability to adequately fit a foam earplug designed for use during basic training. Moreover, it was of interest to determine which fit-training method resulted in the largest skill improvement if a significant difference was observed.
Methods
This study was reviewed by the Naval Submarine Medical Research Laboratory Institutional Review Board and was determined not to be human subject research. Instead, the study was determined to be a study investigating military programme improvement.
Participants
In order to obtain approximately 100 participants in each of the three HPD fit-training cohorts, a total of 821 U.S. Marine Corps (USMC) training recruits located at the USMC Marine Corps Recruit Depot (MCRD), Parris Island completed a “baseline” fit-test. Only those who failed the test were included in subsequent training method cohorts. Prior to the study, all recruits had received a standard hearing conservation programme (HCP) orientation in accordance with DoD Instruction 6055.12 (2010) and Marine Corps Order 6260.3 A (Commandant of the Marine Corps, Citation2016) as part of their basic training. The amount of time between the HCP orientation and the “baseline” initial self-fit (ISF) fit-test varied by participant, while the studied training methods (current, eHPD, integrated) occurred the same day as “baseline” ISF testing. Prior to study inclusion, any recruit identified via otoscopy as requiring cerumen removal received an ear lavage in accordance with standard procedures at MCRD, Parris Island.
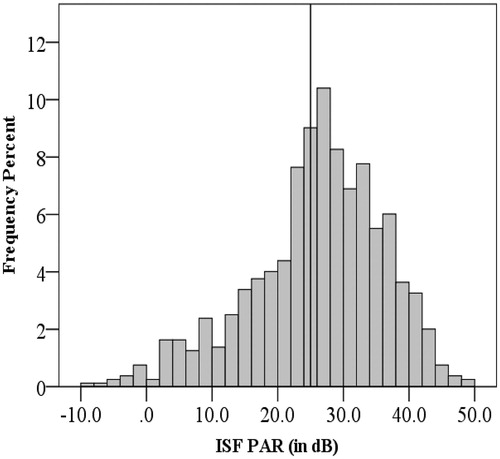
The range and frequency (in percent) of baseline (ISF) PAR values (in dB) for all participants (n = 798) who completed either the training (n = 321) or whose ISF exceeded the 25.0 dB PAR (n = 477) are shown in . The solid vertical line indicates the study pass-fail criterion level of 25.0 dB. Those participants who were able to achieve at least the minimum target attenuation at their baseline fit-test using the issued foam earplug were excluded from further participation and excused from any additional training (n = 477).
Figure 1. Histogram showing initial self-fit (ISF) personal attenuation ratings (PARs) in decibels (dB) achieved (i.e. baseline) for all recruits by percent (n = 798). Note: Not included here are the ISF PAR values of the 23 participants who were excluded. The solid vertical line indicates the study pass-fail criterion level of 25.0 dB.
As shown in , those training recruits who failed to achieve the minimum target PAR of 25.0 dB (n = 344) were randomly assigned to one of three training formats: current (n = 113), experiential HPD (eHPD) fit-training (n = 114), and an integrated training approach (n = 114). Three qualified training recruits whose ISF PAR values were less than 25.0 dB were not assigned a training cohort, and therefore were subsequently excluded prior to data collection. The data from a total of 20 recruits were excluded from analyses after completing the study assigned training. Reasons for exclusion were: fit-testing was completed with an alternate earplug (n = 11), could not be successfully expert fit (EF) with the issued foam earplug (i.e. PAR ≥ 25.0 dB) during either the eHPD (n = 4) or integrated fit-training (n = 3) methods, and did not complete training therefore resulting in incomplete data sets (n = 2).
Figure 2. Study design flow chart. Note. Of the 344 participants who qualified, 341 were randomly assigned a training method. A total of 20 participants were excluded during training for various reasons (e.g., use of an alternate earplug [current n = 2, eHPD n = 5, integrated n = 4], an expert fit PAR value < 25.0 dB [eHPD n = 4, integrated n = 3), and not completing the assigned training [integrated n = 2], which resulted in a data set of 321 participants (i.e., current n = 111, eHPD n = 105, integrated n = 105).
![Figure 2. Study design flow chart. Note. Of the 344 participants who qualified, 341 were randomly assigned a training method. A total of 20 participants were excluded during training for various reasons (e.g., use of an alternate earplug [current n = 2, eHPD n = 5, integrated n = 4], an expert fit PAR value < 25.0 dB [eHPD n = 4, integrated n = 3), and not completing the assigned training [integrated n = 2], which resulted in a data set of 321 participants (i.e., current n = 111, eHPD n = 105, integrated n = 105).](/cms/asset/a268437f-50b3-42d3-8cea-ae2f19519064/iija_a_1811407_f0002_b.jpg)
Equipment
All participants completed testing using the same tapered foam earplug (Moldex Camo Plugs®), a one-size-fits-all disposable with a manufacturer reported NRR of 33 dB. Each participant was provided with a new set of foam earplugs for each fit-test (i.e. initial self-fit (ISF), expert fit (EF), and self-re-fit (SRF)). The FAES used for data collection was a commercially available software-based HPD fit-test system (FitCheck Solo™, Michael & Associates, Inc., State College, PA). The fit-test system used in this study is capable of measuring 125–8000 Hz binaurally or ear specific, and is an adaptation of the laboratory-based Real Ear Attenuation at Threshold (REAT) test (American National Standards Institute, Citation2018). The video training materials used in both the current and integrated methods were from the Military Hearing Preservation (MHP) Toolkit (Sensimetrics Corporation, Gloucester, MA). Statistical analyses were completed using a commercially available statistical software package (IBM SPSS Statistics, Version 23).
Procedures
All participants completed an initial “baseline” (ISF) three-frequency (500, 1000, and 2000 Hz) fit-test with the project issued foam earplug (as shown in ). To account for order effect in obtaining the ISF PAR values, occluded and unoccluded threshold testing was counterbalanced. Determination of order was based on random assignment. Only those persons who donned the issued foam earplug and achieved a PAR of less than 25.0 dB were randomly assigned (n = 341) to one of the three training formats (current n = 114, eHPD n = 113, or integrated n = 113). To measure the immediate effect of training, a post-training fit-test was completed directly after training was concluded.
To determine each participant’s PAR value, and in accordance with Federman and Duhon’s (Citation2016) recommendation for fit-test paradigms, a three-frequency (500, 1000, and 2000 Hz) binaural test protocol was utilised for all fit-tests. The differences between unoccluded (i.e. without earplugs) and occluded (i.e. with earplugs) threshold values are automatically calculated by the FAES, which then outputs an overall PAR value (Hager Citation2011). For further information regarding the mathematical calculation of PAR values, the interested reader is encouraged to review the ANSI standard (Citation2018) that details FAES and PAR (i.e. ANSI S12.71 − 2018 “Performance Criteria for Systems that Estimate the Attenuation of Passive Hearing Protectors for Individual Users”).
Per U.S. Department of Defense (Citation2015) Military Standard 1474E (2015), “… peak-pressure levels of impulsive noises shall be less than 140 dBP, at the ear (protected or unprotected), at all personnel locations during normal operations (8).” The M4 carbine rifle, which is used during basic training, is the most commonly issued small carbine rifle weapon system utilised by the U.S. Military (Gaston and Letowski Citation2012; U.S. Army Public Health Command Citation2014). When measured 15 centimetres from the shooter’s ear, the M4 emits an average peak sound pressure level (SPL) of approximately 165 dBP when standing and fired without use of a suppressor (U.S. Army Public Health Command Citation2013). Therefore, all SMs and training recruits who fire this weapon should achieve a minimum PAR of at least 25.0 dB with their issued HPD in order to reduce their impulse noise exposure level to less than or equal to 140 dBP, as required by MILSTD 1474E. To reduce a subject’s exposure to below 140 dBP, and to be in accordance with the study completed by Federman and Duhon (Citation2016), the target minimum PAR of the current study was set at 25.0 dB.
Training methods
The current training method was a 30-min proctored session that utilised military focussed hearing conservation video training modules from the MHP Toolkit, and was intended to represent the standard hearing conservation training given in DoD occupational settings. Those participants assigned to this group watched the video modules in small groups of up to six persons. Upon completion of the current training, participants refit their issued HPD (i.e. Self-Re-Fit [SRF]) and completed a post-training fit-test.
The MHP video modules selected for use were independently chosen by a group of subject matter experts, comprised of senior audiologists from the DoD and Hearing Centre of Excellence. The chosen video modules were determined to be representative of what is required by DoD Instruction 6055.12 (U.S. Department of Defense Citation2010). Specifically, annual hearing conservation training must cover: the effect of noise on hearing, the purpose of HPDs (including how to report concerns on HPD fit and use), the different types of HPDs (including advantages and disadvantages to each), how to select, fit, use, and care for their HPD, overview of regulations and mandates that require the use of HPDs (including administrative actions for failure to use), the purpose of audiometric testing, what one can expect during an audiometric test, how hearing loss impacts quality of life (on and off the job), and the importance of using HPDs when exposed to hazardous noises. The MHP toolkit allows users to select informational multimedia videos that cover general information, how to use and don HPDs, in addition to disproving common myths regarding hearing, hearing loss, and/or HPDs (Watts, Welles and Zurek Citation2018). In order to simulate the typical standard hearing conservation programme (HCP) orientation, the video modules used in the studied training methods included approximately 5 min of time dedicated specifically to fit-training.
The experiential HPD (eHPD) fit-training technique provided an expert fit (EF) of the issued earplug immediately followed with a fit-test to measure the HPD attenuation achieved by the expert. The EF is a brief (approximately 30 s) one-on-one training session where the expert describes and demonstrates the proper roll-down and insertion technique of the issued earplug that includes the expert inserting the earplug into the end-user’s ears.
Participants who achieved an EF PAR greater than or equal to 25.0 dB were instructed to remove the earplug and to then replicate the fitting they just experienced by refitting the earplug themselves. We have named this the Self Re-Fit, or SRF. A final fit-test was then completed to document the PAR achieved. In the cases where the EF PAR was less than 25.0 dB, the assumption was made that the issued earplug could not be successfully fit for that participant, and an alternative HPD was required. Once an alternate HPD was selected and fit by the expert, the amount of attenuation was then verified with another fit-test. The PARs obtained from these participants were excluded from data analyses.
The third training format studied was an integrated approach that utilised both the eHPD fit-training technique and current video instruction. This approach was approximately 35 min in duration. To account for order effect, approximately half of the integrated training cohort watched the current training video in a small group first then completed the eHPD fit-training. The other half of participants completed the eHPD fit-training first, then viewed the current training video in small groups.
The pass-fail rate for PAR values acquired immediately post-training (SRF) were calculated for each training format investigated. Post-training pass rates were compared using a chi-square analysis to determine whether there was a relationship between fit-training method and fit-test pass rate. The difference in attenuation achieved (i.e. delta PAR) was calculated for each participant (n = 321) by subtracting the participants’ pre-training (ISF) PAR value from their post-training (SRF) PAR value. Delta PAR was compared between fit-training formats using one-way analysis of variance (ANOVA). Post-hoc tests were completed as appropriate. Statistical analyses were conducted using commercially available software (IBM SPSS Statistics, Version 23). The alpha level of 0.05 was used to determine statistical significance.
Results
Of the 821 training recruits who completed the initial self-fit (ISF) fit-test, 344 (or 42%) failed to achieve the minimum target PAR value (i.e. 25.0 dB). As shown in and , of these 344 participants, 341 were randomly assigned to one of three studied HPD fit-training methods (current, eHPD, and integrated). Immediately after completing the assigned fit-training, participants completed a post-training (SRF) fit-test. Data from 20 participants were excluded from further analyses, as described in the Methods section, resulting in a total sample size of 321 participants (current n = 111, eHPD n = 105, integrated n = 105).
Table 1. Pass/fail rate by training method pre- and post-training.
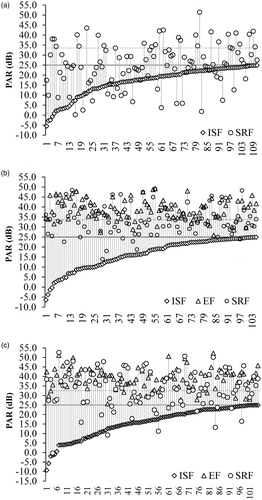
The chi-square analysis revealed a significant association between the fit-training method and post-training (SRF) pass rates (X2 (2) = 57.06, p < 0.001). As shown in , the measured pass rate (≥25.0 dB PAR) for the remaining 321 participants by training method was: 50% (56 of 111) for the current, 92% (97 of 105) for the eHPD, and 84% (88 of 105) for the integrated fit-training formats. Conversely, 80 of the 321 (or 25%) recruits who completed the study were unable to achieve a post-training (SRF) PAR value greater than 25.0 dB. By training format, that was: current = 55, eHPD = 8, and integrated = 17. All participants whose post-training PAR was below the target minimum were re-instructed utilising the EHPD fit-training method, were allowed to refit the current issued earplug and complete an additional fit-test, were issued an alternative earplug, and/or were recommended to use earmuffs when no in-ear product could be successfully fitted. Recorded PARs (ISF, EF when applicable, and SRF) by participant for each training format is shown in . shows the individual PAR values for the current fit-training format, A3(B) shows the eHPD fit-training, and 3(C) shows the integrated fit-training approach. The results are rank ordered by the ISF PAR value, with each vertical column representing the results from a single participant. The solid horizontal line shows the target attenuation of 25.0 dB, and the horizontal dashed line indicates the earplug’s NRR (33 dB).
Figure 3. Attenuation achieved by participant rank ordered by ISF PAR values. Three figures are provided one for each training format: (A) current (n = 111), (B) eHPD (n = 105), and (C) integrated (n = 105). Note. PAR values obtained for ISF (diamonds), EF (triangles), SRF (circles), target PAR (horizontal dark solid line, 25.0 dB), and earplug NRR (horizontal dashed line, 33.0 dB) are shown. Each vertical line connects the PAR values for an individual participant.
The difference between same day pre- and post-training PAR values, or delta PAR, was calculated for each participant. The lowest calculated difference was −20.4 and the highest was 48.7 dB. Descriptive statistics for all three training formats is reported in . A one-way ANOVA showed a significant difference for delta PAR among the three fit-training methods (F2 = 23.341, p < 0.001, ƞ2p = 0.13). A Bonferroni post-hoc analysis revealed that the delta PAR calculated after completing the current fit-training method was significantly lower than both the eHPD and integrated fit-training methods (p < 0.001). As shown in , the mean delta PAR for the current training format was 9.3 dB less than the eHPD delta PAR and 9.4 dB less than the integrated fit-training method. The difference between the eHPD and integrated fit-training methods (0.1 dB) was not found to be statistically significant (p = 1.0).
Table 2. Means and standard deviations of measured PAR values and Delta PAR.
Discussion
Baseline fit-testing (ISF) was used to measure over 800 training recruits’ ability to fit the standard issued foam earplug after receiving the current military HPD fit-training orientation provided during the first week of basic training. Of the 821 recruits tested, 477 (58%) were able to achieve or exceed the minimum target PAR value of 25.0 dB. Since this study was designed to investigate the immediate effect of training for those persons who otherwise would be at risk in a noise hazard environment (like that of a firing range), the recruits who could achieve adequate attenuation were excused and not provided remedial training. A future line of inquiry would be to investigate the short-term effect of these training formats among persons who demonstrate competence over time to see if remedial training improves or helps maintain achieved skill.
Only those who were unable to achieve the target PAR of ≥ 25.0 dB were randomly assigned to one of three fit-training formats. Specifically, of the 821 training recruits tested, 344 (42%) failed to achieve the minimum target attenuation of 25.0 dB with the issued foam earplug. This fail rate was larger than that observed by Federman and Duhon (Citation2016). However, by excluding those participants (n = 23) who were not assigned to a training method, did not complete a training paradigm, or who were tested with an alternate earplug, the overall number of training recruits included in the study’s final analyses reduced to 321. This reduced the fail rate to 39%, which is similar to the Federman and Duhon (Citation2016) reported 35% fail rate among USMC training recruits approximately two-weeks after initial HPD fit-training was provided. Similarly, in studies of non-military industrial workers such as oil-rig inspectors, the fail rate of employees who were unable to achieve the minimum target attenuation of 25.0 dB at baseline was roughly 40% (Murphy, Themann and Murata Citation2016).
Although the low ISF PAR values were likely the result of inadequate personal fitting techniques in most cases, this study revealed that approximately 5% of qualified participants who were randomly assigned to one of the three training methods (18 of 341), the influencing factor for poor fit was the size of the issued foam earplug (Moldex Camo Plugs®). Similarly, 6% of the total population of recruits (46 of 821) tested in this study were found to require an alternate HPD (other earplug, n = 42; earmuffs, n = 4) either by fit-test or expert opinion. This finding falls within the 4 to 14% reported range from other studies of military recruits and conscripts who were unable achieve an adequate fit with a commonly issued earplug (Federman and Duhon Citation2016; Pääkkönen et al. Citation2000; Toivonen et al. Citation2002). Results from those studies suggest that more than 90% of training recruits with proper fit-training are able to achieve an adequate fit and attenuation with the standard issued device. Suggesting in large military populations, the anatomical characteristics of the ear canal can vary wide enough that an earplug size must be considered, as a one-size-fits-all earplug is likely not appropriate for 100% of SMs.
It is well understood that the method to address poor HPD fitting techniques is additional or remedial training. As shown in , the current study found a short-term (immediate) effect of training (regardless of type) with an overall SRF pass rate of 75% (241 of 321) in a group where prior to training (i.e. ISF) the pass rate was 0%. A total of 80 persons remained in the fail category (current n = 55, eHPD n = 8, integrated n = 17) post-remedial training. The persistent inability to score at or above the target PAR could be due to a number of factors. Additionally, the higher rate of fails in the current method cohort may be tied to persons continuing to test and fit an earplug that is the incorrect size for their ear. This cohort did not receive an expert fit, and therefore did not have the ability to verify with an expert that the target PAR value was achievable. However, it should be noted that, although high, the observed post-training fail rate (50%) for this group is consistent with other reported fail rates occupational HPD fit-trainings (Federman and Duhon Citation2016; Murphy, Themann and Murata Citation2016).
Post-training fit-tests revealed a wide range in the achieved attenuation by participants across all training methods (−0.3 to 52.6 dB). Variability in response was expected, as the HPD fit-test used in this study was a psychoacoustic subjective measure of hearing, and the PAR is a calculated value of attenuation achieved (Nélisse et al. 2015). A total of 241 participants were able to demonstrate the skill of inserting and completing the HPD fit-test to achieve attenuation that met or exceeded the study criterion PAR of 25.0, of which 146 participants were able to achieve (or exceed) the earplug NRR of 33.0 dB. These high positive PAR values may provide users over protection, but we cannot say that with any certainty. However, the additive effects and exposure level of more than one round of weapon fire in addition to more than one shooter firing at (or near) the same time is beyond the scope of this paper, and both scenarios are likely on a weapons firing range in a training environment.
When investigating by training method, a trend in the pass/fail rate distribution at the SRF is discernable (see ). Immediately post-training (SRF), a total of 80 participants achieve a PAR value of less than the 25.0 dB criterion. Of these 80 participants, 69% (55 of 80) completed the current fit-training method. This is in comparison with a continued fail rate at the post-training (SRF) fit-test of 10% (8 of 80) for those who completed the eHPD training method, and 21% (17 of 80) of those who completed the integrated fit-training method. These results indicate that, not only are the largest percentage of post-training fail rates occurring in the current training group (50%), the majority of persons who remain unable to achieve a passing score are also in the current group (69%). Future studies should investigate the long-term effect of these fit-training methods.
Delta PAR was calculated (post- minus pre-training PAR) for each participant, and used as the metric of change. Both the eHPD and integrated fit-training formats resulted in a statistically significant increase in achieved attenuation immediately post-training compared to the current military HPD fit-training method. Calculated delta PAR values were found to range from −20 to 48 dB. A negative delta PAR value indicates that the post-training SRF PAR values were lower than the measured ISF PAR value. Possible explanations for this occurrence include: poor fit-technique, inattention of the listener, and tester error either in isolation or combination. For example, a score of −20 is possible if (a) the post-training SRF is roughly 20 dB less than the ISF; (b) if the post-training SRF occluded thresholds were similar to the unoccluded thresholds, indicating a poor fit of the earplug; and (c) if the tester failed to recognise and retest the listener.
The results from this study failed to detect a difference in user achieved attenuation immediately post-training (i.e. delta PAR) among recruits who completed the eHPD and integrated fit-training method. Specifically, by utilising either training method, the expert (i.e. audiologist or hearing conservation technician) could successfully train recruits to don their issued HPDs and achieve adequate attenuation for weapons firing. The greatest difference between these two training methods would be the amount of time spent by the expert per recruit or SM. The eHPD method, as detailed above, is a brief one-on-one training method that can be accomplished in less than 1 min, while the integrated method utilised a proctored 30-min video presented in a small group setting paired with the one-on-one 30 s eHPD method. Worthy of note is that both training methods (eHPD and integrated) utilised a binaural three-frequency fit-test in order to validate the fit achieved by the user. Each fit-test is approximately 6 min per person. Therefore with training and validation, the difference between the two methods is approximately 30 min (7 min for the eHPD method compared to the 37 min integrated method).
The eHPD fit training method is based on experiential learning theories. That is, experiential learning uses experience to teach a new skill rather than a traditional lecture to a group or classroom setting (Taylor and Hamdy, Citation2013; Yardley, Teunissen and Dornan Citation2012). It is a cycle of learning in which the learner experiences an event, reflects upon what just occurred, and replicates the action, both to demonstrate what was learned in a new environment but also to create another experience (Kolb and Kolb Citation2005). With regards to implementation in occupational health and safety, experiential training paradigms have received some research attention. For example, Burke et al. (Citation2011) found that highly engaging safety training methods (i.e. experiential based) have been found to be more effective than less engaging methods (e.g. lectures) in increasing knowledge acquisition and safety performance. Burke et al. (Citation2011) also reported the motivation of the learner to acquire the knowledge provided in the safety brief is partly based on the perceived severity of the hazard. Additionally, Smith et al. (Citation2014) reported that these experiential effects are teaching moments in which users can be instructed on proper HPD fitting.
According to Fowler (Citation2008, 431) experiential learning is facilitated by three components: (a) “external intervention of a ‘teacher’ to provide an experience be it real or vicarious, and then prompting reflective questions, thoughts, and action”, (b) “deliberate action of the student to combine the experience and reflection, which is driven by the student’s own inner motivation”, and (c) “interaction of a third party or action” (e.g. asking questions for clarification). eHPD fit-training incorporates all three components described by Fowler (2008). Specifically, eHPD training provides the learner with one-on-one interaction with an expert (i.e. teacher) who provides the experience of donning an issued HPD. This interaction includes a verbal step-by-step instruction plus a physical demonstration of the proper insertion technique for the device being issued. Lastly, the learner is fit by the expert (i.e. Expert Fit [EF]) with their issued HPD, allowing for the experience of what a correctly fit HPD feels like and how much quieter the ambient environment is while the HPD is donned properly. At any point during this instruction period, the recruit can (and is encouraged to) ask questions for clarification. A confirmatory fit-test with the earplugs that were fit by the expert (EF) provides the recruit with a quantitative PAR value that shows the amount of attenuation possible with the proper fit of the issued device. Immediately following the EF and fit-test, the recruit is asked to remove and reinsert (i.e. Self-Re-fit [SRF]) the earplug as s/he just experienced it and complete a final fit-test. This final fit-test is called the SRF fit-test, and it provides the recruit with a quantitative value as to their achieved attenuation. The resulting SRF fit-test attenuation values also provide quick feedback to the user as to whether s/he has acquired the skill to replicate the EF.
Federman and Duhon (Citation2016) concluded that improper fit at the time of hearing conservation training was likely due to factors such as poor understanding of what a proper HPD fit should feel like or being unaware of proper insertion techniques. As demonstrated in this study, these challenges may be addressed and eliminated by briefly showing the individual how to properly fit the earplug and verify their fit using a FAES fit-test. Additionally, using the eHPD fit-training method described herein, which is based on experiential learning theories, a recruit will experience how a properly fitted device both feels and sounds (“what right feels like”) thereby providing a frame of reference that s/he can replicate.
Conclusion
The goal of this study was to investigate whether HPD fit-training methods (current, eHPD, or an integrated approach) would alter USMC training recruits’ immediate ability to fit and achieve adequate attenuation with a standard issued foam earplug. The use of the eHPD fit-training method (either alone or in combination with the current method) resulted in a higher percentage of the population (by 42 or 34%, respectively) able to achieve the minimum target attenuation immediately post-training. Additionally, of those who completed the eHPD fit-training method (either alone or integrated) were able to fit and achieve a higher attenuation (by 9 dB on average) compared to the current HPD fit-training method.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the U.S. Government. This work was prepared by employees of the U.S. Government as part of their official duties. Title 17 U.S.C. §105 provides that ‘Copyright protection under this title is not available for any work of the United States Government.’ Title 17 U.S.C. §101 defines a U.S. Government work as a work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties. The study was deemed NOT human subjects research but military programme improvement by the Naval Submarine Medical Research Laboratory Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects.
Acknowledgements
The authors of this report greatly appreciate Brigadier General Terry V. Williams, Colonel Neal Pugliese and the rest of USMC MCRD, Parris Island leadership’s willingness to collaborate with us regarding hearing conservation efforts and the programmatic efforts this project represents. Thanks to LT Laura Stephenson (US Navy), CAPT Jenny Davis (US Army), MAJ Johnny Foster Jr. (US Air Force), LT Kyle Shepard (US Navy) and Mr. Michael Boardman for their assistance with data collection. Thanks also to MCRD Branch Health Clinic OIC CAPT George Dyer, and clinic personnel LCDR Charles Hitchock, Mr. Dave Mobley, Ms. Shakira Thomas, HN Marcquis Hamm, HN Heather Hataway, and HM2 Brendan Gordon for their support of this study. For logistic support, we offer thanks to, Mr. Ronald Hackler, CAPT Frank Mastromauro, CAPT Richard Steele, CAPT Jordan Willoughby, and SGT John Ripp. We must also express our appreciation to the USMC Parris Island Mess Hall Staff and SSGT Reberiano Fuentes for preparing, transporting, and coordinating delivery of over 900 meals for our study participants. We also would like to thank the training recruits who participated and made this project possible.
Additional information
Funding
References
- Abel, S. M. 2008. “Barriers to Hearing Conservation Programs in Combat Arms Occupations.” Aviation, Space, and Environmental Medicine 79 (6): 591–598. doi:10.3357/asem.2262.2008.
- Ahroon, W. A., M. E. Hill, and D. P. Goodes. 2011. “Analysis of Army-Wide Hearing Conservation Database for Hearing Profiles Related to Crew-Served and Individual Weapon Systems.” Noise & Health 13 (50): 76–83. doi:10.4103/1463-1741.73992.
- American National Standards Institute. 2018. American National Standard Method: Performance Criteria for Systems That Estimate the Attenuation of Passive Hearing Protectors for Individual Users (ANSI S12.71). New York: American Standards Institute.
- ANSI/ASA S12.71. 2018. American National Standard Method: Performance Criteria for Systems That Estimate the Attenuation of Passive Hearing Protectors for Indiviudal Users. New York: American Standards Institute.
- Berger, E. H. 1996a. E-A-R LOG® 5: Hearing Protector Performance: How They Work – and – What Goes Wrong in the Real World. Indianapolis, IN: Aearo Company.
- Berger, E. H. 1996b. E-A-R LOG® 19: Tips for Fitting Hearing Protectors. Indianpolis, IN: Aearo Company.
- Berger, E. H. 2013. “‘Calibrating’ the Insertion Depth of Roll-Down Foam Earplugs”. Proceedings of Meetings on Acoustics ICA2013 19 (1): 040002.
- Burke, M. J., R. O. Salvador, K. Smith-Crowe, S. Chan-Serafin, A. Smith, and S. Sonesh. 2011. “The Dread Factor: How Hazards and Safety Training Influence Learning and Performance.” The Journal of Applied Psychology 96 (1): 46–70. doi:10.1037/a0021838.
- Commandant of the Marine Corps. 2016. "Marine Corps Hearing Conservation Program." (MCO 6260.3A). Washington, DC: Headquarters USMC
- Federman, J., and C. Duhon. 2016. “The Viability of Hearing Protection Device Fit-Testing at Navy and Marine Corps Accession Points.” Noise and Health 18 (85): 303–311. doi:10.4103/1463-1741.
- Fowler, J. 2008. “Experiential Learning and Its Facilitation.” Nurse Education Today 28 (4): 427–433. doi:10.1016/j.nedt.2007.07.007.
- Gaston, J. R., and T. R. Letowski. 2012. “Listener Perception of Single-Shot Small Arms Fire.” Noise Control Engineering 60(3): 236–245.
- Gong, W., X. Liu, Y. Liu, and L. Li. 2019. “Evaluating the Effect of Training along with Fit Testing on Foam Earplug Users in Four Factories in China.” International Journal of Audiology 58 (5): 269–277. doi:10.1080/14992027.2018.1563307.
- Hager, L. D. 2011. “Fit-Testing Hearing Protectors: An Idea Whose Time Has Come.” Noise & Health 13 (51): 147–151. doi:10.4103/1463-1741.77217.
- Helfer, T. M., M. Canham-Chervak, S. Canada, and T. A. Mitchener. 2010. “Epidemiology of Hearing Impairment and Noise-Induced Hearing Injury among US Military Personnel, 2003–2005.” American Journal of Preventive Medicine 38 (1 Suppl): S71–S77. doi:10.1016/j.amepre.2009.10.025.
- Joseph, A., J. Punch, M. Stephenson, N. Paneth, E. Wolfe, and W. Murphy. 2007. “The Effects of Training Format on Earplug Performance.” International Journal of Audiology 46 (10): 609–618. doi:10.1080/14992020701438805.
- Karch, S. J., J. E. Capó-Aponte, D. S. McIlwain, M. Lo, S. Krishnamurti, R. N. Staton, and K. Jorgensen-Wagers. 2016. “Hearing Loss and Tinnitus in Military Personnel with Deployment-Related Mild Traumatic Brain Injury.” US Army Medical Department Journal 52–63.
- Kolb, A. Y., and D. A. Kolb. 2005. “Learning Styles and Learning Spaces: Enhancing Experiential Learning in Higher Educaiton.” Academy of Management Learning & Education 4 (2): 193–212. doi:10.5465/amle.2005.17268566.
- Liu, Y., and M. Yang. 2018. “Evaluating the Effect of Training along with Fit Testing on Earmuff Users in a Chinese Textile Factory.” Journal of Occupational and Environmental Hygiene 15 (6): 518–526. doi:10.1080/15459624.2018.1456662.
- Marshall, L., P. Weathersby, J. McCluskey, and H. Huebner. 2016. The Introduction of Custom Earplugs aboard LCS-1. (NSMRL/F1401/TM-2016-1315). Groton, CT: Naval Submarine Medical Research Laboratory.
- Murphy, W. J., M. R. Stephenson, D. C. Byrne, B. Witt, and J. Duran. 2011. “Effects of Training on Hearing Protector Attenuation.” Noise & Health 13 (51): 132–141. doi:10.4103/1463-1741.77215.
- Murphy, W. J., C. L. Themann, and T. K. Murata. 2016. “Hearing Protector Fit Testing With Off-Shore Oil-Rig Inspectors in Louisiana and Texas.” International Journal of Audiology 55 (11): 688–698. doi:10.1080/14992027.2016.1204470.
- Nélisse, H., C. Le Cocq, J. Boutin, F. Laville, and J. Voix. 2015. “Systematic Evaluation of the Relationship Between Physical and Psychoacoustical Measurements of Hearing Protectors’ Attenuation.” Journal of Occupational and Environmental Hygiene 12 (12): 829–844. doi:10.1080/15459624.2015.1053893.
- OSHA 2008. “OSHA/NHCA/NIOSH Alliance, Best Practice Bulletin: Hearing Protection-Emerging Trends: Indiviudal Fit-Testing.” https://www.hearingconservation.org/assets/docs/AllianceRecommendationForFitTesting_Final.pdf
- Pääkkönen, R., S. Savolainen, J. Myllyniemi, and K. Lehtomäki. 2000. “Ear Plug Fit and Attenuation – an Experimental Study.” Ata Acustica United with Acustica 86 (3): 481–484.
- Salmani Nodoushan, M., A. H. Mehrparvar, M. Torab Jahromi, S. Safaei, and A. Mollasadeghi. 2014. “Training in Using Earplugs or Using Earplugs with a Higher than Necessary Noise Reduction Rating? a Randomized Clinical Trial.” The International Journal of Occupational and Environmental Medicine 5 (4): 187–193.
- Samelli, A. G., R. F. Gomes, T. V. Chammas, B. G. Silva, R. R. Moreira, and A. C. Fiorini. 2018. “The Study of Attenuation Levels and the Comfort of Earplugs.” Noise & Health 20 (94): 112–119. doi:10.4103/nah.NAH_50_17.
- Samelli, A. G., C. H. Rocha, P. Theodósio, R. R. Moreira, and I. F. Neves-Lobo. 2015. “Training on Hearing Protector Insertion Improves Noise Attenuation.” CoDAS 27 (6): 514–519. doi:10.1590/2317-1782/20152014128.
- Smith, P. S., B. A. Monaco, and S. L. Lusk. 2014. “Attitudes toward Use of Hearing Protection Devices and Effects of an Intervention on Fit-Testing Results.” Workplace Health & Safety 62 (12): 491–499. doi:10.3928/21650799-20140902-01.
- Suter, A. H. 2007. Hearing Conservation Manual. 4th ed. Milwaukee, WI: Council for the Accreditation of Occupational Hearing Conservation.
- Taylor, David C. M., and Hossam Hamdy. 2013. “Adult Learning Theories: Implications for Learning and Teaching in Medical Education: AMEE Guide No. 83.” Medical Teacher 35 (11): e1561–e1572. doi:10.3109/0142159X.2013.828153.
- Tikka, C., J. H. Verbeek, E. Kateman, T. C. Morata, W. A. Dreschler, and S. Ferrite. 2017. “Interventions to Prevent Occupational Noise-Induced Hearing Loss.” Cochrane Database of Systematic Reviews 7: CD006396. doi:10.1002/14651858.CD006396.pub4.
- Toivonen, M., R. Pääkkönen, S. Savolainen, and K. Lehtomäki. 2002. “Noise Attenuation and Proper Insertion of Earplugs into Ear Canals.” The Annals of Occupational Hygiene 46 (6): 527–530. doi:10.1093/annhyg/mef065.
- Tsukada, T., and H. Sakakibara. 2008. “A Trail of Indiviudal Education for Hearing Protection with an Insturment That Measures the Noise Attenuation Effect of Wearing Earplugs.” Industrial Health 46 (4): 393–396. doi:10.2486/indhealth.46.393.
- Tufts, J. B., S. Chen, and L. Marshall. 2013. “Attenuation as a Function of the Canal Length of Custom-Molded Earplugs: A Pilot Study.” The Journal of the Acoustical Society of America 133 (6): EL446–EL451. doi:10.1121/1.4802896.
- U.S. Army Public Health Command. 2013. Before- and After-Noise Control Treatment Risk Assessment at an Indoor Tactical Multi-Lane Army Firing Range, TIP 51-006-1112. Aberdeen Proving Ground, MD: U.S. Army Public Health Command.
- U.S. Army Public Health Command. 2014. Readiness Through Hearing Loss Prevention, TG 250. Aberdeen Proving Ground, MD: U.S. Army Public Health Command.
- U.S. Department of Defense. 2010. Hearing Conservation Program (HCP), Department of Defense Instruction 6055.12. Washington, DC: U.S. Department of Defense.
- U.S. Department of Defense 2015. MIL-STD-1474E, Design Criteria Standard, Noise Limits, AMSC 9542. Washington, DC: U.S. Department of Defense.
- U.S. Department of Defense 2019. Hearing Conservation Program (HCP), Department of Defense Instruction 6055.12. Washington, DC: U.S. Department of Defense.
- Veterans Benefits Administration 2019. Annual Benefits Report: Fiscal Year 2018: Compensation. Washington, DC: U.S. Department of Veterans Affairs. https://www.benefits.va.gov/REPORTS/abr/docs/2018-compensation.pdf
- Voix, J., and L. D. Hager. 2009. “Individual Fit Testing of Hearing Protection Devices.” International Journal of Occupational Safety and Ergonomics : JOSE 15 (2): 211–219. doi:10.1080/10803548.2009.11076802.
- Watts, K. L., R. Welles, and P. Zurek. 2018. “Development of the Warfighter’s Hearing Health Instructional (WHHIP) Primer App.” Military Medicine 183 (suppl_1): 231–236. doi:10.1093/milmed/usx177.
- Wells, Timothy S., Amber D. Seelig, Margaret A. K. Ryan, Jason M. Jones, Tomoko I. Hooper, Isabel G. Jacobson, and Edward J. Boyko. 2015. “Hearing Loss Associated with US Military Combat Deployment.” Noise & Health 17 (74): 34–42. doi:10.4103/1463-1741.149574.
- Williams, W. 2004. “Instruction and the Improvement of Hearing Protector Performance.” Noise and Health 7 (25): 41–47. doi:10.4103/1463-1741.31629.
- Yardley, Sarah, Pim W. Teunissen, and Tim Dornan. 2012. “Experiential Learning: AMEE Guide No. 63.” Medical Teacher 34 (2): e102–e115. doi:10.3109/0142159X.2012.650741.
- Yong, J. S. E., and D. Y. Wang. 2015. “Impact of Noise on Hearing in the Military.” Military Medical Research 2: 6. doi:10.1186/s40779-015-0034-5.