
Abstract
Objectives
To understand how individuals with tinnitus perceive their sound generating devices help them in managing their tinnitus
Design
A qualitative interview based study employing grounded theory methodology to establish a theory as to the mechanisms that sound therapies contribute to coping with tinnitus. Ten National Health Service patient participants (who had been issued with sound generating devices from an Audiology department in England) participated in in depth interviews.
Results
This study identified that sound therapies helped create a sense of escapism and control. In addition, the process of obtaining devices created a sense of validation of the patient and their tinnitus. These mechanisms restore the previously disrupted harmony between the self and body.
Conclusion
Sound generating devices can assist coping through a number of mechanisms. There is no evidence that they ablate or remove perception of tinnitus. This study contributes novel theory based on patient accounts as to the potential benefits of sound generating device use.
Background
Tinnitus is a subjective perception of sound where there is no external sound source (Sereda et al. Citation2018). It can present as ringing, buzzing, hissing or as other sounds and can occur in those with and without hearing loss (Tyler et al. Citation2015; Lee, Makino, and Yamahara Citation2018). Tinnitus has varying degrees of physical and mental impact on individuals, ranging from mild to debilitating (Tyler, Coelho, and Noble Citation2006; Zeman et al. Citation2014; Bruggemann et al. Citation2016; Teixeira et al. Citation2017). A systematic review by Pattyn et al. (Citation2016) established a higher co-morbidity of anxiety related disorders in those with bothersome severe tinnitus than those who were able to manage their tinnitus. The neuroplasticity of the auditory system has raised the prospect of re training sound perception and reducing awareness of tinnitus. However, evidence suggests that these mechanisms are not reliable. Yet sound therapies are effective in some studies. In clinical audiology sound therapy has been a long-standing treatment option which focuses on using external sounds to interfere with the neuronal activity relating to the tinnitus. Such theories has been the basis for Tinnitus Retraining Therapy (TRT) (Jastreboff and Jastreboff Citation2000; Tyler et al. Citation2012; Aazh, Moore, and Glasberg Citation2008; Pedemonte et al. Citation2010). Specific devices to alleviate the perception of tinnitus (sound generating devices) can be used to reduce the contrast between the tinnitus and the ambient sounds in an individual’s surroundings. This form of sound enrichment can be provided via mobile phone apps and through free standing sound generators; combination devices (hearing aids with sound generators built in) and ear level sound generators (Hesser et al. Citation2009; Handscomb Citation2006; Henry et al. Citation2017; Searchfield, Linford, and Durai Citation2019).
Interestingly when comparing the effectiveness of these devices no significant differences have been observed between them (Tutaj, Haare, and Sereda Citation2017). Neuromodulation is based on the theory that the pathophysiology of tinnitus is the sub-optimal involvement of the central nervous system. The approach also focuses on modulating neuronal activity as it may reverse pathologies causing tinnitus (Wurzer and Hauptmann Citation2018). Much of the research in this area has low validity due to the lack of comparison groups within studies (Fisher and Boswell Citation2016). This limitation is difficult to address as the heterogeneous nature of tinnitus means that different forms of tinnitus will vary in their underlying pathophysiology (Wegger, Ovesen, and Larsen Citation2017). Recent NICE guidance proposes that the evidence for sound therapy is too uncertain to base clinical recommendations (NICE Citation2020).
The biomedical model of illness has long been used in managing tinnitus; it assumes a causal relationship between disease and illness (Lane Citation2014). Health professions often exhaust diagnostic test batteries in a bid to explain invisible symptoms/conditions. Marks, Smith, and Mc Kenna (Citation2019) supported this with their findings revealing professionals placed greater emphasis on establishing a medical diagnosis for tinnitus rather than coping strategies. In instances where a diagnosis was not possible, individuals with tinnitus expressed heightened anxiety due to the lack of validation. It is therefore not surprising that clinical encounters can negatively influence tinnitus impact (Pryce and Wainwright Citation2008). The prescription of a specific device to obscure perception of tinnitus is attractive to clinicians (Pryce et al. Citation2018). It is still widely offered despite the lack of research evidence of effectiveness. Anecdotal evidence suggests there remains a perception of benefit from patient and clinicans (Hoare et al. Citation2015; Kochkin and Tyler Citation2008). This suggests that the mechanisms of sound therapy are not well understood and that patient benefit may not be captured by current outcome measures.
The overall purpose and therapeutic value of offering sound therapy is a highly complex intervention involving therapeutic contact, based on counselling & information sharing as well as the device itself. The MRC (Citation2008) (Anderson Citation2008) have long suggested that complex interventions should be understood at the mechanistic level in order to know what the active ingredients of the intervention are. Simple studies examining how well sound reduces tinnitus perception or tinnitus distress have not yet explored the active ingredients of the intervention and an inductive approach to developing a stronger theoretical understanding is required (Anderson Citation2008).
Alongside an understanding of mechanisms, clinicians need insights into the patient experience of tinnitus for which we have limited evidence (Pryce and Shaw Citation2019). Lifeworld-led care is the foundation for caring science (Horberg, Ozolins, and Ekebergh Citation2011). It highlights the importance of viewing the world as the patient does concerning well-being and suffering (Todres and Galvin Citation2010). Embodiment is an aspect of well-being and refers to the internal self and the body co-existing in harmony. To elaborate, it is the physiological and biological presence our bodies have which is an important requirement for our emotions, thoughts and interactions i.e. the self. Whilst humans do not actively assess well-being, it becomes a desired state when illness disrupts the body (Turkel, Watson, and Giovannoni Citation2018). For this reason the phenomenon of embodiment and well-being is understood from a holistic viewpoint (Mills Citation2017). For chronic health conditions, working towards improving well-being is beneficial for people based on their lived experiences (Miles, Chapman, and Francis Citation2015). Dauman et al. (Citation2017) reported participants with tinnitus experienced a “loss of body ownership” and “holding on to a fragile body.” We do not have a clear theoretical understanding of how sound therapies influence the individual sense of coping. A qualitative approach informed by grounded theory procedures has been demonstrated to be is effective in examining changes and adaptations caused by tinnitus and hearing conditions (Pryce et al. Citation2018; Pryce and Chilvers Citation2018; Pryce and Shaw Citation2019).
This project aimed to understand how people with tinnitus who had used sound generators, experienced and benefitted from their use. This facilitates a data driven theoretical understanding of the mechanisms that create a perceived benefit. This approach enables us to learn more about how sound therapies can be helpful to people with tinnitus. A clear theoretical understanding can inform clinicians as to the mechanisms that explain how and why benefit may occur. Furthermore, this can guide appropriate clinical measurement by identifying the active ingredients that warrant measure.
Methods
An inductive study informed by Strauss and Corbin’s approach to grounded theory was designed to develop a theoretical understanding of the ingredients that were beneficial in use of sound therapies from a contrasting set of participant accounts.
NHS ethical approval was obtained through proportionate review on the 11 September 2019 (reference 19/WM/0271).
To ensure anonymity, pseudonyms were assigned to each transcript and all personal identifiable information was de-identified. All audio-recorded interviews were erased once interviews were transcribed.
A total of 1129 patients were fitted with sound generating devices (SGDs) from March 2016 to March 2019.Invitations were sent to 72 patients who had been issued a sound generator over this period. Those over the age of 18 with sufficient English to provide informed consent and participate in interviews were included. In keeping with grounded theory approaches, participants were selected to provide contrast in cases and sampling continued until no new themes were generated in the analysis process (Corbin and Strauss Citation2008). The value of contrasting cases is to explore the themes that have consistency across different life experiences.
Data gathering
Participants were selected from contrasting postcode regions of the midlands in England to ensure there was contrast between participants. Purposive sampling approach led to examination of cases that contrasted in age, sex and demographic profile.
Face-to-face interviews were carried out at UHCW NHS Trust over a period of 2 months. The interviews had a mean duration of 45 min. All interviews were audio-recorded. Written notes and memos were recorded throughout the data gathering period, enabling reflection on the interviews to complement the analysis of the transcribed data. Interviews were semi-structured as this enabled the researcher to obtain rich information about the participant’s thoughts and experiences about tinnitus and SGDs in a manner that was not deemed inflexible or objective (De Jonckheere and Vaughn Citation2019). As noted by Corbin and Strauss (Citation2008), an interview guide was used to facilitate the semi-structured interviews. The guide consisted of open-ended questions that allowed concentrated information to be obtained (Charmaz Citation2009). The questions were designed enable the participants to contextualise their experience with their tinnitus and SGDs. In order to generate themes, the interviews were adapted based on previous interview findings using constant comparative analysis (Charmaz Citation2009) ().
Figure 1. Interview questions.
After each interview, the researcher (SM) transcribed the data verbatim. The transcript was then reviewed (by SM) with the recording before the audio-recording was deleted. Data transcription enabled constant comparison between codes and concepts.
Data analysis
Interviews and analysis were carried out sequentially as the data obtained from the interviews informed the topics and phrasing of questions to further explore. Open coding of all meaning statement covered all content of initial transcripts. These meaning statements were grouped to form ‘codes’ and organised to provide a relational framework description to cover the variation of experience with sound generators that were described in the data set (Charmaz Citation2009). These codes were analysed in terms of their properties (the sub themes that were labelled under the coded heading) and dimensions (the range of descriptions included). Data analysis and data gathering occurred concurrently so that new transcripts were analysed in comparison with previous accounts and promising topic areas were explored directly in interview. In practice there was a high level of consistency in terms of reported mechanisms across the dataset. Both researchers (SM & HP) blind coded transcripts and compared coding to triangulate analysis e.g. provide separate analysis to check the themes and enhance the credibility of the findings.
Results
A total of ten participants were interviewed of which seven were female and three were male. Participants had a mean age of 63.7 years. All participants were of white ethnicity. Four participants reported having right-sided tinnitus, one reported left-sided tinnitus and five reported hearing tinnitus in their head. The mean duration of having tinnitus was 1.9 years. All participants had been issued with a sound generator; in addition to this, four had hearing aids and four were fitted with eWNGs. No participants had a combination device ().
Table 1. Participant Information.
Descriptions of tinnitus distress
Participants described their tinnitus using emotive language which emphasised their view that tinnitus is meaningful. David likened his tinnitus to being “tortured” and described it “as being stuck in a room and having a constant loud shrill being blasted in each direction towards you.” Similarly, Sarah compared her tinnitus to “a bag of snakes… which gradually gets so loud, you head feels like it’s going to explode from all the noise.” John reported, “you don’t feel the same as you were before the tinnitus, it impacts on your personality and it wears you away; it makes you less patient.”
The sense of disembodiment is illustrated in the choice of language, meaning and metaphor. From positioning tinnitus as external “it impacts…” to “it’s like being blasted” to the metaphor of “snakes” there is a sense of separation between the self and the sound. It is “other.” This leads to feelings of discord between the internal self and their “faulty” body.
The participants reported finding benefit from use of sound generator devices. The themes described the range of mechanisms by which sound therapy benefitted the participants.
The first mechanism was validation
Participants reported on the great value in the validation they found in clinical encounters and in the tangible sound generator device (SGD). Acceptance of a SGD provided access to clinical audiology.
As Shirley noted “People can’t relate to it because it’s invisible”; she further went on to say the tinnitus was “not like a hearing loss where you can wear hearing aids and people see them [the SGD]…people think it’s just a noise in your head but it is more than that, it is a constant noise in your head that can consume you.” This implied that the invisible nature of tinnitus made other people less empathetic to the disruptions that the tinnitus caused individuals.
In this context the understanding clinician was particularly important. All participants reported how much they valued having time to talk about their tinnitus with audiology professionals. Janet reported “it was nice to talk about the tinnitus and nice to know that people understand tinnitus.” For many it validated the existence of the tinnitus. Beverley commented “it was a fantastic way of acknowledging the tinnitus, I didn’t want the ‘yes you have tinnitus” it was more “we know how it could manifest if not managed and we have the tools to help you.” In particular she mentioned “that was taken very seriously … people think it’s just ringing in your ears and it’s not. Just knowing someone placed great importance on the impact it was having and then provided me with solutions was just amazing.” Similarly Kate remembered and described her encounter as “informative, I liked the way they took on my concerns and validated that I’m not going mad. They did not make fun of me. I was taken serious all the time, I wasn’t made to feel stupid. I was taken seriously with this invisible sound. It was considered a real issue.”
The sound generator as part of the clinical intervention provided a pragmatic focus as described by Shirley “/accepted it and looked out-side of the tinnitus and thought I have tinnitus now I have a choice in that it’s not life-limiting and I can accept it. The sound generator is a vital part in my acceptance of my tinnitus.” Kate also drew in on the physical nature of the sound generator and referred to it as “a physical crutch- a physical aid to help me deal with the tinnitus. It’s a physical aid which helps to validate the tinnitus to other people.”
Validation has previously been described with invisible health conditions as an important contributor to coping (Pryce and Wainwright Citation2008; Pryce and Shaw Citation2019). In this case the validation occurs in two ways. Firstly the sound generator provides a focus for clinical conversation, validating the lived experience by being taken seriously by the clinician, Secondly the device itself communicates an objective expression of the tinnitus to others, raising the invisible to a visible health condition (“I was taken seriously”). This in turn provides greater social support. The awknowledgement of the tinnitus as a legitimate health condition prompts a greater sense of ownership over the experience and reconnects the tinnitus sound with the individual hearing the sound (“way of acknowledging the sound”).
The second mechanism was coded as “escapism”
This code illustrates the process that enables the sound from the sound generating devices to be effective in reducing tinnitus awareness. It supports participants’ relief from the tinnitus by providing a diversion from the intrusiveness of tinnitus.
Participants described the sounds to provide “a psychological help in reducing tinnitus rather than the masking of the noise” (John). Many participants described that the sounds provided a diversion from the intrusive tinnitus when using SGDs. Derek reported “It takes your mind off the tinnitus. You’re listening to the sea waves and it’s a distraction.” Molly likewise described the sounds helped to “distract your mind.”
The distraction was characterised as an escape, prompting pleasing memories. Janet reported “They’re nice comforting sounds which take you back to nice memories of bird watching. It’s pleasant. It took me back to when I took my son and his friends bird watching, happy times.” Whilst other participants created visualisations to go with the sounds they heard like Beverley, “mine aren ‘t memories, its visual creations of the sounds I hear” .Often this transition to happier/calming thoughts enabled participants to relax and immerse themselves in those pleasant emotions of “comfort, familiarity” and “ peace”. Such descriptions illustrate how sound assisted regaining a sense of relaxation and well-being in the presence of the tinnitus.
Whilest this is described a ‘escape from’ it is a description of reducing distress in the presence of tinnitus – shifting the sense that tinnitus has control over and instead that control can be regained. The escape here is from distress associated with the tinnitus. As David explained “the sound generator helps me to escape from the tinnitus, to have a release and some relief from the tinnitus. It eases it because I can drift off to a different happier place.” Likewise, Shirley narrated “the sound generator does allow you to escape. It definitely provides that escape mechanism because it helps you to stop thinking about the tinnitus and come outside of it.”
Shirley reported the use of the sound was more helpful than mindfulness alone in reducing tinnitus awareness. “Mindfulness is about listening to breathing but it’s not a physical thing, whereas the sound generator is physical, I know the presence of the sound generator gives me comfort in knowing that I can cope with the tinnitus. It’s physical and gives you that focus to concentrate on. But mindfulness, it’s invisible and harder to engage with, your mind can drift.”
This code demonstrates how the use of pleasant sounds triggers the escapism mechanism via memories, visual representations or distractions. When the participant experiences a sense of escapism the tinnitus becomes a less bothersome presence – part of their usual hearing – but not a distressing part.
The third mechanism was regaining control
The sound generator represented physical control over invisible tinnitus Shirley reported “It gives you control or power to overcome the tinnitus.” Similarly, Beverley describes the sound generator symbolising physical control over her tinnitus, “I love the fact that I can turn the volume down on the sound generator because it in my mind it’s like I can turn the volume of the tinnitus down… control over the tinnitus.” Sarah explained the physical nature of the sound generator led her to see it as “definitely comfort it’s almost like it’ s something … this will sound daft but you can touch it… you clasp on to it. . that’s how it is a comfort and it’s something that I do know works 95% of the time.” Sarah further clarified “/can control it… I can turn it down on the machine but not my tinnitus … whether it is something to do with the control over it and that’s possibly where the problem was in the beginning- there was no control. I didn’t know how to control it.” Shirley described how the sound generator symbolised enablement, “initially I was doubtful of the sound generator but over time it has become an enabler, like a friend that you trust.” Whilst Kate felt the sound generator represented “relief, comfort, familiarity, hope, reliance.” David echoed the sentiments of relief. Janet described the sound generator to exemplify a new beginning, “like the winter is starting to retreat and spring is coming and you hear a robin… And you think oh blimey the winter is nearly behind us almost like a new beginning.”
The impact of tinnitus disrupted many aspects of individuals’ lives leaving them feeling alienated from their body and therefore disembodied. Through drivers like validation from clinical encounters and escapism via their SGDs, individuals felt they were able to regain control of the internal chaos created by the tinnitus. This is because through validation and the activation of the escapism mechanism, individuals saw their faulty body begin to function as they had previously known it to. The ability to escape from the sound on demand communicated a possibility of controlling the tinnitus itself and regaining internal mechanisms to reduce the awareness of tinnitus. This led to a new internal sense of control and a reconnection between the tinnitus and the self. demonstrates how each theme interacts to achieve the phenomenon.
Figure 2. The connection between the mechanisms.
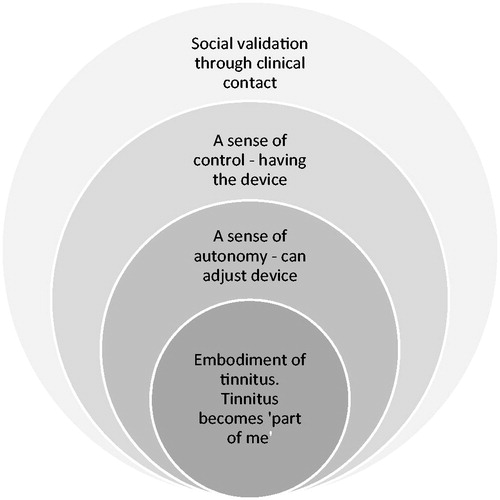
The core process – facilitating embodiment
Embodiment is both a mechanism that described how direct benefit occurred. It is also the core category in these data e.g. it explains variance, occurs in each account repeatedly and links the other categories in an overarching framework.
Embodiment is founded on the belief that the physical body is more than an object; it represents the internal self and encompasses our thoughts, feelings and experiences. As tinnitus creates a feeling of disassociation and separation between the body and self, it leads individuals to feel disembodied. Therefore, understanding the role embodiment plays in restoring an individual’s desired state of well-being is crucial. All participants reported that using their SGDs reduced feelings of disassociation caused by the tinnitus. David found using the sound generator improved his overall well-being, “it helps me to sleep better which then affects our overall well-being… I was waking up before and constantly feeling tired… but now I have enough sleep and feel better overall in myself.”
The sound generator reduced tinnitus occupation in participants’ minds. Beverley found using the sound generator allowed her to take back some control over the tinnitus as “it reduced the tinnitus which overtakes your mind … it allows you to relax, you can stop thinking of the tinnitus and the loudness and the negative thoughts of not getting any sleep and that has a huge impact .”
For the majority of participants, the sound generator and the eWNGs in particular helped with refocusing their mood by re-establishing their inner peace. Shirley reported “I’m at peace with my tinnitus because of the sound generator.” Derek, Shirley and Molly, who have had tinnitus for over a year, reported the tinnitus was no longer considered a threat and had become a part of who they were i.e. embodiment. Shirley reported ‘the tinnitus is a part of me now. It’s there and almost like when someone touches you and you feel it you know you’re still alive, it’s almost like that, by hearing my tinnitus I know that I’m still alive.” Moreover, Molly described her tinnitus as a comfort blanket, “/feel lost without my tinnitus. I’m constantly listening to it; it’s like a comfort blanket.”
Grounded theory aims to produce a core category or process that explains variation in data and is present in every contrasting account. In this case the mechanisms describe an overarching process by which use of external sound generators is therapeutic for individuals. The core process is of achieving embodiment by autonomy in validation, a sense of escapism and a sense of control. Embodiment is driven by a sense of body ownership where the body belongs to the self (Tsakiris Citation2010). Embodiment is the union between the self and body. This reduces the loss of body ownership (Sierra and David Citation2011). Narratives from this study illustrate how tinnitus fundamentally disturbs the embodied self and leads to loss of body ownership. The use of sound generators enhance embodiment by providing a sense of control over the sound both directly – ability to turn devices on and off but indirectly in the prompting of more pleasant sound associations and a sense of escape from the sound. The validation of symptoms by clinicians during the help seeking process is also important in enhancing autonomy as a valuing of embodiment. These processes help bridge the gap between the prototypical healthy (non tinnitus) body and the participants present lived experience of tinnitus.
Discussion
This research has addressed the gap in knowledge about the process, which facilitates tinnitus reduction when using SGDs. This research recognises and reflects the lifeworld of those with tinnitus and the coping mechanism involved in achieving tinnitus reduction by using SGDs The data reveal that mechanisms are multifaceted and complex – extending beyond a simple causal relationship between awareness or distress from tinnitus and use of sound. These findings stress that the active mechanisms are not simple obscuring of tinnitus signal but rather shifts in bodily awareness. It is a common feature of chronic health conditions that there is a sense of disembodiment in which the affected body part is “faulty.” This supports work by Dauman et al. (Citation2017) who found that individuals with tinnitus reported “holding on to a fragile body” as a result of not being able to escape from their tinnitus.
Participants reported positive tinnitus consultations assisting with some tinnitus reduction. This was due to having the space to talk about their tinnitus, which enabled individuals to put their tinnitus into perspective as well as being given a physical sound source i.e. SGD.
It has been established that individuals experience increased stress and anxiety as a result of their tinnitus (Abbas et al. Citation2019). This can be associated with the autonomic nervous system as the tinnitus is a stressor and triggers the “fight or flight” response which alerts the patient to a possible disturbance in homeostasis (Alpini and Cesarani Citation2006). The code “escapism” is a novel discovery and provides an insight of how these devices are effective in restoring embodiment. SGDs enabled participants to overcome the disturbance to homeostasis leading to the union of the self and body consequently reducing tinnitus awareness.
Limitations
The limitations of this study were the recruitment process and the lack of variations in participant demographics. Although the inclusion criteria were broad as per grounded theory requirements, there was limited diversity amongst the participants recruited. Participants who responded to invitation letters were of the same ethnicity and majority of them were aged 50-70. Whilst previous research has failed to establish why SGDs are beneficial in reducing tinnitus awareness, this study was able to use narratives to establish a novel theory on tinnitus embodiment as well as demonstrating the coping mechanism used to reduce tinnitus awareness. This work describes these maechanisms and the process based on this sample of patients. Further comparison with other samples is required to examine this developing theory in different contexts. The researcher (SM) is a clinical scientist in audiology. Researcher (HP) is an experienced qualitative researcher and researcher in tinnitus. HP provided academic supervision to the project. These researchers bring a clinical perspective to the topic.
Conclusion
This study demonstrates the coping mechanism employed to reduce tinnitus awareness when using sound generating devices. It highlights how the devices enable participants to use escapism as the coping mechanism to restore embodiment following the disruption to the union of the self and body initiated by tinnitus onset.
The descriptive analysis of the narratives obtained can impact on practitioner’s attitudes and management of patients in both primary care and tinnitus support consultations. More research exploring narratives of a diverse age-range, ethnicities and a wider geographical area would further build on this theory as patient narratives can offer a great deal from an individualised viewpoint; this will help to shape tinnitus management.
This work contributes important insights from the patient perspective. This has previously been lacking in the literature on sound therapies and indicates that appropriate outcome measures should include measuring the sense of embodiment of tinnitus, the sense of control and ability to escape and the sense of validation. Measures of awareness or overall handicap arising from the tinnitus may not be adequately sensitive to these important coping mechanisms. The sense of embodiment is a core feature of living well with tinnitus. This deserves further investigation.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Aazh, H., B. C. Moore, and B. R. Glasberg. 2008. “Simplified Form of Tinnitus Retraining Therapy in Adults: A Retrospective Study.” BMC Ear, Nose, and Throat Disorders 8: 7. doi:10.1186/1472-6815-8-7.
- Abbas, Jaffar, Muhammad Aqeel, A. Jaffar, Mohammad Nurunnabi, and Shaher Bano. 2019. “Tinnitus Perception Mediates the Relationship between Physiological and Psychological Problems Among Patients.” Journal of Experimental Psychopathology 10 (3): 204380871985855. doi.org/10.1177%2F2043808719858559 doi:10.1177/2043808719858559.
- Alpini, D., and A. Cesarani. 2006. “Tinnitus as an Alarm Bell: Stress Reaction Tinnitus Model.” ORL J Otorhinolaryngol Re/at Spec 68 (1): 31–37. doi:10.1159/000090488.
- Anderson, R. 2008. “New MRC Guidance on Evaluating Complex Interventions.” BMJ (Clinical Research ed.) 337 (oct22 1): a1937–a1937. doi:10.1136/bmj.a1937.
- Bruggemann, P., A. J. Szczepek, M. Rose, L. McKenna, H. Olze, and B. Mazurek. 2016. “Impact of Multiple Factors on the Degree of Tinnitus Distress.” Frontiers in Human Neuroscience. 10: 314. doi:10.3389/fnhum.2016.00341.
- Charmaz, K. 2009. “Shifting the Grounds: Constructivist Grounded Theory Methods.” In Developing Grounded Theory: The Second Generation, edited by J. Morse, P. Stern, J. Corbin, B. Bowers, K. Charmaz and A. E. Clarke, 127–154. Walnut Creek: Left Coast Press.
- Corbin, J., and A. Strauss. 2008. “Basics of Qualitative Research.” Techniques and Procedures for Developing Grounded Theory. 3rd ed. London: SAGE.
- Dauman, N., S. I. Erlandsson, D. Albarracin, and R. Dauman. 2017. “Exploring Tinnitus-Induced Disablement by Persistent Frustration in Aging Individuals: A Grounded Theory Study.” Front Aging Neuroscience 9: 272. doi:10.3389/fnagi.2017.00272.
- De Jonckheere, M., and L. M. Vaughn. 2019. “ Semistructured Interviewing in Primary Care Research: A Balance of Relationship and Rigour.” Journal of Family Medicine & Community Health 7 (2): e000057. doi:10.1136/fmch-2018-000057.
- Fisher, A. J., and J. F. Boswell. 2016. “Enhancing the Personalization of Psychotherapy with Dynamic Assessment and Modeling.” Assessment 23 (4): 496–506. doi:10.1177/1073191116638735.
- Handscomb, L. 2006. “Use of Bedside Sound Generators by Patients with Tinnitus-Related Sleeping Difficulty: Which Sounds Are Preferred and Why.” Acta Oto-Laryngologica 126 (sup556): 59–63. doi:10.1080/03655230600895275.
- Henry, J. A., G. McMillan, S. Dann, K. Bennett, S. Griest, S. Theodoroff, S. P. Silverman, S. Whichard, and G. Saunders. 2017. “Tinnitus Management: Randomized Controlled Trial Comparing Extended-Wear Hearing Aids, Conventional Hearing Aids, and Combination Instruments.” Journal of the American Academy of Audiology 28 (6): 546–561. doi:10.3766/jaaa.16067.
- Hesser, H.,. M. Pereswetoff, C. E. Orath, and G. Andersson. 2009. “Consequences of Controlling Background Sounds: The Effect of Experiential Avoidance on Tinnitus Interference.” Rehabilitation Psychology 54 (4): 381–389. doi:10.1037/a0017565.
- Hoare, D. J., E. Broomhead, D. Stockdale, and V. Kennedy. 2015. “Equity and Person-Centeredness in Provision of Tinnitus Services in UK National Health Service Audiology Departments.” European Journal for Person Centered Healthcare 3 (3): 318–326. doi:10.5750/ejpch.v3i3.984.
- Horberg, U., L. L. Ozolins, and M. Ekebergh. 2011. “Intertwining Caring Science, Caring Practice and Caring Education from a Lifeworld Perspective- Two Contextual Examples.” International Journal of Qualitative Studies on Health and Well-Being 6 (4): 10363. doi:10.3402/qhw.v6i4.10363.
- Jastreboff, P. J., and M. M. Jastreboff. 2000. “Tinnitus Retraining Therapy (TRT) as a Method for Treatment of Tinnitus and Hyperacusis Patients.” Journal of the American Academy of Audiology 11 (3): 162–177. http://neuroagility.com/wp-content/uploads/Jastreboff2000-Tinnitus_retraining_therapy_TRT_as_a_method_for_treatment_and_hyperacusis_patients.pdf.
- Kochkin, Sergei, and R. S. Tyler. 2008. “Tinnitus Treatment and the Effectiveness of Hearing Aids: Hearing Care Professional Perceptions.” The Hearing Review 15 (13): 14–18. https://www.hearingreview.com/practice-building/practice-management/tinnitus-treatment-and-the-effectiveness-of-hearing-aids-hearing-care-professional-perceptions.
- Lane, R. D. 2014. “Is It Possible to Bridge the Biopsychosocial and Biomedical models?” BioPsychoSocial Medicine 8 (1): 3. doi:10.1186/1751-0759-8-3.
- Lee, K., K. Makino, and K. Yamahara. 2018. “Evaluation of Tinnitus Retraining Therapy for Patients with Normal Audiograms versus Patients with Hearing Loss.” Auris Nasus Larynx 45 (2): 215–221. doi:10.1016/j.anl.2017.03.009.
- Marks, E., P. Smith, and L. Mc Kenna. 2019. “Living with Tinnitus and the Health Care Journey: An Interpretative Phenomenological Analysis.” British Journal of Health Psychology 24 (2): 250–264. doi:10.1111/bjhp.12351.
- Medical Research Council. 2008. Developing and Evaluating Complex Interventions: New Guidance. MRC Health Services and Public Health Research Board and the MRC Population Health Sciences Research Network. doi:10.1136/bmj.a1655.
- Miles, M.,. Y. Chapman, and K. Francis. 2015. “Peeling the Onion: Understanding Others’ Lived Experience.” Contemporary Nurse 50 (2–3): 286–295. doi:10.1080/10376178.2015.1067571.
- Mills, I. J. 2017. “A Person-Centred Approach to Holistic Assessment.” Primary Dental Journal 6 (3): 18–23. doi:10.1308/205016817821931006.
- NICE 2020. Tinnitus: Assessment and Management Guidance. Accessed 10 June 2020. https://www.nice.org.uk/guidance/ng155.
- Pattyn, T., F. Van Den Eede, S. Vanneste, L. Cassiers, D. J. Veltman, P. Van De Heyning, and B. C. G. Sabbe. 2016. “Tinnitus and Anxiety Disorders: A Review.” Hearing Research 333: 255–265. doi:10.1016/j.heares.2015.08.014.
- Pedemonte, M., D. Drexler, S. Rodio, D. Geisinger, A. Bianco, D. Pol-Fernandes, and V. Bernhardt. 2010. “Tinnitus Treatment with Sound Stimulation During Sleep.” The International Tinnitus Journal 16 (1): 37–43.
- Pryce, H., and K. Chilvers. 2018. “Losing Silence, Gaining Acceptance: A Qualitative Exploration of the Role of Thoughts in Adult Patients with Subjective Tinnitus.” International Journal of Audiology 57 (11): 801–808. doi:10.1080/14992027.2018.1500041.
- Pryce, H., M. A. Durand, A. Hall, R. Shaw, B. A. Culhane, S. Swift, J. Straus, E. Marks, M. Ward, and K. Chilvers. 2018. “The Development of a Decision Aid for Tinnitus.” International Journal of Audiology 57 (9): 714–719. doi:10.1080/14992027.2018.1468093.
- Pryce, H., and R. L. Shaw. 2019. “Lifeworld Interpretation of Tinnitus.” Medical Humanities 45 (4): 428–433. doi:10.1136/medhum-2019-011665.
- Pryce, H., and D. Wainwright. 2008. “Help-Seeking for Medically Unexplained Hearing Difficulties: A Qualitative Study.” International Journal of Therapy and Rehabilitation 15 (8): 913–930. http://www.ijtr.co.uk/cgi-bin/go.pl/library/abstract.html?uid=30818.
- Searchfield, G. D., T. Linford, and M. Durai. 2019. “Sound Therapy and Aural Rehabilitation for Tinnitus: A Person Centred Therapy Framework Based on an Ecological Model of Tinnitus.” Disability and Rehabilitation 41 (16): 1966–1973. doi:10.1080/09638288.2018.1451928.
- Sereda, M., J. Xia, A. El Refaie, D. A. Hall, and D. J. Hoare. 2018. “Sound Therapy (Using Amplification Devices and/or Sound Generators) for Tinnitus in Adults.” Cochrane Database of Systematic Reviews (12). doi:10.1002/14651858.CD013094.pub2.
- Sierra, M., and A. S. David. 2011. “Depersonalization: A Selective Impairment of Self-Awareness.” Consciousness and Cognition 20 (1): 99–108. doi:10.1016/j.concog.2010.10.018.
- Teixeira, Adriane Ribeiro, Leticia Petersen Schmidt Rosito, Andréa Kruger Gonçalves, Michelle Gassen Paulo Nunes, Silvia Dornelles, and Maira Rozenfeld Olchik. 2017. “Tinnitus in Elderly Individuals: Discomfort and Impact in the Quality of Life.” International Archives of Otorhinolaryngology 21 (1): 66–71. doi:10.1055/s-0036-1572562.
- Todres, L., and K. Galvin. 2010. “Dwelling-Mobility: An Existential Theory of Well-Being.” International Journal of Qualitative Studies on Health and Well-Being 5 (3): 5444–5446. doi:10.3402/qhw.v5i3.5444.
- Tsakiris, M. 2010. “My Body in the Brain: A Neurocognitive Model of Body-Ownership.” Neuropsychologia 48 (3): 703–707 1. doi:10.1016/j.neuropsychologia.2009.09.034.
- Turkel, M. C., J. Watson, and J. Giovannoni. 2018. “Caring Science or Science of Caring.” Nursing Science Quarterly 31 (1): 66–71. doi:10.1177/0894318417741116.
- Tutaj, L., D. J. Haare, and M. Sereda. 2017. “Combined Amplification and Sound Generation for Tinnitus: A Scoping Review.” Ear Hear 39 (3): 412–422. doi:10.1097/AUD.0000000000000516.
- Tyler, R. S., C. Coelho, and W. Noble. 2006. “Tinnitus: Standard of Care, Personality Differences, Genetic Factors.” ORL; Journal for Oto-Rhino-Laryngology and Its Related Specialties 68 (1): 14–22. doi:10.1159/000090486.
- Tyler, Richard S., A. J. Keiner, Kurt Walker, Aniruddha K. Deshpande, Shelley Witt, Matthijs Killian, Helena Ji, et al. 2015. “A Series of Case Studies of Tinnitus Suppression with Mixed Background Stimuli in a Cochlear Implant.” American Journal of Audiology 24 (3): 398–410. doi:10.1044/2015_AJA-15-0005.
- Tyler, R., W. Noble, C. Coelho, and H. Ji. 2012. “Tinnitus Retraining Therapy: Mixing Point and Total Masking Are Equally Effective.” Ear and Hearing 33 (5): 588–594. 10.1097./AUD.0b013e31824f2a6e. doi:10.1097/AUD.0b013e31824f2a6e.
- Wegger, M., T. Ovesen, and D. G. Larsen. 2017. “Acoustic Coordinated Reset Neuromodulation: A Systematic Review of a Novel Therapy for Tinnitus.” Front Neural 8: 36. doi:10.3389/fneur.2017.00036.
- Wurzer, H., and C. Hauptmann. 2018. “Adapted Acoustic CR Neuromodulation in Patients with Chronic Tonal Tinnitus and Hearing Loss.” Frontiers in Medicine 5: 288. doi:10.3389/fmed.2018.00288.
- Zeman, F., M. Koller, B. Langguth, and M. Landgrebe. 2014. “ Which Tinnitus-Related Aspects Are Relevant for Quality of Life and Depression: Results from a Large International Multicentre Sample.” Health Qual Life Outcomes 12: 7. doi:10.1186/1477-7525-12-7.