
Abstract
Objectives
The risk of noise injury from recreational firearm use is well known. Despite preventive measures it is uncertain whether it has become less harmful. We assessed whether the association between recreational firearm use and hearing has changed during the last two decades.
Design
We used a repeated cross-sectional design and determined hearing thresholds by pure-tone audiometry. Frequency-specific associations between recreational firearm use and hearing thresholds were assessed by multivariate linear regression stratified by sex and adjusted for age and other covariates.
Study sample
Two cross-sectional population-based cohorts 20 years apart (1998 and 2018) comprised 27,580 (53% women, mean age 53 years) and 26,606 individuals (56% women, mean age 54 years), respectively.
Results
Recreational firearm use was reported by 28% in 1998 and 30% in 2018. The proportion that reported wearing hearing protection increased. Exposure to recreational firearms was associated with elevated thresholds at 3-6 kHz in both cohorts. The association increased with the number of lifetime shots. The associations increased by age and were substantially smaller in the most recent cohort.
Conclusions
Analyses of two cohorts revealed a reduction in the association between recreational firearm use and hearing over 20 years, coinciding with the introduction of hearing preservation measures.
Introduction
Impulse noise from firearms can cause serious, irreversible mechanical and metabolic damage to the cochlea, resulting in high-frequency hearing loss (Ylikoski Citation1987). The use of recreational firearms has been suggested to be the most important source of excessive noise outside the workplace (Clark and Bohne Citation1999) and is associated with hearing loss (Taylor and Williams Citation1966; Johnson and Riffle Citation1982; Prosser et al. Citation1988; Kryter Citation1991; Pekkarinen et al. Citation1993; Nondahl et al. Citation2000; Stewart et al. Citation2001; Marlenga et al. Citation2012; Hoffman et al. Citation2017).
The prevalence of hunting and sport shooting in the general population varies widely between countries. Exposure to firearms is highly prevalent, especially in the USA, where life-time exposure rates of 37% are reported for adults >18 years old (Bhatt et al. Citation2017) and a high prevalence of 18% among children <18 years old (Bhatt et al. Citation2020). Gunfire noise exposure (i.e. lifetime exposure exceeding a total of 10 rounds from a shotgun or military rifle, not counting a .22 rifle), was reported by approximately 3% of a population of young adults in England in both 1980 and 1994 (Smith et al. Citation2000). Hunting and sport shooting are relatively popular activities in Norway, with roughly 4% of the population paying hunting fees in 1997 (Statistics Norway Citation1998) and 2017 (Statistics Norway Citation2021). Four percent of the population registered as active shooters in the Norwegian Civilian Marksmanship Association in 1997, and 3% of the population registered in 2020 (DFS Citation2021).
The sound from a recreational firearm typically reaches peak sound pressure levels of 150-175 dB (Meinke et al. Citation2017), but protection by hearing protection devices (HPDs) such as earplugs and earmuffs is effective because of the relatively high-frequency content of the sound, with attenuation of up to 30 dB (Ylikoski et al. Citation1987; Dancer et al. Citation1992; Pääkkönen and Lehtomäki Citation2005). Double hearing protection (earplugs plus earmuffs) may add 15–20 dB of peak reduction (Murphy and Tubbs Citation2007). Protection may also be obtained by optimising the shooting environment and the type of ammunition, reducing the distance between shooters, and by using suppressors (Finan et al. Citation2017; Meinke et al. 2017; Murphy et al. Citation2018). There has been increased effort in regards to preventive measures, such as the use of HPDs becoming mandatory at all Norwegian shooting ranges. Therefore, updated studies are needed to assess the risk of recreational firearm use and hearing loss.
The present study was based on two large population-based cross-sectional hearing studies performed 20 years apart. The main objective was to assess whether recreational firearm use has become less harmful by assessing whether the association between recreational firearm use and hearing threshold has changed over the last 20 years.
Methods
Participants
The Trøndelag Health (HUNT) Study is a large general health-screening study for the entire adult population of Nord-Trøndelag County, Norway. It consists of four surveys conducted between 1984 and 2019 (Krokstad et al. Citation2013). We used data from two hearing surveys: HUNT2 Hearing (1996–1998) and HUNT4 Hearing (2017–2019).
HUNT2 Hearing included 17 of the 24 municipalities in the county. The participation rate was 63%, and a total of 51,529 persons attended. Valid audiometry and data from a questionnaire (HUNT2-Q1) that was distributed to all participants and returned at the site of the examination were available for 49,594 participants. A second questionnaire (HUNT2-Q2) was distributed to cases with a certain degree of hearing loss, as well as a control group, and returned by mail. Cases were individuals with at least one hearing threshold of 25 dB or more at 0.25–2 kHz or one age-adjusted threshold of 25 dB or more at 3–8 kHz in at least one ear. The present study included these participants. Valid audiometric and HUNT2-Q2 data were available for 27,580 adult respondents.
HUNT4 Hearing was carried out in the six larger municipalities, representing approximately two-thirds of Nord-Trøndelag County. The participation rate was 43%, and a total of 28,388 persons attended. Valid audiometry and data from a questionnaire (HUNT4-Q) that was distributed to all participants and returned at the site of the examination were available for 26,606 participants. The hearing studies are described in detail elsewhere (Engdahl et al. Citation2005; Engdahl et al. Citation2021).
The present study included a pooled cross-sectional sample of 54,186 observations from 47,340 subjects attending HUNT2 or HUNT4 Hearing (27,580 and 26,606 observations, respectively). The two cohorts will be referred to as the 1998 cohort and 2018 cohort.
Measurement
In addition to the questionnaires, both hearing studies included the same otoscopy and audiometric procedure. Pure-tone air-conduction hearing threshold levels were determined in accordance with ISO 8253-1, with fixed frequencies at eight test frequencies between 0.25–8 kHz using an automatic procedure with the ascending method. Hearing thresholds were defined relative to the hearing threshold levels of a population of otologically normal subjects aged 19–23 years (Engdahl, Strand, and Aarhus 2021; Strand et al. Citation2021).
Outcome measures
We determined the worst ear hearing thresholds at each frequency tested. The worst ear was chosen because firearms are known to result in asymmetric hearing loss affecting mostly the left ear (Chung et al. Citation1981). As secondary outcomes, we determined the left-right ear difference in hearing thresholds at the same frequency as the difference between the left and right hearing threshold (i.e. positive when the left ear is worse than the right ear) and asymmetric hearing thresholds as the absolute value of the ear side difference.
Exposure
HUNT2 included data on the number of shots, HUNT4 only included a yes/no measure. Accordingly, the analyses of the amount of use were restricted to the HUNT2 cohort. HUNT2-Q2 included questions on the duration of firearm use in years and the number of shots per year. In the analyses restricted to the 1998 cohort, we defined recreational firearm use as the lifetime number of shots, which was calculated as the number of years times the number of shots per year.
Exposure to firearms in hunting or sport or recreational shooting was determined from identical questions in HUNT2-Q2 and HUNT4-Q: “Have you ever been hunting?” “Have you been involved in sport or recreational shooting?” The possible answers in HUNT2 were “no” or “yes”, and in HUNT4 “no”, “don’t know”, or “yes”. “Don’t know” was coded as “yes” in HUNT4 (0.1% of hunting, 0.2% of sport shooting). Missing values on hunting or sport shooting were coded as “no” (2% of hunting, 5% sport shooting). We defined recreational firearm use as “yes” for participants who had either been hunting or been involved in sport or recreational shooting.
Each question was followed by a question on the use of hearing protection: “Did you use hearing protection? (never, sometimes, always)” on HUNT2-Q2; “Did you normally use hearing protection? (no, don’t know, yes)” on HUNT4-Q. Use of hearing protection was coded as “no” (“never” or “sometimes” in HUNT2 and “no” or “don’t know” in HUNT4) and “yes” (“always” in HUNT2 and “yes” in HUNT4).
Finally, impulse noise exposure in general was measured in HUNT2-Q1 by the following question: “Have you, more often than most people, been exposed to impulse noise (explosions, shooting etc.)? (no, yes, don’t know).”
Covariates
From similar questions in HUNT2 and HUNT4, we obtained estimates of risk factors for hearing loss: occupational noise (regularly been exposed to loud noise at your present or previous work [no/less than 5 hours/week, 5–15 hours/week, > 15 hours/week]); recurrent ear infections (no, maybe, yes), and hospitalisation for head injuries (no, maybe, yes). We treated missing values on any of these covariates as no exposure, which accounted for < 5% in each variable. We obtained information on education from national registers (primary school, secondary school, university < 4 years, university ≥ 4 years). All covariates were treated as continuous variables in the analyses.
Statistical analysis
We used Stata version 16.0. The effect of exposure to recreational firearm use was estimated by multivariate regression (mvreg in Stata) with each hearing threshold from 0.25–8 kHz serving as the dependent variables. The secondary analyses included left-right ear differences and asymmetric hearing thresholds as dependent variables.
First, we analysed the 1998 cohort, which included more details on the amount of firearm use. Firearm use was quantified as log10(lifetime number of shots + 1), where one unit corresponded to an increase in number of shots by a factor of 10. The analyses were stratified by sex. To assess whether the association depended on age, we included two-way interactions between the amount of recreational firearm use and age.
Second, to assess whether the association between firearm use (yes/no) and hearing was different in the two cohorts, we assessed associations in the pooled sample including two-way interactions between firearm use and cohort. By including a three-way interaction between firearm use, age, and cohort, we finally estimated whether the influence of age was different in the two cohorts. The number of exposed women was very low, female shooters tended to shoot much less than men, and the initial analyses in the HUNT2 cohort revealed no association between shooting and hearing threshold among women; therefore, we restricted the cohort analyses to men only. We also performed supplementary analyses on the impact of self-reported use of hearing protection.
All analyses were adjusted for other covariates. We predicted the average marginal effects from the interaction models with the margins command in Stata and 95% confidence intervals.
The relationship between age and hearing threshold is highly nonlinear. Therefore, age was modelled as a restricted cubic spline with five knots, which created a better model fit than simpler models with age as a linear variable at all tested frequencies (likelihood-ratio test, p < 0.001). Selecting fewer or more knots did not improve the fit. To account for dependency in the pooled data because of subjects participating in both surveys, cluster-robust standard errors were estimated using cluster bootstrapping with 1000 replications.
To account for possible selection bias caused by non-random selection of participants in the 1998 cohort, we used inverse probability weighting (IPW) (Cole and Hernán Citation2008). This methodology allowed us to correct the analysis by weighting the observations with the probability of being selected using information from the whole 1998 sample, including data from HUNT2-Q1. Variables included in predicting selection were age, sex, hearing thresholds at 0.25-8 kHz, all covariates mentioned above, and the impulse noise exposure in general from HUNT2-Q1. We then took the inverse of the predicted probability to attempt to account for potential selection bias. Finally, we performed sensitivity analyses using list-wise deletion instead of imputing missing responses as no exposure.
Results
The 1998 cohort included 27,580 participants (53% women) with a mean age of 53 years. The 2018 cohort included 26,606 participants (56% women) with a mean age of 54 years (). The proportion of participants who reported hunting increased from 23% in 1998 to 26% in 2018, whereas the number involved in sport shooting decreased from 17% to 14%. The reported overall use of recreational firearms (hunting or sport shooting) was 28% in 1998 and 30% in 2018. This number increased in women from 6% to 14%. The proportion reporting wearing hearing protection increased and was higher among younger subjects. Use of recreational firearms was more common among younger subjects and men in both cohorts. In 1998, 14% of men (13% in aged 20–44 years and 14% in aged 45 and older) and only 0.4% of women had shot more than 5000 rounds.
Table 1. Sample description.
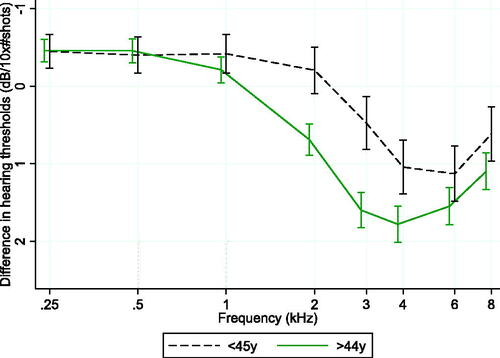
There was a highly significant overall association between firearm use quantified as lifetime number of shots and hearing threshold among men in the 1998 cohort (F(8, 12,211) = 54.6, p < 0.0001; , Supplementary Table 1). We found positive associations at single frequencies in the range 2–8 kHz, with the largest effect at 4 kHz (1.6 dB per 10-times increase in number of lifetime shots [95% CI, 1.4–1.8]). We found no associations among women (F(8, 14,254) = 1.33, p = 0.22). Due to the negative results and the low number of highly exposed women, we restricted further analyses to men. We identified a significant two-way interaction between the number of shots and age (F(32, 12,207) = 3.49, p < 0.0001), with stronger associations at older age and at 2 kHz ().
Figure 1. Hearing thresholds, firearm use, and sex. Regression coefficients are given in dB with 95% confidence intervals for log10(lifetime number of shots) as a function of sex, adjusted for age, education, occupational noise exposure, recurrent ear infections, and head injury. The regression coefficients represent mean differences in the worst ear hearing threshold for each increase in the number of lifetime shots by a factor of 10.
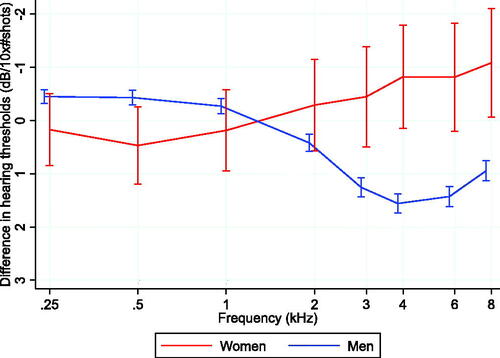
Figure 2. Hearing thresholds, firearm use, and age in men. Average marginal effects on the hearing threshold are given in dB with 95% confidence intervals for log10(lifetime number of shots) as a function of age in men, adjusted for education, occupational noise exposure, recurrent ear infections, and head injury. Average marginal effects represent mean differences in the worst ear hearing threshold for each increase in the number of lifetime shots by a factor of 10.
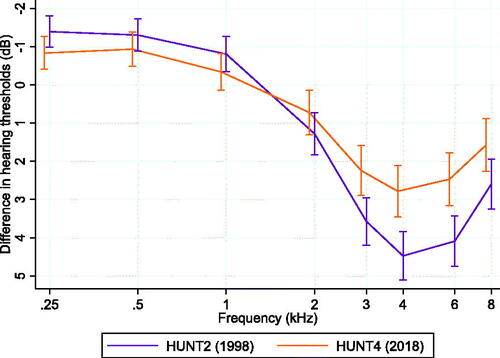
We estimated whether the associations between firearm use and the hearing threshold were different in the two cohorts by including a two-way interaction term between firearm use and cohort in the pooled sample, which was significant (F(8, 24,647) = 3.67, p < 0.0001). Positive associations were present at 2–8 kHz in both cohorts but significantly weaker in the more recent cohort at 3–6 kHz (, Supplementary Table 2). The effect at 4 kHz decreased from 4.5 dB (95% CI, 3.8–5.1) in 1998 to 2.8 dB (95% CI, 2.1–3.5) in 2018.
Figure 3. Hearing thresholds, firearm use, and cohort in men. Average marginal effects on the hearing threshold are given in dB with 95% confidence intervals for exposure to recreational firearm use as a function of cohort in men, adjusted for age, education, occupational noise exposure, recurrent ear infections, and head injury. Average marginal effects represent mean differences in the worst ear hearing threshold between exposed and non-exposed groups.
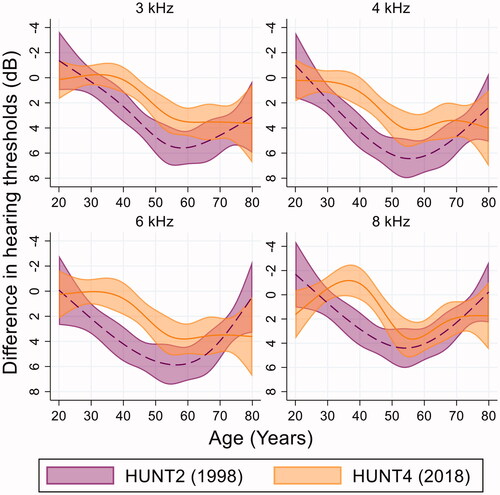
We found a significant three-way interaction between recreational firearm use, cohort, and age (F(32, 24,635) =1.53, p = 0.029; ). The age effect at 3–8 kHz was delayed in the 2018 cohort. Though the association started to increase already at the age of 20–30 years in 1998, there was little evidence of an association among subjects < 40 years old in 2018. Accordingly, the cohort effect increased with age up to 40–50 years, and then decreased in those > 50 years old. The association observed among 50-year-olds in 2018 was similar to the association observed among 35-year-olds in 2018. Thus, the cohort difference in 50-year-olds was of the same magnitude as an increase in age of 15 years in the 1998 cohort.
Figure 4. Hearing thresholds, firearm use, cohort, and age in men. Average marginal effects on the hearing threshold are given in dB with 95% confidence intervals for exposure to recreational firearm use as a function of cohort and age in men, adjusted for sex, education, occupational noise exposure, recurrent ear infections, and head injury. Average marginal effects represent mean differences in the worst ear hearing threshold between exposed and non-exposed groups.
To evaluate whether the cohort effect could be explained by an increase in self-reported use of HPDs, we estimated the interaction between recreational firearm use and cohort with and without controlling for self-reported use of HPDs. The interaction was reduced at 3, 4, 6, and 8 kHz, but by less than 0.4 dB. However, analyses restricted to the 1998 cohort revealed that HPD use was positively associated with the number of shots; non-users reported 1703 (95% CI, 205 to 3,202) fewer shots than users of HPDs.
The cohort effects were also analysed with the secondary outcomes asymmetric and left-right ear difference in hearing thresholds. The two-way interaction term between firearm use and cohort in the pooled sample was significant for the left-right ear difference (F(8, 24,618)=3.03, p = 0.002; Supplementary Table 3) but not for asymmetric hearing threshold (F(8, 24,618)=1.29, p = 0.241; Supplementary Table 4). The largest association between firearm use and left-right ear difference in hearing threshold was found at 6 kHz, at which the association was reduced from 2.0 dB (95% CI, 1.4–2.6) in 1998 to 0.8 dB (95% CI, 0.2–1.5) in 2018.
Finally, we performed regression analysis restricted to the 1998 sample with and without IPW for selection. The weighting reduced the observed effect estimates of recreational firearm use ≤ 0.3 dB. List-wise deletion resulted in effect estimates that differed no more than 0.2 dB from estimates when imputing missing responses as no exposure.
Discussion
Principal findings
Our study showed an association between recreational firearm use and hearing thresholds at 3–6 kHz in both 1998 and 2018. Analysis of the 1998 cohort showed that the association was dose-dependent, increasing by the number of lifetime shots. The association was weaker in the more recent cohort and stronger in older participants. Among older participants, the association expanded to 2 kHz. The influence of age on the association became less evident in the more recent cohort. Accordingly, the difference between the two cohorts depended on age, with the largest difference at 40–50 years old. In 50-year-olds, the 20-year cohort effect matched the effect of reducing age by 15 years. Finally, the association between firearm use and the left-right difference in the hearing threshold was weaker in the more recent cohort.
Comparison to other studies
In the present study, exposure to recreational firearms was associated with elevated hearing thresholds, mainly at 3–6 kHz, in both cohorts. In the 2018 cohort, the effect was approximately 3 dB at 4 kHz. Most studies of the effect of recreational firearm use on hearing are older (Taylor and Williams Citation1966; Johnson and Riffle Citation1982; Kryter Citation1991; Iki et al. Citation1993; Pekkarinen et al. 1993; Cruickshanks et al. Citation2000; Nondahl et al. 2000; Stewart, Konkle, and Simpson 2001; Konkle et al. Citation2001), with few studies representative of the last two decades. A longitudinal study followed a cohort of young workers for 16 years and found odds ratios (ORs) for any gun use of 3.1 (95% CI, 1.6 to 5.9) on high frequency hearing loss (3, 4, or 6 kHz) (Berg et al. Citation2012; Marlenga et al. 2012). A cross-sectional study of 202 Swedish hunters showed no effect of the number of reported rifle shots (protected and unprotected), but a small effect of 1 to 6 unprotected shots on high-frequency hearing loss (prevalence ratio, 1.5 [95% CI, 1.1 to 2.1]) (Honeth et al. Citation2015). Furthermore, a cross-sectional study based on the 2011-2012 cycle of the US National Health and Nutrition Examination Survey found high gunfire exposure (≥ 1000 lifetime firearm rounds) to be associated with hearing loss at speech frequencies (OR, 1.8 [95% CI, 1.1 to 3.0]) (Dobie et al. Citation2017; Hoffman et al. 2017).
To the best of our knowledge, this is the first study to show generational or cohort changes in the effect of recreational firearm use on hearing. There has been increased effort in regards to preventive measures. In 1987, a mandatory course was introduced in Norway for hunters that included education and training on using HPDs. In 1988, the regulations on the construction, control, and approval of civilian shooting ranges was introduced and the use of HPDs became mandatory at all civilian shooting ranges, though some efforts may have been introduced much earlier. The Norwegian Civilian Marksmanship Association (DFS) claims to have introduced mandatory use of HPDs at their shooting ranges already in the late 1960s. The introduction of electronic target systems at shooting ranges, which became the norm after 2005, has improved safety and reduced the likelihood of being exposed to noise. Since 1993, DFS has received annual funds earmarked for noise reduction measures at their firing ranges. Moreover, the use of suppressors has become more common. The use of suppressors became legal and freely available in Norway in 2008. The use of ammunition has probably not changed much since 1960, though indoor shooting with .22′' calibre has increased in the last few years. Most rifle shooting is with 6.5 × 55 mm or similar calibres. Shooting with a shotgun mostly uses 12 mm, though some use 20 mm and 16 mm. Norway has implemented regulations to limit workers’ exposure to loud sounds, with limits of 85 dB set in 1982. The generational improvement was found to be greatest in 50-year-olds. Assuming that hearing conservation measures became evident at the end of the 1980s, 60-year-olds in 2018 were then in their 20 s, whereas 60-year-olds in 1998 were in their 30 s and had already been shooting up to 20 years. We can only speculate, but we believe that the present observed cohort effect is related to these preventive measures. For example, some part of the cohort effect may reflect changes in the use of HPDs over time; participants who were born later are less exposed because of more widespread use of HPDs even though they report the same level of noise exposure.
The rate of HPD use while hunting was low in our study (38% in 2018) but comparable to a study of Swedish hunters in which 39% always, 21% often, and 19% never used HPDs while hunting (Honeth et al. 2015; Ström et al. Citation2015) and an American study reporting that 95% of hunters never wore HPDs while shooting in the past year (Nondahl et al. 2000; Cruickshanks et al. Citation2000). We registered an increase in self-reported use of HPDs that did not seem to fully explain the cohort effect. However, self-reported use of HPDs was positively associated with the amount of shooting; thus, it is plausible that increased shooting offset the positive effect of hearing protection. In addition, hearing impairment may affect the use of HPDs, so HPD use may act as a collider variable in the relationship between shooting and hearing loss. Conditioning on a collider may impose a non-causal association that further distorts the assessment.
The fact that the association between firearm use and the left-right ear difference was weaker in the in the more recent cohort, suggests that asymmetric exposure associated with the shooter’s own activity has been reduced. The shadow effect results in more exposure in the left ear among right-handed shooters.
Prior cross-sectional studies have suggested that the relationship between firearm use and hearing threshold is stronger among older subjects. Our finding, namely that the associations between exposure to firearm use and hearing threshold increased and expanded to lower-frequency hearing with higher age, confirms previous results from the 1998 cohort on impulse noise in general (Tambs et al. Citation2006). However, our analyses indicate that some of the increased effect observed among older participants in 1998 could be explained by a cohort effect, and that a 20-year cohort effect corresponded to a 15-year age effect. These findings indicate that the age effect found in the previous study also represents, to some extent, a cohort effect. However, we cannot confidently determine whether the interaction between age and firearm use in our most recent cohort represents actual age differences or a continued secular trend of better hearing protection. Regarding actual age differences, they could reflect that older subjects are more vulnerable to noise than younger subjects or that the effect of noise and age are super-additive, so that noise exposure accelerates age-related hearing loss. That older subjects are more vulnerable to noise than younger subjects is not very plausible (Ohlemiller et al. Citation2000). However, there is some evidence for the effect of noise exposure and age being super-additive (Gates et al. Citation2000; Kujawa and Liberman Citation2006; Xiong et al. Citation2014; WHO Citation2015), though others suggest it to be additive (Rosenhall Citation2003). Finally, we cannot exclude that some of the age difference is due to accumulated exposure, though we also found age differences in association with the number of lifetime shots.
Strength and limitations
The major strength of our study is the large sample size with cohorts separated by 20 years and the use of a standardised audiometric procedure with equal exposure measures in the two cohorts. We cannot fully reject the possible influences of selection bias. Most concerns apply to the 1998 cohort, which consisted of cases with a certain degree of hearing loss and a control group. The sample, however, was very large, containing more than half of the original population-based sample. By including a general question of impulse noise in the whole original sample, IPW indicated that the possible bias due to selection from the original sample was small. As with all studies using self-reported exposure, the results may have been affected by differential recall bias. However, it is not very likely that recall bias is frequency-specific or different in the two cohorts.
Conclusions
Cross-sectional analyses of two cohorts 20 years apart showed a reduction in the association between recreational firearm use and hearing. This reduction coincides with the introduction of hearing preservation measures in Norway. However, the size of the association is substantial and there is a need to further focus on preventive measures.
Ethical approval
The Regional Committees for Medical and Health Research Ethics approved the study (23178 HUNT hørsel). Only participants who provided written consent were included in the study.
Author contributions
Bo Engdahl: Investigation, Conceptualisation, Methodology, Data curation, Software, Formal analyses, Writing original draft.
Lisa Aarhus: Investigation, writing – review and editing
Supplemental Material
Download MS Word (27.7 KB)Acknowledgements
The Trøndelag Health Study (the HUNT Study) is a collaboration between the HUNT Research Center (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU)), Trøndelag County Council, Central Norway Regional Health Authority, and Norwegian Institute of Public Health. We also thank the HUNT4 Hearing team for their diligence.
Disclosure statement
Both authors declare no competing interests.
Data availability statement
Due to Norwegian legal restrictions and the current ethical approval for the study, data are not publicly available to share, but the research group can provide descriptive data in table form.
Additional information
Funding
References
- Bhatt, J. M., H. W. Lin, and N. Bhattacharyya. 2017. “Epidemiology of Firearm and Other Noise Exposures in the United States.” The Laryngoscope 127 (10): E340–E346. doi:10.1002/lary.26540.
- Bhatt, J. M., H. W. Lin, and N. Bhattacharyya. 2020. “Epidemiology and Gender Differences in Pediatric Recreational and Firearms Noise Exposure in the USA.” The Laryngoscope 130 (2): 541–545. doi:10.1002/lary.27958.
- Chung, D. Y., R. P. Gannon, G. N. Willson, and K. Mason. 1981. “Shooting, Sensorineural Hearing Loss, and Workers' Compensation.” Journal of Occupational Medicine 23 (7): 481–484. doi:10.1097/00043764-198107000-00015.
- Clark, W. W., and B. A. Bohne. 1999. “Effects of Noise on Hearing.” Journal of American Medical Association 281 (17): 1658–1659. doi:10.1001/jama.281.17.1658.
- Cole, S. R., and M. A. Hernán. 2008. “Constructing Inverse Probability Weights for Marginal Structural Models.” American Journal of Epidemiology 168 (6): 656–664. doi:10.1093/aje/kwn164.
- Dancer, A., P. Grateau, A. Cabanis, G. Barnabé, G. Cagnin, T. Vaillant, D. Lafont, et al. 1992. “Effectiveness of Earplugs in High-Intensity Impulse Noise.” The Journal of the Acoustical Society of America 91 (3): 1677–1689. doi:10.1121/1.402447.
- DFS. 2021. The Norwegian Civilian Marksmanship Association. https://www.dfs.no/om-dfs/english-dfs/. Accessed 11 March 2022.
- Engdahl, B., B. H. Strand, and L. Aarhus. 2021. “Better Hearing in Norway: A Comparison of Two HUNT Cohorts 20 Years Apart.” Ear and Hearing 42 (1): 42–52. doi:10.1097/AUD.0000000000000898.
- Engdahl, B., K. Tambs, H. M. Borchgrevink, and H. J. Hoffman. 2005. “Screened and Unscreened Hearing Threshold Levels for the Adult Population: Results from the Nord-Trøndelag Hearing Loss Study.” International Journal of Audiology 44 (4): 213–230. doi:10.1080/14992020500057731.
- Gates, G. A., P. Schmid, S. G. Kujawa, B. H. Nam, and R. D’Agostino. 2000. “Longitudinal Threshold Changes in Older Men with Audiometric Notches.” Hearing Research 141 (1-2): 220–228. doi:10.1016/S0378-5955(99)00223-3.
- Hoffman, H. J., R. A. Dobie, K. G. Losonczy, C. L. Themann, and G. A. Flamme. 2017. “Declining Prevalence of Hearing Loss in US Adults Aged 20–69 Years.” Journal of American Medical Association Otolaryngology-Head and Neck Surgery 143 (3): 274–285. doi:10.1001/jamaoto.2016.3527.
- Honeth, L., P. Ström, A. Ploner, D. Bagger-Sjöbäck, U. Rosenhall, and O. Nyrén. 2015. “Shooting History and Presence of High-Frequency Hearing Impairment in Swedish Hunters: A Cross-Sectional Internet-Based Observational Study.” Noise and Health 17 (78): 273–281. doi:10.4103/1463-1741.165043.
- Johnson, D. L., and C. Riffle. 1982. “Effects of Gunfire on Hearing Level for Selected Individuals of the Inter-Industry Noise Study.” The Journal of the Acoustical Society of America 72 (4): 1311–1314. doi:10.1121/1.388410.
- Krokstad, S., A. Langhammer, K. Hveem, T. Holmen, K. Midthjell, T. Stene, G. Bratberg, J. Heggland, and J. Holmen. 2013. “Cohort Profile: The HUNT Study, Norway.” International Journal of Epidemiology 42 (4): 968–977. doi:10.1093/ije/dys095.
- Kryter, K. D. 1991. “Hearing Loss from Gun and Railroad Noise-Relations with ISO Standard 1999.” The Journal of the Acoustical Society of America 90 (6): 3180–3195. doi:10.1121/1.401427.
- Kujawa, S. G., and M. C. Liberman. 2006. “Acceleration of Age-Related Hearing Loss by Early Noise Exposure: Evidence of a Misspent Youth.” The Journal of Neuroscience 26 (7): 2115–2123. doi:10.1523/JNEUROSCI.4985-05.2006.
- Marlenga, B., R. L. Berg, J. G. Linneman, D. J. Wood, S. R. Kirkhorn, and W. Pickett. 2012. “Determinants of Early-Stage Hearing Loss among a Cohort of Young Workers with 16-Year Follow-up.” Occupational and Environmental Medicine 69 (7): 479–484. doi:10.1136/oemed-2011-100464.
- Meinke, D. K., D. S. Finan, G. A. Flamme, W. J. Murphy, M. Stewart, J. E. Lankford, and S. Tasko. 2017. “Prevention of Noise-Induced Hearing Loss from Recreational Firearms.” Seminars in Hearing 38 (4): 267–281. doi:10.1055/s-0037-1606323.
- Murphy, W. J., G. A. Flamme, A. R. Campbell, E. L. Zechmann, S. M. Tasko, J. E. Lankford, D. K. Meinke, D. S. Finan, and M. Stewart. 2018. “The Reduction of Gunshot Noise and Auditory Risk through the Use of Firearm Suppressors and Low-Velocity Ammunition.” International Journal of Audiology 57 (1): S28–S41. doi:10.1080/14992027.2017.1407459.
- Murphy, W. J., and R. L. Tubbs. 2007. “Assessment of Noise Exposure for Indoor and Outdoor Firing Ranges.” Journal of Occupational and Environmental Hygiene 4 (9): 688–697. doi:10.1080/15459620701537390.
- Nondahl, D. M., K. J. Cruickshanks, T. L. Wiley, R. Klein, B. E. Klein, and T. S. Tweed. 2000. “Recreational Firearm Use and Hearing Loss.” Archives of Family Medicine 9 (4): 352–357. doi:10.1001/archfami.9.4.352.
- Ohlemiller, K. K., J. S. Wright, and A. F. Heidbreder. 2000. “Vulnerability to Noise-Induced Hearing Loss in 'Middle-Aged' and Young Adult Mice: A Dose-Response Approach in CBA, C57BL, and BALB Inbred Strains.” Hearing Research 149 (1–2): 239–247. doi:10.1016/S0378-5955(00)00191-X.
- Pääkkönen, R., and K. Lehtomäki. 2005. “Protection Efficiency of Hearing Protectors Against Military Noise from Handheld Weapons and Vehicles.” Noise and Health 7 (26): 11–20. doi:10.4103/1463-1741.31644.
- Pekkarinen, J., M. Iki, J. Starck, and I. Pyykkø. 1993. “Hearing Loss Risk from Exposure to Shooting Impulses in Workers Exposed to Occupational Noise.” British Journal of Audiology 27 (3): 175–182. doi:10.3109/03005369309076691.
- Prosser, S., M. C. Tartari, and E. Arslan. 1988. “Hearing Loss in Sports Hunters Exposed to Occupational Noise.” British Journal of Audiology 22 (2): 85–91. doi:10.3109/03005368809077802.
- Rosenhall, U. 2003. “The Influence of Ageing on Noise-Induced Hearing Loss.” Noise and Health 5 (20): 47–53.
- Smith, P. A., A. Davis, M. Ferguson, and M. E. Lutman. 2000. “The Prevalence and Type of Social Noise Exposure in Young Adults in England.” Noise and Health 2 (6): 41–56.
- Statistics Norway. 1998. Hunting Statistics 1997. Oslo-Kongsvinger: Statistics Norway, 1–59.
- Statistics Norway. 2021. 03440: Hunters, by Sex and Age (C) 2001–2002–2020–2021 Statbank. Oslo: Statistics Norway.
- Stewart, M., D. F. Konkle, and T. H. Simpson. 2001. “The Effect of Recreational Gunfire Noise on Hearing in Workers Exposed to Occupational Noise.” Ear, Nose, and Throat Journal 80 (1): 32–34. 36, 38-40. doi:10.1177/014556130108000109
- Tambs, K., H. J. Hoffman, H. M. Borchgrevink, J. Holmen, and B. Engdahl. 2006. “Hearing Loss Induced by Occupational and Impulse Noise: Results on Threshold Shifts by Frequencies, Age and Gender from the Nord-Trøndelag Hearing Loss Study.” International Journal of Audiology 45 (5): 309–317. doi:10.1080/14992020600582166.
- Taylor, G. D., and E. Williams. 1966. “Acoustic Trauma in the Sports Hunter.” The Laryngoscope 76 (5): 863–879. doi:10.1288/00005537-196605000-00005.
- World Health Organization. 2015. Hearing Loss Due to Recreational Exposure to Loud Sounds: A Review. Geneva: World Health Organization.
- Xiong, M., C. Yang, H. Lai, and J. Wang. 2014. “Impulse Noise Exposure in Early Adulthood Accelerates Age-Related Hearing Loss.” European Archives of Oto-Rhino-Laryngology 271 (6): 1351–1354. doi:10.1007/s00405-013-2622-x.
- Ylikoski, J. 1987. “Audiometric Configurations in Acute Acoustic Trauma Caused by Firearms.” Scandinavian Audiology 16 (3): 115–120. doi:10.3109/01050398709042165.
- Ylikoski, J., J. Pekkarinen, and J. Starck. 1987. “The Efficiency of Earmuffs Against Impulse Noise from Firearms.” Scandinavian Audiology 16 (2): 85–88. doi:10.3109/01050398709042160.