
Abstract
Objective
Despite previous research into the psychosocial impact of hearing loss, little detail is known regarding the hearing and hearing-aid-related emotional states experienced by adults with hearing loss in everyday life, and how they occur.
Design
Individual remote semi-structured interviews were audio-recorded, transcribed verbatim and qualitatively analysed with reflexive and inductive thematic analysis.
Study sample
Seventeen participants (9 female) with hearing loss (age range 44–74 years) participated. Ten used bilateral hearing aids, four unilateral and three used no hearing aids at the time of interviews.
Results
The four main themes which emerged from the data were: identity and self-image, autonomy and control, personality and dominant emotional states and situational cost/benefit analysis with respect to use of hearing aids.
Conclusions
This study goes beyond previous literature by providing a more detailed insight into emotions related to hearing and hearing-aids in adults. Hearing loss causes a multitude of negative emotions, while hearing aids generally reduce negative emotions and allow for more positive emotions. However, factors such as lifestyle, personality, situational control, the relationship with those in conversation and the attribution of blame are key to individual emotional experience. Clinical implications include the important role of social relationships in assessment and counselling.
Introduction
Positive and negative emotions are strongly linked to health status (Costa and McCrae Citation1980) and understanding such affect may be crucial to the optimisation of health interventions (Lee et al. Citation2008). People experience emotions almost continuously, resulting from, and in turn influencing, daily-life situations (Oatley and Duncan Citation1994). Emotions are “instinctive or intuitive feelings deriving from one’s circumstances, mood or relationships” (OED online 2021), as distinct from moods, which are non-specific, slow acting and exist on a positive to negative scale (Beedie, Terry, and Lane Citation2005). Emotions are integral to the experience of everyday life and satisfaction with one’s life situation (Bastian et al. Citation2014). Similarly, satisfaction with health interventions is guided by emotions (Linssen et al. Citation2013). This could influence factors such as the uptake or continuation of treatment, which have obvious implications for health and well-being. For adults with hearing loss, the emotional effects of their hearing loss and hearing-aid use are of personal and clinical importance.
Previous literature has identified a predominantly negative impact of hearing loss on emotions (Heffernan et al. Citation2016; Holman et al. Citation2019). Hearing loss is related to reduced emotional vitality (the capacity to effectively regulate emotions) which leaves people at increased risk of negative emotions in challenging situations (Contrera et al. Citation2016). Difficulty communicating has been described as resulting in frustration and irritation during conversations (Bennett et al. Citation2022; Heffernan et al. Citation2016). Hearing loss has also been linked to increased feelings of fatigue (Holman, Drummond, and Naylor Citation2021a). While additional listening effort caused by reduced audibility can cause fatigue, negative emotions such as frustration and reduced motivation to engage in listening situations can increase fatigue (Holman et al. Citation2019).
As hearing loss is more prevalent in older people, there is a societal stigma that some people attach to having a hearing loss (Wallhagen Citation2010). The perception of being “old” or “faulty” leads some people to experience emotions such as embarrassment or anxiety (Wallhagen Citation2010). The development of hearing loss threatens social identity (Hétu Citation1996). Individuals who are not comfortable with their social identity have a more person-based or internal locus of identity, meaning that stigmatising behaviour is reflected against oneself rather than the group (Dovidio et al. Citation2000). Social isolation is strongly linked with hearing loss, presumably due to difficulties in communication settings, and it naturally follows that loneliness is more common in adults with hearing loss (Bennett et al. Citation2022; Shukla et al. Citation2020). The impact of hearing loss on relationships can result in negative emotions for both the person with hearing loss and their communication partners (Manchaiah, Stephens, and Lunner Citation2013).
The numerous negative emotions that have been linked to hearing loss can often be viewed as transient and related to specific instances of difficulty. However, there are some emotions which persist and can become mental health concerns such as depression and anxiety. Depression can be viewed as a variable emotional state or as a stable personality trait diagnosable by health professionals (Krohne et al. Citation2002). In older adults, hearing loss is associated with 1.47 greater odds of depression, identified through a meta-analysis of studies of depressive symptoms as well as scales giving thresholds for “diagnosis” (Lawrence et al. Citation2020). Anxiety can also be classified as either trait (enduring predisposition to react to situations in a consistent manner) or state (cognitive or emotional reactions to situational factors), sometimes referred to as clinical and sub-clinical respectively. Hearing loss is linked to increased levels of both state and trait anxiety (Jayakody et al. Citation2018).
Most research regarding hearing-aid fitting has identified at least some positive emotional change relative to the unaided state, usually in the collective form of emotional or psychosocial well-being (Contrera et al. Citation2016). Beyond the experience of emotions in everyday situations, hearing aids have been shown to improve depressive symptoms (Marques, Marques, and Miguéis Citation2022). However, adults with hearing loss also report negative feelings towards the hearing aids themselves (Heffernan et al. Citation2016; Stark and Hickson Citation2004). Most research investigating the stigma associated with hearing loss has focused on hearing aid use (Ruusuvuori et al. Citation2021). The stigma associated with hearing aids and physical irritation can both lead to underuse or a refusal to wear hearing aids (McCormack and Fortnum Citation2013). There is also a greater chance of negative emotions immediately following hearing-aid fitting due to the multifactorial process of getting used to hearing aids with practical difficulties and psychosocial challenges (Dawes, Maslin, and Munro Citation2014).
While the topic of emotions regularly arises in discussions of the psychosocial impact of hearing loss, comparatively little detail is known regarding the hearing and hearing-aid related emotional states experienced by adults with hearing loss, and how they occur. A better understanding of the specific causes of positive and negative emotional reactions to hearing-dependent situations and hearing devices would assist future attempts to improve clinical assessment and counselling, as well as improving the targeting of interventions and the setting of expectations. The overall goal of this study was to qualitatively assess hearing and hearing-aid related emotional states experienced by adults with hearing loss. To address this goal, the present study aimed to address three research questions:
What hearing-related emotions are experienced by adults with hearing loss in everyday life, and how do they occur?
What impact does hearing-aid use have on emotion in the hearing-aid wearer?
To what extent does the experience of hearing-related emotions vary between adults with hearing loss?
Method
Design
A phenomenological qualitative methodology was followed. This methodology allows for the focused study of individuals’ lived experiences relating to a specific phenomenon. This methodology was chosen as it facilitates the investigation of the phenomenon of emotions in adults with hearing loss in great detail (Creswell Citation2013) and closely informed the entirety of the study. Semi-structured interviewing was chosen as the most appropriate method to explore the phenomena being researched in a focused manner. In contrast to unstructured interviews, this involves a set of pre-determined questions in a topic guide that the interviewer poses to participants in interviews, while (in contrast to structured interviews) providing participants some flexibility to discuss concepts and experiences they consider relevant to them, which the researcher may not have anticipated or included in the interview topic guide beforehand. Interviews took place remotely in August 2020 due to social distancing restrictions imposed by the UK government at the time. Participants were offered a choice between interviews via telephone, video call or written questions and answers. Remote communication has been identified as an effective means of conducting semi-structured interviews (Cachia and Millward Citation2011). One participant opted for video call, one for written questions and the rest for telephone calls. Participants were asked to sit in a quiet room with no distractions for the interview. Before the interview there was a brief conversation to confirm that the participant was fully aware of what to expect. Participants were informed at the recruitment stage and again at the beginning of the interview that the study was investigating hearing and hearing-aid related emotions in daily-life. An interview question guide was used to ensure coverage of all relevant question areas. All interviews were conducted by author JH (a male postdoctoral researcher). Brief field notes were taken during the interviews to further inform stage 1 of the analysis process. Telephone and video calls were conducted using Skype (a telecommunications application used for videotelephony, videoconferencing and voice calls). Interview audio was recorded using the software MP3 Skype Recorder 6.1 (https://voipcallrecording.com). Interviews were transcribed verbatim by an external transcription service. The interviews ranged from 29 to 71 minutes (mean 42.5). The study was designed in collaboration with the Hearing Sciences – Scottish Section patient and public involvement group.
Participants and recruitment
Participants were 17 adults (>18 years old) with hearing loss who had previously reported to NHS audiology across Glasgow with hearing problems. Participants consented to taking part in research and were subsequently recruited from the participant database of University of Nottingham Hearing Sciences – Scottish Section. Participants were contacted via email and therefore needed to have an email address. The participants were recruited using stratified purposeful sampling which involves sampling based on key variables within the initial major variable sample (Palinkas et al. Citation2015). This allows the potentially differing experiences of individuals to be revealed. Key variables considered during sampling were hearing-aid status, degree of hearing loss, age and gender. The aim was to include participants of a roughly equal gender split, with a range of ages, severity of hearing loss and hearing-aid status, that is, unilateral, bilateral or no hearing aid. Variables were known to the researchers prior to invitation but were confirmed during interview. Prior to study commencement, a minimum sample of 14 participants was established based on previous experience and the ability to successfully undertake stratified purposeful sampling. To establish a pragmatic stopping point for participant sample size, inductive thematic sufficiency (Saunders et al. Citation2018) was utilised, whereby the number of codes is scrutinised subjectively during concurrent data collection and analysis. No invited participants who replied subsequently dropped out. The demographic information of participants can be found in . This study was approved by the West of Scotland Research Ethics Committee (18/WS/0007). All participants provided informed consent which was recorded online.
Table 1. Participant demographic information.
Interview question guide
The question guide was designed to elicit information relevant for answering the three main research questions, as well as other potentially relevant topics such as the coordination of emotion between self and others, and the impact of COVID-19 restrictions on daily-life emotions. The question guide was developed by authors JH and GN and was piloted on two participants. After piloting it was deemed that the guide did not need to be altered, so the results from the two pilot participants were included for analysis.
The question guide began with introductory questions regarding the participants’ history of hearing loss and the associated emotions, and the impact of COVID-19 restrictions on emotions experienced in daily-life situations. These questions allowed the participant to get used to talking about emotion. In order to cover as many aspects of daily life as possible, the main questions were broken down into different types of daily-life activities (i.e. social, leisure, work, daily chores). Participants were asked to explain what they do for each type of activity, both currently and when there were no social restrictions in place. Prompts were used to cover specific situations, experienced emotions and the role of hearing loss and hearing-aid use. If applicable, participants were asked about their feelings towards their hearing aid(s). Coordination of emotion was investigated by asking how well participants can successfully express emotions and understand the emotions of others. Participants were then asked to list any discrete emotions they experience in everyday listening situations, when they think of their hearing and when they think of their hearing aid(s). The aim was to graphically depict the spectrum of hearing and hearing-aid related emotions experienced. The interview concluded with a rundown of their responses and a debrief, providing participants with an opportunity to expand on previous responses or give new responses which they had missed. The full question guide is available in supplementary digital content 1.
Analysis
Anonymised transcripts were imported into NVIVO 12 software (QSR International, Melbourne, Australia) and subjected to inductive reflexive thematic analysis. Inductive reflexive thematic analysis was established as the best way of examining the lived experience of individuals via analysis grounded in the data, not explicitly theory-led, whilst being aware of the researchers’ role in the subjective aspects of analysis (Braun and Clarke Citation2022). Thematic analysis comprises of six stages designed to identify important themes that are generated from the data (Braun and Clarke Citation2006). The stages are an iterative process which involves repeating previous steps in order to generate themes. The initial stages of analysis were undertaken concurrently with interviews. Once the minimum of 14 participants had been interviewed, after each subsequent interview a decision on inductive thematic sufficiency was undertaken by authors JH and GN. Authors JH and YA, who have relevant qualitative research training and previous experience with thematic analysis in populations with hearing loss, independently analysed the completed transcripts from familiarisation with the data by reading through the interview transcripts (stage 1) to defining and naming themes (stage 5). The researchers highlighted meaning units (word, phrase, sentence or paragraph) and manually coded them. Both semantic and latent codes were generated as appropriate. Searching for themes and reviewing of those themes took place iteratively alongside the coding. The authors then compared their results and discussed how best to come to conclusions on final results. Coding quality comes from the depth of engagement with the data, and situated, reflexive interpretation rather than consensus between coders (Braun and Clarke Citation2022). This was considered during discussions. Once there was agreement on results, the thematic analysis final report of themes and sub-themes was created with the input of author GN. This study used the Consolidated Criteria for Reporting Qualitative Research (COREQ) (COREQ checklist in Supplementary digital content 2). COREQ is a 32-item checklist designed to enhance the explicit, comprehensive and transparent reporting of qualitative studies (Tong, Sainsbury, and Craig Citation2007).
Results
Discrete emotions
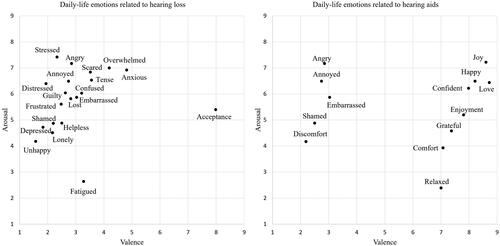
Participants mentioned many hearing-related emotions in everyday life, which, naturally enough, ranged from joy to sadness depending on the activity. However, when considering the role of hearing loss in listening situations the emotions were decidedly negative. Likewise, hearing aids were involved in a wide range of emotions, but with a predominantly positive emotional impact. Discrete emotions expressed by participants regarding their hearing loss and their hearing aids respectively are plotted on valence (pleasantness or unpleasantness)/arousal (intensity from calm to exciting) graphs in . The valence/arousal scale scores are taken from the Affective Norms for English Words (ANEW; Bradley and Lang Citation1999). These norms were created by participants scoring their impression of where words should lie on scales, rather than their impression of what it would feel like to experience a given emotion. However, this provides an impression of the nature and strength of the experienced emotions. is not an exhaustive list of the discrete emotions expressed by our participants, as only those words present in ANEW (or those with very close synonyms) could be plotted. Where two emotions were deemed to be interchangeable (e.g. angry and enraged), only one was plotted.
Figure 1. Graphical depiction of discrete emotions related to hearing loss and hearing aid(s) expressed by participants, on a valence/arousal scale (Bradley and Lang Citation1999). Valence: 1 = negative, 5 = neutral, 9 = positive. Arousal: 1 = low, 9 = high.
Themes
Following thematic analysis four major themes were generated:
A: Identity and self-image
B: Autonomy and control
C: Personality and dominant emotional states
D: Situational cost/benefit analysis with respect to use of hearing aids
A fifth theme was established listing additional information about emotion that was specifically sought but does not directly relate to the research questions. illustrates the five themes and eighteen sub-themes that arose from the analysis.
Figure 2. Thematic analysis results: Main themes and subthemes. See supplementary digital content 3 for the full results table, including a full description and a relevant quotation for each main theme and subtheme.
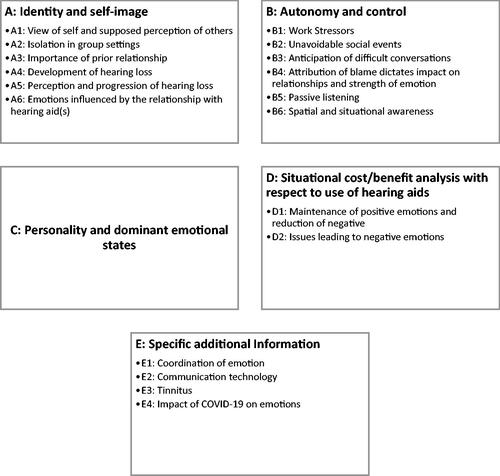
See supplementary digital content 3 for the full results table, including a full description and a relevant quotation for each main theme and subtheme.
A: Identity and self-image
Participants described how their own view of themselves, as well as their suppositions about how others might see them, led to many different negative emotions (subtheme A1). Self-stigma played a role in the negative view of oneself: “It makes me feel…a bit stupid” (p08). The view of oneself is linked to sense of identity, whether that be as a person with hearing loss, part of the hearing loss community, or part of normal social circles. Negative self-image (exemplified by feelings of embarrassment, sadness and anxiety) and concern for one’s place in a social group or setting (characterised by a wish not to annoy the conversation partner or seem stupid or old) were demonstrated by participants who felt that pretending that they were following a conversation was preferable to interjecting for clarifications: “They think you're a bit daft if you ask them to repeat things” (P01). Trouble identifying themselves as a person with hearing loss in the context of their social groups caused reluctance to be open with others: “It impacted on my relationships…caused me to feel ignored, isolated, unsupported” (P15). This caused feelings of conflict, shame, self-consciousness, poorer self-worth, feeling faulty, and of wanting to replace this with feeling “normal”. This view was expressed even when the participant knew that others would not view them in that way. P01 said: “That's my perception, I know it’s not true but that’s my perception of it”.
The difficulties in conversation caused by hearing loss led to emotional and social disconnection and widespread feelings of sadness, depression, loneliness and isolation (A2): “I can’t hear…and I feel a bit lonely” (P16). Participants felt that they were not an important part of the group, which resulted in them being “a bit uncomfortable” and disliking certain social scenarios. Nodding along whilst feeling bad was a common experience. Identity turmoil left people feeling different and that “emotionally, I started losing contact with people” (P14). An important characteristic influencing the emotions experienced in challenging conversations was the relationship to the others in the conversation (A3). Participants described conversations with family and close friends as more relaxed, comfortable and enjoyable than conversations with less familiar people. Being open and comfortable with one’s hearing loss allowed participants to identify both as part of the group and as a person with hearing loss, meaning participants not only spoke up more but accepted humour in connection with their hearing difficulties: “they’re sort of slagging me off… but it’s just a laugh we have” (P12). With less close contacts, participants described greater likelihood of feeling nervous, embarrassed, frustrated, annoyed and angry. P01 said: “I probably wouldn’t ask for clarification or repetition if it was a social group. That depends on how close you are”. Self-identity could play a role as being able to identify as a key part of a family group after a change is less problematic than identifying as a key part of other social groups. The difference in emotions felt when conversing with close versus distant contacts was also expressed by some participants regarding telephone conversations. When receiving calls from unknown contacts, people expressed anxiety at the greater likelihood of misunderstanding.
The development of hearing loss was heavily linked to the self-identity of the participant, which in turn influenced emotion (A4) (see supplementary digital content 4 for individual participant details). Those who experienced hearing loss from an early age described more acceptance than others, leading to less disruptive negative emotions: “I didn’t know any different” (P11). Participants who experienced progressive hearing loss expressed a mixture of hearing-related emotions in daily-life including surprise at the diagnosis and some level of acceptance. Participants who experienced sudden onset hearing loss described this as having caused major disruption to their daily lives, which in turn resulted in very negative emotions. Such disruption to daily life included problems with responsibilities and relationships at work which caused shock, frustration, anger, disbelief and embarrassment. P10 explained: “There is a sudden awareness of how it impacted on my daily life… My boss was not very sympathetic… I was very very frightened… I lost my confidence and I lost my self-worth”. Identifying as a person with hearing loss or part of the hearing loss community is simpler from an earlier age, allowing for a more positive self-image and seems beneficial in avoiding negative emotion.
The perception of one’s hearing loss and thoughts on its progression related to a settled or unsettled sense of identity (A5). In general, hearing loss was an overwhelmingly negative aspect of lives eliciting hearing-related emotions such as worry, annoyance, disappointment, embarrassment, frustration and anxiety. However, some participants did describe an acceptance of their hearing loss which may be linked to a settled identity and positive self-image: “It’s just how it is” (P11). Some anxiety and worry about the future progression of their hearing loss was linked to not fully identifying as a person with hearing loss, as people didn’t want to become “deaf-deaf” (p06).
The relationship with hearing aid(s) was shown to influence emotions (A6). Most participants acknowledged that their hearing aids are a force for good and make their lives more positive emotionally, and less negative. Participants variously regarded hearing aids as entirely positive and essential, useful in specific situations or a reassuring backup: “That’s exactly it… I don’t feel comfortable without them” (P14). The relationship with hearing aids is strongly linked to self-image (including stigma): “angry, annoyed…they’re so visible” (P06), and identity (through acceptance): “I just love my hearing aids… It was not always like that… At odds with them and being angry with them…I did not want to accept them. Once I had accepted them, I now would be lost without them” (P10). Perceived deficits, or inability of the hearing aids to improve a situation caused some participants to feel frustration but no negativity towards the hearing aids, while others developed a love/hate relationship with them. For some, the relationship was influenced by comparisons with previously owned hearing aids, or by the initial period of adjustment following hearing aid fitting causing the greatest negative emotional impact.
B: Autonomy and control
Participants described many different types of situations where their hearing loss played a role. The participants’ freedom of choice and control over listening situations influenced the emotions experienced. The workplace was commonly listed as a place where a hearing loss negatively impacted emotion (B1). Participants generally had little control over workplace listening scenarios: “end up getting pushed into some space that I don’t want to sit in” (P05), and these often high-stress, formal conversations required coping strategies, that were often hindered, to deal with feelings of frustration, annoyance, fatigue, anxiety, guilt, anger, stress and dejection: “if you’re deaf you’re never late for meetings…guess where [the chairperson] is going to sit” (P05). Similar issues were expressed by participants with respect to unavoidable non-work events (e.g. weddings) that afford little control over the listening situation and limited chances for the utilisation of coping strategies (B2): “It comes down to control and if I can adapt great, if I can’t that’s when the frustration and the problems kick in” (P11).
Negative emotions were caused not just by struggling in listening situations, but also by the prospect of upcoming difficult listening situations in work or social events (B3): “I would effectively not enjoy the dining out experience because I can’t hear whilst I’m there and I get perhaps perplexed that there is some level of concern before you get there” (P11). Knowing a difficult conversation is likely to occur could cause anxiety, worry and trepidation, particularly when coping strategies would be hard to implement.
Control was also a factor which influenced the experienced emotions when conversations broke down (B4). When the participant attributed blame to themselves, emotions were muted and less strong, with no impact on relationships. However, when the participant attributed blame to another person (e.g. for not speaking clearly or for facing the wrong way) the emotions experienced were much stronger, and the relationship was damaged, even if only in a minor way: “If it’s somebody thoroughly obnoxious you can be very annoyed with them” (P05). Participants expressed feelings of frustration, anger and resentment because they felt that the conversation partner had a choice (control) over how they engaged in the conversation: “For being so selfish” (P05). While most participants explained that emotions were more positive when in familiar company (A3), some negative emotions arose due to a progressive breakdown in relationships. The hearing loss could act as a trigger for arguments as both parties blamed the other for not trying hard enough to aid communication. The impacted relationship could lead to more frequent arguments and negative emotions: “He can get frustrated. He often forgets that I need to see him…that can lead to difficulties” (P02).
People usually have very little control over the sound environment, particularly when out of the home. Participants expressed frustration at being unable to hear sounds such as announcements because of background noise, and higher arousal emotions when outside due to not being aware of their surroundings (B6): “I get anxious when I’m by myself because I don’t really hear people behind me, and you get a wee bit jumpy and agitated like that sometimes as well, it makes me uncomfortable” (P04).
Passive listening situations such as listening to music, watching the television and going to the cinema involve a high degree of choice and control (B5). Participants described many different coping strategies, techniques and tools (including hearing aids) which allow them to listen successfully, resulting in happiness and enjoyment. When coping strategies were disrupted, such as the failure of a hearing loop system, there was a reduction in positive emotions as well as more negative emotions: “It feels like a waste of time, I feel switched off, isolated” (P16).
C: Personality and dominant emotional states
The interviews did not include deliberate assessment of personality types. However, a few comments by participants offered useful insight into the potential influence of personality on emotion. Participants who reported perfectionism-type traits during the interviews like wanting situations or oneself to be “just right” seemed to experience more negative hearing-related emotions, such as stress, annoyance and anger. Participants who explicitly identified themselves as introverts or ‘homebody’ types, or reported their social lives as being uneventful and with most activities centred around the home, reported fewer negative impacts of hearing loss and COVID-19 social restrictions: “I haven’t had to deal with the outside world, so I am OK with it…I’m quite an introvert” (P02). Several participants reported struggling to find words to describe emotions, particularly at the beginning of interviews, but one male participant reported difficulty with emotion entirely: “I’ve been surprised mainly that I’ve spoke of this stuff I’ve never spoke about to anybody, not that I’ve hidden it, but I’ve not had cause, don’t do emotions” (P04). This is in keeping with the, possibly outdated, stereotype that men are less in touch with their emotions than women. On the other hand, several other male participants had no problems with emotional introspection.
D: Situational cost/benefit analysis with respect to use of hearing aids
Participants described how they would weigh up the positives and negatives of wearing their hearing aids in different situations, sometimes consciously, sometimes unconsciously: “You have learnt the environments where it is going to benefit you and the environments it is not” (P11). Hearing aids were widely described as allowing for more positive emotions (enjoyment, happiness, comfort, relaxation) and reducing the frequency and strength of negative emotions (annoyance, effort/strain, worry, frustration) (D1). However, hearing aids were also the cause of negative emotions for some participants (D2). The supposed impressions of others caused some embarrassment due particularly to the visibility of the hearing aids: “I’m not going to feel happy wearing these, I’ll be so self-conscious” (P02). Hearing aids also caused some annoyance and frustration due to physical irritation and interference with sound quality: “It was annoying me because it was kind of echoey” (P07).
E: Specific additional information
E1: Coordination of emotion
Participants were asked about how well they can successfully portray their emotions to others, as well as how successfully they can understand the emotions of others in conversation. All participants apart from one reported no problem expressing their emotions verbally. One participant had problems with this because of a speech disorder. Some participants explained that they have trouble understanding the emotions portrayed verbally by others. Where this was expressed, a common strategy was to look at facial and body cues, rather than relying on auditory cues.
E2: Communication technology
Phone and video calls could be enjoyed and dreaded. Participants had varying levels of comfort with both. The enjoyment (or not) of phone and video calls was based on the participant’s conversational ability in the given situation, and on the context and the complexity of the conversation (i.e. work or pleasure, number of conversation partners). Hearing loops were described as helpful but very often not working. This, in addition to the unhelpfulness of others in resolving issues, was described as frustrating.
E3: Tinnitus
Participants who mentioned that they have tinnitus stated that it often has a negative impact on their emotions (frustration, annoyance). For some, tinnitus interfered with sleep which on occasion would result in feelings of fatigue. Some participants expressed an acceptance of their tinnitus, and that it did not impact their emotions greatly.
E4: COVID-19 restrictions
COVID-19 lockdown restrictions did not seem to have much impact on the hearing-related emotions of participants. Many found that their life was not that different, and that they were in fact less often in challenging listening scenarios or were wearing their hearing aids less during lockdown. Situations with people wearing face masks were described as harder and more frustrating and worrying than mask-less conversations.
Discussion
This study addressed in detail the hearing and hearing-aid related emotional states experienced by adults with a hearing loss. The three main research questions were: (1) what hearing-related emotions are experienced by adults with hearing loss in everyday life, and how do they occur? (2) What impact does hearing-aid use have on emotion in the wearer? (3) To what extent does the experience of hearing-related emotions vary between adults with hearing loss? In this study we found that:
Adults with hearing loss experience the full spectrum of emotion in daily-life listening situations. Hearing loss, via personal factors such as identity or situational factors such as control, causes a multitude of negative hearing-related emotions such as annoyance, worry, frustration, loneliness, anger, guilt, fatigue and embarrassment.
Hearing-aid use in general reduces the negative emotions caused by hearing loss (e.g. worry, frustration, annoyance) and allows for the experience of more positive emotions (e.g. enjoyment, happiness, relaxation). Hearing-aid use can also result in negative emotions (e.g. irritation, frustration) due to the perceived deficiencies and limitations of the hearing aids.
The experience of hearing-related emotions varies greatly between participants, as factors such as the development of hearing loss, personality, relationship with hearing aid, coping strategy use, sense of identity and numerous situation-specific aspects can influence the experienced emotion. However, feelings of frustration, anxiety and isolation were expressed by almost all participants.
demonstrates that discrete hearing loss-related daily-life emotions are numerous and of varying intensity (arousal) but are principally negative. Only feelings of acceptance could be considered as positive. Heffernan et al. (Citation2016) identified that “muted emotions” such as acceptance in reaction to hearing loss were linked to gradual hearing loss. Similarly, this study identified more acceptance in those with gradual hearing loss compared to sudden-onset hearing loss in adulthood, however participants who experienced hearing loss onset in childhood exhibited the most positive relationships with their hearing loss and the most prominent feelings of acceptance. The results from this study support findings from previous research that adults with hearing loss can suffer from negative self-image (Bennett et al. Citation2022) and overt or perceived stigma which leads to feelings of embarrassment and impaired sense of identity (Wallhagen Citation2010). This in turn can lead to withdrawal from social situations, loneliness and social isolation (Bennett et al. Citation2022; Bott and Saunders Citation2021; Heffernan et al. Citation2016). Here, we identified that an individual’s sense of identity, settled or conflicted, could play a key role in the emotions experienced in everyday life. We found that the supposed impression of others can cause negative emotions and behaviours, even when the person knows that it is not a belief held by their conversation partner, suggesting self-stigma may play an important role. Adults who are not comfortable with their social identity are more likely to reflect stigmatising behaviour against themselves rather than the group (Dovidio et al. Citation2000). Additionally, the relationship between those involved in the conversation can have a large impact on the development of negative or positive emotions (closer contacts related to preferred emotions). Social connectedness, the experience of belonging to a network or relationship, (Lee and Robbins Citation1995) is related to identity and may play a role. Group ties enhance shared social identification, in turn providing effective social support and improving health more than interpersonal ties (Haslam et al. Citation2016), and hearing loss is linked to feelings of disconnection from an individual’s social network (Galloway et al. Citation2019).
Perfectionism-type traits were associated with more negative hearing-related emotions. This is supported by previous literature which links self-oriented perfectionism with greater negative affect following failure experiences (Besser, Flett, and Hewitt Citation2004). Participants who described themselves as introverted or who preferred to stay at home described comparatively fewer negative effects of hearing loss on emotions. This is to be expected as listening situations at home would be less varied and challenging. One male in the study reported struggling to access their emotions. Research evidence differs regarding the importance of gender in affective experiences; however, women have been demonstrated to have longer and more complex emotional pathways (Lively Citation2008) and higher emotional awareness (Barrett et al. Citation2000).
Previous research has identified that the perception of how much control one has over a situation can influence one’s emotions (Smith and Ellsworth Citation1985). In this study, we identified that the control adults with hearing loss have over a situation can influence their experienced emotions, even before the situation itself. The link between control and emotions was associated with the reduced effectiveness or utilisation of coping strategies unique to listening situations, which could mean that the control over a situation would be an even more important factor for the emotions of adults with hearing loss than those without. It is also possible that if coping strategies such as withdrawal are utilised, adults with hearing loss may not only reduce the risk of experiencing strong negative emotions, but also the chance to experience strong positive emotions. Situations with high levels of control such as passive listening were associated with more enjoyment, as long as coping strategies were not impeded. Hearing loss impacts one’s spatial awareness, particularly in more complex listening situations (Brungart et al. Citation2014), resulting in the highlighted negative emotions. The impact of hearing loss on relationships is well documented (Manchaiah et al. Citation2013). Here, we identified that when conversations break down, if the conversation partner is blamed (as opposed to the hearing loss) then strong negative emotions like resentment and anger can be experienced by both parties and relationships can be damaged. If the hearing loss is blamed, then any negative emotions tend to be focused inward and could eventually lead to a detrimental impact on self-image and feelings of worth. Conversational difficulties and communication breakdown could be characterised as experiences of failure depending on the attribution of blame.
Hearing-aid use tended to increase the chance of positive emotions like happiness and reduce negative emotions such as frustration and fatigue. This concurs with previous literature (Holman, Drummond and Naylor Citation2021b; Stark and Hickson Citation2004). The deficiencies of hearing aids were perceived in different ways by different participants. When weighing up the costs and benefits of wearing hearing aids, some felt that the positives would always outweigh any negatives, whereas others would feel negatively towards the hearing aids and perhaps only wear them begrudgingly. Similar negative feelings towards hearing aids have been demonstrated previously (McCormack and Fortnum Citation2013). The fact that even where people had a love/hate relationship with their aids some keep them in a pocket “just in case”, demonstrates that hearing aids can give reassurance even to those who have negative feelings towards their aids. The self-identity of an individual may influence the relationship with hearing aids. Identifying as a person with hearing loss would make acceptance of hearing aids easier. However, self-identity is not usually a binary factor, and there are nuanced differences between identity labels in a hearing dominated society (Mcilroy and Storbeck Citation2011). demonstrates that although participants used some negative discrete emotion terms to describe the impact of hearing aids, more positive discrete emotions and far fewer negative discrete emotions were mentioned when compared to the impact of hearing loss. No fundamental differences in the experience of emotions in daily-life between people who use and do not use hearing aids were ascertained in this study.
Beyond the emotions experienced in daily life, research has identified that hearing loss can affect the recognition of emotion (Christensen et al. Citation2019). Several participants struggled to understand the emotional content of speech and resorted to facial and body cues. No participants struggled to express emotion in their own speech, potentially because no participants had a profound bilateral hearing loss. The impact of COVID-19 restrictions on feelings of worry and frustration for adults with hearing loss when in conversations with people wearing masks supports previous literature (Naylor, Burke, and Holman Citation2020). The limited impact of COVID-19 restrictions, such as staying indoors, on day-to-day emotions may be due in part to the links between hearing loss and lower levels of social and physical activity prior to the COVID-19 pandemic (Holman et al. Citation2021). There may also have been some relief at not having to attend challenging social situations (Naylor, Burke, and Holman Citation2020).
None of the three authors have a hearing loss meaning that information provided by participants was interpreted without first-hand experience. All authors work in hearing research and with populations with hearing loss. As such there was likely a level of expectation when it came to the experiences of participants. Hearing aids were included as a key part of the study as they are the most common audiological intervention. The research team believes the inclusion of hearing aids was important and that the representation of hearing aids outlined was factual as expressed directly by the participants and reflected in the results.
Limitations
The interviews were initially intended to be face-to-face, but due to the COVID-19 restrictions interviews had to take place remotely. As recruitment took place online, we had to exclude people who did not have an email address, which may bias our sample towards more technologically astute participants. Participants were offered either phone calls, video calls or written questions. It is possible that some invitees failed to respond because they were not comfortable with any of those options. The interviews went smoothly otherwise and in keeping with research indicating the suitability of telephone calls for semi-structured interviews (Cachia and Millward Citation2011), and data resembled the data the authors have seen in their previous face-to-face interview studies. The interviews were based on the discussion of emotion and thus required a level of introspection from participants. Some participants took some time to get used to talking about emotions, which was as we anticipated. Several participants struggled to put their feelings into words even by the end of the interview. The different levels of emotional awareness between individuals are representative of the general population (Nandrino et al. Citation2013).
Conclusions
This study provides a more detailed insight than was previously available regarding the hearing and hearing-aid related emotions experienced by adults with hearing loss. In addition to the multitude of potential emotions caused by the negative impact of hearing loss, there are many individual and situational factors which can influence emotion. Lifestyle, personality, control over a situation, the relationship with those in conversation, the relationship with hearing loss, the relationship with hearing aids and the attribution of blame are just some of the relevant factors which should be considered when investigating hearing-related emotion. Hearing aids are generally a positive influence on the lives and emotions of adults with hearing loss. They reduce negative emotions, allow for the experience of positive emotions and are a reassurance even when not being worn. Understanding the causes of positive and negative emotional reactions to hearing-dependent situations and hearing devices can be beneficial in improving clinical assessment and counselling. The influential role that relationships play in the affective experiences of adults with hearing loss show that social networks and significant others should be included in some form in clinical assessment, follow-up, rehabilitation and counselling. The possible influence of personality on the affective experiences of adults with hearing loss strengthens the importance of individualised treatment. Additionally, addressing the self-stigma exhibited by adults with hearing loss could encourage the open use of hearing aids and reduce the negative affective impact of hearing loss. There is still much to learn regarding the situational impact of hearing aids on the emotional experiences of adults with hearing loss. In order to provide interventions which promote positive emotions in daily life, future research should investigate the situations where hearings aids provide the greatest and the least emotional improvements/deterioration, and how this relates to the full spectrum of hearing-aid use, satisfaction, benefit and different lifestyles.
Supplemental Material
Download MS Word (17.9 KB)Supplemental Material
Download MS Word (38.1 KB)Supplemental Material
Download PDF (419.4 KB)Supplemental Material
Download MS Word (28.7 KB)Acknowledgements
The authors thank all participants who took part in the study. Thanks also to Dr. Gurjit Singh for his help with the study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Barrett, L. F., R. D. Lane, L. Sechrest, and G. E. Schwartz. 2000. “Sex Differences in Emotional Awareness.” Personality and Social Psychology Bulletin 26 (9):1027–1035. doi:10.1177/01461672002611001.
- Bastian, B., P. Kuppens, K. D. Roover, and E. Diener. 2014. “Is Valuing Positive Emotion Associated with Life Satisfaction?” Emotion (Washington, D.C.) 14 (4):639–645. doi:10.1037/a0036466.
- Beedie, C., P. Terry, and A. Lane. 2005. “Distinctions Between Emotion and Mood.” Cognition and Emotion 19 (6):847–878. doi:10.1080/02699930541000057.
- Bennett, R. J., L. Saulsman, R. H. Eikelboom, and M. Olaithe. 2022. “Coping with the Social Challenges and Emotional Distress Associated with Hearing Loss: A Qualitative Investigation using Leventhal’s Self-regulation Theory.” International Journal of Audiology 61 (5):353–364. doi:10.1080/14992027.2021.1933620.
- Besser, A., G. L. Flett, and P. L. Hewitt. 2004. “Perfectionism, Cognition, and Affect in Response to Performance Failure vs. Success.” Journal of Rational-Emotive and Cognitive-Behavior Therapy 22 (4):297–324. doi:10.1023/B:JORE.0000047313.35872.5c.
- Bott, A, and G. Saunders. 2021. “A Scoping Review of Studies Investigating Hearing Loss, Social Isolation and/or Loneliness in Adults.” International Journal of Audiology 60 (sup2):30–46. doi:10.1080/14992027.2021.1915506.
- Bradley, M. M, and P. J. Lang. 1999. “Affective Norms for English Words (ANEW): Instruction Manual and Affective Ratings.” Technical Report C-1, the Center for Research in Psychophysiology, University of Florida 30 (1):25–36.
- Braun, V, and V. Clarke. 2006. “Using Thematic Analysis in Psychology.” Qualitative Research in Psychology 3 (2):77–101. doi:10.1191/1478088706qp063oa.
- Braun, V, and V. Clarke. 2022. “Conceptual and Design Thinking for Thematic Analysis.” Qualitative Psychology 9 (1):3–26. doi:http://dx.doi.org/10.1037/qup0000196.
- Brungart, D. S., J. Cohen, M. Cord, D. Zion, and S. Kalluri. 2014. “Assessment of Auditory Spatial Awareness in Complex Listening Environments.” The Journal of the Acoustical Society of America 136 (4):1808–1820. doi:10.1121/1.4893932.
- Cachia, M, and L. Millward. 2011. “The Telephone Medium and Semi‐structured Interviews: A Complementary Fit.” Qualitative Research in Organizations and Management: An International Journal 6 (3):265–277. doi:10.1108/17465641111188420.
- Christensen, J. A., J. Sis, A. M. Kulkarni, and M. Chatterjee. 2019. “Effects of Age and Hearing Loss on the Recognition of Emotions in Speech.” Ear and Hearing 40 (5):1069–1083. doi:10.1097/AUD.0000000000000694.
- Contrera, K. J., J. Betz, J. A. Deal, J. S. Choi, H. N. Ayonayon, T. Harris, E. Helzner, K. R. Martin, K. Mehta, S. Pratt, for the Health ABC Study, et al. 2016. “Association of Hearing Impairment and Emotional Vitality in Older Adults.” The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 71 (3):400–404. doi:10.1093/geronb/gbw005.
- Costa, P. T, and R. R. McCrae. 1980. “Influence of Extraversion and Neuroticism on Subjective Well-being: Happy and Unhappy People.” Journal of Personality and Social Psychology 38 (4):668–678. doi:10.1037/0022-3514.38.4.668.
- Creswell, J. W. 2013. Qualitative Inquiry and Research Design: Choosing Among Five Approaches (3rd ed)”. Thousand Oaks, CA: SAGE Publications, Inc.
- Dawes, P., M. Maslin, and K. J. Munro. 2014. “Getting used to’ Hearing Aids from the Perspective of Adult Hearing-aid Users.” International Journal of Audiology 53 (12):861–870. doi:10.3109/14992027.2014.938782.
- Dovidio, J. F., S. L. Gaertner, and G. Kafati. 2000. “Group Identity and Intergroup Relations The Common In-group Identity Model.” In Advances in Group Processes, 1–35. Emerald Group Publishing Limited: Bingley. doi:10.1016/S0882-6145(00)17002-X.
- Galloway, J., V. Zhang, V. Marnane, S. Hou, G. Stewart, and F. Bardy. 2019. “The impact of unilateral hearing loss on adult life.”
- Haslam, C., T. Cruwys, M. Milne, C. H. Kan, and S. A. Haslam. 2016. “Group Ties Protect Cognitive Health by Promoting Social Identification and Social Support.” Journal of Aging and Health 28 (2):244–266. doi:10.1177/0898264315589578.
- Heffernan, E., N. S. Coulson, H. Henshaw, J. G. Barry, and M. A. Ferguson. 2016. “Understanding the Psychosocial Experiences of Adults with Mild-moderate Hearing Loss: An Application of Leventhal's Self-regulatory Model.” International Journal of Audiology 55 Suppl 3:S3–s12. doi:10.3109/14992027.2015.1117663.
- Hétu, R. 1996. “The Stigma Attached to Hearing Impairment.” Scandinavian Audiology. Supplementum 43:12–24. PMID: 8738641.
- Holman, J. A., A. Drummond, and G. Naylor. 2021a. “The Effect of Hearing Loss and Hearing Device Fitting on Fatigue in Adults: A Systematic Review.” Ear and Hearing 42 (1):1–11. doi:10.1097/AUD.0000000000000909.
- Holman, J. A., A. Drummond, and G. Naylor. 2021b. “Hearing Aids Reduce Daily-Life Fatigue and Increase Social Activity: A Longitudinal Study.” Trends in Hearing 25:23312165211052786. doi:10.1177/23312165211052786.
- Holman, J. A., A. Drummond, S. E. Hughes, and G. Naylor. 2019. “Hearing Impairment and Daily-life Fatigue: A Qualitative Study.” International Journal of Audiology 58 (7):408–416. doi:10.1080/14992027.2019.1597284.
- Holman, J. A., W. Y. Hornsby Benjamin, F. H. Bess, and G. Naylor. 2021. “Can Listening-related Fatigue Influence Well-being? Examining Associations Between Hearing Loss, Fatigue, Activity Levels and Well-being.” International Journal of Audiology 60 (sup2):47–59. doi:10.1080/14992027.2020.1853261.
- Jayakody, D. M. P., O. P. Almeida, C. P. Speelman, R. J. Bennett, T. C. Moyle, J. M. Yiannos, and P. L. Friedland. 2018. “Association Between Speech and High-frequency Hearing Loss and Depression, Anxiety and Stress in Older Adults.” Maturitas 110:86–91. doi:10.1016/j.maturitas.2018.02.002.
- Krohne, H. W., S. C. Schmukle, H. Spaderna, and C. D. Spielberger. 2002. “The State-trait Depression Scales: An International Comparison.” Anxiety, Stress and Coping 15 (2):105–122. doi:10.1080/10615800290028422.
- Lawrence, B. J., D. M. P. Jayakody, R. J. Bennett, R. H. Eikelboom, N. Gasson, and P. L. Friedland. 2020. “Hearing Loss and Depression in Older Adults: A Systematic Review and Meta-analysis.” The Gerontologist 60 (3):e137–e154. doi:10.1093/geront/gnz009.
- Lee, R. M, and S. B. Robbins. 1995. “Measuring Belongingness: The Social Connectedness and the Social Assurance scales.” Journal of Counseling Psychology 42 (2):232–241. doi:10.1037/0022-0167.42.2.232.
- Lee, S. Y., H. Hwang, R. Hawkins, and S. Pingree. 2008. “Interplay of Negative Emotion and Health Self-efficacy on the Use of Health Information and its Outcomes.” Communication Research 35 (3):358–381. doi:10.1177/0093650208315962.
- Linssen, A. M., M. A. Joore, R. K. H. Minten, Y. D. van Leeuwen, and L. J. C. Anteunis. 2013. “Qualitative Interviews on the Beliefs and Feelings of Adults Towards their Ownership, but Non-use of Hearing Aids.” International Journal of Audiology 52 (10):670–677. doi:10.3109/14992027.2013.808382.
- Lively, K. 2008. “Emotional Segues and the Management of Emotion by Women and Men.” Social Forces 87 (2):911–936. doi:10.1353/sof.0.0133.
- Manchaiah, V. K. C., D. Stephens, and T. Lunner. 2013. “Communication Partners’ Journey through their Partner’s Hearing Impairment.” International Journal of Otolaryngology 2013:1–11. doi:10.1155/2013/707910.
- Marques, T., F. D. Marques, and A. Miguéis. 2022. “Age-related Hearing Loss, Depression and Auditory Amplification: A Randomized Clinical Trial.” European Archives of Oto-Rhino-Laryngology 279 (3):1317–1321. doi:10.1007/s00405-021-06805-6.
- McCormack, A, and H. Fortnum. 2013. “Why Do People Fitted with Hearing Aids not Wear Them?” International Journal of Audiology 52 (5):360–368. doi:10.3109/14992027.2013.769066.
- McIlroy, G, and C. Storbeck. 2011. “Development of Deaf Identity: An Ethnographic Study.” The Journal of Deaf Studies and Deaf Education 16 (4):494–511. doi:10.1093/deafed/enr017.
- Nandrino, J., M. Baracca, P. Antoine, V. Paget, S. Bydlowski, and S. Carton. 2013. “Level of Emotional Awareness in the General French Population: Effects of Gender, Age, and Education Level.” International Journal of Psychology : Journal International de Psychologie 48 (6):1072–1079. doi:10.1080/00207594.2012.753149.
- Naylor, G., L. A. Burke, and J. A. Holman. 2020. “Covid-19 Lockdown Affects Hearing Disability and Handicap in Diverse Ways: A Rapid Online Survey Study.” Ear and Hearing 41 (6):1442–1449. doi:10.1097/AUD.0000000000000948.
- Oatley, K, and E. Duncan. 1994. “The Experience of Emotions in Everyday Life.” Cognition and Emotion 8 (4):369–381. doi:10.1080/02699939408408947.
- Palinkas, L. A., S. M. Horwitz, C. A. Green, J. P. Wisdom, N. Duan, and K. Hoagwood. 2015. “Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research.” Administration and Policy in Mental Health 42 (5):533–544. doi:10.1007/s10488-013-0528-y. 24193818
- Ruusuvuori, J. E., T. Aaltonen, I. Koskela, J. Ranta, E. Lonka, I. Salmenlinna, and M. Laakso. 2021. “Studies on Stigma Regarding Hearing Impairment and Hearing Aid Use Among Adults of Working Age: A Scoping Review.” Disability and Rehabilitation 43 (3):436–446. doi:10.1080/09638288.2019.1622798.
- Saunders, B., J. Sim, T. Kingstone, S. Baker, J. Waterfield, B. Bartlam, H. Burroughs, and C. Jinks. 2018. “Saturation in Qualitative Research: Exploring its Conceptualization and Operationalization.” Quality & Quantity 52 (4):1893–1907. doi:10.1007/s11135-017-0574-8.
- Shukla, A., M. Harper, E. Pedersen, A. Goman, J. J. Suen, C. Price, J. Applebaum, M. Hoyer, F. R. Lin, and N. S. Reed. 2020. “Hearing Loss, Loneliness, and Social Isolation: A Systematic Review.” Otolaryngology-Head and Neck Surgery : official Journal of American Academy of Otolaryngology-Head and Neck Surgery 162 (5):622–633. doi:10.1177/0194599820910377.
- Smith, C. A, and P. C. Ellsworth. 1985. “Patterns of Cognitive Appraisal in Emotion.” Journal of Personality and Social Psychology 48 (4):813–838. doi:10.1037//0022-3514.48.4.970.
- Stark, P, and L. Hickson. 2004. “Outcomes of Hearing aid Fitting for Older People with Hearing Impairment and their Significant Others.” International Journal of Audiology 43 (7):390–398. doi:10.1080/14992020400050050.
- Tong, A., P. Sainsbury, and J. Craig. 2007. “Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups.” International Journal for Quality in Health Care : journal of the International Society for Quality in Health Care 19 (6):349–357. doi:10.1093/intqhc/mzm042.
- Wallhagen, M. I. 2010. “The Stigma of Hearing Loss.” The Gerontologist 50 (1):66–75. doi:10.1093/geront/gnp107.