
Abstract
Objective
The aim of the current study was to examine the presence of positive experiences reported by individuals with tinnitus in the United States.
Design
The study used a cross-sectional survey design. The data were analysed using qualitative (content analysis) and quantitative (t-test or Chi-square test) analyses.
Study Sample
Study participants were individuals participating in clinical trials involving Internet-based cognitive behavioural therapy (ICBT) for tinnitus. A total of 439 respondents, 211 (48.1%) male and 228 (51.9%) female responded, and data were collected via an online questionnaire.
Results
Of the 439 participants, 164 (i.e. 37.4%) reported at least one positive experience. Younger participants and those with lower hearing disability were more likely to report positive experiences. The responses were categorised into six categories: Outlook (n = 139), Personal development (n = 42), Treatment-related (n = 42), Coping (n = 29), Support (n = 19), and Disease-specific (n = 19).
Conclusions
The ability of individuals with chronic tinnitus to identify positive experiences may give insights regarding acceptance and coping with tinnitus as well as the temperament of individuals reporting positive experiences. Considering these variables may help when planning individualised rehabilitation programs.
Introduction
Tinnitus is a common condition that is defined as a perceived sensation of sound in the absence of an external stimulus (Hesser et al. Citation2011). Tinnitus may be experienced as a buzzing, tonal, hissing, or ringing sound (or combined sounds), and can be intermittent, pulsatile, or continuous (Bhatt, Lin, and Bhattacharyya Citation2016). Epidemiologic studies estimate that among the US population, as many as one in ten adults are affected by tinnitus (Bhatt, Lin, and Bhattacharyya Citation2016). Tinnitus can be intrusive, persistent and debilitating, resulting in sleep deprivation as well as a functional impairment in cognition, emotional regulation, hearing, and concentration (Hesser et al. Citation2011). The relationship between tinnitus and increased risk of depression, anxiety, and insomnia have been identified but are not fully understood (Hesser et al. Citation2011). Patients with major depressive disorder or generalised anxiety disorder are up to 3 times as likely to report tinnitus (Salazar et al. Citation2019). At present, there is no cure for most forms of tinnitus and spontaneous resolution is rare, especially in chronic forms (Holmes and Padgham Citation2009). Tinnitus is a significant problem affecting considerable numbers of people worldwide, providing both a social and economic demand for an intervention (Holmes and Padgham Citation2009). As mainstream therapeutic options are often ineffective, evidence-based psychological interventions, such as cognitive behaviour therapy, should be considered (Ghosh and Deb Citation2017).
Positive psychology been defined as the study of conditions and behaviours which contribute to the success, prosperity, and emotional well-being of an individual or group (Gable and Haidt Citation2005). The number of studies looking at positive experiences have grown in recent decades since the rise of ‘Positive Psychology’ as a new framework of psychology. The concept was coined by Seligman and Csikszentmihalyi (Citation2000) who acknowledged that psychology’s adoption of a disease model had led to a lack of attention towards the important role of human attributes such as contentment, optimism, and perseverance in mental health. Over the past two decades, positive psychology has been linked to improved physical and psychological health (Moskowitz, Addington, and Cheung Citation2019). Positive psychology aims to understand health conditions and processes that contribute to the optimal functioning of an individual, despite the difficulties they face (Gable and Haidt Citation2005).
While there is a growing appreciation and recognition for positive psychology among many chronic health conditions there is currently limited research in tinnitus. It is known that chronic health issues have a close relationship with psychological disorders such as depression (Moskowitz, Addington, and Cheung Citation2019) and that psychological resources such as self-esteem, hope, and optimism can positively influence health (Schiavon et al. Citation2016). Research on coping has shown that a positive perspective can protect against such comorbidities (Moskowitz, Addington, and Cheung Citation2019). Several studies on this intersection of psychiatry and chronic disease have reported promising results (Tindle et al. Citation2009; Schiavon et al. Citation2016; Ghosh and Deb Citation2017). Schiavon et al. (Citation2016) identified two major themes among the positive psychology literature, being optimism and hope. In fact, an optimistic mindset has shown to be physiologically protective (Tindle et al. Citation2009).
Optimism has been associated with greater success in heart conditions, with lower rates re-hospitalization and similarly, in head and neck cancer optimism was correlated with survival and an enhanced ability to manage stressors while on the other hand less optimistic cancer patients experienced more negative psychological changes (Schiavon et al. Citation2016). Several existing studies looking at optimism and cardiac health found reduced rehospitalisation post coronary artery bypass graft surgery, reduced mortality in chronic heart disease (Ghosh and Deb Citation2017), and reduced risk of heart disease even after controlling for healthy behaviours (Tindle et al. Citation2009). The use of positive psychology in multiple sclerosis (MS) has found that having more positive experiences led to an improvement in ones quality of life and functional limitations while reducing depressive symptoms (Ghosh and Deb Citation2017). Additionally, among MS patients, optimism lead to positive physical health outcomes as patients sought opportunities to alter their disease experiences despite their adverse circumstances (Schiavon et al. Citation2016). Among patients with Irritable Bowel Disease improved optimism correlates with reduced levels of emotional worry and negative attitudes (Schiavon et al. Citation2016). Furthermore, optimistic people have been recognised as being better prepared to face the challenges of adopting healthy behaviours which may improve their lived experience with a chronic disease (Schiavon et al. Citation2016).
Research has found that emotional well-being and hope for the future were strengthened during the rehabilitation process in patient with respiratory conditions (Schiavon et al. Citation2016). Various other studies have found that hope contributes to overall satisfaction in individuals with neurological disorders (i.e. spinal or acquired brain injuries) when they embark on their rehabilitation journey. Among HIV-positive individuals, hope has been inversely correlated with symptoms, suggesting that increased hope is correlated a better quality of life and symptom reduction (Schiavon et al. Citation2016). A similar finding has also been found in patients with chronic combat-related post-traumatic stress disorder (Schiavon et al. Citation2016). The literature suggests that there is an important relationship between positive psychology (i.e. optimism and hope) and a perceived reduction in the effects of chronic disease. These attitudes may facilitate an improved perspective on life enabling chronic condition suffers to better deal with their diseases while the hope for an improved future empowers them to implement change
Research has described a range of positive experiences in people with acquired hearing loss (Kerr and Stephens Citation1997; Stephens and Ken Citation2003). Positive psychology interventions have shown promise in the management of otolaryngological disorders like Meniere’s disease (Stephens et al. Citation2010). From our background research, only two studies are directly relatable to this current work.
The first notable study that explored positive psychology in tinnitus was by Kentala et al. (Citation2008). This study recruited members of the Finnish Meniere Federation who were patients attending a tertiary level ENT and audiology clinics across Finland with the aim to identify self-reported positive aspects associated with tinnitus to strengthen peer-support systems. The study described responses to an open-ended questionnaire by 121 participants (53 men, 68 women) that attended a specialist tinnitus clinic at the Welsh Hearing Institute. They found that 41.3% of participants reported at least one positive response. These responses were categorised into four themes:
Treatment-related: for example, “I can take steps to alleviate the cause of the increase in volume of the tinnitus by relaxing, deep breathing, going for a walk, etc. I am quite sure that this must be beneficial to my general health and well-being”.
Personal development: for example, “taught me not to take things for granted”.
Disease-specific: an understanding that the symptoms are “only temporary” and will ease with time.
Other people: the participants considered the empathy or help of other people important in their positive experience.
The most common theme was ‘Treatment-related’. Kentala et al. (Citation2008) concluded that, despite many participants being unable to report positive experiences, these experiences could help improve tinnitus habituation programmes and the insights may be tailored to supplement counselling or peer-support programmes for sufferers. The authors noted that the open-ended questionnaires format was problematic regarding each patient’s insight and ability to articulate their experiences, and suggested that a more appropriate option would be a structured questionnaire where participants are asked whether or not particular statements apply to them.
A second study is a cross-sectional survey in the United Kingdom by Beukes et al. (Citation2018b). This study included a broader, UK-wide population by recruiting participants through various platforms (online and in clinics) with the aim to gain further insight related to positive experiences in those experiencing tinnitus. The study described responses of 240 participants (137 males, 103 females) that were gathered during the enrolment to another trial investigating the feasibility and efficacy of internet-based CBT in the UK (Beukes et al. Citation2018a). Beukes et al. (Citation2018b) found that 32.5% of participants reported at least one positive experience. Individuals reporting positive experiences were typically younger, had less severe hearing disability and fewer cognitive failures. The positive responses were categorised into four themes:
Coping: for example, “became more aware of the impact of stress”.
Personal development: for example, “gained better understanding of tinnitus”.
Support: for example, “compassion from others with tinnitus”.
Outlook: for example, “MRI results found no other problems”.
The most frequently identified themes were ‘Coping’ and ‘Personal development’. Based on the results of this study, the authors recommended that treatment programs ought to include information for patients support network (i.e. friends and family) to facilitate a deeper understand of tinnitus and how to support those with bothersome tinnitus. Beukes et al. (Citation2018b) identified several limitations such as lacking a standardised measure of positive and negative thinking to strengthen results and enable comparison to other studies. We attempted to address this issue by utilising the Tinnitus Cognitions Questionnaire, a questionnaire designed to measure positive and negative thoughts related to tinnitus (Wilson and Henry Citation1998). Similarly to Kentala et al. (Citation2008), Beukes et al. (Citation2018b) identified the need to glean more positive responses which may be achieved through using a structure questionnaire format.
Based on the limited studies exploring positive psychology in tinnitus (Kentala et al. Citation2008; Beukes et al. Citation2018b), the paper by Beukes et al. (Citation2018b) concluded that personal development and a positive outlook are possible with tinnitus. The authors identified that a better understanding of the association between positive experiences and coping with tinnitus is needed (Beukes et al. Citation2018b). Furthermore, Beukes et al. (Citation2018b) highlighted the importance of “Coping” with this chronic condition and reiterates the importance of interventions such as cognitive behaviour therapy in chronic disease management. It may also help identify gaps in patient-centred care, hence the aim of the current study was to examine any positive experiences reported by individuals with tinnitus in the United States. We hypothesised that the positive experiences found in an American cohort would be similar to those reported in the identified UK-based studies.
Materials and methods
Study design and ethical considerations
The study used a cross-sectional survey design. Ethics approval was granted by the Institutional Review Board at Lamar University (IRB-FY17-209 and IRB-FY20-200). Study participants enrolled in clinical trials involving Internet-based cognitive behavioural therapy (ICBT) for tinnitus (Clinical Trials.gov registration numbers NCT04004260, NCT04335812). Details regarding recruitment strategy and study population can be found in Beukes et al. (Citation2021a); Beukes et al. (Citation2021b).
Data collection
The data was collected from individuals with chronic tinnitus while they were enrolling for the ICBT study. Data collection was via an online questionnaire and included data regarding demographics (gender, age, employment, education), and clinical variables. The Tinnitus Functional Index (TFI) (Meikle et al. Citation2012) was used to quantify tinnitus duration and severity, the Patient Health Questionnaire 9 (PHQ9) (Kroenke, Spitzer, and Williams Citation2001) was used to grade depression, Generalised Anxiety Disorder 7 (GAD7) (Spitzer et al. Citation2006) was used to measure anxiety, the Insomnia Severity Index (ISI) (Bastien, Vallières, and Morin Citation2001) assessed insomnia, the Tinnitus and Hearing Survey (THS) (Henry et al. Citation2015) was used to describe self-reported hearing disability, the Tinnitus Cognitions Questionnaire (TCQ) (Wilson and Henry Citation1998) was used to measure positive and negative thinking, the EQ-5D-5L VAS (Rabin and de Charro Citation2001) measured health-related quality of life and participants were also asked to complete a single open-ended positive experiences question (PEQ). To enable comparison with the outcomes of Kentala et al. (Citation2008) and Beukes et al. (Citation2018b), the same open-ended positive effects question was used: ‘Make a list of any positive effects or outcomes related to having tinnitus, list as many as you can think of’.
Data analysis
Quantitative analysis
A t-test was used to compare the means of the continuous variables between two groups and Chi-square testing was used to examine the association between groups and baseline demographics of categorical variables. For all statistical analyses, a level of p < 0.05 was considered statistically significant.
Qualitative analysis
Responses to the PEQ were analysed using the qualitative content analysis approach outlined in Graneheim and Lundman (Citation2004). The experiences described in the PEQ responses were coded into ‘meaning units’ (a coding unit that collects all statements that relate to the same central meaning). Similar ‘meaning units’ were further consolidated into ‘condensed meaning units’. This process was independently carried out by two researchers (JL and VD) and compared for inconsistencies, in which case coding was performed by a third researcher (VM). The ‘condensed meaning units’ were then brought together into one text to be examined as a whole and summated into ‘sub-categories’ which were finally condensed into ‘categories’. To enable responses comparison, answers were collated into categories and sub-categories outlined by Beukes et al. (Citation2018b) (i.e. coping, personal development, support and outlook) and Kentala et al. (Citation2008) (i.e. Treatment-related and Disease-specific).
Results
Participants characteristics and number of positive Responses
Out of 439 respondents, 211 (48.1%) were male, 228 (51.9%) were female. The mean age was 55.3 years (SD 13.4) with a mean tinnitus duration of 12.1 years (SD 13.0) (see ). The majority (n = 275, 62.6%) did not report any positive experiences but 164 participants (37.4%) reported at least one positive experience, 75 of whom (17.1%) reported more than one positive experience. Of the 164 people who provided positive responses, the mean and median responses were 1.8 (SD = 1.1) and 1 respectively. compares the number of positive responses per participant to those reported by Kentala et al. (Citation2008) and Beukes et al. (Citation2018b). Similar trends can be seen in the frequency of positive responses across all 3 studies, with the highest percentage of positive responses reported by Kentala et al. (Citation2008). Younger participants (p = 0.001) and those with lower self-reported hearing disability (p = 0.03) were more likely to report positive experiences when compared to older and those with higher self-reported hearing disability (see ). No significant differences/associations were found on any other demographic or clinical variables.
Figure 1. The number of positive responses per participant compared to those reported by Kentala et al. (Citation2008) and Beukes et al. (Citation2018b).
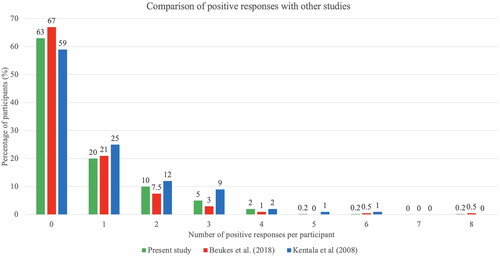
Table 1. Statistical analysis of demographic and clinical variables between those who reported at least one positive experience and those that did not.
Positive experiences
A total of 290 positive responses were reported by 164 participants (see ). The responses were categorised into six categories: ‘Coping’ (n = 29), ‘Outlook’ (n = 139), ‘Personal Development’ (n = 42), ‘Support’ (n = 19), ‘Treatment-related’ (n = 42) and ‘Disease-specific’ (n = 19).
Table 2. Positive responses to the open-ended questions.
The most positive responses fell into the category of ‘Outlook’ (47.9%). This category captured those experiences that led to a change in participants’ way of understanding and thinking, for example, one participant identified a change in attitude of “[becoming] more accepting and not trying to fix or change everything that I do not like”. These positive experiences indicate that tinnitus can lead to positive changes in a person’s point of view, such as developing empathy for other sufferers, appreciating that it could be worse, and being resilient in overcoming obstacles presented by the condition.
The category with the second highest number of meaning units was ‘Personal development’ (14.5%). This category included positive responses that described a progress in a person’s capabilities or attributes, for example, one participant described self-improvement through commenting “I pay more attention when people are talking”. Meaning units captured by this category included responses about taking better care of one’s health, realising one’s own strength and being a better listener/listening actively. This indicates that, despite social and psychological pressures, sufferers are still able to develop in a holistic way.
Participant responses related to ‘Coping’ (10.0%) category describes positive experiences that arise from successfully managing tinnitus and/or its challenges. This is distinct from ‘personal development’ and ‘treatment-related’ which capture experiences that participant’s felt improved them, or those which stemmed directly from the treatment respectively. For example, a participant identified a positive change in behaviour commenting, “I avoid anxiety”. This included meditation, managing anxiety, and developing a stronger connection with one’s spirituality. This proposes that despite the lack of an effective treatment for tinnitus, sufferers find ways to cope and ultimately enact positive change in their lives.
The participants responded with positive experiences around giving or receiving assistance which were classified under the category of ‘Support’ (6.6%). Stronger and more meaningful relationships developed with others, more intimate friendships, and a chance to help other sufferers were some of the experiences that were placed in this category. For example, this included comments such as “I was able to tell my children that the sound of buzzing or cracking was our family normal”.
Positive experiences that were identified as unexpected benefits of the tinnitus-specific treatment were classified under the category of ‘Treatment-related’ (14.5%). This suggested that tinnitus treatment measures themselves are associated with positive outcomes, such as developing new hobbies, forming new relationships with other sufferers/care givers, and adopting healthy behaviour changes. An example of such a comment being, “Not wanting to go out to loud venues will cause me to save money”.
Lastly, a subset of positive experiences fell into the category of ‘Disease-specific’ (6.6%) which were those experiences that resulted directly or indirectly from having tinnitus itself. This suggested that developing tinnitus was associated with positive experiences such as benefits experienced due to the constant ringing (i.e. drowning out other noises), and improving one’s knowledge about hearing. For example, looking at tinnitus as a strength through the comment, “I rarely need an alarm clock because the ringing wakes me up by 6am almost every day”.
Discussion
We took the definition of a positive experience as the intrinsic experiences that an individual considers to be a source of motivation or support and contributors towards physical, spiritual, social, and emotional wellbeing (Kentala et al. Citation2008). This study found that over one-third (37.4%) of the participants were able to report at least one positive experience associated with tinnitus. Similar studies of positive experiences in tinnitus have been reported by Beukes et al. (Citation2018b) and Kentala et al. (Citation2008) who reported at least one positive experience in 32.5% and 41.3% of participants respectively. Outside of the tinnitus space, positive experiences have also been identified in up to 75.1% of patients with Meniere’s disease and in 21.6% to 40.1% of hearing loss sufferers (Kerr and Stephens Citation1997; Kerr and Stephens Citation2000; Stephens et al. Citation2007). This confirms the hypothesis that despite the debilitating effects, some patients with chronic conditions such as tinnitus are able to identify positive experiences (Kentala et al. Citation2008; Beukes et al. Citation2021b).
In the present study, ‘Outlook’ was the most reported category (47.9%) compared to the least reported one in Beukes et al. (Citation2018b) (8.7%). This difference may, in part, be explained by specific demographics within each study. Of the participants in Beukes et al. (Citation2018b), 129 (53.8%) had attained a tertiary level qualification or higher compared with 388 (88.4%) from our study. A higher level of education may correlate to heightened emotional awareness and introspection. Moreover, the average age of our study, was 55.3 years, compared with 48.16 years in Beukes et al. (Citation2018b). It is possible that the over 50 population has an increased sense of health-awareness due to public health policies and screening programs which routinely commence at this age. We propose that the combination of a higher level of education and advanced age may correlate to an enhanced level of introspection and health-awareness manifesting in an improved ability to think critically about ones ‘Outlook’. In this study, tinnitus was linked to positive changes in a person’s (participant) outlook and personal development. This may be related to the description by Sutin et al. (Citation2013) that portrays the development of a chronic disease as an event in an individual’s life, that may have significant physiological, social, and psychological ramifications which may subsequently translate to long-term changes in self-perception. In addition, Wilson and Henry (Citation1998) showed that negative thinking was associated with more problematic tinnitus when compared to positive thinking. This poses the question of whether a reduction in negative thinking or enhancement of positive thinking is more useful in the management of tinnitus. Currently, it is still unclear. Psychological interventions aimed at instilling a positive outlook have been explored in cancer patients (Fitch, Nicoll, and Lockwood Citation2020). They have demonstrated that an improvement in self-esteem, optimism and self-efficacy helped reduce distress, and facilitated the resumption of pleasurable activities (Sutin et al. Citation2013; Fitch, Nicoll, and Lockwood Citation2020).
The present study also found that having tinnitus can stimulate support networks which have associated positive experiences, albeit this was the least reported category (‘Support’, 6.6%) while being the third most frequent in Beukes et al. (Citation2018b) (27.8%). This suggests that the current population was more capable of coping and less reliant on support-networks when compared with the population in Beukes et al. (Citation2018b). It remains unclear why this may be, but it is possible that such a marked difference may simply reflect the subjective nature and inherent bias of a qualitative research method. The category of ‘Support’ has also been reported by cancer survivors in that being able to share experiences and stories with others helped cultivate positive experiences (Fitch, Nicoll, and Lockwood Citation2020). While not a prominent category in the present study, this category predominantly consisted of responses relating to the ability to develop more meaningful relationships, which highlights the idea that interactions with friends and family can be invaluable in achieving positive experiences (Kerr and Stephens Citation1997; Fitch, Nicoll, and Lockwood Citation2020). Similarly, the categories of ‘Personal development’ (14.5%) and ‘Coping’ (10%) were more frequently reported by Beukes et al. (Citation2018b) (31% and 32.5% respectively) than they were in the present study, once again likely due to the subjective nature of the research methods.
We found that simply having tinnitus can have positive effects which were categorised as ‘Disease-specific’ (6.6%), a finding that was reported in 13.0% of participants in Kentala et al. (Citation2008). This is reflected in literature where positive experiences have been reported as a direct result of hearing loss, for example, as reduced disturbance from unwanted sounds (Kerr and Stephens Citation1997). Some individuals have reported how the positive experience was simply knowing what tinnitus is and how it feels (Andersson and Edvinsson Citation2008).
Similarly, we found positive experiences around tinnitus treatment in 14.5% of our participants as opposed to Kentala et al. (Citation2008), where it was the most reported category at 59.8%. One possible reason which attempts to resolve the discrepancies between this study and Kentala et al. (Citation2008) is that the major focus of the latter was to gain insight into tinnitus habituation programmes. Consequently, the major outcome was to determine the positive aspects that patients relate to tinnitus and balance problems rather than tinnitus alone. This information was then intended to be utilised to improve such programmes, hence the goal of the study was treatment-related rather than positive psychology-specific. Kentala et al. (Citation2008) also reported therapies that were associated with positive experiences in tinnitus patients. We found that many of the therapies were also mentioned by participants in our study but were not specifically reported in this paper. These modalities included masking, relaxation, avoidance, distraction, exercise, and acceptance. The similarity suggests that, in future, it may be pertinent to identify therapies received by the participants, so that we may understand whether treatment-related positive experiences are dependent upon access to affordable, quality treatment. If so, identifying which therapies are strongly associated with self-reported positive experiences could help improve patient outcomes in tinnitus. Treatment-related positive experiences were also reported by Kerr and Stephens (Citation1997) in cohorts with hearing loss.
This study found that younger individuals were more likely to report positive experiences with tinnitus, which is consistent with the findings from Beukes et al. (Citation2018b). This finding has also been reported in hearing loss studies (Kerr and Stephens Citation2000). For instance, in one study, the average age of those who reported positive experiences was 12.2 years younger than those who did not (56.6 years versus 68.8 years) (Kerr and Stephens Citation2000). Based on these trends, we hypothesise that, in tinnitus and hearing loss, younger people may have a more optimistic outlook about their condition, and therefore more likely to have positive experiences. This is supported by previous studies that linked optimism with positive health outcomes, reporting that optimists are more knowledgeable about health risks, more likely to engage in healthy behaviours, employ healthy coping mechanisms, and have good social supports (Chopik, Kim, and Smith Citation2015). Such underlying protective factors may also be present in younger tinnitus patients and warrant further investigation.
We also found that participants with lower levels of self-reported hearing disability were more likely to report positive experiences with tinnitus compared to higher levels of hearing disability. With similar findings reported by Beukes et al. (Citation2018b) this suggests that the combination of tinnitus and significant hearing disability may cause more disease burden and reduce the number of positive experiences an individual has. In line with Beukes et al. (Citation2018b) we also found a significant relationship between hearing loss and positive responses in tinnitus. Beukes et al. (Citation2018b) postulated that severe tinnitus can deleteriously impact cognitive performances (i.e. working memory and attention) and may hinder the recognition of positive experiences.
Similarly to our research, prior studies have not found an association between the majority of demographic and clinical characteristics, and positive experiences (Kerr and Stephens Citation2000). In the present study, the total TCQ score did not significantly differ between patients who did and did not report positive experiences. The scoring system of the TCQ is such that high total scores are indicative of a greater tendency to embrace negative thoughts and a lower tendency to embrace positive ones. Further Wilson and Henry (Citation1998) reported that the total score is correlated to the degree to which tinnitus is perceived to be problematic. This proposes that patients in both groups experienced similarly problematic tinnitus, a finding that is further supported by the similar tinnitus distress (i.e. TFI scores), yet the degree to which tinnitus was problematic did not impact one’s ability to identify positive experiences.
In our study, tinnitus severity scores (TFI) did not differ between the two groups suggesting that disease burden was equal across both groups. Athough, one group reported positive experiences, the quality of life (ED-5D-5L) and insomnia severity (ISI) scores were not significantly different. This may suggest that positive thinking does not protect from some of the physical side effects of the disease. Similarly, from the lack of correlation between depression and anxiety scores between the two groups, we may also infer that positive thinking does not protect the individual from the mental health impact of their disease. This is a reasonable conclusion given the multifactorial nature of depression and anxiety. This is likely reflective of the fact that being able to think positive thoughts about tinnitus is understandably not the same as having positive health outcomes due to the condition. However, the lack of correlation likewise suggests that despite depression, sufferers of tinnitus are still able to recognise positive experiences related to this condition. This was contrary to our initial thoughts as, purely based on the nature of depression we anticipated identifying fewer positive experiences in these patients. Similarly, recent studies have found optimism was linked to greater psychological well-being and confidence in one’s ability to achieve a favourable outcome predicted increases in positive affect (Lyons, Heywood, and Rozbroj Citation2016).
Finally, positive thinking was not correlated to tinnitus duration, gender, or the level of education completed by the participant. This is an encouraging finding in terms of implications for psychological interventions in tinnitus sufferers, as demographic variables may not limit the efficacy of such interventions. Furthermore, this may provide evidence that positive experiences are not reliably predicted by demographic or clinical variables but may instead be attributed to experiential factors. Experiential factors may be described by self-management which is defined as the strategies undertaken by an individual to control a disease, promote health, and live well (Audulv Citation2013). This is a critical part of any chronic condition. Traditionally, health professionals have focussed on the “disease”, with minimal regard for self-management. With this being said, contemporary literature suggests that there has been a shift to self-management programs with seemingly good outcomes (Audulv Citation2013). Research has shown that development of these self-management strategies is best achieved through a combination of support strategies which are tailored to the individual (Audulv Citation2013). This seems to provide evidence for the ongoing support and positive psychological interventions in the treatment of tinnitus and other chronic conditions. Furthermore, a standardised measure like the Tinnitus Cognitions Questionnaire may provide an objective way to measure changes in positive and negative thinking when evaluating psychological interventions in tinnitus (Wilson and Henry Citation1998).
Strengths & limitations
A strength of this study was the use of an open-ended questionnaire format which was completed online. This may have facilitated more honest responses from the participants without any predetermined biases. The study participants were enrolled voluntarily, from the public as a study sample, which may introduce a sampling bias. Furthermore, the study included members of tinnitus support groups, the American Tinnitus Association, primary care, audiology, and ENT clinics and thus may represent a smaller population of individuals who may have more severe tinnitus, greater health literacy and access to healthcare or predisposition to enrolling in our study. These confounders have also been identified in other studies (Fackrell et al.; Beukes et al. Citation2018b). Finally, including the TCQ as a standardised measure for positive and negative thinking in tinnitus in this study will enable comparison of cognitive reactions in the present cohort to future studies using the same questionnaire. Alternatively, other suitable questionaries that also correlate with the TCQ may be used; these include the Tinnitus Effects Questionnaire, Tinnitus Handicaps Questionnaire, or Tinnitus Reaction Questionnaire (Wilson and Henry Citation1998). However, gain from use of the TCQ may have been maximised through the subdivision of the total score into positive and negative subscales. A high score on the positive subscale suggests fewer positive thoughts, whereas a high score on the negative subscale suggests more negative thinking. Using the subscales individually may have provided an idea of whether participants who did or did not report positive thoughts differed in their tendency to have negative cognitions or their tendency to engage in positive thinking.
Future directions
The categories identified in our research build on those already observed in similar studies (Kentala et al. Citation2008; Beukes et al. Citation2018b), providing further evidence for the use of open-ended questionnaires in exploring the positive aspects related to tinnitus. We support further exploration of positive experiences using the structured questionnaire that can be developed based on the current study. It is also worth exploring the association between positive experiences and outlook, personal development, coping with disease outcomes and finally, the prognosis of tinnitus. We encourage the use of the Tinnitus Cognitions Questionnaire to objectively quantify positive and negative thinking but remain uncertain about its utility for studies exploring positive psychology due to the poor association of the positive subscale with self-reported tinnitus distress (Wilson and Henry Citation1998). Exploring of how clinicians can facilitate positive experiences and/or thinking, as well as the consequences that this may have on the outcome is also needed. Furthermore, continued research to determine whether positive experiences may predict the treatment outcomes is imperative (Fackrell et al. Citation2016; Beukes et al. Citation2018b).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been republished with minor change. This change do not impact the academic content of the article.
Additional information
Funding
References
- Andersson, G., and E. Edvinsson. 2008. “Mixed feelings about living with tinnitus: A qualitative study.” Audiological Medicine 6:48–54. doi:10.1080/16513860801899355
- Audulv, Å. 2013. “The over time development of chronic illness self-management patterns: a longitudinal qualitative study.” BMC Public Health 13:452. doi:10.1186/1471-2458-13-452
- Bastien, C. H., A. Vallières, and C. M. Morin. 2001. “Validation of the Insomnia Severity Index as an outcome measure for insomnia research.” Sleep Medicine 2 (4):297–307. doi:10.1016/s1389-9457(00)00065-4.
- Beukes, E. W., G. Andersson, M. Fagelson, and V. Manchaiah. 2021a. “Audiologist-Supported Internet-Based Cognitive Behavioral Therapy for Tinnitus in the United States: A Pilot Trial.” Am J Audiol 30:717–729. doi:10.1044/2021_AJA-20-00222
- Beukes, E. W., G. Andersson, M. A. Fagelson, and V. Manchaiah. 2021b. “Dismantling internet-based cognitive behavioral therapy for tinnitus. The contribution of applied relaxation: A randomized controlled trial.” Internet Interventions. 25:100402. doi:10.1016/j.invent.2021.100402
- Beukes, E. W., D. M. Baguley, P. M. Allen, V. Manchaiah, and G. Andersson. 2018a. “Audiologist-Guided Internet-Based Cognitive Behavior Therapy for Adults With Tinnitus in the United Kingdom: A Randomized Controlled Trial.” Ear Hear 39:423–433. doi:10.1097/AUD.0000000000000505
- Beukes, E. W., V. Manchaiah, T. E. Valien, D. M. Baguley, P. M. Allen, et al. 2018b. “Positive experiences related to living with tinnitus: A cross-sectional survey.” Clinical Otolaryngology 43:489–495. doi:10.1111/coa.13002
- Bhatt, J. M., H. W. Lin, and N. Bhattacharyya. 2016. “Prevalence, Severity, Exposures, and Treatment Patterns of Tinnitus in the United States.” JAMA Otolaryngology- Head & Neck Surgery 142 (10):959–965. doi:10.1001/jamaoto.2016.1700.
- Chopik, W. J., E. S. Kim, and J. Smith. 2015. “Changes in Optimism Are Associated With Changes in Health Over Time Among Older Adults.” Social Psychological and Personality Science 6 (7):814–822. doi:10.1177/1948550615590199.
- Fackrell, K., D. A. Hall, J. G. Barry, and D. J. Hoare. 2016. “Psychometric properties of the Tinnitus Functional Index (TFI): Assessment in a UK research volunteer population.” Hear Res 335:220–235. doi:10.1016/j.heares.2015.09.009
- Fitch, M. I., I. Nicoll, and G. Lockwood. 2020. “Positive cancer experiences: perspectives from cancer survivors.” Journal of Patient Experience 7 (6):1501–1508. doi:10.1177/2374373520942420.
- Gable, S. L., and J. Haidt. 2005. “What (and Why) is Positive Psychology?” Review of General Psychology 9:103–110. doi:10.1037/1089-2680.9.2.103
- Ghosh, A., and A. Deb. 2017. “Positive Psychology Interventions for Chronic Physical Illnesses: A Systematic Review.” Psychological Studies 62:1–20.
- Graneheim, U. H., and B. Lundman. 2004. “Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness.” Nurse Education Today 24 (2):105–112. doi:10.1016/j.nedt.2003.10.001.
- Henry, J. A., S. Griest, T. L. Zaugg, E. Thielman, C. Kaelin, et al. 2015. “Tinnitus and hearing survey: a screening tool to differentiate bothersome tinnitus from hearing difficulties.” Am J Audiol 24:66–77. doi:10.1044/2014_AJA-14-0042
- Hesser, H., C. Weise, V. Z. Westin, and G. Andersson. 2011. “A systematic review and meta-analysis of randomized controlled trials of cognitive-behavioral therapy for tinnitus distress.” Clinical Psychology Review 31 (4):545–553. doi:10.1016/j.cpr.2010.12.006.
- Holmes, S., and N. D. Padgham. 2009. “Review paper: more than ringing in the ears: a review of tinnitus and its psychosocial impact.” Journal of Clinical Nursing 18 (21):2927–2937. doi:10.1111/j.1365-2702.2009.02909.x.
- Kentala, E., C. Wilson, I. Pyykkö, K. Varpa, and D. Stephens. 2008. “Positive experiences associated with tinnitus and balance problems.” Audiological Medicine 6:55–61. doi:10.1080/16513860801959639
- Kerr, P., and D. Stephens. 2000. “Understanding the nature and function of positive experiences in living with auditory disablement.” Scandinavian Journal of Disability Research 2:21–38. doi:10.1080/15017410009510750
- Kerr, P. C., and D. Stephens. 1997. “The use of an open-ended questionnaire to identify positive aspects of acquired hearing loss.” Audiology 36:19–28. doi:10.3109/00206099709071958
- Kroenke, K., R. L. Spitzer, and J. B. Williams. 2001. “The PHQ-9: validity of a brief depression severity measure.” Journal of General Internal Medicine 16 (9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x.
- Lyons, A., W. Heywood, and T. Rozbroj. 2016. “Psychosocial factors associated with flourishing among Australian HIV-positive gay men.” BMC Psychology 4 (1):46. doi:10.1186/s40359-016-0154-z.
- Meikle, M. B., J. A. Henry, S. E. Griest, B. J. Stewart, H. B. Abrams, et al. 2012. “The tinnitus functional index: development of a new clinical measure for chronic, intrusive tinnitus.” Ear Hear 33:153–176. doi:10.1097/AUD.0b013e31822f67c0
- Moskowitz, J. T., E. L. Addington, and E. O. Cheung. 2019. “Positive psychology and health: Well-being interventions in the context of illness.” General Hospital Psychiatry 61:136–138. doi:10.1016/j.genhosppsych.2019.11.001.
- Rabin, R., and F. de Charro. 2001. “EQ-5D: a measure of health status from the EuroQol Group.” Annals of Medicine 33 (5):337–343. doi:10.3109/07853890109002087.
- Salazar, J. W., K. Meisel, E. R. Smith, A. Quiggle, D. B. McCoy, et al. 2019. “Depression in Patients with Tinnitus: A Systematic Review.” Otolaryngology–Head and Neck Surgery 161:28–35. doi:10.1177/0194599819835178
- Schiavon, C. C., E. Marchetti, L. G. Gurgel, F. M. Busnello, and C. T. Reppold. 2016. “Optimism and Hope in Chronic Disease: A Systematic Review.” Frontiers in Psychology. 7:2022.
- Seligman, M. E., and M. Csikszentmihalyi. 2000. “Positive psychology-An introduction.” American Psychology 55:5–14. doi:10.1037/0003-066X.55.1.5
- Spitzer, R. L., K. Kroenke, J. B. W. Williams, and B. Löwe. 2006. “A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7.” Archives of Internal Medicine 166 (10):1092–1097. doi:10.1001/archinte.166.10.1092.
- Stephens, D., and P. Ken. 2003. “The role of positive experiences in living with acquired hearing loss.” International Journal of Audiology 42:118–127. doi:10.3109/14992020309074633
- Stephens, D., E. Kentala, K. Varpa, and I. Pyykkö. 2007. “Positive experiences associated with Ménière’s disorder.” Otology & Neurotology 28 (7):982–987. doi:10.1097/MAO.0b013e318068b2dd.
- Stephens, D., I. Pyykko, E. Kentala, and H. Levo. 2010. “Positive experiences reported by people with Ménière’s disorder: a quantitative study.” Acta Oto-Laryngologica 130 (9):1013–1018. doi:10.3109/00016481003629341.
- Sutin, A. R., A. B. Zonderman, L. Ferrucci, and A. Terracciano. 2013. “Personality traits and chronic disease: implications for adult personality development.” The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences 68 (6):912–920. doi:10.1093/geronb/gbt036.
- Tindle, H. A., Y.-F. Chang, L. H. Kuller, J. E. Manson, J. G. Robinson, et al. 2009. “Optimism, Cynical Hostility, and Incident Coronary Heart Disease and Mortality in the Women’s Health Initiative.” Circulation 120:656–662. doi:10.1161/CIRCULATIONAHA.108.827642
- Wilson, P. H., and J. L. Henry. 1998. “Tinnitus Cognitions Questionnaire: development and psychometric properties of a measure of dysfunctional cognitions associated with tinnitus.” The International Tinnitus Journal 4 (1):23–30.