
Abstract
Frewen and Lanius (in press) recently articulated a 4-D model as a framework for classifying symptoms of posttraumatic stress into those that potentially occur within normal waking consciousness (NWC) versus those that intrinsically represent dissociative experiences of trauma-related altered states of consciousness (TRASC). Four dimensions were specified: time-memory, thought, body, and emotion. The 4-D model further hypothesizes that in traumatized persons, symptoms of TRASC, compared with NWC forms of distress, will be (a) observed less frequently; (b) less intercorrelated, especially as measured as moment-to-moment states; (c) observed more frequently in people with high dissociative symptomatology as measured independently; and (d) observed more often in people who have experienced repeated traumatization, particularly early developmental trauma. The aim of the present research was to begin to evaluate these 4 predictions of the 4-D model. Within a sample of 74 women with posttraumatic stress disorder (PTSD) primarily due to histories of childhood trauma, as well as within a 2nd sample of 504 undergraduates (384 females), the 1st 2 hypotheses of the 4-D model were supported. In addition, within the PTSD sample, the 3rd hypothesis was supported. However, inconsistent with the 4th hypothesis, severity of childhood trauma history was not strongly associated with TRASC. We conclude that the hypotheses articulated by the 4-D model were generally supported, although further research in different trauma-related disorders is needed, and the role of childhood trauma history in the etiology of TRASC requires further research.
Research increasingly validates the study of trauma-related dissociation as a multidimensional construct (e.g., Briere, Weathers, & Runtz, Citation2005; Dell & Lawson, Citation2009). For example, theorists commonly differentiate between compartmentalization and detachment as different kinds of dissociative experiences (Brown, Citation2006; Holmes et al., Citation2005). Whereas compartmentalization refers to a disintegration between normally integrated psychological functions, detachment essentially refers to experiences of altered states of consciousness such as derealization and depersonalization (Steele, Dorahy, van der Hart, & Nijenhuis, Citation2009). Thus, experiences of altered states of consciousness are considered to fall under the umbrella term that is dissociation by most contemporary theorists (Holmes et al., Citation2005).
A dissociative subtype of posttraumatic stress disorder (PTSD) was also recently defined by the presence of self-reported experiences of depersonalization and/or derealization and is therefore operationalized exclusively by experiences of dissociative detachment rather than those of compartmentalization (e.g., Carlson, Dalenberg, & McDade-Montez, Citation2012; Dalenberg & Carlson, Citation2012; Ginzburg et al., Citation2006; Lanius, Brand, Vermetten, Frewen, & Spiegel, Citation2012; Lanius et al., Citation2010; Spiegel et al., Citation2011, Citation2013). It seems unlikely, however, that experiences of depersonalization and derealization represent the only kinds of dissociative symptoms experienced by certain persons with PTSD. For example, researchers have increasingly acknowledged the dissociative character of flashbacks of traumatic memories (Brewin, Gregory, Lipton, & Burgess, Citation2010; Friedman, Resick, Bryant, & Brewin, Citation2011) and amnesia for important aspects of traumatic events. Moreover, recent diagnostic formulations for depersonalization disorder have been expanded to include not only out-of-body experiences but also feelings of being in a dream, a sense of the unreality or absence of a self, perceptual alterations, emotional and/or physical numbing, and an altered (typically dilated or slowed down) sense of the passage of time (Spiegel et al., Citation2011, Citation2013). It therefore becomes relevant to also examine how often these additional phenomena occur in persons with PTSD.
Relevant to such developments, Frewen and Lanius (Citationin press) recently proposed a four-dimensional framework (4-D model; see ) that theoretically differentiates states of posttraumatic distress that they argue intrinsically exemplify trauma-related altered states of consciousness (TRASC) from those that do not. The 4-D model was developed with reference to philosophical work in phenomenology (e.g., Thompson & Zahavi, Citation2007) and neurophysiological studies of altered states of consciousness (e.g., Vaitl et al., Citation2005). In essence, the 4-D model classifies clinically significant symptoms of temporal-memory, cognitive, bodily, and emotional disturbance into either those that remain exemplary of normal waking consciousness (NWC) or those that intrinsically exemplify TRASC; only TRASC, therefore, are regarded as fundamentally dissociative in nature by the 4-D model.
FIGURE 1 The 4D-model of the traumatized self. Notes. Posttraumatic symptom dimensions of the consciousness of time, thought, body, and emotion are differentiated in so far as they present in trauma-related altered states of consciousness (TRASC) form (red, top) versus in normal waking conscious (NWC) form (blue, bottom). The background coloring of the two states, however, is illustrated as blending into one another in order to represent that it is presently not known whether the difference between the TRASC and NWC forms is a qualitative (categorical) or only quantitative (dimensional) one. The arrow that is increasing in infrequency from bottom (NWC) to top (TRASC) represents the first hypothesis that symptom endorsements of TRASC are expected to be less frequent than symptom endorsements of NWC distress. The arcs connecting the four dimensions are drawn with greater weight when referring to NWC distress versus TRASC in order to represent the second hypothesis that the experience of forms of NWC will be more intercorrelated when compared with the experience of forms of TRASC. The arrow labeled “dissociative” that is increasing from bottom (NWC) to top (TRASC) is intended to illustrate the third hypothesis that the four dimensions in TRASC form, while being distinct in concept from the measurement of dissociation as a disintegration and/or compartmentalization of psychological functions (e.g., Holmes et al., Citation2005; Steele et al., Citation2009), will nevertheless be more often observed in people who also experience dissociative disintegration and/or compartmentalization of psychological functions. Finally, the arrow labeled “Developmental TE [Trauma Exposure],” oriented in the same direction, is intended to illustrate the hypothesis that the etiology of TRASC may often be developmental in origin, that is to say, typically requires repeated trauma exposure at an early age of onset, when a child’s brain is naturally more vulnerable to deviations from NWC such as is normally exhibited through age-appropriate imaginary play.©W. W. Norton and Company. Reproduced with the permission of W. W. Norton and Company. Permission to reuse must be obtained from the rightsholder.
![FIGURE 1 The 4D-model of the traumatized self. Notes. Posttraumatic symptom dimensions of the consciousness of time, thought, body, and emotion are differentiated in so far as they present in trauma-related altered states of consciousness (TRASC) form (red, top) versus in normal waking conscious (NWC) form (blue, bottom). The background coloring of the two states, however, is illustrated as blending into one another in order to represent that it is presently not known whether the difference between the TRASC and NWC forms is a qualitative (categorical) or only quantitative (dimensional) one. The arrow that is increasing in infrequency from bottom (NWC) to top (TRASC) represents the first hypothesis that symptom endorsements of TRASC are expected to be less frequent than symptom endorsements of NWC distress. The arcs connecting the four dimensions are drawn with greater weight when referring to NWC distress versus TRASC in order to represent the second hypothesis that the experience of forms of NWC will be more intercorrelated when compared with the experience of forms of TRASC. The arrow labeled “dissociative” that is increasing from bottom (NWC) to top (TRASC) is intended to illustrate the third hypothesis that the four dimensions in TRASC form, while being distinct in concept from the measurement of dissociation as a disintegration and/or compartmentalization of psychological functions (e.g., Holmes et al., Citation2005; Steele et al., Citation2009), will nevertheless be more often observed in people who also experience dissociative disintegration and/or compartmentalization of psychological functions. Finally, the arrow labeled “Developmental TE [Trauma Exposure],” oriented in the same direction, is intended to illustrate the hypothesis that the etiology of TRASC may often be developmental in origin, that is to say, typically requires repeated trauma exposure at an early age of onset, when a child’s brain is naturally more vulnerable to deviations from NWC such as is normally exhibited through age-appropriate imaginary play.©W. W. Norton and Company. Reproduced with the permission of W. W. Norton and Company. Permission to reuse must be obtained from the rightsholder.](/cms/asset/bc8ddcca-183b-4792-a281-8e8af1540f0f/wjtd_a_873377_f0001_oc.jpg)
For a fuller discussion of the 4-D model, readers should consult Frewen and Lanius (Citationin press); only a summary overview can be accomplished herein. In brief, the 4-D model classifies (a) dissociative flashbacks as TRASC of a person’s sense of time-memory, considered distinct from other NWC forms of intrusive recall of traumatic events that fail to provoke a marked sense of reliving (e.g., Brewin, Gregory, Lipton, & Burgess, Citation2010); (b) thoughts that occur in second-person perspective, akin to voice hearing (e.g., experiencing a voice inside one’s head screaming “I hate you”; e.g., Beaven, Read, & Cartwright, Citation2011; Longden, Madill, & Waterman, Citation2012), as TRASC of thought demarcated from the NWC experience of having distressing thoughts in first-person perspective (e.g., having the thought “I hate myself”); (c) experiences of depersonalization as TRASC of the body, theoretically differentiated from embodied experiences of distress (i.e., as occur in NWC; e.g., psychophysiological arousal, panic attacks without depersonalization/derealization experiences); and (d) marked cases of emotional numbing and affective shutdown as TRASC of emotion (akin to a feeling of being numb [Frewen, Dozois, et al., Citation2012] or emotionless), considered unique as such relative to other states of emotion dysregulation (and pervasive emotional states; Friedman et al., Citation2011) that can occur within NWC (e.g., experiences of fear, anxiety, sadness, guilt, or shame).
In addition, the 4-D model also makes four explicit hypotheses (Frewen & Lanius, Citationin press). Specifically, within traumatized persons, symptoms of TRASC, compared with NWC forms of distress, are predicted to be (a) observed less frequently (because of NWC, by definition, being the more frequent psychological state of human beings even in states of distress, and consistent with the majority of persons with PTSD not being diagnosed with the dissociative subtype in past research; Stein et al., Citation2013; Steuwe, Lanius, & Frewen, Citation2012; Wolf, Lunney, et al., Citation2012; Wolf, Miller, et al., Citation2012); (b) less intercorrelated, especially as measured as moment-to-moment states (being that the four dimensions are theoretically held to be less integrated, or more compartmentalized [Brown, Citation2006; Holmes et al., Citation2005] when expressed as TRASC); (c) observed more often in people high in dissociative experiences as measured independently, such as via the Dissociative Experiences Scale (DES; E. M. Bernstein & Putnam, Citation1986); and (d) observed more frequently specifically in people who have experienced repeated trauma, especially at a young age, because of the presumed particularly harmful effects of early traumatization on the development of reality orientation (e.g., Carrick, Quas, & Lyon, Citation2010) and sense of self (Cicchetti & Lynch, Citation1995; Cole & Putnam, Citation1992; Putnam, Citation1990).
The 4-D model was presented as a hypothesis requiring empirical evaluation, although to our knowledge no study has yet evaluated the four aforementioned hypotheses made by the 4-D model (Frewen & Lanius, Citationin press). Accordingly, we sought out to preliminarily evaluate the four principal predictions of the 4-D model in a study of 74 women with PTSD predominantly related to childhood abuse who had been recruited via community advertisement. Such a sample is of particular relevance given that early life trauma has been proportionately more frequently associated with the dissociative subtype of PTSD in past research (Steuwe et al., Citation2012; Wolf, Lunney, et al., Citation2012; Wolf, Miller, et al., Citation2012; cf. Stein et al., 2012). The first and second hypotheses of the 4-D model were also explored in a second convenience sample of 504 undergraduate students.
STUDY 1
Method
Participants
A total of 74 women ages 22 to 55 (M = 40.22, SD = 8.34) who met Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM–IV–TR) diagnostic criteria for PTSD as assessed by the Clinician-Administered PTSD Scale (CAPS; Blake et al., Citation1995) took part in this study. In some cases analyses refer to a subsample because of missing data (for all analyses n ≥ 70). Prior study exclusion criteria, in order to increase sample homogeneity and ensure confidence that the primary diagnosis in comorbid samples was that of PTSD, were past/present diagnoses of bipolar I or II, any psychotic disorder, as well as present substance abuse disorders as assessed by the Structured Clinical Interview for DSM–IV. All participants were also required to report at least a moderate level of PTSD symptom severity as operationalized by the total severity ≥45 scoring rule for the CAPS (Weathers, Ruscio, & Keane, Citation1999). Participants were predominantly Caucasian (77%), and marital status was as follows: separated/divorced (41%), single (32%), married/common law (22%), remaining marital status unspecified. Most participants had graduated from secondary school (79%), with 60% obtaining some level of postsecondary education. A substantial minority (41%) were currently working in some capacity at the time of the study.
Participants exhibited varying levels of PTSD symptom severity (CAPS scores ranged from 48 to 120; M = 76.82, SD = 17.51) and dissociation (DES scores [E. M. Bernstein & Putnam, Citation1986] ranged from 1 to 90; M = 23.50, SD = 18.58). Previous research (Steuwe et al., Citation2012; Wolf, Lunney, et al., Citation2012; Wolf, Miller, et al., Citation2012) has operationalized the presence versus absence of the dissociative subtype of PTSD via endorsement of the depersonalization and/or derealization item(s) of the CAPS (frequency ≥ 1, intensity ≥ 2 scoring rule; Weathers et al., Citation1999). By the same convention, 32 participants (43%) in the present sample would have been diagnosed with the dissociative subtype of PTSD. Many participants reported severe histories of childhood maltreatment as assessed retrospectively by the short form (28-item version) of the Childhood Trauma Questionnaire (CTQ; D. P. Bernstein et al., Citation2003). Specifically, CTQ subscale scores were distributed as follows: Total (range = 25–122, M = 78.32, SD = 21.72), Sexual Abuse (range = 5–25, M = 16.25, SD = 7.91), Physical Abuse (range = 5–25, M = 13.17, SD = 6.11), Emotional Abuse (range = 5–25, M = 18.75, SD = 5.32), Emotional Neglect (range = 5–25, M = 17.99, SD = 4.94), and Physical Neglect (range = 5–25, M = 13.17, SD = 6.11). Participants evidenced a range of comorbid psychiatric diagnoses, most notably major depression (current: n = 46, 62%; past: n = 19, 25%), panic disorder with/without agoraphobia (n = 22, 30%), social anxiety disorder (n = 22, 30%), and undifferentiated somatoform disorder (n = 10, 14%) as assessed by the Structured Clinical Interview for DSM–IV; other comorbid disorders occurred in less than 10% of the sample. Nearly all participants were assessed as part of a study investigating the subjective and neural correlates of socioemotional imagery, the primary results of which were published previously (e.g., Frewen et al., Citation2010).
Measures
CAPS
The CAPS (Blake et al., Citation1995) is widely considered to be the gold standard in semistructured diagnostic interviews for PTSD. The CAPS was used to assess both the past-month frequency and intensity of each of the DSM–IV PTSD symptoms as well as the experience of depersonalization.
DES
The DES (E. M. Bernstein & Putnam, Citation1986) is a widely known and utilized 28-item measure of dissociative experiences.
CTQ–Short Form
The CTQ (D. P. Bernstein & Fink, Citation1998; D. P. Bernstein et al., Citation2003) is a widely known and population standardized retrospective measure of a person’s experience of abuse and neglect during childhood and adolescence. The CTQ has five subscales (5 items per subscale): Emotional Neglect, Emotional Abuse, Sexual Abuse, Physical Abuse, and Physical Neglect.
Cognitive Distortion Scales
The Cognitive Distortion Scales (Briere, Citation2000) is a population standardized 40-item questionnaire assessing the past-month frequency (from never to very often) of participants’ experiences of negative cognition associated with five different themes, specifically self-criticism, hopelessness, helplessness, self-blame, and preoccupation with danger. Construct validity evidence includes not only correlations with similar scales but also the fact that scores were predictive of PTSD severity and brain responses during trauma memory recall in a longitudinal study (Daniels et al., Citation2011). Only self-criticism scores (e.g., “putting yourself down,” “hating yourself”) were examined in this study.
Multiscale Dissociation Inventory
The Multiscale Dissociation Inventory (Briere, Citation2002; Briere et al., Citation2005) is a population standardized 30-item measure of dissociative symptoms, specifically of experiences of dissociative disengagement, depersonalization, derealization, emotional constriction, memory disturbance, and identity dissociation. Only items from the identity dissociation subscale (e.g., “feeling like two or more people were fighting or arguing inside of yourself”) were examined in this study.
Feeling of being emotionally numb
Four items (α = .94) were administered to assess participants’ experience of feeling emotionally numb over the past month as previously described by Frewen, Dozois, et al. (Citation2012). An example item is “You’ve felt emotionally ‘numb,’ as if you can’t experience emotions or feelings”). Participants’ agreement with and/or past-month frequency of experience of such items was assessed on a 0–10 scale. Construct validity evidence for the items includes correlations with alexithymia and PTSD symptoms as well as their prediction of brain responses occurring during socioemotional imagery (Frewen, Dozois, et al., Citation2012).
Negative emotional states
Six relatively straightforward items were administered in order to assess the frequency of participants’ experience of negative emotions over the past month. The same 0–10 item anchors used to assess the feeling of being emotionally numb were used to assess these negative emotions. The negative emotional states assessed were (a) “sadness, misery, and despair,” (b) “fear, terror, and panic,” (c) “anxiety (nervous agitation, worrying),” (d) “irritability/anger,” (e) “guilt,” and (f) “humiliation and shame” (α = .81).
Procedure
Participants were interviewed by trained diagnosticians with MSc degrees in psychology or higher, as supervised by the authors. Participants completed the indicated questionnaires as part of a study investigating the subjective and neural correlates of socioemotional imagery (Frewen et al., 2010). The ethics of the study procedure were approved by an institutional review board.
Data Reduction
To operationalize symptoms exemplary of NWC versus TRASC of the dimensions of (a) time-memory, (b) thought, (c) body, and (d) emotion, we compared the frequency of response to psychological test items representing what we considered to approximate, as best as was available from the literature, the NWC versus TRASC variants of these dimensions as specified by the 4-D model. To directly compare item frequencies between scales (i.e., paired means), use of the same rating scale (i.e., identical Likert scale item anchors) is obviously essential. Fortunately we were able to locate in the literature, or developed for the present study, internally reliable measures of each of the four symptom dimensions in their NWC versus TRASC forms that utilized the same item anchors as previously described in the “Measures” section and outlined in . Across subscales, item endorsements were averaged rather than summed in order to afford paired tests of means between subscales that were composed of differing numbers of items. Internal consistency across item endorsements within subscales was uniformly high (α > .80). Please see for a description of the questionnaires administered in order to operationalize the experience of distressing NWC versus TRASC forms of the time-memory, thought, body, and emotion dimensions of the 4-D model.
TABLE 1 Operational Measures of Posttraumatic Symptomatology Exemplary of Nondissociative Distress (NWC) versus Dissociative Distress (TRASC) Referring to the 4-D Model Dimensions Time, Thought, Body, and Emotion in Study 1
Statistical Analysis
In order to evaluate our first hypothesis, that in traumatized persons, symptoms of TRASC, relative to NWC forms of distress, would be observed less frequently, paired tests of means compared frequency scores between the TRASC and NWC dimensions (i.e., akin to comparing across rows within ).
In order to evaluate our second hypothesis, that in traumatized persons, symptom co-occurrences would be less intercorrelated in TRASC than in NWC form, we calculated the mean intercorrelations between scales measuring the NWC and TRASC dimensions (i.e., akin to comparing the correlations observed among the measures occupying the cells of Column 1 with those occupying Column 2 within ).
In order to evaluate our third hypothesis, that symptoms of TRASC would be observed more often in people high in dissociative experiences as measured independently (e.g., referring to experiences of dissociative compartmentalization), we examined differences in the magnitude of correlations between the DES and each of the symptoms of NWC versus TRASC as well as conducted multiple regressions to examine whether symptoms of TRASC would be concurrently predictive of DES scores after we accounted for symptoms of NWC (and vice versa). For comparison purposes, we also conducted the same analyses with CAPS as the dependent measure.
Finally, in order to evaluate our fourth hypothesis, that symptoms of TRASC would be found more often specifically in people who have experienced repeated trauma, particularly at a young age, we examined correlations between symptoms of TRASC and responses to the CTQ (D. P. Bernstein et al., Citation2003).
Results
Hypothesis 1: Symptom Dimensions of TRASC Will Be Endorsed Less Frequently Than NWC Symptoms
Comparisons of the frequency ratings obtained for the NWC versus TRASC symptoms for each dimension of the 4-D model are presented in (blue vs. red bars, respectively). Consistent with predictions, in each case, NWC symptoms of distress were endorsed more frequently than were TRASC. See for statistics; all comparisons were highly statistically significant (p < .001) and yielded effect sizes in the large range (d′ > .80).
FIGURE 2 Posttraumatic symptom dimensions of the consciousness of time, thought, body, and emotion are endorsed less frequently in trauma-related altered states of consciousness (TRASC) form (red) than in normal waking consciousness (NWC) form (blue) (data from Study 1). Notes. Please see for survey items used to operationalize each symptom dimension. Error bars denote SD which is also reported in brackets. Differing degrees of freedom due to missing data.
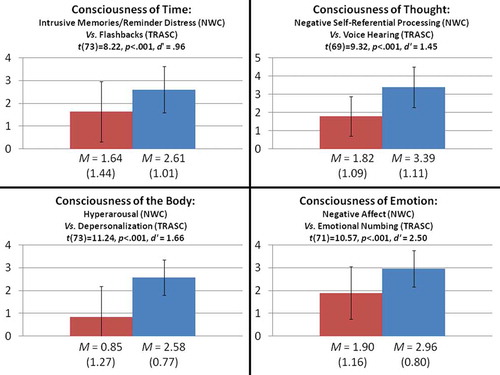
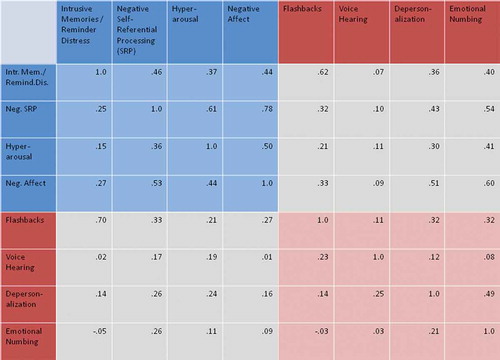
FIGURE 3 Posttraumatic symptom dimensions of the consciousness of time, thought, body, and emotion are less intercorrelated in trauma-related altered states of consciousness (TRASC) form (red) than in normal waking consciousness (NWC) form (blue). Notes. Please see and for survey items used to operationalize each symptom dimension. Results from Study 1 below diagonal, and results from Study 2 above the diagonal.
Hypothesis 2: Symptom Dimensions of TRASC Will Be Less Intercorrelated Than NWC Symptoms
presents the intercorrelations observed between the NWC and TRASC forms of each symptom dimension of the 4-D model for Study 1 participants (below the diagonal; results for Study 2 participants are presented above the diagonal). Referring to Study 1, consistent with predictions, NWC symptoms of distress were generally more highly intercorrelated (dark blue cells; range = .15 ≤ r ≤ .53, Mr = .33, SDr = .14) in comparison with symptoms of TRASC (dark red cells; range = –.03 ≤ r ≤ .25, Mr = .14, SDr = .11). Moreover, symptoms of TRASC were not strongly correlated, on average, with NWC symptoms of distress (grey cells; range = –.05 ≤ r ≤ .70, Mr = .19, SDr = .17), although flashbacks were generally more strongly correlated with NWC symptoms of distress than were other dimensions of TRASC, and in particular with other PTSD reexperiencing symptoms (r = .70, p < .001).
Hypothesis 3: Symptoms of TRASC Will Be Endorsed More Often by Persons High in Other Measures of Dissociation
Consistent with predictions, between-person variability in the frequency of experiencing TRASC was significantly correlated with DES scores (see for statistics; range = .20 ≤ r ≤ .58, Mr = .39, SDr = .18). In addition, in a two-step multiple regression analysis, the four TRASC symptom dimensions incremented over the four NWC forms of distress in accounting for variation in DES scores (ΔR2 = .31, total R2 = .49, Δp < .001). In comparison, symptoms defined as NWC within the 4-D model failed to incrementally predict variance in concurrent DES scores over symptoms defined as TRASC (ΔR2 = .04, total R2 = .49, Δp = .34).
FIGURE 4 Trait dissociation (Dissociative Experiences Scale; DES) is more strongly correlated with posttraumatic symptom dimensions of the consciousness of time, thought, body, and emotion in trauma-related altered states of consciousness (TRASC) form (red) than in normal waking consciousness (NWC) form (blue) (data from Study 1). Notes. Please see for survey items used to operationalize each symptom dimension. Error bars denote SD which is also reported in brackets. Differing degrees of freedom due to missing data.
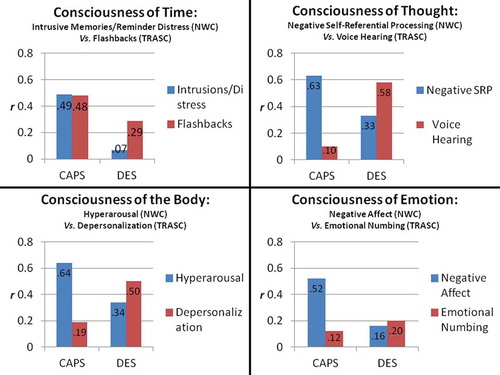
By comparison, although both TRASC and NWC symptom dimensions were concurrently associated with CAPS scores (see for statistics), NWC symptom dimensions were generally more strongly correlated with CAPS than were TRASC, and NWC symptom dimensions incremented over TRASC in accounting for variation in CAPS scores (ΔR2 = .43, total R2 = .66, Δp < .001). In comparison, TRASC symptom dimensions failed to incrementally account over NWC distress in concurrently predicting CAPS scores (ΔR2 = .01, total R2 = .66, Δp = .67).
Hypothesis 4: Symptoms of TRASC Will Be Endorsed More Often Specifically by Repetitively Traumatized Persons, Particularly Those With More Extensive Histories of Childhood Abuse
Only a single association between endorsements of TRASC was found with CTQ Total scores, specifically voice hearing, r(71) = .20, p < .05. Follow-up analysis found that this correlation was specific to severity of childhood sexual abuse histories: r(71) = .27, p < .05. There were no other significant correlations associating CTQ scores with severity of symptoms, whether defined by the 4-D model as forms of distress exemplary of NWC or TRASC.
STUDY 2
Participants and Procedure
Responses from 504 undergraduate students (384 female, 75%) ranging in age from 17 to 48 (M = 20.52, SD = 3.65), amalgamated from two previously described samples (n = 225, Frewen, Allen, Lanius, & Neufeld, Citation2012; n = 229, Frewen, Schmittmann, Bringmann, & Borsboom, Citation2013), were reanalyzed in terms of their past-month frequency responses to a 40-item 7-point symptom rating scale that included face-valid items for each of the NWC and TRASC items of the 4-D model (please see the prior publications for psychometric validation of the item list). Based on responses collected from the first 225 such participants (from Frewen, Allen, et al., Citation2012) who also completed the Posttraumatic Diagnostic Scale (Foa, Cashman, Jaycox, & Perry, Citation1997), PTSD diagnosis was considered probable in approximately 11% of such participants. gives verbatim the survey items that were used to operationalize the NWC versus TRASC dimensions. Given that this sample was not administered a separate measure of dissociation or trauma exposure, Hypotheses 3 and 4 of the 4-D model could not be evaluated.
TABLE 2 Operational Measures of Posttraumatic Symptomatology Exemplary of Nondissociative Distress (NWC) versus Dissociative Distress (TRASC) Referring to the 4-D Model Dimensions Time, Thought, Body, and Emotion in Study 2
Results
Hypothesis 1: Symptom Dimensions of TRASC Will Be Endorsed Less Frequently Than NWC Symptoms
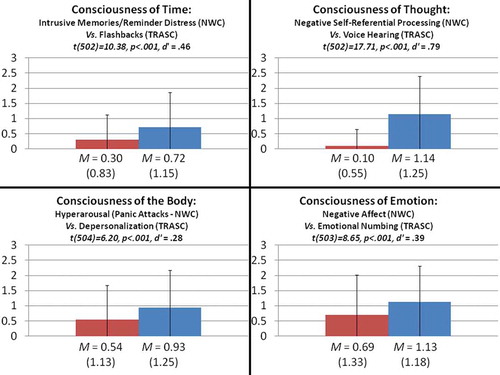
Comparisons of the frequency ratings obtained for the NWC versus TRASC symptoms for each dimension of the 4-D model are presented in (blue vs. red bars, respectively). Consistent with Study 1 results and predictions, NWC symptoms of distress were again endorsed more frequently than were TRASC. Please see for statistics; all comparisons were again highly statistically significant (p < .001) and associated with effect sizes generally in the small to moderate range (.28 ≤ d′ ≤ .79).
FIGURE 5 Posttraumatic symptom dimensions of the consciousness of time, thought, body, and emotion are endorsed less frequently in trauma-related altered states of consciousness (TRASC) form (red) than in normal waking consciousness (NWC) form (blue) (data from Study 2). Notes. Please see for survey items used to operationalize each symptom dimension. Error bars denote SD which is also reported in brackets. Differing degrees of freedom due to missing data.
Hypothesis 2: Symptom Dimensions of TRASC Will Be Less Intercorrelated Than NWC Symptoms
(above the diagonal) presents the intercorrelations observed between the NWC and TRASC forms of each symptom dimension of the 4-D model. Consistent with Study 1 results and predictions, NWC symptoms of distress were again more highly intercorrelated (dark blue cells; range = .37 ≤ r ≤ .78, Mr = .53, SDr = .15) in comparison with symptoms of TRASC (dark red cells; range = .08 ≤ r ≤ .49, Mr = .24, SDr = .16). Symptoms of TRASC were also generally not strongly correlated, on average, with NWC symptoms of distress (grey cells; range = .07 ≤ r ≤ .62, Mr = .35, SDr = .18), particularly in the case of voice hearing.
GENERAL DISCUSSION
The 4-D model (Frewen & Lanius, Citationin press) classifies forms of posttraumatic distress as either those potentially occurring within NWC or those whose presence alone is considered to intrinsically exemplify dissociative forms of detachment—that is, TRASC. Four dimensions of consciousness are specified: time-memory, thought, body, and emotion. The present studies represent, to our knowledge, the first empirical exploration of the principal tenets of the 4-D model.
Support for the first two predictions of the 4-D model, that experiences of TRASC would occur less frequently and would be less intercorrelated compared with distress associated with NWC, was obtained across both samples. Hypothesis 3, that experiences of TRASC would be more strongly associated with independent measures of dissociation, also received empirical support as tested in female participants with PTSD predominantly related to childhood abuse. In fact, TRASC incremented in predicting concurrent dissociative experiences beyond data describing participants’ level of NWC distress, whereas PTSD symptom severity, as a whole, was more strongly associated with symptoms of distress that the 4-D model classifies as NWC, with the exception of the case of reexperiencing symptoms.
Given that experiences of TRASC are not fully accounted for by other forms of PTSD symptomatology in their association with other measures of dissociation, including experiences of compartmentalization, and that experiences of TRASC are correlated with but clearly unique from PTSD symptomatology associated with NWC, the present findings provide further argument for recognizing a dissociative subtype of PTSD (Carlson et al., Citation2012; Dalenberg & Carlson, Citation2012; Ginzburg et al., Citation2006; Lanius et al., Citation2010, Citation2012; Spiegel et al., Citation2011, Citation2013). They also support further investigations of experiences of depersonalization (e.g., Sierra, Baker, Medford, & David, Citation2005) and depersonalization–derealization disorder (e.g., Spiegel et al., Citation2011, Citation2013) as multidimensional psychological phenomena or syndromes.
In comparison, findings generally failed to support the 4-D model prediction of a specific role for repeated developmental trauma exposure in the genesis of TRASC as evaluated within traumatized women (Study 1). Extent of childhood trauma history was statistically unrelated to symptom severity in Study 1, excepting for an association between extent of childhood sexual abuse history and an increased experience of voice hearing (and/or identity dissociation; Briere, Citation2002; Briere et al., Citation2005) during adulthood. Clearly a robust association exists linking early trauma exposure with the development of dissociative symptoms as assessed in adulthood (review by Dalenberg et al., Citation2012). However, few studies have compared the degree to which distinct dimensions of dissociative experience covary with repeated developmental trauma exposure. The present findings highlight voice hearing, perhaps more so than flashbacks, depersonalization, and emotional numbing, as a form of TRASC that may be a particularly specific long-term outcome of frequent childhood sexual abuse, in line with several other studies (e.g., Dorahy et al., Citation2009; reviews by Beaven et al., Citation2011; Longden et al., Citation2012). However, we also recommend that future studies investigating TRASC as a possible long-term outcome of adverse childhood experiences include a more thorough assessment of early experience than that afforded by the CTQ—for example, also including measures of unresponsive parenting and attachment dysregulation known to be predictive of dissociative symptoms in longitudinal designs (e.g., Bureau, Martin, & Lyons-Ruth, Citation2010; Ogawa, Sroufe, Weinfield, Carlson, & Egeland, Citation1997). In addition, some individuals may be inherently more vulnerable to TRASC in the context of trauma exposure, and Gene × Environment interactions should be taken into account (e.g., Meaney, Citation2010). Finally, analyses should examine the specificity rather than only the simple correlation between measures of repeated childhood maltreatment history and TRASC as pertains more directly to the fourth hypothesis of the 4-D model.
Limitations of the present studies should be addressed in future research. Our samples were restricted to adult women with a primary diagnosis of PTSD (Study 1) and predominantly female undergraduate students (Study 2); generalization of our findings to men and persons with other trauma-related disorders may be inappropriate. We envision the 4-D model as a transdiagnostic approach to studying trauma-related disorders, including borderline personality disorder, dissociative disorders, and even mood disorders, and therefore recommend that additional studies be conducted within other diagnostic groups. In addition, in the present studies assessments of TRASC were undertaken at only a single point in time via clinician rating or retrospective self-report questionnaires, and in several instances in response to only a single question, thereby calling into possible concern the psychometric reliability of the assessments as well as the influence of method variance. Moreover, the validity of the measures used as operationalizations of the constructs specified by the 4-D model remains in question. Future work might derive operationalizations of the 4-D model dimensions from factor analyses of other existing questionnaires or develop a psychometric scale designed specifically as a measure of TRASC of time-memory, thought, body, and emotion. Experimental-behavioral assessments of TRASC should also be investigated, for example the rubber hand illusion (Botvinick & Cohen, Citation1998) as a measure of partial disembodiment as induced by a multisensory perceptual illusion. It has also been argued that differentiating between dissociative and nondissociative presentations of trauma symptoms may be clinically significant in that tendencies toward dissociation during trauma memory reprocessing may interfere with standard exposure-based treatments of PTSD and borderline personality disorder, although evidence to date is mixed (cf. Cloitre, Petkova, Wang, & Lu, Citation2012; Hagenaars, van Minnen, & Hoogduin, Citation2010; Resick, Suvak, Johnides, Mitchell, & Iverson, Citation2012); research using measures specific to different dimensions of TRASC might prove more sensitive as a predictor of treatment outcome. Finally, although diagnostic systems in psychiatry continue to emphasize phenomenology, they have historically been little influenced by formal developments in consciousness studies or neurophenomenology (Varela, Citation1996); the assessment of objective neurobiological markers of the moment-to-moment experience of TRASC via such methods may better researchers’ understanding not only of dissociation and TRASC but also of consciousness itself.
Related Research Data
REFERENCES
- Beavan, V., Read, J., & Cartwright, C. (2011). The prevalence of voice-hearers in the general population: A literature review. Journal of Mental Health, 20(3), 281–292. doi: 10.3109/09638237.2011.562262
- Bernstein, D. P., & Fink, L. (1998). Childhood Trauma Questionnaire: A retrospective self-report. San Antonio, TX: Psychological Corporation.
- Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, R., … Zule, W. (2003). Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse & Neglect, 27, 169–190. doi: 10.1016/S0145-2134(02)00541-0
- Bernstein, E. M., & Putnam, F. W. (1986). Development, reliability, and validity of a dissociation scale. Journal of Nervous and Mental Disease, 174, 727–735. doi: 10.1097/00005053-198612000-00004
- Blake, D. D., Weathers, F. W., Nagy, L. M., Kaloupek, D. G., Gusman, F. D., Charney, D. S., & Teane, T. M. (1995). The development of a Clinician-Administered PTSD Scale. Journal of Traumatic Stress, 8, 75–90. doi: 10.1007/BF02105408
- Botvinick, M., & Cohen, J. (1998, February 19). Rubber hands “feel” touch that eyes see. Nature, 391, 756. doi: 10.1038/35784
- Brewin, C. R., Gregory, J. D., Lipton, M., & Burgess, N. (2010). Intrusive images in psychological disorders: Characteristics, neural mechanisms, and treatment implications. Psychological Review, 117(1), 210–232. doi: 10.1037/a0018113
- Briere, J. (2000). Cognitive Distortion Scales. Lutz, FL: Psychological Assessment Resources.
- Briere, J. (2002). Multiscale Dissociation Inventory. Lutz, FL: Psychological Assessment Resources.
- Briere, J., Weathers, F. W., & Runtz, M. (2005). Is dissociation a multidimensional construct? Data from the Multiscale Dissociation Inventory. Journal of Traumatic Stress, 18, 221–231. doi: 10.1002/jts.20024
- Brown, R. J. (2006). Different types of “dissociation” have different psychological mechanisms. Journal of Trauma & Dissociation, 7(4), 7–28. doi:10.1300/J229v07n04_02
- Bureau, J.-F., Martin, J., & Lyons-Ruth, K. (2010). Attachment dysregulation as hidden trauma in infancy: Early stress, maternal buffering and psychiatric morbidity in young adulthood. In R. A. Lanius, E. Vermetten, & C. Pain ( Eds.), The impact of early life trauma on health and disease: The hidden epidemic ( pp. 48–56). New York, NY: Cambridge University Press.
- Carlson, E. B., Dalenberg, C., & McDade-Montez, E. (2012). Dissociation in posttraumatic stress disorder part I: Definitions and review of research. Psychological Trauma: Theory, Research, Practice, and Policy, 4, 479–489. doi:10.1037/a0027748
- Carrick, N., Quas, J. A., & Lyon, T. (2010). Maltreated and nonmaltreated children’s evaluations of emotional fantasy. Child Abuse & Neglect, 34, 129–134. doi:10.1016/j.chiabu.2009.02.009
- Cicchetti, D., & Lynch, M. (1995). Failures in the expectable environment and their impact on individual development: The case of child maltreatment. In D. Cicchetti & D. Cohn ( Eds.), Developmental psychopathology ( Vol. 2, pp. 32–71). New York, NY: Wiley-Interscience.
- Cloitre, M., Petkova, E., Wang, J., Lu, L. F. (2012). An examination of the influence of a sequential treatment on the course and impact of dissociation among women with PTSD related to childhood abuse. Depression and Anxiety, 29(8), 709–17. doi: 10.1002/da.21920
- Cole, P. M., & Putnam, F. W. (1992). Effect of incest on self and social functioning: A developmental psychopathological perspective. Journal of Consulting & Clinical Psychology, 60, 174–184. doi:10.1037/0022-006X.60.2.174
- Dalenberg, C. A., Brand, B. L., Gleaves, D. H., Dorahy, M. J., Loewenstein, R. J., Cardeña, E., … Spiegel, D. (2012). Comparison of the trauma and fantasy models of dissociation. Psychological Bulletin, 138, 550–588. doi:10.1037/a0027447
- Dalenberg, C., & Carlson, E. B. (2012). Dissociation in posttraumatic stress disorder part II: How theoretical models fit the empirical evidence and recommendations for modifying the diagnostic criteria for PTSD. Psychological Trauma: Theory, Research, Practice, & Policy, 4(6), 551–559. doi: 10.1037/a0027900
- Daniels, J. K., Hegadoren, K., Coupland, N. J., Rowe, B. H., Neufeld, R. W. J., & Lanius, R. A. (2011). Cognitive distortions in an acutely traumatized sample: An investigation of predictive power and neural correlates. Psychological Medicine, 41, 2149–2157. doi:10.1017/S0033291711000237
- Dell, P. F., & Lawson, D. (2009). An empirical delineation of the domain of pathological dissociation. In P. F. Dell and J. A. O’Neil (Eds.) Dissociation and the Dissociative Disorders (pp. 667–692). New York, NY: Routledge.
- Dorahy, M. J., Shannon, C., Seagar, L., Corr, M., Stewart, K., Hanna, D., … Middleton, W. (2009). Auditory hallucinations in dissociative identity disorder and schizophrenia with and without a childhood trauma history: Similarities and differences. Journal of Nervous & Mental Disease, 197, 892–898. doi:10.1097/NMD.0b013e3181c299eaXXX
- Foa, E. B., Cashman, I., Jaycox, L., & Perry, K. (1997). The validation of a self-report measure of posttraumatic stress disorder: The Posttraumatic Stress Diagnostic Scale. Psychological Assessment, 9, 445–451. doi: 10.1037/1040-3590.9.4.445
- Frewen, P. A., Allen, S. A., Lanius, R. A., & Neufeld, R. W. J. (2012). Measuring perceived symptom causal relations: Examination with posttraumatic stress, depression, and anxiety symptomatology. Assessment, 19, 480–493. doi:10.1177/1073191111418297
- Frewen, P. A., Dozois, D. J. A., Neufeld, R. W. J., Densmore, M., Stevens, T. K., & Lanius, R. A. (2010). Social emotions and emotional valence during imagery in women with PTSD: Affective and neural correlates. Psychological Trauma: Theory, Research, Practice, & Policy, 2(2), 145–157. doi:10.1037/a0019154
- Frewen, P. A., Dozois, D. J. A., Neufeld, R. W. J., Lane, R. D., Densmore, M., Stevens, T. K., & Lanius, R. A. (2012). Emotional numbing in PTSD: An fMRI study. Journal of Clinical Psychiatry, 73, 431–436. doi:10.4088/JCP.10m06477
- Frewen, P. A., & Lanius, R. A. (in press). Healing the traumatized self: Consciousness, neuroscience, treatment. New York, NY: Norton.
- Frewen, P. A., Schmittmann, V. A., Bringmann, L. A., & Borsboom, D. (2013). Perceived causal relations between anxiety, posttraumatic stress and depression: Extension to moderation, mediation and network analysis. European Journal of Psychotraumatology, 4, 20656. doi:10.3402ejpt.v4i0.20656
- Friedman, M., Resick, P., Bryant, R., & Brewin, C. R. (2011). Considering PTSD for DSM–5. Depression and Anxiety, 28, 750–769. doi:10.1002/da.20767
- Ginzburg, K., Koopman, C., Butler, L. D., Palesh, O., Kraemer, H. C., Classen, C. H., & Spiegel, D. (2006). Evidence for a dissociative subtype of post-traumatic stress disorder among help-seeking childhood sexual abuse survivors. Journal of Trauma & Dissociation, 7, 7–27. doi:10.1300/J229v07n02_02
- Hagenaars, M. A., van Minnen, A., & Hoogduin, K. A. L. (2010). The impact of dissociation and depression on the efficacy of prolonged exposure treatment for PTSD. Behaviour Research and Therapy, 48, 19–27. doi: 10.1016/j.brat.2009.09.001
- Holmes, E. A., Brown, R. J., Mansell, W., Fearon, R. P., Hunter, E. C. M., Frasquilho, F., & Oakley, D. A. (2005). Are there two qualitatively distinct forms of dissociation? A review and some clinical implications. Clinical Psychology Review, 25(1), 1–23. doi:10.1016/j.cpr.2004.08.006
- Lanius, R. A., Brand, B., Vermetten, E., Frewen, P. A., & Spiegel, D. (2012). The dissociative subtype of posttraumatic stress disorder: Rationale, clinical and neurobiological evidence, and implications. Depression & Anxiety, 29, 701–708. doi:0.1002/da.21889
- Lanius, R. A., Vermetten, E., Loewenstein, R. J., Brand, B., Schmahl, C., Bremner, J. D., & Spiegel, D. (2010). Emotion modulation in PTSD: Clinical and neurobiological evidence for a dissociative subtype. American Journal of Psychiatry, 167, 640–647. doi:10.1176/appi.ajp.2009.09081168
- Longden, E., Madill, A., & Waterman, M. (2012). Dissociation, trauma, and the role of lived experience: Toward a new conceptualization of voice hearing. Psychological Bulletin, 138(1), 28–76. doi:10.1037/a0025995
- Meaney, M. J. (2010). Epigenetics and the biological definition of gene × environment interactions. Child Development, 81, 41–79. doi:10.1111/j.1467-8624.2009.01381.x
- Ogawa, J. R., Sroufe, L. A., Weinfield, N. S., Carlson, E. A. & Egeland, B. (1997). Development and the fragmented self: A longitudinal study of dissociative symptomatology in a non-clinical sample. Development & Psychopathology, 9, 855–879. doi: 10.1017/S0954579497001478
- Putnam, F. W. (1990). Disturbances of “self” in victims of childhood sexual abuse. In R. P. Kluft ( Ed.), Incest-related syndromes of adult psychopathology ( pp. 113–133). Washington, DC: American Psychiatric Press.
- Resick, P. A. Suvak, M. K., Johnides, B. D., Mitchell, K. S., & Iverson, K. S. (2012). The impact of dissociation on PTSD treatment with cognitive processing therapy. Depression and Anxiety, 29(8), 718–730. doi: 10.1002/da.21938
- Sierra, M., Baker, D., Medford, N., & David, A. S. (2005). Unpacking the depersonalization syndrome: An exploratory factor analysis of the Cambridge Depersonalization Scale. Psychological Medicine, 35, 1523–1532. doi: 10.1017/S0033291705005325
- Spiegel, D., Lewis-Fernández, R., Lanius, R., Vermetten, E., Simeon, D., & Friedman, M. (2013). Dissociative disorders in DSM–5. Annual Review of Clinical Psychology, 9, 299–326. doi: 10.1146/annurev-clinpsy-050212-185531
- Spiegel, D., Loewenstein, R. J., Lewis-Fernandez, R., Sar, V., Simeon, D., Vermetten, E., … Dell, P. F. (2011). Dissociative disorders in DSM–5. Depression and Anxiety, 28(12), 17–45. doi:10.1002/da.20923
- Steele, K., Dorahy, M. J., van der Hart, O., & Nijenhuis, E. R. S. (2009). Dissociation versus alterations in consciousness: Related but different concepts. In P. F. Dell, & J. A. O’Neil (Eds.), Dissociation and the dissociative disorders (pp. 155–169). New York, NY: Routledge/Taylor & Francis Group.
- Stein, D. J. Koenen, K. C., Friedman, M. J., Hill, E., McLaughlin, K., Petukhova, M., . . . Kessler, R. C. (2013). Dissociation in posttraumatic stress disorder: Evidence from the World Mental Health Surveys. Biological Psychiatry, 73, 302–312. doi:10.1016/j.biopsych.2012.08.022
- Steuwe, C., Lanius, R. A., Frewen, P. A. (2012). Evidence for a dissociative sybtype of PTSD by latent profile and confirmatory factor analysis in a civilian sample. Depression & Anxiety, 29(8), 689–700. doi: 10.1002/da.21944
- Thompson, E., & Zahavi, D. (2007). Philosophical issues: Phenomenology. In P. D. Zelazo, M. Moscovitch, & E. Thompson ( Eds.), Cambridge handbook of consciousness studies ( pp. 67–87). New York, NY: Cambridge University Press.
- Vaitl, D., Birbaumer, N., Gruzelier, J., Jamieson, G. A., Kotchoubey, B., Kübler, A., & Weiss, T. (2005). Psychobiology of altered states of consciousness. Psychological Bulletin, 131(1), 98–127. doi: 10.1037/0033-2909.131.1.98
- Varela, F. J. (1996). Neurophenomenology: A methodological remedy for the hard problem. Journal of Consciousness Studies, 3(4), 330–349.
- Weathers, F. W., Ruscio, A. M., & Keane, T. M. (1999). Psychometric properties of nine scoring rules for the Clinician-Administered Posttraumatic Stress Disorder Scale. Psychological Assessment, 11(2), 124–133. doi:10.1037/1040-3590.11.2.124
- Wolf, E. J. Lunney, C. A., Miller, M. W., Resick, P. A., Friedman, M. J., & Schnurr, P. P. (2012). The dissociative subtype of PTSD: A replication and extension. Depression & Anxiety, 29, 679–688. doi: 10.1002/da.21946
- Wolf, E. J., Miller, M., Rearon, A. F., Rybchenko, K. A., Castillo, D., & Freund, R. (2012). Latent class analysis of dissociation and PTSD: Evidence for a dissociative subtype. Archives of General Psychiatry, 69, 698–705. doi: 10.1001/archgenpsychiatry.2011.1574