
ABSTRACT
A prospective longitudinal mixed-method study was undertaken to evaluate an intergenerational community program involving older adults and school aged-children. Data were collected from nine children, and 18 non-frail, frail, and cognitively impaired older adults. Quantitative data collected from intergenerational interactions and self-ratings (0–10) assessed program satisfaction, while qualitative data included 89 session observations, and then both were integrated. Findings suggested that non-frail older adults interacted more verbally with children while the frail and cognitively impaired adults had mainly passive non-verbal interactions. The results indicated that promoting linguistic, emotional, and positive experiences for both generations led to their meaningful and satisfying relationships.
Introduction
Developed countries, such as Japan, are prime examples of aging populations with declining birth rates, resulting in some challenging consequences for health and well-being (Ministry of Internal Affairs and Communications of Japan, Citation2019; World Health Organization, Citation2018). Older and frail older adults are at risk of declining health, reduced social participation, and fewer relationships (Atchley, Citation2000; Kuzuya, Citation2012; The Japan Geriatrics Society, Citation2014; Xue, Citation2011). Also, fewer children have siblings from whom they can learn through first-hand experiences (McHale et al., Citation2012). With interpersonal relationships outside of the home weakening, both older adults and children have limited naturally occurring opportunities to engage with the community (Kusano et al., Citation2009). Instituting specific social programs may be necessary to maintain social relationships and interactions for older adults and children in the community.
Intergenerational programs where children and older adults engage socially have shown an increase in well-being and the prevention of possible social isolation for older adults, even in cases of neurocognitive impairment, and have had a positive impact on children (Gualano et al., Citation2018). The design of intergenerational group programs should focus on the reciprocal, relational, and social participatory needs of both generations. The characteristics of the participants such as frailty and neurocognitive disorders also have to be addressed to meet their various needs and to improve social interactions that facilitate generativity, reciprocity, and communication for the entire community. For instance, in fulfilling individual needs and satisfaction for older adults with moderate neurocognitive disorders through the program, continuous participation was effective in relieving depressive symptoms (Meguro & Kamei, Citation2018). Nevertheless, facilitating intergenerational interaction between frail, cognitively impaired older adults and children in the community has received little discussion.
To explore appropriate support for improving intergenerational interactions in diverse groups of older adults and children, a qualitative and quantitative mixed methods approach (Creswell, Citation2015; Tashakkori & Teddlie, Citation2010) could be useful to provide a deeper understanding through combining verbal and non-verbal, qualitative and quantitative interactions and the perceived satisfaction of each participant during the programs. Additionally, a means of expressing satisfaction with the program and the use of integrative approaches to assess the participants’ subjective experiences simultaneously are required.
Therefore, the purposes of this study were (a) to evaluate the intergenerational program process through observation and document the interactions of older adults (non-frail, frail, or with cognitive impairments) and school-aged children during a series of intergenerational community sessions; and (b) to qualitatively and quantitatively evaluate the levels of satisfaction and types of interaction emerging from the observations. The research question of this study was as follows: Are there differences in the quantity and quality of interactions and what is the level of satisfaction of each group participating in the program?
Theoretical background and conceptual framework of the study
The theoretical background of this study was based on a social interaction theory (Argyle, Citation1972). Based on Argyle’s theory, social interactions are facilitated through the following modes: conversation monitoring of the underlying emotion, the speed and tempo of interactions, reciprocity, developing closeness to other people, and talking about various subjects. In an intergenerational program, human growth and satisfaction are enhanced through social interactions that provide the experience of a range of feelings and cultures, and develop social and emotional facets in the lives of the participants (Eliopoulos, Citation2001). Verbal and non-verbal social interactions between older adults and school-aged children occur naturally in social relationships where each interprets what the other means and responds accordingly. However, older adults who are frail and cognitively impaired show a decrease in interpreting the verbal and non-verbal cues in these interactions as they care less about the interaction. Even if an older adult has a neurocognitive impairment, they should still be valued as a member of the family and community. They should be able to interact and connect with others, and as part of the natural order be shown recognition and respect (Eliopoulos, Citation2001).
Intergenerational programs are grounded in growth theories and theories of reciprocal and shared needs (Newman & Smith, Citation1997). These theories include the goals of creating relationships, improving social adjustment, deepening knowledge, improving functional and scholastic abilities, creating better mutual understanding, and providing benefits for both generations by creating greater self-respect (McCrea & Smith, Citation1997; Ward, Citation1997).
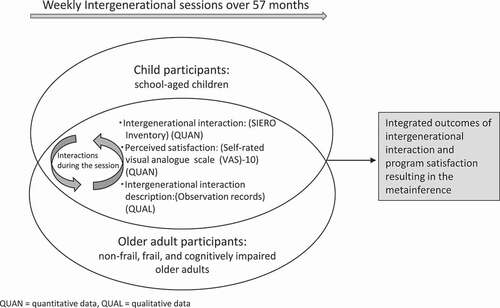
In this study, the researchers evaluated the process of a weekly intergenerational program focusing on the significance of interactions with participants of diverse ages and abilities. Perceived program satisfaction was used as a quantitative indicator and observations of both older adults’ and children’s intergenerational interactions as qualitative indicators. Both types of indicator were collected at each session, then the data were integrated and metainferred. The conceptual and study framework is shown in .
Figure 1. Conceptual framework of the study.
Methods
Study design
This prospective longitudinal mixed methods parallel convergent design (Creswell, Citation2015; Kakai, Citation2016; Plano-Clark, Citation2014; Teddlie & Tashakkori, Citation2009) included the following groups: older adults who were non-frail, frail, or had cognitive impairments, and school-age children. Qualitative and quantitative data were simultaneously collected through 89 sessions over a period of 57 months. The qualitative data were used to describe intergenerational interactions, and the quantitative data were used to measure the amount of intergenerational interactions and the perceived level of satisfaction. The procedural diagram of the mixed methods design is shown in .
Figure 2. Procedural diagram of the prospective longitudinal mixed methods parallel convergent design of the study.
Setting
The study field was an intergenerational program offered by the St. Luke’s College of Nursing University (St. Luke’s College of Nursing, Citation2008) to its surrounding community located in the Tokyo metropolitan area. The first author has been holding weekly on-going intergenerational programs for this community for over 13 years and provides volunteer and learning opportunities for nursing faculty, graduate students, and community members. The venue for the sessions was a multipurpose room at the university (Kamei et al., Citation2020).
Faculty members initiated the intergenerational program as a project for the development of people-centered care conducted through the 21st-century Center of Excellence program carried out by Japan’s Ministry of Education, Culture, Sports, Science and Technology (MEXT) (St. Luke’s College of Nursing, Citation2008). The purpose of the program was to promote mutual interaction and understanding across generations and create social capital. In recent years, a community care manager was introduced to the program to support older adult participants by means of informal community services. As the participants’ needs differed, individual support was required to pass on local culture and wisdom so that mixed generations would feel comfortable and trusting.
Participants
The study included adults aged 65 years and older: (a) non-frail (n = 8) living independently with no observable decline in their physical and cognitive functions; (b) frail (n = 6), in a vulnerable state with physical limitations including any one or all of the following: decreased physical strength, decreased activity level, decreased cognitive functions, or decreased psychological activity; (c) cognitively impaired (n = 4), such as Alzheimer’s disease, cognitive decline, and dementia as diagnosed by a physician; and (d) 7-to-12-year-old school-aged children who were in the first to sixth grades (n = 9). Older adults with medical conditions and children with learning disabilities were also accepted into the program. Owing to space limitations, registration was limited to 15 participants: 5 children and 10 older adults per year.
The eligibility criteria for the older adults were (a) being able to come to the program venue alone or with the help of their family, (b) having sufficient physical stamina to participate in the three-hour-long program without difficulty, and (c) having a mild to moderate neurocognitive impairment. Participants for the study were recruited through the distribution of flyers within the community and through a website for health-related community events operated by the university. The children included in the study were school-aged children from the first to sixth grades who could arrive independently at the program venue after school and whose parents gave consent. Nursing staff conducted detailed assessments of the physical and mental status of each participant at the first meeting and then reassessed them every three months.
Program
The weekly sessions were three hours long. The older adults began their session about 90 minutes before the children arrived from school. The children arrived at various times depending on their grade. Once there, they would join the session. In accordance with the people-centered care policy (Kamei et al., Citation2017), program providers and participants should have mutual understanding, trust, and respect. They should help each other and learn together through the same activities. Therefore, the sessions included a snack time and activities designed to incorporate the interests of both groups, such as intergenerational games, cooking, and traditional Japanese activities. Five to six staff members were involved in each session: one nursing staff who served as a session facilitator, two to three session management nursing staff, and two to three community volunteers. They guided the participants and provided direct support by sitting next to frail and cognitively impaired older adults who were in need of help with activities, eating, or going to the restroom.
Study procedure
Assessment of the participants
The nursing staff assessed the older adult participants to determine their suitability for activities during the first day of the program. They assessed their demographic status, family structure, and motivation for joining the program, as well as their physical, mental, and social state, and their usage of long-term care insurance services in Japan (e.g., a visiting nurse or home helper). Frailty was measured by assessing physical strength, activity level, cognitive functions, and social relations (Arai, Citation2014). The activities of daily living were assessed using the Barthel Index (0 = most dependent–20 = very independent) (Collin et al., Citation1987) and the researchers developed assessment forms that recorded diseases, medications, ailments, appetite, bathroom habits, and general condition. The frequency of going out into the community during the week was also noted. Cognitive functions were assessed using the Japanese N-Mental Status for Older Adults Scale (NM Scale) (Kobayashi & Nishimura, Citation2003). The NM Scale scores are classified as follows: severe (0–16), moderate (17–30), mild (31–42), borderline (43–47), and normal (50–48). The risk of falling was assessed using the Fall Risk Assessment (Flemming, Citation2006), with higher scores indicating a higher fall risk. Mental state was assessed using the Japanese version of the Geriatric Depression Scale (GDS)-15 (Kurlowicz & Greenberg, Citation2007; Niino et al., Citation1991). GDS-15 scores are interpreted as follows: no depression (0–4), mild depression (5–8), moderate depression (9–11), and severe depression (12–15). Social state was assessed through interviews. All of the participants were asked about their motivation for joining the program, the type of social participation in which they engaged, and the activities they enjoyed. The children freely reported their perceptions of the older adults, which were documented.
Measurements
Qualitative measures
The qualitative data came from observing behavior, attitudes, and dialogs during sessions. An ethnographic methodology guided the participant observation (Roper & Shapira, Citation2000). Seven nursing researchers rotated session observations with two to four researchers participating in each session. Each researcher observed three to five members of the target group while taking part in the group activities or being at the table with them. The contents of the observations were the observable behaviors, attitudes, non-verbal expressions like facial expressions, dialogs, and verbal expressions between the children and older adults. Observations were conducted unobtrusively so that they did not interfere with the interaction between the generations. The observers moved freely around the room throughout the sessions and also provided support during the activities. After each session, the observers were able to triangulate and validate their data by reporting the content they had observed to one another and checking to ensure that there were no omissions in the observations until a consensus was obtained. The dialogue observation records were then entered into the field notes. Observations were made for time periods ranging from 60 to 120 minutes, beginning when the children arrived between 15:00, 15:30 hours until the end of the program at 17:00 hours.
Quantitative measures and data collection
The researchers assessed the interactions based on the program observations and used St. Luke’s Intergenerational Exchanges and Relations Observation (SIERO) inventory (Kamei et al., Citation2013). The SIERO inventory is scored by observers and ranges from 0 to 17 (Cronbach’s α =.82) with the following four factors: pace matched with other generation (PACE), generativity succession (passing on of wisdom from the older to the younger generation) (GEN), dialogs with other generations (TALKS), and enjoyment of sessions (ENJOY) (Kamei et al., Citation2013). A higher score indicates more engagement and participation. The researchers assigned three to five participants to intensive observations and after each session, all of the program staff confirmed the results and totaled the SIERO points of each participant. Participants provided a self-rating of their satisfaction at the end of each session using a 10 cm visual analog scale (VAS-10). It ranged from 0 (completely dissatisfied) to 10 (extremely satisfied). Data were collected from April 2014 to December 2018.
Data analysis
To evaluate the program, the qualitative and quantitative characteristics of the intergenerational interactions were categorized according to the attributes of the older adults. During the analysis stage, the older adults were divided into three groups: non-frail, frail, and cognitively impaired. Children comprised the fourth group.
Qualitative data analyses
Field notes on the behavior, attitude, and dialogue observation records were divided according to the program content of the session that day. Because there are no breaks between Japanese sentences (Kamermans, Citation2010), a morphological analysis was used. This yielded coding and the organization of verbs and nouns from the observation records to identify linguistic resources that contained correspondence between positive and negative texts. These were sorted into categories of participants’ intergenerational relations. The Japanese version of the Text Analytic for Surveys version 4.0 software (IBM SPSS, Japan) was used for categorizing and integrating the results.
Quantitative data analyses
The demographic data, data from the SIERO inventory, and perceived satisfaction (VAS-10) data were analyzed using descriptive statisticswith Kruskal-Wallis test or, a one-way analysis of variance, and the F test to assess the differences between the four groups (non-frail, frail, cognitively impaired older adults, and children). The analyses were conducted according to the activity that was being performed within the session if that activity occurred more than three times. The significance level was set to P < .05, and the Japanese version of SPSS version 24.0 J for Windows (IBM SPSS, Japan) software was used for the analysis.
Mixed methods data converging
The qualitative and quantitative data were analyzed separately according to the attributes of the participants and sessions. After that, the qualitative and quantitative data were integrated and converged. The results of the convergence were shown as a contrast and comparison with a joint display. After convergence, we conducted a metainference to interpret both types of data (Creswell, Citation2015; Fetters, Citation2020) regarding the qualitative characteristics of intergenerational interactions dependent on the attributes of the participants. Based on the convergence, the components of intergenerational interactions could be conceptualized and sorted into a four-fold table: highly or not highly interactional and highly or not highly satisfied in each group.
Ethical considerations
Older adults, children, and parents were provided with oral and written explanations of the purpose of this study prior to their participation. In compliance with the Declaration of Helsinki, participants were assured that they could decide to continue participation or withdraw at any time without facing any disadvantage and that their privacy would be protected. The Ethics Committee of St. Luke's International University provided approval for this study (13–031, 17-A019).
Results
Characteristics of the intergenerational program and its participants
The older adult participants were all women: 8 non-frail, 6 frail, and 4 cognitively impaired females with median ages of 77, 85, and 86 years, respectively. Nine school-aged children in the third to sixth grades with a median age of nine years participated. There was no significant difference among the ratio of adult groups living with their families, psychological status, with fall risk, or the Barthel Index. Frailty ratios were higher for physical strength in the frail group (F = 14.0 (2), p = .001) and for decreased cognitive functions in the cognitively impaired group (F = 18.0 (2), p < .001). The NM Scale score was significantly different (F = 9.3 (2), p = .009) between the three groups; the non-frail group scored in the normal range while the frail and cognitively impaired groups showed a slight degree of cognitive impairment. There were no significant differences among the three groups in the GDS-15 score. The motivation for participation was largely to revive social interaction. For example, participants talked about lost opportunities to go out, reduced contact with children, and wanting to interact with other generations ().
Table 1. Characteristics of participants according to generation
The researchers observed 89 intergenerational program sessions over a 57-month period. The seven major types of session were (a) self-work (e.g., origami or water coloring), (b) group-work (e.g., calligraphy or quilting), (c) intergenerational games, (d) cooking, (e) physical movement, (f) traditions focused on seasonal events and Japanese culture, and (g) talking ().
Table 2. Observed and analyzed program sessions
Intergenerational interactions and perceived satisfaction of specific sessions and activities for each participant group
The SIERO mean scores and the VAS-10 mean scores by session and group are displayed in . The SIERO score ranged from 2.3 for group-work in the cognitively impaired group to 7.6 for the talking sessions in the children’s group. The program satisfaction scores (VAS-10) ranged from 7.2 for the group-work sessions in the children’s group to 9.7 for the cooking and talking sessions in the frail older adults’ group, and the talking session in the cognitively impaired older adults’ group. Most of the sessions showed significant differences within the participant group except group-work and physical session in the SIERO score and cooking and traditional sessions in the satisfaction scores.
Table 3. Interaction and satisfaction score
We plotted the SIERO mean scores on the vertical line by participant group and the type of session and VAS-10 mean scores on the horizontal axis by participant group and type of session. These lines intersect at a mean score of SIERO 4.8 and VAS-10 9.0. The higher means of satisfaction are at the upper end. displays the resulting four-fold table converging interactions (SIERO) and satisfaction (VAS-10). Bulleted shapes (black and white dots and black and white triangles) were used to designate the four groups.
Figure 3. Distribution of interactions (SIERO) and program satisfaction (VAS-10) scores by program and participant group.
The plot in the upper right quadrant shows that the sessions with the highest degree of interaction were mostly among the non-frail and frail older adults. The upper right quadrant also shows high satisfaction levels for both participant groups in the talking and physical sessions. The lower right quadrant shows high program satisfaction, but interaction was lower than average. In the frail group (black dot), the VAS-10 scores ranged from 9.2 to 9.7, which were higher than the other groups, while the SIERO scores ranged from 3.3 to 4.7, with little difference between the sessions. The VAS-10 of the cognitively impaired group (white triangle) showed high values for all sessions (range = 9.0–9.7). Nevertheless, the SIERO score was lower at under 4.6 (range = 2.3–4.6) in seven sessions, and the observed degree of interaction was low.
Children’s (black triangle) VAS-10 scores varied from 7.2–8.7 depending on the session. The SIERO score (range = 3.9–7.6) was more than 4.0 in six sessions, including the self-work, traditions, cooking, physical, talking sessions, and intergenerational games.
The following four SIERO sub-factors were analyzed: PACE (sub-scale 1), GEN (sub-scale 2), TALKS (sub-scale 3), and ENJOY (sub-scale 4). The cognitively impaired group showed significantly lower scores in PACE (F = 18.6 (3), p < .001) and TALKS (F = 10.4 (3), p < .001). The children’s group showed a significantly higher GEN score compared to the frail group and the cognitively impaired group (F = 6.6 (3), p < .001). The non-frail group showed significantly higher scores in ENJOY (F = 7.0 (3), p < .001).
Observed intergenerational interactions
Morphological analysis of the morphemes (words or parts of words) was applied to the total 411 participant-observation records. Both positive and negative interactions were identified. For example, in the cooking sessions, the researchers observed that the frail and non-frail groups took the initiative to help the children. In the session of rakugo, a traditional performing arts form of story-telling, one person played all the different people in a conversation. To play each person skillfully, the child had to change his or her voice and turn his or her head right or left. Some children were very skillful at rakugo and all of the older adults looked at them with surprise.
Meanwhile, on other days, the older adults occasionally scolded the children during self-work activities. The observed morpheme items were categorized into positive and negative interactions via morphological analysis, and each emergence rate is shown in . In the positive morphemes, we recorded that non-frail older adults talked to the children (27.1%), praised the children (15.1%), and enjoyed the conversations with the children more than the other two groups. Frail older adults also talked to (17.5%) and praised the children (9.0%). The cognitively impaired group was generally passive (e.g., did not initiate conversations or activities) and conversed less with others. They showed more non-verbal communication; for example, they followed the children with their eyes and smiled more than the other groups (18.3%). Children talked with the older adults (20.5%), listened to conversations (10.2%), and showed awareness that they should pay attention to the older adults (23.9%).
Table 4. Intergenerational session observation morpheme results
The negative morphemes such as scolding children were observed from the non-frail older adults (1.8%). Paying attention only to one’s age group or not showing interest in their surroundings were observed in adults with cognitive impairments (6.6%) and children (7.2%).
Data converging with the quantitative (SIERO score) and qualitative (state of interactions) results
The SIERO interaction scores of each session by group and the morphological analysis of the participant observation records were converged and are jointly displayed in . The highest amount of interaction was found among the non-frail group in self-work, intergenerational games, cooking, traditional and talking sessions, followed by the frail and child group. The results of the participant observations generally indicated that the non-frail not only initiated conversations but also “acted in a grandmotherly role” when speaking to the children. The participants in the frail group were observed listening to the children’s stories and offering words of encouragement. The older adults with cognitive impairments followed the children with their eyes and smiled at them; however, they mainly focused on the session. In other words, they had more non-verbal interactions with the children.
Figure 4. Joint display of mean SIERO scores in each session by group.
From this data, we established the metainference that the positive interactions of both generations were based on the frequency and qualitative verbal communication, which depended on the older adults’ physical and mental status. Listening to children’s conversations with passive and non-verbal interaction trended in vulnerable older adults. Children were receptive to being taught and/or teaching the older generation, showing positive reciprocity. The metainference is presented at the top of .
Discussion
Differences in the quantity of interactions and satisfaction of each group in each program
This intergenerational program was implemented in a university setting in Tokyo. Faculty researchers assessed the participants’ interactions using SIERO and VAS-10 to quantify participant satisfaction in each group. Cooking sessions, intergenerational games, and traditional sessions’ interaction scored highly among the non-frail group. In the cooking session, the researchers observed that the non-frail group took the initiative in exchanges based on natural conversations between children and older adults where they could demonstrate their social skills, knowledge, culture, and roles. These interactions clearly indicated reciprocity (Lowenstein & Katz, Citation2012). Moreover, the children’s group showed a higher generativity succession. The SIERO GEN sub-scale suggested that children were receptive to frail and cognitively impaired older adults’ messages. The talking, traditions, and cooking sessions were highly satisfactory because they facilitated natural conversations between both generations where older adults could share their experience and knowledge, and children could be taught generative and developmental tasks (Ehlman et al., Citation2014). Those sessions were situated as social means for creating a dialogue for mutual learning and for the intentional and continuous exchange of emotional and material resources between generations (Kaplan et al., Citation2006). Generativity is a primary concern for older adults providing purpose in their lives and establishing and guiding the next generation as the younger participants acknowledged the older adults’ life experiences (Erikson, Citation1963). It was suggested that these interactions facilitate the developmental process in children, and help in their personal growth, as well as develop their sense of self-respect (Erikson, Citation1963) and acquired sociality (Vygotsky, Citation1978). Thus, children’s understanding and compassion for older adults would also be deepened (Heyman et al., Citation2011).
The cognitively impaired group showed some PACE differences and fewer dialogs with the other generation; however, they rated almost all activities as highly satisfying. Their reactions suggested they could not demonstrate the succession of generativity through their experience and wisdom, and this was a point of concern because there was a gap between the observed interactions and the subjective satisfaction scores. Additional research is needed to establish the congruence between the interpretation of the observed interactions and the subjective reports of satisfaction.
While minute differences were observed in the degree of satisfaction in the three older adult groups, the children were less satisfied with the physical sessions. The physical sessions, like sitting stretches and exercise, were designed to accommodate the frail older adults, but the children would have enjoyed more fun-filled and energetic sessions. Some SIERO items could not assess the capacities of the cognitively impaired group because cognitive impairments were not taken into consideration when designing the SIERO inventory. Thus, the inventory might not have adequately captured the more non-verbal interactions such as eye-following and listening passively to the children. Thus, the physical sessions and activities combining a variety of older adults and children could not be further refined.
Quality of the observed interactions of each group in each program
The frail and non-frail groups conversed with the children and praised their accomplishments. They used verbal communication, displaying affection and positive attitudes toward the children. The cognitively impaired group rarely conversed with others; there were several instances where they merely watched the children and smiled. The children approached the older adults with both caution and interest, yet they did reach out to them to help them with the activities. This kind of reciprocity was not only demonstrated by children to older adults, but also by older adults to children.
Other researchers also found positive outcomes for both older adults and children detailed in a review of the impact of intergenerational programs (Gualano et al., Citation2018). Whitehouse (Citation2013) reported that intergenerational sessions between cognitively impaired older adults and children enhanced deeper thinking and richer ethical deliberation through a mutual understanding. These interactions were assumed to be meaningful for both generations, and it was assumed that children understood older adults in their own way in this study as well.
Contrarily, the older adults occasionally scolded the children and girls sometimes formed a clique, which required the session leaders to provide appropriate facilitation such as fairly listening to opinions from both groups to avoid conflicting emotions. Vygotsky (Citation1978) reported that children’s interactions with others in social settings are a crucial factor that shapes their thinking. He also proposed that both the environment and interactions influence the course of a child’s development in a dialectical manner. Hence, it is imperative to evaluate the efficacy of interactions, including seemingly trivial conflicts arising from the sharing of space by both children and older adults.
These findings suggest that appropriate communication would facilitate intentional interactions between the generations. Particularly in the cognitively impaired group, it was crucial to understand the group’s interests and to improve their social and emotional interactions with the other generations.
Evaluation of intergenerational programs in the community, based on the interaction and satisfaction of both generations
This study aimed to elucidate the process of an intergenerational program in the community through prospective quantitative and qualitative intergenerational interactions and perceived satisfaction. The program facilitators, comprised of nursing staff, planned each session to promote interactions that could bridge the gap between older adults and children. The results of this study showed that the facilitators were aware of and considered each participant’s characteristics and preferences, promoted natural communication, and identified each person’s special skills and strengths. These practices were observed to create a comfortable zone with more trusting relationships between the children and older adults in the program. Similarly, earlier studies of participant satisfaction with various programs revealed intergenerational programs to be nurturing, allow teaching and sharing of knowledge, and be high in reciprocity (Newman & Smith, Citation1997). Furthermore, there should be opportunities to create interest in interrelated futures using generativity (such as sharing skills) (McAdams & De St. Aubin, Citation1992). However, in this study, it was found that the needs and interests of the frail and cognitively impaired groups might not have matched the sessions and activities planned for the non-frail older adults and children. Other researchers found that programs providing meaning and shared opportunities tended to be satisfying to the cognitively impaired and children regardless of the type of program (Galbraith et al., Citation2015). Therefore, establishing an intergenerational partnership that provides high-quality programs that fulfill the needs of all participants is necessary to enhance participant satisfaction.
Limitations of the study
This observational study had the same limitations that are characteristic of most observational studies. Although each session had two or more researchers making participant observations, who provided adequate descriptions of the interactions, it was difficult to observe some behaviors or conversations occurring outside the range of the observers, especially among the children. Moreover, the presence of several researchers observing the same situation and sharing perceptions decreased the threat of interpretation bias, but caution is still warranted, especially with regard to understanding the behavior of the adults with cognitive impairments. The small number of participants and lack of a control group limited the evidence gathered and the results’ generalizability. Furthermore, the SIERO inventory was not designed to document non-verbal expressions during intergenerational interactions, especially among older participants with cognitive impairments, suggesting a fruitful area for future research.
Conclusions
In this study, we evaluated an intergenerational community program to determine whether intergenerational interactions differed depending on selected attributes of the participants. A mixed methods prospective longitudinal parallel convergent design was used. The findings suggested that non-frail older adults communicated more using proactive and spontaneous conversations with children during sessions. However, frail and cognitively impaired older adults had mainly passive interactions featuring non-verbal communication. The linguistic, emotional, and positive attitudinal experiences of both generations led to the creation of meaningful and satisfying relationships.
Acknowledgement
The authors would like to thank the participants, program volunteers and collaborating nurse researchers.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Arai, H. (2014). The significance of frail. Journal of Japan Geriatrics Society, 51(6), 497–501. (in Japanese). https://www.jpn-geriat-soc.or.jp/publications/other/pdf/review_51_6_497.pdf
- Argyle, M. (1972). The psychology of interpersonal behaviour. (S. Tsuji & H. Nakamura, Trans). Penguin Books Ltd. (Original work published 1967).
- Atchley, R. C. (2000). Basic aspects of individual aging. In Atchley (Ed.), Social forces and aging (9th ed., pp. 75–179). Wadsworth Thomson Learning.
- Collin, C., Wade, D. T., Davies, S., & Horne, V. (1987). The Barthel ADL index: A reliability study. International Disability Studies, 10(2), 61–63. https://doi.org/https://doi.org/10.3109/09638288809164103
- Creswell, J. W. (2015). A concise introduction to mixed methods research. SAGE Publications, Inc.
- Ehlman, K., Ligon, M., & Moriello, G. (2014). The impact of intergenerational oral history on perceived generativity in older adults. Journal of Intergenerational Relationships, 12(1), 40–53. https://doi.org/https://doi.org/10.1080/15350770.2014.870865
- Eliopoulos, C. (2001). Solitude and connection: Conditions affecting mood and cognition. In Gerontological nursing (5th ed., pp. 131–137, 319–344). Lippincott Williams & Wilkins.
- Erikson, E. H. (1963). Generativity vs. stagnation. In E. H. Erikson (Ed.), Childhood and society (2nd ed., pp. 266–268). W. W. Norton & Company, Inc.
- Fetters, M. D. (2020). The mixed methods research workbook. SAGE Publications, Inc.
- Flemming, P. J. (2006). Utilization of a screening tool to identify homebound older adults at risk for falls: Validity and reliability. Home Health Care Services Quarterly, 25(3–4), 1–26. https://doi.org/https://doi.org/10.1300/J027v25n03_01
- Galbraith, B., Larkin, H., Moorhouse, A., & Oomen, T. (2015). Intergenerational programs for persons with dementia: A scoping review. Journal of Gerontological Social Work, 58(4), 357–378. https://doi.org/https://doi.org/10.1080/01634372.2015.1008166
- Gualano, M., Voglino, G., Bert, F., Thomas, R., Camussi, E., & Siliquini, R. (2018). The impact of intergenerational programs on children and older adults: A review. International Psychogeriatric, 30(4), 451–468. https://doi.org/https://doi.org/10.1017/S104161021700182X
- Heyman, J. C., Gutheil, I. A., & White-Ryan, L. (2011). Preschool children’s attitudes toward older adults: Comparison of intergenerational and traditional day care. Journal of Intergenerational Relationships, 9(4), 435–444. https://doi.org/https://doi.org/10.1080/15350770.2011.618381
- Kakai, H. (2016). Introducing mixed methods research. Tomisyobo. Co., Ltd. (in Japanese).
- Kamei, T., Meguro, S., Yamamoto, Y., & Kanamori, T. (2020). St. Luke’s intergenerational day program; Nagomi-no-kai (Harmonized program). Journal of Intergenerational Relationships, 18(1), 106-112. https://doi.org/https://doi.org/10.1080/15350770.2020.1709952
- Kamei, T., Takahashi, K., Omori, J., Arimori, N., Hishinuma, M., Asahara, K., Shimpuku, Y., Ohashi, K. & Tashiro, J. (2017). Toward advanced nursing practice along with people-centered care partnership model for sustainable universal health coverage and universal access to health. Recista Latino-Americana De Enfermagem, Jan 30;25;e2839. https://doi.org/https://doi.org/10.1590/1518-8345.1657.2839
- Kamei, T., Yamamoto, Y., & Kajii, F. (2013). Developing a St. Luke’s intergenerational exchanges and relations observation (SIERO) inventory and analysis of the reliability and validity. Journal of St. Luke’s Society for Nursing Research, 17(1), 9–18. http://arch.luke.ac.jp/adspace/handle/10285/11451
- Kamermans, M. (2010). Japanese syntax and structure. In M. Kameraman (Ed.), An introduction to Japanese syntax, grammar and language (pp. 53–55). Ghost Research Publishing.
- Kaplan, M., Liu, S. N., & Hannon, P. (2006). Intergenerational engagement in retirement communities: A case study of a community capacity-building model. Journal of Applied Gerontology, 25(5), 406–426. https://doi.org/https://doi.org/10.1177/0733464806292862
- Kobayashi, T., & Nishimura, K. (2003). A new clinical scale for rating of mental status and activities of daily living of the elderly (NM scale and N-IADL). Japanese Journal of Clinical Medicine, 61(9), 187–191. (in Japanese). https://jglobal.jst.go.jp/detail?JGLOBAL_ID=200902286938290159
- Kurlowicz, L., & Greenberg, S. (2007). The Geriatric Depression Scale (GDS). American Journal of Nursing, 107(10), 67–68. https://doi.org/https://doi.org/10.1097/01.NAJ.0000292207.37066.2f
- Kusano, A., Kaneda, T., Mano, Y., & Kakinuma, Y. (2009). Sedaikan koryu kouka [Effectiveness of intergenerational exchanges]. Sangaku Publishing Co., Ltd. (in Japanese).
- Kuzuya, M. (2012). Evaluation of frailty and the importance of interventions in a super-aged society. Japan Medical Journal, 4599, 27–31. (in Japanese).
- Lowenstein, A., & Katz, R. (2012). Reciprocity and exchange in kin and nonkin intergenerational relationships. Journal of Intergenerational Relationship, 10(4), 333–336. https://doi.org/https://doi.org/10.1080/15350770.2012.726602
- McAdams, D. P., & De St. Aubin, E. (1992). A theory of generativity and its assessment through self-report, behavioral acts, and narrative themes in autobiography. Journal of Personality and Social Psychology, 62(6), 1003–1015. https://doi.org/https://doi.org/10.1037/0022-3514.62.6.1003
- McCrea, J., & Smith, T. (1997). Social issues addressed by intergenerational program. In S. Newman, C. Ward, T. Smith, J. Wilson, & J. McCrea (Eds.), Intergenerational programs: Past, present, and future (pp. 37–51). Taylor & Francis.
- McHale, S. M., Updegraff, K. A., & Whiteman, S. D. (2012). Sibling relationships and influences in childhood and adolescence. Journal of Marriage and the Family, 74(5), 913–930. https://doi.org/https://doi.org/10.1111/j.1741-3737.2012.01011.x
- Meguro, S., & Kamei, T. (2018). Changes of depressive symptoms in older adults with dementia by continuous participation in the intergenerational exchange program with school-age children: A case report using mixed methods. Journal of Japan Society for Intergenerational Studies, 8(1), 51–59. (in Japanese).
- Ministry of Internal Affairs and Communications of Japan. (2019). Statistical topics No. 121, Older Adults of Japan. https://www.stat.go.jp/data/topics/topi1211.html
- Newman, S., & Smith, T. (1997). Developmental theories as the basis for intergenerational programs. In S. Newman, C. Ward, T. Smith, J. Wilson, & J. McCrea (Eds.), Intergenerational programs: Past, present, and future (pp. 3–19). Taylor & Francis.
- Niino, N., Imaizumi, T., & Kawakami, N. (1991). A Japanese translation of the geriatric depression scale. Clinical Gerontologist, 10, 85–87. (in Japanese). https://ci.nii.ac.jp/naid/10015148435
- Plano-Clark, V. L. (2014). Conceptualizing longitudinal mixed methods designs: A methodological review of health sciences research. Journal of Mixed Methods Research, 9(4), 297-319. https://doi.org/https://doi.org/10.1177/1558689814543563
- Roper, J. M., & Shapira, J. (2000). Ethnography in nursing research. SAGE Publications, Inc.
- St. Luke's College of Nursing. (2008). St. Luke's College of Nursing21st Century COE program final report. http://arch.luke.ac.jp/dspace/bitstream/10285/2446/2/0808-final.pdf (in Japanese).
- Tashakkori, A., & Teddlie, C. (Eds). (2010). SAGE Handbook of mixed methods in social and behavioral research. SAGE Publications, Inc.
- Teddlie, C., & Tashakkori, A. (2009). Foundations of mixed methods research. SAGE Publications, Inc.
- The Japan Geriatrics Society. (2014). Statement from the Japan Geriatrics Society regarding frailty. https://jpn-geriat-soc.or.jp/info/topics/pdf/20140513_01_01.pdf (in Japanese).
- Vygotsky, L. S. (1978). Interaction between learning and development. In M. Gauvain & M. Cole (Eds.), Readings on the development of children (pp. 34–40). Scientific American Books.
- Ward, C. (1997). The context of intergenerational programs. In S. Newman, C. Ward, T. Smith, J. Wilson, & J. McCrea (Eds.), Intergenerational programs: Past, present, and future (pp. 21–35). Taylor & Francis.
- Whitehouse, P. (2013). The challenges of cognitive aging: Integrating approaches from neuroscience to intergenerational relationships. Journal of Intergenerational Relationships, 11(2), 105–117. https://doi.org/https://doi.org/10.1080/15350770.2013.782740
- World Health Organization. (2018). Ageing and health. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
- Xue, Q. (2011). The frailty syndrome: Definition and natural history. Clinical Geriatric Medicine, 27(1), 1–15. https://doi.org/https://doi.org/10.1016/j.cger.2010.08.009