
Abstract
Objective: Traffic fatalities among motorcycle users are intolerably high in Thailand. They account for 73% of the total number of road fatalities. Children are also among these victims. To improve countermeasures and design of protection equipment, understanding the biomechanics of motorcycle users under impact conditions is necessary. The objective of this work is to analyze the overall kinematics and injuries sustained by riders and child pillion passengers in various accident configurations.
Methods: Motorcycle accident data were analyzed. Common accident scenarios and impact parameters were identified. Two numerical approaches were employed. The multibody model was validated with a motorcycle crash test and used to generate possible accident cases for various impact conditions specified to cover all common accident scenarios. Specific impact conditions were selected for detailed finite element analysis. The finite element simulations of motorcycle-to-car collisions were conducted to provide insight into kinematics and injury mechanisms.
Results: Global kinematics found when the motorcycle’s front wheel impacts a car (config-MC) highlighted the translation motion of both the rider and passenger toward the impact position. The rider’s trunk impacted the handlebar and the head either impacted the car or missed. The hood constituted the highest head impact occurrence for this configuration. The child mostly impacted the rider’s back. Different kinematics were found when car impacted the lateral side of the motorcycle (config-CM). Upper bodies of both rider and child were laterally projected toward the car front. The windshield constituted the highest proportion of head impacts. The hood and A-pillar recorded a moderate proportion. The rider in finite element simulations with config-MC experienced high rib stress, lung strain, and pressure beyond the injury limit. A high head injury criterion was observed when the head hit the car. However, the simulation with config-CM exhibited high lower extremities stress and lung pressure in both occupants. Hyperextension of the rider’s neck was observed. The cumulative strain damage measure of the child’s brain was higher than the threshold for diffuse axonal injury (DAI).
Conclusions: This study revealed 2 kinematics patterns and injury mechanisms. Simulations with config-MC manifested a high risk of head and thorax injury to the rider but a low risk of severe injury to the child. Thorax injury to the rider due to handlebar impact was only found in simulations with config-MC. However, a high risk of skull, lower extremity, brain, and neck injuries were more pronounced for cases with config-CM. A high risk of DAI was also noticed for the child. In simulations with config-CM the child exhibited a higher risk of severe injury.
Introduction
In 2015, the World Health Organization (WHO Citation2015) reported that 73% of road deaths in Thailand involved riders and pillion passengers of 2- and 3-wheeled vehicles, which is 6 times that of other vehicles. Motorcycles are considered a convenient and cheap mode of transportation. The Department of Land Transport, Thailand (Citation2017), reported 20.5 million registered motorcycles in 2017. Small motorcycles with a capacity less than 125 cc accounted for 86% of motorcycle domestic sales in 2016 (Board of Investment Thailand Citation2016). They are often used as daily transportation to send children to schools. Save the Children Thailand (Citation2014) reported that there are 1.3 million child motorcycle pillion passengers. In 2009, it was reported that 62% of traffic injuries in Thailand were among children under 15 years old and were due to motorcycle accidents (WHO, Regional Office for South-East Asia Citation2015). In addition, 37% of motorcycle injuries in Thailand occur to the head and neck (WHO, Regional Office for South-East Asia Citation2015). In order to improve countermeasures, understanding of kinematics and injury mechanisms of rider and child passengers during a crash is necessary. This article aims to analyze the overall kinematics and injuries sustained by motorcycle riders and child pillion passengers in various accident configurations.
Since 2002, there has been only one complete report on in-depth motorcycle accident investigation in Thailand (Kasantikul Citation2002). A total of 723 motorcycle accident cases in Bangkok were investigated. The motorcycle speed was between 20 and 50 km/h and the speed of other vehicles was between 11 and 40 km/h. Recently, Karnjanapollert et al. (Citation2018) reconstructed motorcycle accidents in Thailand. The range of speeds found from the reconstructions was 30–60 km/h. However, up-to-date, in-depth motorcycle accident data are rare in Thailand. Macro accident data are inadequate to produce effective vehicle-related safety solutions or countermeasures. Multibody simulations have often been used to virtually generate pedestrian and cyclist accidents, which subsequently provides an understanding of the kinematics and injury mechanisms of pedestrians/cyclists (Bourdet et al. Citation2014; Fiest et al. Citation2009; Magriet et al. Citation2012; Untaroiu et al. Citation2010; Watson et al. Citation2006). Utaroiu et al. (2010) developed an advanced methodology that combined multibody simulations and an optimization technique to identify the adult and child pedestrian pre-impact postures and vehicle speeds. Fiest et al. (Citation2009) also used combined approaches of multibody simulation and finite element simulation to investigate the relevance of rotation-induced head injuries to pedestrians hit by a large flat-front vehicle. In addition, Watson et al. (Citation2006) and Magriet et al. (Citation2012) employed a multibody dynamics model as a tool to study cyclists’ kinematics during crash. They found that the head impact of the cyclist was further rearward than that of the pedestrian. The head impact angles were also different, although the head impact velocity was similar. Bourdet et al. (Citation2014) simulated a large number of pedestrian and bicyclist accident scenarios involving small electric vehicles using multibody simulations. In relation to physical or virtual motorcycle crash tests, ISO 13232 (International Organization for Standardization [ISO] 2005) is usually employed to set up crash configurations (Deguchi Citation2003; Mukherjee et al. Citation2001; Namiki et al. Citation2003). Seven scenarios are recommended in ISO 13232 (ISO 2005) for assessment of protective devices installed on a motorcycle. They include 143-9.8/0, 114-6.7/13.4, 413-0/13.5, 413-6.7/13.4, 412-6.7/13.4, 414-6.7/13.4, 225-0/13.4.
In order to improve the understanding of the kinematics of the rider and child pillion passenger, a number of accident cases with various impact conditions are required. Multibody modeling is an inexpensive computerized tool suitable for simulating a large number of cases. It was employed to generate a number of possible accident cases based on defined impact parameters so that the typical kinematic patterns were drawn from these generated data. Nevertheless, the kinematics obtained were carefully considered because the vehicle deformation was not well considered. However, finite element simulation can provide more accurate results, including detailed injury analysis. However, it is relatively computer-intensive and not optimal to simulate many impact conditions. Only 3 simulation conditions were selected for finite element simulations so that further detailed investigation on occupants’ injuries could be performed. In addition, whole-body collision simulations were performed because they provide an understanding of potential injury risk to various body segments.
Materials and methods
Motorcycle accident data classification formed the basis for simulation work in this research. Selection of simulation configurations was based on the analysis of these data. Multibody simulations were employed to generate additional possible motorcycle accidents cases based on identified real-world accident scenarios. Three simulation conditions were selected based on the results of multibody simulation for detailed injury analyzes using finite element simulation.
Motorcycle accident data classification and common accident scenarios
Motorcycle accident data were provided by a Thai insurance company that insured 80% of registered motorcycles. They were analyzed in terms of frequency and pattern. All data were classified according to type of crash, type of other vehicle involved, rider and passenger age range, injury severity level, and injured body region. The classification of data for each category is shown in Figures A1–A6 (Appendix A, see online supplement). The total number of motorcycle accidents in 2014–2015 was 615,542, and 58.7% of motorcycle accidents were due to the rider losing control. Sideswipe/angular collision was the second highest, accounting for 30.5%. The number of rear-end (2.3%) and head-on (0.003%) collisions was low. Accidents with passenger cars (40.6%) were most common, followed by collisions with pickup trucks (14.9%). Common age ranges for the rider were 14–20 years (22.9%) and for the passenger, 10–19 years old (30.4%). Around 20% of victims sustained serious and severe injuries. Fatalities accounted for 1.12%. Head injury constituted 50.3% of all fatalities. Common accident scenarios were identified from sideswipe/angular collision because they accounted for the highest portion when considering only fatalities and severe/serious injuries. Common scenarios included motorcycle/other vehicle changing lane or overtaking, motorcycle/other vehicle making a U-turn, and turning at a junction or turning into an alley across the path of the other. These are summarized in Table A3 (Appendix A, see online supplement). The identified scenarios were also classified into 2 impact configurations, including (a) motorcycle impacting other vehicle (config-MC) and (b) other vehicle impacting motorcycle (config-CM).
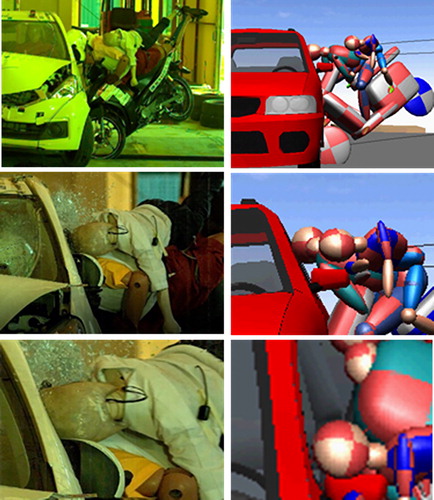
Figure 1. Comparison of kinematics of the rider and the child passenger during a crash.
Multibody motorcycle–car collision model setup
A motorcycle–car collision model was developed using the multibody simulation program PC-Crash. The child pillion passenger was also included in the model because the accident data showed a significant number of child pillion passengers (Figure A4) in motorcycle accidents. First the impact configuration was set to be the same as that in the experiment of Koetniyom et al. (Citation2018). The motorcycle was set to impact the car at 42.2 km/h. The height and weight of the rider and child were set to be same as those of the 50th percentile rider dummy (1.75 m, 78 kg) and the P6 child dummy (1.17 m, 21 kg) respectively (Figure A8, see online supplement). The simulation results were compared to the experimental results for validation.
Multibody simulation configurations and conditions
The validated motorcycle–car collision model was employed to generate more accident scenarios. This enabled a study of the effects of the parameters that are insufficiently available in real-world situations, such as impact speed, position, and angle, which encouraged further investigation into rider and passenger kinematics as well as head impact location during a crash. Because the anthropometry of Thai population is smaller than the 50th percentile dummy, the rider was scaled to represent an average Thai rider in the age group 14–20 years. A rider with a height of 1.59 m and weight of 52 kg was used for subsequent studies. Two impact configurations obtained from the accident analysis were considered (Figure A7, see online supplement). Impact parameters including speed, position, and angle were specified to generate accident simulations that represented accident scenarios (Table A3) in the previous section. Impact speeds for both simulation configurations were selected based on the studies of Kasantikul (Citation2002) and Karnjanapollert et al. (Citation2018). Simulation conditions are summarized in . These simulation conditions also included some configurations recommended by ISO 13232 (ISO 2005) such as 413-0/13.4 for config-MC and 143-9.8/0 for config-CM. However, the motorcycle speed of 50 km/h was used instead of 48.24 km/h and 40 km/h was used for the car speed instead of 35.28 km/h. Furthermore, the impact angle and position recommended in 412-6.7/13.4, 135-114/13.4 were also considered.
Table 1. Multibody simulation conditions.
Motorcycle impacting car configuration (config-MC)
The front wheel of the motorcycle was set to impact the stationary car with 4 impact speeds as detailed in . Four impact positions (Figure A7a) were selected to represent accident scenarios when a car was changing lanes, overtaking, turning, or making a U-turn. Furthermore, Kasantikul (Citation2002) reported that the points of first collision contact on the other vehicle frequently occurred at the front bumper and the area between the front corner and the front door. The motorcycle was set to impact the lateral side of the car at position P1 (half the car length) and P2 (one-sixth of the car length) with 6 impact angles (). However, only 120° and 150° impact angles were assigned to position P3 and P4 at the front bumper because an angle of 180° or more did not represent the scenarios of interest.
Car impacting motorcycle configuration (config-CM)
The car front end was set to impact the lateral side of a stationary motorcycle (Figure A7b). Three impact positions (Figures A7b, A8) including front wheel (F), center of motorcycle length (M), and rear wheel (R) were selected to represent accident scenarios when a motorcycle was changing lanes, overtaking, turning, or making a U-turn. The positions were selected based on Kasantikul’s (Citation2002) investigation, which classified the points of first collision on the motorcycle’s lateral side into front, center, and rear (Figure A9, see online supplement). Four impact angles between 30° and 90° were selected to represent the scenarios of interest ().
Finite element motorcycle–car collision model setup
A finite element motorcycle–car collision model was developed (Figure B1, Appendix B, see online supplement). The NCAC Toyota model was utilized for the simulations. Meshes of some components were refined to 3–4 mm (Figure B2, see online supplement). The revised model was validated against the crash test data. The motorcycle’s finite element model was developed using reverse engineering (Appendix B). The dimensions and weight of the main components were measured (Figures B3, B4, see online supplement). The thickness of the motorcycle frame, handlebar, tire, rim, and front fork tube was also measured and was reflected in the shell elements. Spokes were modeled using beam elements and the engine was assumed rigid. The seat was simplified using rubber composite behavior. Material properties were obtained from the experiments. The dynamic behavior of the shock absorber was simplified using spring elements and its stiffness was obtained from the experiment. Details of the model are given in Appendix B. A validation with the experiments was performed for the front wheel impact because it is the first point of contact with the other object in a frontal collision (Figures B8–B10, see online supplement). The whole motorcycle kinematics was qualitatively compared with a crash test. Fifth percentile and 6-year-old occupant human body models (THUMS) were employed. Their heights and weights were close to those of the rider and passenger models used in multibody simulations. Both THUMS models were validated in terms of component response and whole-body kinematics (Ito et al. Citation2017; Iwamoto et al. Citation2007; Kimpara et al. Citation2005; Shigeta et al. Citation2009; Watanabe et al. Citation2012). The postures of THUMS were adjusted by forced displacement applied to nodes of bones of upper and lower extremities. Presimulations were performed to position each body part but prestrains were not considered in the main simulations. Details of the THUMS positioning procedure are illustrated in Appendix C (see online supplement). Beam elements with 0.2 failure strain were used to tie the rider’s palms to the handlebar and the child’s palms to the rider’s hip bone. The motorcycle with the occupant model was combined with the car model. Gravity was applied to all models. A friction coefficient of 0.1 was assumed for the contacts between THUMS and other parts. The friction coefficient for the car–ground–motorcycle was assumed 0.3. Two impact configurations, config-MC and config-CM, were set up (Figures A7, B1).
Figure 2. Typical kinematics and head impact locations of the rider and the child pillion passenger.
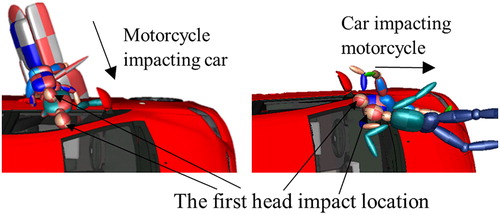
Figure 3. Simulations of config-MC with condition MC.1 (position P3, angle 120°, speed 20 km/h).
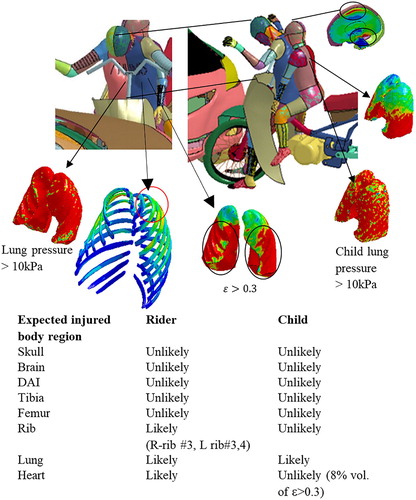
Figure 4. Simulations of config-MC with condition MC.2 (position P1, angle 45°, speed 40 km/h).
Finite element simulation conditions and injury indices
Three simulation conditions were selected to represent a motorcycle impacting a car at the lateral position as well as the front position and a car impacting a motorcycle. Based on the multibody simulation results, the impact conditions that led to severe head and chest injuries were considered for detailed injury investigation. Illustration of each selected condition is provided in (see online supplement). Justification of each selection was explained in the Results section. Injury indices and criteria for each body part were postulated as summarized in Table D2 (see online supplement). A head injury criterion (HIC15) of 700 was utilized to evaluate skull fracture (NHTSA Citation1999). It was calculated based on the linear acceleration at the head center of gravity. Brain cerebral contusion will occur when the principal strain on the brain exceeds 0.3 (Margulies et al. Citation1985). Furthermore, the risk of diffuse axonal injury (DAI) was estimated using a cumulative strain damage measure (CSDM). DAI occurred if the percentage volume of elements having a maximum principal strain over 0.25 exceeded 42.5% (Takhounts and Eppinger Citation2003). A 0.81 strain level was assumed as an indicator of risk of cervical ligament damage (Bass et al. Citation2007). To postulate on lung contusion, a pressure index with a ±10 kPa threshold was utilized (Schaffer et at. 1958). A principal strain of 0.3 was also used for predicting soft tissue injury (Yamada Citation1970). Bone fracture was assumed to occur once the Von Mises stress reached 130 MPa (Arnoux et al. Citation2008).
Results
Multibody simulations
Multibody simulation results were first compared with the experiment. The child’s head impact velocity was 40 km/h in the simulation and 40.5 km/h in the experiment. Occupant kinematics are shown in and Figures D1 and D2 (see online supplement). The child’s head impacted the A-pillar and the rider’s head impacted the front window. The rider’s head rebounded rather than entering the compartment because the car was modeled as a rigid body. This slightly affected the child kinematics after impacting the A-pillar. The child’s head peak linear acceleration was 789.4 g in the simulation, which is slightly higher than the 777.8 g in the experiment (Figure D3, see online supplement). The difference was only 1.49%. Overall, the simulation results were comparable with the experiment during the first impact. The model was employed for kinematics study. In total, 124 simulations were conducted for config-MC and config-CM.
Typical kinematics are shown in (see also Figures D4–D5 and D7–D8, online supplement). Each impact configuration revealed different global kinematics. For config-MC, the front wheel of the motorcycle hit the car, and both rider and child were translated toward the impact position at the first instance. If the impact angle was less than 60°, the motorcycle tended to slide forward along the side of the car. The occupants were then translated further away from the wheel’s first contact position (Figure D4b). If the angle was greater than 60°, the front wheel did not often slide away from the impact position and the rear wheel raised up. The occupants translated toward the wheel impact position (, left) until the rider hit the handlebar. The lower extremities and abdomen were blocked by the motorcycle and the upper body and the head hurled forward. The rider’s trunk also impacted the handlebar. It was observed that the occupant’s head may not strike the car directly depending on the impact position, angle, and speed. Simulations with impact position P1 resulted in rider’s head impact for all speeds and angles, whereas with positions P3 and P4, head impact occurred only at an angle of 150° for all speeds. Simulations with impact position P2 at a 30° angle showed no head strikes against the car for all speeds, similar to positions P3 and P4 at a 120° angle. The hood was the location with the most occurrences (29.7%) of rider’s head impact (Figure D6, see online supplement), and the A-pillar, windshield, and front window constituted 12.5, 9.4, and 7.8%, respectively (Figure D6). No impact of the rider’s head occurred 28% of the time. The head striking the B-pillar, C-pillar, or rear window was found only at impact position P1 with 120° and 150° angles. The child’s head mostly made contact with the rider’s back (62.5%) or the hood (10.9%). In addition, the child fell down without the head impacting the car 23.4% of the time.
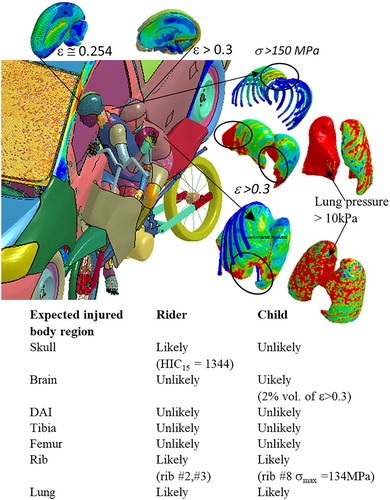
Figure 5. Simulations of config-CM with condition CM.3 (position R, angle 45°, speed 40 km/h).
On the other hand, simulations with config-CM revealed different kinematics. After the front of the car impacted the occupants’ legs, their upper bodies were projected laterally toward the car front (, right; Figure D8) and then rotated before their heads impacted the car. However, if the impact position was at the front wheel, which is before the seating position, the car did not impact the occupants directly. The motorcycle then rotated (Figure D7b) and no instances of head impact against the car were observed. These constituted 40 and 48.3% of simulations with config-CM for the rider and the child, respectively (Figure D9, see online supplement). The windshield was the location on the car most often struck by the rider’s head (43.6%) and the child’s (30%) head. The hood accounted for 10.9 and 13.3% for the rider and the child, respectively. The A-pillar ranked third, with a significant number of head impact occurrences (10.9% for the rider and 5% for the child).
Finite element simulations
Simulation conditions were selected based on the multibody simulation results. The first 2 conditions were selected from config-MC, which represented scenarios when the car was changing lanes, making a U-turn, or turning right at a junction across the motorcycle’s path. Because it is possible that the motorcycle either impacted the front or the side of the car, one location was taken from the front and one from the side. The first simulation condition was impact position P3 (front), with a 20 km/h speed and 150° angle. This condition (MC.1) resulted in the rider’s head hitting the hood (29.7% head impact occurrences) and the torso contacting the handlebar (expecting serious thorax injury). The second condition (MC.2) was impact position P1 (side), with a 40 km/h speed and 45° angle. This condition resulted in the rider’s head striking the A-pillar, which could lead to serious head injury. The third condition was selected from config-CM, which represented the motorcycle changing lanes, overtaking, turning, or making a U-turn across the car’s path. The simulation with impact position at the rear wheel of the motorcycle at 40 km/h and with a 45° angle (condition CM.3) revealed the rider’s head impacting the windshield (close to the A-pillar) and the child’s head striking the A-pillar, for which severe head injury is expected. All selected simulation conditions are summarized in Table D1 (Appendix D, see online supplement).
The overall kinematics and head impact locations obtained from the multibody simulations and the finite element simulations were compared for each corresponding condition (Figures D10, D11, see online supplement). Kinematics through time are illustrated in Figures D12–D14 (see online supplement). Global kinematics were similar but slightly different head impact locations were observed. The difference is due to the deformable motorcycle and the car structure in the finite element simulation.
For condition MC.1, the finite element simulation exhibited no head strike against the hood due to the direct impact of the torso and handlebar (; Figure D10a). The torso was blocked and slowed down and the lower extremities did not make contact with the car. In multibody simulation, the right side of the handlebar contacted the torso and then rotated. This allowed the rider to move forward and hit the hood.
Thorax injury was very likely to occur (), due to the direct impact of the torso against the handlebar. Three ribs experienced stress that exceeded the 130 MPa threshold for fracture (Table D2). Seventy-six percent of lung volume had internal pressure exceeding the postulated injury criteria (Schaffer et al. Citation1958). It was also found that 78% of heart volume had a strain exceeding the 0.3 criteria for soft tissue injury (Yamada Citation1970). The risk of rider’s head injury was low (HIC15 = 23.5, maximum brain strain = 0.19) because the head did not hit other objects. Lower extremity stress was low for both occupants. Because the child struck the rider’s back, the HIC15 was only 59. It was observed that a small portion of the child’s brain (0.5%) near the brain stem experienced strain that exceeded 0.3. CSDM-0.25 was only 2%. Although the child’s rib stress did not exceed the postulated fracture limit, almost 60% of the lung volume had pressure beyond the injury threshold. The child’s maximum lung strain was as high as 1.2.
For condition MC.2, the rider’s head hit the lower edge of the A-pillar in finite element simulation and hit the upper edge of the A-pillar in multibody simulation (; Figure D10b). The head impact speed was lower in finite element simulation due to the deformation of both vehicles. The motorcycle front wheel slightly deformed and slid along the car and the bodies made contact with the side of the car. The rider’s head hit the A-pillar, resulting in a high HIC15 (1,344), but brain strain was lower than 0.3. The child’s head hit the rider’s back, resulting in a low HIC15 of 173; 2.7% of brain volume had strain exceeded 0.3 limit. Nevertheless, the CSDM level was insignificant. Lower extremity stress was less than the postulated fracture limit for both occupants. The occurrence of thorax injury for both occupants was likely because the right part of the upper body impacted against the door. Two right ribs of the rider had a tendency to break because the stress exceeded the limit. In addition, 72.5% of the lung volume had internal pressure exceeding the injury criteria (). Heart and lung strain, which exceeded the 0.3 threshold, accounted for almost 78% of volume. Similarly, in the child’s thorax, one rib (no. 8) had stress just beyond 130 MPa; in addition, 60% of lung volume had pressure exceeding the limit. The child’s maximum lung strain was also high (2.2).
For condition CM.3, the head impact location of both occupants in finite element simulation slightly shifted to the left of the occupants (Figure D11). The rider’s head location moved closer to the A-pillar and the child’s head impacted the outer edge of the A-pillar. The head impact speed was slightly lower in the finite element simulation.
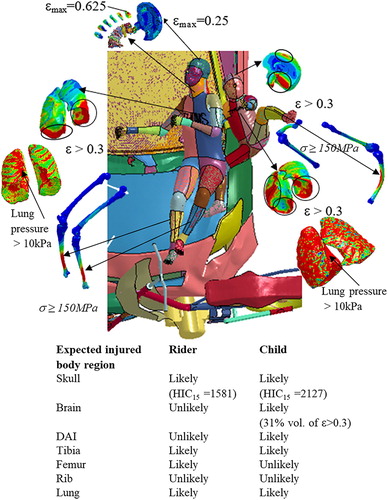
The hood leading edge (HLE) firstly made contact with the lower extremities, resulting in high stress above the fracture limit on both the rider’s tibia and femur. However, the child’s femur did not directly impact against the HLE, which struck the right leg below the knee. Furthermore, because the right leg was trapped between the car and the motorcycle, the child’s left tibia was extended outward by the frame of the motorcycle. The bending in the left tibia led to stress beyond the fracture limit (). After the first contact, the pelvis of both occupants ran onto the hood. Both upper bodies twisted and moved toward the car front. As a result, the child’s right back hit the fender, followed by the head hitting the A-pillar. The child’s HIC15 was 2,127, leading to high risk of skull fracture (NHTSA Citation1999). Maximum brain strain (εmax = 0.86) was higher than 0.3. CSDM-0.25 was 48%, which implied the possibility of DAI. In addition, 72.5% of lung volume had pressure beyond the injury criteria (red area in ). After the hip slid on the hood, the rider’s elbow struck the windshield, followed by the rider’s back and the head; 62% of the lung had pressure exceeding the injury criteria. Only 18% of the lung had strain beyond 0.3. The rider’s HIC15 was 1,518, and a high risk of skull fracture was expected. Brain strain was insignificant. Because the initial shoulder impact with the car arrested the movement of the rider’s torso, the momentum of the head swayed it backwards before contacting the windshield. The swinging motion led to neck hyperextension (). High strain was found on cervical discs C2–C3 (εmax = 0.625). However, this value is still less than the damage criterion of 0.81 (Bass et al. Citation2007).
Discussion
The simulation results revealed 2 different overall kinematics and injury mechanisms for each impact configuration. Typical global kinematics found in the simulations with config-MC involved initial forward translation of the rider and the passenger as well as the motion of the motorcycle after the first collision contact of the front wheel. It was observed that when the front wheel impacted the car at a small impact angle (less than 60°), the motorcycle rotated on a vertical axis, causing the occupants to be thrown sideways flat against the car. The rider’s head impact location depended on the impact position. The impact position near the front end tended to result in no head impact against the car. The main injury mechanisms were due to body’s side impact against the car. Lower limbs exhibited a low risk of bending or fracture because the limbs interacted with a relatively flat door panel, unlike the HLE. Risk of thorax injury was noticed due to the torso side impact. The risk of the rider’s skull fracture depended on the location of head impact. Striking against a stiff part like the A-pillar would lead to a high HIC and hence possible skull fracture. For an impact angle greater than 60°, the motorcycle tended to rotate on a horizontal axis, the rear wheel then raised up, and both occupants were ejected upwards while translating. Initial contact was between the rider’s torso and the handlebar followed by the rider’s head striking the car if the speed was high. Thorax and head injuries were highlighted. A high risk of thorax injury due to impact with the handlebar was expected. The child passenger translated together with the rider and frequently experienced a low risk of severe injury regardless of ground impact. However, high pressure within the lung was observed due to compressing against the rider’s back. The location of head impact against the car differed depending on the impact position, angle, and speed. Simulations with config-CM exhibited different kinematics. Both the rider and passenger were laterally projected toward the car front while the upper body rotated during collision. Both occupants sustained similar injury patterns. The main injury mechanisms were similar to those of pedestrians. The occurrence of lower limb fracture was likely due to the first collision contact with the HLE. Relatively low rib stress was found in comparison with config-MC. A bent-knee posture resulted in relatively less severe injury than the pedestrian’s stretched leg posture. Hyperextension of the neck was observed, which is in line with the study of Kasantikul et al. (Citation2003). A high risk of skull fracture and thorax injury was likely in config-CM due to direct head and upper body impact with the car front. Component stiffness of the car is a main influence on head acceleration due to inertia effect. Wearing a helmet would definitely help mitigate the head injury. However, the rate of helmet use is less than 50% in Thailand. Law enforcement regarding helmet use would help reduce the number of fatalities. The findings from the current study will be useful for improvements in the design of protective equipment such as helmets and airbag jackets. The rider’s head impact speed found in this study at a car collision speed at 40 km/h is higher than the helmet standard drop test speed (20.6 km/g). Furthermore, a risk of DAI due to the brain rotation was observed. The rotational effect has not yet been considered in helmet drop tests. It is challenging to design a helmet that can mitigate this type of injury. In addition, the thorax injury due to handlebar impact implies the need for protective equipment to mitigate this type of injury.
Limitations
One limitation of this work is that the whole motorcycle impact response was only qualitatively validated with crash test data from the literature. However, motorcycle key components were separately validated with experiments. The other limitation is that THUMS organ impact responses were validated against postmortem human subjects (Shigeta et al. Citation2009) but the validity was only confirmed for the selected force conditions. In addition, this study utilized CSDM to predict the occurrence of DAI (Takhounts and Eppinger Citation2003). The validity of CSDM has not yet been fully proved.
Supplemental Material
Download PDF (2.6 MB)Additional information
Funding
Related Research Data
References
- Arnoux PJ, Behr M, Llari M, Thollon L, Brunet C. Injury criteria implementation and evaluation in FE models applications to lower limb segments. Int J Crashworthiness. 2008;13:653–665.
- Bass CR, Lucas SR, Salzar RS. Failure properties of cervical spinal ligaments under fast strain rate deformations. Spine. 2007;32:7–13.
- Bourdet N, Luttenberger P, Teibinger A, Mayer C, Winllinger R. Pedestrian and bicyclists head impact conditions against small electric vehicle. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI); September 10–14, 2014; Berlin, Germany.
- Board of Investment Thailand. Thailand automotive industry: the next generation. 2016. Available at: https://www.boi.go.th/upload/content/BOI-brochure%202015-automotive-20150325_70298.pdf. Accessed October 17, 2018.
- Deguchi M. Modeling of a motorcycle for collision simulation. Paper presented at: 18th International Conference on the Enhanced Safety of Vehicles (ESV); May 19–22, 2003; Nagoya, Japan.
- Department of Land Transport, Thailand. Government open statistical data. 2017. Available at: http://www.data.go.th. Accessed October 17, 2018.
- Fiest F, Gugler J, Arregui-Dalmases C, et al. Pedestrian collisions with flat-fronted vehicles: injury patterns and importance of rotational accelerations as a predictor for traumatic brain injury (TBI). Paper presented at: 21st International Technical Conference on the Enhanced Safety of Vehicles Conference (ESV); June 15–18, 2009; Stuttgart, Germany.
- International Organization for Standardization. Motorcycles—Test and Analysis Procedures for Research Evaluation of Rider Crash Protective Devices Fitted to Motorcycles. Geneva, Switzerland: ISO Secretariat; 2005. ISO 13232:2005. Available at: https://www.iso.org/standard/37426.html. Accessed February 2, 2019.
- Ito K, Tokuyama M, Miyazaki H, Hayashi S, Kitagawa Y, Yasuki T. Development of child finite element (FE) models and vehicle-to-pedestrian collision simulations. Paper presented at: 25th Technical Conference on the Enhanced Safety of Vehicles (ESV); June 5–8, 2017; Detroit, MI.
- Iwamoto M, Nakahira Y, Tamura A, Kimpara H, Watanabe I, Miki K. Development of advanced human models in THUMS. Paper presented at: 6th European LS-DYNA User’s Conference; May 29–30, 2007; Gothenburg, Sweden.
- Karnjanapollert P, Koetniyom S, Carmai J. The use of multibody dynamics simulations to investigate motorcyclist kinematics and injuries in accidents. Paper presented at: 14th International Conference of Automotive Engineering (ICAE); April 2–3, 2018; Bangkok, Thailand.
- Kasantikul V. Motorcycle Accident Causation and Identification of Countermeasures in Thailand: Volume I. Bangkok. 2002. Available at: http://www.mosac.eu/public/file/KasantikulMotorcycleAccidentResearchinThailand-Bangkok2002.pdf. Accessed October 17, 2018.
- Kasantikul V, Ouellet JV, Smith TA. Head and neck injuries in fatal motorcycle collisions as determined by detailed autopsy. Traffic Inj Prev. 2003;4:255–262.
- Kimpara H, Lee JB, Yang KH, et al. Development of a three-dimensional finite element chest model for the 5th percentile female. Stapp Car Crash J. 2005;49:251–269.
- Koetniyom S, Carmai J, Kassim KAA, Ahmad Y. Kinematics and injury analysis of front and rear child pillion passenger in motorcycle crash. International Journal of Automotive and Mechanical Engineering. 2018;15:5522–5534.
- Magriet VS, Stefanie H, Radarius C, Fredriksson R. Cyclist kinematics in car impacts reconstructed in simulation and full scale testing with Polar dummy. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI); September 12–14, 2012; Dublin, Ireland.
- Margulies SS, Thibault LE, Gennarelli TA. A study of scaling and head injury criteria using physical model experiments. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI); June 24–26, 1985; Gothenburg, Sweden.
- Mukherjee M, Chawla A, Mohan D, Singh M, Sakurai M, Tamura Y. Motorcycle–car side impact simulation. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI); October 10–12, 2001; Isle of man, UK.
- Namiki H, Nakamura T, Lijima S. A Computer Simulation for Motorcycle Rider-Motion in Collision. Pennsylvania: SAE International; 2003. SAE Technical Paper 2003-32-0044.
- NHTSA. Development of improved injury criteria for the assessment of advanced automotive restraint systems–II. 1999. Available at: https://www.nhtsa.gov/sites/nhtsa.dot.gov/files/rev_criteria.pdf. Accessed September 10, 2018.
- Save the Children Thailand. The 7% Project. 2014. Available at: http://www.7pecent.org/about/. Accessed March 19, 2018.
- Schaffer KE, McNulty WP, Carey C, Liebow AA. Mechanisms in development of interstitial emphysema and air embolism on decompression from depth. J Appl Physiol. 1958;13:15–29.
- Shigeta K, Kitagawa Y, Yasuki T. Development of next generation human FE model capable of organ injury prediction. Paper presented at: 21st International Technical Conference on the Enhanced Safety of Vehicles (ESV); June 15–18, 2009; Stuttgart, Germany.
- Takhounts EG, Eppinger RH. On the development of the SIMon finite element head model. Stapp Car Crash J. 2003;47:107–133.
- Untaroiu C, Cradall JR, Takahashi Y, Okamoto M, Ito O, Fredriksson R. Analysis of running child pedestrians impacted by vehicle using rigid body models and optimization techniques. Saf Sci. 2010;48:259–267.
- Watanabe R, Katsuhara T, Miyazaki H, Kitagawa Y, Yasuki T. Research of the relationship of pedestrian injury to collision speed, car-type, impact location and pedestrian sizes using human FE model (THUMS version 4). Stapp Car Crash J. 2012;56:269–321.
- Watson J, Hardy R, Kayvantash K. Understanding the nature of cyclist’s head impacts. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI); September 20–22, 2006; Madrid, Spain.
- World Health Organization. Global Status Report on Road Safety 2015. 2015. Available at: https://www.who.int/violence_injury_prevention/road_safety_status/2015/en/. Accessed September 26, 2017.
- World Health Organization, Regional Office for South-East Asia. Child development and motorcycle safety. 2015. Available at: http://www.who.int/iris/handle/10665/173782. Accessed March 16, 2017.
- Yamada H. Strength of biological materials. In: Evean FG, ed. Baltimore, MD: Williams & Wilkins; 1970:106–204.