
Abstract
Objective: Emergency braking can potentially generate precrash occupant motion that may influence the effectiveness of restraints in the subsequent crash, particularly for rear-seated occupants who may be less aware of the impending crash. With the advent of automated emergency braking (AEB), the mechanism by which braking is achieved is changing, potentially altering precrash occupant motion. Further, due to anatomical and biomechanical differences across ages, kinematic differences between AEB and manual emergency braking (MEB) may vary between child and adult occupants. Therefore, the objective of this study was to quantify differences in rear-seated adult and pediatric kinematics and muscle activity during AEB and MEB scenarios.
Methods: Vehicle maneuvers were performed in a recent model year sedan traveling at 50 km/h. MEB (acceleration ∼1 g) was achieved by the driver pressing the brake pedal with maximum effort. AEB (acceleration ∼0.8 g) was triggered by the vehicle system. Inertial and Global Positioning System data were collected. Seventeen male participants aged 10–33 were restrained in the rear right passenger seat and experienced each maneuver twice. The subjects’ kinematics were recorded with an 8-camera 3D motion capture system. Electromyography (EMG) recorded muscle activity. Head and trunk displacements, raw and normalized by seated height, and peak head and trunk velocity were compared across age and between maneuvers. Mean EMG was calculated to interpret kinematic findings.
Results: Head and trunk displacement and peak velocity were greater in MEB than in AEB in both raw and normalized data (P ≤ .01). No effect of age was observed (P ≥ .21). Peak head and trunk velocities were greater in repetition 1 than in repetition 2 (P ≤ .006) in MEB but not in AEB. Sternocleidomastoid (SCM) mean EMG was greater in MEB compared to AEB, and muscle activity increased in repetition 2 in MEB.
Conclusions: Across all ages, head and trunk excursions were greater in MEB than AEB, despite increased muscle activity in MEB. This observation may suggest an ineffective attempt to brace the head or a startle reflex. The increased excursion in MEB compared to AEB may be attributed to differences in the acceleration pulses between the 2 scenarios. These results suggest that AEB systems can use specific deceleration profiles that have potential to reduce occupant motion across diverse age groups compared to sudden maximum emergency braking applied manually.
Introduction
Previous analysis of naturalistic data has found that emergency braking was the most common precrash evasive maneuver conducted in crash and near-crash scenarios across all age groups (Seacrist et al. Citation2018). Furthermore, crash data have documented that a majority (61–79%) of intersection crashes were preceded by emergency braking (Scanlon et al. Citation2015). The recent development of automated crash avoidance technologies may change the way emergency braking is achieved—from driver-applied manual braking to vehicle-triggered automatic braking. Automated emergency braking (AEB) systems have the potential to avoid or mitigate the crash; data suggest that such systems reduce police-reported rear-end crash rates by as much as 43% (Cicchino Citation2017). NHTSA has included AEB systems in their 5-star rating system since 2016 (NHTSA Citation2016), and many manufacturers have committed to including AEB in nearly all vehicles by 2022 (NHTSA Citation2017). Therefore, it is important to characterize the type of loading environment that vehicle occupants experience with AEB—across all passenger ages—and compare it with manual emergency braking (MEB).
Current vehicle safety designs are assessed using anthropometric test devices with standard seating procedures. Crash avoidance maneuvers may displace the occupant outside the optimal seated position, potentially affecting restraint performance. These precrash maneuvers have been defined as low acceleration time extended events (Kent et al. Citation2016); low acceleration time extended events have the potential to alter an occupant’s posture and position prior to an impact.
Several studies have investigated the influence of braking maneuvers on occupant kinematics (Ólafsdóttir et al. Citation2013; Stockman et al. Citation2013; Baker et al. Citation2017). These previous studies were able to quantify the forward head and trunk displacement during the braking maneuver. However, fewer studies have compared occupant response between AEB and MEB. One previous study quantified drivers’ lower extremity kinematics and muscle activity during automated braking; however, sternum and head kinematics were not investigated (Behr et al. Citation2010). Osth et al. (Citation2013) reported greater head and sternum forward excursions as a result of AEB compared to MEB. However, only adult (age >23) drivers were considered. As drivers, participants were actively involved in the MEB event but not AEB and thus different muscle activation likely contributed to different kinematics. Carlsson and Davidsson (Citation2011) found that front-seated adult passengers exhibit larger forward excursions during AEB compared to drivers. The influence of AEB on rear-seated passengers, who may have less situational awareness, is less understood. The increased prevalence of ridesharing services such as Uber and Lyft could lead to an increase in adults seated in the rear seat. In addition, rear seat passengers include those of varied age and size. No previous study was found that compared passenger kinematics between AEB and MEB among passenger occupants from different age groups, including child passengers. Children also exhibit different neuromuscular control strategies than adults, irrespective of body size (Dotan et al. Citation2012; Arbogast and Maltese Citation2015).
To enhance knowledge in these areas, the purpose of this study was to quantify rear passenger head and sternum kinematics across multiple age groups when passengers are exposed to 2 different vehicle braking methods: A specific AEB deceleration pulse currently in a vehicle and MEB deceleration. We hypothesized that participants would exhibit increased body segment excursions and velocities in the MEB maneuver compared to AEB, because AEB systems may engage farther in advance of an obstruction and produce lower accelerations on the vehicle occupants. We further hypothesized that child passengers would exhibit a different neuromuscular strategy than adults in their bracing behavior.
Methods
The study protocol was reviewed and approved by the Institutional Review Board of the Ohio State University and the Children’s Hospital of Philadelphia.
Participants
Seventeen healthy participants () without neuromuscular or musculoskeletal conditions or previous injury were enrolled. Height and weight inclusion criteria were based on ranges related to the Centers for Disease Control and Prevention growth charts (Citation2000) and anthropometric test device size to capture the range of adult and child sizes typical of rear seat occupants. Only male participants were selected to avoid introducing gender differences as a potentially confounding factor (Tierney et al. Citation2005; Seacrist et al. Citation2012).
Table 1. Mean (SD) of participants’ age, height, and weight.
Experimental procedures
The vehicle maneuvers were conducted with a recent model sedan at the Vehicle Dynamics Area (VDA) of TRC Inc. (Marysville, OH). Two maneuvers were performed: AEB and MEB. For the MEB maneuver, an average acceleration of ∼1 g was achieved by the driver depressing the brake pedal with maximum effort following 120 m of constant velocity at 50 km/h achieved with cruise control. In case of AEB, the maneuver was initiated by directing the vehicle toward a 3D Guided Soft Target (Dynamic Research, Inc., Torrance, CA) intended to simulate a real vehicle. Similar to MEB, AEB was performed while traveling at 50 km/h constant velocity, achieving an average acceleration of ∼0.8 g. An auditory warning preceded braking in the AEB maneuver and stopped when auto-braking was activated. The warning timing was part of the in-built AEB system and was not programmable by the study investigators. Participants were not told that the warning would be present or what the warning meant.
All participants were seated in the right rear seat of the vehicle. Before performing the maneuvers, a muscle activity baseline was established by a static trial. In the static trial, participants were instructed to sit in the vehicle in a normal nontensed posture, with feet on the floor and hands in their lap looking straight ahead for 5 s. After the static trial, each participant remained in the vehicle for a baseline drive where the vehicle was driven on a straight path for approximately 120 m at approximately 50 km/h. This baseline drive was performed to familiarize the participants, in particular the children, with the vehicle setting. After the baseline drive, each maneuver described above was performed twice for each participant. Each participant was not aware of the exact time at which the maneuver was to occur. Each participant was instructed to sit with feet on the floor and hands in his lap in a nontensed posture for initial position and act spontaneously during the maneuver as one would do in a real crash-avoidance situation. A brief break of approximately 5 min followed each repetition. The 2 AEB maneuvers were performed one after the other either first or at the end of the testing day; this was randomized across participants. The same professional driver conducted the maneuvers for each participant.
Instrumentation
Vehicle dynamics were measured with an inertial and Global Positioning System measurement unit (Oxford RT 3003, Oxford Technical Solutions Ltd, UK), connected to a data acquisition system (Somat eDAQlite HBM, Inc.) placed in the vehicle trunk. The data acquisition system sampled data from the navigation system and the 3 seat belt load cells (shoulder belt, each side of lap belt) (Measurement Specialties, TE Connectivity, Inc., Aliso Viejo, CA) at 200 Hz. The right rear seat position was instrumented with an 8-camera infrared 3D motion capture system (Optitrack, NaturalPoint, Inc., Corvallis, OR) with sampling frequency of 200 Hz. The right front seat was moved to the full forward position to leave sufficient space for a compression pole on which the cameras were mounted. Photo-reflective markers were placed on participants’ heads (on a tightly fitted head piece with the markers on the forehead, 2 on the temple and one on the head top) and trunk (bilateral acromion, suprasternal notch, and xiphoid process) and on the shoulder seat belt (one close to the shoulder area and one on the trunk area). The markers on the seat belt, suprasternal notch, and xiphoid process consisted of an array of 4 markers placed on rigid structures. Electromyography (EMG; Trigno EMG System Delsys Inc., Natick, MA) sensors were placed bilaterally on deltoids, brachioradialis, biceps, rectus femori, rectus abdomini, middle trapezii, and sternocleidomastoids (SCM). These muscles were selected because they were hypothesized to be most involved in bracing behavior. Muscle activity was collected at 2,000 Hz.
Data processing and analysis
All data processing and analyses were performed with custom MATLAB (MathWorks 2015) programs. Vehicle forward acceleration was filtered with a zero-lag second-order low-pass Butterworth filter with the cutoff frequency set to 6 Hz. Vehicle acceleration profiles from each trial were averaged and standard deviation was calculated to examine repeatability of the maneuver. Motion capture data were processed in Motive 2.0 (Optitrack, NaturalPoint Inc.). Head and trunk positions were defined as the geometric center of the group of markers placed on the head and the suprasternal notch rigid bodies, respectively. For the head, the rigid body center approximated the geometric center of the head. Head and trunk positions were filtered with a moving average method spanning 5 frames. The initial position of head and trunk were defined as their average position for 1 s prior to the maneuver. The initial position was subtracted from head and trunk displacements measured during the maneuver. Head and trunk positions were first analyzed nonnormalized and then normalized by seated height. Head and trunk velocity was also calculated in order to understand whether there were differences by age in the rate at which a subject achieved maximum excursion.
Secondary outcome measures were extracted from EMG and load cells. The raw EMG signals were filtered with a bandpass filter (20–500 Hz, filter order: 558) based on the finite impulse response (Kaiser Window method) filter (De Luca et al. Citation2010). A root mean square method with a 200-ms moving average smoothing window was applied. EMG signals during the maneuver were normalized by the average EMG signal during the static trial. Therefore, muscle activity during the maneuver was expressed as a percentage of rest, with rest defined as the muscle activity during the static trial. After mean EMG was calculated for each trial and each maneuver phase, data were checked for the presence of outliers, and any data point greater than 3 standard deviations above the mean was removed. Seat belt forces were filtered by an 8-pole Butterworth filter (Somat TCE, HBM, Inc.) and the mean force for 0.5 s before the maneuvers was subtracted from the force signal.
The jerk of each maneuver was calculated as the average rate of change of vehicle acceleration from onset of maneuver to the steady-state acceleration phase (defined below). Vehicle acceleration bias was removed by subtracting the mean for 0.5 s before the maneuver initiated. From the forward acceleration profile of each trial of the MEB and AEB maneuver, 3 events were defined for analysis ():
Figure 1. Mean (SD) of AEB (right) and MEB (left) vehicle acceleration used in this study. The steady-state phase was defined for each trial and was based on the vehicle acceleration profile. The 2 dashed lines define the boundaries of the steady-state phase ad the black line represents the onset of the maneuver (i.e., maneuver start).
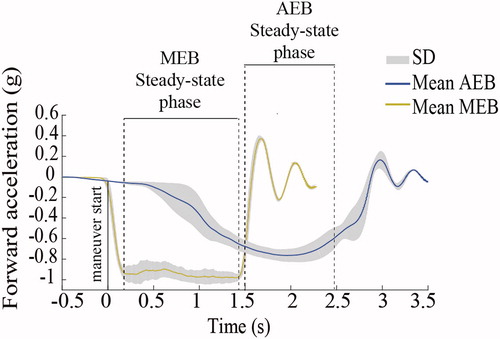
Maneuver start: The first time at which the vehicle’s forward acceleration was equal to 5% of the maximum forward acceleration during the maneuver (Osth et al. Citation2013).
Steady-state acceleration start: The first time at which the vehicle acceleration was above 85% of the peak acceleration.
Steady-state acceleration end: The last time at which the vehicle acceleration was above 85% of the peak acceleration.
The following outcome measures were calculated:
Mean head and trunk displacements over the duration of the steady-state phase.
Head and trunk peak displacement rate of change between maneuver start and the end of the steady-state phase (to examine the velocity of the head and trunk).
Mean EMG and peak EMG for the steady-state phase.
Peak seat belt forces within the steady-state phase.
Repeated measure mixed 3-way analyses of variance were performed to examine the effect of age (children vs. teens vs. adults), maneuver (MEB vs. AEB), and repetition (first vs. second) on the displacement and velocity data. Tukey’s post hoc test was used for multiple comparisons (P ≤ .05). Linear correlations between mean head and trunk displacements and vehicle acceleration were assessed with Pearson’s correlation coefficient to understand whether the differences in displacement between maneuvers could have been influenced by variations in acceleration magnitude rather than the different shape of the acceleration pulse between maneuvers.
Results
Vehicle dynamics
For MEB the average acceleration was 0.94 ± 0.05 g and for AEB it was 0.74 ± 0.05 g. The jerk was 4.75 g/s for MEB and 0.52 g/s for AEB. The duration of the acceleration phase (i.e., from maneuver start to steady-state acceleration end) was 1.48 ± 0.09 s for MEB and 2.45 ± 0.3 s for AEB.
Kinematics
Mean steady-state head and trunk forward displacement was greater for MEB compared to AEB (Table A.1, see online supplement). Head and trunk peak forward displacement rate of change was greater in MEB than in AEB (Table A.1). All dependent measures showed no main effect of age (Table A.1).
There was a significant interaction effect between maneuver and repetition (P = .006 for head and P = .003 for trunk) for peak displacement rate. Specifically, the peak displacement rate of the head was greater in repetition 1 (100.4 ± 13.7 cm/s) than in repetition 2 (85.7 ± 13.8 cm/s; P < .004) in the MEB but not in the AEB maneuver (37.6 cm/s ± 18.1 cm/s vs. 38.5 cm/s ± 16.5 cm/s; P = .99). This was also observed in the trunk (MEB: repetition 1: 58.9 ± 14.9 cm/s; repetition 2: 50.4 ± 11.6 cm/s; P < .006; AEB: repetition 1: 18.2 cm/s ± 6.1 cm/s; repetition 2: 20.7 cm/s ± 11.59 cm/s; P = .66).
Pearson’s correlation coefficient between head and trunk displacement (raw and normalized) ranged between 0.008 and 0.1, showing weak correlations between the magnitudes of head and trunk displacements and vehicle acceleration (Figure A.1, see online supplement).
Muscle activity
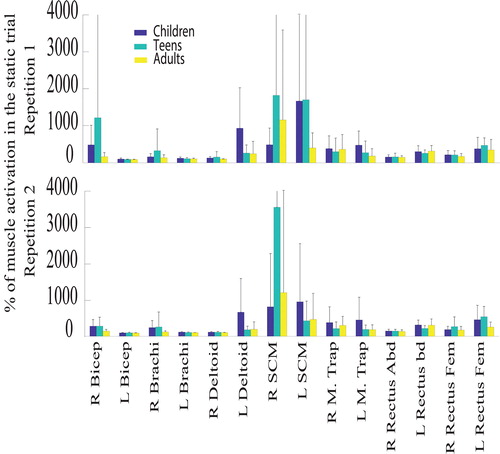
Mean EMG, both raw and expressed as a percentage of muscle activation in the static trial, was greater overall during the MEB maneuver than during the AEB maneuver for each age group. In particular, SCM mean EMG was greater in MEB compared to AEB and also in children and teens in repetition 2 compared to repetition 1 in MEB (, Figure A.2, see online supplement).
Figure 2. Mean (SD) of EMG represented as a percentage of muscle activation in the static trial of mean EMG in repetition 1 (top graphs) and repetition 2 (bottom graphs) in MEB.
Adults exhibited significantly greater maximum shoulder belt loads (162.3 ± 85.8 N) than children (99.6 ± 74.0 N; P = .01). Maximum shoulder belt loads were greater in MEB (201.9 ± 55.0 N) than in AEB (65.3 ± 40.9 N). Right and left lap belt load ranges were small (18–76 N) and therefore were not considered in the analysis.
Discussion
In this study, the effect of specific AEB vs. MEB deceleration profiles on rear passenger motion was compared across age groups, demonstrating that head and sternum excursions were less in AEB conditions. These observed differences likely are related to the manner in which the AEB system investigated in this study achieves the deceleration and the biomechanical and neuromuscular response to those loading conditions. Further, the MEB was not intended to represent normal attentive defensive driving, which would be preferred to any sudden emergency evasive maneuver.
The decreased head and sternum forward excursion and velocity in AEB compared to MEB may have been more likely due to the different shapes of the 2 acceleration curves, rather than the 0.2 g difference in acceleration magnitude, considering that the correlation between the magnitudes of head and trunk displacements and vehicle acceleration were weak (Figure A.1). The AEB maneuver in our study exhibited a more gradual acceleration pulse than the MEB maneuver, likely contributing to the reduced excursions and body segment velocities. Previous findings showed that head and sternum excursions increased in AEB compared to MEB (Osth et al. 2013). In their study, they examined driver kinematics and applied similar acceleration pulses (1.1 g) between manual and emergency braking. Our results suggest that with the AEB system used in our study, a more gradual rate of change of acceleration may reduce the displacement of the occupant. In addition, by studying drivers who were by definition responsible for the MEB pulse, Osth and colleagues (2013) did not capture the response of a naïve occupant across the 2 braking maneuvers. It is possible that drivers in the MEB trials demonstrated anticipatory muscle activity, thus reducing their displacement. This interpretation seems to be in agreement with a previous finding that drivers had smaller forward motion than passengers in both AEB and MEB maneuvers (Carlsson and Davidsson 2011). Ólafsdottir and colleagues (2013) investigated more naïve occupants than drivers (e.g., front-seated passengers) with the same acceleration pulse (1.1 g) used by Osth et al (2013). Front seat occupants with unobstructed forward visibility through the windscreen may be able to utilize their vestibular system in different ways to stabilize their movements. Our study examined rear-seated occupants whose biomechanical responses in magnitude and timing differ from these previous studies due in part to less forward visibility reducing anticipation of the maneuver.
Head and sternum excursions in the braking events studied herein, even when normalized to seated height, were not significantly different across age groups (Table A.1). Previous research has reported that children exhibit greater normalized head and sternum excursions in response to a low-speed frontal loading condition (Arbogast et al. Citation2009). The frontal pulse experienced by the children in Arbogast et al. (Citation2009) was 3.4 g compared to 0.7–0.9 g in the current study. It is possible that the lower pulse in our study was not severe enough to elicit a different biomechanical response across ages. However, muscle activity in our study was greater in children and teens compared to adults, particularly in the SCM, suggesting that although children and teens showed the same kinematic response to the maneuvers, to achieve that response they used a different neuromuscular strategy that required a greater activation of the neck muscles.
Differences in neuromuscular response were also seen across maneuvers. Across all ages, head and trunk excursions were greater in MEB than AEB, despite increased muscle activity in MEB. This may suggest that the bracing strategy in MEB was insufficient to reduce head and trunk excursions to the same values observed in AEB. The startle reflex could have also contributed to the greater muscle activation in MEB. Considering that in MEB, some participants (in the children and teens groups) increased their SCM muscle activity in repetition 2, it is plausible that the subjects were attempting to exert more muscle force during their second trial to counteract the forward velocity of head and trunk. Increased activity in SCM was also found in passengers exposed to a greater AEB pulse (1.1 g). In contrast, participants in our AEB condition demonstrated overall reduced muscle activity—across both repetitions—perhaps highlighting that the rate of acceleration in our AEB condition was not sufficient to elicit the startle effect. These differences were likely not influenced by the auditory warning before the AEB braking, because participants’ premaneuver muscle activity (i.e., 0.5 s before maneuver onset and warning was activated within this time) was not different between AEB and MEB (Douglas et al. Citation2018). In the interpretation of muscle responses, it must be noted that the data were normalized to a nontensed position rather than maximum voluntary isometric contraction (MVIC) and therefore may include a greater level of noise than if normalized to MVIC. The use of the static trial as a normalization method was chosen to minimize testing burden on subjects, particularly the younger ones.
This study has several limitations. There are a variety of AEB systems currently available in the modern fleet. Our study examined a specific production AEB deceleration profile; therefore, our results can be generalized only to vehicles with similar AEB acceleration pulses. The maneuver was performed in a single-vehicle environment and the generalizability of these results to other vehicle interior geometries has not been studied. Other muscles besides those measured in this study may have contributed to participants’ motion, such as deep muscles that are unable to be measured by surface EMG. Muscle activity was also not normalized to MVIC but rather to rest and therefore may be noisier than MVIC normalized data. Subcutaneous EMG and MVIC assessments were not utilized because of the challenge of testing children and minimizing test time. The testing environment was not fully naturalistic because it was conducted with instrumentation on a test track and not in a real traffic situation; this was mitigated by participants being unaware of the timing of the maneuvers.
In conclusion, the comparisons between the AEB and MEB systems investigated herein demonstrated that AEB has potential to modulate the specific deceleration pulse to reduce rear seat occupant motion during emergency braking across diverse age groups compared to sudden maximum manual braking. These results extend previous findings by examining the response of a different occupant population (adult and pediatric rear seat occupants). This study may guide future development of AEB standards that can potentially enhance safety for vehicle occupants.
Supplemental Material
Download Zip (1.6 MB)Acknowledgments
The authors thank the human volunteers who participated in this study and Drew Zeronik and Darek Zook at TRC Inc.; Thierry Chevalier, PhD (NaturalPoint Inc.); Gretchen Baker and Yadetsie Zaragoza-Rivera at Ohio State University; and Christine Holt at the Children’s Hospital of Philadelphia for their help and suggestions
Additional information
Funding
Related Research Data
References
- Arbogast K, Balasubramanian S, Seacrist T, Maltese M, García-España JF, Hopely T, Constans E, Lopez-Valdes FJ, Kent RK, Tanji H, Higuchi K. 2009. Comparison of kinematic responses of the head and spine for children and adults in low-speed frontal sled tests. Stapp Car Crash J. 53:329–372.
- Arbogast K, Maltese M. 2015. Pediatric biomechanics. In: Yoganandan N, Nahum AM, Melvin JW, editors. Accidental injury: biomechanics and prevention. New York: Springer-Verlag. p. 643–696.
- Baker G, Stockman I, Bohman K, Jakoboson L, Osvalder A, Svensson M, Wimmerstedt M. 2017. Kinematics and shoulder belt engagement of children on belt‐positioning boosters during emergency braking events. Paper presented at: Proceeding of IRCOBI Conference.
- Behr M, Poumarat G, Serre T, Arnoux P-J, Thollon L, Brunet C. 2010. Posture and muscular behaviour in emergency braking: an experimental approach. Accid Anal Prev. 42(3):797–801.
- Carlsson S, Davidsson J. 2011. Volunteer occupant kinematics during driver initiated and autonomous braking when driving in real traffic environments. Paper presented at: Proceeding of IRCOBI Conference.
- CDC growth charts. 2000. Center for Disease Control and Prevention Growth Charts- Published May 30, 2000. Available at: http://www.cdc.gov:GrowthCharts/
- Cicchino JB. 2017. Effectiveness of forward collision warning and autonomous emergency braking systems in reducing front-to-rear crash rates. Accid Anal Prev. 99:142–152.
- De Luca CJ, Gilmore DL, Kuznetsov M, Roy SH. 2010. Filtering the surface EMG signal: movement artifact and baseline noise contamination. J Biomech. 43(8):1573–1579.
- Dotan R, Mitchell C, Cohen R, Klentrou P, Gabriel D, Falk B. 2012. Child—adult differences in muscle activation — a review. Pediatr Exerc Sci. 24(1):2–21.
- Douglas E, Graci V, Seacrist T, Kerrigan J, Mansfield J, Bolte J, Sherony R, Hallman J, Arbogast K. 2018. Anticipatory neck muscle activity in automatic and manual emergency braking. Paper presented at: American Society of Biomechanics Conference, Rochester, Minnesota.
- Kent R, Arbogast K, Seacrist T, Holt C, Kerrigan J. 2016. Low-acceleration, time-extended events (LATEs): update on a study of human volunteer and PMHS responses. Pacifico Yokohama (Japan): Japan Society of Automotive Engineers (JSAE).
- National Highway Traffic Safety Administration (NHTSA). 2016. Driver assistance technologies. https://www.nhtsa.gov/equipment/driver-assistance-technologies
- National Highway Traffic Safety Administration (NHTSA). 2017. NHTSA-IIHS announcement on AEB. https://www.nhtsa.gov/press-releases/nhtsa-iihs-announcement-aeb
- Ólafsdóttir J, Östh J, Davidsson J, Brolin K. 2013. Passenger kinematics and muscle responses in autonomous braking events with standard and reversible pre‐tensioned restraints. Paper presented at: Proceeding of IRCOBI Conference
- Osth J, Olafsdóttir JM, Davidsson J, Brolin K. 2013. Driver kinematic and muscle responses in braking events with standard and reversible pre-tensioned restraints: validation data for human models. Stapp Car Crash J. 57:1–41.
- Scanlon JM, Kusano KD, Gabler HC. 2015. Analysis of driver evasive maneuvering prior to intersection crashes using event data recorders. Traffic Inj Prev. 16(Sup2):S182–S9.
- Seacrist T, Douglas EC, Huang E, Megariotis J, Prabahar A, Kashem A, Elzarka A, Haber L, MacKinney T, Loeb H. 2018. Analysis of near crashes among teen, young adult, and experienced adult drivers using the SHRP2 naturalistic driving study. Traffic Inj Prev. 19(sup1):S89–S96.
- Seacrist T, Saffioti J, Balasubramanian S, Kadlowec J, Sterner R, García-España JF, Arbogast K, Maltese M. 2012. Passive cervical spine flexion: the effect of age and gender. Clin Biomech (Bristol, Avon)). 27(4):326–333.
- Stockman I, Bohman K, Jakobsson L, Brolin K. 2013. Kinematics of child volunteers and child anthropomorphic test devices during emergency braking events in real car environment. Traffic Inj Prev. 14(1):92–102.
- Tierney R, Sitler M, Swanik C, Swanik K, Higgins M, Torg J. 2005. Gender differences in head–neck segment dynamic stabilization during head acceleration. Med Sci Sports Exerc. 37(2):272–279.
