
Abstract
Objective: To reduce the number of severe injuries sustained by cyclists in crashes with vehicles, it is important to understand which kinds of injuries are occurring to identify what should be assessed by means of virtual testing.
Method: A detailed analysis of injuries was made based on Swedish and Dutch accident data. The most frequently injured body regions and the most frequent single injuries of these body regions were analysed.
Results: Cyclists most frequently injured their heads, upper and lower extremities, and bone fractures as well as brain injuries were identified as one of the most important injuries.
Conclusions: For the virtual assessment of cyclist protection, injury predictors for long bone, skull and pelvic fractures as well as brain injuries are required in Human Body Models.
Introduction
In 2016, cyclists represented 8% of all road fatalities registered by the police in Sweden and 19% in the Netherlands (ERSO Citation2018). As the proportion of cyclists in transport is steadily increasing (Pucher and Buehler Citation2017), especially in larger European cities, cyclists will be involved in cyclist-to-passenger-car collisions more often in the future. It is thus, an essential task to analyze their injuries in detail, because understanding which injuries are most common can help preventing them.
While other studies have mainly focused on the relevance of different injuries according to Abbreviated Injury Scale (AIS) body regions (Fredriksson and Rosen Citation2012; Otte et al. Citation2012; Weijermars et al. Citation2016), the current study was carried out to investigate injuries in more detail. The aim was to identify which injuries were most common in different databases. This is needed to define requirements for Human Body Models (HBMs) to be used for virtual testing of cyclist protection.
Methods
Data from the Swedish national accident database STRADA (Swedish Traffic Accident Data Acquisition) and from the Dutch Institute for Road Safety Research (SWOV) were analyzed to identify injuries in cyclist-to-passenger-car collisions. STRADA is the Swedish database with national coverage of information related to road traffic accidents collected from emergency care hospitals and police reports (Howard and Linder Citation2014). Only data on accidents that occurred from 2016 to 2018, including both police report and hospital record information, were included in the present study. These data were available for 1932 cyclists with a total of 3,840 injuries, covering 365 different AIS2005 codes. The data from the Netherlands included cases from 2000 to 2014. For 2000–2011, only those injuries of patients who were included in both police registration and hospital data were included, as hospital data alone (ICD-9-CM) did not include detailed information on the road users involved. In more recent years (2012–2014), hospitals have used ICD-10 coding methods, providing more information. Therefore, injuries were also included of patients who were only registered at hospitals for these years. However, passenger cars and light goods vehicles cannot be separated for those years, as they belong to the same category. Injuries in ICD-9-CM and ICD-10 were mapped to AIS1990 (ICDmap90) (Johns Hopkins University Citation1998), and subsequently converted to AIS2005-Update2008 using the AIS Crosswalk. This allowed us to compile a dataset of 15,650 cyclists with a total of 29,515 injuries and 269 different AIS codes. The most common AIS body regions were evaluated in both datasets (Swedish and Dutch). The body regions head, face and neck were grouped together. After identifying the three most frequently injured body regions in both datasets, the full AIS codes were evaluated (Association for the Advancement of Automotive Medicine Citation2008). Because many minor injuries to an entire body area (e.g., skin, subcutaneous and muscle such as abrasion or hematoma) were recognized, especially in the STRADA database, only injuries with an AIS severity ≥ 2 were evaluated in detail to identify injuries which should be specifically addressed by virtual testing.
Results
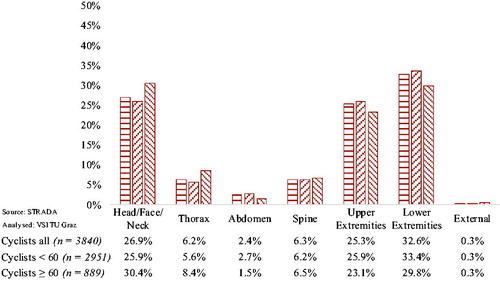
The three most frequently injured body regions identified in both accident datasets were the head, upper and lower extremities ( and ). The analysis of the Dutch accident data revealed that the most frequently injured body region was the head, followed by the lower extremities and then the upper extremities. The analysis of the Swedish data revealed a slightly different ranking: the lower extremities were followed by head and then the upper extremities.
Figure 1. Injured body regions according to AIS of Dutch accident data.
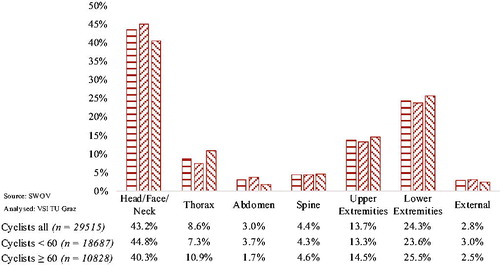
Figure 2. Injured body regions according to AIS of Swedish accident data.
The three most frequently detailed AIS codes for AIS2+ injuries are listed in for each of the three most frequently injured body regions. The percentages in the table refer to the total number of injuries for this body region (considering all severities as it was not possible to conduct the AIS Crosswalk for all injuries).
Table 1. AIS2+ injury codes for the three most frequently injured body regions based on Dutch and Swedish accident data and their shares in the total number of injuries (including AIS1).
Regarding injuries to the head, the following most relevant AIS2+ injuries were identified in the Dutch dataset: serious cerebrum injuries (140688.3), followed by cerebral concussions with a loss of consciousness for less than one hour (161003.2) and skull base fractures (150200.3). The most frequent head injuries in the Swedish accident dataset were cerebral concussions with a loss of consciousness for less than 30 min (161004.2), skull base fractures without cerebrospinal fluid (CSF) leak (150202.3) and maxilla fractures (250800.2).
In the Dutch dataset, clavicle fractures (750500.2), humerus fractures (751100.2) and radius fractures (752800.2) were identified as the most frequent AIS2+ injuries to the upper extremities. Analysis of the Swedish accident data revealed that the three most common injuries were two different distal radius fractures (752311.2, 752351.2) and carpus fractures (752451.2).
Regarding the last body region, the lower extremities, the following three AIS2+ injuries were found most frequently in the Dutch accident dataset: tibia fractures (854000.2), proximal tibia fractures (854171.2) and fibula fractures (854441.2). The Swedish dataset analysis showed that pelvic ring fractures (856151.2), proximal tibia fractures (854171.2) and fibula fractures (854471.2) were most common.
Discussion
The data in this study was collected during two different time periods. However, when analyzing the Dutch data, no significant change in injuries over the years was observed, which is why the authors assume that this does not influence the results. The selection criterion of the data, i.e., being recorded by both police and hospital or at least involvement of a vehicle, was done in order to get an as comparable data between the countries as possible. This is necessary, because a significant difference among hospital and police reported data was observed in previous studies (Juhra et al. 2012).
The most relevant body regions were the same in both datasets and are in line with previous studies (Otte et al. Citation2012; Weijermars et al. Citation2016). In future studies, the risk of permanent medical impairment (Malm et al. Citation2008) should be also considered additionally to the analysis of AIS severities.
It was shown that the ranking of the most frequent injured body regions differed between the countries: head injuries were more common in the Dutch dataset than in the Swedish one. This difference might be caused by a difference in helmet wearing rates. The overall helmet wearing rate in Sweden is measured yearly, and in 2017 it was 44% (The Swedish Transport Administration Citation2018), while it is supposed to be much lower in the Netherlands. According to an international survey conducted in 2014, only 34% of 712 Dutch respondents owned a helmet, 7% of often wore it and 2% always wore it (Haworth et al. Citation2015).
Difference in injuries to the different body regions between younger and elderly cyclists was identified (e.g., elderly cyclists suffered more often for head injuries in Sweden while an opposite trend can be observed in the Netherlands). A detailed analysis of these findings was not part of this study, but should be kept in mind for future HBM developments.
To assess the safety of cyclists, evaluation criteria that can capture the probability of long bone fractures as well as brain injuries are needed as a first step. In a next step, the modeling and assessment of the other bones should be in focus, as for example fractures of the skull or the pelvic ring are mainly represented by AIS3+ injuries.
Pedestrian legform impactors are not representative for the leg posture of cyclists. Furthermore, current pedestrian headform tests neglect rotational loads. Virtual testing with HBMs has the potential to fill these gaps. However, the modeling of detailed fracture patterns is challenging with the available constitutive models in LS-DYNA (Khor et al. Citation2018). Probabilistic evaluation approaches, comparable to (Forman et al. Citation2012) should be developed for the long bones to enable the application of HBMs for the virtual testing of cyclist safety. Furthermore, a probabilistic brain injury criterion should be applied, either based on a FE brain model (Sahoo et al. Citation2016) or on rotational loads (Gabler et al. Citation2018).
As a next step virtual testing protocols and HBMs will be developed, which fulfill the requirements derived in the current study.
Additional information
Funding
References
- Association for the Advancement of Automotive Medicine. 2008. Abbreviated injury scale 2005 update 2008. Barrington, IL.
- ERSO. 2018. European Commission, Traffic Safety Basic Facts on Cyclists, European Commission, Directorate General for Transport.
- Forman JL, Kent RW, Mroz K, Pipkorn B, Bostrom O, Segui-Gomez M. 2012. Predicting Rib fracture risk with whole-body finite element models: development and preliminary evaluation of a probabilistic analytical framework. Ann Adv Automot Med. 56:109–24.
- Fredriksson R, Rosen E. 2012. Priorities for bicyclist protection in car impacts-a real life study of severe injuries and car sources. In: International Research Council on the Biomechanics of Injury, ed. 2012 IRCOBI Conference Proceedings. http://www.ircobi.org/downloads/irc12/default.htm.
- Gabler LF, Crandall JR, Panzer MB. 2018. Development of a metric for predicting brain strain responses using head kinematics. Ann Biomed Eng. 46(7):972–85. doi:10.1007/s10439-018-2015-9.
- Haworth N, Schramm A, Houtenbos M, Shinar D. 2015. International survey of bicycling exposure, crash involvement, behaviors, and attitudes: preliminary results. In: International Cycling Safety Conference 2015; Hanover, Germany.
- Howard C, Linder A. 2014. Review of Swedish experiences concerning analysis of people injured in traffic accidents: Swedish National Road and Transport Research Institute (VTI).
- Johns Hopkins University. 1998. ICDMAP-90 user’s guide.
- Juhra C, Wieskötter B, Chu K, Trost L, Weiss U, Messerschmidt M, Malczyk A, Heckwolf M, Raschke M. 2012. Bicycle accidents–do we only see the tip of the iceberg? A prospective multi-centre study in a large German city combining medical and police data. Injury. 43(12):2026–34. doi:10.1016/j.injury.2011.10.016.
- Khor F, Cronin DS, Watson B, Gierczycka D, Malcolm S. 2018. Importance of asymmetry and anisotropy in predicting cortical bone response and fracture using human body model femur in three-point bending and axial rotation. J Mech Behav Biomed Mater. 87:213–29. doi:10.1016/j.jmbbm.2018.07.033.
- MacKenzie E, Sacco W. 1997. ICDMAP-90: A Users Guide. Baltimore, (MD): The Johns Hopkins University School of Public Health and Tri-Analytics.
- Malm S, Krafft M, Kullgren A, Ydenius A, Tingvall C. 2008. Risk of permanent medical impairment (RPMI) in road traffic accidents. Ann Adv Automot Med. 52:93–100.
- Otte D, Jänsch M, Haasper C. 2012. Injury protection and accident causation parameters for vulnerable road users based on German In-Depth Accident Study GIDAS. Accid Anal Prev. 44(1):149–53. doi:10.1016/j.aap.2010.12.006.
- Pucher J, Buehler R. 2017. Cycling towards a more sustainable transport future. Transp Rev. 37(6):689–94. doi:10.1080/01441647.2017.1340234.
- Sahoo D, Deck C, Willinger R. 2016. Brain injury tolerance limit based on computation of axonal strain. Accid Anal Prev. 92:53–70. doi:10.1016/j.aap.2016.03.013.
- The Swedish Transport Administration. 2018. Analysis of road safety trends 2017. Management by objectives for road safety work towards the 2020 interim targets; 2019:035 [accessed 2019 Apr 10]. https://trafikverket.ineko.se/Files/sv-SE/57185/Ineko.Product.RelatedFiles/2019_035_analysis_of_road_safety_trends_2017_management_by_objectives_for_road_safety_work_towards_the_2020_interim_targets.pdf.
- Weijermars W, Bos N, Stipdonk HL. 2016. Serious road injuries in The Netherlands dissected. Traffic Inj Prev. 17(1):73–9. doi:10.1080/15389588.2015.1042577.