
Abstract
Introduction: Cyclists account for a large share of injured road users in traffic. The crash data analysis for cyclist safety and protection should be based on a representative dataset of real-world crashes. This manuscript aimed to explore the patterns of cyclists’ fractures and factors associated with fractures of higher severity.
Methods: This paper exemplifies a methodology that combines injuries from a crash database, including both hospital and police reports and fracture registry database from orthopedic centers nationally in Sweden.
Results: Car occupants were most frequently involved in crashes resulting in fractures (37%), followed by motorcyclists (27.6%) and bicyclists (15.4%). Common fracture locations differed by the type of road user, where cyclists were more frequently fractured in the lower arm, compared to other road users, such as car drivers, motorcyclists and pedestrians who suffered mostly of fractures in the lower leg. Within cyclists, injuries also differed by gender, suggesting that combination of different countermeasures may be needed in order to provide sufficient protection for all cyclist. In the analyzed data, male cyclists with an average age of 49 were the most frequently fractured cyclists. Fractures of cyclists to the acetabulum (100%), pelvis (84.2%), vertebra (75%) and tibia (70.3%) were most frequently high energy fractures. Single bicycle incidents (OR = 0.165) and collisions with another bicycle (OR = 0.148) were significantly less likely to result in a high energy fracture than a collision with a car.
Conclusions: The results of this study may guide the design of appropriate protective devices for the cyclists based on the different injury mechanisms and provide implications for prioritizing new countermeasures, campaigns, or regulations.
Introduction
In Sweden, crashes involving cyclists account for a higher proportion (45%) of hospital reported crashes than any other road user (STA Citation2014). Fractures have been found to be the most common injury type to cyclists and Juhra et al. (2011), found that, while traumatic brain injury accounted for the largest proportion of cyclists admitted to hospital, fractures to the upper and lower extremity were the injuries with largest resource consumption as a result of major surgery (Juhra et al. Citation2012).
Niska and Eriksson (Citation2013) also explain that about 70% of the serious injuries, or those whose injuries are predicted to result in 1% permanent medical impairment (PMI 1%), from cycling crashes are damage to the arm, shoulder, leg or hip. Of the very serious injuries, those resulting in 10% permanent medical impairment (PMI 10%), 39% were head injuries; however, arm, shoulder, leg and hip injuries accounted for 42%. There is therefore a need to look more closely at these injuries to provide the possibility of designing personal protection also for these body parts.
The main purpose of this study was to analyze data on bicycle crashes which lead to fractures through linking multiple in-depth data registries including fracture registry information, police records and hospital records, providing a greater detail of information than has been examined before based on the individual registries. This analysis, among other things, will form the basis for guidelines for designing personal protection for cyclists and prioritizing measures in cyclists’ infrastructure.
Two existing national databases formed the basis of this study, the Swedish TRaffic Crash Data Acquisition (STRADA) and the Swedish Fracture Register (SFR). STRADA was created in response to a governmental direction to the former Swedish Road Administration. The task was to establish a new national information system which should be able to collect all police reported road crashes and additionally include emergency hospital information about injuries sustained in road crashes (Forward and Samuelsson Citation2007). SFR was developed by orthopedic specialists affiliated with Sahlgrenska University Hospital, beginning in 2011. The purpose of the SFR is to lay a solid foundation of knowledge concerning the effectiveness of Swedish fracture care (Wennergren et al. Citation2015; Wennergren and Möller Citation2018).
These datasets provide unique information in relation to the fracture and the crash, which, when combined, provide in-depth information on the crash scenario and outcome. This gave the opportunity to find connections between fracture types and the energy of the fracture as SFR has detailed information on the fractures, and the crash conditions as described in STRADA, including road conditions, weather conditions, and crash location.
This study aimed to: 1) match two datasets, SFR with the STRADA database for various transport modes and describe the matched dataset; 2) examine fractures occurring to bicyclists after bicycle crashes based on both STRADA and SFR in terms of the circumstances under which these fractures occur and to whom they occur, and 3) examine factors associated with higher severity of fracture in the matched data.
Methods
Datasets
Two different datasets were involved in this study. The first dataset was STRADA, which is a national information system in Sweden that contains all police reported road crashes and emergency hospital admission data related to road crashes.
The Swedish police are obligated by law (SFS 1965:561, last update in SFS 2014:1244) to report every road crash which led to at least one personal injury. Reports are based on observations by police officers at the crash site. The type of police reported road crashes which are submitted to STRADA is regulated by law. The criteria for the police to report a road crash coincide with Sweden’s official definition of a road crash. According to the Swedish government agency, Transport Analysis, a road crash in Sweden is defined:
to be a crash which has occurred in traffic on a road
to involve at least one vehicle in motion
to involve at least one personal injury.
The hospitals on the other hand report voluntarily. The reporting criteria for hospitals are to report everyone who seeks medical attention because of a road crash or a crash that occurred in the public traffic environment. This does not require that an injury is found. Additionally, it is necessary that a patient consents to the transmission of the hospital report to STRADA (Howard and Linder Citation2014). The data is then based on patient self-reported information.
Police and hospital reports are matched using Swedish personal identity numbers of involved persons, the crash time and location by the Swedish Transport Agency. The Swedish Transport Agency manages the data collection and storage. There is not a 100% match between hospital and police cases, but all collected cases are kept in the database, regardless of whether it contains only hospital or police data.
The Swedish Fracture Register (SFR) was the second dataset used in this study. This dataset contains information on fractures provided by medical professionals and includes details on the type and severity of fractures as well as treatment and surgical procedures undertaken. Additionally, patients are asked to complete follow-up questionnaires providing information of long-term effects of the fracture. Cases are those patients treated at and reported to SFR via about 35 of Sweden’s 55 orthopedic clinics, therefore it consists of only those patients requiring orthopedic care. Entry into SFR is not compulsory. Information was provided to SFR through medical notes and patient questionnaires (Möller et al. Citation2013).
A closer study of injury mechanisms is made possible when supplementing STRADA data with data from SFR, which among other things contains very detailed information on the fracture.
Data from the two registers were selected based on the following criteria: transport related incidents in Sweden and persons of all genders from 16 years of age. Available data included those crashes occurring from January 2014 to December 2016, which involved most recent data when this study began. Cases from the two different datasets were then matched by the Swedish Transport Agency, using the Swedish Personal Identity Number to match SFR cases with STRADA.
Variables
The variables available in each dataset can be seen in the Appendix, Table A1. All injury details used in the analysis were taken from SFR, while crash details were taken from the relevant database in STRADA. The fracture location was classified in each dataset into: clavicle, scapular, humerus, radius or ulna, bones in the hand (carpals, metacarpals and phalanges), pelvic bone, acetabulum, femur, acetabulum, tibia or fibular (excluding malleolar regions), bones in the ankle (malleolar bones), bones in the foot (tarsals, metatarsals and phalanges), and vertebral bones.
Table 1. Results of the binary logistic regression examining the association between the impacted vehicle and the energy of the fracture.
Analysis
Descriptive analysis was conducted on available variables in the full SFR dataset to obtain baseline fracture data, the matched STRADA and SFR dataset to examine fractures within all transport types and only cyclists within the matched dataset. Geographical locations were normalized by the total population for each region in 2016 as reported by Statistics Sweden (SCB Citation2017).
Significant associations between variables were explored using chi-squared tests of independence in both the total matched dataset and for cyclists only. Specifically, associations between age and gender with the location of fracture and age and gender with transport mode.
High and low energy fractures were used as a measure of higher and lower severity fractures. The energy of the fracture was defined in SFR, where a ‘high energy’ fracture was one resulting from a traffic crash involving a fall from height and a ‘low energy’ fracture involved a fall in the same plane. These definitions are analogous to ‘high-side’ and ‘low-side’ motorcycle crashes, where ‘low-side’ (low energy) refers to a loss of traction, resulting in the rider falling with the bike and skidding along the roadway and the term ‘high-side’ (high energy) refers to any crash when the rider is thrown up and off the bike. High-side motorcycle crashes are typically associated with higher severity.
Logistic regression was used to examine factors influencing the occurrence of a high energy fracture in crash involving cyclists.
Analysis was conducted with IBM SPSS Statistics 24 (IBM Citation2016).
Results
Description of the data
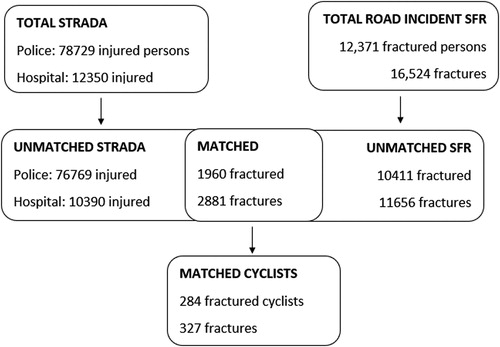
The total STRADA dataset consisted of 12,350 injured persons recorded based on hospital records and 78,729 injured persons based on police records from all road crashes (). The total SFR dataset of those fractured in road crashes between 2014 and 2016 consisted of 12,371 fractured persons. A total of 15.8% of the SFR cases were able to be matched against STRADA (either hospital or police), resulting in a total matched dataset of 1,960 fractured persons, amongst them suffering 2,881 fractures. When cyclist crashes were extracted from the matched dataset, there were 284 fractured cyclists who suffered 327 fractures among them. Of this, 200 cyclists had police report information and 139 cyclists had hospital information.
Figure 1. Number of injured persons and injuries between 2014 and 2016 for the different datasets in all crashes and matched dataset.
Total Swedish fracture register
The total SFR dataset related to road crashes involved 12,371 patients who suffered a fracture on at least one body part, which consisted of 14,537 fractures. Most of those fractured persons suffered only one (n = 10,883) or two fractures (n = 1,114), but some had up to 15 fractures from the crash.
As seen in , fractures resulting from a crash in a bus (median age 70) and train or tram (median age 73) involved older patients, whereas fractures following a motorcycle crash more frequently involved younger patients (median age 33). The median age of pedestrians and cyclists who had a fracture were in the 50–60-year-old age range, while three-wheelers, cars and trucks were in the 40-year-old age range. These differences, as well as several results presented below, may be driven by differences in exposure; this will be elaborated further in the “Discussion” section.
Figure 2. Boxplot of the age of fractured persons for each transport mode in SFR.

Total matched dataset
The total matched dataset involved 1,960 patients who suffered a fracture on at least one body part and among them, they suffered 2,352 fractures. The age and gender distribution can be seen in the Appendix, Figure A1. The highest proportion of fractures were to those aged between 21 and 25 (11.7%). Males dominated overall (61.1%) and within age groups, except for those over the age of 76.
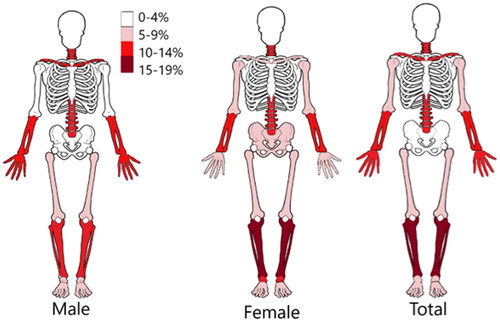
The main body regions fractured were the tibia/fibula (14.7%) and the vertebra (12.8%). The distribution of the fractured body regions by gender is shown in , with numbers provided in Appendix, Table A2. According to χ2 test of independence, the relation between fractured body region and gender was significant (p < 0.0005), with the main observable differences being fractures at the clavicle and pelvis.
Figure 3. Percentage of fractures within the different body regions for persons involved in all matched crashes.
Car occupants were most frequently involved (37%), followed by motorcyclists (27.6%) and bicyclists (15.4%) - Appendix, Figure A2. There was a significant association between transport mode and gender (p < 0.0005). Overall, there was a larger number of female pedestrians with a fracture than male; however, there was a much larger number of male motorcyclists fractured than there were females. Overall, the 21–25-year-old age group was the largest (11.7%), followed by 16–20-year-olds (9.9%), see Appendix, Figure A3.
The proportion of fractures on the different body regions by transport mode can be seen in the Appendix, Figure A4. Notably, 69.4% of all vertebral fractures were to car occupants, 39% of all foot fractures happened to a motorcycle rider. Additionally, 54.9% of acetabulum fractures were to car occupants and 32.5% for pelvic fractures were to pedestrians.
Fractures occurred most frequently in the summer months (June – August), see Appendix, Figure A5. Contrarily, 75% of the fractures occurring while on a train/tram were in March and 50% of fractures which occurred while on a bus were between January and March, with a further 38.5% occurring in December. However, the overall numbers in these groups were very small.
Cyclists
There was a total of 284 cases of cyclists who suffered a fracture who were included for analysis, with one cyclist being included twice due to being involved in two separate cases. The warmer months (May to October) had a higher proportion of fractured riders, and the most common month was August (15.8%), Appendix Table A3. Västra Götalands county involved the largest number of riders (21.8%), see Appendix Figure A6.
Fractured riders were predominantly males (53.9%). The average age of all fractured cyclists was 48.75 years, ranging from 16 to 87 years. Appendix, Table A4 displays the proportion of cyclists within the different age groups by gender. Those aged 50+ years accounted for the largest proportion of both males (21.6%) and females (24.4%). There was a smaller proportion of females than males in the youngest three age groups.
Among the 284 cyclists, there were 327 fractures. These fractures were predominantly to the radius/ulna (17.4%), clavicle (14.1%) and tibia/fibula (13.1%). Fractures to the hand (12.8%), vertebra (8%) and humerus (7%) also occurred frequently.
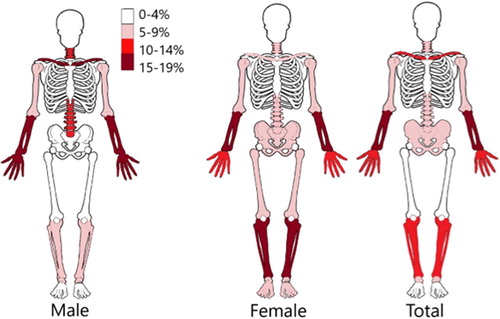
χ2 test of independence found significant association between gender and location of fracture (p = 0.004). Females mostly suffered a higher percentage of fractures than males to the lower limbs including the pelvis, acetabulum, femur, tibia ankle and feet ( and Appendix Table A5). Males tended to have a higher percentage of fractures to the upper limbs, including the clavicle, scapular, radius/ulna and hand. Males also suffered a higher percentage of fractures to the vertebra.
Figure 4. Percentage of fractures in each body region of the cyclist.
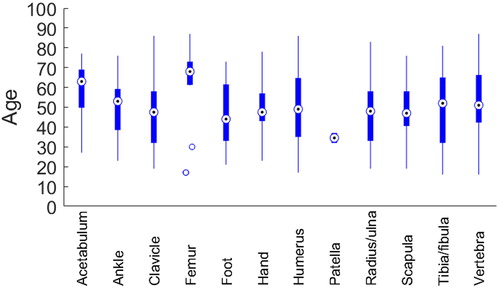
The results in suggest a difference of injury location by age group. However, the difference was not statistically significant according to a chi-square test of independence (p = 0.27). Initial analysis did not meet expected cell counts, so small numbers were grouped and reanalyzed, but the repeated tests still did not give significant differences.
Figure 5. Mean age for the fractured body regions of the cyclist.
Out of the 327 injuries, 162 (49.5%) were coded as a ‘high energy injury’ and 38.5% were ‘low energy’, with 12% unknown. Fractures to the acetabulum (100%), pelvis (84.2%), vertebra (75%) and tibia (70.3%) were most frequently high energy fractures, whereas fractures to the upper extremities, including radius/ulna (58.8%) and humerus (63.2%) were more frequently low energy fractures (Appendix, Figure A7). A test of independence found that body region and the energy of the impact were significantly associated (p = 0.006).
Males contributed to 51.9% of the high energy injuries and 54.8% of the low energy injuries, and there was no significant relationship observed between gender and the energy of the injury.
The most common impact partner to the cyclists was a car (58.5%). Single bicycle crashes (no impact partner) were also frequent (21.8%). Logistic regression found that single bicycle incidents (OR = 0.165) and collisions with another bicycle (OR = 0.148) were significantly less likely to result in a high energy fracture than a collision with a car ().
Police reports were available in 200 of the 284 fractured cyclist cases. Results from these police reports found that, disregarding unknown values, collisions with a car frequently occurred in an urban environment (88.9%) and on an urban street (62.6%), most frequently at an intersection (47.7%), see Appendix, Table A6. Only one collision occurred on a motorway. The weather was mostly dry (84%), with a dry road (71.6%) and under daylight conditions (77.7%).
Discussion
The first aim of this investigation was to match SFR with STRADA and to examine this matched dataset. This investigation found that the number of cases which were able to be matched were low, with only 15.8% of SFR being matched with STRADA. From a total number of 12,371 cases of fractured people involved in road crashes, only 1960 were able to be matched with the STRADA dataset, and this consisted of 284 cyclists. One contributing factor could be that there was a mismatch in national coverage in the regions where STRADA and SFR collect data and additionally that reporting to STRADA hospital data is voluntary and requires consent by the patients. However, further analysis is needed to identify all factors contributing to the low matching percentage and understand the type of fractures in road crashes that exist in SFR but are not matched in STRADA.
The combined datasets provided a high number of variables, with both details about the crash, including road conditions and weather conditions, as well as detailed information about the fracture, including energy of the fracture, and long-term follow-up information. However, the long-term follow up information was not available for our use at this stage but would be of great use in the future.
The matched dataset was used to look at the overall pattern of fractured road users. Cars were the vehicle type which were most frequently involved in crashes resulting in fractures (37%), followed by motorcycles (27.6%) and bicycles (15.4%). Fractured cyclists were typically younger than bus, train or tram riders, but older on average than motorcyclists.
Additionally, there were gender differences. Overall, there was a larger number of female pedestrians with a fracture than male; however, there was a much larger number of males who were fractured when riding a motorcycle. This may be a result of exposure, as shown in a study in Australia, where the population data reported 88% males and correspondingly, 94% of the injured sample were males (Brown et al. Citation2015). In Sweden, males have also been recorded to travel a higher number of kilometers per day than females, and those males aged 55–64 years rode the longest every day (7 km per day) (Holmström Citation2017). Furthermore, it has been found by Wennergren et al. (Citation2018) that there is predominance of men among tibia fractures caused in traffic.
Cyclists fracture locations differed to all other road users as all other road users suffered the highest proportion of fractures to the bones in the lower leg (14.7%), whereas cyclists were more frequently injured in the lower arm (17.4%).
The different kinematics, ages and genders typically seen in drivers of different vehicle types may explain the difference in the fracture pattern. Cars were the most frequent impact partner resulting in a fracture to a cyclist in this investigation. Single bicycle crashes were also frequent. The fracture energy was different in different crash scenarios, with single bicycle incidents and collisions with another bicycle were significantly less likely to result in a high energy fracture than a collision with a car. This is indicative of different kinematics within different impact scenarios, with single bicycle incidents resulting in the rider sliding along the roadway; whereas impacts with another car or other vehicle result in the rider being thrown in to the air. As such, protection should be designed accordingly.
There is a high number of single bicycle crashes in the STRADA dataset, with single bicycle crashes comprising 69% of all crashes between 2012 and 2014 (Dozza Citation2016), while cars were the most frequent impact partner in SFR, indicating that perhaps impacts with another vehicle tend to lead to fractures more often than those single bicycle crashes. It is worth noting that there have been under-reporting problems identified within the police reporting of STRADA, specifically with regards to single vehicle crashes (Held Citation2016). Additionally, until May 2014, within the study time period, the police reporting system for STRADA had some issues, so approximately 20% of police-reported cases in the first half of 2014 were missing in the database.(Transport Styrelsen, n.d.)
Additionally, within cyclists, the injury location varied based on gender. Females mostly suffered a higher percentage of fractures than males to the lower limbs including the pelvis, acetabulum, femur, tibia ankle and feet. Males tended to have a higher percentage of fractures to the upper limbs, including the clavicle, scapular, radius/ulna and hand. Males also suffered a higher percentage of fractures to the vertebra. This could be associated with intrinsic differences in males and females body types such as height and weight differences as well as potentially indicating that there could be different kinematics between female and male riders following a collision as a result of different body types, or that males and females are involved in different types of collisions. The results showed a significant correlation between high-energy and low-energy crashes and collision partner, which would explain different injuries in different types of collisions. Unfortunately, for this study, data was not available on patient details such as height and weight, so it was not possible to observe differences in gender based on height and weight and injury outcome. Collision types and falling patterns should be explored further, particularly in relation to gender differences. There may be a need for improved mitigation strategies, which should address both gender-related effects and other differences associated with gender.
Protection should also be designed for different crash scenarios, with high and low energy fractures occurring in crashes with different impact partners and resulting in fractures to different parts of the body. In cyclists, therefore, there is also a need to examine closely the injury kinematics for fractures to different body regions so that body region and cyclist specific protection can be created. Additionally, while independence of age group and injury location could not be rejected by the chi-square test, differences in the corresponding percentages suggest that a significant dependence could possibly be found in larger samples.
A study by Stigson et al. (Citation2014) examined kinematics of fractures to the clavicle, which were found to be the most frequently occurring injury. Injury to the shoulder was a result of a direct blow to the shoulder in 90% of cases and falling onto an outstretched arm in only 1 case. Similarly to Stigson et al. (Citation2014) this study found that the upper limbs were the most frequently fractured, involving mostly the radius, ulna and clavicle. However, high energy fractures were most frequently to pelvis, vertebra and lower limbs. Low energy fractures occurred more frequently to the radius and ulna. It is therefore necessary to focus on protection for the upper limbs as well as the pelvis, vertebra and lower limbs, with different protection to suit the different impact scenarios, so that both most frequently occurring injuries and highest severity injuries can be prevented.
Motorcycle protection focuses on garments with fitted energy absorption, or ‘impact protectors’, at certain regions in motorcycle specific clothing and this could be an option for cyclists. However, while impact protection has been shown to attenuate sufficient energy to prevent fractures (Nygren Citation1987), in the real world, it was shown to prevent injury overall but not specifically fractures (Rome et al. Citation2011). More recent advancements, such as airbag jackets, may provide further protection.
Cyclists were more frequently fractured in the summer months, which matched with previous reports on cyclist flow in Gothenburg, where cyclists flow was greater in the warmer months, with the exception of July when the Swedish population is on holidays (Dozza Citation2017). These results are also in line with previous study on tibia fractures caused by traffic (Wennergren et al. Citation2018). This indicates that the increase in cyclists suffering fractures as a result of a crash in summer is likely due to increased exposure. No cyclists reported having a crash in the snow; however, one was riding on a snowy road. This may additionally indicate that there a fewer cyclists riding in bad weather.
Supplemental Material
Download MS Word (304.8 KB)Acknowledgments
We would like to thank Marianne Andersson and Robert Thomson for the discussions and earlier involvement in the project. We would also like to thank Jan Ekelund and Michael Möller from SFR for their support and assistance. The work was carried out at the SAFER Vehicle and Traffic Safety Center at Chalmers University of Technology, Gothenburg, Sweden.
Additional information
Funding
References
- Brown J, Fitzharris M, Baldock M, Albanese B, Meredith L, Whyte T, Oomens M, Ma A. 2015. Motorcycle In-depth Crash Study. Sydney: Austroads.
- Dozza M. 2017. Crash risk: How cycling flow can help explain crash data. Accid Anal Prev. 105:21–29. 10.1016/j.aap.2016.04.033.
- Forward S, Samuelsson P. 2007. Strada - blev det som det var tänkt? (Tech. rep. No. 600). https://www.vti.se/sv/publikationer/pdf/strada–blev-det-som-det-vartankt.%0Apdf.
- Held F. 2016. Investigation of under-reporting and the consistency of injury severity classifications in Swedish police crash data compared to hospital injury data based on the Swedish Traffic Accident Data Acquisition (STRADA). Chalmers University of Technology, Gothenburg.
- Holmström A. 2017. The Swedish national travel survey 2015–2016. Stockholm: Trafikanalys. https://www.trafa.se/kommunikationsvanor/RVU-Sverige/.
- Howard C, Linder A. 2014. Review of Swedish experiences concerning analysis of people injured in traffic accidents. Linköping: VTI. http://vti.diva-portal.org/smash/get/diva2:699198/FULLTEXT01.pdf.
- IBM .2016. SPSS Statistics 24. United States.
- Juhra C, Wieskötter B, Chu K, Trost L, Weiss U, Messerschmidt M, Malczyk A, Heckwolf M, Raschke M. 2012. Bicycle accidents – Do we only see the tip of the iceberg? A prospective multi-centre study in a large German city combining medical and police data. Injury. 43(12):2026–2034. doi:10.1016/j.injury.2011.10.016
- Möller M, Ekholm C, Sandelin A, Akrami L, Leandersson M. 2013. The Swedish Fracture Register: Annual report 2013. Vástra Götaland: Svenska Frakturregistret (The Swedish Fracture Register).
- Niska A, Eriksson J. 2013. Statistik över cyklisters olyckor Faktaunderlag till gemensam strategi för säker cykling. https://www.vti.se/sv/publikationer/pdf/statistik-over-cyklisters-olyckor-faktaunderlag-till-gemensam-strategi-for-saker-cykling.pdf.
- Nygren A. 1987. Protective effect of a specially designed suit for motorcyclists. Bochum, Germany: Institut fur Zweiradsicherheit (IFZ).
- Rome L. D, Ivers R, Fitzharris M, Du W, Haworth N, Heritier S, Richardson D. 2011. Motorcycle protective clothing: Protection from injury or just the weather? Accid Anal Prev. 43(6):1893–1900. doi:10.1016/j.aap.2011.04.027
- SCB. 2017. Population in the country, counties and municipalities on 31 December 2016 and Population Change in 2016. https://www.scb.se/en/finding-statistics/statistics-by-subject-area/population/population-composition/population-statistics/pong/tables-and-graphs/yearly-statistics–municipalities-counties-and-the-whole-country/population-in-the-country-counties-and-municipalities-on-31-december-2016-and-population-change-in-2016/.
- STA. 2014. Analys av trafiksäkerhetsutvecklingen inom vägtrafik 2013. Borlänge: Trafikverkat (Swedish Transport Administration).
- Stigson H, Krafft M, Rizzi M, Kullgren A. 2014. Shoulder injuries in single bicycle crashes. Paper presented at International Cycling Safety Conference. p. 1–8.
- Transport Styrelsen. (n.d.). Mörkertal i statistiken. https://www.transportstyrelsen.se/sv/vagtrafik/statistik/Olycksstatistik/morkertal-i-statistiken/.
- Wennergren D, Bergdahl C, Ekelund J, Juto H, Sundfeldt M, Möller M. 2018. Epidemiology and incidence of tibia fractures in the Swedish Fracture Register. Injury. 49(11):2068–2074. doi:10.1016/j.injury.2018.09.008
- Wennergren D, Ekholm C, Sandelin A, Möller M. 2015. The Swedish fracture register: 103,000 fractures registered. BMC Musculoskelet Disord. 16:338. doi:10.1186/s12891-015-0795-8
- Wennergren D, Möller M. 2018. Implementation of the Swedish Fracture Register. Unfallchirurg. 121(12):949–955. doi:10.1007/s00113-018-0538-z