
Abstract
Background
Alcohol consumption is a well-known risk factor for sustaining road traffic injuries worldwide. Malawi is a low-income country with a large and increasing burden of road traffic injuries. It has generally been viewed as a country with relatively little alcohol consumption. This study investigates the role of alcohol in road traffic injuries in and around the capital Lilongwe.
Methods
All patients presenting to the emergency department of Kamuzu Central Hospital after being injured in road traffic crashes were asked to participate in the study. Alcohol testing was done with a breathalyzer or a saliva test. Participants were asked about alcohol use before the injury as well as hazardous drinking using the AUDIT-C questionnaire.
Results
Of 1347 patients age 18 years or older who were asked to participate, 1259 gave informed consent, and data on alcohol use (alcohol test results and/or self-reported intake) were available for 1251 participants. Of those, 251 (20.1%) tested positive for alcohol, whereas 221 (17.7%) reported alcohol use before the crash; in total 311 (24.9%, 95% CI 22.5–27.3) either tested positive, reported use, or both. Females had a low prevalence of alcohol use (2.5%), while 30.6% of males had consumed alcohol before the injuries. Pedestrians had the highest prevalence at 41.8% (95% CI 35.5–48.4), while car drivers had 23.8% (95% CI 18.2–30.5). Among male pedestrians, 49.5% had used alcohol before the injury. Alcohol-associated injuries had a peak in the evening and at night, especially in the weekends. Of the patients, 63.1% reported that they had not consumed alcohol during the last year, while 21.4% had an AUDIT-C score suggesting hazardous drinking, and 66.2% of those had used alcohol before the injury.
Conclusions
A large percentage of road traffic injured patients had been drinking alcohol before their injury, especially male pedestrians. A large proportion of the patients were abstaining from alcohol, but those not abstaining had a high prevalence both of alcohol use when injured and hazardous drinking identified by AUDIT-C. This has important implications for prevention.
Introduction
Injuries and deaths due to road traffic crashes are a major concern globally. In the World Health Organization (WHO) African Region, the mortality from road traffic injuries (RTI) was estimated to be 26.6/100 000 in 2016, nearly three times that in the WHO European region at 9.3/100 000 (World Health Organization Citation2018b). Alcohol consumption is considered to be an important risk factor for road traffic injuries worldwide. An international survey of official crash statistics revealed that an average of 21.8% of road deaths were alcohol related (Vissers et al. Citation2017). As the authors of that report state, this is probably an underestimation because of underreporting and lack of testing.
In most high-income countries, the incidence of road traffic injuries is decreasing (World Health Organization Citation2018b). In low-income countries, however, road traffic injuries are still expected to increase due to increasing economic growth and motorization (World Health Organization Citation2018c) and also because of increasing use of alcohol and consequently a likely increase in drunk driving (Christophersen et al. Citation2016). Low-income countries also have large proportions of vulnerable road users such as pedestrians and cyclists, poor road infrastructure, insufficient law enforcement, bad technical standards on vehicles, and it is likely that road users under the influence of alcohol have a larger traffic crash risk in these settings.
A major obstacle for efforts to reduce drink driving, and thereby reducing injuries, is the lack of data and reliable information about the magnitude of the problem (Stewart et al. Citation2012). Relatively little is known about alcohol use among those sustaining road traffic injuries in Sub-Saharan Africa. Most of the research on the subject is from South Africa, where there are very high rates of alcohol use in road traffic injuries. For example, one study found that 58% of pedestrian fatalities in that country were alcohol related (Mabunda et al. Citation2008), and many other studies also point to alcohol as a particularly big problem in this country (Nicol et al. Citation2014; Du Plessis et al. Citation2016). However, South Africa is an upper-middle income country, and it is in many respects very different from its poorer neighboring countries, and results from here might not be relevant for the rest of the region.
Outside South Africa, there are only a very few studies that have addressed the problem of alcohol associated road traffic injuries in Sub-Saharan Africa. Alcohol testing of road traffic injury patients in the emergency room has been done in two studies from Ghana. In one of the studies, Damsere-Derry and coworkers found that 53% of cyclists, 34% of motorcyclists and 21% of pedestrians had used alcohol before the injury. There were only 6 car drivers in this study, and 76% of the injured road users were motorcyclists (Damsere-Derry et al. Citation2018). In another study where 1085 road traffic injury patients were investigated, it was found that 42% of both drivers and pedestrians tested positive for alcohol (Forson et al. Citation2017). In a study from the Ivory Coast they performed blood alcohol testing in the emergency department on 672 patients (Diakite et al. Citation2014). The blood alcohol concentration (BAC) at the time of injury was estimated by back-calculation using the recorded time lag between the crash and collection of blood sample. They extrapolated that 30% of drivers, 13% of passengers and 17% of injured pedestrians had a BAC over 0.05% at the time of injury. A recent study from Kampala, Uganda (Biribawa et al. Citation2019), found that 29.7% of road traffic injured patients had been consuming alcohol before their injury. Among the pedestrians, 44% had been consuming alcohol while 17% of the vehicle occupants had consumed alcohol. Patients with alcohol consumption prior to the injury had a higher risk of dying in the emergency room.
Malawi has generally been viewed as a country with relatively low alcohol consumption. A household survey conducted in 2012 found that 27% of males and 1.6% of females had consumed alcohol the last 12 months, and that 85.5% of the population had abstained from drinking alcohol the last year (Eide et al. Citation2013). In 2016 the WHO estimated that 86.1% of females and 66.4% of males above 14 years of age had abstained from drinking alcohol the last year in Malawi, and that the average consumption of alcohol was 3.7 liters pure alcohol per person, far lower than the African average of 6.3 liters (World Health Organization Citation2018a). A previous study at Kamuzu Central Hospital in Lilongwe, the site of the present study, recorded that alcohol was involved in 9.3% of trauma admissions between 2011 and 2015. This was based only on clinical judgment, not objective testing (Eaton et al. Citation2017).
Despite that Malawi has a low consumption of alcohol, it has a very high rate of road traffic deaths at 31/100 000 inhabitants (World Health Organization Citation2018b). The aim of this study was to investigate the prevalence of alcohol use among injured road traffic crash victims, in relation to gender and age, level of education, type of road user, and time of day and week. We also wanted to determine the prevalence of hazardous drinking by using a short questionnaire.
Materials and methods
Study design and setting
This was a cross sectional study of road traffic injury patients admitted to the emergency department at Kamuzu Central Hospital (KCH). KCH is a 900-bed hospital located in the Central Region of Malawi. Central Region has eight districts including Lilongwe, the capital city, where KCH is located. It serves as the only referral hospital for Central Region’s population of 7.5 million. Lilongwe district alone has a population of 1,600,000. Each district has a public district hospital that manage minor trauma cases and refer more severe cases needing further treatment to KCH.
Data collection
All patients 18 years and above presenting to the KCH Emergency Department with road traffic injuries were asked to participate in the study. Injury victims younger than 18 years, those brought in dead and those who did not consent, were excluded. Those who could not immediately give consent, e.g., because of altered state of consciousness, were tested and included and consent was sought later when the patient was stable. If consent was not obtained later, the data were deleted.
Data were collected from May 25, 2019 to August 22, 2019. Data collection was done by two qualified medical doctors who were employed and trained by the project. They worked shifts to cover all hours of the day every week during the inclusion period. Project coordinators (authors CK & GM) supervised the data collection to ensure that adequate and comprehensive data were collected. Data were collected using an electronic tablet that had the questionnaire and database installed (FileMaker Pro software, Apple Inc., Cupertina, CA).
Alcohol testing and self-reported alcohol use
Patients who could cooperate and were respiratory stable were tested with a breathalyzer (Dräger Alcotest 5820, Drägerwerk AG & Co., Lübeck, Germany). Unconscious patients, non-cooperative patients or patients with respiratory distress were tested using a saliva alcohol test (Q.E.D.® A150, Orasure Technologies, Inc., Bethlehem, PA, USA). Alcohol concentrations corresponding to BAC of 0.010% or higher were regarded as positive. The diagnostic performance of the two types of testing was good (see online supplemental material, Appendix A1).
If the time between crash involvement and arrival at hospital was more than a few hours, alcohol testing of breath or saliva might not reflect the presence of alcohol in the body at the time of injury due to metabolism and elimination of alcohol. Therefore, the patients were also asked whether they had used alcohol before the injury. A patient was characterized as alcohol positive if either the analysis of alcohol in breath or saliva gave a positive result or the patient reported alcohol use before the injury.
AUDIT-C
The AUDIT-C questionnaire is a validated screening tool used to detect hazardous drinking (Bradley et al. Citation2007). Using a three-item questionnaire, respondents were asked about how often they drink alcohol, how many units they drink on a typical day of drinking, and how often they drink more than 6 units, and points from 0 to 4 are given for each of the alternative answers (Warne Citation2018). The AUDIT-C was considered positive if the respondent got 4 or more points for males, 3 or more for females. The doctors doing the inclusion were familiar with the local types of alcohol consumed, and the alcohol content of these beverages was converted to standard alcohol units by using a table (see online supplemental material, Appendix A2).
Statistical analysis
To evaluate the statistical significance of differences between groups, logistic regression was performed. Alcohol use prior to the injury and being AUDIT positive were used as dependent variables, and age groups, gender, road user types and education were used as independent variables. The results are presented as odds ratios. Confidence intervals (95% CI) were calculated for prevalences and odds ratios. Patients with missing data on alcohol use before the injury were excluded. Data analysis was done with STATA (version 15 Stata Corp LLC, College Station, TX, USA) and SPSS Statistics version 25 (IBM Corporation, Armonk, NY, USA). The manuscript was prepared adhering to the principles of the STROBE-statement (Vandenbroucke et al. Citation2014).
Ethical issues
Strict confidentiality was ensured in the inclusion process and data handling, and law enforcement officials were not able to access this information. The name, date of birth or any other direct identifiable information was not recorded, and the signed informed consent sheets were stored in a separate archive with restricted access, and without any link to the questionnaire and database.
The study was approved by the Malawi National Health Sciences Research Committee (approval no. 1962/2018). The Norwegian Regional Health Research Committee was consulted and they stated that a formal application to them was not needed (Norwegian Health Research Act §2 and §4a). The Data Protection Officers of Diakonhjemmet Hospital and the Norwegian Institute of Public Health have approved the data handling, after conducting a Data Protection Impact Assessment according to EU legislation.
Results
Inclusion and missing data
A total of 1347 road traffic injury patients met the inclusion criteria and were asked to participate in the study. Consent was not given by 88 patients (6.5%). Eight patients lacked registrations for alcohol use (alcohol test result or self-reported alcohol intake) and were therefore excluded, leaving 1251 patients for analysis. Of these, there were missing information about previous drinking the last year and AUDIT-C values for 24 patients, gender was missing in 16 patients and age was missing for 14 patients. Patients with missing values were excluded from analyses where these missing values were needed.
Participants
There were 19.4% females and 80.6% males. 20.5% were 18–24 years old, 38.0% were 25–34 years, 23.7% were 35–44 years, and 16.6% were older. Level of education had the following distribution; 40.8% had only completed primary education, 34.6% secondary education, 20.6% college or university, whereas 2.9% had no formal education. For 1.1%, education level was not recorded. Passengers in cars, minibuses, on lorry beds, motorcycles and bicycles constituted the largest group of injured road users with 35.9%, followed by pedestrians (17.6%), bicycle riders (14.6%), car and pickup drivers (14.5%), motorcycle drivers (12.0%), and others or not specified (5.4%). The majority (73.9%) were injured in road traffic crashes on urban roads.
Alcohol use before injury
In total, 221 (17.7%; 95% CI 15.7–19.9) road users reported drinking alcohol before the injury, whereas 251 (20.1%; 95% CI 17.9–22.4) tested positive for alcohol on arrival to the hospital. A total of 311 patients (24.9%; 95% CI 22.5–27.3) either tested positive, or reported alcohol use, or both, before the injury.
A smaller proportion of female injured patients had used alcohol (either self-reported or positive alcohol test) before the road traffic crash (2.5%; 95% CI 1.2–5.4) than male patients (30.7%; 95% CI 27.9–33.6); the odds ratio for alcohol use among females relative to males was 0.06 (95% CI 0.03–0.13). The highest prevalence of alcohol use was found among patients aged 25–44 years; there seemed not to be any significant association between alcohol use and education level; see .
Table 1. Prevalence (%) and odds ratio for alcohol use in relation to age and education.
The prevalence of alcohol use among different types of injured road users is presented in ; the largest prevalence of alcohol use was found among injured pedestrians. When looking only at the male group, we found that 49.5% of male pedestrians had consumed alcohol before the injury, 25.5% of male motorcycle drivers, 27.5% of male car/pickup drivers, 20.8% of male bus/minibus/lorry drivers, 31.5% of male passengers and 19.7% of male bicycle riders (results not shown in tables).
Table 2. Prevalence (%) and odds ratio for alcohol use among road user groups.
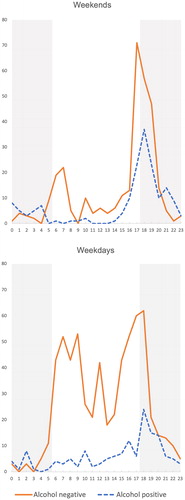
The distribution of injuries during weekdays and weekends is presented in , with separate graphs for alcohol positives and negatives. The figure shows that the injuries most often happened in the morning and afternoon of weekdays, and early evening during weekends. We see that during the week, the alcohol negative cases had two spikes corresponding to the morning and evening traffic rush hours.
Figure 1. Time of injury, dark background corresponding to hours of light reduced conditions.
Alcohol drinking patterns
There were 452 patients who reported drinking alcohol during the last year, 36.9% of the total. Of these, 272 (60.2%) had been drinking alcohol before the injury and 257 (58.9%) had an AUDIT-C result indicating hazardous drinking. Of the 263 patients (21.4%) with an AUDIT-C above cutoff, 174 (66.2%) had been drinking alcohol before the injury. shows the distribution of participants with an AUDIT-C result above cutoff. Twenty-four participants did not answer the AUDIT-C questions.
Table 3. Prevalence (%) and odds ratio for positive AUDIT-C results.Table Footnote*
Discussion
This study demonstrated that one in four road traffic injury patients in Lilongwe had been drinking alcohol before being injured, despite expectations that the level of alcohol use in Malawi was low. As expected, males were much more likely to have used alcohol when injured. About half of the injured male pedestrians and about one fourth of male drivers/riders had use alcohol before the crash occurred. The injuries had a diurnal variation, where the incidence of injuries peaked in the evening hours. After around 8 PM, around half of all injured patients had been drinking alcohol.
We may assume that the percentage of alcohol related injuries actually is even higher: some of the patients who had not been drinking in our material, still might have been involved in alcohol related road traffic crashes, where the drivers of the other vehicle involved in the crash was influenced by alcohol. It is, however, important to note that even if a patient had been drinking alcohol, we cannot automatically claim a causal relation between the intake of alcohol and the injury. In many of the cases, for example in drivers and in some cases pedestrians, such a causal relation most likely exists, but for example in car passengers, the use of alcohol cannot be viewed as a cause of the injury. We can also not exclude the possibility that some injured road users had consumed alcohol after the crash.
Our results resemble those from Uganda (Biribawa et al. Citation2019), where the pedestrians had a much higher prevalence of alcohol use than drivers. The one Ghanaian study with an adequate number of car drivers shows a different pattern, with approximately the same prevalence in pedestrians and drivers (Forson et al. Citation2017). In Ivory Coast, drivers also had a higher prevalence among drivers compared to pedestrians (Diakite et al. Citation2014). The reason for these differences between the countries are probably multifactorial, and cannot readily be explained by the amount of alcohol use in the population, as the WHO estimates that Uganda and Ivory coast has a much higher alcohol consumption than Malawi and Ghana, both for the total population and the average consumption by males that are regular drinkers (World Health Organization Citation2018a). What Uganda and Malawi have in common, however, is that they are low-income countries with a GDP per capita that is less than half of the two other middle-income countries (World Health Organization Citation2018b). Factors related to economic development such as the composition of the vehicle fleet, or timing and speed of increase in vehicle ownership rates might be possible reasons for these differences.
Almost two thirds of the patients reported no alcohol use during the last year. Given previous knowledge about alcohol use in Malawi (Eide et al. Citation2013), this is not surprising. However, of those reporting any alcohol use at all in the last year, more than half had an AUDIT-C result indicating hazardous alcohol use. Two out of five of those reporting alcohol use in the last year, and two out of three of the Audit-C -positives had been drinking alcohol before their injury. This gives an impression of a pattern of alcohol use where a large part of the population is abstaining from alcohol, but those who are not abstaining, have a high incidence of risk drinking and drink driving.
Our study has demonstrated a high prevalence of alcohol use among those injured in traffic, especially in the evening hours and at night, and during weekends. Malawi has a legal BAC limit of 0.08%, with fines for first time offenses and possible prison sentences for recurrent offenses. In this very resource limited setting, it is vital that interventions aimed at reducing road traffic injuries are cost effective. Ditsuwan et al. (Citation2013) studied the cost-effectiveness of interventions aimed at reducing injuries caused by driving under the influence of alcohol in Thailand and found that mass media campaigns and both random and selective breath testing were cost-effective. Increasing all three interventions were estimated to decrease the burden of road traffic injuries related to drunk driving by 24%. Our study also demonstrates that drunk driving was not the only alcohol-related problem; many pedestrians had also been injured while being under the influence of alcohol. Legal blood alcohol limits for pedestrians will never be an issue, so preventive measures should aim at protecting these vulnerable road users from harmful impact. Speed control by building speed bumps and speed tables (Bishai and Hyder Citation2006; Damsere-Derry et al. Citation2019) is shown to be very cost-effective, as well as increased law enforcement (Bishai et al. Citation2008). Safer road crossings where vehicles are forced by physical interventions to lower their speed, are vital for pedestrian safety especially when pedestrians are intoxicated or behave irresponsibly (Gårder Citation2018).
To conclude, one in four road traffic injured patients had been drinking alcohol before sustaining their injury in this study, and male pedestrians had the highest prevalence of alcohol use at 49.5%. Though 63% of RTI patients did not normally drink alcohol, the 37% not abstaining had a high prevalence of possible risk drinking and alcohol use when injured. This has important implications for prevention.
Strengths and limitations
The study had several strengths, including its large size, with representative selections of many subgroups of patients, and the objective nature of the alcohol testing. The relative completeness of the inclusion during the study period, and the relatively low rate of refusal of consent at only 6.5%, also contributed to reliable data.
The study had a cross-sectional design, and it was not possible to make inferences about causal relations. The relatively long time from injury to presentation for some patients is a limitation in the reliability of alcohol testing in this study. Thus, the prevalence of alcohol use in the study was most likely underestimated because of the metabolizing of alcohol, resulting in negative tests. There are multiple possible sources for bias, as the following groups of patients are not included: patients that die before admission to hospital, patients under 18 years of age, patients with very mild injuries, patients that do not consent to participate, and patients that are treated at private or other hospitals. Lilongwe is one of two major urban areas in Malawi, but most of the population in Malawi live in rural areas. The results from this study might therefore not be representative for the country as a whole, even if it is a referral hospital for large rural areas.
Supplemental Material
Download MS Word (18.5 KB)Acknowledgments
The study had not been possible without the recruitment work done by Lovemore Kamange and Noel Yotamu at the KCH and the administrative and technical support from Elin H. Wyller at the Norwegian Institute of Public Health and Håvard Furuhaugen at Oslo University Hospital.
Data availability statement
We do not have permission to share non-aggregated research data.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Biribawa C, Kobusingye O, Mugyenyi P, Baguma E, Bua E, Alitubeera PH, Tumwesigye NM. 2019. Pre-injury alcohol use and road traffic injury among patients at Mulago National Referral Hospital, Kampala, Uganda: cross-sectional study. JACRS. 30(4):17–25. doi:10.33492/JACRS-D-18-00261
- Bishai D, Asiimwe B, Abbas S, Hyder AA, Bazeyo W. 2008. Cost-effectiveness of traffic enforcement: Case study from Uganda. Inj Prev. 14(4):223–227. doi:10.1136/ip.2008.018341
- Bishai DM, Hyder AA. 2006. Modeling the cost effectiveness of injury interventions in lower and middle income countries: Opportunities and challenges. Cost Eff Resour Alloc. 4:2–11. doi:10.1186/1478-7547-4-2
- Bradley KA, Debenedetti AF, Volk RJ, Williams EC, Frank D, Kivlahan DR. 2007. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcoholism Clin Exp Res. 31(7):1208–1217. doi:10.1111/j.1530-0277.2007.00403.x
- Christophersen AS, Mørland J, Stewart K, Gjerde H. 2016. International trends in alcohol and drug use among motor vehicle drivers. Forensic Sci Rev. 28(1):38–66.
- Damsere-Derry J, Ebel BE, Mock CN, Afukaar F, Donkor P, Kalowole TO. 2019. Evaluation of the effectiveness of traffic calming measures on vehicle speeds and pedestrian injury severity in Ghana. Traffic Inj Prev. 20(3):336–342. doi:10.1080/15389588.2019.1581925
- Damsere-Derry J, Palk G, King M. 2018. Prevalence of alcohol among nonfatally injured road accident casualties in two level III trauma centers in northern Ghana. Traffic Inj Prev. 19(2):118–124. doi:10.1080/15389588.2017.1369533
- Diakite A, Gadegbeku B, Dano SD, Yapo Ette H, Botti K, Malan AK, Laumon B. 2014. Road traffic injuries involving illegal blood alcohol levels and psychoactive drug use in Côte d’Ivoire: A hospital-based study. Univ J Public Health. 2(5):154–162. doi:10.13189/ujph.2014.020503
- Ditsuwan V, Lennert Veerman J, Bertram M, Vos T. 2013. Cost-effectiveness of interventions for reducing road traffic injuries related to driving under the influence of alcohol. Value Health. 16(1):23–30. doi:10.1016/j.jval.2012.08.2209
- Du Plessis M, Hlaise KK, Blumenthal R. 2016. Ethanol-related death in Ga-Rankuwa road-users, South Africa: A five-year analysis. J Forensic Leg Med. 44:5–9. doi:10.1016/j.jflm.2016.08.006
- Eaton J, Grudziak J, Hanif AB, Chisenga WC, Hadar E, Charles A. 2017. The effect of anatomic location of injury on mortality risk in a resource-poor setting. Injury. 48(7):1432–1438. doi:10.1016/j.injury.2017.05.023
- Eide AH, Braathen SH, Azalde G, Munthali A, Chiocha M, Ndawala J, Natvig H, Hoel E. 2013. Fighting poverty through alcohol misuse prevention in Malawi — revised summary report. Oslo, Norway: SINTEF Technology and Society. https://www.sintef.no/globalassets/upload/helse/levekar-og-tjenester/alma-summary-report-revised-december-2013.pdf.
- Forson PK, Gardner A, Oduro G, Djan D, Adu KO, Ofori-Anti K, Maio RF. 2017. Harmful alcohol use among injured adult patients presenting to a Ghanaian emergency department. Inj Prev. 23(3):190–194. doi:10.1136/injuryprev-2016-042104
- Gårder P. 2018. Providing for pedestrians. In: Lord D, Washington S, editors. Safe mobility: Challenges, methodology and solutions (transport and sustainability) (Vol. 11). Bingley, UK: Emerald Publishing Limited; p. 207–228. doi:10.1108/S2044-994120180000011011
- Mabunda MM, Swart L-A, Seedat M. 2008. Magnitude and categories of pedestrian fatalities in South Africa. Accid Anal Prev. 40(2):586–593. doi:10.1016/j.aap.2007.08.019
- Nicol A, Knowlton LM, Schuurman N, Matzopoulos R, Zargaran E, Cinnamon J, Fawcett V, Taulu T, Hameed SM. 2014. Trauma surveillance in Cape Town, South Africa: An analysis of 9236 consecutive trauma center admissions. JAMA Surg. 149(6):549–556. doi:10.1001/jamasurg.2013.5267
- Stewart K, Silcock D, Wegman F. 2012. Reducing drink driving in low- and middle-income countries: Challenges and opportunities. Traffic Inj Prev. 13(2):93–95. doi:10.1080/15389588.2011.634464
- Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M, Blettner M, Boffetta P, et al. 2014. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int J Surg. 12(12):1500–1524. doi:10.1016/j.ijsu.2014.07.014
- Vissers L, Houwing S, Wegman F. 2017. Alcohol-related road casualties in official crash statistics. Paris, France: OECD International transport Forum. https://www.itf-oecd.org/sites/default/files/docs/alcohol-related-road-casualties-official-crash-statistics.pdf.
- Warne D. 2018. Alcoholism and substance abuse. In: Rakel D, editor. Integrative medicine. 4th ed. Philadelphia, PA: Elsevier; p. 818–828.
- World Health Organization. 2018a. Global status report on alcohol and health 2018. Geneva, Switzerland: World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/274603/9789241565639-eng.pdf?ua=1.
- World Health Organization. 2018b. Global status report on road safety. Geneva, Switzerland: World Health Organization. https://www.who.int/violence_injury_prevention/road_safety_status/2018/en/.
- World Health Organization. 2018c. Projections of mortality and causes of death, 2016 and 2030. Geneva, Switzerland: World Health Organization 2018. [accessed 2020 July 16]. https://www.who.int/healthinfo/global_burden_disease/projections/en/.