
Abstract
Objective
The purpose of this study was to generate biomechanical response corridors of the small female thorax during a frontal hub impact and evaluate scaled corridors that have been used to assess biofidelity of small female anthropomorphic test devices (ATDs) and human body models (HBMs).
Methods
Three small female postmortem human subjects (PMHS) were tested under identical conditions, in which the thorax was impacted using a 14.0 kg pneumatic impactor at an impact velocity of 4.3 m/s. Impact forces to PMHS thoraces were measured using a load cell installed behind a circular impactor face with a 15.2 cm diameter. Thoracic deflections were quantified using a chestband positioned at mid-sternum. Strain gages installed on the ribs and sternum identified fracture timing. Biomechanical response corridors (force-deflection) were generated and compared to scaled small female thoracic corridors using a traditional scaling method (TSM) and rib response-based scaling method (RRSM). A BioRank System Score (BRSS) was used to quantify differences between the small female PMHS data and both scaled corridors.
Results
Coefficients of variation from the three small female PMHS responses were less than 2% for peak force and 7% for peak deflection. Overall, the scaled corridor means determined from the TSM and RRSM were less than two standard deviations away from the mean small female PMHS corridors (BRSS < 2.0). The RRSM resulted in smaller deviation (BRSS = 1.1) from the PMHS corridors than the TSM (BRSS = 1.7), suggesting the RRSM is an appropriate scaling method.
Conclusions
New small female PMHS force-deflection data are provided in this study. Scaled corridors from the TSM, which have been used to optimize current safety tools, were comparable to the small female PMHS corridors. The RRSM, which has the great benefit of using rib structural properties instead of requiring whole PMHS data, resulted in better agreement with the small female PMHS data than the TSM and deserves further investigation to identify scaling factors for other population demographics.
Keywords:
Introduction
Rib fracture mitigation in motor vehicle crashes (MVCs) remains a significant challenge, despite the fact that rib fractures are the most common of thoracic injuries in MVCs (Pattimore et al. Citation1992; Hanna and Hershman, Citation2009; Forman et al. Citation2019). Female drivers have a higher risk of thorax injuries than male drivers in comparable crash conditions based on FARS and NASS-CDS data analysis (Bose et al. Citation2011; Kahane, Citation2013; Parenteau et al. 2013; Ramachandra et al. 2017; Forman et al. Citation2019).
To reduce thoracic injury risk to small females, recent efforts have been made to enhance anthropomorphic test devices (ATDs) and computational human body models (HBMs) (Kimpara et al. Citation2005; Davis et al. Citation2016; Lee et al. 2020). Ideally, large PMHS datasets for small female thoracic impact experiments would be available to generate thoracic biomechanical response corridors in order to improve the biofidelity of ATDs and HBMs. Obtaining such datasets is difficult due to the nature of the PMHS research (e.g., limited availability of subjects). Therefore, scaling methods have been developed to target thoracic responses for small female ATDs and HBMs (Neathery Citation1974; Mertz et al. Citation1989; Kang et al. Citation2019). A thoracic response corridor for the 50th percentile male based on Kroell’s PMHS data (Kroell et al. Citation1971, Citation1974) is typically scaled to approximate the response of the small female. Neathery (Citation1974) used PMHS characteristics, testing inputs, and testing outcomes to determine relationships among these variables and to develop responses for the small female ATD. Mertz et al. (Citation1989) also developed a scaling technique (hereafter called the “traditional scaling method” or “TSM”) for the small female as well as other demographics (e.g., large male). They used a mid-size male thoracic force-deflection corridor generated from Neathery (Citation1974) and a scaling factor from anthropometry of the target small female demographic to create a scaled small female thoracic corridor (Mertz et al. Citation1989). Although this traditional scaling approach has been an accepted basis for designing ATDs and HBMs, some assumptions were necessary when developing the method: a constant density and elastic modulus were applied to derive scaling factors between mid-size males and small females. Recently, a novel scaling method was developed using experimental force-deflection data from a large sample of human ribs that represented a breadth of various demographics (Kang et al. Citation2019). Individual ribs were all tested to failure in a dynamic anterior-posterior bending scenario described in detail in Agnew et al. (Citation2018). Unlike the traditional scaling method, the new rib-based scaling method (hereafter called “rib response-based scaling method” or “RRSM”) applied rib force-deflection data to computing scaling factors from the reference demographic (e.g., mid-size male) to a target demographic (e.g., small female). This approach was introduced in Kang et al (Citation2019), but has not yet been evaluated against small female PMHS thoracic data due to the lack of small female thoracic response data in the literature.
Existing scaling techniques have enhanced small female ATDs and HBMs, but these safety tools may be further improved and validated by using thoracic impact data directly measured from small female PMHS to modify thoracic properties. Given the thoraces of current safety tools (e.g., HIII5th, THOR5th, GHBMC5th, and THUMS AF05) have been developed using traditional scaling factors, assessing the validity of the traditional scaling method is essential to better understand possible limitations of our current ATDs and HBMs. In addition, evaluating the novel rib response-based scaling technique is important since human rib data from various demographics are available to utilize for additional applications (Agnew et al. Citation2018). The main objectives of this study were to (1) generate thoracic biomechanical corridors for small female PMHS and (2) evaluate current scaling techniques by comparing the small female PMHS thoracic response to scaled small female corridors.
Method
Experimental setup
A series of frontal thoracic impacts were conducted on three small female PMHS that were selected to approximate the 5th percentile female anthropometry (). A DXA scan (GE Lunar Prodigy) provided lumbar spine (mean L2-L4) areal bone mineral density (aBMD), although aBMD was not utilized as a selection criterion. The experimental setup for small female thoracic impact tests used here was intentionally consistent with Kroell’s hub impact experimental design (“Kroell’s setup”) (Kroell et al. Citation1974), as shown in . To assess the traditional scaling technique, an impactor mass of 14 kg and an impactor diameter of 15.2 cm were chosen for this study () (Mertz et al. Citation2001). A six-axis load cell (Denton 2944JFL, Humanetics, Plymouth, MI, USA) was installed behind the impactor face () to measure impact forces. An inertial load induced from the mass and acceleration of the impactor face was compensated to calculate applied forces to the PMHS thorax (). An armrest was designed to support the PMHS arms, which replicated Kroell’s setup (). A linear potentiometer (Celesco CLWG-600-MC4, TE Connectivity Co., Berwyn, PA, USA) was attached to the end of the impactor to measure impactor displacement ().
Figure 1. Overall experimental setup (top) and lateral X-ray (bottom) showing instrumentation on an exemplar PMHS. A: a circular impactor (diameter = 15.2 cm); B: six-axis loadcell; C: accelerometer; D: armrest; E: displacement potentiometer; F: chestband.
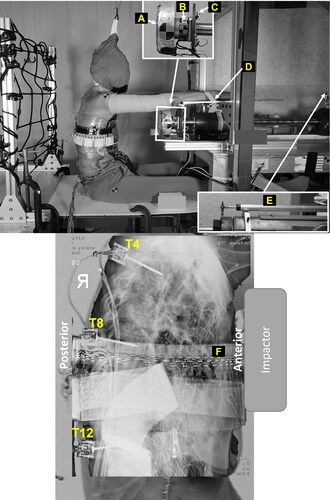
Table 1. PMHS characteristics.
The impactor was aligned to the 4th intercostal space (approximately mid-sternum), consistent with Kroell’s setup, and impacted the PMHS thoraces at a velocity of 4.3 m/s (, see online supplement) (Nahum et al. Citation1970; Neathery Citation1974; Lebarbe and Petit 2012). A 59-channel chestband (Chestband, Humanetics, Plymouth, MI, USA) was installed at the impact location to quantify chest deflection of each PMHS throughout the event (). To maintain coupling of the chestband to the PMHS during the impact, the chestband was stitched to the skin at four locations: anterior, posterior, right lateral, and left lateral. Motion blocks (6DXPRO, Diversified Technical Systems, Seal Beach, CA, USA) comprised of three accelerometers and three angular rate sensors (3aω) were attached at T4, T8, and T12 to quantify spinal displacement during the event (). Strain gages (CEA-13-062UW-350/P2, Micro Measurements, Wendell, NC, USA) were attached at the manubrium, mid-sternal body, and anterior and lateral locations on ribs 3 through 9 (left and right) to quantify strain and identify fracture timing if an injury occurred. Filtering information for all channels is provided in . Since previous scaling techniques did not account for any external soft tissue such as breast tissue, the breasts were removed prior to testing to allow for a direct comparison between skeletal scaling techniques.
Force vs. external- and internal-deflection corridors
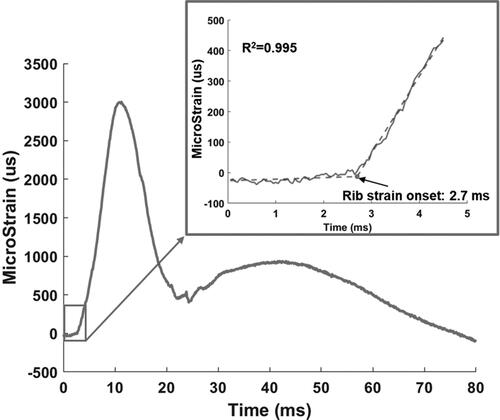
Current small female ATDs and HBMs have been evaluated utilizing both scaled force vs. external-deflection corridors (FEDC) and scaled force vs. internal-deflection corridors (FIDC) (Davis et al. Citation2016; Wang et al. Citation2018; Lee et al. 2020). Therefore, this study generated and compared both FEDC and FIDC of the small female PMHS to scaled corridors. External chest deflections of the PMHS were quantified using the relative difference between impactor displacement and spinal displacement, consistent with previous studies (Kroell et al. Citation1974; Bouquet et al. Citation1994). For the internal chest deflection measure, unlike ATDs, internal deflection sensors (i.e., IRTRACC and linear potentiometer) could not be installed inside the PMHS without damaging the thorax or compromising the closed thoracic cavity which would alter the biomechanical response. Thus, this study used a new methodology using both chestband and strain gage data to calculate PMHS internal chest deflections. shows exemplar strain gage data and rib strain onset timing, determined using a piecewise linear fit (i.e., intersection of two lines). To calculate internal chest deflection, the average strain onset time was first quantified using the strain gage data from the ribs that were directly engaged with the impactor (levels 3-6). Internal chest deflection was assumed to be zero before the onset of rib strain. The ribs experienced no strain despite the impactor contacting the anterior portion of the PMHS chest, due to superficial soft tissue deflection. This soft tissue deflection was subsequently removed to calculate internal chest deflections, again allowing for direct assessment of the thoracic skeleton.
Figure 2. Exemplar strain gage data and determination of rib strain onset time. A piecewise fit (dashed line) was applied to strain data after strain data were truncated at 4.5 ms.
Small female scaling factors
TSM: The small female thoracic force and deflection scaling factors were 0.732 and 0.817, respectively, using the traditional scaling method (TSM) (Mertz et al. Citation2001, Citation2016).
RRSM: To calculate scaling factors using the RRSM, sex and age information for the target and reference demographics must be defined first (Kang et al. Citation2019). The target demographic here was 60- to 90-year-old based on the PMHS age tested in this study (). Mid-size males with ages between 50- to 90-year-old used in Lebarbe and Petit’s study (2012) were the reference demographic for FEDC, while mid-size males with ages from 60- to 90-year-old tested at the low speed in Nahum and colleagues study (Nahum et al. Citation1970; Neathery Citation1974) were the reference demographic for FIDC. The sex and age information for the target and reference demographics were then input into the RRSM algorithm (Kang et al. Citation2019). Given this method solely relied on actual rib force-deflection bony responses, no assumption that females had consistent material properties with the male was made to calculate scaling factors. As RRSM outcomes, force and deflection scaling factors for the small female thorax were 0.628 and 0.997, respectively, for the FEDC, and 0.658 and 1.063, respectively, for the FIDC. The scaling factors from both TSM and RRSM were applied to the mid-size male corridors presented in .
Comparison of scaled corridors to small female PMHS corridors
BioRank System Score (BRSS): To quantify the difference in force-deflection responses between the scaled corridors and those from the small female PMHS tests, BRSS was calculated (Kang et al. Citation2021). BRSS in this application evaluates deviations between two corridors and a lower BRSS indicates better agreement between the two corridors. For instance, a BRSS of 1 implies the mean curve of each corridor is one standard deviation from the other. An exemplar BRSS calculation is provided in for reference.
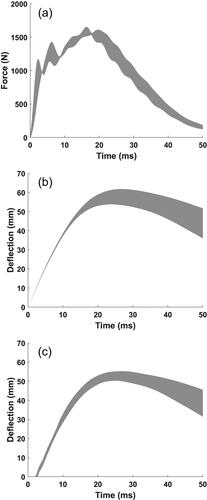
Figure 3. Corridors (n = 3 PMHS) of time histories for (a) force, (b) external deflection, and (c) internal deflection.
Corridor generation: The small female response corridors were generated using a two-dimensional (force and deflection) standard deviation method (Shaw et al. Citation2006).
Injury information
Following each PMHS test, a detailed whole-body dissection was performed to document injury outcomes. The Abbreviated Injury Scale (AIS) (AAAM 2015) was utilized by a Certified AIS Specialist (CAISS) to classify all thoracic injuries.
Results
Response corridors
Time history biomechanical response corridors (mean ± one standard deviation) for compensated force, external deflection, and internal deflection were generated and are provided in , respectively, while individual PMHS responses can be found in . shows peak force and deflection values measured from each PMHS as well as means, and standard deviations.
Table 2. Summary of PMHS injuries.
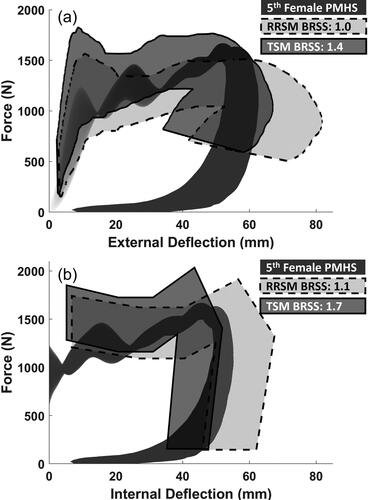
Force-deflection corridors for the small female PMHS and both scaled corridors (i.e., TSM and RRSM corridors) were plotted for comparison (). Individual force-deflection responses for each PMHS are shown in . Qualitatively and quantitatively, both scaled corridors were consistent with the small female PMHS corridors with BRSS < 2, although the RRSM scaled corridors had better (i.e., lower) BRSS values than the TSM scaled corridors (). For FEDC, time-deflection and time-force corridors for the small female PMHS and the scaled female corridors are provided in . For FIDC, time history data for scaled corridors were unavailable, so BRSS was calculated only in the force-deflection domain.
Figure 4. Comparison of the small female PMHS corridor (black) with TSM (solid line) and RRSM (dashed line) scaled corridors for (a) FEDC and (b) FIDC.
Injuries
All PMHS sustained rib and sternum fractures (). PMHS1 had AIS3 due to ≥ 3 rib fractures, while the other PMHS had fewer rib fractures but along with sternum fractures resulted in AIS2. Specific fracture locations per PMHS are provided in .
Discussion
This study focused on (1) generating small female skeletal-based thoracic biomechanical corridors in a frontal impact hub condition and (2) assessing the validity of TSM and RRSM. The TSM scaled corridors (i.e., TSM) resulted in BRSS < 2.0, which was somewhat consistent with the small female PMHS corridors generated in this study (). The RRSM scaled corridors for small females (60–90 year-old) exhibited lower BRSS than the TSM, indicating that the RRSM is an improved and alternative scaling method for small females (). The RRSM database includes rib force-deflection data from all ages, sexes, and body sizes, which can be utilized for scaling to other populations as well (e.g., pediatric).
Female thoracic responses
A large dataset of PMHS thoracic biomechanical responses in frontal hub impacts was generated from the GM research group in the 1970s (Kroell data) (Nahum et al. Citation1970; Kroell et al. Citation1971, Citation1974). A total of 47 PMHS (37 male; 10 female) were tested at various impact energies using different impactor masses and speeds. summarizes the female data from Kroell’s and the current study. The table includes PMHS age, size, impact conditions, results, and injury outcomes. One small female PMHS (30FF) test was excluded due to different impact conditions (1.6 kg impactor mass and 13.2 m/s impact speed - see Kroell et al. Citation1974 for more details). None of the input conditions (e.g., impactor mass, speed, and energy) applied to Kroell‘s female PMHS were identical to the inputs in the current study (). The closest impact condition from Kroell’s female PMHS data was from 7FF with an impactor mass of 19.5 kg, speed of 4.0 m/s, and energy of 157.9 J (Nahum et al. Citation1970). The peak force (1584 N) and deflection (64.0 mm) measured from 7FF were comparable to the current study (1594 − 1649 N and 53.5 − 61.2 mm). Since input parameters (impact mass and speed) varied between Kroell’s and the current study, correlation analyses between those and output variables (force and deflection) were conducted with and without combining PMHS data from the current study with Kroell’s data, to explore if combining PMHS data affected statistical outcomes. Both impactor speed vs. force and energy vs. deflection resulted in Pearson correlation (R) values > 0.9 (p < 0.001) with peak force and deflection shown in . Combining the PMHS data did not affect the correlations for the comparisons of impactor speed vs. force and energy vs. deflection. However, impactor speed vs. deflection and impact energy vs. force became significant (p-values of 0.002 and 0.039, respectively) after combining data, indicating that the PMHS data from the current study are a valuable complement to Kroell’s data for highlighting the significant influence of input parameters on output variables (). However, caution should be made with the results given that breasts were removed in this study as opposed to the intact female PMHS tested in the Kroell studies. Additional female data from tests at various input energy levels are required to confirm this linear relationship between the input and output variables. The information should help refine female scaling factors accounting for different impact energies.
Scaling methods
Due to limited female biomechanical data in the literature, mid-size male to small female scaling approaches contributed to the design and tuning of current female ATDs and HBMs (McDonald et al. Citation2003; Davis et al. Citation2016; Wang et al. Citation2018). The TSM assumed material properties (e.g., Young’s moduli and density) to be the same between mid-size males and small females, and as a result, global geometric properties (e.g., chest depth and height) had to be used to calculate stiffness scaling factors. This material property assumption is supported by experimental studies that found no sex differences in rib material properties (Kimpara et al. Citation2003; Katzenberger et al. Citation2020). However, sex differences in structural properties have been identified in rib anterior-posterior (i.e., frontal) tests and a three-point bending scenario (Kimpara et al. Citation2003; Agnew et al. Citation2018; Kang et al. Citation2021), which were not accounted for in the TSM. In contrast, the RRSM did not require assumptions about sex differences in rib properties but directly incorporated experimental rib force-deflection data to create the scaling factors. Consequently, scaled thoracic corridors determined from the RRSM were more consistent (i.e., lower BRSS) with the small female PMHS data than TSM. The RRSM also accounted for “age” as an input parameter in the algorithm, another notable benefit to the method. Many researchers have found that rib fracture risk increases with age (Neathery, Citation1974; Zhou et al. Citation1996; Kent and Patrie, Citation2005), and ribs and thoraces of younger individuals absorb more energy and result in larger force and deflection scaling factors than older individuals (Zhou et al. Citation1996; Malthese et al. 2010; Mertz et al. Citation2016; Agnew et al. Citation2018; Kang et al. Citation2019). Due to effects of aging on ribs and thoracic responses, it is essential to include an age term to improve scaling methods. Therefore, the RRSM is a valid methodology for small females and should be further explored to improve scaling factors for other populations, including pediatrics.
Injuries
The youngest PMHS utilized in this study (PMHS1) also had the highest aBMD t-score (-0.2), which is considered in the normal range. This PMHS also experienced the highest MAIS (3) and the greatest number of skeletal injuries. On the contrary, the subject (PMHS3) with the lowest aBMD t-score (-2.8), which is considered osteoporotic, sustained the fewest fractures despite all impacts being almost identical (see ). While the sample size in this study is too small to establish any definitive conclusions, these contradictions suggest the injury biomechanics community should explore more robust predictors of thoracic injuries than simply age and aBMD and caution should be used when making assumptions about the role of these factors in determining vulnerability to injury.
Thoracic response corridors normalized to mid-size males have been generated at two different speeds (4.3 m/s and 6.7 m/s) (Neathery Citation1974; Lebarbe and Petit 2012). In the current study, the impactor speed of 4.3 m/s was selected to avoid catastrophic damage to the small female thorax, which might also affect force-deflection responses. Consequently, the PMHS tested in the current study sustained fewer rib fractures (≤ 4) than Kroell’s female PMHS (ranged from 7 - 23 in ) (Kroell et al. Citation1971, Citation1974). However, female occupants tend to be at greater risk of rib fractures than males (Carroll et al. Citation2010; Bose et al. Citation2011; Parenteau et al. 2013; Forman et al. Citation2019). To explore differences in rib fracture risk between sexes, both female and male PMHS should be tested in identical conditions. Unfortunately, no male PMHS were tested in the same conditions as this study in the literature. It may be prudent to conduct similar size male PMHS tests to investigate differences in injury outcomes between sexes.
Limitations
Only three small female PMHS were tested in this study. However, the variations in force-deflection responses were minimal and resulted in coefficients of variation (CV) of 1.7%, 6.8%, and 4.9% for force, external deflection, and internal deflection, respectively (, see online supplement). For this reason, a normalization technique was not applied to generate corridors. The three PMHS utilized in this study were elderly (67-89 years), so further investigation should be employed on a larger sample size and consider other sources of biological variability as well (e.g., young adults, larger females, etc.).
The internal deflection was calculated under the assumption there was no additional soft tissue compression after the onset of the rib strain, which may be valid given the force-deflection shape exhibited a plateau and the internal deflection was smaller than the external deflection. However, soft tissue compression should be investigated to check the validity of the proposed internal deflection method.
Given that none of the previous scaling techniques accounted for the influence of breast tissue on the scaled thoracic response corridors, this study similarly focused on skeletal-specific scaling methods and responses. However, Kroell et al. (Citation1971) noted the most extreme example of interface effects (defined as compressibility of superficial tissues and deviation from a square impact) was one female PMHS with relatively larger breasts and more subcutaneous tissue. A large chest deflection (119.4 mm) was observed in this PMHS (21FF in ), which influenced the resulting force-deflection curve shape. Even in the current study, the external deflection CV (6.8%) was larger than that for the internal deflection (4.9%), see , indicating soft tissues likely have a strong influence on external deflection measures. Therefore, it would likely have been difficult to minimize variations from the breasts and evaluate current scaling techniques against small female PMHS if breast tissue was included in the study. Lebarbe et al. (2005) investigated thoracic injuries and rib fractures in frontal airbag deployment using both male and female PMHS. They also removed the breasts of female PMHS to minimize variation from the breast tissue. This study provided baseline data for direct comparison to previous data for skeletal response. A logical next step will be to replicate such experiments with breasts intact to isolate their effects. Breasts are an essential component of the female torso and the influence of different volumes, thicknesses, and positioning of breast tissue should be thoroughly investigated in future work to enhance efforts to understand realistic response and injury differences in females.
To replicate the mid-size male Kroell setup, a hub impactor, designed for simulating an unbelted occupant with a steering wheel impact, was used in this study. The hub impact condition is beneficial to maximize the reproducibility of a physical and virtual environment for ATD and HBM evaluation. However, different loading conditions affect PMHS thoracic responses. Kent et al. (Citation2004) found that hub loading produced lower effective thoracic stiffness than belt and distributed loading conditions (Kent et al. Citation2004). In real-world vehicle crashes, direct thorax-to-steering wheel interactions are unlikely with proper belt use and airbag deployments. Therefore, small female PMHS responses in more realistic seat belt and airbag loading conditions should be explored in future work. Moreover, the interaction between restraint systems and female thoraces in frontal crashes may vary from the male due to anthropometry (e.g., seated height) and anatomical (e.g., breast tissue) differences. Additionally, small female drivers are often positioned close to the steering wheel; therefore, they may be at higher risk of injuries due to frontal airbag deployment, which should be further investigated. Nonetheless, this study provides valuable primary small female PMHS data which are rare in the literature.
Supplemental Material
Download Zip (1.3 MB)Acknowledgments
We would like to deeply thank the anatomical donors. Without these selfless gifts, it would not be possible to conduct this research. This study would not have been possible without the contributions of students, staff, and faculty in the Injury Biomechanics Research Center.
Additional information
Funding
References cited
- Abbreviated Injury Scale – 2015 Revision. 2015. Association for the advancement of automotive medicine. Des Plaines (IL): Abbreviated Injury Scale – 2015 Revision.
- Agnew AM, Murach MM, Dominguez Vm A, Sreedhar E, Misicka A, Harden J, Bolte K, Moorhouse J, Stammen Y, Kang 1. 2018. Sources of variability in structural bending response of pediatric and adult human ribs in dynamic frontal impacts. Stapp Car Crash J. 62:119–192. PMID: 30608995.
- Bose D, Segui-Gomez M, Crandall JR. 2011. Vulnerability of female drivers involved in motor vehicle crashes: an analysis of US population at risk. Am J Public Health. 101(12):2368–2373. doi: 10.2105/AJPH.2011.300275. PMID: 22021321.
- Bouquet R, Ramet M, Bermond F, Cesari D. 1994. Thoracic and pelvis human response to impact. Paper presented at: 14th International Technical Conference on the Enhanced Safety of Vehicles (ESV), Munich, Germany; May 23–26.
- Carroll J, Adolph T, Chauvel C, Labrousse M, Trosseille X, Pastor C, Eggers A, Smith S, Hynd D. 2010. Overview of serious thorax injuries in European frontal car crash accidents and implications for crash test dummy development. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI), Hanover, Germany; September 15–16.
- Davis M, Koya B, Schap J, Gayzik F. 2016. Development and full body validation of a 5th percentile female finite element model. Stapp Car Crash J. 60:509–544. PMID: 27871105.
- Forman J, Poplin GS, Shaw CG, McMurry TL, Schmidt K, Ash J, Sunnevang C. 2019. Automobile injury trends in the contemporary fleet: Belted occupants in frontal collisions. Traffic Inj Prev. 20(6):607–612. doi: 10.1080/15389588.2019.1630825. PMID: 31283362.
- Hanna R, Hershman L. 2009. Evaluation of thoracic injuries among older motor vehicle occupants. Washington (DC): National Highway Traffic Safety Administration.
- Kahane CJ. 2013. Injury vulnerability and effectiveness of occupant protection technologies for older occupants and women. Washington (DC): National Highway Traffic Safety Administration.
- Kang YS, Bolte JH, Stammen J, Moorhouse K, Agnew AM. 2019. A novel approach to scaling age-, sex-, and body size-dependent thoracic responses using structural properties of human ribs. Stapp Car Crash J. 63:307–329. PMID: 32311062.
- Kang YS, Kwon HJ, Stammen J, Moorhouse K, Agnew AM. 2021. Biomechanical response targets of adult human ribs in frontal impacts. Ann Biomed Eng. 49(2):900–911. doi: 10.1007/s10439-020-02613-x. PMID: 32989590.
- Katzenberger MJ, Albert DL, Agnew AM, Kemper AR. 2020. Effects of sex, age, and two loading rates on the tensile material properties of human rib cortical bone. J Mech Behav Biomed Mater. 102:103410. doi: 10.1016/j.jmbbm.2019.103410. PMID: 31655338
- Kent R, Lessley D, Sherwood C. 2004. Thoracic response to dynamic, non-impact loading from a hub, distributed belt, diagonal belt, and double diagonal belts. Stapp Car Crash J. 48:495–519. PMID17230280.
- Kent R, Patrie J. 2005. Chest deflection tolerance to blunt anterior loading is sensitive to age but not load distribution. Forens Sci. Int. 149(2-3):121–128. doi: 10.1016/j.forsciint.2004.04.086. PMID: 15749351.
- Kimpara H, Iwamoto M, Miki K, Lee JB, Begeman PC, Yang KH, King AI. 2003. Biomechanical properties of the male and female chest subjected to frontal and lateral impacts. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI); Lisbon, Portugal; September 25–26.
- Kimpara H, Lee JB, Yang KH, King AI. 2005. Development of a three-dimensional finite element chest model for the 5th percentile female. Stapp Car Crash J. 49:251–269. PMID: 17096277.
- Kroell C, Schneider D, Nahum A. 1971. Impact tolerance and response of the human thorax. SAE Technical Paper. doi: 10.4271/710851.
- Kroell C, Schneider D, Nahum A. 1974. Impact tolerance of the human thorax II. SAE Technical Paper. doi: 10.4271/741187.
- Lebarbé M, Petit P. 2012. New biofidelity targets for the thorax of a 50th percentile adult male in frontal impact. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI), Dublin, Ireland; September 12–14.
- Lebarbé M, Potier P, Baudrit P, Petit P, Trosseille X, Vallancien G. 2005. Thoracic injury investigation using PMHS in frontal airbag out-of-position situations. Stapp Car Crash J. 49:323–342. PMID17096280.
- Lee EL, Parent D, Craig M, McFadden J, Moorhouse K. Biomechanical response manual: THOR 5th percentile female NHTSA advanced frontal dummy, Revision 2. Washington (DC): National Highway Traffic Safety Administration. Report DOT HS 812 811.
- Maltese MR, Arbogast KB, Nadkarni V, Berg R, Balasubramanian S, Seacrist T, Kent RW, Parent DP, Craig M, Ridella SA. 2010. Incorporation of CPR data into ATD chest impact response requirements. Paper presented at Annals of Advances in Automotive Medicine/Annual Scientific Conference. Association for the Advancement of Automotive Medicine. PMID: 21050593.
- McDonald JP, Shams T, Rangarajan N, Beach D, Huang T-J, Freemire J, Artis M, Wang Y, Haffner M. 2003. Design and development of a THOR based small female crash test dummy. Stapp Car Crash J. 47:551–570. PMID17096264.
- Mertz HJ, Irwin AL, Melvin JW, Stanaker RL, Beebe M. 1989. Size, weight and biomechanical impact response requirements for adult size small female and large male dummies. SAE Technical Paper. doi: 10.4271/890756.
- Mertz HJ, Irwin AL, Prasad P. 2016. Biomechanical and scaling basis for frontal and side impact injury assessment reference values. Stapp Car Crash J. 60:625–657. PMID27871108.
- Mertz HJ, Jarrett K, Moss S, Salloum M, Zhao Y. 2001. The hybrid III 10-year-old dummy. Stapp Car Crash J. 45:319–328. PMID17458751.
- Neathery RF. 1974. Analysis of chest impact response data and scaled performance recommendations. SAE Technical Paper. doi: 10.4271/741188.
- Nahum AM, Gadd CW, Schneider DC, Kroell CK. 1970. Deflection of the human thorax under sternal impact. SAE Technical Paper. doi: 10.4271/700400.
- Parenteau CS, Zuby D, Brolin K, Svensson My Palmertz, C, Wang Sc. 2013. Restrained male and female occupants in frontal crashes: are we different?. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI), Gothenburg, Sweden; September 11–13.
- Pattimore D, Thomas P, Dave SH. 1992. Torso injury patterns and mechanisms in car crashes: an additional diagnostic tool. Injury. 23(2):123–126. doi: 10.1016/0020-1383(92)90047-v. PMID: 1572708.
- Ramachandran R, Kashikar T, Bolte J. 2017. Injury patterns of elderly occupants involved in side crashes. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI), Antwerp, Belgium; September 13–15.
- Shaw JM, Herriott RG, McFadden JD, Donnelly BR, Bolte JH. IV 2006. Oblique and lateral impact response of the PMHS thorax. Stapp Car Crash J. 50:147–167. PMID17311163.
- Wang ZJ, Lee E, Bolte J, Below J, Loeber B, Ramachandra R, Greenlees B, Guck D. 2018. Biofidelity evaluation of THOR 5th percentile female ATD. Paper presented at: International Research Council on Biomechanics of Injury (IRCOBI), Athens, Greece; September 12–14.
- Zhou Q, Rouhana SW, Melvin JW. 1996. Age effects on thoracic injury tolerance. SAE Technical Paper. doi: 10.4271/962421.