
Abstract
Objective
Two wheel motorized vehicles used in both street transportation and recreation are a common cause of severe injury in the United States (US). To date, there has been limited data describing the spinal injury patterns among these motorcycle injury patients in the US. The goal of this study is to characterize and compare differences in specific injury patterns of patients sustaining traumatic spinal injuries after motocross (off-road) and street bike (on-road) collisions in the southwestern US at a Level I Trauma Center.
Methods
Trauma registry data was queried for patients sustaining a spinal injury after motorcycle collision from 2010 to 2019 at a single Level I Trauma Center. Computed tomography (CT) scan and magnetic imaging resonance imaging (MRI) reports from initial trauma evaluation were reviewed and data was manually obtained regarding injury morphology and location.
Results
A total of 1798 injuries were identified in 549 patients who sustained a motorcycle collision, specifically 67 off-road and 482 on-road motorcycle patients. Off-road motorcycle patients were found to be significantly younger (34.75 vs. 42.66, p = 0.00015). A total of 46.2% of the off-road injuries were determined to be from compression mechanisms, compared to 32.9% in the on-road cohort (p = 0.0027). The on-road cohort was more likely to have an injury classified as insignificant, such as transverse and spinous process fractures (60.1% vs. 42.5%, p = 00.25). There was no significant difference in regards to junctional, mobile, and semirigid spine segments between the two cohorts.
Conclusions
Different fracture patterns were seen between the off-road and on-road motorcycle cohorts. Off road motorcyclists experienced significantly more compression and translational injuries, while on road motorcyclists experienced more frequent insignificant injury patterns. Data on the different fracture patterns may help professionals develop safety equipment for motorcyclists.
Keywords:
Introduction
Background/rationale
Two wheel motorized vehicle related injuries are a common cause of traumatic spine injury in the United States (US). Off-road motorcycles (dirt bikes/motocross) are predominantly used in a recreational setting with crashes being either solo or while racing similar vehicles (Singh et al. Citation2018). Injuries sustained from off-road motorcycle use are typically related to riding terrain and obstacles such as jumps, rocks, heights, and collision with other motorcyclists. Off-road motorcycles have a higher potential for vertical falls and an axial load mechanism for spinal injury than on-road counterparts. On-road motorcycles (street bikes) are primarily used as transportation with crashes most often occurring on streets at higher speeds with road hazards and larger vehicle traffic. Higher kinetic energy and immobile hazards lead to more frequent translational-type crash mechanisms where the moving rider is abruptly stopped by objects such as other vehicles, road signs, light posts, guardrails, etc. This is in contrast to off-road riders that often sustain a fall from an elevated height to the ground. On-road injury mechanisms are known to contribute to more severe systemic injuries and higher fatality rates, although spinal injury patterns have not been well-described (Ashie et al. Citation2018; Chaudhuri et al. Citation2019).
There were 109,000 reported motorcycle crashes in the US in 2018 with 79,000 injured motorcyclists as reported by the National Center for Statistics and Analysis (Citation2020) through police reports and registered motorcycle data. An estimated 51,415 Emergency Room (ER) injuries occurred in 2018 due to off-road motorcycles from a National Electronic Injury Surveillance System-All Injury Program (NEISS-AIP) query search (National Electronic Injury Surveillance System Citation2022). A previous retrospective database study observing injury patterns in off-road and on-road motorcycle collisions found that 21.4% of on-road and 18.9% of off-road motorcycle patients sustained an associated spine injury (Fierro et al. Citation2019). In a United Kingdom (UK) study on off-road motorcycle spine injuries, the most common spinal injuries were thoracolumbar burst fractures and chance fractures (Singh et al. Citation2018). In the same study, up to 54% of injuries required operative management (Singh et al. Citation2018). In a similar study, the thoracic spine was found to have the highest incidence of injury at 54.8% for on-road motorcycle crashes in the UK (Robertson et al. Citation2002).
There is a high prevalence of both on and off-road motorcycle riding in the southwestern U.S. with unique recreational modalities such as motocross and desert racing (Grant and Whipp Citation1976; Kraus et al. Citation1995; Burns et al. Citation2015). There has been no inquiry comparing spinal injury patterns between on and off-road motorcycle trauma in the United States, to the best of our knowledge. The effectiveness of back and neck protectors in both on and off-road motorcycle injuries is ambiguous, with limited data and no significant correlation to reduced injury rate shown (Ekmejian et al. Citation2016; Afquir et al. Citation2020). In-depth analysis of specific spine injuries could provide data to guide future improvement in safety via protective equipment advances and EMS response.
Objectives
This is a retrospective cohort study at a community-based Level I Trauma Center in the southwest US with the goal of providing insight to the distribution and severity of on and off-road motorcycle spinal injuries over the past decade. Our hypothesis is that on and off-road motorcycle injuries will have different fracture patterns. Specifically, we believe off-road motorcycles will have a greater rate of compression-type spinal injuries secondary to the higher risk of axial load. This would likely be due to the existence of jumps in the motocross sport, as well as vertical hazards in trail riding compared to on-road crash mechanisms. Given compression-type spinal injuries most commonly occur in the mid-thoracic and thoracolumbar regions, we believe that there will be more injuries of the mid-thoracic and thoracolumbar regions for off-road motorcycles than on-road (Cooper et al. Citation1992; Ensrud and Schousboe Citation2011). We also predict that on-road motorcycles will have a higher rate of flexion/extension with distraction injuries from collisions with automobiles and immobile hazards, as well as the higher energy involved due to increased speeds. Given flexion/extension with distraction injuries most commonly occur in the cervical spine, we believe on-road motorcycle injuries will have more cervical spine involvement than off-road (Harris et al. Citation1986).
Methods
The study is a retrospective cohort chart review using Level I Trauma Center Registry data from 2010 to 2019 at a single institution, tertiary referral hospital in the southwest United States. Trauma Registry data was used to retrospectively evaluate spinal injuries from patients from 2010 to 2019. The Trauma Registry database was queried for patients sustaining spine injuries after an on or off-road motorcycle collision based on ICD-9/ICD-10 codes from the Crosswalk of Common Spine ICD-9-CM Codes to ICD-10 Codes (Citation2015) resulting in 1035 patients. Specific ICD-9/ICD-10 Injury Codes can be seen in Table A1 (see online supplement). Motorcycle passengers were excluded from the population yielding 989 total patients. On and off-road motorcycle cohorts (On-road: 908/Off-road: 81) were then constructed based on the appropriate mechanism ICD E-code. Further exclusion criteria were applied; dead on arrival, chronic spinal injury, lack of spine imaging. All consecutive patients who arrived with a documented motorcycle collision and who sustained an acute bony spinal injury as diagnosed on CT scan or MRI were included (On-road: 482/Off-road: 67). The patient flowchart can be seen in . CT scan is the gold standard initial imaging modality for suspected spine injury and the preferred study to diagnose fracture/bony pathology. MRI is typically used as a secondary imaging modality to further evaluate soft and connective tissue spinal injury in the acute trauma setting and is not routinely utilized for every trauma patient.
Figure 1. Flowchart of patients that were selected based on exclusion criteria and then separated into respective cohorts based on ICD codes. These patients were then analyzed for spinal injuries. (ICD: International Classification of Diseases).
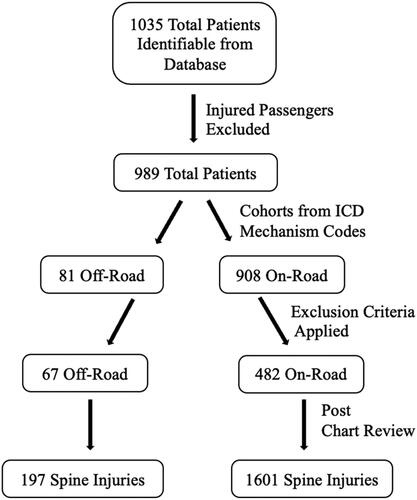
Table 1. Demographics.
Once participants were identified, the medical record/imaging was reviewed and spine injury data was recorded. The clinical history and injury mechanism was then reviewed to identify whether the patient was using an on-road or off-road motorcycle. The data was obtained from initial trauma evaluation only, and no follow-up or long term clinical data was collected. Specific injury, vertebral level, and morphologies were then documented based on findings from advanced imaging which included CT scans or MRI depending on availability. Injuries were then grouped into vertebral segments based on the location category of the Spine Instability Neoplastic Score (SINS) classification; a widely accepted scoring system used for neoplasm in spine literature (Fisher et al. Citation2010; Arana et al. Citation2016). Specific vertebrae were grouped together into junctional (Occiput-C2, C6-T2, T11-L1, and L5-S1), mobile spine (C3-6 and L2-4), and semirigid (T3-T10). Additionally, the injury morphologies were further grouped by mechanism based on the AO Spine Injury Classification System (Vaccaro et al. Citation2013; Kepler et al. Citation2016). The AO classification system distinguishes injuries by compression, distraction, translation, C1 ring and C1-2 joint, and insignificant injuries. Refer to Table A2 (see online supplement) for the injury morphologies that belong to the different mechanisms based on the AO Spine Injury Classification System. Injuries were identified from CT scan and MRI radiographic reports provided by board certified radiologists. Student’s T-test in Microsoft Excel(™) and Two tail Z-test in Microsoft Excel(™), were used to identify statistically significant differences in quantitative variables among the two cohorts. P-values <0.05 were deemed clinically significant. Chi square in Microsoft Excel(™) test was used to evaluate categorical variables.
Table 2. SINS classification grouped vertebrae off-road and on-road motorcycles.
Results
A total of 989 patients were identified via ICD code Trauma Registry query. There were a total of 81 off-road motorcycle patients, of whom 67 (82.7%) sustained spinal injuries, compared to a total of 908 on-road motorcycle patients, of whom 482 (53.4%) sustained spinal injuries. A total of 549 patients between the two cohorts were identified to have sustained spinal injuries and were eligible for inclusion in the study. Patient demographics are listed in .
There was a high male dominance among both injury cohorts; 1 of 67 (1.5%) were female in the off-road motorcycle cohort, and 38 of 482 (7.8%) were female in the on-road motorcycle cohort (p = 0.056). The average age of the off and on-road motorcycle cohorts were 34.75 years and 42.66 years, respectively. This was found to be a statistically significant difference (p < 0.001).
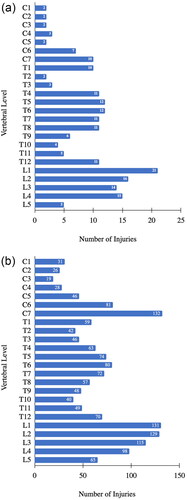
There were a total of 197 spine injuries identified among off-road motorcycle patients. Of these injuries, 28 (14.2%) were located in the cervical spine, 98 (49.8%) in the thoracic spine, and 71 (36.0%) in the lumbar spine. A total of 1601 spine injuries were identified among on-road motorcycle patients, which included 363 (22.7%) cervical, 700 (43.7%) thoracic, and 538 (33.6%) lumbar. The thoracic spine was the most common injured segment in both cohorts. Specific vertebral levels of injury are shown in and .
Figure 2. (a) Off-road motorcycle injury by individual vertebrae. (b) On-road motorcycle injury by individual vertebrae. Number of injuries that occurred on each vertebral level in the off-road motorcycle cohort. (C: Cervical, T: Thoracic, L: Lumbar).
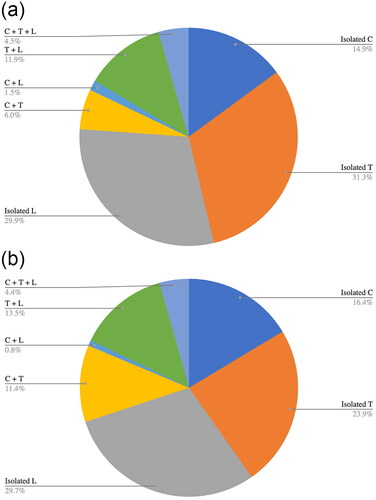
In the on-road motorcycle cohort, 337 of 482 patients (69.9%) had injuries isolated to one vertebral segment. In the off-road motorcycle cohort, 51 of 67 patients (76.1%) had injuries isolated to one vertebral segment. The distribution of injury among spinal segments is demonstrated in and . On-road motorcycle patients were more likely to have multiple spinal injuries when compared to the off-road motorcycle cohort, although not statistically significant. There were a total of 197 injuries in 67 patients (2.94 injuries per patient), compared to 1601 injuries in 482 patients (3.32 injuries per patient), in the off and on-road motorcycle groups, respectively (p = 0.103).
Figure 3. (a) Off-road motorcycle injury by vertebral segment. (b) On-road motorcycle injury by vertebral segment. Percentage of injuries that occurred in each vertebral segment as well as combined vertebral segments in the off-road motorcycle cohort. (C: Cervical, T: Thoracic, L: Lumbar).
Vertebrae were also categorized based on spinal characteristics used in the SINS classification system, such as junctional, mobile spine, and semirigid sections. Junctional vertebral levels accounted for 34.5% and 37.8% of off and on-road motorcycle injuries, respectively (p = 0.479). Mobile spine sections comprised 29.9% off-road and 32.3% on-road injuries (p = 0.593). Semi-rigid spine segments comprised 35.6% off-road and 30.0% on-road injuries (p = 0.184). Additional SINS sub-section analysis of the individual grouped segments showed no statistically significant difference. The data for the different groupings based on their characteristics and specific vertebrae can be seen in .
Specific injury morphologies for each cohort are listed in Tables A3 and A4 (see online supplement). The most common injury type in both off and on-road motorcycle cohorts were transverse process fractures and compression fractures. Injury morphologies were further grouped by mechanism based on the AO Spine Injury Classification system, which can be seen in . A total of 46.2% of the off-road injuries were determined to be from compression mechanisms, compared to 32.9% in the on-road cohort (p = 0.0027). A total of 42.6% of the off-road cohort injuries were classified as insignificant, as compared to 60.1% of the on-road cohort (p = 0.0025). A total of 6.6% of the off-road cohort injuries were classified as translational, as compared to 4.8% of the on-road cohort (p < 0.001).
Table 3. AO classification injury mechanism off-road and on-road motorcycles.
Discussion
Previous literature has shown that patients sustaining traumatic injuries due to off-road motorcycle collisions are frequently in a younger age demographic. This is thought to be secondary to children and adolescents making up a larger portion of the off-road motorcycle community. A previous study found that 38% of off-road motorcycle-related injuries at a southern California Level I Trauma Center were less than 20 years old (Singh et al. Citation2018). The current study supports this data as the average age at spinal injury for off-road motorcyclists was found to be approximately 35, compared to 43 in the on-road group.
Males are more commonly riders of both on and off-road motorcycles. In one study, male riders were found to comprise over 90% of fatal motorcycle crashes from 2000 to 2016 in the US (Chaudhuri et al. Citation2019). Our study also demonstrates a significant male predominance for both off-road and on-road motorcycle collisions as reported in the previous literature. Only 1.5% of our patients were female in the off-road cohort, and 7.8% in the on-road cohort. Despite the increased number of female on-road patients, there was found to be no statistically significant injury trends among female riders. Lack of statistical significance is likely secondary to the single institution population size evaluated and would become significant if applied to a larger sample.
The thoracic spine was found to be the most common segment injured in both off and on-road motorcycle cohorts. Although the thoracic spine was the most commonly injured segment, the single vertebral level with the most injuries in the on-road cohort was C7, followed closely by L1 and L2. In the off-road cohort, L1 was the most commonly injured vertebrae. This is thought to be secondary to the high amount of stress which is seen at the thoracolumbar junction during axial loading. An example of this in the off-road cohort would be landing from a jump, applying force parallel to the long axis of the spine.
There was a higher incidence of multi-segment spinal injury in the on-road cohort (30.1%) compared to the off-road cohort (23.9%). In addition, on-road patients were more likely to have multiple spine injuries (197 injuries in 67 patients (2.94) vs. 1601 injuries in 482 patients (3.32)) although not found to be statistically significant in this sample.
The most common injury morphology was found to be transverse process fractures. This injury was not recorded in previous literature. Although this was the most common injury pattern, it is generally considered a low acuity injury that has good outcomes with conservative management. The second most predominant injury morphology was compression fractures, most commonly located in the thoracic spine. This high incidence of thoracolumbar compression fractures is consistent with previous findings (Singh et al. Citation2018).
Analysis using the SINS vertebral grouping system showed no significant difference in injury rates of the junctional, mobile, and semirigid spinal segments between the two cohorts. The junctional vertebrae injuries are considered to be more unstable from a biomechanical and neurological standpoint (Fisher et al. Citation2010; Wood et al. Citation2014; Arana et al. Citation2016). Injuries to these transitional vertebrae groups are theoretically more common in higher energy collisions. Further subsectional analysis of SINS classification groupings showed no significant difference in injury rates, and can be found in . The T3-10 segment was the most involved, followed closely by the L2-4 segment in both cohorts. Though it was hypothesized that the off-road cohort would have a greater proportion of thoracic involvement and the on-road cohort would have more cervical involvement, this was not statistically significant in the study.
Further grouping the injury morphologies by mechanism utilizing the AO Spine Injury Classification, there were statistically significant differences between the off-road and on-road cohorts (Vaccaro et al. Citation2013; Kepler et al. Citation2016). Specifically, the off-road motorcycle group had a greater proportion, 46.2%, of compression mechanism injuries compared to the on-road group, 32.9%, which was statistically significant. This is consistent with our hypothesis and could be due to the higher amount of axial loading with off-road motorcycle injury profiles as described above. The off-road motorcycle cohort also had a greater proportion of translational injuries than the on-road cohort, which was also statistically significant but not consistent with our hypothesis. The mix of horizontal and vertical falls from the off-road cohort could explain the rejection of our hypothesis in regards to the off-road motorcycle cohort having greater translational mechanism injuries. Our analysis also found a statistically significant increase in spinal injuries classified as insignificant in the on-road motorcycle cohort (60.1%), as compared to the off-road cohort (42.6%). This may be secondary to on-road motorcyclists having more frequent presentations to the emergency department and thorough evaluation after traffic incidents, as compared to off-road motorcyclists presenting only for more severe injuries. There was no significant difference in distraction, C1 ring, or C1-C2 injuries between the two cohorts.
Strengths of the current study include being performed at a Level I Trauma Center with a wide catch radius. The study was performed in a diverse region of the US and may be widely generalizable to the overall population. It may also be more generalizable to the United States given differences in traffic laws compared to previous studies in the UK.
The primary limitation of this study is that it is an observational study and does not assess clinical outcomes regarding injuries or treatments after injuries were sustained. Selection bias is low even though this is a retrospective study as every patient with a motorcycle collision was included. Further information could be gleaned with a prospective study, including use of protective equipment in off-road motorcycle use. There is evidence that protective equipment can reduce overall injury severity in motorcycle trauma patients, however there is questionable benefit in regards to fracture (de Rome et al. Citation2011; Wu et al. Citation2019). Further investigation is needed to determine if there is any benefit to spinal injuries using protective equipment. Richness of data, and depth of understanding would be enhanced by a prospective study that included follow-up, ASIA scores, and patient reported outcome measures.
In summary, this study found that both off and on-road motorcycle spine injury patients tend to be male, while off-road injury patients tend to be of younger age. Different fracture patterns were seen between the off-road and on-road motorcycle cohorts, which could be due to their different injury profiles. Off-road motorcyclists experienced significantly more compression and translational injuries, while on-road motorcyclists experienced more frequent insignificant injury patterns. There was no significant variation between groups in regards to injured spine segments that were grouped based on spinal characteristics and vertebral levels. Data on the different fracture patterns may help professionals develop safety equipment for motorcyclists.
Supplemental Material
Download Zip (42.9 KB)Acknowledgments
There are no acknowledgements or disclosures for this study.
Conflicts of interest and source of funding
No author or any member of his or her immediate family have any funding or commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. No research support was received for this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The authors confirm the data supporting the findings of this study are within the article and its supplementary materials.
Additional information
Funding
References
- Afquir S, Melot A, Ndiaye A, Hammad E, Martin JL, Arnoux PJ. 2020. Descriptive analysis of the effect of back protector on the prevention of vertebral and thoracolumbar injuries in serious motorcycle accidents. Accid Anal Prev. 135:105331. PMID: 31751784. doi:10.1016/j.aap.2019.105331.
- Arana E, Kovacs FM, Royuela A, Asenjo B, Pérez-Ramírez Ú, Zamora J. 2016. Spine Instability Neoplastic Score: agreement across different medical and surgical specialties. Spine J. 16(5):591–599. PMID: 26471708. doi:10.1016/j.spinee.2015.10.006.
- Ashie A, Wilhelm A, Carney D, DiPasquale T, Bush C. 2018. Comparing fracture patterns of younger versus older riders involved in nonfatal motorcycle accidents. Traffic Inj Prev. 19(7):761–765. PMID: 29985641. doi:10.1080/15389588.2018.1494384.
- Burns ST, Gugala Z, Jimenez CJ, Mileski WJ, Lindsey RW. 2015. Epidemiology and patterns of musculoskeletal motorcycle injuries in the USA. F1000Res. 4:114. PMID: 26309727. doi:10.12688/f1000research.4995.1.
- Chaudhuri U, Ratnapradipa KL, Shen S, Rice TM, Smith GA, Zhu M. 2019. Trends and patterns in fatal US motorcycle crashes, 2000–2016. Traffic Inj Prev. 20(6):641–647. PMID: 31283363. doi:10.1080/15389588.2019.1628224.
- Cooper C, Atkinson E-J, O’Fallon W-M, Melton L-J. 1992. Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985–1989. J Bone Miner Res. 7(2):221–227. PMID: 1570766. doi:10.1002/jbmr.5650070214.
- Crosswalk of Common Spine ICD-9-CM Codes to ICD-10 Codes. 2015. Oct. National Association of Spine Specialists. https://www.spine.org/Portals/0/Assets/Downloads/PolicyPractice/ICD10Codes.pdf.
- de Rome L, Ivers R, Fitzharris M, Du W, Haworth N, Heritier S, Richardson D. 2011. Motorcycle protective clothing: protection from injury or just the weather? Accid Anal Prev. 43(6):1893–1900. PMID: 21819816. doi:10.1016/j.aap.2011.04.027.
- Ekmejian R, Sarrami P, Naylor JM, Harris IA. 2016. A systematic review on the effectiveness of back protectors for motorcyclists. Scand J Trauma Resusc Emerg Med. 24(1):115. PMID: 27716409. doi:10.1186/s13049-016-0307-3.
- Ensrud KE, Schousboe JT. 2011. Clinical practice. Vertebral fractures. N Engl J Med. 364(17):1634–1642. PMID: 21524214. doi:10.1056/NEJMcp1009697.
- Fierro N, Inaba K, Aiolfi A, Recinos G, Benjamin E, Lam L, Strumwasser A, Demetriades D. 2019. Motocross versus motorcycle injury patterns: a retrospective National Trauma Databank analysis. J Trauma Acute Care Surg. 87(2):402–407. PMID: 31045729. doi:10.1097/TA.0000000000002355.
- Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, Harrop JS, Fehlings MG, Boriani S, Chou D, et al. 2010. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine. 35(22):E1221–E1229. PMID: 20562730. doi:10.1097/BRS.0b013e3181e16ae2.
- Grant T, Whipp J-A. 1976. Injuries resulting from motorcycle desert racing. Am J Sports Med. 4(4):170–172. PMID: 984293. doi:10.1177/036354657600400408.
- Harris JH, Jr, Edeiken-Monroe B, Kopaniky DR. 1986. A practical classification of acute cervical spine injuries. Orthoped Clin North Amer. 17(1):15–30. PMID: 3511428. doi:10.1016/S0030-5898(20)30415-6.
- Kepler CK, Vaccaro AR, Koerner JD, Dvorak MF, Kandziora F, Rajasekaran S, Aarabi B, Vialle LR, Fehlings MG, Schroeder GD, et al. 2016. Reliability analysis of the AOSpine thoracolumbar spine injury classification system by a worldwide group of naïve spinal surgeons. Eur Spine J. 25(4):1082–1086. PMID: 25599849. doi:10.1007/s00586-015-3765-9.
- Kraus JF, Peek C, Williams A. 1995. Compliance with the 1992 California motorcycle helmet use law. Am J Public Health. 85(1):96–99. PMID: 7832270. doi:10.2105/ajph.85.1.96.
- National Center for Statistics and Analysis. 2020. November. Traffic safety facts 2018 annual report: a compilation of motor vehicle crash data (Report No. DOT HS 812 981). National Highway Traffic Safety Administration.
- National Electronic Injury Surveillance System. 2022. April. National Estimate of Injuries Treated in Emergency Departments Treatment Dates: 01/01/2018 – 12/31/2018. United States Consumer Product Safety Commission.
- Robertson A, Giannoudis PV, Branfoot T, Barlow I, Matthews SJ, Smith RM. 2002. Spinal injuries in motorcycle crashes: patterns and outcomes. J Trauma. 53(1):5–8. PMID: 12131381. doi:10.1097/00005373-200207000-00002.
- Singh R, Bhalla A, Ockendon M, Hay S. 2018. Spinal Motocross Injuries in the United Kingdom. Orthop J Sports Med. 6(1):2325967117748644. PMID: 29349095. doi:10.1177/2325967117748644.
- Vaccaro AR, Oner C, Kepler CK, Dvorak M, Schnake K, Bellabarba C, Reinhold M, Aarabi B, Kandziora F, Chapman J, et al. 2013. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine. 38(23):2028–2037. PMID: 23970107. doi:10.1097/BRS.0b013e3182a8a381.
- Wood KB, Li W, Lebl DR, Ploumis A. 2014. Management of thoracolumbar spine fractures. Spine J. 14(1):145–164. PMID: 24332321. doi:10.1016/j.spinee.2012.10.041.
- Wu D, Hours M, Ndiaye A, Coquillat A, Martin JL. 2019. Effectiveness of protective clothing for motorized 2-wheeler riders. Traffic Inj Prev. 20(2):196–203. PMID: 30901230. doi:10.1080/15389588.2018.1545090.