
Abstract
Objective
Many children with physical disabilities need additional postural support when sitting and supplementary padding is used on standards approved child restraints to achieve this when traveling in a motor vehicle. However, the effect of this padding on crash protection for a child is unknown. This study aimed to investigate the effect of additional padding for postural support on crash protection for child occupants in forward facing child restraints.
Methods
Forty frontal sled tests at 49 km/h were conducted to compare Q1 anthropometric test device (ATD) responses in a forward-facing restraint, with and without additional padding in locations to increase recline of the restraint, and/or support the head, trunk and pelvis. Three padding materials were tested: cloth toweling, soft foam, and expanded polystyrene (EPS). The influence of padding on head excursion, peak 3 ms head acceleration, HIC15, peak 3 ms chest acceleration and chest deflection were analyzed.
Results
The influence of padding varied depending on the location of use. Padding used under the restraint to increase the recline angle increased head injury metrics. Toweling in multiple locations which included behind the head increased head excursion and chest injury metrics. There was minimal effect on injury risk measures with additional padding to support the sides of the head or the pelvis position. Rigid EPS foam, as recommended in Australian standards and guidelines, had minimal effect on injury metrics when used inside the restraint, as did tightly rolled or folded toweling secured to the restraint at single locations around the body of the child.
Conclusions
This study does not support the use of postural support padding to increase recline of a forward-facing restraint or padding behind the head. Recommendations in published standards and guidelines to not use foam that is spongy, soft or easily compressed, with preference for secured firm foam or short-term use of tightly rolled or folded toweling under the child restraint cover is supported. This study also highlights the importance of considering the whole context of child occupant protection when using additional padding, particularly the change in the child’s seated position when adding padding in relation to the standard safety features of the restraint.
Introduction
Promotion of correct use of size-appropriate child restraints is a widespread measure used to improve protection of children in motor vehicles and reduce risk of fatalities and injuries (Du et al. Citation2010). However, child restraints designed for typically developing children often fail to provide adequate support for the safe transportation of children with impaired motor or sensory function, challenging behaviors, orthopedic conditions or respiratory compromise (Huang et al. Citation2009; Baker et al. Citation2011; Downie et al. Citation2019). As a result, these children are often required to travel in inappropriate child restraints, modified restraints, their own wheelchair, or special purpose child restraints (Anund et al. Citation2003; Falkmer and Gregersen Citation2001).
In Australia, 7.7% of children under the age of 15 are reported as having a disability; with the prevalence of disability increasing with age, from 3.7% of children aged 0–4 years to 9.6% of children aged 5–14 years (Australian Bureau of Statistics Citation2018). Internationally, in the United States of America, 4.3% of children under the age of 18 have a disability (United States Census Bureau, 2019); with 4% of children in Europe under 16 years having moderate to severe activity limitations, and 6.5% of children under 16 years having limitations in activities in the United Kingdom (Eurostat Citation2020). Like typically developing children and despite impairments, children with a disability must use an approved restraint when traveling in cars, in accordance with jurisdictional rules, regulations, and standards.
For children with physical disabilities, poor postural seated position is a common concern for parents (Falkmer and Gregersen Citation2002; Black et al. Citation2023), and modifications, including additional padding, to child restraints are often made to improve support and position of children in the seat (O’Neil et al. Citation2009; Black et al. Citation2023; Cook et al. Citation2024). Guidelines for transporting children with disabilities, including the use of additional padding on compliant child restraints, have been published by The American Academy of Pediatrics (Citation1999, updated in 2019); and in the Australian/New Zealand Standard 4370:2013 Restraint of children with disabilities or medical conditions in motor vehicles. Both publications provide guidance on the use of rolled towels, cloth nappies and foam for positioning. Both also direct against using soft padding beneath or behind the child due to compression in a crash potentially creating slack in the harness, with the Australian standard specifying the maximum weight (must not exceed 2 kg in total weight) and type of allowable foam (firm foam, flame retardant and slow burning, suitably covered and secured in flame retardant material). Fitting additional padding, on top of the original manufacturer’s padding, to a standard child restraint is also recommended in clinical practice literature (Lovette Citation2008; Bull Citation2008; Bull et al. Citation2009: O’Neil et al. Citation2019; Teerds and Cameron Citation2015; Carmen et al. Citation2021).
Despite these recommendations on additional padding use and types, there are no known studies examining the effect of this padding in the event of a crash. Previous research on padding for child restraints has primarily focused on the impact of the manufacturer’s padding in the head area on injury mitigation for typically developing children (Abdelilah et al. Citation2005; Arsdell et al. Citation2009); or on the use of a customized foam positional device for premature babies which had favorable results in simulated crash testing and driving scenarios (Chen et al. Citation2014; Czubernat et al. Citation2014).
The aim of this study was to investigate the effect of additional padding, as recommended in clinical guidelines for children with disability and seen in a recent survey of real world practices (Cook et al. Citation2024), on injury risk for a restrained child occupant in simulated frontal crash tests.
Methods
Study design
The effect of three different types of additional padding added to the child restraint in various locations (wedge under the restraint to increase recline (hereafter called wedge padding); at head wings; trunk, under knees, behind pelvis, as a crotch roll; and multiple toweling locations) was evaluated in a series of forty frontal sled crash tests. The responses in these cases were compared to the restraint with no additional padding (baseline). Each test was conducted twice under identical conditions as indicated in . The full test matrix and results are in Table S1.
Table 1. Summary of test conditions.
Sled testing setup
Tests were conducted using a custom-designed deceleration sled (Escribano, Spain). The target test pulse was calibrated as per the standard frontal impact test from AS/NZS 3629.1 (2013), which requires a sled velocity change of not less than 49 km/h with peak deceleration between 24 and 34 g lasting for at least 20 ms. An example sled pulse is shown in Appendix (Figure S1). The child restraint was secured to a bench seat rig that adheres to the standard AS/NZS 3629.1 (2013). The sled was fitted with a single TE Connectivity 64 series 200-g accelerometer (Schaffhausen, Switzerland) to record deceleration of the sled. Accelerometer signals from the ATD were collected by a modular data acquisition system (Slice Pro, DTS) to calculate the resultant maximum head and chest acceleration, and chest deflection. Data was filtered in line with SAE J211 (Society of Automotive Engineers, 2014).
Two high speed cameras, one mounted directly to the side of the impact point and one mounted overhead (Phantom Miro C210, Phantom Miro C111, Vision Research, Wayne, NJ, USA) recorded the impact event.
Child restraint
A forward-facing child restraint with inbuilt 6 point harness suitable for use by children aged 6 months to 8 years (Britax Maxi-Guard Pro, Type G under AS/NZS 1754:2013). The restraint was used in the forward-facing upright configuration with the built-in harness. It was secured in the upright position to the bench seat using a lap sash seat belt and top tether, following the test procedures in AS/NZS 3629.1 (2013). The restraint, seat belt and top tether were inspected for damage after each test run, including webbing, harness, buckle and shell. The restraint was replaced if any sign of damage was identified. The same child restraint was used for each test, until replacement with a new restraint for the final 10 tests due to signs of plastic whitening adjacent to the mounting of the top tether observed in test 30. This restraint is certified for use by children aged up to approximately 8 years and has been shown to fully maintain its structural integrity in a 56 km/h frontal test with a larger Q10 ATD in consumer testing programs.
Padding
Three different padding materials were used. Further details on the set up of each padding are provided in the Appendix.
Pure cotton terry toweling cloth nappies (diapers) (600 mm × 600 mm). Each toweling was folded into various thicknesses required to provide the postural support.
Dunlop Enduro Protect EN36-90 (Dunlop Foams, Wetherill Park, Australia) “medium-firm density” square cushion foam was cut to various sizes and thickness depending on where it was positioned for required postural support. For the wedge, a Dunlop Enduro Protect EN40-230 “medium-firm density” foam precut wedge was used. This foam was selected as it is readily available to allied health professionals and the general public and is commonly used for armrests on chairs, seats and cushions.
Expanded polystyrene (EPS) (Standard grade (13.5kg/m3, The Foam Company, Sydney, Australia). This is a lightweight, closed cell, rigid material. EPS sheets were cut to various sizes to provide consistent postural support with the other padding types.
Each padding material was secured to itself and the child restraint under the cover of the restraint (excluding wedge padding) using 3 M Micropore paper tape (25 mm) (3 M, Saint Paul, MN, USA). This surgical tape is readily available to allied health professionals.
Thickness of padding was measured before and after each crash test to determine any crush of the padding. A needle was inserted into an identical point on each padding, with depth of the padding marked on the needle and distance from the needle tip measured with a measuring tape.
Anthropometric test device
A Q1 anthropomorphic test device (ATD) (Humanetics, Farmington Hills, MI, USA), representative of a 1-year-old child was secured in the child restraint for each test. Children in Australia are legally permitted to travel in forward facing restraints from 6 months of age but are recommended to remain rearward facing for as long as possible; and the Q1 ATD was chosen to represent the youngest age where a child is commonly forward facing.
The ATD was instrumented with three single-axis accelerometers at the head center of gravity (Gx and Gy – Endevco 7264 C-2KTZ-5V-10V − 2000 G, Gz – Endevco 7264B-500T − 500 G, Irvine CA, USA) and in the chest (Gx, Gy and Gz - TE Connectivity – 64x-2000-197 – 2000 G, Schaffhausen, Switzerland), with further instrumentation to measure chest deflection (Firstmark 170-0161-2 N Position Transducer, Creedmor NC, USA). Tracking markers were used at the head center of gravity on the ATD and a second marker on the sled test bench common to all tests.
Test protocol
For baseline tests (with no additional padding), the child restraint was installed onto the test bench according to the manufacturer’s instructions. The ATD was secured in the restraint following Australian standard (AS/NZS 3629.1:2013) procedures. Markings for the initial position of the knee joint and center of the head were made on the child restraint cover. These positions were visually reviewed post-crash and any changes measured.
Each padding condition (see ), excluding trunk padding, was installed prior to the restraint being secured to the test bench. To apply the padding (excluding wedge), the cover of the child restraint was removed to access the shell; the ATD was placed in the child restraint; padding was secured onto the shell in the required area around the ATD to provide postural support. The ATD was then removed from the restraint and the cover re-fitted. The Australian Standard procedure was followed to install the restraint onto the bench, place the ATD in the restraint and tighten the 6 point harness. Further details of the baseline set up and padding set up are provided in the Appendix.
To secure the restraint in the reclined position with wedge padding, an additional 270 mm length of seat belt webbing was required from the upper sash anchorage compared to the unmodified upright restraint (see ). The crotch strap for the harness on the restraint was also adjusted to a longer position (by 40 mm) when using pelvic padding to accommodate the altered ATD position.
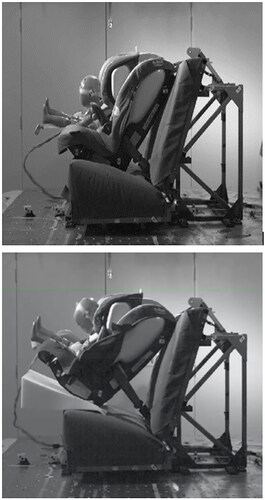
Figure 1. High speed video still shots 74 ms after onset of impact from tests of the unmodified restraint (top) and restraint with soft foam wedge underneath (bottom) to increase seat recline. Note the increased recline along with longer seatbelt required for installation in the latter, result in substantially larger forward motion of the restraint and ATD.
Data analysis
Head excursion, HIC15, chest deflection, and head and chest peak 3 ms resultant accelerations were examined as outcome variables. Maximum head excursion in the forward direction was calculated from the side view using ProAnalyst Software (XCitex, Woburn, MA) as the maximum distance between the furthest point of the head and seat bight.
The resultant maximum head and chest acceleration and Head Injury Criterion (HIC) were calculated using a custom MATLAB program. Non-biofidelic head contacts with the arms or legs of the ATD identified in high-speed video footage was excluded from analysis.
Statistical analysis was conducted in Graphpad Prism version 9.0 (GraphPad Inc., La Jolla, CA). Repeated measures ANOVA was used to compare each of the outcome measures with the presence/location of padding and type of padding. A post-hoc Dunnett’s test (hereafter called Dunnett’s test) was used to determine whether injury metrics were different between padding in each location and baseline, and compare the effect of padding type used in each location to baseline. An alpha of 0.05 was considered statistically significant.
Injury assessment reference values
The child restraint used complies with AS/NZS 1754:2013, however there are no established injury assessment reference values for the Q1 ATD in Australian restraints, as they are compliance tested with P-series ATDs. The Child Restraint Evaluation Program (CREP) in Australia assesses crash protection performance of car seats in simulated front impact tests and offers safety recommendations to the public. Minimum requirements are provided in CREP for a Q1 ATD in a Type G child restraint (450 mm for head excursion, 82 g for head acceleration, 55 g for chest acceleration). Therefore, CREP’s scoring criteria for the Q1 were used as a basis for comparing the performance of the restraint with and without padding in this study.
Results
A total of 40 frontal impact tests were completed. The impact of each padding condition on each primary outcome variable is shown in Table S1. The variation in measured variables between replicates of each padding condition is provided in Figure A2. Variability did not appear to increase with repeated use of the same restraint, nor with the introduction of a new restraint. In all tests, the ATD remained contained within the restraint. In most cases, the padding remained in position during the pre-impact and deceleration phases of the tests. However, all types of wedge padding were ejected forward during impact, and the toweling wedge became dislodged as the sled accelerated pre-impact.
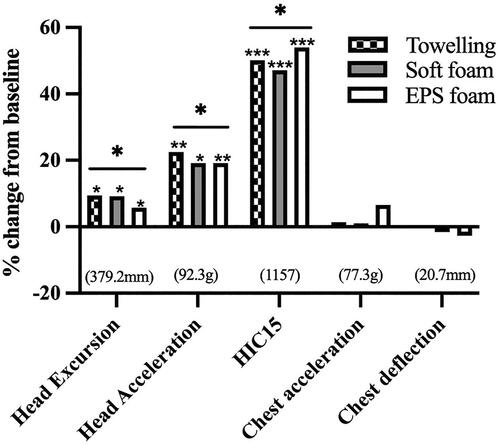
Figure 2. Effect of wedge padding to recline restraint on injury metrics. % change in mean of injury metric from baseline restraint. Mean baseline value shown in brackets. * indicates a significant main effect of padding on head injury metrics (head excursion, acceleration and HIC15) from baseline (p < 0.0001). Asterisks represent significance levels for dunnett’s post hoc tests comparing padding type to baseline: *p < 0.05, **p < 0.01, ***p < 0.001. Toweling and soft foam (*p = 0.014) and EPS foam (*p = 0.017) significantly increased head excursion. Toweling (**p = 0.004), soft foam (*p = 0.0175), and EPS foam (**p = 0.0096) significantly increased HIC15.
Toweling positioned on the restraint moved the most and showed the greatest change in thickness from pre to post-crash. When placed between the head wings and shell of the restraint, the toweling slid down increasing the distance between the head wings by 10–15mm after the crash. This did not occur with other padding types in the head location.
Toweling experienced crush when under the knees (crush of 20 mm) and behind the pelvis (crush of 25 mm). EPS foam under the knees crushed by 10 mm under the legs of the ATD. Crumbling of the EPS was observed following the use in the crotch area. No permanent crush of the soft foam in any location was observed post-crash.
The location of padding had significant main effect on head injury metrics (head excursion (F (7, 24) = 14.83, p < 0.0001; head acceleration (F (7,24) = 11.07, p < 0.0001; HIC 15 (F (7, 24) = 40.27, p < 0.0001). The effect of padding type varied depending on the location it was applied, with significant interaction effect between padding location and type for chest acceleration (F (14,24) = 4.871, p = 0.0003); and chest deflection (F (14, 24) = 3.867, p = 0.0018).
Wedge padding to increase recline of restraint
With all wedge padding types, greater forward movement of the child restraint on the test bench occurred (see ). Less than half of the base of the child restraint was in contact with the test bench when toweling padding was used, while only the rear base legs of the restraint remained in contact with the test bench with EPS and soft foam. The child restraint rotated toward the seat belt upper anchorage during impact, with the ATD head contacting the left head wing. The recline position of the restraint also resulted in the ATD head position being behind the shoulders at the time of peak sled deceleration with all padding types, in comparison to the baseline ATD position, resulting in the head having a greater distance to travel during deceleration.
All types of wedge padding increased peak forward head excursion compared to baseline (Dunnett’s test, p < 0.0001), with toweling (35.6 mm (9.4%) increase) and soft foam (34.8 mm (9.2%) increase) having greater effect than EPS foam (24.8 mm (6.5%) increase) (see ). Head acceleration was significantly increased (Dunnett’s test, p < 0.0001), ranging from 17.7 g (19.2%) for soft foam, to 20.8 g (22.5%) with toweling. The time at which the ATD head reached peak acceleration was later compared to baseline of 77.7 ms. Maximum head acceleration was reached at 90.6 ms (increase of 12.9 ms) with toweling; 93.0 ms (increase of 15.3 ms) with soft foam; and 94.1 ms (increase of 16.4 ms) with EPS foam. The use of all padding types increased HIC15 (Dunnett’s test, p < 0.0001), with increases from 47.1% to 54% from baseline.
Head padding
The reduced space between the head wings with the side head support padding did not alter the forward trajectory of the ATD head compared to baseline. The head remained contained within the head wings during rebound. Nor did padding in the head wings significantly alter any head or chest injury metrics compared to baseline (see Figure A2). Time to reach maximum resultant chest acceleration was increased, by between 1.9–17.9 ms, with EPS foam giving the greatest delay compared to baseline (Dunnett’s test, p = 0.046).
Trunk padding
The ATD’s arms were unable to be positioned against the body with trunk padding in place, and both arms extended forward at time of sled deceleration. Arm to head contact was observed with all padding types. Bilateral foot to head contact was also observed with EPS and soft foam. The addition of EPS foam resulted in the ATD slightly rotating toward the upper seat belt anchorage during rebound. This did not occur with toweling or soft foam.
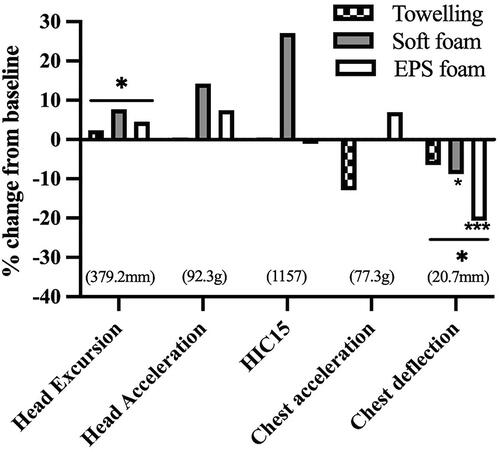
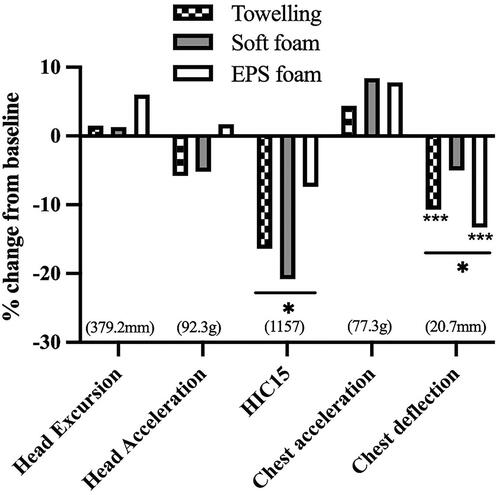
Padding at the trunk increased head excursion (Dunnett’s test, p = 0.04) with soft foam having the greatest increase from baseline of 29.2 mm (7.7% increase) (see ). There were no significant differences between trunk padding types on head excursion compared to baseline. There was a reduction in chest deflection ranging from −6.5% to −20.6% (Dunnett’s test, p < 0.0001), with an interaction effect of the type of padding used. Post-hoc testing showed soft foam (8.8% decrease, Dunnett’s test, p = 0.017) and EPS foam (20.6% decrease, Dunnett’s test, p < 0.0001) having the greatest impact on decreasing chest deflection.
Figure 3. Effect of trunk padding on injury metrics. % change in mean of injury metric from baseline. Mean baseline value shown in brackets. * indicates a significant main effect of trunk padding on head excursion (p = 0.04 and chest deflection (p < 0.0001). Asterisks represent significance levels for dunnett’s post hoc tests comparing padding type at the trunk to baseline: *p < 0.05, **p < 0.01, ***p < 0.001. Soft foam (*p = 0.017) and EPS foam (***p < 0.0001) significantly decreased chest deflection from baseline.
Knee padding
Despite raising the knee position compared to baseline, there was no knee to head contact with any padding. Toweling under the knees resulted in left foot strikes to the head. This did not occur with other padding types. The ATD demonstrated symmetrical forward movement during deceleration of the sled.
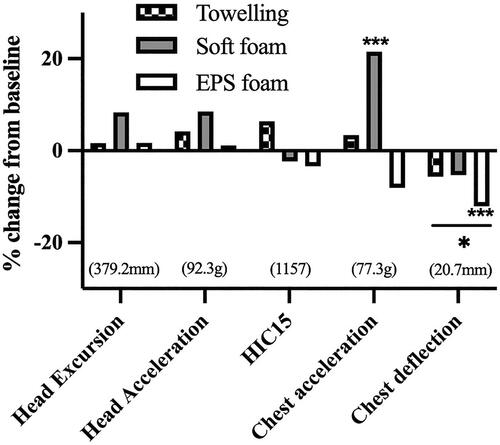
Padding under the knees had no significant effect on head injury metrics (see ). The type of padding used influenced chest acceleration, with soft foam increasing chest acceleration by 21.5% over baseline (Dunnett’s test, p = 0.002). Chest deflection was reduced by all padding types compared to baseline (main effect Dunnett’s test, p < 0.0001) with EPS foam having the greatest decrease (12.1% decrease, Dunnett’s test, p = 0.0006).
Figure 4. Effect of knee padding on injury metrics. % change in mean of injury metric from baseline. Mean baseline value shown in brackets. * indicates a significant main effect of knee padding on chest deflection (p < 0.0001). Asterisks represent significance levels for dunnett’s post hoc tests comparing padding type to baseline: *p < 0.05, **p < 0.01, ***p < 0.001. Soft foam significantly increased chest acceleration from baseline (p = 0.002) and EPS foam reduced chest deflection compared to baseline (p = 0.0006).
Pelvis padding
The addition of padding behind the pelvis pushed the lower body of the ATD forward in the restraint. With all padding types, there was foot to head contact. Post-impact, the ATD pelvic position had moved 20 mm forward from original seated position with all padding types.
Padding behind the pelvis did not significantly increase injury metrics (see ). There was a main effect decrease in HIC15 with pelvic padding, with an average decrease of 14.9% (main effect Dunnett’s test, p = 0.015), however no significant differences from baseline with the type of padding. Time to reach maximal head excursion was increased by 2.2% compared to baseline (Dunnett’s test, p = 0.041). All padding decreased chest deflection by an average of 2 mm (main effect Dunnett’s test, p < 0.0001), with post-hoc testing showing significant effect of toweling (2.2% decrease, Dunnett’s test, p = 0.003) and EPS foam (2.7% decrease, Dunnett’s test, p = 0.0002) compared to baseline.
Figure 5. Effect of pelvis padding on injury metrics. % change in mean of injury metric from unpadded baseline restraint. Mean baseline value shown in brackets. * indicates a significant main effect of pelvis padding on HIC15 (p = 0.015) and chest deflection (p < 0.0001) from baseline. Asterisks represent significance levels for dunnett’s post hoc tests comparing padding type to baseline: *p < 0.05, ** p < 0.01, *** p < 0.001. Both toweling (p = 0.003) and EPS foam (p = 0.0002) reduced chest deflection from baseline.
Crotch roll padding
The ATD made head contact with the rolled toweling padding. The ATD moved in a symmetrical forward direction during sled deceleration. There were no visible changes in the positioning of the ATD post-crash. Padding in the crotch area did not significantly increase or decrease injury metrics (see Figure A3).
Combined toweling padding
The combined toweling padding included padding behind the head, along both sides of the trunk, behind the pelvis, and lateral to the thighs (see ). Despite the padding placing the ATD with a slight upper body tilt (consistent with pelvis padding), there was no forward translation of the ATD on the restraint post-crash. In contrast to individual trunk padding tests, the arms of the ATD were able to be positioned beside the body, and there was only arm to head contact during one of the tests. However, bilateral foot to head contact occurred in all tests. The head of the ATD remained within the head wings during rebound, with the shoulders symmetrical and moving forward equally.
Figure 6. Multiple toweling padding, behind the head (left), supporting body (right).

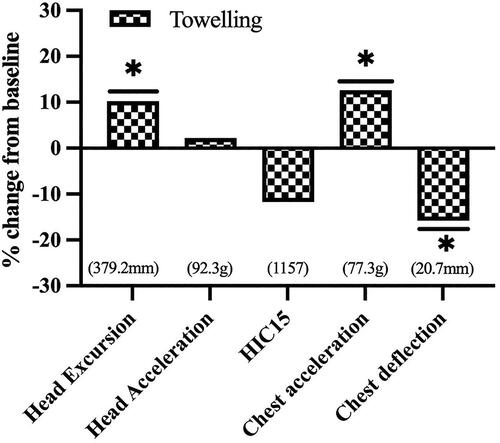
The combined toweling padding, which included padding placed behind the head increased head excursion by 10.2% (absolute increase of 38.7 mm) from baseline (Dunnett’s test, p < 0.0001) (see ). This padding also increased the time to reach peak head excursion by 3.3% (Dunnett’s test, p = 0.006), resultant peak head acceleration by 13.5% (Dunnett’s test, p = 0.032), and chest acceleration by 9.76 g from baseline (Dunnett’s test, p = 0.0007). Chest deflection was reduced by 3.2 mm (15.8%) compared to baseline (Dunnett’s test, p < 0.0001).
Figure 7. Effect of combined toweling padding on injury metrics. % change in mean of injury metric from unpadded baseline restraint. Mean baseline value shown in brackets. * indicates a significant main effect of combined toweling padding on increasing head excursion (p < 0.0001) and chest acceleration (p = 0.0007) and decreasing chest deflection (p < 0.0001) from baseline.
Discussion
This series of crash tests performed using a forward-facing child restraint with a range of additional padding showed that some forms of padding used for postural support for children with disability can significantly impact measures that increase injury risk. While additional padding to support the sides of the head, pelvis, knees, and at the crotch had minimal effect on head or injury risk measures, padding used as a wedge under the restraint to increase the recline angle increased head injury metrics substantially (by 5–54% depending upon the metric). Combined toweling padding behind the head and pelvis, and along the sides of trunk and thighs, and soft foam padding at the trunk also increased injury metrics. Rigid EPS foam, as recommended by AS/NZS 4370, had minimal effect on injury metrics when used inside the restraint, as did tightly rolled or folded toweling secured to the restraint around single locations on the body of the child.
Increasing the recline angle of child restraints with padding may be recommended to assist in preventing a child’s head falling forward and airway obstruction (O’Neil et al. Citation2019; AS/NZS 4370, 2013). However, all padding types used as a wedge to increase the recline of the restraint increased head acceleration by over 20% and chest acceleration by up to 6.6%. These increased values exceeded CREP reference values, indicating increased risk. The change in position of the restraint and child from the additional padding, and the need for an extended seatbelt to secure the modified restraint likely contributed to these increases. In the reclined position, the child’s upper body is not aligned vertically above the pelvis, the distribution of crash forces on the restraint and ATD is therefore altered, and the upper body and head have a greater distance to travel forward during sled deceleration. While the whole restraint was reclined here, our findings are consistent with recent studies showing that reclined seat back positions, whether in adults (Górniak et al. Citation2003), or children using booster seats (Bohman et al. Citation2022), result in increased head acceleration and head displacement compared to upright positions. The ejection of the padding from under the restraint during impact, resulting in the restraint being loosely secured by the longer seatbelt, also contributed to greater ATD movement and rotation, increasing head excursion and head acceleration. These findings align with misuse studies where seatbelt slack has been found to increase forward head excursion (Manary et al. Citation2019). The padding ejection and resulting loose installation of the restraint could also have detrimental effects for secondary impacts. This study does not support the use of wedge padding to increase recline of a forward facing restraint. Alternative compliant restraints with inbuilt features for additional head support, lie flat restraints, or maintaining a child in a rearward facing restraint should be considered in contrast to supplementary padding for recline.
A key approach to reducing head injury risk for children is minimizing head excursion, as this lowers the chance of head impact during a crash. In these tests, padding behind the head in the combined toweling tests increased head excursion by nearly 10%. This is likely at least partially due to the head’s initial position being 50 mm further forward. Use of a combination of toweling padding is common in Australian hospitals for children wearing lower limb casts or splints. As the child needs to be positioned further forward in the seat to accommodate the cast, padding behind the head reduces gaps and supports the head to be in line with the trunk. While the head excursion results were still under the CREP reference value, the increased risk associated with higher head excursion needs to be balanced against potential advantages of the padding. AS/NZS 4370:2013 and the American Academy of Pediatrics (2019) recommend not using padding behind a child, since compression of the padding can introduce slack in the harness system. Consideration also needs to be given to padding placing the child in a more forward position and increasing risk of head impact with the vehicle interior in a frontal crash. There is also the risk of this padding reducing the effective depth of the side wings and potentially exposing more of the head outside of the side wings in a side impact (which was not tested here). Previous studies have found child restraints and booster seats with shallower side wings are unable to retain the torso or head of an ATD to prevent contact with the side door structure (Huot et al. Citation2005; Bilston et al. Citation2005).
Chest acceleration is used for evaluating risk of thoracic injuries during a crash. The combined use of toweling padding in multiple locations, as recommended in Australia for children with orthopedic conditions to provide clearance for leg casts/splints, substantially increased chest acceleration by 12.6%. Since use of toweling at the trunk alone reduced chest acceleration (by 12.9%), and at the pelvis increased chest acceleration (by 4.4%), this increase is likely due to the simultaneous use of the padding, which also included padding behind the head and along the thighs (which were not tested individually). The combination of the upper body of the ATD being slightly tilted back due to pelvic padding and the head also being positioned further forward, might have reduced the ability for the trunk toweling to support the torso. The use of more conforming, tighter foam around the trunk area may be required if a child needs to be positioned further forward in a restraint.
Although padding to the head wings, trunk, pelvis, knees and crotch areas did not significantly increase injury risk, careful selection of the type of padding used in these areas may help lower risks. Toweling padding in the side wings adjacent to the head, trunk and under the pelvis had lower increases in overall head and chest injury metrics from baseline than when soft foam and EPS was used in these locations. This is likely because of its capability to be shaped and conform closely to the contours of the restraint and ATD, as seen with toweling at the trunk reducing chest acceleration by 12.9% from baseline in comparison to soft foam and EPS increasing this injury metric from baseline. Toweling had the greatest change in thickness from pre to post-crash, possibly due to compression when maneuvering the padding into position. Rigid foam was effective when used in locations to counteract the occupant sliding forward, such as under the knees and as a crotch roll. The compression of soft foam may likely have contributed to increases in head injury risks when used in the head and trunk areas, however this could not be visualized during the crash and was not present post-crash. This supports recommendations in AS/NZS 4370: 2013 and from American Academy of Pediatrics to not use foam that is spongy, soft or easily compressed, with preference for firm foam or short-term use of towels.
In considering implications of these results, the following limitations must be considered. The study was limited to a single type of forward facing child restraint and Q1 ATD in frontal impacts only. Results therefore may not be applicable to other forward facing restraints; cannot be extrapolated to rearward facing restraints, a larger child or side impact crashes. Moreover, real-world children with disabilities have muscle weakness, stiffness or physical characteristics which are not replicated by the rigid, symmetrical Q1 ATD. Movement of children in restraints, or repeated transferring of the child in and out the restraint may also cause padding to shift. This series tested new padding appropriately secured to the restraint on each separate test. The performance of padding that has been repeatedly used, as likely in real-world practice, was not tested and is not known. Padding used was also cut to fit the size of the ATD, with the Q1 was chosen to represent the smallest child likely to use a forward facing restraint. Customized padding or thicker padding may be required by larger children or children with disabilities resulting in greater muscle tone resistance. There is limited literature on how padding is being used in the real world and further testing of other padding types or location configurations would need to be further studied. Relying on previous literature from Whyte et al. (Citation2021) on child restraints maintaining their performance in repeated impacts, our study used the same child restraint for crash tests 1 to 30, with a new child restraint used for crash tests 31 to 40 due to visible signs of plastic whitening damage to the initial restraint. Comparisons in child restraint performance with padding were also made to two replicate baseline tests performed at the beginning of the test matrix. Therefore, presence of minor (not visible) cumulative damage to webbing and the restraint altering the baseline restraint performance across the test series cannot be ruled out, but since variability of ATD accelerations did not increase with repeated use of the same restraint, any such effect is likely to be very small.
With there being no established injury assessment reference values for the Q1 ATD in Australian restraints, the minimum requirements of the Child Restraint Evaluation Program in Australia were used to assist in interpreting safety implications of padding modifications. All additions of padding fell under the head excursion criterion from CREP. However, all test results for head acceleration and chest acceleration with all locations and padding types, including the baseline tests, were above CREP criteria for head and chest acceleration, indicating the modified restraint would have low safety scores for child safety performance in CREP. Further work is indicated on different combinations of child restraints, padding and ATD to compare to published injury assessment values.
In conclusion, this study does not support the use of wedge padding to increase recline of a forward facing restraint, or padding that is placed behind the head, since these conditions substantially increased head excursion and head acceleration in frontal sled tests, increasing a child’s risk of head injury. If additional postural support is needed, firm rigid (EPS) foam, which maintains position and is less susceptible to deformation, is preferred. Tightly rolled or folded toweling may be used around the body of a child, but should not be used behind the child. As per Australian standards, all foam or toweling should be secured to the child restraint under the cover of the restraint. Guidance specified by the American Academy of Pediatrics, and Mobility and Accessibility for Children in Australia (MACA Ltd) for modifying child should be followed pending any manufacturer alterations to currently existing restraints that meet standards for use. Special purpose child restraints designed for specifically transporting children wearing lower body casts/splints are an available option in America; however currently do not meet standards for use in Australia. Further research is needed to determine the best options for children requiring forward facing restraints to be reclined due to risk of respiratory compromise during travel.
Supplemental Material
Download Zip (3.1 MB)Disclosure statement
This work was conducted at the Transurban Road Safety Center at Neuroscience Research Australia. The first author is supported by a Philanthropic donation from the T&K Wonderland Foundation. The authors have no financial interest or benefit from this study.
Additional information
Funding
References
- Abdelilah Y, Sherwood CP, Marshall R, Gopalan S, Crandall JR. 2005. The effects of head padding in rear facing child restraints. SAE Technical Paper Series. doi:10.4271/2005-01-1839.
- Arsdell E, Amirault D, Marsden A, Oltman S, Richards D, Prange M. 2009. Effect of padding on child restraint performance during side impact collisions. SAE Technical Paper Series. doi:10.4271/2009-01-1244.
- American Academy of Pediatrics. 1999. Transporting children with special health care needs. Pediatrics. 104(4):988–992. doi:10.1542/peds.104.4.988.
- Anund A, Falkmer T, Forsman A, Gustafsson S, Matstoms Y, Sorensen G, Turbell T, Wenall J. 2003. Child safety in cars: literature review. VTI Rapport. https://diva-portal.org/smash/get/diva2:675232/Fulltext01.pdf.
- Australian Bureau of Statistics. 2018. Disability, ageing and carers, Australia: summary of findings. https://www.abs.gov.au/statistics/health/disability/disability-ageing-and-carers-australia-summary-findings/latest-release.
- Baker A, Galvin J, Vale L, Lindner H. 2011. Restraint of children with additional needs in motor vehicles: knowledge and challenges of paediatric occupational therapists in Victoria, Australia. Aust Occup Ther J. 59(1):17–22. doi:10.1111/j.1440-1630.2011.00966.x.
- Bilston LE, Brown J, Kelly P. 2005. Improved protection for children in forward-facing restraints during side impacts. Traffic Inj Prev. 6(2):135–146. doi:10.1080/15389580590931608. PMID: 16019399.
- Black MH, Hayden-Evans M, McGarry S, Lindner H, Clarkson E, Vale L, Picen T, Kuzminski R, Falkmer T. 2023. Safe transport of children with disabilities and medical conditions: caregiver experiences. Scand J Occup Ther. 30(8):1383–1393. doi:10.1080/11038128.2023.2210801.
- Bohman K, El-Mobader S, Jakobsson L. 2022. Effects of restraint parameters using PIPER 6y in reclined seating during frontal impact. Traffic Inj Prev. 23(sup1):S123–S129. doi:10.1080/15389588.2022.2125304. PMID: 36214799.
- Bull MJ. 2008. Safe transportation of children with special healthcare needs. Pediatr Ann. 37(9):624–631. doi:10.3928/00904481-20080901-02. PMID: 18795573.
- Bull MJ, Engle WA, American Academy of Pediatrics. Committee on Injury, Violence, and Poison Prevention and Committee on Fetus and Newborn, American Academy of Pediatrics. 2009. Safe transportation of preterm and low birth weight infants at hospital discharge. Pediatrics. 123(5):1424–1429. doi:10.1542/peds.2009-0559.
- Carmen S, Irvine H, Goman H. 2021. Travel and positioning after orthopaedic surgery. Allied Health Telehealth Virtual Education, NSW Children’s Healthcare Network.
- Chen X, Czubernat K, Zanettin L, Bondy M, Altenhof W, Snowdon A, Vrkljan B. 2014. Restraint device for airway management in low-birthweight infants. Int J Crashworthiness. 19(5):431–445. doi:10.1080/13588265.2014.909623.
- Cook L, Bilston L, Whyte T. 2024. Modifications to child restraints for children with disabilities – Experiences of Australian caregivers and health professionals. JRS. 35(1):1–14. doi:10.33492/JRS-D-24-1-2126682.
- Czubernat K, Chen X, Bondy M, Altenhof W, Snowdon A, Vrkljan B. 2014. Crash performance of a preemie positioning device to enhance infant safety in vehicles. Int J Crashworthiness. 19(6):588–599. doi:10.1080/13588265.2014.927657.
- Downie A, Chamberlain A, Kuzminski R, Vaz S, Cuomo B, Falkmer T. 2019. Road vehicle transportation of children with physical and behavioral disabilities: a literature review. Scand J Occup Ther. 27(5):309–322. doi:10.1080/11038128.2019.1578408.
- Du W, Finch CF, Hayen A, Bilston LE, Brown J, Hatfield J. 2010. Relative benefits of population-level interventions targeting restraint-use in child car passengers. Pediatrics. 125(2):304–312. doi:10.1542/peds.2009-1171. PMID: 20064863.
- Eurostat. 2020. Health statistics - children. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Health_statistics_-_children#Disability_.28activity_limitations_due_to_health_problems.29.
- Falkmer T, Gregersen NP. 2001. A questionnaire-based survey on road vehicle travel habits of children with disabilities. IATSS Res. 25(1):32–41. doi:10.1016/S0386-1112(14)60004-2.
- Falkmer T, Gregersen NP. 2002. Perceived risk among parents concerning the travel situation for children with disabilities. Accid Anal Prev. 34(4):553–562. doi:10.1016/s0001-4575(01)00053-7.
- Górniak A, Matla J, Górniak W, Magdziak-Tokłowicz M, Krakowian K, Zawiślak M, Włostowski R, Cebula J. 2003. Influence of a passenger position seating on recline seat on a head injury during a frontal crash. Sensors (Basel). 22(5):5. PMID: 35271149. doi:10.3390/s22052003.
- Huang P, Kallan MJ, O’Neil J, Bull MJ, Blum NJ, Durbin DR. 2009. Children with special health care needs: patterns of safety restraint use, seating position, and risk of injury in motor vehicle crashes. Pediatrics. 123(2):518–523. doi:10.1542/peds.2008-0092. PMID: 19171617.
- Huot M, Brown J, Kelly P, Bilston LE. 2005. Effectiveness of high back belt positioning booster seats in side impacts. Traffic Inj Prev. 6(2):147–155. Jundoi:10.1080/15389580590931626. PMID: 16019400. PMID: 16019400.
- Lovette B. 2008. Safe transportation for children with special needs. J Pediatr Health Care. 22(5):323–328.e5. PMID: 18761235. doi:10.1016/j.pedhc.2008.05.002.
- Manary MA, Flannagan CAC, Reed MP, Orton NR, Klinich KD. 2019. Effects of child restraint misuse on dynamic performance. Traffic Inj Prev. 20(8):860–865. doi:10.1080/15389588.2019.1665177. PMID: 31670975.
- O’Neil J, Yonkman J, Talty J, Bull MJ. 2009. Transporting children with special health care needs: comparing recommendations and practice. Pediatrics. 124(2):596–603. doi:10.1542/peds.2008-1124. PMID: 19596733
- O’Neil J, Hoffman B, Agran PF, Denny SA, Hirsh M, Johnston B, Lee LK, Monroe K, Schaechter J, Tenenbein M, et al. 2019. Transporting children with special health care needs. Pediatrics. 143(5):1–7. PMID: 31010906. doi:10.1542/peds.2019-0724.
- Standards Australia & Standards New Zealand. 2013b. AS/NZS 4370: restraint of children with disabilities, or medical conditions, in motor vehicles. Standards Australia.
- Teerds S, Cameron T. 2015. Restraining children with disabilities or medical conditions safely. Australasian Road Safety Conference, Australia. https://trid.trb.org/view/1399465.
- US Census Bureau. 2019. Childhood disability in the United States: 2019. Census.gov. https://www.census.gov/library/publications/2021/acs/acsbr-006.html.
- Whyte T, Kent N, Griffiths M, Bilston LE, Brown J. 2021. Dynamic crash performance of old and used child restraint systems. Traffic Inj Prev. 22(7):570–575. PMID: 34432557. doi:10.1080/15389588.2021.1958208.
