
Abstract
Increasing physical activity (PA) is a complex and challenging task in patients with chronic obstructive pulmonary disease (COPD). However, some questions are raised regarding the evaluation of PA in these patients: Have all aspects of PA evaluation in patients with COPD already been explored in the scientific literature and clinical practice? What is the clinical importance of assessing PA inequality? PA inequality is defined as the Gini coefficient (Ginicoef) of the PA distribution of a population and is already shown to have implications for public health in the general population. It is a simple tool that might allow a better understanding of PA disparities among different COPD populations, although to our knowledge there is no previous investigation of PA inequality in patients with COPD using the Ginicoef. In this perspective study we have provided examples of the Ginicoef use in different scenarios. Future studies might try to apply it in order to identify subpopulations with higher PA inequality, and perhaps are therefore more prone to benefit most from interventions specifically tailored to promote PA. In summary, we propose the quantification of PA inequality with the Ginicoef as a tool that might allow us to see PA even more comprehensively than we already do, expanding our perspective on PA in patients with COPD.
Perspective
There is clear evidence that regular physical activity (PA) is recommended for patients with chronic obstructive pulmonary disease (COPD) [Citation1,Citation2], since physical inactivity and sedentary behavior are associated with higher rates of death and exacerbations [Citation1,Citation3]. However, some questions are raised regarding the evaluation of PA in patients with COPD: Have all aspects of PA evaluation in patients with COPD already been explored in the scientific literature and clinical practice? What is the clinical importance of assessing PA inequality? This paper aims to bring some light on the importance of the assessment of PA inequality in patients with COPD.
Review of relevant literature
PA is essential to prevent and manage chronic diseases, especially in older people. However, data from the National Health and Nutrition Examination Survey (NHANES) showed that only 27% of older adults meet the recommended PA guidelines [Citation4]. Patients with COPD present even lower levels of PA when compared to healthy subjects with the same age and sex. For example, previous studies have shown that patients with moderate-severe COPD reached 30–50% lower number of steps/day [Citation5] as well as spent 50% lower walking time/day and 3 times higher lying time during the day [Citation6] when compared to matched controls. This scenario of physical inactivity impact on other important clinical outcomes, leading to increased rates of exacerbations and death [Citation1,Citation3]. Therefore, improving PA has become of great interest in these patients, with different forms of interventions being studied, such as the creation of telecoaching programmes and urban trails in outdoor public spaces specifically for COPD patients [Citation7,Citation8]. A recent study systematically reviewed a diverse range of interventions, including pulmonary rehabilitation, high-intensity interval exercise training, self-management strategies, nutritional supplementation, noninvasive ventilation and pharmacological treatments, among others [Citation9]. The objective of the review was to evaluate which types of interventions are effective to improve objectively-assessed PA in daily life, also known as PADL. However, after evaluating more than 8,000 patients with COPD from different places and undergoing different interventions, the authors could not reach a verdict, neither regarding which is the best intervention to improve PADL nor regarding what is needed to improve PA in the long term.
This reasoning leads to the following question: Have all aspects of PA evaluation in patients with COPD already been explored in the scientific literature and clinical practice? One potential and still underexplored aspect is the disparity in PA among different COPD populations and profiles. A few previous studies have touched upon this aspect. For instance, patients from Central Europe and Belgium presented a significantly lower PADL than patients from South America, although they were carefully matched for several potential influencing factors such as age, disease severity, body mass index, exercise capacity and season [Citation10,Citation11]. Differences in PADL were also found in rural versus urban populations, with evidence showing that COPD patients from rural areas reported to spend less time in sedentary behavior, although the proportion of regular exercise practice was higher in patients from urban areas [Citation12]. Furthermore, Watz et al. [Citation13] showed considerable disparities in PA level (assessed by different PA variables) among GOLD stages and BODE scores. However, although PA level in patients with COPD is quite heterogeneous among populations and profiles, there is a lack of studies that take into account in what way these disparities are characterized. We hypothesized that these gaps can be filled with a measurement that takes into consideration different populations at the same time. The Ginicoef is a measurement of groups of individuals that is being proposed to assess the distribution of PA (i.e. PA inequality) in patients with COPD.
The gini coefficient to measure physical activity inequality
The Ginicoef is the most common method to measure inequality, and is widely used to quantify poverty and income distribution [Citation14]. It was also already shown to be an important tool to quantify disparities in PA in the general population [Citation15]. For instance, individuals from countries with higher PA inequality were more likely to be obese than individuals from countries with lower PA inequality, and the prevalence of obesity increased more for females as PA decreased. In other words, PA inequality was considered a better predictor of obesity than the average activity level for the general population [Citation15].
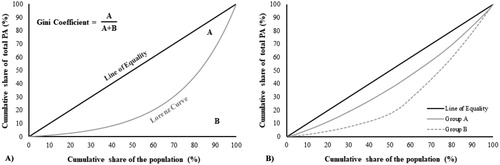
Inequality itself can be defined as the Ginicoef of any distribution of a population; in the case of PA, its calculation requires only the total number of individuals and a given PA variable, such as the number of steps taken by each individual of that population. The Ginicoef ranges from 0 to 1 and can be calculated using formulas (available in the supplementary spreadsheet file) or statistical packages (such as R and Stata) [Citation16,Citation17]. The calculation of the Ginicoef is based on the Lorenz curve, illustrated in , where the x axis represents the cumulative percentage of the population and the y axis represents the cumulative percentage of the share of the population’s total average steps per day. A completely “equal” population would be represented if the first 10% of the population walked 10% of total steps, the first 50% of the population walked 50% of total steps, and so on. In this case, the Lorenz curve would be a diagonal line with 45 degrees (Ginicoef = zero, or complete equality). As inequality occurs, the Lorenz curve deviates from the line of equality, with the highest possible value of the Ginicoef of 1 (or complete inequality). The calculation of the Ginicoef is equal to the ratio of the area that lies between the line of equality and the Lorenz curve (area A) by the total area under the line of equality (area A + B). With this measurement, it is possible to compare PA inequality of different populations. The further the Lorenz curve deviates from the line of equality, the higher the Ginicoef and, consequently, the higher the population inequality. We will now provide an example, and for better understanding, we suggest to follow the reading of this example along with the supplementary spreadsheet file. Example: supposing there are two different populations of patients with COPD (populations A and B), both with the same average number of steps/day. However, for population A the first 10% of the patients walked 5% of total steps, and the first 50% of the population walked 36% of total steps, resulting in inequality of the PA with the Lorenz curve deviating from the line of equality (). As for population B, the first 10% of the patients walked approximately 2% of total steps, and the first 50% of the population walked 17% of total steps. In this case, the Lorenz curve of the population B deviated more from the line of equality than population A (also shown in ). In other words, half of population A walked 36% of total number of steps of population A, whereas half of the population B walked only 17% of total number of steps of population B, highlighting its higher PA inequality. Therefore, although populations A and B have similar average number of steps, the discrepancies in the distribution of PA might help to understand particularities of the populations, enabling more targeted interventions.
Figure 1. Illustration of physical activity inequality definition and an example with real data. 1A) The graph represents the cumulative percentage of the population on the x axis and the cumulative percentage of the share of the population’s total physical activity (e.g. steps/day) on the y axis. The diagonal line (line of equality) represents complete equality and the gray line represents the Lorenz curve. The Gini coefficient is calculated as the ratio of the area that lies between the line of equality and the Lorenz curve (A) by the total area under the line of equality (A + B). The further the Lorenz curve lies from the diagonal line, the higher the inequality. 1B) Representation of the Lorenz curves from two groups of patients with COPD. Group A: n = 78, Ginicoef: 0.190; Group B: n = 78, Ginicoef: 0.396 (data used to construct the curves are available in the supplementary spreadsheet file).
Of note, the Ginicoef can be calculated using any PA variable, but we have used steps/day in our examples because it is a simple unit of locomotion, easy to understand and that can be objectively measured with wearable devices such as accelerometers, step counters (or pedometers) and by the increasingly used PA trackers, watches and smartphones. However, caution is necessary about the accuracy of such devices since they may underestimate the number of steps in patients with COPD, especially in severe disease [Citation9,Citation18] as well as in any slow-walking population. It is important to consider manufacturer’s instructions, such as the position of the devices, as well as international recommendations to standardize PA measurement [Citation19] and future investigations on accuracy. The better the precision to characterize PA, the better the understanding of its relationship with COPD severity and inequality.
How can this be used in a clinical approach?
Despite the extensive literature on PA with several different types of intervention, changing (and maintaining) PA habits in daily life is recognizably very challenging in patients with COPD [Citation9,Citation20]. The quantification of PA inequality could be an added feature: the Ginicoef may be related to other important characteristics and can help identifying subpopulations who could benefit most from interventions to promote PA, such as women (as previously shown in a nonspecific COPD study [Citation15]). For instance, considering that one will implement a public health program aiming to promote PA in patients with COPD. There is great probability that this health program will involve different subpopulations, such as patients from urban versus rural communities, or patients with low or high symptom burden, for example. We believe that the evaluation of PA inequality may reveal differences in the PA distribution, contributing to a better interpretation of the results beyond the average number of steps. With this information, one could identify poor PA subgroups who could benefit from tailored interventions, leading to a more equally distributed group regarding PA.
Now considering that one is comparing two different strategies to promote PA in patients with COPD and both were able to achieve the same average activity level at the end (e.g. > 7500 steps/day). The Ginicoef can be used to evaluate if one intervention presented a higher PA inequality than the other (as previously exemplified in ). It may be reasoned that the intervention with lower PA inequality can be preferable, since it would mean that this intervention resulted in a more equal distribution of PA. Further on, a promising next step would be to investigate PA inequality in different groups of patients with COPD as well as among different countries and regions across the globe. In this way, it might be possible to move from studying groups of patients in isolation to studying groups of patients simultaneously, enabling a more comprehensive understanding of the determinant factors of PA, while also considering the characteristics from different populations.
Future studies are certainly needed to confirm the usefulness of the Ginicoef in patients with COPD, so we invite you to take a look at the PA inequality of your patients. A better understanding of the scenario might help defining the real applicability(ies) of this new approach in the proposed context. In summary, we believe that the quantification of PA inequality with the Ginicoef is a simple tool that might allow us to see PA even more comprehensively than we already do, expanding our perspective on PA in patients with COPD.
Supplemental online material
A spreadsheet file is available for download with further explanations about how the Gini coefficient can be calculated as well as an example with real data.
Supplemental Material
Download MS Excel (43.4 KB)Acknowledgements
RPH, JMO, LPS, MPB, AR, LCM, FP and KCF were supported by individual grants from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) or Fundação Nacional do Desenvolvimento do Ensino Superior Particular (FUNADESP).
Disclosure statement
The authors report no conflict of interest.
Additional information
Funding
References
- Watz H, Pitta F, Rochester CL, et al. An official European Respiratory Society statement on physical activity in COPD [Research Support, Non-U.S. Gov't]. Eur Respir J. 2014;44(6):1521–1537. DOI:10.1183/09031936.00046814
- Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2018 Report 2018 [cited 2018]. Available from: www.goldcopd.org.
- Gimeno-Santos E, Frei A, Steurer-Stey C, PROactive consortium, et al. Determinants and outcomes of physical activity in patients with COPD: a systematic review. Thorax. 2014;69(8):731–739. DOI:10.1136/thoraxjnl-2013-204763
- Keadle SK, McKinnon R, Graubard BI, et al. Prevalence and trends in physical activity among older adults in the United States: a comparison across three national surveys. Prev Med. 2016;89:37–43. DOI:10.1016/j.ypmed.2016.05.009
- Troosters T, Sciurba F, Battaglia S, et al. Physical inactivity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005–1011. DOI:10.1016/j.rmed.2010.01.012
- Pitta F, Troosters T, Spruit MA, et al. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972–977. DOI:10.1164/rccm.200407-855OC
- Arbillaga-Etxarri A, Gimeno-Santos E, Barberan-Garcia A, et al. Long-term efficacy and effectiveness of a behavioural and community-based exercise intervention (Urban Training) to increase physical activity in patients with COPD: a randomised controlled trial. Eur Respir J. 2018;52(4):1800063. DOI:10.1183/13993003.00063-2018
- Demeyer H, Louvaris Z, Frei A, et al. Physical activity is increased by a 12-week semiautomated telecoaching programme in patients with COPD: a multicentre randomised controlled trial. Thorax. 2017;72(5):415–423. DOI:10.1136/thoraxjnl-2016-209026
- Burge AT, Cox NS, Abramson MJ, et al. Interventions for promoting physical activity in people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2020;4:CD012626. DOI:10.1002/14651858.CD012626.pub2
- Furlanetto KC, Demeyer H, Sant'anna T, et al. Physical activity of patients with COPD from regions with different climatic variations. COPD. 2017;14(3):276–283. DOI:10.1080/15412555.2017.1303039
- Pitta F, Breyer MK, Hernandes NA, et al. Comparison of daily physical activity between COPD patients from Central Europe and South America. Respir Med. 2009;103(3):421–426. DOI:10.1016/j.rmed.2008.09.019
- Yan R, Wang Y, Bo J, et al. Healthy lifestyle behaviors among individuals with chronic obstructive pulmonary disease in urban and rural communities in China: a large community-based epidemiological study. COPD. 2017;12:3311–3321. DOI:10.2147/COPD.S144978
- Watz H, Waschki B, Meyer T, et al. Physical activity in patients with COPD. Eur Respir J. 2009;33(2):262–272. DOI:10.1183/09031936.00024608
- De Maio FG. Income inequality measures. J Epidemiol Community Health. 2007;61(10):849–852. DOI:10.1136/jech.2006.052969
- Althoff T, Sosic R, Hicks JL, et al. Large-scale physical activity data reveal worldwide activity inequality. Nature. 2017;547(7663):336–339. DOI:10.1038/nature23018
- Wright Muelas M, Mughal F, O'Hagan S, et al. The role and robustness of the Gini coefficient as an unbiased tool for the selection of Gini genes for normalising expression profiling data. Sci Rep. 2019;9(1):17960. DOI:10.1038/s41598-019-54288-7
- Tourani S, Zarezadeh M, Raadabadi M, et al. Association of regional disparity of obstetrics and gynecologic services with children and infants mortality rates: a cross-sectional study. Int J Reprod Biomed (Yazd). 2017;15(3):147–154. DOI:10.29252/ijrm.15.3.147
- Nolan CM, Maddocks M, Canavan JL, et al. Pedometer step count targets during pulmonary rehabilitation in chronic obstructive pulmonary disease. A randomized controlled trial. Am J Respir Crit Care Med. 2017;195(10):1344–1352. DOI:10.1164/rccm.201607-1372OC
- Demeyer H, Burtin C, Van Remoortel H, et al. Standardizing the analysis of physical activity in patients with COPD following a pulmonary rehabilitation program. Chest. 2014;146(2):318–327. DOI:10.1378/chest.13-1968
- Cindy Ng LW, Mackney J, Jenkins S, et al. Does exercise training change physical activity in people with COPD? A systematic review and meta-analysis. Chron Respir Dis. 2012;9(1):17–26. DOI:10.1177/1479972311430335