
Abstract
Leukotriene A4 hydrolase (LTA4H) is associated with inflammation and emphysema. Nevertheless, clinical implications of LTA4H genetic polymorphism in chronic obstructive pulmonary disease (COPD) has been understudied to date. A prospective study was performed to investigate the clinical implications of LTA4H genetic polymorphism in patients with COPD. AA, GA, and GG types of genetic polymorphism of LTA4H were assayed in patients with COPD at the baseline. Then all patients were followed up for 12 months. At the baseline, the number of participants with AA, GA, and GG type of LTA4H rs7971150 were 22 (14.2%), 43 (27.7%), and 90 (58.1%) in the COPD group (n = 155), whereas 55 (36.7%), 38 (25.3%), and 57 (38.0%) in the control group (n = 150) (p = 0.001). During the follow-up, the variations with respect to forced expiratory volume in one second (FEV1), 6 min walking distance (6MWD), and BODE (body-mass index, obstruction, dyspnea, and exercise capacity) were similar between patients with AA and GA types, which were both lower than those of GG type. The patients with GG type had more hospitalizations than patients with AA (p = 0.001) and GA (p = 0.001) types, respectively. The cumulative hospitalization-free rate in patients with GG type was lower than those of patients with AA and GA types, respectively (p = 0.019). Compared with COPD patients with AA and GA types, patients with GG type were positively correlated with smoking, more hospitalizations, worse FEV1, 6MWD, and BODE index. The current study suggests that GG type of LTA4H is a predisposing factor in COPD development, functional decline, and exacerbation of patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, killing more than 3 million people every year. It is estimated to result in an expected death of 4.4 million yearly by 2040. COPD afflicts people in low-income, middle-income, and wealthy countries with a worldwide prevalence of 10.1% [Citation1,Citation2]. In China, the prevalence of COPD was 13.7% in people aged 40 years or older [Citation3]. Tobacco smoking is the main cause of COPD globally [Citation1–3].
Leukotriene A4 hydrolase (LTA4H) is a bifunctional enzyme which possesses both proinflammatory and anti-inflammatory functions. LTA4H can be converted to the proinflammatory mediator and neutrophil attractant leukotriene B4 (LTB4) which promotes the pathogenesis of pulmonary emphysema [Citation4], by epoxide hydrolase site catalyzation. Meanwhile, LTA4H has aminopeptidase activity that degrades proline-glycine-proline (PGP) which is a neutrophil chemoattractant tripeptide playing a significant role in the chronic neutrophilic inflammatory response, resulting in the resolution of inflammation [Citation5,Citation6].
In one study, LTA4H rs1978331 (intron 11) may have a modest effect on lung function parameters of smokers [Citation7]. In patients with COPD, tobacco smoking exposure facilitates the development of smoking-induced emphysema by inhibiting the enzymatic activities of the LTA4H aminopeptidase in lung tissues and accumulating PGP as well as neutrophils in airspace [Citation8]. For patients with COPD, once chronic inflammation is established, the changes to LTA4H aminopeptidase persist, even in the absence of subsequent tobacco exposure [Citation9]. In the study of Szul et al., two candidate single-nucleotide polymorphisms (SNPs), rs17025122 (4.1 kb) (p = 1.46 × 10−147) and rs7971150 (5.4 kb) (p = 2.06 × 10−49), are strongly associated with LTA4H expression in vivo. rs17025122 is located at the site 4.1 kilobase from the start site of ATG initiation codon, whereas rs7971150 is located at the site 5.4 kilobase from the start site of ATG initiation codon [Citation10]. Accordingly, genetic polymorphism of LTA4H may have clinical implications in patients with COPD. Nevertheless, the definite clinical implications of LTA4H genetic polymorphism in COPD has been understudied to date. Thus, the current study was designed to explore this topic.
Methods
Study design
Study protocol
A prospective study was performed to investigate the clinical implications of LTA4H genetic polymorphism in patients with COPD. Patients with stable COPD were enrolled as COPD group. In line with the age, sex, and smoking status of patients in the COPD group, approximately same number of healthy subjects with normal pulmonary function were enrolled as control group. Genetic polymorphism of LTA4H was compared between patients with COPD and healthy controls. Pulmonary function and BODE (body-mass index, obstruction, dyspnea, and exercise capacity) index were measured for patients in the COPD group at the baseline. Dyspnea was assessed by using a modified medical research council (MMRC) dyspnea scale. Exercise capacity was assessed by using a 6 min walking distance (6MWD) test [Citation11]. According to the GOLD (Global Initiative for Chronic Obstructive Lung Disease), COPD grouping was determined based on pulmonary function test (PFT), MMRC score and previous exacerbation and/or hospitalization events [Citation12]. Then the COPD group was followed up for 12 months. All the patients in the COPD group received routine treatment of COPD strictly following the recommendations of the GOLD [Citation12]. Number of hospitalizations and death due to acute exacerbation of COPD (AECOPD) in each month were inquired by phone and documented during the follow-up period. The cumulative hospitalization and survival rates during 12-month follow-up were compared among subgroups with different genetic polymorphism of LTA4H in the COPD group. At the 12-month follow-up visit, mandatory PFT, BODE index, and COPD grouping were remeasured. In case a patient was at the state of AECOPD at the 12-month follow visit, the measurement of the aforementioned variables was postponed till the state of patient was stable. The variations of clinical variables and hospitalizations from baseline through 12-month follow-up visit were compared among subgroups with different genetic polymorphism of LTA4H in the COPD group. The variations of the aforementioned variables were defined as the variable at the follow-up visit minus those at the baseline. The correlation between different genetic polymorphism of LTA4H and age, sex, smoking, FEV1 (forced expiratory volume in one second), MMRC, 6MWD, BODE, hospitalizations and deaths during 12-month follow-up were analyzed for all patients in the COPD group.
Gene detection
Genetic polymorphism of LTA4H rs7971150 [Citation10] was assayed in the current study. The upstream and downstream primer sequence of rs7971150 was 5′-GA CT CC TGG TCTC AGT TG GGT GA-3 ′ and 5′- TC CCT TG GAT TGT ATG CCA AA AA-3 ′, respectively. The sequence of linkage primers was rs 79 71 15 0R G: 5’T CTC TC GGG TCA ATT CG TC CT TT GA AG GAT TT TAA GCA GGG GAG TG AC AC-3 ′, rs 79 71 15 0 RA: 5′-TG TTC GTG GGC CG GA TT AG TT GA AG GA TT TTA AG CA GG GG AG TG AC AT-3 ′, and rs 79 71 150 RP: 5′-GA TTA CA TT AGA AAG AAT GCT CTA GC AG AT AA CA-3′, respectively. The genotypes of rs7971150 locus were divided into wild-type (AA), mutant heterozygous (GA) and mutant homozygous (GG). Four milliliters of fastening peripheral venous blood of all subjects were collected in the morning and placed in the ethylene diamine tetraacetic acid (EDTA) anticoagulant tube. Then deoxyribonucleic acid (DNA) was extracted and stored in the refrigerators at −20 °C. Improved multiple ligase detection reaction (imLDR) multi-ligase SNP typing kit (Shanghai Tianhao Biological Technology Co., Ltd) was adopted to determine the genetic polymorphism of LTA4H rs7971150.
Experimental design and operation instructions
The region where the target SNP is located was amplified in one system using multiple polymerase chain reaction (PCR) reaction. Amplified products were purified by exonuclease I and shrimp alkaline phosphatase (ExoI/SAP), then used as templates for subsequent ligase reactions. In a ligation reaction, each site contained two 5′-terminus allele-specific probes and an immediately following fluorescent allele-specific probe at 3′-terminus. The linkage products were distinguished by capillary electrophoresis with ABI3730XL.
Specific experimental operation steps
One microliter (µL) of 1% agarose electrophoresis was used for quality check and concentration estimation for DNA samples, then the samples were diluted to the working concentration of 5–10 nanogram (ng)/µL according to the estimated concentration. Then the next step was multiple PCR reaction. The reaction system (20 µL) in PCR consisted of 2× GCbuffer (Takara.), 3.0 mm (mM) of magnesium (Mg)2+, 0.3 mM of deoxy-ribonucleoside triphosphate (dNTP), 1 U of HotStarTaq Polymerase (Qiagen Inc.), 1 µL of sample DNA, and 1 µL of multiple PCR primer. Then the next step was the purification of multiple PCR products. 5 U of SAP enzyme and 2 U of exonuclease I enzyme were added to 20 µL of PCR product at 37 °C for 1 h and then were inactivated at 75 °C for 15 min. Then the next step was the connection reaction. The reaction system consisted of 1 µL of 10× linkage buffer, 0.25 µL of high temperature ligase, 0.4 µLof 5′ linkage primer mixture (1 micrometer [µM]), 0.4 µL of 3′ linkage primer mixture (2 µM), 2 µL of purified multiple PCR products, and 6 µL of mixed double distilled H2O (ddH2O). Then 0.5 µL of diluted linkage products mixed with 0.5 µL of Liz500 SIZE STANDARD and 9 µL of highly deionized formamide (Hi-Di) were denatured at 95 °C for 5 min. Finally, the linkage products were put on ABI3730XL sequencer.
Ethics
The current study was undertaken by the investigators of Shanghai Punan Hospital, North Bund Community Health Center, and Shanghai Xinhua Hospital. All authors vouch for the completeness and accuracy of the data. No one who is not an author contributed to the writing of the manuscript. All enrolled participants signed the informed consent forms. The study protocol was approved by the ethics committee of Shanghai Punan Hospital (No. 20170704).
Study population
The participants were enrolled as per the inclusion and exclusion criteria. The inclusion criteria comprised: 1) all eligible patients were 18 years old or older; 2) all eligible patients had a confirmed diagnosis of COPD according to the GOLD. As per the diagnostic criteria of COPD in the GOLD, COPD was diagnosed if patients had dyspnea, chronic cough, or sputum production, and/or a history of exposure to risk factors for COPD, and the presence of a post-bronchodilator FEV1/FVC (forced vital capacity) <0.70 [Citation12]; and 3) all eligible patients with COPD were at stable state when they were enrolled. The exclusion criteria comprised: 1) patients with asthma, bronchiectasis, tuberculosis, obliterative bronchiolitis, and diffuse panbronchiolitis; 2) patients with end-stage COPD and/or comorbidities who were expected to survive less than one year; 3) pregnant patients with COPD; and 4) patients with cognitive disorder who were unable to cooperate with investigation.
Statistical analyses
Based on the worldwide prevalence of 10.1% for COPD, to ensure a confidence level of 95% that the real value was within ±5% of the measured value, a total of 140 patients with COPD was the minimum number of necessary samples to meet the desired statistical constraints. In consideration of an estimated 10% loss to follow-up, eventually an estimated number of 154 or more patients were needed to be investigated.
Measurement data were presented as mean ± standard deviation or median with interquartile range based on whether or not they were in normal distribution. Categorical data were presented as percentages. T-test or ANOVA (analysis of variance) was used for comparison among groups. Hardy–Weinberg equilibrium law was used to evaluate the population representation of the samples (p > 0.05 denoted statistical significance). The genotype frequency and allele frequency of each locus were counted by using direct counting methods. The genotype frequency and allele frequency were compared by using Chi-square test. The time-to-event cumulative hospitalization and survival rates during 12-month follow-up compared among subgroups with different genetic polymorphism of LTA4H in the COPD group were performed by using Kaplan–Meier method. The correlation between genetic polymorphism of LTA4H and PFT, BODE, hospitalizations, as well as deaths during 12-month follow-up were analyzed by using univariate and multivariate Cox regression analyses. SPSS 28 was used for the statistical analysis. Statistical significance was defined as a p value being less than 0.05.
Results
Demographics and characteristics of participants at the baseline
From September 2017 through January 2020, as per the inclusion criteria, 183 patients with COPD of Shanghai Punan Hospital and North Bund Community Health Center were included. After the exclusion of 20 patients with asthma, bronchiectasis, tuberculosis, obliterative bronchiolitis, as well as diffuse panbronchiolitis, 5 patients with end-stage COPD and/or comorbidities who were expected to survive less than one year, 1 pregnant patient with COPD, and 2 patients with cognitive disorder who were unable to cooperate with investigation, a total of 155 patients finally were enrolled into the COPD group. After the matching of age, sex, and smoking status of patients in the COPD group, 150 healthy subjects with normal pulmonary function were enrolled into the control group. After the 12-month follow-up for the COPD group, 4 patients were lost to the follow-up, 5 patients died due to AECOPD, whereas 146 patients finished the whole study. The demographics and characteristics of participants at the baseline are summarized in . Study roadmap is demonstrated in .
Figure 1. Study roadmap. One hundred and eighty-three patients with COPD were included. After the exclusion of 28 patients, a total of 155 patients finally were enrolled into the COPD group. Meanwhile, 150 healthy subjects with normal pulmonary function were enrolled into the control group. Genetic polymorphism of LTA4H between COPD and control groups was compared at the baseline. After 12-month follow-up for the COPD group, 4 patients were lost to the follow-up, 5 patients died due to AECOPD, whereas 146 patients finished the whole study. Clinical variables variation and hospitalizations during follow-up were compared among COPD subgroups with different genetic polymorphism of LTA4H. Cumulative one-year hospitalizations and deaths were compared among COPD subgroups with different genetic polymorphism of LTA4H. Correlation between genetic polymorphism of LTA4H and clinical characteristics during follow-up were analyzed. Note: COPD, chronic obstructive pulmonary disease; AECOPD, acute exacerbation of chronic obstructive pulmonary disease.
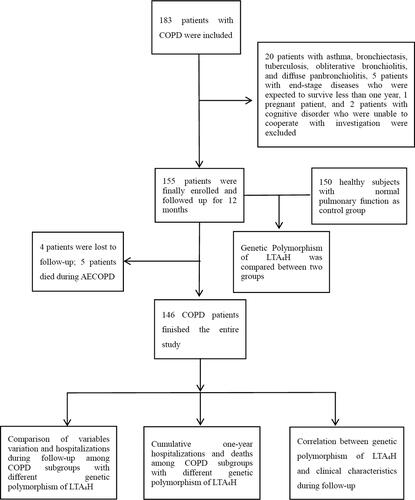
Table 1. Demographics and characteristics of participants at the baseline.
Comparison of genetic polymorphism of LTA4H between COPD patients and controls at the baseline
At the baseline, the number of participants with AA, GA, and GG types of genetic polymorphism of LTA4H were 22 (14.2%), 43 (27.7%), and 90 (58.1%) in the COPD group, whereas 55 (36.7%), 38 (25.3%), and 57 (38.0%) in the control group (p = 0.001). The prevalence of AA type in the COPD group was lower than that of the control group, whereas the prevalence of GG type in the COPD group was higher than that of the control group. No difference with respect to the GA type was found between two groups ().
Comparison of clinical variables variation and hospitalizations during follow-up among COPD subgroups with different genetic polymorphism of LTA4H
Four patients with COPD were lost, whereas five ones died during the follow-up. Among nine of them, two patients were with AA type of LTA4H, another two were with GA type, whereas the rest five were with GG type. Accordingly, 20 COPD patients with AA type of LTA4H, 41 ones with GA type, and 85 ones with GG type finished the entire study.
Except for MMRC, the variations during the follow-up with respect to FEV1, 6MWD, and BODE were similar between patients with AA and GA type, which were both lower than those of GG type. During the follow-up, the patients with GG type had more hospitalization episodes than patients with AA (p = 0.001) and GA (p = 0.001) types, respectively. The COPD patients with GG type presented with the worst functional decline and the most exacerbation in term of the degree of airflow obstruction, exercise capacity and hospitalization episodes ().
Table 2 Comparison of clinical variables variation and hospitalizations during follow-up among COPD subgroups with different genetic polymorphism of LTA4H
Cumulative one-year hospitalizations and deaths among COPD subgroups with different genetic polymorphism of LTA4H
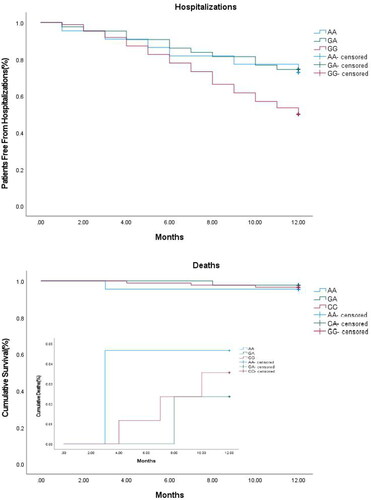
Apart from 4 patients who were lost to the follow-up, for 151 patients with COPD, cumulative one-year hospitalizations and survival rates were compared among patients with AA (n = 21), GA (n = 42) and GG (n = 88) types. The results demonstrated that the time-to-event cumulative hospitalization-free rate in patients with GG type was lower than those of patients with AA and GA types, whereas no difference was found between patients with AA, and GA types (p = 0.019) (Panel A, ). No difference was found with respect to time-to-event cumulative survival rate among patients with AA, GA, and GG types (p = 0.879) (Panel B, )
Figure 2 Cumulative one-year hospitalizations and deaths among COPD subgroups with different genetic polymorphism of LTA4H. The time-to-event cumulative hospitalization-free rate in patients with GG type is lower than those of patients with AA and GA types, whereas no difference is found between patients with AA, and GA types (P = 0.019) (Panel A). No difference is found with respect to time-to-event cumulative survival rate among patients with AA, GA, and GG types (P = 0.879) (Panel B). Note: COPD, chronic obstructive pulmonary disease; LTA4H, Leukotriene A4 hydrolase; AA, wild-type; GA, mutant heterozygous; GG, mutant homozygous.
Correlation between genetic polymorphism of LTA4H and clinical characteristics during follow-up
After a univariate followed by a multivariate Cox regression analysis, the results demonstrated that age, sex, MMRC, and mortality were not correlated with genetic polymorphism of LTA4H.
In contrast with AA type, the hazard ratio of GG type with respect to smoking status, smoking index, FEV1 volume, FEV1 percentage, 6MWD, BODE, and hospitalizations were (2.653, p < 0.001), (1.743, p = 0.015), (2.324, p = 0.001), (2.246, p = 0.001), (2.156, p = 0.001), (2.774, p < 0.001), and (2.301, p = 0.001).
In contrast with GA type, the hazard ratio of GG type with respect to smoking status, FEV1 volume, FEV1 percentage, 6MWD, BODE, and hospitalizations were (2.454, p < 0.001), (2.276, p = 0.001), (2.457, p = 0.001), (2.016, p = 0.005), (2.412, p < 0.001), and (2.152, p = 0.001) ().
Table 3 Correlation between genetic polymorphism of LTA4H and clinical characteristics during follow-up
Discussion
The results of the current study suggested that patients with COPD had more GG type and less AA type of LTA4H rs7971150, in contrast with healthy controls. The COPD patients with GG type of LTA4H rs7971150 showed the worst functional decline and the most exacerbation in term of airflow obstruction, exercise capacity, and hospitalization episodes in a 12-month follow-up. The time-to-event cumulative hospitalization-free rate in COPD patients with GG type was lower than those of patients with AA and GA types, whereas no difference was found with respect to time-to-event one-year cumulative survival rate among patients with AA, GA, and GG types. In contrast with COPD patients with AA and GA types, patients with GG type were positively correlated with smoking, more hospitalizations, worse FEV1, 6MWD, and BODE index.
To our best knowledge, the current study is the first one on such topic, since no comparable study has been identified to date. Accordingly, there is no way to compare the current study with previous ones. In previously relevant studies, LTA4H was a bifunctional enzyme in both proinflammatory and antiinflammatory ways. It may have a modest impact on pulmonary function of smokers. Inhibition of enzymatic activities of LTA4H aminopeptidase induced by tobacco smoking facilitated the development of emphysema even after the cessation of smoking [Citation4–9]. Based on the study of Szul et al. in which polymorphisms (SNPs) rs17025122 (4.1 kb) and rs7971150 (5.4 kb) (p = 2.06 × 10−49) are strongly correlated with LTA4H expression in vivo [Citation10], we chose both of them to reflect the polymorphisms of LTA4H. The parallel study with respect to rs17025122 is still underway.
In the current study, patients with COPD were prone to have more GG type and less AA type of LTA4H rs7971150, compared with controls. In addition, COPD patients with GG type of LTA4H were prone to have the worst decline of airflow obstruction and exercise capacity, as well as the most hospitalizations. GG type was positively correlated with smoking, more hospitalizations, worse FEV1, 6MWD, and BODE index. The results of the current study suggested that genetic polymorphism of LTA4H did have clinical implications in patients with COPD. It denoted that GG type of LTA4H may be regarded as a predisposing factor in COPD development, functional decline and exacerbation of patients with COPD.
The current study suffered from some limitations. First of all, the sample size of the current study was not spectacular. The results of the current study need to be validated in multi-center external large sample size prospective studies. Secondly, the comprehensive monitoring on the routine treatment of COPD during the follow-up was insufficient. Owing to potentially heterogeneous adherence of different patients, this may confound the one-year clinical outcome more or less.
In conclusion, the current study suggests that genetic polymorphism of LTA4H has clinical implications in patients with COPD. The GG type of LTA4H is a predisposing factor in COPD development, functional decline and exacerbation of patients with COPD. Such genetic polymorphism may help clinicians to assess the risk of COPD development, functional decline and exacerbation of COPD patients in clinical practice.
Ethics approval and consent to participate
The study protocol was approved by by the ethics committee of Shanghai Punan Hospital (No. 20170704).
Authors’ contributions
YFZ and WX were in full charge of the design and performance of the study, the analysis and interpretation of the data, and the writing of the manuscript. MX, ML, and QZ contributed more or less to the study design, data analysis and interpretation, and the writing of the manuscript. All authors have read and approved the final manuscript.
Consent for publication
Not applicable.
Acknowledgements
We are indebted to all the participants involved in this study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of interest
The authors declare no competing interests.
Additional information
Funding
References
- Celli BR, Wedzicha JA. Update on clinical aspects of chronic obstructive pulmonary disease. N Engl J Med. 2019;381(13):1257–1266. DOI:https://doi.org/10.1056/NEJMra1900500
- Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. DOI:https://doi.org/10.1016/S0140-6736(17)31222-9
- Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. DOI:https://doi.org/10.1016/S0140-6736(18)30841-9
- Shim YM, Paige M, Hanna H, et al. Role of LTB4 in the pathogenesis of elastase-induced murine pulmonary emphysema. Am J Physiol Lung Cell Mol Physiol. 2010;299(6):L749–L759. DOI:https://doi.org/10.1152/ajplung.00116.2010
- Snelgrove RJ, Jackson PL, Hardison MT, et al. A critical role for LTA4H in limiting chronic pulmonary neutrophilic inflammation. Science. 2010;330(6000):90–94. DOI:https://doi.org/10.1126/science.1190594
- Snelgrove RJ. Leukotriene A4 hydrolase: an anti-inflammatory role for a proinflammatory enzyme. Thorax. 2011;66(6):550–551. DOI:https://doi.org/10.1136/thoraxjnl-2011-200234
- Tulah AS, Parker SG, Moffatt MF, et al. The role of ALOX5AP, LTA4H and LTB4R polymorphisms in determining baseline lung function and COPD susceptibility in UK smokers. BMC Med Genet. 2011;12:173. DOI:https://doi.org/10.1186/1471-2350-12-173
- Paige M, Wang K, Burdick M, et al. Role of leukotriene A4 hydrolase aminopeptidase in the pathogenesis of emphysema. J Immunol. 2014;192(11):5059–5068. DOI:https://doi.org/10.4049/jimmunol.1400452
- Wells JM, O’Reilly PJ, Szul T, et al. An aberrant leukotriene A4 hydrolase-proline-glycine-proline pathway in the pathogenesis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;190(1):51–61. DOI:https://doi.org/10.1164/rccm.201401-0145OC
- Szul T, Castaldi P, Cho MH, et al. Genetic regulation of expression of leukotriene A4 hydrolase. ERJ Open Res. 2016;2(1):00058-2015. DOI:https://doi.org/10.1183/23120541.00058-2015
- Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. DOI:https://doi.org/10.1056/NEJMoa021322
- GOLD Science Committee Members (2020–2021). Global Initiative for Chronic Obstructive Lung Disease. Report: global strategy for prevention, diagnosis and management of COPD; 2021. https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.