
Abstract
Triple therapy for chronic obstructive pulmonary disease (COPD) is recommended for some patients, but the inhaled corticosteroids (ICS) may differ in effectiveness and safety. We compared budesonide-based and fluticasone-based triple therapy given in two inhalers on the incidence of exacerbation, mortality and severe pneumonia, using an observational study approach. We identified a cohort of patients with COPD, new users of triple therapy given in two inhalers during 2002–2018, age 50 or older, from the UK’s CPRD database, and followed for one year. The hazard ratio (HR) of exacerbation, all-cause death and pneumonia was estimated using the Cox regression model, weighted by fine stratification of the propensity score of treatment initiation. The cohort included 29,716 new users of fluticasone-based triple therapy and 9,646 of budesonide-based. The HR of a first moderate or severe exacerbation with budesonide-based triple therapy was 0.98 (95% CI: 0.94–1.03), relative to fluticasone-based, while for a severe exacerbation it was 0.97 (95% CI: 0.87–1.07). The incidence of all-cause death was lower with budesonide-based therapy among patients with no prior exacerbations (HR 0.80; 95% CI: 0.66–0.98). The HR of severe pneumonia with budesonide-based therapy was 0.84 (95% CI: 0.75–0.95). In a real-world clinical setting of COPD treatment, budesonide-based triple therapy given in two inhalers was generally as effective at reducing exacerbations as fluticasone-based triple therapy. However, the budesonide-based triple therapy was associated with a lower incidence of severe pneumonia and possibly also of all-cause death, especially among patients with no prior exacerbations for whom triple therapy is not recommended.
Supplemental data for this article is available online at https://doi.org/10.1080/15412555.2022.2035705 .
Introduction
The pharmacological treatment of chronic obstructive pulmonary disease (COPD) includes long-acting bronchodilators, namely long-acting muscarinic antagonists (LAMAs) and long-acting beta2-agonists (LABAs), as well as inhaled corticosteroids (ICS) recommended to be added with increasing disease severity [Citation1]. Triple therapy combining the three inhaler classes is now prevalent in the management of COPD [Citation2]. With this background, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) group emphasized the need for evidence on the effectiveness of triple therapy, particularly on major disease outcomes of COPD, including mortality [Citation1,Citation3].
Two large trials assessed the effectiveness and safety of single inhaler triple therapy (LAMA-LABA-ICS) compared with a dual bronchodilator (LAMA-LABA) in COPD on several major outcomes, including exacerbations, mortality and pneumonia. Indeed, the Informing the Pathway of COPD Treatment (IMPACT) and the Efficacy and Safety of Triple Therapy in Obstructive Lung Disease (ETHOS) trials suggest that the two triple therapies may have somewhat different effectiveness and safety profiles [Citation4,Citation5]. While there are no studies of the direct comparisons of different triple therapies, some studies of LABA-ICS inhalers reported that budesonide-based inhalers were associated with lower rates of exacerbation, hospitalization or pneumonia compared with fluticasone-based inhalers [Citation6–11]. Other studies found no differences on these outcomes between the two combined inhalers [Citation12,Citation13]. These studies, however, had methodological challenges, including the use of intent-to-treat analysis, which does not account for treatment duration and discontinuation, and no studies considered blood eosinophil counts, an important biomarker in COPD [Citation14].
We compared the effectiveness and safety of budesonide-based with fluticasone-based triple therapy given in two inhalers on exacerbation, mortality and severe pneumonia, using an observational study approach in a real world setting of clinical practice [Citation15,Citation16]. We examined these comparative effects according to history of asthma, prior exacerbations, and blood eosinophil levels.
Methods
Data source
The base cohort of patients was identified from the Clinical Practice Research Datalink (CPRD), a primary care database from the United Kingdom (UK) that contains primary care medical records for over 50 million people enrolled in more than 1,800 general practices. Participating general practitioners in the CPRD-GOLD and Aurum networks record medical information as part of the routine care of patients, including demographic data, lifestyle factors, medical diagnoses recorded using Read and SNOMED codes, and prescriptions. Over 85% of the CPRD practices can be linked to the Hospital Episodes Statistics (HES) database. The CPRD population is representative of the overall population and these data sources have been validated [Citation17–19]. The information on medications and diagnoses has been validated and shown to be of high quality, particularly for studies of COPD [Citation18–22]. This base cohort was used for previous studies of COPD treatment.
Study design
The source population included all patients with a diagnosis of COPD from January 1995 to November 2018 who subsequently received at least one prescription for a LAMA or a LABA (with or without ICS) after January 2002, the date when LAMAs became available. To increase the likelihood of a diagnosis of COPD, we excluded all patients less than 50 years of age on the date of their initial prescription for these long-acting bronchodilators. The source population was restricted to patients linkable to the Hospital Episodes Statistics (HES) database to obtain data on hospitalizations.
The study cohort was formed by identifying all subjects who received their first treatment with two-inhaler triple therapy, defined as a LAMA inhaler and a LABA-ICS single inhaler combination on the same day, from January 2002 until November 2018. Thus, the cohort included patients already treated with LAMA monotherapy who added a LABA-ICS and patients already treated with LABA-ICS monotherapy who added a LAMA inhaler. We excluded patients receiving ICS monotherapy prior to triple therapy initiation. The study was restricted to the most commonly used LABA-ICS inhalers, namely fluticasone-based or budesonide-based. All patients required at least one year of medical history prior to cohort entry, defined by the date of the first triple therapy prescription, to allow a baseline period to measure covariates and to identify new use of these study combinations.
We used an incident new-user cohort design to compare the initiators of budesonide-based with the initiators of fluticasone-based triple therapy inhalers, weighted by fine stratification weights computed using the probability of treatment propensity scores [Citation23–25]. Subjects in the study cohort were followed up for one year from cohort entry, or until death, 30 November 2018, or the end of the patient’s registration in the practice, whichever occurred first.
Outcome events
The effectiveness outcomes were the occurrence of a first moderate or severe COPD exacerbation during follow-up, of a severe exacerbation and of all-cause mortality. A severe exacerbation was defined as hospitalization with a primary diagnosis of COPD (ICD-10 J41-J44) while a moderate exacerbation by a new prescription for prednisolone. The safety outcome was the first severe pneumonia defined by a hospitalization for community-acquired pneumonia (ICD-10 J10.0, J11.0, J12-J18, J22, J69, J85.0, J85.1, J86). These diagnostic codes have been shown to have good accuracy and were used in several studies of COPD using the CPRD [Citation21,Citation22,Citation26–28].
Covariates
The covariates used to balance the two treatment groups included several factors identified using lifestyle, diagnoses and prescriptions from the CPRD and HES databases. The covariates thus included age, sex, body mass index (BMI), smoking status and excessive alcohol consumption, measured at or prior to cohort entry. The severity of COPD at treatment initiation was first measured by the number of prior COPD exacerbations, as well as the use of other respiratory drugs, identified during the one-year baseline period. The respiratory drugs included short-acting inhaled beta-agonists and anticholinergics, LABA, LAMA and methylxanthines, as well as antibiotics used for respiratory conditions. Another measure of the severity of COPD was the most recent measure of FEV1, for which the spirometry procedure quality in these general practices was found to be high [Citation29]. The percent predicted FEV1 measurement was calculated from the absolute FEV1 value using age, sex and height, with race classified as “Caucasian” for all [Citation30]. Dyspnea prior to cohort entry, measured by mMRC, CAT score or dyspnea symptoms as previously defined [Citation31], was identified. The most recent measure of blood eosinophil count available prior to cohort entry was also identified.
Baseline co-morbidity in the year prior to cohort entry was measured using clinical diagnoses, hospitalizations and prescriptions. Cardiovascular disease was defined using diagnoses for myocardial infarction, heart failure and stroke, as well as by prescriptions for cardiovascular conditions. Other comorbidities included diagnoses for diabetes, renal disease and cancer, all prior to cohort entry. Prescriptions for PPIs, NSAIDs, opioids, and aspirin were identified during the one-year baseline period.
Data analysis
The propensity score of treatment initiation was estimated by logistic regression using all covariates. Fine stratification weights were computed using 100 strata defined by the propensity score to create comparable arms of initiators of budesonide-based triple therapy and initiators of fluticasone-based triple therapy, with the same covariate distribution as the study cohort [Citation25]. Standardized mean differences of covariates were computed to assess the comparability of the two treatment groups.
Rates of outcomes were computed crudely and weighted using fine stratification of propensity score weights. A weighted Cox proportional hazard regression with a robust variance estimator was used in an as-treated analysis to compare current use of budesonide-based triple therapy with fluticasone-based triple therapy on the risks of moderate or severe exacerbation, severe exacerbation, death and severe pneumonia during the first year after treatment initiation. Continuing exposure was measured by successive prescriptions of the initial treatment with a maximal 60-day gap between the prescription dates, with current use defined by the 60-day period after the last such prescription date. As-treated time ended with a discontinuation of one component of the triple therapy or a switch to the other treatment.
The comparative analysis was stratified by prior asthma diagnosis, by the presence of exacerbations during the baseline year, and by baseline blood eosinophil counts as <150, 150–300, and >300 cells/µL, using the regression model with an interaction term between these factors and treatment. In addition, the adjusted hazard ratio of each outcome was fitted by continuous values of blood eosinophils counts using cubic splines.
Sensitivity analyses included an intent-to-treat analysis over the one-year follow-up as well as an alternative definition for a moderate or severe exacerbation that has been validated in the CPRD [Citation32]. It is defined by an outpatient or inpatient diagnosis of lower respiratory tract infection or acute exacerbation of COPD, or a prescription of COPD-specific antibiotics combined with an oral corticosteroid, or a record of two or more respiratory symptoms of acute exacerbation of COPD along with a prescription of COPD-specific antibiotics and/or an oral corticosteroid on the same day [Citation32]. We varied the continuous use definition for the as-treated analysis using 30- and 90-day gaps. In addition, the analysis was stratified by whether the combination treatments were initiated de novo or stepped up from LAMA or from LABA-ICS during the baseline year. Finally, we adjusted further the hazard ratio of a moderate or severe exacerbation for the region of residence. All analyses were conducted using SAS version 9.4. The study protocol was approved by the Independent Scientific Advisory Committee of the CPRD (Protocol 21_000491) and the Ethics Committee of the Jewish General Hospital (JGH Protocol #18-026), Montreal, Quebec, Canada.
Results
The study cohort included 29,716 new users of fluticasone-based triple therapy and 9,646 new users of budesonide-based triple therapy (Figure S.1). The baseline characteristics of the patients, comparing initiators of fluticasone-based with budesonide-based triple therapy, after weighting by fine stratification of propensity scores, confirm excellent balance on all covariates between the two groups (). In particular, 45% had no exacerbations in the year prior to triple therapy initiation, 29% had a prior diagnosis of asthma, the mean percent predicted FEV1 was 51% and the mean blood eosinophil count was around 245 cells/µL. The unweighted baseline characteristics (Table S.1) show that even without weighing the two groups are rather well balanced, suggesting that the choice of LABA-ICS is quite independent of the patient characteristics.
Table 1. Baseline characteristics of the study cohort of 29,716 initiators of fluticasone-based and 9,646 initiators of budesonide-based triple therapy, after fine stratification weighting from probability of treatment propensity scores, with corresponding standardized mean differences.
The mean treatment duration of the budesonide-based triple therapy group was 3.9 months, due to 54% discontinuing at least one treatment component during the one-year follow-up. For the fluticasone-based triple therapy initiators, the mean treatment duration was 3.8 months, due to 52% discontinuing at least one treatment component. The LAMAs included tiotropium (89%), umeclidinium (7%), glycopyrronium (2%) and aclidinium (2%).
The weighted cumulative incidence of a first moderate or severe exacerbation over 1 year was 50.0% for budesonide-based triple therapy and 51.1% for fluticasone-based triple therapy (), while for a severe exacerbation it was 12.2% and 12.4% respectively (). The adjusted hazard ratio of a first moderate or severe exacerbation with budesonide-based triple therapy was 0.98 (95% CI: 0.94–1.03), relative to fluticasone-based triple therapy, while for a severe exacerbation it was 0.97 (95% CI: 0.87–1.07) (). The weighted cumulative incidence of death () and of severe pneumonia () suggest small differences between the two groups. The hazard ratio of all-cause mortality with budesonide-based relative to fluticasone-based triple therapy was 0.89 (95% CI: 0.78–1.01), while for severe pneumonia requiring hospitalization it was 0.84 (95% CI: 0.75–0.95) ().
Figure 1. One-year cumulative incidence of moderate-severe exacerbation (a) and severe exacerbation (b), comparing fluticasone-based with budesonide-based triple therapy, estimated using the Kaplan-Meier method, after adjustment by fine stratification weights from the probability of treatment propensity scores.
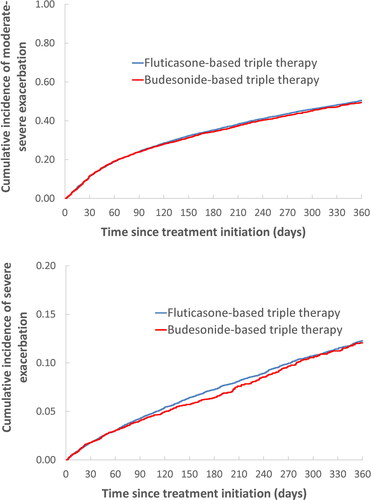
Figure 2. One-year cumulative incidence of all-cause death (a) and severe pneumonia (b), comparing fluticasone-based with budesonide-based triple therapy, estimated using the Kaplan-Meier method, after adjustment by fine stratification weights from the probability of treatment propensity scores.
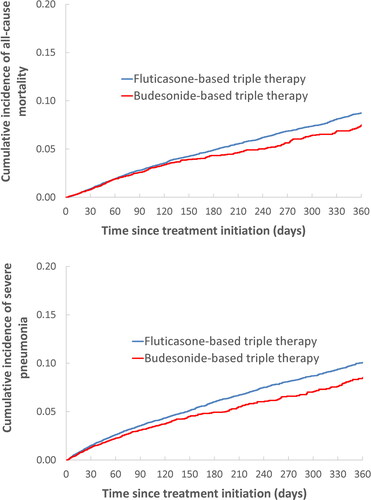
Table 2. Adjusted hazard ratios of COPD exacerbation, all-cause mortality and severe pneumonia requiring hospitalization comparing fluticasone-based with budesonide-based triple therapy in COPD patients in the first year after initiation, from the as-treated analysis.
shows that the incidence of a moderate or severe exacerbation was lower with budesonide-based triple therapy than with fluticasone-based triple therapy among patients with no exacerbations during the year prior to treatment initiation (HR 0.90; 95% CI: 0.83–0.99) but was similar among patients with prior exacerbations (HR 1.01; 95% CI: 0.96–1.06). There were no differences between the two triple therapies according to a prior diagnosis of asthma or by the level of blood eosinophils. The comparative incidence of severe exacerbation is not affected by a prior diagnosis of asthma, prior exacerbation or blood eosinophil count (Table S.2).
Table 3. Adjusted hazard ratios of moderate or severe exacerbation comparing fluticasone-based with budesonide-based triple therapy initiation in patients with COPD, from the as-treated analyses over one-year follow-up, stratified by prior asthma, prior exacerbations and peripheral blood eosinophil count.
The incidence of all-cause death was lower with budesonide-based triple therapy among patients with no prior exacerbations (HR 0.80; 95% CI: 0.66–0.98), but not among those with prior exacerbations (HR 0.94; 95% CI: 0.80–1.11), when compared with fluticasone-based triple therapy (Table S.3). Table S.3 also shows that the comparative incidence of all-cause death is not affected by a prior diagnosis of asthma, but appears to decrease with increasing blood eosinophil count ().
Figure 3. Adjusted hazard ratio (solid line) of all-cause death (a) and severe pneumonia (b) comparing fluticasone-based with budesonide-based triple therapy and 95% confidence intervals (dashed lines) according to blood eosinophil count (cells/µL) prior to treatment initiation, from the as-treated analysis fit by cubic splines.
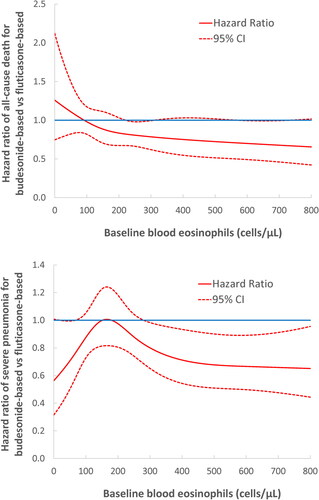
The overall hazard ratio of a severe pneumonia of 0.84 (95% CI: 0.75–0.95) comparing budesonide-based versus fluticasone-based triple therapy was not affected by prior asthma diagnosis or prior exacerbations (Table S.4). However, the hazard ratio appears to decrease with increasing blood eosinophil count, starting to be significantly lower than unity with blood eosinophil count >290 cells/µL, dropping to 0.71 (95% CI: 0.54–0.93) at 400 cells/µL and 0.67 (95% CI: 0.50–0.89) at 600 cells/µL ().
Sensitivity analyses mainly confirmed the robustness of the results (Supplemental Table S.5 and S.6). As expected, the HRs for all outcomes were slightly attenuated in the intention-to-treat analyses over the one-year follow-up (Table S.5). Altering the gap between prescriptions to define the as-treated analysis did not alter the main results (Supplemental Table S.6). Sensitivity analyses using the validated definition of moderate or severe exacerbation found the hazard ratio with budesonide-based triple therapy to be 0.93 (95% CI: 0.89–0.97) (Table S.6). Stratifying by whether the triple therapy was used de novo or stepped up from LABA-ICS or from LAMA did not affect the hazard ratio, nor did the further adjustment for region of residence.
Discussion
This large observational study in the real-world setting of clinical practice found that patients with COPD prescribed a budesonide-based triple therapy given in two inhalers had a similar incidence of exacerbation, moderate or severe, over the first year of use, compared with fluticasone-based triple therapy. However, the incidence of death, among those with no prior exacerbations, and of severe pneumonia were lower with budesonide-based compared with fluticasone-based triple therapy, particularly with increasing blood eosinophil count.
The recent IMPACT and ETHOS trials involving fluticasone furoate-based and budesonide-based triple therapy combinations suggested somewhat different effects of these triple therapies on all-cause mortality, when compared with a dual bronchodilator inhaler [Citation4,Citation5]. However, these different effects could be due to study design issues such as the extent of ICS discontinuation at randomization and differences in the severity of COPD [Citation33–35].
There are no head-to-head randomized trials or observational studies comparing fluticasone-based and budesonide-based triple therapy in patients with COPD, but there are comparative observational studies. Four studies reported significantly lower rates of severe exacerbation requiring hospitalization with budesonide-based inhalers [Citation6,Citation8,Citation10,Citation28], while two others did not find a difference [Citation12,Citation13]. Four studies reported significantly lower rates of severe pneumonia with budesonide-based inhalers [Citation7,Citation9,Citation10,Citation28], with one study concluding no difference [Citation13]. Thus, our findings of no difference on exacerbations appear discordant with the results of most studies, which did not employ new-user designs and did not control for blood eosinophil count, an important biomarker in COPD [Citation14]. On the other hand, the results on severe pneumonias are rather concordant with our findings of lower rates of severe pneumonia with budesonide-based triple therapy.
Only one study comparing the two LABA-ICS combined inhalers examined the outcome of mortality, reporting a hazard ratio of all-cause death with the budesonide-based inhaler of 0.93 (95% CI: 0.88–1.07) and of pneumonia-related death of 0.57 (95% CI: 0.40–0.82) [Citation9]. Our study found an overall hazard ratio of death with budesonide-based triple therapy of 0.89 (95% CI: 0.78–1.01), particularly pronounced among patients with no prior exacerbations (HR 0.80; 95% CI: 0.66–0.98) and those with higher blood eosinophil count.
Our study revealed important discrepancies in treatment patterns as compared with recommended management for COPD patients. For example, the GOLD group does not recommend the use of triple therapy as the initial maintenance treatment for COPD [Citation36]. Yet, 24% of the study cohort patients did not receive any LAMA, LABA, or ICS prior to initiating triple therapy. Moreover, triple therapy is recommended for patients with a history of exacerbations, yet 45% of the patients treated with triple therapy in the study cohort did not have an exacerbation in the year prior to initiating this treatment. These patients would not have been eligible for most trials of triple therapy such as IMPACT and ETHOS, which require at least two exacerbations in the prior year. Finally, 20% of the patients initiating triple therapy had no or mild dyspnea and 27% of the patients had a blood eosinophil count <150 cells/µL. Observational studies conducted in a real-world setting of COPD treatment found that multiple-inhaler triple therapy was no more effective than dual bronchodilators at preventing COPD exacerbations and all-cause mortality, but was associated with an increased risk of severe pneumonia [Citation37,Citation38]. This benefit-risk evidence should be considered, particularly when treating such patients for whom triple therapy is not recommended.
The analysis according to peripheral blood eosinophilia suggested potential lower mortality with budesonide-based triple therapy only in patients with higher blood eosinophil count (>300 cells/µL). However, this was statistically uncertain with the upper confidence curve of the hazard ratio hovering around 1. On the other hand, the lower incidence of severe pneumonia with budesonide-based triple therapy was clear for patients with higher blood eosinophil count (>300 cells/µL), and possibly for those with count < 100. Our ability to clearly link mortality, and to a lesser extent pneumonia risk, with eosinophil counts is certainly limited by the absence of eosinophil counts in more than 20% of patients and the timing and variability of eosinophil counts over time [Citation14]. Previous observational studies and meta-analysis of clinical trials have provided discordant results as to blood eosinophil counts and the overall risk of pneumonia [Citation39].
The new-user design that identifies initiators of the two-inhaler triple combinations, including those adding to prior LAMA or LABA-ICS inhalers, is a major strength of our study. Indeed, this design reduces the potential for confounding in comparing the two therapies head-to-head at the time of their initiation and avoids bias from prevalent users [Citation23,Citation40]. As a result, the two groups were very similar even before statistical adjustments (Table S.1). Nonetheless, we used accurate methods of weighing, by fine stratification of propensity scores, to make the two groups as similar as possible on a large number of covariates. The major outcomes of severe exacerbation and pneumonia based on hospitalization records are less subject to misclassification than the moderate exacerbation definition, while all-cause mortality is highly valid in the CPRD [Citation20,Citation21]. Finally, the size of this study, including close to 40,000 patients with COPD treated with triple therapy, is a major strength, as is the availability of data on smoking status, FEV1, dyspnea, and blood eosinophil count. Limitations of the study include the measures of exposure to the two triple therapies which were based on prescriptions, not necessarily dispensed, which could introduce misclassification and which can be magnified by the variable and potentially less than optimal inhaler technique in the real-world setting. The continuous treatment duration was relatively short because many patients either discontinued or switched, with only 46% continuing treatment for the full year, a reflection of the real-world clinical setting. The use of physician diagnoses to identify the cohort may have misclassified some patients with asthma as COPD, though this risk of misclassification was reduced with the 50 years of age cutoff. Finally, residual confounding cannot be ruled out despite the use of propensity score weighting which created groups highly comparable on COPD severity.
Conclusion
This large study in the real-world clinical setting of COPD treatment suggests that budesonide-based triple therapy given in two inhalers is generally as effective at reducing exacerbations as fluticasone-based triple therapy. However, the budesonide-based triple therapy is associated with a modestly lower incidence of death, especially among patients with no prior exacerbations, and a lower incidence of severe pneumonia, particularly in patients with higher blood eosinophil count. Moreover, our study reveals that the profile of patients with COPD receiving triple therapy treatment, either budesonide-based or fluticasone-based, diverges substantially from current treatment recommendations, which may place patients at unnecessary risk.
Author’s contributions
Dr Ernst participated in study design, data interpretation, and writing of the manuscript. Ms Dell’Aniello participated in data analysis and writing of the manuscript. Pr. Suissa participated in data acquisition, study design, data interpretation, writing of the manuscript, and acts as guarantor of this entire manuscript.
Supplemental Material
Download (){kind=link}
Acknowledgments
This study was conducted thanks to infrastructure funding from the Canadian Institutes of Health Research (CIHR) and the Canadian Foundation for Innovation (CFI). Pr. Suissa is the recipient of the Distinguished James McGill Professorship award. These sponsors had no input in the study.
Declaration of interest
Pr. Suissa has previously received research grants from Boehringer Ingelheim and Novartis and has participated in advisory board meetings or as speaker for AstraZeneca, Boehringer‐Ingelheim, and Novartis. Dr. Ernst and Ms Dell’Aniello have no conflicts of interest.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
Data availability statement
This study is based in part on data from the Clinical Practice Research Datalink obtained under license from the UK Medicines and Healthcare products Regulatory Agency. The data are provided by patients and collected by the UK National Health Service as part of their care and support. The interpretation and conclusions contained in this study are those of the author/s alone. Because electronic health records are classified as “sensitive data” by the UK Data Protection Act, information governance restrictions (to protect patient confidentiality) prevent data sharing via public deposition. Data are available with approval through the individual constituent entities controlling access to the data. Specifically, the primary care data can be requested via application to the Clinical Practice Research Datalink (https://www.cprd.com).
References
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Eur Respir J. 2017;49(3):1700214. DOI:10.1183/13993003.00214-2017
- Quint JK, O’Leary C, Venerus A, et al. Prescribing pathways to triple therapy: a Multi-Country, retrospective observational study of adult patients with chronic obstructive pulmonary disease. Pulm Ther. 2020;6(2):333–350. DOI:10.1007/s41030-020-00132-7
- Rodriguez-Roisin R, Rabe KF, Vestbo J, et al. Global initiative for chronic obstructive lung disease (GOLD) 20th anniversary: a brief history of time. Eur Respir J. 2017;50(1):1700671. DOI:10.1183/13993003.00671-2017
- Lipson DA, Crim C, Criner GJ, et al. Reduction in All-Cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201(12):1508–1516. DOI:10.1164/rccm.201911-2207OC
- Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced All-Cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease. A randomized, Double-Blind, multicenter, Parallel-Group study. Am J Respir Crit Care Med. 2021;203(5):553–564. DOI:10.1164/rccm.202006-2618OC
- Blais L, Forget A, Ramachandran S. Relative effectiveness of budesonide/formoterol and fluticasone propionate/salmeterol in a 1-year, population-based, matched cohort study of patients with chronic obstructive pulmonary disease (COPD): effect on COPD-related exacerbations, emergency department visits and hospitalizations, medication utilization, and treatment adherence. Clin Ther. 2010;32(7):1320–1328. DOI:10.1016/j.clinthera.2010.06.022
- Suissa S, Patenaude V, Lapi F, et al. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax. 2013;68(11):1029–1036. DOI:10.1136/thoraxjnl-2012-202872
- Larsson K, Janson C, Lisspers K, et al. Combination of budesonide/formoterol more effective than fluticasone/salmeterol in preventing exacerbations in chronic obstructive pulmonary disease: the PATHOS study. J Intern Med. 2013;273(6):584–594. DOI:10.1111/joim.12067
- Janson C, Larsson K, Lisspers KH, et al. Pneumonia and pneumonia related mortality in patients with COPD treated with fixed combinations of inhaled corticosteroid and long acting β2 agonist: observational matched cohort study (PATHOS). BMJ. 2013;346:f3306. DOI:10.1136/bmj.f3306
- Chang TY, Chien JY, Wu CH, et al. Comparative safety and effectiveness of inhaled corticosteroid and long-acting β(2)-agonist combinations in patients with COPD. Chest. 2020;157(5):1117–1129. DOI:10.1016/j.chest.2019.12.006
- Suissa S, Dell’Aniello S, Ernst P. Comparing initial LABA-ICS inhalers in COPD: real-world effectiveness and safety. Respir Med. 2021;189:106645.
- Roberts M, Mapel D, Petersen H, et al. Comparative effectiveness of budesonide/formoterol and fluticasone/salmeterol for COPD management. J Med Econ. 2011;14(6):769–776. DOI:10.3111/13696998.2011.622817
- Kern DM, Davis J, Williams SA, et al. Comparative effectiveness of budesonide/formoterol combination and fluticasone/salmeterol combination among chronic obstructive pulmonary disease patients new to controller treatment: a US administrative claims database study. Respir Res. 2015;16(1):52. DOI:10.1186/s12931-015-0210-x
- Bafadhel M, Pavord ID, Russell REK. Eosinophils in COPD: just another biomarker? Lancet Respir Med. 2017;5(9):747–759. DOI:10.1016/S2213-2600(17)30217-5
- Sherman RE, Anderson SA, Dal Pan GJ, et al. Real-World evidence — what is it and what can it tell Us? N Engl J Med. 2016;375(23):2293–2297. DOI:10.1056/NEJMsb1609216
- Frieden TR. Evidence for health decision making — beyond randomized, controlled trials. N Engl J Med. 2017;377(5):465–475. DOI:10.1056/NEJMra1614394
- Wolf A, Dedman D, Campbell J, et al. Data resource profile: clinical practice research datalink (CPRD) aurum. Inter J Epidemiol. 2019;48(6):1740–1740g. DOI:10.1093/ije/dyz034
- Herrett E, Thomas SL, Schoonen WM, et al. Validation and validity of diagnoses in the general practice research database: a systematic review. Br J Clin Pharmacol. 2010;69(1):4–14. DOI:10.1111/j.1365-2125.2009.03537.x
- Herrett E, Gallagher AM, Bhaskaran K, et al. Data resource profile: clinical practice research datalink (CPRD). Int J Epidemiol. 2015;44(3):827–836. DOI:10.1093/ije/dyv098
- Quint JK, Mullerova H, DiSantostefano RL, et al. Validation of chronic obstructive pulmonary disease recording in the clinical practice research datalink (CPRD-GOLD). BMJ Open. 2014;4(7):e005540. DOI:10.1136/bmjopen-2014-005540
- Rothnie KJ, Müllerová H, Thomas SL, et al. Recording of hospitalizations for acute exacerbations of COPD in UK electronic health care records. Clin Epidemiol. 2016;8:771–782. DOI:10.2147/CLEP.S117867
- Suissa S, Dell’Aniello S, Ernst P. Comparative effectiveness of LABA-ICS versus LAMA as initial treatment in COPD targeted by blood eosinophils: a population-based cohort study. Lancet Respir Med. 2018;6(11):855–862. DOI:10.1016/S2213-2600(18)30368-0
- Johnson ES, Bartman BA, Briesacher BA, et al. The incident user design in comparative effectiveness research. Pharmacoepidemiol Drug Saf. 2013;22(1):1–6. DOI:10.1002/pds.3334
- Suissa S, Moodie EE, Dell’Aniello S. Prevalent new-user cohort designs for comparative drug effect studies by time-conditional propensity scores. Pharmacoepidemiol Drug Saf. 2017;26(4):459–468. DOI:10.1002/pds.4107
- Desai RJ, Franklin JM. Alternative approaches for confounding adjustment in observational studies using weighting based on the propensity score: a primer for practitioners. BMJ. 2019;367:l5657. DOI:10.1136/bmj.l5657
- Meropol SB, Metlay JP. Accuracy of pneumonia hospital admissions in a primary care electronic medical record database. Pharmacoepidemiol Drug Saf. 2012;21(6):659–665. DOI:10.1002/pds.3207
- Suissa S, Dell’Aniello S, Ernst P. Comparative effectiveness and safety of LABA-LAMA vs LABA-ICS treatment of COPD in Real-World clinical practice. CHEST. 2019;155(6):1158–1165. DOI:10.1016/j.chest.2019.03.005
- Suissa S, Dell’Aniello S, Ernst P. Comparative effectiveness of initial LAMA versus LABA in COPD: real-world cohort study. COPD. 2021;18(1):1–8. DOI:10.1080/15412555.2021.1877649
- Rothnie KJ, Chandan JS, Goss HG, et al. Validity and interpretation of spirometric recordings to diagnose COPD in UK primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:1663–1668. DOI:10.2147/COPD.S133891
- Quanjer PH, ERS Global Lung Function Initiative, Stanojevic S, Cole TJ, Baur X. Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. DOI:10.1183/09031936.00080312
- Rebordosa C, Plana E, Aguado J, et al. GOLD assessment of COPD severity in the clinical practice research datalink (CPRD). Pharmacoepidemiol Drug Saf. 2019;28(2):126–133. DOI:10.1002/pds.4448
- Rothnie KJ, Müllerová H, Hurst JR, et al. Validation of the recording of acute exacerbations of COPD in UK primary care electronic healthcare records. PLOS One. 2016;11(3):e0151357. DOI:10.1371/journal.pone.0151357
- Suissa S, Drazen JM. Making sense of triple inhaled therapy for COPD. N Engl J Med. 2018;378(18):1723–1724. DOI:10.1056/NEJMe1716802
- Suissa S, Ariel A. Triple therapy in COPD: only for the right patient. Eur Respir J. 2019;53(4):1900394. DOI:10.1183/13993003.00394-2019
- Suissa S. Perplexing mortality data from triple therapy trials in COPD. Lancet Respir Med. 2021;9(7):684–685.
- Global strategy for the diagnosis, management, and prevention of Chronic Obstructive Pulmonary Disease (2019 Report). http://goldcopd.org/gold-2019-global-strategy-diagnosis-management-prevention-copd/. 2019.
- Suissa S, Dell’Aniello S, Ernst P. Comparative effects of LAMA-LABA-ICS vs LAMA-LABA for COPD: cohort study in real-world clinical practice. CHEST. 2020;157(4):846–855. DOI:10.1016/j.chest.2019.11.007
- Suissa S, Dell’Aniello S, Ernst P. Triple inhaler versus dual bronchodilator therapy in COPD: real-world effectiveness on mortality. COPD. 2021:1–9. DOI:10.1080/15412555.2021.1977789. [Epub ahead of print].
- Ernst P. Blood eosinophils in COPD and the future risk of pneumonia. Eur Respir J. 2018;52(1):1800981. DOI:10.1183/13993003.00981-2018
- Ray WA. Evaluating medication effects outside of clinical trials: new-user designs. Am J Epidemiol. 2003;158(9):915–920. DOI:10.1093/aje/kwg231