
ABSTRACT
Hip strength has been shown to influence the incidence of injury in women’s football. The first objective of our study was to examine the differences in isometric strength of the adductors and abductors between two test positions (0° vs. 45° hip angle). Our second objective was to verify the sensitivity of the two test positions in discriminating between women footballers with and without a history of groin pain in the last twelve months. One hundred and one elite players from the Slovenian women’s football league were tested. The isometric strength of the adductors, abductors, and the ratio between hip abductor and adductor strength in two different test positions were assessed. We found statistically significant differences (p < 0.05; effect size range 0.12–0.13) between the two test positions in hip adduction, abduction strength, and abductor/adductor strength ratio. The ROC analysis showed that only the abductor/adductor strength ratio at the 0° hip angle position can differentiate between players with and without a history of groin pain, with an optimal cut-off point of ≤ 1.01 (p < 0.05; AUC = 0.734). The results should help practitioners plan hip strength training for returning to sport or preventing groin pain among women football players.
Introduction
Hip and groin injuries are common in football (Wollin et al., Citation2018). Previous studies have shown that in women’s football, hip and groin injuries account for approximately 5.1% of injuries sustained in competition and 10% of injuries that occur during practice, leading to increased time lost from competition (Ralston et al., Citation2020). Chronic groin pain appears to be more prevalent (73%) than acute pain (27%) with the primary cause being adductor-related groin pain (Marušič & Šarabon, Citation2022; Werner et al., Citation2009).
Among all risk factors for groin injuries, hip adductor (add) strength in men’s football has gained significant scientific interest (Collings et al., Citation2021; Markovic et al., Citation2020; Nielsen et al., Citation2022; Serner et al., Citation2005). Decreased isometric and eccentric strength of the add muscles has been identified as risk factors for future groin pain in men’s football (Engebretsen et al., Citation2010; Markovic et al., Citation2020). However, there is conflicting information in the literature regarding the relationship between hip joint add strength and previous groin injuries. For example, Marušič and Šarabon (Citation2022) reported that lower isometric add strength in men football did not distinguish whether players had experienced groin pain in the past year. However, Esteve et al. (Citation2018) found that men football players with groin pain lasting longer than six weeks in the previous season exhibited 11.5–15.3% decreased add isometric strength. Previous studies have also indicated that the strength imbalance between hip add and hip abductor (abd) muscles could pose a risk for groin injuries (Nicholas & Tyler, Citation2002). Belhaj et al. (Citation2016) reported a significantly lower abd/add isokinetic strength ratio in men football players who developed chronic groin pain in the future. However, there is limited knowledge regarding the impact of prior groin injuries on hip add and abd strength, as well as the abd/add strength ratio among women football players. To the best of the author’s knowledge, only Collings et al. (Citation2021) found no difference in add and abd isometric strength between uninjured and groin-injured players over the past year in a study of 369 women football players.
Research investigating the influence of add and abd isometric strength, as well as abd/add strength ratios on incidence of groin injuries includes assessments of strength in extended and flexed hip positions (Belhaj et al., Citation2016; Markovic et al., Citation2020; Spudić et al., Citation2023; Thorborg et al., Citation2011). The capacity to generate add and abd torque varies based on the add and abd muscles’ moment arms (Neumann, Citation2010) and force-length relationships (Fujisawa et al., Citation2014; Lovell et al., Citation2012). Previous studies have identified higher add and abd torque values at a hip angle of 45° in comparison to hip angle of 0° (Spudić et al., Citation2023). While torque-generating capacity and relative contribution to the total torque produced by different add and abd muscles is influenced by the hip flexion angle, it is essential to consider hip position when testing isometric hip add or abd strength. This consideration helps in targeting the most vulnerable muscle groups concerning groin pain. Additionally, the hip flexion angle also affects the abd/add strength ratio. As a result, it impacts the significance of conclusions drawn regarding their associations with the occurrence of groin pain.
Female football players are more vulnerable to severe injuries than their male counterparts (Larruskain et al., Citation2017). Therefore, prevention and rehabilitation strategies should be tailored to the needs of female football players, which could positively influence the further development and general level of interest in women’s football among youth. Specifically, isometric add and abd strength reference values for elite female football players are absent in the literature. Moreover, the sensitivity of add and abd strength results assessed in different hip flexion angles to distinguish between previously injured and uninjured women football players is unknown. Hence, the primary objective of our study was to investigate the differences in isometric add and abd strength, as well as the abd/add isometric strength ratio between the two test positions (i.e., 0° hip angle and 45° hip angle). The secondary objective of our study was to assess the sensitivity of the variables obtained in these two test positions in distinguishing between players with and without groin pain in the past twelve months.
Methods
Study design
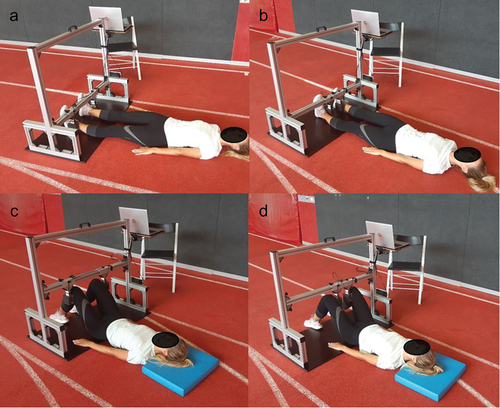
To obtain reference values of hip add, abd isometric strength and hip abd/add strength ratios in two different test positions (i.e., 0° hip angle and 45° hip angle) in female football players we have conducted a cross-sectional study. Following this, we have investigated if any of the obtained variables can be used to discriminate between women football players with and without groin pain in the past twelve months. Participants underwent hip strength testing on a custom-made, frame-stabilized dynamometer system device () with excellent intra-set and inter-set reliability (ICC >0.90) and good reliability for test-retest results (ICC range 0.79–0.90) of hip add and abd strength measures (Spudić et al., Citation2023). Before the testing procedure, participants provided a self-reported football-related injury history and performed a standardized warm-up as described by Spudić et al. (Citation2023).
Figure 1. Testing setup for hip strength assessment using frame-stabilized dynamometer system device. a − 0° hip angle abduction. b − 0° hip angle adduction. c − 45° hip angle abduction. d − 45° hip angle adduction.
Participants
One hundred one (N = 101) elite women football players from the Slovenian Women’s Football League participated in the study. The main characteristics of the participants are as follows (mean and 95% confidence intervals): age 19.2 (18.5; 20.0) years, body height: 167.9 (166.8; 169.0) cm, body mass 61.8 (60.5; 63.2) kg, body mass index: 21.9 (21.5; 22.3) and football training experience 8.7 (7.9; 9.6) years. The exclusion criteria were: any hip and knee injuries (e.g. ligament, meniscus or cartilage damage), chronic diseases (systemic, cardiac and/or respiratory diseases and neuromuscular disorders), history of lower back pain or other acute injuries in the past month that could in any way negatively influence hip muscles maximal voluntary isometric performance. After considering exclusion criteria, five participants were excluded from the analyses – therefore the results of 96 players were analysed. The study was approved by the National Medical Ethics Committee (no. 0120–690/2017/8) and adhered to the tenets of the Oviedo Convention and Declaration of Helsinki. Participants were informed about the testing procedures prior to signing an informed consent. They were instructed to avoid any strenuous exercise at least two days prior to the testing session.
Adduction and abduction strength measurements
Hip add and abd in two testing positions were conducted in a randomized order to minimize test learning and fatigue effect. The tests were performed by one experienced examiner. Tests on a custom‐made frame-stabilized dynamometer system device (Spudić et al., Citation2023) were performed bilaterally (). Abd and add at 0° hip angle position [abd0°, add0°] strength was measured with the participant lying supine with knees and hips fully extended. Sensors were placed on the lateral malleoli for abd0° and medial malleoli for add0°. Abd and add at 45° hip angle position [abd45°, add45°] strength was measured with the participant lying supine, knees flexed at 90° and hips at 45°. Sensors were placed on the lateral femoral condyles for abd45° and medial femoral condyles for add45°. Testing positions were individually adjusted based on participants’ anthropometric characteristics. During all tests, ankles and knees were aligned hip-width apart. Lever arms were measured prior each test to the nearest 0.5 cm, as follows. Leg length (0° hip angle position) from the greater trochanter to the middle of the sensor. Thigh length (45° hip angle position) from lateral femoral epicondyle to the middle of the sensor.
Each test was repeated three times (maximal voluntary isometric contraction lasted approximately 5 s) with 30 s break between repetitions. Contraction time was controlled by an examiner with the use of real‐time feedback displayed on the computer screen. The break between different test positions was approximately three minutes and served for adjusting the participant to the following randomly assigned testing position. The correct test execution was provided by an investigator.
Data analysis
Signals from frame-stabilized dynamometer system device were obtained from two load-cell sensors (S-Type 200 kg Steel Weighting Sensor, Changsha TAIHE Electronic Equipment Co., China) mounted vertically on the firm frame. The sensor assembly provided an average horizontal force‐time data of the left and right legs. Raw analogue signals were converted using A/D converter (Loadcell sensor 24-bit ADC – HX711, Circuit Systems, India), monitored using Arduino-Uno (ATmega328P, Robot ItalY, Italija) microcontroller and, finally, analysed using custom-developed software (github.com/robert-cv/HipStrengthTesterGUI, Črnomelj, Slovenia). Data were sampled at 100 Hz. The highest force level achieved in a one-second average moving interval was considered as the peak force. The peak force values were multiplied by the lever arms (m) and normalized by participants’ body mass to obtain normalized peak torque (Nm/kg) for each repetition. As gravity does not influence the results in this testing position, no corrections were performed before the analysis.
Injury history data
Prevalence of hip and groin problems was monitored using the Oslo Sports Trauma Research Center Overuse Injury Questionnaire for hip and groin problems (OSTRC-O) (Clarsen et al., Citation2014). In addition, we asked for the presence of any acute injuries in the past month, that could in any way limit the maximum isometric hip add or abd performance. In the presence of researchers, a short questionnaire was filled-out. The participants filled-out the following topics: Ia) Presence of acute injuries in the past month [yes, no]; Ib) if “yes”, identify the location of the injury. IIa) Presence of overuse injuries in the past 12 months [yes, no]; IIb) if “yes”, identify the location of the injury. Injury locations were offered as follows: head, neck, shoulder, upper arm, elbow, forearm, wrist and hand, chest, trunk and abdomen, thoracic spine, lumbar spine, pelvis and buttock, thigh, knee, lower leg, ankle and foot. We defined injuries with gradual onset as “overuse” and problems starting with sudden onset during a single injury event as “acute.” IIIa) Then, we specifically asked after the presence of hip and groin pain in the past 12 months [yes, no]. Hip and groin pain were more precisely described and referred to the history of add tenderness and pain on resisted add movements, inguinal-related groin pain located in the inguinal canal region and tenderness of the inguinal canal, local tenderness of the pubic symphysis and the immediately adjacent bone, hip pain when flexing-abducting-externally rotating or/and flexing-adduction-internal rotating the hip (Weir et al., Citation2015). Those players who described hip and groin pain in the previous year, excluding players reporting acute and overuse injuries of trunk and abdomen, lumbar spine, pelvis and buttock, thigh, knee, lower leg, ankle and foot in the past month (i.e. injuries that could affect maximal voluntary contraction values), were categorized as previously injured. Then, they answered questions specifically referring to their hip and groin status. The questionnaire continued with five questions, assessing IV) the onset of hip and groin problems (gradual or sudden), V) the effect of hip and groin pain on the ability to participate in training and match play [full – without problems, full – but with problems, reduced due to problems, cannot – due to problems], VI) potential reduction in training volume [no reduction, minor, moderate, major, cannot participate], VII) performance [no reduction, minor, moderate, major, cannot participate], and VIII) pain experience during sport participation [no pain, mild, moderate, severe].
Statistical analyses
The normal distribution of the data was checked using the Shapiro – Wilk test (p > 0.05). Agreement between the two testing positions was assessed with Pearson correlation coefficient (r) and paired samples t-tests. The Cohen’s d was used to determine the effect size with d ≤ 0.01 considered to be very small, d ≥ 0.20 small, d ≥ 0.50 medium and d ≥ 0.80 large (Cohen, Citation1988). The magnitude of correlation was interpreted as negligible (<0.1), weak (0.1–0.39), moderate (0.4–0.69), strong (0.7–0.89) and very strong (>0.9) (Schober & Schwarte, Citation2018). Then, percentiles were calculated for all the variables. The prevalence of groin injuries was reported in relation to the population included in the study and injury characteristics (participation, training volume reduction, performance, pain). Finally, receiver operating characteristic (ROC) statistics were constructed independently for all dependent variables to determine (1) the overall discriminative accuracy of each variable for discern among the history of groin pain and groin pain-free players and (2) the optimal practical cut-off value of each in order to distinguish between a positive and negative test for history of groin pain. The overall accuracy of each variable was assessed by evaluating the area under the curve, which ranged from 0 to 1 (0.5 equating to no better than chance alone and 1 inferring perfect accuracy). Moreover, the optimal clinical cut-off point for each variable was selected by extrapolating the value on the ROC curve that maximized the sum of sensitivity and specificity (Youden index). The corresponding sensitivity and specificity were reported. For the analyses SPSS (IBM SPSS version 25.0; Armonk, NY) was used. An alpha of 5% was used to determine statistical significance.
Results
Using the t-test, statistically significant differences were found between the two test positions for add and abd strength and add/abd strength ratio (p < 0.05). The differences were large (ranged from 1.02 for the abd/add ratio to 5.4 for the abd strength) according to the Cohen’s d effect size. The correlations between the two test positions were statistically significant (p < 0.05) regardless of the observed variable and ranged from 0.51 for the abd/add ratio to 0.80 for the add strength) ().
Table 1. Descriptive statistics and agreement between testing positions.
We provide reference values of the obtained variables for 96 women football players as percentiles in . Higher median values of add45° strength, in comparison to abd45° strength, were found, and vice versa, higher median values of abd0° strength, in comparison to add0° strength, were found.
Table 2. Percentiles for maximal isometric adduction and abduction strength and abduction to adduction strength ratio.
A total of 10/96 players reported hip or groin pain in the past twelve months (9.9%). In all cases, gradual or overuse hip or groin pain problems were reported. Hip and groin pain caused absence from at least one training or game in 3/10 players, in 2/10 players it reduced their participation because of the problems and in 5/10 they participated fully with problems. Training volume was reduced fully in 3/10 players (cannot participate), 2/10 majorly, 4/10 moderately and 1/10 minorly. Performance was fully reduced in 3/10 players (cannot participate), in 2/10 it was majorly reduced, 4/10 moderately and 1/10 minorly. During sport participation the pain experience was severe in 2/10, moderate in 4/10 and mild in 1/10).
The ROC analysis () indicated that only abd0°/add0° strength ratio can significantly distinguish between players with and without a history of groin pain better than chance alone (area under the curve statistically significantly different than 0.5).
Table 3. Receiver operating statistics for distinguishing between women football players with and without previous groin pain.
The Youden index was calculated. The cut-off value for the abd0°/add0° ratio was ≤ 1.01, suggesting that lower abd muscle strength in comparison to add strength was associated with groin pain. The sensitivity of the value was 77.8% and the specificity was 77.0%. This means that 77.8% of players with an abd0°/add0° ratio ≤ 1.01 were correctly identified with a history of groin pain and 77.0% of players with an abd0°/add0° ratio ≤ 1.01 were correctly identified as having no groin pain.
Discussion
The main findings of our study are statistically significant differences between the two test positions in hip add and abd strength and add/abd isometric strength ratio. Moreover, only abd/add ratio assessed in the extended hip position can significantly differentiate between women football players with and without a history of groin pain. The results confirm our assumptions that hip flexion angle must be considered when evaluating the strength of the hip add, abd muscles and abd/add muscles strength ratio particularly for the sensitivity in detecting previous groin injuries in women football players.
Higher values in the 45° hip angle position were presumably found due to favourable lever arms and/or force-length relationships of the add magnus and the upper part of the gluteus maximus muscles, respectively. In comparison to other add and abd muscles, these two muscles have a large physiological cross-sectional area and long fibres, which suggests that they are expected to generate high forces over a wide range of lengths (Ward et al., Citation2010). While other synergistic add muscles (e.g., gracilis, pectineus, adductor brevis and longus) and synergistic abd muscles (e.g., tensor fasciae latae, piriformis, gluteus minimus and medius) of the hip are oriented towards stability and tend to have favourable abd lever arms in the extended hip position (Ward et al., Citation2010), it is unlikely that their force-length relationship changes to such an extent when the hip is flexed that they could significantly contribute to higher add and abd torque production.
We presented evidence that abd/add ratio is lower when the hip is flexed. These results may be attributed to the optimal length of the add muscles for generating force in the flexed position (Delmore et al., Citation2014), while the abd muscles have moment arms that favour an extended position (Fujisawa et al., Citation2014; Neumann, Citation2010). This observation is reinforced by the fact that most add muscles are also classified as hip flexors, with the exception of the posterior head of the add magnus (Benn et al., Citation2018). Therefore, they may be in a more mechanically advantageous position when the hip is flexed to 45°. In contrary, primary abd muscles’ moment arms (Kwilas et al., Citation2015) and muscle activity change negatively with increasing flexion of the hip – with the exception of the anterior part of the gluteus maximus, which has the possibility to act as a hip abd when the hip joint is flexed (Fujisawa et al., Citation2014).
It was found that lower isokinetic add strength is a risk factor for future groin injury and that current groin pain reduces add eccentric, but not isometric strength (Thorborg et al., Citation2014). However, whether previous groin pain symptoms have a long-lasting effect on add strength is less clear. In our study, we reported that add and abd strength may not be indicative of previous groin injury. In the only other study of women football players that examined the effects of previous groin injury on current strength, isometric strength tests were performed for hip add and abd in the extended hip position (Collings et al., Citation2021). They reported no differences between women football players with and without previous groin injuries. Studies conducted in men football players also support our findings, showing that previous groin pain does not affect isometric strength performance results (DeLang et al., Citation2020; Marušič & Šarabon, Citation2022).
The novel finding of our study is that, despite the higher strength values found at the 45° hip angle position, the abd/add strength ratio at the extended (0°) hip position appears to be more sensitive to a history of groin pain in women football players. This finding is consistent with the finding of Belhaj et al. (Citation2016) who found increased risk of future groin injuries in men football players with abd/add isokinetic strength imbalance. In contrast, it diverges from the findings of Marušič and Šarabon (Citation2022), who reported no abd/add isometric strength imbalance in youth men football players with a history of groin injuries. We reported that players with an abd0°/add0° ratio with a clinical cut-off value ≤ 1.01 were identified with a history of groin pain. Our results suggest that lower abd strength (including gluteus medius, minimus, and tensor fasciae latae muscles (Fujisawa et al., Citation2014; Neumann, Citation2010) in comparison to add strength in the extended hip position may be a consequence of previous groin injuries. This could be because the coactivation of add and abd muscles in the extended hip position play an important role in stabilizing the pelvis during ballistic activities, such as sudden change of direction and kicking (Brophy et al., Citation2007). While we did not observe a decrease in add strength, it is plausible to speculate that injuries among the participants in our study occurred due to lower abd strength, and that this abd weakness persisted after the injury. The reduced strength of the abd muscles could have disrupted hip joint stability, affected movement patterns, and consequently, the add muscle group became overworked. It is worth noting that all the reported groin injuries in our study were classified as overuse injuries. Additionally, as we lack information about the players’ strength values before their injuries, we cannot definitively conclude whether the lower abd/add strength ratio in the injured group is a consequence of previous injuries or a potential contributing factor to injury occurrence in the past.
Our study has some limitations which need to be mentioned. Participants’ injury history was self-reported and did not include specific imaging (ultrasound, magnetic resonance imaging, etc.), which could lead to a misreported injury and thus misclassification of the participant into the injured group. We used an isometric contraction to measure hip muscle strength. It has already been established that isometric contraction is not specific to the performance of most human movements, which require dynamic contraction of the muscles throughout the range of motion. Therefore, an isometric test could be a poor predictor of dynamic performance, and the testing lacks external validity. The duration of the groin symptoms was not considered in the questionnaire. Therefore, the message of our study could be different if the duration of the pain had been considered, as the duration of groin pain in the past year affects the recovery time and strength of the add muscles (Esteve et al., Citation2018). Moreover, our results are generalizable only to female soccer players, as the groin anatomy, as well as pelvic and hip joint morphology, may explain differences in torque production in comparison to man (Schache et al., Citation2016).
This was the first study to test abd and add strength and abd/add strength ratio in such a large sample of elite women football players. Our results show that hip flexion angle must be considered when evaluating the strength of the hip add and abd muscles. Moreover, testing abd/add strength ratio in the extended hip position is recommended in the future while 77% of players in our study with the ratio ≤ 1.01 was correctly identified with a history of groin pain. We provide reference values for the identified variables, which can serve as targets for hip add and abd strength training programmes in women’s football.
Acknowledgements
The Slovenian Research Agency provided authors D.S. and V.H. with support in the form of salary through the programmes ‘Kinesiology of monostructural, polystructural and conventional sports’ [P5‐0147]. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The authors would like to thank the participants for their cooperation.
The data that support the findings of this study are available from the corresponding author, D. S., upon reasonable request.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Belhaj, K., Meftah, S., Mahir, L., Lmidmani, F., & Elfatimi, A. (2016). Isokinetic imbalance of adductor–abductor hip muscles in professional soccer players with chronic adductor-related groin pain. European Journal of Sport Science, 16(8), 1226–1231. https://doi.org/10.1080/17461391.2016.1164248
- Benn, M. L., Pizzari, T., Rath, L., Tucker, K., & Semciw, A. I. (2018). Adductor magnus: An EMG investigation into proximal and distal portions and direction specific action. Clinical Anatomy, 31(4), 535–543. https://doi.org/10.1002/ca.23068
- Brophy, R. H., Backus, S. I., Pansy, B. S., Lyman, S., & Williams, R. J. (2007). Lower extremity muscle activation and alignment during the soccer instep and side-foot kicks. Journal of Orthopaedic and Sports Physical Therapy, 37(5), 260–268. https://doi.org/10.2519/jospt.2007.2255
- Clarsen, B., Rønsen, O., Myklebust, G., Flørenes, T. W., & Bahr, R. (2014). The Oslo sports trauma research center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. British Journal of Sports Medicine, 48(9), 754–760. https://doi.org/10.1136/bjsports-2012-092087
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Associates.
- Collings, T. J., Diamond, L. E., Barrett, R. S., Timmins, R. G., Hickey, J. T., du Moulin, W. S., Gonçalves, B. A. M., Cooper, C., & Bourne, M. N. (2021). Impact of prior anterior cruciate ligament, hamstring or groin injury on lower limb strength and jump kinetics in elite female footballers. Physical Therapy in Sport, 52, 297–304. https://doi.org/10.1016/j.ptsp.2021.10.009
- DeLang, M. D., Garrison, J. C., Hannon, J. P., McGovern, R. P., Christoforetti, J., & Thorborg, K. (2020). Short and long lever adductor squeeze strength values in 100 elite youth soccer players: Does age and previous groin pain matter? Physical Therapy in Sport, 46, 243–248. https://doi.org/10.1016/j.ptsp.2020.10.001
- Delmore, R. J., Laudner, K. G., & Torry, M. R. (2014). Adductor longus activation during common hip exercises. Journal of Sport Rehabilitation, 23(2), 79–87. https://doi.org/10.1123/JSR.2012-0046
- Engebretsen, A. H., Myklebust, G., Holme, I., Engebretsen, L., & Bahr, R. (2010). Intrinsic risk factors for groin injuries among male soccer players: A prospective cohort study. The American Journal of Sports Medicine, 38(10), 2051–2057. https://doi.org/10.1177/0363546510375544
- Esteve, E., Rathleff, M. S., Vicens-Bordas, J., Clausen, M. B., Hölmich, P., Sala, L., & Thorborg, K. (2018). Preseason adductor squeeze strength in 303 Spanish male soccer athletes: A cross-sectional study. Orthopaedic Journal of Sports Medicine, 6(1), 1–8. https://doi.org/10.1177/2325967117747275
- Fujisawa, H., Suzuki, H., Yamaguchi, E., Yoshiki, H., Wada, Y., & Watanabe, A. (2014). Hip muscle activity during isometric contraction of hip abduction. Journal of Physical Therapy Science, 26(2), 187–190. https://doi.org/10.1589/jpts.26.187
- Kwilas, A. R., Donahue, R. N., Tsang, K. Y., & Hodge, J. W. (2015). 乳鼠心肌提取 HHS public access. Cancer Cell, 2(1), 1–17. https://doi.org/10.1016/j.jbiomech.2020.109968.Dysplastic
- Larruskain, J., Lakue, J. A., Diaz, N., Odriozola, A., & Gil, S. M. (2017). A comparison of injuries in elite male and female football players: A five – season prospective study. Scandinavian Journal of Medicine & Science in Sports, February(1), 237–245. https://doi.org/10.1111/sms.12860
- Lovell, G. A., Blanch, P. D., & Barnes, C. J. (2012). EMG of the hip adductor muscles in six clinical examination tests. Physical Therapy in Sport, 13(3), 134–140. https://doi.org/10.1016/j.ptsp.2011.08.004
- Markovic, G., Šarabon, N., Pausic, J., & Hadžić, V. (2020). Adductor muscles strength and strength asymmetry as risk factors for groin injuries among professional soccer players: a prospective study. Environmental Research and Public Health, 17(4946), 1–9. https://doi.org/10.3390/ijerph17144946
- Marušič, J., & Šarabon, N. (2022, October). Hip adduction and abduction strength in youth male soccer and basketball players with and without groin pain in the past year. PLoS ONE, 17(10), 1–13. https://doi.org/10.1371/journal.pone.0275650
- Neumann, D. A. (2010). Kinesiology of the hip: A focus on muscular actions. Journal of Orthopaedic and Sports Physical Therapy, 40(2), 82–94. https://doi.org/10.2519/jospt.2010.3025
- Nicholas, S. J., & Tyler, T. F. (2002). Adductor muscle strains in sport. Sports Medicine, 32(5), 339–344. https://doi.org/10.2165/00007256-200232050-00005
- Nielsen, M. F., Thorborg, K., Krommes, K., Thornton, K. B., Hölmich, P., Peñalver, J. J. J., & Ishøi, L. (2022). Hip adduction strength and provoked groin pain: A comparison of long-lever squeeze testing using the ForceFrame and the Copenhagen 5-second-squeeze test. Physical Therapy in Sport, 55(February), 28–36. https://doi.org/10.1016/j.ptsp.2022.02.002
- Ralston, B., Arthur, J., Makovicka, J. L., Hassebrock, J., Tummala, S., Deckey, D. G., Patel, K., Chhabra, A., & Hartigan, D. (2020). Hip and groin injuries in national collegiate athletic association women’s soccer players. Orthopaedic Journal of Sports Medicine, 8(1), 232596711989232. https://doi.org/10.1177/2325967119892320
- Schache, A. G., Woodley, S. J., Schilders, E., Orchard, J. W., & Crossley, K. M. (2016). Anatomical and morphological characteristics may explain why groin pain is more common in male than female athletes. Br J Sports Med Month, 51(7), 554–555. https://doi.org/10.1136/bjsports-2016-096945
- Schober, P., & Schwarte, L. A. (2018). Correlation coefficients: Appropriate use and interpretation. Anesthesia and Analgesia, 126(5), 1763–1768. https://doi.org/10.1213/ANE.0000000000002864
- Serner, A., Tol, J. L., Jomaah, N., Weir, A., Whiteley, R., Thorborg, K., Robinson, M., & Hölmich, P. (2005). Diagnosis of acute groin injuries: a prospective study of 110 athletes. American Journal of Sports Medicine, 42(8), 1857–1864. https://doi.org/10.1177/0363546515585123
- Spudić, D., Vodičar, J., & Hadžić, V. (2023). Validity and reliability of hip strength assessment using a frame-stabilized dynamometer system device. Measurement in Physical Education and Exercise Science, 27(3), 269–282. https://doi.org/10.1080/1091367X.2023.2171796
- Thorborg, K., MSportsphysio, B., Nielsen, S., P, M., Tang, L., Nielsen, M. B., & Hölmich, P. (2014). Eccentric and isometric hip adduction strength in male soccer players with and without adductor-related groin pain: An assessor-blinded comparison. Orthopaedic Journal of Sports Medicine, 2(2). https://doi.org/10.1177/2325967114521778
- Thorborg, K., Serner, A., Petersen, J., Moller Madsen, T., Magnusson, P., & Hölmich, P. (2011). Hip adduction and abduction strength profiles in elite soccer players: Implications for clinical evaluation of hip adductor muscle recovery after injury. The American Journal of Sports Medicine, 39(1), 121–126. https://doi.org/10.1177/0363546510378081
- Ward, S. R., Winters, T. M., & Blemker, S. S. (2010). The architectural design of the gluteal muscle group: Implicati ons for movement and rehabilitation. Journal of Orthopaedic and Sports Physical Therapy, 40(2), 95–102. https://doi.org/10.2519/jospt.2010.3302
- Weir, A., Brukner, P., Delahunt, E., Ekstrand, J., Griffin, D., Khan, K. M., Lovell, G., Meyers, W. C., Muschaweck, U., Orchard, J., Paajanen, H., Philippon, M., Reboul, G., Robinson, P., Schache, A. G., Schilders, E., Serner, A., Silvers, H., Thorborg, K. … Hölmich, P. (2015). Doha agreement meeting on terminology and definitions in groin pain in athletes. British Journal of Sports Medicine, 49(12), 768–774. https://doi.org/10.1136/bjsports-2015-094869
- Werner, J., Hägglund, M., Waldén, M., & Ekstrand, J. (2009). UEFA injury study: A prospective study of hip and groin injuries in professional football over seven consecutive seasons. British Journal of Sports Medicine, 43(13), 1036–1040. https://doi.org/10.1136/bjsm.2009.066944
- Wollin, M., Thorborg, K., Welvaert, M., & Pizzari, T. (2018). In-season monitoring of hip and groin strength, health and function in elite youth soccer: Implementing an early detection and management strategy over two consecutive seasons. Journal of Science and Medicine in Sport, 21(10), 988–993. https://doi.org/10.1016/j.jsams.2018.03.004