
Abstract
Many studies into surface contamination of hospital environments have demonstrated that occupational exposure to cytotoxics through the dermal route remains a possible risk. In this study, we assess the actual dermal exposure of the hands of pharmacy technicians and cleaning personnel in a panel of hospitals performing tasks that pose a risk of exposure. We compare the dermal exposure to a tentative limit value for cyclophosphamide. Pharmacy technicians and cleaning personnel were asked for hand rinsing after performance of nine tasks previously identified as posing a risk of occupational exposure. All samples were analyzed for the presence and quantity of eight antineoplastic drugs. By using data on both the frequency of the performance of the tasks and the measured dermal contamination during these tasks, weekly exposure to the marker drug (cyclophosphamide) was calculated. In five Dutch hospitals, 70 hand rinse samples and 8 blanks were collected. These were analyzed and results were used to calculate weekly exposure. The tentative limit value used was 0.74 µg of cyclophosphamide. For cleaning personnel, all results remained below this threshold value. For pharmacy technicians, the compounding itself also remained well below the limit; however, the task involving preparatory work, as well as the checking of compounded drugs, had a 13% chance of exceeding the limit. All of the highest values were found when employees were not wearing gloves on these tasks. Cleaning personnel and pharmacy technicians compounding cytotoxic drugs in our study were sufficiently protected from occupational exposure. In contrast, pharmacy technicians who perform preparatory and finishing tasks (before and after the actual compounding) are not protected enough when they do not wear gloves.
Introduction
Occupational exposure to antineoplastic drugs has been demonstrated to cause adverse health effects in hospital staff. Since the late 1970s, several studies (Selevan et al. Citation1985; Stücker et al. Citation1990; Valanis et al. Citation1999; Fransman et al. Citation2007) have demonstrated negative effects of cytotoxic exposure on reproduction in humans, and even though a direct effect on cancer incidence has never been proven irrefutably, oncogenicity of prolonged exposure to traces of these drugs cannot be ruled out. A direct correlation between surface exposure to certain levels of antineoplastics and harmful effects is very difficult to establish, as reviewed by Kibby (Citation2017) and thus hospital management should aim for zero exposure. As zero is in general not easy to measure, we use the “as low as reasonably achievable” (ALARA principle), taking into account the current status of scientific and technical possibilities to achieve an exposure as low as possible (EC directive 2004/37/EC Citation2004; NIOSH Citation2004).
There are three distinct pathways through which internal exposure can occur: by oral ingestion, inhalation, or dermal contact (including ocular exposure). Both oral and ocular exposure can easily be prevented by using adequate protective gear and establishing hygienic work protocols. The inhalation route can be minimized, for example, by compounding in a biological safety cabinet or isolator and by wearing respiratory protection during risky tasks. As such, the dermal route is generally considered to be the major pathway through which occupational exposure occurs (Fransman et al. Citation2005). This potential route of exposure has been substantiated by several studies showing that gloves can be permeated by cytotoxic drugs (Wallemacq et al. Citation2006) as well as by studies finding cytotoxic traces on the hands of health care workers despite the use of gloves (Hon et al. Citation2014) and on the inside of gloves worn during preparation and administration of cytotoxic drugs (Turci et al. Citation2003).
Several methods to assess dermal exposure exist: taking wipe samples of the skin, using biomonitoring by collection of urine or blood, wearing pads on possibly exposed skin or using washing or rinsing methods. The rinsing method is expected to provide an accurate measure of actual dermal exposure as it calculates the actual amount of cytotoxic on the skin (Fransman et al. Citation2005; Ng et al. Citation2014) rather than extracting cytotoxics from gloves or pads, while it is less invasive than biomonitoring. Hands are the most likely skin area to be contaminated with cytotoxics, as most tasks involving cytotoxics are done using the hands. Therefore, washing samples of hands as opposed to other body parts will eliminate the possibility of underestimating skin exposure. Several previous studies have examined hand exposure to antineoplastic drugs, mainly cyclophosphamide. A previous trial from the Netherlands by Fransman et al. (Citation2007) found considerable actual hand exposure in nurses and in pharmacy technicians and cleaning personnel, which was later substantiated by Italian (Turci et al. Citation2003), French (Crauste-Manciet et al. Citation2005), and Canadian (Hon et al. Citation2014) studies measuring contamination of used gloves or hands. Cleaning personnel, especially, could potentially be at risk, as several studies showed high levels of contamination on floors of both the pharmacy as well as wards and patient toilets (Hedmer et al. Citation2008; Connor et al. Citation2010; Fleury-Souverain et al. Citation2015; Chauchat et al. Citation2019).
Since the beginning of this century, regulations on safe handling of antineoplastic drugs have evolved in the Netherlands by continuously evaluating and updating mandatory guidelines within the health care sector. The aim of this study was to assess the dermal exposure to cytotoxic agents of pharmacy technicians and cleaning personnel during routine work practice in Dutch hospitals and to check this actual dermal exposure against a previously established tentative limit value.
Methods
Setting
The study was performed in five hospitals, including a large academic center as well as regular community hospitals. In each hospital, the national guidelines for safe working with cytotoxics had been implemented previously. These guidelines from the Society for the labor market in hospitals (Stichting Arbeidsmarkt Ziekenhuizen (STAZ) Citation2012) include the following for pharmacies: (a) the use of a separate, dedicated room to compound cytotoxics with entry through a lock; (b) recirculation of air from the compounding room should be zero percent; (c) preparation must be performed in a safety cabinet or isolator with negative air pressure; (d) use of (semi)closed needle-free drug transfer systems (two types of devices are allowed under this regulation: closed-system transfer devices or spikes, which are vented, needle-free devices); (e) the use of fully protective clothing including footwear, which should be changed at least daily; and (f) double packaging of compounded cytotoxics for transport. Because the compounding of the cytotoxics has to take place in a separate clean-room, all hospitals use one or more adjacent rooms for the pre- and post-compounding process, comprising the gathering of materials, printing of labels, and checking the final product. For cleaning, the guidelines specify: (a) use of a daily cleaning protocol with a dedicated set of cleaning equipment; (b) cleaning must start from the cleanest surface area working toward the most contaminated surface area; (c) personal protective equipment including gloves should be worn during cleaning; and (d) performance of annual wipe tests to check the efficacy of the cleaning protocol. Pharmacy technicians are responsible for the cleaning of the safety cabinets, while the cleaning of the pharmacy facility, including the clean rooms where compounding takes place, is performed by the cleaning staff. Formal ethical approval for this study was deemed not necessary by the medical ethics committee.
Survey into the frequency and duration of tasks
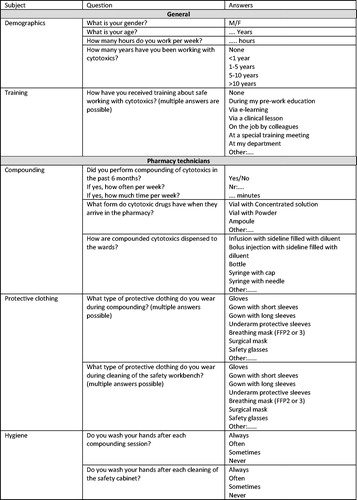
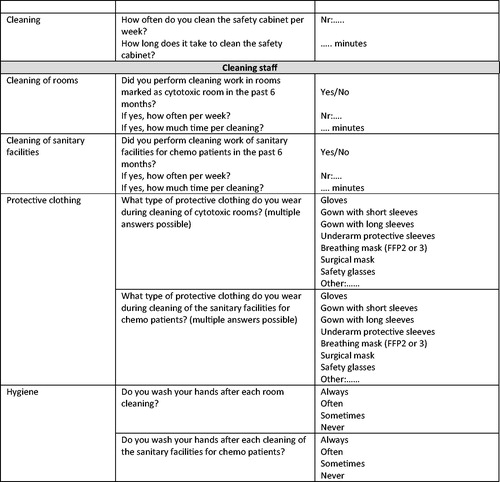
A survey into the frequency of performance of tasks involving cytotoxic drugs and duration of these tasks was prepared by the researchers and sent out online prior to the collection of the samples to pharmacy technicians and cleaning personnel of 8 different hospitals. The questionnaire is shown in . The online questionnaire was brought to the attention of the workers via their supervisor, and participation was voluntary. The questionnaire remained open for two months to collect responses. In addition, short interviews were held to check the frequency and duration of the tasks with the participants during the on-site investigations, and adherence to the guidelines (e.g., the use of gloves) was checked by observation by the analyst performing the sampling.
Figure 1. Questionnaire into frequency and duration of tasks involving cytotoxic drugs.
Hand rinse sampling strategy
Nine tasks that involve direct cytotoxic handling of cyclophosphamide (for pharmacy technicians) or cleaning of possibly contaminated areas (for cleaning personnel) were chosen for assessment. These tasks comprised the following: aseptic reconstitution (compounding technician), helping the compounding technician (the second technician in the compounding room who disinfects starting materials, and serves as the checker for measured volumes), cleaning the biological safety cabinet (technician), preparatory work for the reconstitution process (i.e., gathering of materials, printing labels, technician), checking the final product (technician), cleaning patient rooms (cleaner), cleaning the outpatient (daycare) unit (cleaner), cleaning the pharmacy (cleaner), and cleaning sanitary facilities on oncology wards/outpatient unit (cleaner).
After finishing each task, the circumstances (date, time and, if applicable, deviations from the use of personal protective equipment protocols) were registered. Next, the employee washed his or her hands in 250-mL 10%-isopropyl alcohol in water solution as previously described by Fransman et al. (Citation2005). In addition, 8 field blanks were taken at the different hospitals on the same day of the study samples by filling a sample bag with just 250 mL of 10%-isopropyl alcohol in water solution. These field blanks were anonymized and sent along with the study samples to be analyzed for comparison. Samples were immediately frozen and shipped to the analyzing laboratory.
Sample preparation and analysis
All samples were analyzed for the presence and quantity of eight cytotoxic drugs (). Samples were prepared and analyzed by a previously published validated LC-MS/MS procedure (Tuerk et al. Citation2011), consisting of extraction by sonification with deionized water that was produced in-house in the analytical laboratory with an Elix-10-Milli-Q plus water purification system (Millipore, Eschborn, Germany), followed by filtration through a regenerated cellulose acetate syringe filter (Macherey-Nagel, Dueren, Germany). Analysis was carried out using a 1100 binary pump (Agilent Technologies, Waldbronn, Germany) with an HTS-PAL autosampler (CTC Analytics, Zwingen, Switzerland). The injection volume was set at 20 µL. Separation of the eight compounds was performed on a 50 × 3 mm Shim-Pack XR-ODS, 2.2 mm column (Shimadzu, Duisburg, Germany) at 30 °C and a flow rate of 300 µL/min. The binary gradient of 0.1% formic acid (Sigma Aldrich, Taufkirchen, Germany) in water (v/v, phase A) and 0.1% formic acid in acetonitrile (Sigma Aldrich, Taufkirchen, Germany, v/v, phase B) consisted of the following steps: 0–0.55 min 5% B, 12 min 80% B, 13 min 80% B, 20 min 5% B. Detection was performed with an API 3000 triple quadruple mass spectrometer (Applied Biosystems MDS Sciex, Darmstadt, Germany) equipped with TurboIonSprayTM interface operating at 450 °C in positive and negative mode with ion spray probe voltages of 5000 V and −4500 V. To enable measuring in positive and negative mode within one run, a settling time of 700 millisecond (ms) was installed. The parameter settings for nebulizer, curtain, and collision gases (nitrogen each) were 15, 12, and 6 arbitrary units, respectively. The antineoplastic drugs were detected by multiple reaction monitoring (MRM). The pause time was set at 5 ms and the dwell times at 100 ms. lists the analyzed drugs and the limits of detection (LOD).
Table 1. Analyzed cytotoxics and their limit of detection in hand rinse samples.
Analysis of exposure and calculation of risks
For several cytotoxics, limit values for private or public environments in air have been established by the European Health Council. Official limit values for dermal exposure or surface contamination, however, do not exist. In 2006, a tentative health-based limit value for weekly dermal exposure was set by Fransman et al. based on data from a study in nurses. This limit value amounted to a maximum of 0.74 µg dermal exposure of the hands per week using cyclophosphamide as a marker for total cytotoxic exposure. Nurses who had been exposed at levels above this value experienced reproductive effects: time to conceive was significantly prolonged, and offspring with a lower birth weight was observed (Fransman et al. Citation2007). Even though tasks performed by nurses differ from tasks performed by pharmacy technicians and cleaning personnel, we used the same limit value for dermal exposure, based on the assumption that cyclophosphamide concentrations are a good representation of the mix of cytotoxics that employees are potentially exposed to, because cyclophosphamide is still handled on a daily basis in all participating hospitals. Moreover, adverse health effects are not different in the job categories.
To calculate the actual weekly dermal exposure to cyclophosphamide, the measured dermal exposure per task was multiplied with the frequency at which the task was performed, as given by the employees during the survey and interview part of the study. The sums of these task exposures were calculated per staff type, so the total weekly exposure for a pharmacy compounding technician, for example, consists of the weekly exposure when compounding, plus the weekly exposure when helping the compounder, plus the weekly exposure when cleaning the safety cabinet. The following calculations were used:
Weekly exposure pharmacy compounding technician =
(frequency compounding * dermal contamination after compounding) +
(frequency compounding * dermal contamination after compounding help) +
(frequency cleaning safety cabinet * dermal contamination after cleaning safety cabinet)
Weekly exposure pharmacy technician doing preparatory and checking tasks =
(frequency compounding * dermal contamination after preparatory tasks) +
(frequency compounding * dermal contamination after checking tasks)
Weekly exposure cleaner =
(frequency cleaning cytotoxic rooms * dermal contamination after cleaning cytotoxic rooms) +
(frequency cleaning chemo patients’ sanitary facilities * dermal contamination after cleaning chemo patients’ sanitary facilities)
These calculations were performed using Excel (Microsoft Office 2016, Microsoft, Redmond, USA). In these calculations, special consideration was given to the data that were below the limit of detection (LOD), because it is uncertain whether these values are zero, or lie somewhere between zero and the LOD. For these so called non-detectables, the values were estimated based on the statistical variation of the data in the measurable range. This approach, using the NDexpo-tool (University of Montreal, Montreal, Canada, http://www.expostats.ca/site/app-local/NDExpo/apropos_en.htm) and described by Helsel, assigns a predicted value to each result below the LOD (Helsel Citation2012).
Subsequently, for pharmacy technicians and cleaning personnel, Monte Carlo simulations were performed to evaluate the variability and uncertainty of the data, with the aim of calculating the weekly exposure (median, 10th and 90th percentile) and the probability of exceeding the limit value (Cullen and Frey Citation1999; Meyster et al. Citation2006). For concentration and frequency, log-normal distributions were assigned, and for tasks that were mutually exclusive (the pharmacy technician cannot be the compounder as well as the compounder help at the same time) a Bernoulli distribution was assigned. For each job category, 10,000 Monte Carlo simulations were performed using the Excel add-in ModelRisk Software (Vose software, Sint-Amandsberg, Belgium).
Results
Survey into the frequency and duration of tasks
In total, 71 pharmacy technicians and 40 hospital cleaners completed at least part of the questionnaire, providing frequency and duration of tasks where a potential risk of exposure to cytotoxic substances exists. In addition, because this questionnaire was performed before the actual measurements, small interviews to obtain confirmation of the frequency and duration of tasks were held during sample collection. The results for the compounder and compounder help are identical by nature because they perform each task together. The preparatory and checking work (pre- and post-compounding) by the pharmacy technician were estimated at the same duration and are also the same in frequency by nature, because each compounding has to be preceded by preparatory work and followed by checking of the compounded drug. The results of the survey are given in . During sampling, adherence to the guidelines was checked through observation by the independent analyst taking the samples. Non-adherence to the use of gloves by the pharmacy technicians was found in the preparatory tasks (50%) and in checking of compounded drugs (57%) as well as by the cleaning staff on several occasions (11%). In addition, the material and brand of the used gloves was recorded during sampling. For compounding and cleaning of the hoods, only gloves complying with EN 374-3 2003 (resistant to chemicals for a minimum of 30 min) are allowed, with different brands in use in different hospitals (the materials being nitrile, latex and polychloroprene). For the other tasks, the same or other gloves in non-sterile variants were used. An overview is given in online supplemental materials.
Table 2. Survey results into the frequency and duration of tasks where exposure to cytotoxics can occur.
Dermal exposure of the hands to cytotoxic drugs
In total, 70 hand rinse samples were analyzed together with 8 blanks. For the pharmacy technicians, the following number of hand rinse samples were obtained from 25 individuals: aseptic reconstitution 12, helping the compounding technician 5, cleaning the biological safety cabinet 9, preparatory work for the reconstitution process 10, and checking the final product 7. For the cleaners, hand rinse samples were obtained from 20 individuals in the following numbers: cleaning patient rooms 9, cleaning the outpatient unit 3, cleaning the pharmacy 6, and cleaning sanitary facilities on oncology wards/outpatient unit 9. The 70 hand rinse samples were obtained from 45 individuals.
Methotrexate and docetaxel were not detectable in any of the samples. Paclitaxel, 5-fluorouracil and etoposide were present in detectable quantities in one sample each. The drug present in the largest number of samples was cyclophosphamide, which was expected, as we performed the measurements on days that cyclophosphamide was handled. Hands from the pharmacy technicians showed contamination more often than the hands of the cleaning personnel, in 11 out of 43 vs. 6 out of 27 cases. Hands of the pharmacy technicians that showed contamination were contaminated with more than one drug in 38% of cases. For the cleaning staff, only single contamination with either cyclophosphamide (n = 5) or gemcitabine (n = 1) was detected. All the field blanks showed negative results for all analyzed cytotoxics. Seventeen of the hand rinse samples of pharmacy technicians were taken after preparatory (before compounding) or checking (after compounding) tasks. In five of the 17 samples, cyclophosphamide was detected. In these positive samples, 4 came from technicians who wore no gloves when performing the task (80% of the positive samples), whereas one came from a technician who did wear gloves (20%). In the tasks compounder and compounder help, all technicians wore gloves. For the cleaning tasks, gloves were worn in the majority of cases, only on three occasions when an employee cleaned a patient room, this was done without gloves. In all of these three, detectable cyclophosphamide concentrations on the hands were found. The results of the hand rinse samples are summarized in and detailed data are provided in supplemental file B. No single measurement was above the weekly threshold value.
Table 3. Contamination in the hand rinse samples (in µg/L).
Weekly exposure to cyclophosphamide
The calculated weekly exposure to cyclophosphamide on the hands for (a) pharmacy compounding technician, (b) pharmacy technician doing preparatory and checking tasks, and (c) cleaning personnel is given in . All median values were well below the limit value of 0.74 µg cyclophosphamide per week: 0.05 µg per week for compounding technicians, 0.15 µg per week for the technicians performing preparatory work and final checking, and 0.02 µg per week for cleaning personnel. For the pharmacy technicians involved in compounding as well as for the cleaning staff (irrespective of whether gloves were worn), the 90th percentile also remained well below the limit level. However, the pharmacy technicians performing the preparatory tasks and the final checking, showed a large variability in exposure, resulting in a relatively high probability of exceeding the limit value (13%).
Table 4. Calculated weekly exposure to cyclophosphamide on the hands per function type.
Discussion
The present study shows that, in general, the working protocols for the compounding of cytotoxic drugs and the cleaning of areas that may be contaminated with cytotoxic drugs function well in protecting workers from occupational exposure. However, the pharmacy technicians who perform preparatory tasks such as gathering the required vials for compounding, although remaining below the limit value on average, have a risk of exceeding this value. The most likely explanation for this finding is that exposure occurs from vials that are contaminated on the outside. This is a well-known phenomenon, studied most extensively by Favier et al. (Citation2003), who measured external contamination on commercial vials containing cytotoxic drugs and found a contamination rate of 100% in over 800 tests. Post-compounding handling could contribute in theory, as we did not measure pre- and post-compounding tasks independently, but seems to be less likely, since a previous study in a panel of nine Dutch hospitals by Breukels et al. (Citation2018) showed no contamination on the outside of prepared infusion bags containing cytotoxics. In the Netherlands, wearing gloves when performing tasks not directly involving compounding, administration, patient contact, or cleaning is not mandatory, although it is recommended by the National Pharmacists Association. The observation that cleaning and compounding results in very low levels of exposure proves that the Dutch guidelines on personal protective equipment as well as the use of spikes in a biological safety cabinet, provide good risk control.
To date, there is a large, mainly industry-driven lobby that strives for making the use of expensive close system devices (CSTDs) for compounding cytotoxic drugs mandatory. However, our results show that the present protocols using spikes in safety cabinets provide adequate protection. This finding is substantiated by a recent study in a large cohort of 83 hospitals in Canada by Chauchat et al. (Citation2019), which showed no benefit from reducing surface contamination by using such devices, as well as by a large Cochrane meta-analysis by Gurusamy et al. (Citation2018) on the same subject, which concluded that there is no scientific basis for the implementation of CSTDs. Moreover, our results show that our aims to improve worker protection further, should better be directed at the preparatory tasks in the pharmacy before the actual compounding, as we show that these result in the highest levels of exposure and probability of exceeding the threshold limit.
Our results are in accordance with several previous studies using mainly wipe sampling of surfaces as a measure of exposure risks. We chose the hand rinsing approach rather than surface or hand wiping to enable direct comparison with the previous Dutch studies by Fransman et al. (Citation2005, Citation2007) without having to adjust for a potential difference in recovery between the two methods. A very large study from Germany by Schierl et al. (Citation2009) including 1,008 wipe sample results from hospital surface monitoring programs revealed high levels of contamination on storage shelves and floors, which is a strong indicator that in German hospitals, preparatory tasks in the pharmacy could pose a risk of unintended exposure as well. An earlier Dutch benchmark trial in nine hospital pharmacies by Crul and Simons-Sanders (Citation2018) also found contamination on surfaces in rooms adjacent to the actual compounding cleanrooms, which has also been described in a U.S. trial by Connor et al. (Citation2010), especially in those pharmacies where compounding was executed in areas that were open to adjoining rooms. Finally, a Swedish multicenter study by Hedmer et al. (Citation2008) also showed high concentrations of surface contaminations in rooms adjacent to the compounding area (dressing rooms) in the pharmacy and in utility rooms in the wards. Studies looking directly at the hands of workers are sparser. One study that was conducted in the Netherlands, demonstrated hand exposure of pharmacy technicians, nurses and cleaning personnel (Fransman et al. Citation2005), but this study stems from before the National Guidelines were issued. In a Canadian study, Hon et al. (Citation2014) wiped the hands of a large panel of personnel from six hospitals, and also found that exposure was higher in personnel not actually involved in the potentially most risky tasks such as compounding or administration.
Our study investigated a large number of hand rinse samples in a cohort of different hospitals. The use of rinsing of the hand gives a closer estimate to actual dermal exposure than merely wiping surfaces, as it is hard to estimate internal exposure from surface contamination levels (Kibby Citation2017). Moreover, we tested the measured levels to a limit value below which exposure does not lead to reprotoxic effects, as demonstrated by Fransman et al. (Citation2007). Some limitations to our study have to be considered however, when interpreting the results. First, we used cyclophosphamide as a marker compound for a range of cytotoxic drugs to calculate weekly exposure, as was done in the study among Dutch nurses in which the limit value was determined. In practice, workers are exposed to an ever-expanding panel of antineoplastics. It cannot be excluded that a change in composition of this panel of cytotoxic drugs may influence the toxicity of the whole set of cytotoxics. However, cyclophosphamide is most likely a good marker drug, as it is still a widely and frequently used cytotoxic drug in hospitals and therefore still a dominant drug in the whole set of cytotoxics currently used. Second, only hospitals from one country were included, and thus the results may not be extrapolated to other nations, where other guidelines on safe handling might be in practice. Also, a sample of five hospitals from the original eight were included in the sampling study. Third, participation for hospitals was voluntary, which could bias the results, as it is possible that those hospitals where the guidelines were not implemented fully, were more likely to decline participation.
Further attempts to reduce occupational exposure to cytotoxic drugs should aim to decrease the contamination of materials, especially commercial vials. In addition, it is pivotal to promote the use of personnel protective gear, especially gloves, for those workers who can come into contact with possible sources of contamination, even though they are not directly involved in the tasks that are generally considered to be the most dangerous.
Conclusions
In conclusion, we have shown that pharmacy technicians involved in the compounding of chemotherapy and cleaning personnel involved in the cleaning of oncology wards and pharmacy premises were sufficiently protected against occupational exposure in our study. The pharmacy technicians involved in pre- and post-compounding activities, however, are not protected as adequately when they do not wear gloves. For this category of activities, improvement of practices is advised.
Supplemental Material
Download MS Word (34.5 KB)Conflict of interest
All authors declare no conflict of interest
Additional information
Funding
References
- Breukels O, van der Gronde T, Simons-Sanders K, Crul M. 2018. Antineoplastic drug contamination on the outside of prepared infusion bags. Int J Pharm Compd. 22(4):345–349.
- Chauchat L, Tanguay C, Caron NJ, Gagné S, Labrèche F, Bussières JF. 2019. Surface contamination with ten antineoplastic drugs in 83 Canadian centers. J Oncol Pharm Pract. 25(5):1089–1098. doi:10.1177/1078155218773862
- Connor TH, DeBord DG, Pretty JR, Oliver MS, Roth TS, Lees PSJ, Krieg EF, Rogers B, Escalante CP, Toennis CA, et al. 2010. Evaluation of antineoplastic drug exposure of health care workers at three university-based US cancer centers. J Occup Environ Med. 52(10):1019–1027. doi:10.1097/JOM.0b013e3181f72b63
- Crauste-Manciet S, Sessink PJM, Ferrari S, Jomier J-Y, Brossard D. 2005. Environmental contamination with cytotoxic drugs in healthcare using positive air pressure isolators. Ann Occup Hyg. 49(7):619–628. doi:10.1093/annhyg/mei045
- Crul M, Simons-Sanders K. 2018. Carry-over of antineoplastic drug contamination in Dutch hospital pharmacies. J Oncol Pharm Pract. 24(7):483–489. doi:10.1177/1078155217704990
- Cullen AC, Frey HC. 1999. Probabilistic techniques in exposure assessment: a handbook for dealing with variability and uncertainty in models and inputs. New York: Plenum Press.
- EC directive 2004/37/EC. 2004. Directive 2004/37/EC of the European parliament and of the council on the protection of workers from the risks related to exposure to carcinogens or mutagens at work (Sixth individual Directive within the meaning of Article 16(1) of Council Directive 89/391/EEC). April 29. http://eur-ex.europa.eu/LexUriServ/LexUriServ.do?uri¼OJ:L:2004:229:0023:0034:EN:PDF.
- Favier B, Gilles L, Ardiet C, Latour JF. 2003. External contamination of vials containing cytotoxic agents supplied by pharmaceutical manufacturers. J Oncol Pharm Pract. 9(1):15–20. doi:10.1191/1078155203jp102oa
- Fleury-Souverain S, Mattiuzzo M, Mehl F, Nussbaumer S, Bouchoud L, Falaschi L, Gex-Fabry M, Rudaz S, Sadeghipour F, Bonnabry P, et al. 2015. Evaluation of chemical contamination of surfaces during the preparation of chemotherapies in 24 hospital pharmacies. Eur J Hosp Pharm. 22(6):333–341. doi:10.1136/ejhpharm-2014-000549
- Fransman W, Vermeulen R, Kromhout H. 2005. Dermal exposure to cyclophosphamide in hospitals during preparation, nursing and cleaning activities. Int Arch Occup Environ Health. 78(5):403–412. doi:10.1007/s00420-004-0595-1
- Fransman W, Roeleveld N, Peelen S, de Kort W, Kromhout H, Heederik D. 2007. Nurses with dermal exposure to antineoplastic drugs: reproductive outcomes. Epidemiology. 18(1):112–119. doi:10.1097/01.ede.0000246827.44093.c1
- Gurusamy LS, Best KM, Tanguay C, Lennan E, Korva M, Bussieres J-F. 2018. Closed-system drug-transfer devices plus safe handling of hazardous drugs versus safe handling alone for reducing exposure to infusional hazardous drugs in healthcare staff. Cochrane Database Syst Rev. 3(3):CD012860. doi:10.1002/14651858.CD012860.pub2.
- Hedmer M, Tinnerberg H, Axmon A, Jönsson BAG. 2008. Environmental and biological monitoring of antineoplastic drugs in four workplaces in a Swedish hospital. Int Arch Occup Environ Health. 81(7):899–911. doi:10.1007/s00420-007-0284-y
- Helsel RD. 2012. Statistics for censored environmental data using minitab and R. Hoboken, NJ: John Wiley & Sons.
- Hon CY, Teschke K, Demers PA, et al. 2014. Antineoplastic drug contamination on the hands of employees working throughout the hospital medication system. Ann Occup Hyg. 58:761–770. doi:10.1093/annhyg/meu019
- Kibby T. 2017. A review of surface wipe sampling compared to biologic monitoring for occupational exposure to antineoplastic drugs. J Occup Environ Hyg. 14(3):159–174. doi:10.1080/15459624.2016.1237026
- Meyster T, Fransman W, van Hemmen J, et al. 2006. A probabilistic assessment of the impact of interventions on oncology nurses’ exposure to antineoplastic agents. Occup Environ Med. 63:530–537.
- Ng MG, de Poot S, Schmid K, Cowie H, Semple S, van Tongeren M. 2014. A preliminary comparison of three dermal exposure sampling methods: rinses, wipes and cotton gloves. Environ Sci Process Impacts. 16(1):141–147. doi:10.1039/c3em00511a
- NIOSH. 2004. Preventing occupational exposure to antineoplastic and other hazardous drugs in health care settings. Publication Number 2004-165.
- Schierl RA, Bohlandt A, Nowak D. 2009. Guidance values for surface monitoring of antineoplastic drugs in German pharmacies. Ann Occup Hyg. 53(7):703–711. doi:10.1093/annhyg/mep050
- Selevan SG, Lindbohm ML, Hornung RW, Hemminki K. 1985. A study of occupational exposure to antineoplastic drugs and fetal loss in nurses. N Engl J Med. 313(19):1173–1178. doi:10.1056/NEJM198511073131901
- Stichting Arbeidsmarkt Ziekenhuizen (STAZ). 2012. Branche-afspraak cytotoxica ziekenhuizen. https://www.betermetarbo.nl/fileadmin/user_upload/Gevaarlijke_stoffen/Branche-afspraak-Cytotoxica.pdf.
- Stücker I, Caillard JF, Collin R, Gout M, Poyen D, Hémon D. 1990. Risk of spontaneous abortion among nurses handling antineoplastic drugs. Scand J Work Environ Health. 16(2):102–107. doi:10.5271/sjweh.1811
- Turci R, Sottani C, Spagnoli G, Minoia C. 2003. Biological and environmental monitoring of hospital personnel exposed to antineoplastic agents: a review of analytical methods. J Chrom B. 789(2):169–209. doi:10.1016/S1570-0232(03)00100-4
- Tuerk J, Kiffmeyer TK, Hadtstein C, Heinemann A, Hahn M, Stuetzer H, Kuss H-M, Eickmann U. 2011. Development and validation of an LC-MS/MS procedure for environmental monitoring of eight cytotoxic drugs in pharmacies. Int J Environ Anal Chem. 91(12):1178–1190. doi:10.1080/03067319.2010.494769
- Valanis B, Vollmer WM, Steele P. 1999. Occupational exposure to antineoplastic agents: self-reported miscarriages and stillbirths among nurses and pharmacists. J Occup Environ Med. 41(8):632–638. doi:10.1097/00043764-199908000-00004
- Wallemacq PE, Capron A, Vanbinst R, Boeckmans E, Gillard J, Favier B. 2006. Permeability of 13 different gloves to 13 cytotoxic agents under controlled dynamic conditions. Am J Health Syst Pharm. 63(6):547–556. doi:10.2146/ajhp050197
