
Abstract
Respirable Crystalline Silica (RCS) is a hazardous substance with known effects that can be well correlated with exposure levels that still persist in many traditional sectors, such as construction or stone processing. In the past decade, exposure scenarios for RCS have been found in the sector of artificial stone processing. The aim of this study is to evaluate the levels of RCS in facilities specialized in the production of artificial stone countertops and other accessories for the furnishing of kitchens, bathrooms, and offices after the introduction of some preventive technical measures such as wet processing or local exhaust ventilation systems. The study involved 51 subjects in four facilities. Personal silica exposure assessment was carried out using GS3 cyclones positioned in the breathing zone during the work shift. Quantitative determination of silica was carried out by X-ray diffraction analysis. Respirable dust levels were in the range 0.046–1.154 mg/m3 with RCS levels within the range <0.003-0.098 mg/m3. The highest exposure was found in dry finishing operations. Although there was a remarkable reduction in RCS exposure levels compared to what was observed in the past before the introduction of preventive measures, the data still showed hazardous exposure levels for some of the monitored activities.
Introduction
At the end of the last century and, more recently during the early 2000s, new artificial materials with particular esthetical and technological characteristics (e.g., resistance to mechanical and chemical aggressions, flexibility, and workability) have been introduced in the stone processing sector in addition to the traditional natural stones (marble, granite, etc.).
These new engineering materials, which include quartz-resin stones and ceramic/porcelain stones, have found extensive use in furnishing and building coatings such as kitchen and bathrooms countertops, offices and shops, floor and wall coatings, thresholds and window sills, or furniture decoration (Hering et al. Citation2003; Kramer et al. Citation2012). Quartz-resin stones, also called agglomerates, reconstituted stones, or quartz conglomerates, are made of composites of quartz (the major filler) and colored glass, shells, metals, or mirrors, bound together by a polymer resin (Ophir et al. Citation2016), while the ceramic/porcelain products consist mainly of kaolin clays, feldspar, siliceous sands, and small percentages of other minerals. The latter do not contain binding resins and undergo a cooking at a temperature of about 1,200 °C.
The silica content in quartz-resin stones is about 70–90%, while the percentage of silica in ceramic products ranges from 10–30%. The silica content of quartz-resins is much higher than that of natural calcium-based stones, including limestone, certain varieties of marble (e.g., calcite, dolomite, and onyx) that contain little or no silica, and ceramic products whose silica contents is comparable to that of granite and in the range of 10–45% (OSHA Occupational Safety and Health Administration, NIOSH National Institute for Occupational Safety and Health Citation2015). Processing artificial stones involves a series of mechanical processes including cutting, drilling, sanding, and polishing of slabs, all performed with water-cooled machinery to reduce the dustiness (wet processing). Subsequently, the produced pieces are subjected to some additional finishing processing (such as smoothing of the edges or holes) carried out manually (manual finishing). Manual finishing operations are performed by the use of hand-held equipment (e.g., angle grinders), in most of cases, without the water dust suppression (dry finishing).
More rarely, the tools are water feed (wet finishing). Workers involved in these tasks have the highest potential for exposure to respirable crystalline silica (RCS) dust.
During the past decade, an increased number of silicosis cases were reported in these manufacturing setting. The first report of artificial stone-associated silicosis was published in Spain in 2010, where three cases of silicosis were highlighted in young workers involved in the installation of quartz agglomerate surfaces in buildings and exposed to high levels of aerosolized silica during the decoration and installation phases of countertops for bathrooms and kitchens (Martínez et al. Citation2010). Since that publication, other cases have been reported in Spain and in other countries such as Israel, Italy, Australia, the United States, Belgium, and China (García Vadillo et al. Citation2011; Bartoli et al. Citation2012; Kramer et al. Citation2012; Friedman et al. Citation2015; Paolucci et al. Citation2015; Hoy et al. Citation2018; Ronsmans et al. Citation2019; Rose et al. Citation2019; Guarnieri et al. Citation2020; Wu et al. Citation2020). Because silicosis is an irreversible progressive and potentially fatal disease with no effective treatment, prevention through exposure control is fundamental.
The Occupational Safety and Health Administration (OSHA) and the National Institute for Occupational Safety and Health (NIOSH) in the United States have identified exposure to silica as a “health hazard to workers involved in manufacturing, finishing and installing natural and manufactured stone countertop products, both in fabrication shops and during in-home finishing/installation” (OSHA Occupational Safety and Health Administration, NIOSH National Institute for Occupational Safety and Health Citation2015).
Occupational exposure limits for RCS have been established in many countries. NIOSH and OSHA set an 8-hr time weighted average (TWA) occupational exposure limit value of 0.050 mg/m3. OSHA Permissible Exposure Limit (PEL) was updated in 2016, supplementing the standard with an action level of 0.025 mg/m3, which is equal to the value recommended by the American Conference of Governmental Industrial Hygienists (ACGIH®) as limit values (OSHA Citation2016; ACGIH Citation2010). In Europe, a binding TWA limit value of 0.100 mg/m3 was set by EU Directive 2017/2398 and transposed by several European countries (Directive (EU) Citation2017/2398 of the European Parliament and of the Council Citation2017).
The aims of this study are to assess the occupational exposure levels for respirable dust and RCS in Italian facilities where artificial stone processing were performed, identify the activities characterized by the highest exposure, and evaluate the effectiveness of preventive measures to reduce workers’ exposure.
Methods
Study population
The study was carried out from April 2018 to August 2019 on 51 subjects employed at 4 different facilities (labeled A, B, C, and D) located in Northern Italy and specializing almost exclusively in the processing of artificial stones. Before enrollment, all subjects involved received information about the aim of the study. The facilities ranged from small, with few employees (n = 6), to medium facilities, with several employees (n = 65). Three facilities (A, B, and C) mainly process large quartz-resin slabs for production of countertops for kitchens, shops, and furniture, while facility D processes only ceramic materials on medium and large slabs for the production of coverings used for construction and furniture. The characteristic of the facilities are summarized in .
Table 1. Characteristic of the facilities involved in the study.
Dust sampling and analysis
A total of 51 samples were collected in the four facilities investigated and specifically four samples in facility A, 9 samples in facility B, 29 samples in facility C, and 9 samples in facility D.
Personal exposure to respirable dust was assessed in all subjects in the breathing zone, using respirable cyclones (Model GS-3, SKC Inc., Eighty Four, PA) equipped with silver fiber filters (25 mm diameter, 0.8 μm pore size, model 45334, Sterlitech Corporation, Kent, WA) and connected to a battery-operated pump (Model XR5000, SKC Inc., Eighty Four, PA) operating at a flow rate of 2.75 L/min calibrated before and after each sampling using a primary standard calibrator (Model Dry Cal DC-LITE, Bios International Corporation, Butler, NJ). Sampling was carried out during all work activities and lasted throughout the entire work shift (8 hours).
Gravimetric analysis of dust collected on the filters was performed by weighing the filters before and after sampling using a microbalance with a detection threshold of 0.0005 mg (Model XPR6UD5, Mettler Toledo, Columbus, OH). To ensure standard weighing conditions, filters were allowed to equilibrate for a minimum of 48 hr in a climatic hood (Model Activa Climatic Cabinet, Aquaria, Milan, Italy) with constant temperature and humidity (20 ± 1 °C; 50 ± 5%, respectively) prior to weighing. Crystalline silica analysis of filter samples was performed by X-ray diffraction according to a direct-on-filter method (ISO 16258-1, Citation2015). The limit of detection was 5 µg per sample.
Statistical analysis
Statistical analysis was carried out using the software StatsDirect version 2.7.7 (StatsDirect Ltd, UK). A log-normal distribution of all variables was observed via the Shapiro-Wilk test. Differences between groups were assessed using a nonparametric test (Mann-Whitney U-test). Correlations between variables were assessed by linear regression analysis. In all tests, a p-value lower than 0.05 (two-tailed) was considered as statistically significant.
Results
The respirable dust and RCS levels found in the different facilities are shown in .
Table 2. Levels of airborne respirable dust and RCS exposure in facilities involved in the study.
All measured RCS levels were lower than the exposure limit mandated by the European Directive (0.100 mg/m3), although values near the limit were found in all facilities except facility B. Indeed, in facility B the levels of airborne respirable dust were significantly lower than those found in facilities A, C and D (p = 0.0112, p = 0.023, p < 0.0001, respectively), while the levels of RCS were significantly lower than those found in facilities C and D (p = 0.0007, p < 0.0001, respectively). 21.6% of all levels were over the limit value recommended by the AGCIH and the OSHA action level of 0.025 mg/m3 and 13.7% over the OSHA and NIOSH exposure limit values.
RCS levels measured in the facilities A and D, where comparable respirable dust exposure levels were found, showed, as expected, how the dispersion in air of this hazardous substance and consequently the occupational personal exposure was related to the silica content in the material processed (quartz-resin slabs with 90% of silica content vs. ceramic products with 30% of silica content, respectively).
The highest levels of exposure to airborne respirable dust and RCS were found for workers in the manual finishing process (). RCS levels were statistically higher than those found for mechanical processing workers (p = 0.047) and for workers involved in other job tasks such as bonding, packaging, or warehouse management (p = 0.03).
Table 3. Levels of airborne respirable dust and RCS exposure categorized by type of working process.
shows respirable dust and RCS levels found in the studied facilities during the manual finishing according to the processing method: with the use of water feed tools in order to reduce the exposure (wet) or with no-water feed tools (dry).
Table 4. Levels of airborne respirable dust and RCS exposure categorized by method of manual finishing.
Dry manual finishing produced higher amounts of respirable dust and silica than wet processing but the difference was statistically significant only for the respirable dust.
Although the quartz content in the materials used in facilities A, B, and C was approximately 90% by weight, as reported by manufacturers, we measured substantially lower quartz content in the sampled respirable dust with levels of 13%, 11%, and 19%, respectively. Even in facility D, which uses a ceramic material with a silica content of about 30%, the RCS content in the collected dust was lower (8%).
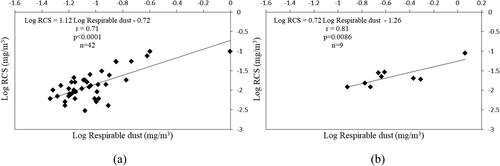
Significant correlations, reported in , were found between the respirable dust and the RCS content according to the worked material (r = 0.71, p < 0.0001 for quartz-resin material; r = 0.81, p = 0.0086 for ceramic material). The correlation improves for the quartz-resin material removing data from one worker (r = 0.85, p < 0.0001) who also manipulated marble with RCS content equal to 2% (data not shown).
Figure 1. Correlation between respirable dust and RCS content in the facility where quartz-resin (a) or ceramic (b) material were used.
Discussion
This study evaluated the exposure to RCS due to the artificial stone processing, materials that contain very high percentages of this hazardous substance (from 30–90%).
Despite many cases of silicosis were reported in literature in the artificial stones processing, at best of our knowledges, only few studies reported environmental monitoring data. Bartoli et al., in a study carried out on workers involved in the processing of artificial stone countertops, measured RCS levels in the range 0.011 and >0.519 mg/m3 (Bartoli et al. Citation2012). Another study reports a geometric mean of RCS exposure equal to 0.060 mg/m3 for workers performing tasks entirely wet and 0.87 mg/m3 for workers performing tasks entirely dry (Phillips et al. Citation2013). Two studies, that investigated artificial stone silicosis in patients, reported exposure histories of subjects in the range 0.260–0.744 mg/m3 (Guarnieri et al. Citation2020) or over 1 mg/m3 (Rosengarten et al. Citation2017).
The results of environmental monitoring in all workplaces investigated in our study showed personal occupational exposure to RCS lower than those found in the other studies (mean 0.022 mg/m3, range <0.003-0.098 mg/m3).
RCS content measured in the sampled respirable dust (from 8–19%) was lower than in the raw materials. This is consistent with previous findings where artificial stone countertops processed with a hand-held grinder in controlled laboratory tests were found to contain 91% total crystalline silica by weight while the respirable silica content for particles <10 µm ranged between 14% and 21% (Carrieri et al. Citation2020). In the same study, dust generated from grinding a natural stone sample made of granite contained 31% total silica but the silica content in the respirable fraction was 5% (Carrieri et al. Citation2020).
Although RCS levels found in this study were lower than those reported in literature, personal occupational exposure to RCS was high.
In our study, 21.6% of measured occupational levels of RCS were over the 0.025 mg/m3 action levels adopted by OSHA and recommended by ACGIH as limit value. Moreover, 13.7% of our data was over the OSHA PEL of 0.050 mg/m3 and in facilities A, C, and D, some RCS levels were close to the limit value of 0.100 mg/m3 adopted by the European Union and subsequently received in Italy.
It is absolutely necessary to remark that such limit of 0.100 mg/m3 could be inadequate to protect workers against silicosis or carcinogenic effects of RCS and it could introduce the possible perception of a false safety condition as well. In 2002, NIOSH noted that workers exposed at levels of silica equal to 0.050 mg/m3 for their working lifetimes (40-45 years) still have a significant risk of developing chronic radiographic silicosis (at least 1 per 100) (‘t Mannetje et al. Citation2002). More recently, in the process of updating the PEL for RCS, OSHA conducted a risk assessment for workers exposed at its older limit of 0.100 mg/m3. The Agency concluded that “employees exposed to respirable crystalline silica value of 0.100 mg/m3 are at significant risk of developing silicosis and other non-malignant respiratory disease, lung cancer, kidney effects, and immune system effects” (OSHA Occupational Safety and Health Administration, Department of Labor Citation2016). ACGIH, in its documentation, reports that a TLV-TWA® of 0.025 mg/m3 will protect against the development of silicosis and also against the development of lung cancer (ACGIH Citation2010).
The highest levels of exposure to respirable dust and RCS were found for subjects involved in the manual finishing, probably in relation to close proximity of workers to the source of pollution, represented by the portable equipment tools used. Furthermore, among the manual finishing operations, those performed without the use of water to reduce the dust dispersion were more critical.
RCS levels significantly lower were found during the mechanical processing, including cutting and grinding performed by stationary equipment, characterized by a greater distance between the operator and the source of pollution and the use of water. Indeed, in all studied facilities, this processing were carried out with water spraying equipment to cool the equipment and reduce the dustiness and the worker activity often consisted of setting the operation by control panels placed at a distance of at least a meter from the source of exposure. A comparison between the mechanical processing, all performed with water suppression and wet manual finishing showed no differences in airborne respirable dust neither in RCS exposure levels (data not shown). Instead the comparison, between manual finishing tasks (wet and dry), showed a statistical significant difference between the two different tasks although only for the respirable dust, probably because of the small size of sample.
These data confirm the role of the use of water (wet processing) in the reduction of exposure (Phillips et al. Citation2013; Pérez-Alonso et al. Citation2014; NEPSI - European Network for Silica Citation2016) but it requires a careful assessment of the risk of electrocution due to the use of electrically powered tools, and the risk of thermal discomfort due to operating conditions in a humid environment (Cooper et al. Citation2015). Additionally, the use of water alone may not be sufficient to reduce the exposure levels under a “safe” exposure level (Qi and Echt Citation2016).
Another fundamental aspect that affects exposure was represented by the role of local exhaust systems. In facilities A and C, all manual finishing operations were performed inside booths equipped with a wall extraction system while in facilities B and D, the manual finishing operations were carried out on benches aspirated along the perimeter. All suction systems allowed the operators to move along the sides of the work surfaces and be able to use portable tools without particular obstacles. As for their effectiveness in the reduction of exposure levels, both systems had advantages and disadvantages.
Extraction wall booths created a horizontal flow of air from the inlet section to the extraction wall and the finishing station was located within this horizontal flow. The worker faced the extraction wall so that clean air was pulled in from behind. This system quite easily prevented the dust escaping from the booth, thus avoiding contamination of the working environment outside the booth itself but, considering the dimensions of the booths and the distances of the finishing operations from the extraction walls, capture speeds were relatively low and not always sufficient to limit the levels of exposure (data not shown).
In addition, workers occasionally interpose themselves between the work surface and the extraction wall with a resulting pull of the plume of dust directly toward their breathing zone instead of pushing it away.
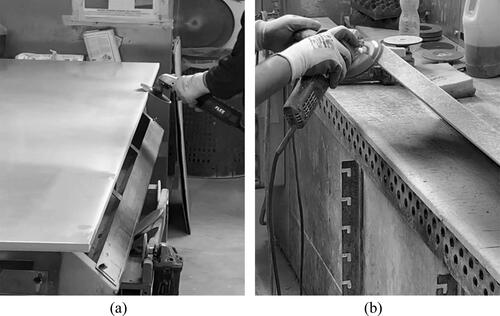
On the other hand, the aspirated benches achieved high capture speeds near the finishing operations performed although the effectiveness of dust capture was constrained by the correct positioning of the edges of the countertops’ surfaces with respect to the suction slots and by the correct use of the grinding wheel with projection of dust toward the slot itself. The aspirated benches used in the facilities B and D () seemed to have different effectiveness of dust capture, indeed respirable dust and RCS levels measured in the facility B were significantly lower (p = 0.0317 and p = 0.0159, respectively) than those found in facility D (data not shown). However, the use of aspirated benches could be limited by the size of slabs, in fact they did not allow the processing of large slabs (about 3 m long), such as those used for example in facility C.
Figure 2. Aspirated benches in facility B (panel a) and facility D (panel b).
An additional control measure that has been found effective at lowering indoor dust exposure, is housekeeping (Plog and Quinlan Citation2012). This consists of keeping the workstations and workplace clean and free of dust that can become resuspended. Indeed, the sedimentation of aerosols on floors and equipment, also generated by wet processing, can cause secondary exposure of workers: deposited dust, once dried, can be dispersed again in the air via foot traffic, movement of materials and air currents (Carrieri et al. Citation2020). The subjects with higher dust and RCS exposure levels worked in areas where, during the monitoring, a layer of dust deposited on the floor was noted. This underlines the importance of frequent cleaning procedures with vacuum systems or by the use of a floor drainage system before the wet dust dries. A clean workplace avoids also the exposure of workers performing other tasks in areas close where silica dust generating operations occur.
The use of respirators for personal protective equipment should be considered as a last resource to be used in conjunction with engineering controls and housekeeping, especially when dry processing operations are performed. This is because the performance of tight-fitting respirators depends on achieving a good contact between the wearer’s skin and the face seal of the face-piece in order to protect the workers. Fit testing should be performed to ensure that workers are adequately protected and the respirators are effective.
Personal protective equipment (PPE) was provided to all workers although most of them did not wear the respirator masks correctly (worn under the nose or not worn during all the duration of the operation). Moreover, fit testing was not performed in any of the studied facilities.
The incorrect use of PPE underlines the importance of providing training courses for the workers which should also include information on awareness about the risk of silica exposure.
Conclusions
The processing of artificial stones, and in particular quartz-resin conglomerates, has continued to generate serious concerns for the health of workers in the past twenty years due to the onset of severe silicosis associated with particularly short latency periods (Hoy et al. Citation2018). Our study revealed how an unacceptable risk condition for some of the monitored activities was still present despite preventive measures in place. Exposure levels were related to the different operating methods and the different effectiveness of the dust extraction systems. In general, the risk was higher for the workers involved in manual, dry or wet, finishing tasks in comparison to mechanical operations. A combination of engineering controls, such as tools equipped with water feeds and well-designed local exhaust ventilation, correct work practices, worker training, and the use of appropriate PPE, need to be emphasized to protect workers from overexposure to silica. Monitoring surveys need to be periodically carried out in order to verify the effectiveness of these measures. Finally, a revision of the current limit value adopted in Italy should be considered.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
Additional information
Funding
References
- ACGIH American Conference of Governmental Industrial Hygienists. 2010. Silica Crystalline – α-Quartz and Cristobalite. Cincinnati (OH): ACGIH TLV and BEI Documentation.
- Bartoli D, Banchi B, Di Benedetto F, Farina GA, Iaia TE, Poli C, Romanelli M, Scancarello G, Tarchi M. 2012. Silicosis in employees in the processing of kitchen, bar and shop countertops made from quartz resin composite. Provisional results of the environmental and health survey conducted within the territory of USL 11 of Empoli in Tuscany among employees in the processing of quartz resin composite materials and review of the literature. Ital J Occup Environ Hyg. 3(3):138–143.
- Carrieri M, Guzzardo C, Farcas D, Cena LG. 2020. Characterization of silica exposure during manufacturing of artificial stone countertops. IJERPH. 17(12):4489–4415. doi:https://doi.org/10.3390/ijerph17124489
- Cooper JH, Johnson DL, Phillips ML. 2015. Respirable silica dust suppression during artificial stone countertop cutting. Ann Occup Hyg. 59(1):122–126. doi:https://doi.org/10.1093/annhyg/meu083
- Directive (EU) 2017/2398 of the European Parliament and of the Council. 2017. Directive (EU) 2017/2398 of the European Parliament and of the Council of 12 December 2017 amending Directive 2004/37/EC on the protection of workers from the risks related to exposure to carcinogens or mutagens at work (Text with EEA relevance). OJ L 345, 27. 12:87–95.
- Friedman GK, Harrison R, Bojes H, Worthington K, Filios M. 2015. Notes from the field: silicosis in a countertop fabricator-Texas, 2014. MMWR Morb Mortal Wkly Rep. 64(5):129–130.
- García Vadillo C, Gómez JS, Morillo JR. 2011. Silicosis en trabajadores de conglomerados de cuarzo [Silicosis in quartz conglomerate workers]. Arch Bronconeumol. 47(1):53–54. doi:https://doi.org/10.1016/j.arbres.2010.09.005
- Guarnieri G, Salasnich M, Lucernoni P, Sbaraglia M, Putzu MG, Zuliani P, Rossi F, Vio S, Bianchi L, Martinelli A, et al. 2020. Silicosis in finishing workers in quartz conglomerates processing. Med Lav. 111(2):99–106. doi:https://doi.org/10.23749/mdl.v111i2.9115
- Hering KG, Jacobsen M, Bosch-Galetke E, Elliehausen HJ, Hieckel HG, Hofmann-Preiss K, Jacques W, Jeremie U, Kotschy-Lang N, Kraus T, et al. 2003 . Further development of the International Pneumoconiosis Classification-from ILO 1980 to ILO 2000 and to ILO 2000/German Federal Republic version. Pneumologie. 57(10):576–584. doi:https://doi.org/10.1055/s-2003-43020
- Hoy RF, Baird T, Hammerschlag G, Hart D, Johnson AR, King P, Putt M, Yates DH. 2018. Artificial stone-associated silicosis: a rapidly emerging occupational lung disease. Occup Environ Med. 75(1):3–5. doi:https://doi.org/10.1136/oemed-2017-104428
- ISO 16258-1. 2015. Workplace air — analysis of respirable crystalline silica by X-ray diffraction —part 1: direct-on-filter method.
- Kramer MR, Blanc PD, Fireman E, Amital A, Guber A, Rhahman NA, Shitrit D. 2012 . Artificial stone silicosis [corrected]: disease resurgence among artificial stone workers. Chest. 142(2):419–424. doi:https://doi.org/10.1378/chest.11-1321
- Martínez C, Prieto A, García L, Quero A, González S, Casan P. 2010. Silicosis: a disease with an active present. Arch Bronconeumol. 46(2):97–100. doi:https://doi.org/10.1016/j.arbres.2009.07.008
- NEPSI - European Network for Silica. 2016. Good practice guide – workers’ health protection through the good handling and use of crystalline silica and products containing it. [accessed 2021 May 4]. https://guide.nepsi.eu/wp-content/uploads/2020/12/NEPSI-Good-Practice-Guide.pdf.
- Ophir N, Shai AB, Alkalay Y, Israeli S, Korenstein R, Kramer MR, Fireman E. 2016. Artificial stone dust-induced functional and inflammatory abnormalities in exposed workers monitored quantitatively by biometrics. ERJ Open Res. 2(1):00086-2015. doi:https://doi.org/10.1183/23120541.00086-2015
- OSHA Occupational Safety and Health Administration, Department of Labor. 2016. Occupational Exposure to Respirable Crystalline Silica; Final Rule; Fed. Regist.; vol. 81, No. 58; Friday, March 25, 2016 Document ID OSHA 2010–0034–2177. [accessed 2021 May 19]. https://www.govinfo.gov/content/pkg/FR-2016-03-25/pdf/2016-04800.pdf.
- OSHA Occupational Safety and Health Administration, NIOSH National Institute for Occupational Safety and Health. 2015. Hazard alert: worker exposure to silica during countertop manufacturing, finishing, and installation. Washington (DC): US Department of Labor, Occupational Safety and Health Administration; US Department of Health and Human Services, CDC, National Institute for Occupational Safety and Health. [accessed 2021 May 4]. https://www.osha.gov/Publications/OSHA3768.pdf.
- OSHA Occupational Safety and Health Administration. 2016. OSHA Standard Number 1910.1053 - Respirable crystalline silica in general industry and maritime. [accessed 2021 May 4]. https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1053 and https://www.osha.gov/Publications/OSHA3911.pdf.
- Paolucci V, Romeo R, Sisinni AG, Bartoli D, Mazze MA, Sartorelli P. 2015. Silicosis in workers exposed to artificial quartz conglomerates: does it differ from chronic simple silicosis? Arch Bronconeumol. 51(12):e57–e60. doi:https://doi.org/10.1016/j.arbr.2015.06.003
- Pérez-Alonso A, Córdoba-Doña JA, Millares-Lorenzo JL, Figueroa-Murillo E, García-Vadillo C, Romero-Morillos J. 2014. Outbreak of silicosis in Spanish quartz conglomerate workers. Int J Occup Environ Health. 20(1):26–32. doi:https://doi.org/10.1179/2049396713Y.0000000049
- Phillips ML, Johnson DL, Johnson AC. 2013. Determinants of respirable silica exposure in stone countertop fabrication: a preliminary study. J Occup Environ Hyg. 10(7):368–373. doi:https://doi.org/10.1080/15459624.2013.789706
- Plog BA, Quinlan PJ. 2012. Fundamentals of industrial hygiene. Itasca (IL): National Safety Council.
- Qi C, Echt A. 2016. In-depth survey report: engineering control of silica dust from stone countertop fabrication and installation. Cincinnati (OH): Department Of Health And Human Services, Centers For Disease Control and Prevention. National Institute for Occupational Safety and Health. EPHB Report: 375–311.
- Ronsmans S, Decoster L, Keirsbilck S, Verbeken EK, Nemery B. 2019. Artificial stone-associated silicosis in Belgium. Occup Environ Med. 76(2):133–134. doi:https://doi.org/10.1136/oemed-2018-105436
- Rose C, Heinzerling A, Patel K, Sack C, Wolff J, Zell-Baran L, Weissman D, Hall E, Sooriash R, McCarthy RB, et al. 2019 . Severe silicosis in engineered stone fabrication workers - California, Colorado, Texas, and Washington, 2017-2019. MMWR Morb Mortal Wkly Rep. 68(38):813–818. doi:https://doi.org/10.15585/mmwr.mm6838a1
- Rosengarten D, Fox BD, Fireman E, Blanc PD, Rusanov V, Fruchter O, Raviv Y, Shtraichman O, Saute M, Kramer MR. 2017 . Survival following lung transplantation for artificial stone silicosis relative to idiopathic pulmonary fibrosis. Am J Ind Med. 60(3):248–254. doi:https://doi.org/10.1002/ajim.22687
- Mannetje A ‘t, Steenland K, Attfield M, Boffetta P, Checkoway H, DeKlerk N, Koskela RS. 2002. Exposure-response analysis and risk assessment for silica and silicosis mortality in a pooled analysis of six cohorts. Occup Environ Med. 59(11):723–728. doi:https://doi.org/10.1136/oem.59.11.723
- Wu N, Xue C, Yu S, Ye Q. 2020. Artificial stone-associated silicosis in China: a prospective comparison with natural stone-associated silicosis. Respirology. 25(5):518–524. doi:https://doi.org/10.1111/resp.13744