
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Background
Despite the robust evidence demonstrating positive effects from creatine supplementation (primarily when associated with resistance training) on measures of body composition, there is a lack of a comprehensive evaluation regarding the influence of creatine protocol parameters (including dose and form) on body mass and estimates of fat-free and fat mass.
Methods
Randomized controlled trials (RCTs) evaluating the effect of creatine supplementation on body composition were included. Electronic databases, including PubMed, Web of Science, and Scopus were searched up to July 2023. Heterogeneity tests were performed. Random effect models were assessed based on the heterogeneity tests, and pooled data were examined to determine the weighted mean difference (WMD) with a 95% confidence interval (CI).
Results
From 4831 initial records, a total of 143 studies met the inclusion criteria. Creatine supplementation increased body mass (WMD: 0.86 kg; 95% CI: 0.76 to 0.96, I2 = 0%) and fat-free mass (WMD: 0.82 kg; 95% CI: 0.57 to 1.06, I2 = 0%) while reducing body fat percentage (WMD: −0.28 %; 95% CI: −0.47 to −0.09; I2 = 0%). Studies that incorporated a maintenance dose of creatine or performed resistance training in conjunction with supplementation had greater effects on body composition.
Conclusion
Creatine supplementation has a small effect on body mass and estimates of fat-free mass and body fat percentage. These findings were more robust when combined with resistance training.
1. Introduction
Creatine, a non-protein organic amino acid [Citation1], is synthesized from arginine, glycine, and methionine [Citation2]. Within a cell, ~ 66% of creatine is stored as phosphocreatine (PCr) with the remainder stored as free creatine [Citation2]. Creatine is degraded non-enzymatically into creatinine at a rate of 1–2% per day, which needs to be replaced via endogenous production and/or through exogenous sources (i.e. red meat, seafood, creatine supplementation). The combination of endogenous production (primarily in the liver and kidneys) and habitual dietary sources of creatine causes ~ 80% intramuscular creatine saturation levels [Citation3]. The addition of creatine supplementation further augments these levels by ~ 20% [Citation4]. Mechanistically, elevated stores of PCr will enhance the capacity to rapidly re-synthesize adenosine triphosphate (ATP). Furthermore, creatine is pleiotropic and can alter calcium, glycogen, protein kinetics, insulin-like growth factor-1, myogenic regulatory factors, satellite cells, inflammation, and oxidative stress [Citation5].
The most common creatine supplementation protocols use either absolute or relative dosing strategies. From an absolute perspective, one strategy is to ingest 20 g/day for 5–7 (referred to as the creatine loading phase) followed by 2–5 g/day thereafter (creatine maintenance phase) [Citation6]. This strategy is well established to increase intramuscular creatine stores and/or exercise performance [Citation6,Citation7]. Alternatively, 3 g/day (without the creatine loading phase) can be adopted and will saturate intramuscular creatine stores in ~28 days [Citation8]. Relative dosing strategies (0.03 to 0.14 g/kg/day) may account for individual differences in body mass [Citation3] and have been shown to be effective over time [Citation9,Citation10].
To date, only a single systematic review involving older adults has been performed that examined the influence of different creatine dosing strategies and resistance training on measures of fat-free mass [Citation11]. Results showed no significant differences between low (≤5 g/day) vs. high (>5 g/day) doses of creatine, with and without a creatine loading phase, on gains in estimates of fat-free mass. Fat mass was not assessed in this review. The effects of different creatine dosing strategies on measures of body composition in younger adults remains to be elucidated. Beyond dosing strategies, creatine supplementation appears to be more efficacious when combined with resistance training compared to creatine supplementation alone [Citation12]. However, it is worth noting that other types of physical activity, such as high-intensity interval training (i.e. repeated sprints) may also benefit from creatine supplementation [Citation13]. For example, Nemezio et al. found greater gains in fat-free mass following 5 days of creatine supplementation (20 g/day) in 19 male amateur cyclists [Citation14].
Another gap in the literature involves the efficacy of different forms of creatine. Creatine monohydrate is the most studied and predominant form of creatine often included in dietary supplements [Citation6,Citation15–17]. Based on empirical research, creatine monohydrate undergoes little degradation during the digestive processes and is nearly completely absorbed by muscle tissue, with an approximate retention rate of 99% after oral consumption [Citation18]. However, manufacturers of dietary supplements have introduced alternate forms of purported creatine. The physical and chemical properties of these variants are theorized (not proven) to provide greater bioavailability and efficacy compared to creatine monohydrate [Citation16]. Nevertheless, the available evidence is insufficient to establish the superiority or safety of these various alternate forms of creatine, whether used alone or in combination with other nutrients, compared to creatine monohydrate. The impact of different forms of creatine supplementation on body composition remains to be systematically evaluated.
Therefore, the purpose of this systematic review is to provide a comprehensive evaluation of creatine supplementation on body composition including an analysis of potential modifiers, such as dosing protocols, alternative forms of creatine, and mode of exercise. Further, this systematic review evaluated several components of body composition including body mass, body mass index, and estimates of fat mass, body fat percentage, and fat-free mass. There is animal research showing that creatine supplementation plays an important role in fat bioenergetics and influences whole-body energy expenditure [Citation19–21] which may influence body fat percentage over time. To date, two meta-analyses have been performed showing that the combination of creatine supplementation and resistance training results in very small reductions in body fat percentage compared to resistance training alone [Citation21,Citation22]. Lastly, there is evidence that sex [Citation12] and age [Citation23] differences may exist regarding muscle changes over time, however, the effects on other indices of body composition are unknown. Collectively, this study aimed to systematically review randomized controlled trials (RCTs) evaluating the effects of creatine supplementation on body composition and to determine if the dosing protocol, exercise type, or alternative forms of creatine, as well as sex and age, influence the results.
2. Materials and methods
2.1. Search strategy and study selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) were selected among the various methods for reporting systematic reviews and meta-analyses, to perform this study [Citation24]. This study has been registered in PROSPERO (CRD42023416349). Up to July 2023, an exhaustive search was conducted in PubMed, Scopus, and ISI Web of Science, as well as other online databases, to identify relevant articles, with no date or language limitation. The following search items in titles and abstracts were used; ((Creatine[Title/Abstract]) AND (“Body Weight”[Title/Abstract] OR “Body Mass Index”[Title/Abstract] OR “Weight Loss”[Title/Abstract] OR Obesity[Title/Abstract] OR “Waist Circumference”[Title/Abstract] OR “Quetelet Index”[Title/Abstract] OR BMI[Title/Abstract] OR “Weight Reduction”[Title/Abstract] OR “Abdominal Obesity”[Title/Abstract] OR “Central Obesity”[Title/Abstract] OR “Visceral Obesity”[Title/Abstract] OR obese[Title/Abstract] OR overweight[Title/Abstract] OR “fat mass”[Title/Abstract] OR “Body Fat”[Title/Abstract])) AND (Intervention[Title/Abstract] OR “Intervention Study”[Title/Abstract] OR “Intervention Studies”[Title/Abstract] OR “controlled trial”[Title/Abstract] OR randomized[Title/Abstract] OR random[Title/Abstract] OR randomly[Title/Abstract] OR placebo[Title/Abstract] OR “clinical trial”[Title/Abstract] OR Trial[Title/Abstract] OR “randomized controlled trial”[Title/Abstract] OR “randomized clinical trial”[Title/Abstract] OR RCT[Title/Abstract] OR blinded[Title/Abstract] OR “double blind”[Title/Abstract] OR “double blinded”[Title/Abstract] OR trial[Title/Abstract] OR trials[Title/Abstract] OR “Pragmatic Clinical Trial”[Title/Abstract] OR “Cross-Over Studies”[Title/Abstract] OR “Cross-Over”[Title/Abstract] OR “Cross-Over Study”[Title/Abstract] OR parallel[Title/Abstract] OR “parallel study”[Title/Abstract] OR “parallel trial”[Title/Abstract] OR OR[Title/Abstract]).
2.2. Eligibility criteria
All studies that met the following criteria were included: 1) RCTs evaluating the effects of creatine supplementation on body composition as an outcome (body mass, body mass index, fat mass, body fat percentage, and fat-free mass) with a control group, 2) studies conducted on adults (≥18 years), 3) that received creatine supplementation as an intervention, 4) studies with at least 4 days of the intervention period, 5) parallel or crossover designs, 6) studies with outcome reporting at the beginning and the end of the intervention.
2.3. Exclusion criteria
All studies that followed these features were excluded after the full-text assessment: 1) ecological, review, animal, and observational studies, 2) studies executed on individuals younger than 18 years of age, and 3) studies without randomization or placebo or control groups.
2.4. Data extraction
The records were screened primarily for eligibility based on the title and abstract. Next, the full text of the studies was assessed for the possibility of being included in this meta-analysis. Ultimately, the following data were extracted: the name of the first author, the year of publication, the location of the study, the study design, the sample size in each group, the characteristics of the subjects such as mean age, sex, and body mass index, the doses of creatine administered for the intervention, the duration of the interventions, the mean changes and standard deviation (SD) of the markers during the study for both the intervention and control groups. When a study provided multiple data at different time points, only the most recent was considered. It is important to acknowledge that in the current study, any references to fat mass and fat-free mass are to their estimation values.
2.5. Quality assessment
The quality of the articles that were qualified was assessed by two separate researchers applying the Cochran scoring method [Citation25]. The risk of bias was evaluated based on seven criteria, which are as follows: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Accordingly, terms such as “Low,” “High,” or “Unclear” were used to estimate each field. Moreover, any dissemblance was elucidated by the corresponding authors.
2.6. Data synthesis and statistical analysis
To identify the overall effect sizes, weighted mean differences (WMD) and the SD of measures were extracted from both intervention and control groups applying the random-effects model following the protocol of DerSimonian And Laird [Citation26]. Moreover, without mean changes reporting, it was calculated by using this formula: mean change = final values − baseline values, and SD changes were calculated by the following formula [Citation24]:
Also, standard errors (SEs), 95% confidence intervals (CIs), and interquartile ranges (IQRs) were converted respectively to SDs using the Hozo et al. protocol [Citation27]. The random-effects model that accounted for between-study variations was applied to detect the overall effect size. Additionally, the Between-studies heterogeneity was checked by Cochran’s Q test and measured by using the I-squared statistic (I2) [Citation28]. I2 >40% or p-values <0.05 were considered significant between-studies heterogeneity. Furthermore, to check potential sources of heterogeneity [Citation29], subgroup analyses were conducted following the preplanned criteria, including study duration (≤30 days vs. >30 days), baselines of body composition indices (body mass index: 18.5–24.9 kg/m2 vs. 25.0–29.9 kg/m2), supplementation protocols (≤5 g/day vs/> 5 g/day, with and without loading and with and without maintenance doses), training status (active vs. trained vs. non-active), exercise (aerobic vs. resistance vs. combined vs. no exercise), age (≤40 vs. >40 years of age), sex (males vs. females), and creatine type (creatine monohydrate vs. alternative forms of creatine). Moreover, a sensitivity analysis was executed to determine the impact of each specific study on the overall estimation [Citation30]. The possibility of publication bias was checked using Egger’s regression test and the visually inspected funnel plot examination [Citation31]. Meta-regression analysis using the random-effects model was undertaken to investigate the potential association between changes in dose and duration with body composition variables. Statistical analysis was carried out applying STATA, version 11.2 (Stata Corp, College Station, TX). The p-values <0.05 were considered statistically significant in all analyses.
3. Results
3.1. Study selection
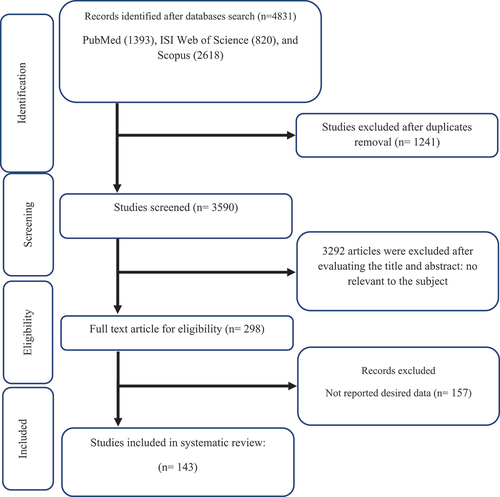
As mentioned in , at first, an exhaustive systematic search was conducted in online datasets and resulted in finding 4831 studies. Then, 1241 studies were identified as duplicates, and 3292 unrelated studies were removed after a comprehensive assessment of the titles and abstracts. Moreover, 157 studies without desired data reporting were excluded following the full-text evaluation of the studies. Finally, according to the inclusion criteria, 143 studies were identified.
Figure 1. Flow chart of study selection for inclusion trials in the systematic review.
3.2. Study characteristic
Ultimately, 143 qualified articles with 172 study arms were included, with 3655 participants (2069 in the intervention group and 1922 in the control group). All included studies had the publication date of between 1993 and 2023. The duration of the intervention in all included trials was from four days [Citation32] to 365 [Citation33] days. The sample size of all studies in this meta-analysis varied from 6 [Citation34] to 109 [Citation33] participants. Moreover, the design of 124 studies was parallel RCT [Citation9,Citation32,Citation33,Citation35–156], and the design of 19 was crossover [Citation34,Citation81,Citation157–173]. The qualified studies were mainly conducted in the USA [Citation9,Citation32,Citation38,Citation39,Citation42,Citation43,Citation45–47,Citation51–53,Citation55–57,Citation60–63,Citation66–69,Citation74,Citation77,Citation78,Citation81,Citation84,Citation86,Citation87,Citation89,Citation91,Citation93,Citation95,Citation97,Citation101,Citation103,Citation105,Citation107–109,Citation111,Citation113,Citation114,Citation116–118,Citation120,Citation124,Citation126,Citation137,Citation138,Citation147,Citation148,Citation152,Citation153,Citation157,Citation160,Citation166,Citation167,Citation169,Citation170,Citation173], the UK [Citation71,Citation85,Citation102,Citation133,Citation142,Citation158,Citation165], Sweden [Citation35], Iran [Citation112,Citation121,Citation143], Australia [Citation41,Citation44,Citation70,Citation76,Citation98,Citation99], France [Citation36,Citation40], Belgium [Citation37,Citation48,Citation65,Citation159,Citation162], Estonia [Citation34,Citation128], Japan [Citation49,Citation82], Netherland [Citation50,Citation139,Citation156], Canada [Citation54,Citation59,Citation64,Citation72,Citation80,Citation90,Citation96,Citation106,Citation130–132,Citation134,Citation145,Citation149,Citation163], Norway [Citation58], Germany [Citation88,Citation92,Citation104,Citation161,Citation168], Poland [Citation75,Citation119], Denmark [Citation73], Thailand [Citation79], Spain [Citation83], Switzerland [Citation164], Portugal [Citation94], Brazil [Citation33,Citation100,Citation115,Citation123,Citation125,Citation127,Citation129,Citation141,Citation144,Citation146,Citation150,Citation155,Citation172], Scotland [Citation174], Italy [Citation110], Mexico [Citation171], Finland [Citation122,Citation136], New Zealand [Citation135], and Turkey [Citation140]. Twenty-one studies were performed on females [Citation33,Citation37,Citation51,Citation52,Citation55,Citation70,Citation77,Citation81,Citation90,Citation94,Citation95,Citation103,Citation115,Citation122,Citation124,Citation125,Citation130,Citation132,Citation138,Citation140,Citation173], 81 studies on males [Citation9,Citation32,Citation34,Citation35,Citation38,Citation39,Citation42,Citation45–50,Citation56–58,Citation60–64,Citation66–69,Citation71,Citation73,Citation75,Citation76,Citation78,Citation79,Citation82–84,Citation88,Citation89,Citation93,Citation96,Citation98–101,Citation104–112,Citation114,Citation118–120,Citation123,Citation126–129,Citation136,Citation137,Citation139,Citation143–145,Citation147,Citation148,Citation150,Citation151,Citation156–158,Citation160,Citation165–167,Citation169,Citation171], and the others were conducted on both [Citation36,Citation40,Citation44,Citation53,Citation54,Citation59,Citation65,Citation72,Citation74,Citation80,Citation85–87,Citation91,Citation92,Citation97,Citation102,Citation116,Citation117,Citation121,Citation131,Citation133–135,Citation141,Citation142,Citation146,Citation149,Citation153–155,Citation161–164,Citation168,Citation170,Citation172]. The characteristics of the included studies are indicated in .
Table 1. Characteristic of included studies in meta-analysis.
3.3. Quality assessment
Evaluating the general risk of bias mentioned 111 studies with a low risk of bias [Citation32,Citation33,Citation36,Citation38–40,Citation42–46,Citation48,Citation49,Citation51–57,Citation60–62,Citation64–66,Citation68,Citation69,Citation72–74,Citation76,Citation77,Citation79–81,Citation84–86,Citation90–94,Citation96–109,Citation111–120,Citation122–129,Citation131,Citation132,Citation134–140,Citation142–145,Citation147–150,Citation152–155,Citation158–163,Citation165–168,Citation170–173], 17 studies with a high risk of bias [Citation34,Citation37,Citation41,Citation47,Citation58,Citation70,Citation71,Citation78,Citation82,Citation87,Citation88,Citation121,Citation141,Citation151,Citation156,Citation157,Citation169], and the others indicated an unclear risk of bias [Citation9,Citation35,Citation50,Citation59,Citation63,Citation67,Citation75,Citation83,Citation89,Citation95,Citation110,Citation130,Citation133,Citation146,Citation164] ().
Table 2. Risk of bias assessment.
4. Meta-analysis
4.1. Effect of creatine supplementation on body composition in adults
4.1.1. Effect of creatine supplementation on body mass and body mass index
Analyzing 154 overall effect sizes demonstrated a significant increase in body mass following creatine supplementation (WMD: 0.86 kg; 95% CI: 0.76 to 0.96; p < 0.001) (). However, no degree of heterogeneity was found (I2 = 0.0%). Evaluating the results of subgroup analysis showed that the effect of creatine supplementation on body mass was independent of age, sex, activity status of participants, trial duration, intervention dose, loading protocol, type of creatine, and type of training program during the intervention (). Overall, results from the random effects model indicated that creatine supplementation failed to change body mass index (WMD: 0.20 kg/m2; 95% CI: −0.17 to 0.58; p = 0.299) (). Moreover, no degree of between-studies heterogeneity was observed (I2 = 0.0%) ().
Figure 2. Forest plot detailing weighted mean difference and 95% confidence intervals (CIs) for the effect of creatine supplementation on A) body weight (kg); B) BMI (kg/m2); C) FM (kg); D) BFP (%); E) and FFM (kg).
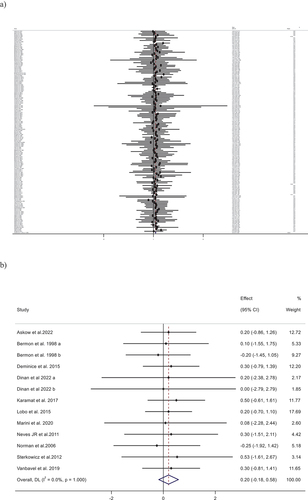
Figure 2. Continued
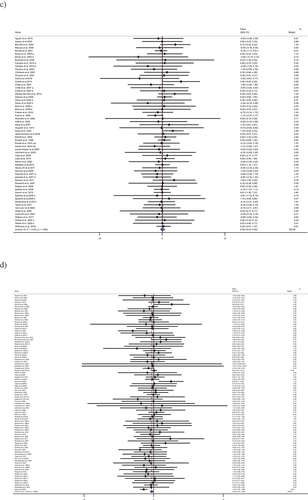
Table 3. Subgroup analyses of creatine supplementation on body composition in adults.
4.1.2. Effect of creatine supplementation on fat-free mass
Combined results from 95 effect sizes indicated a small, yet significant increase in fat-free mass following creatine supplementation (WMD: 0.82 kg; 95% CI: 0.57 to 1.06; p < 0.001) (). Additionally, we observed no degree of between-studies heterogeneity (I2 = 0.0%). Subgroup analysis revealed that creatine supplementation increased fat-free mass in studies that used combined or resistance training interventions or creatine monohydrate as a supplement. Moreover, using a maintenance dose, or creatine loading with a long maintenance dose had significant effects on fat-free mass. Descriptively, the results appeared to be greater among males ().
Figure 2. Continued
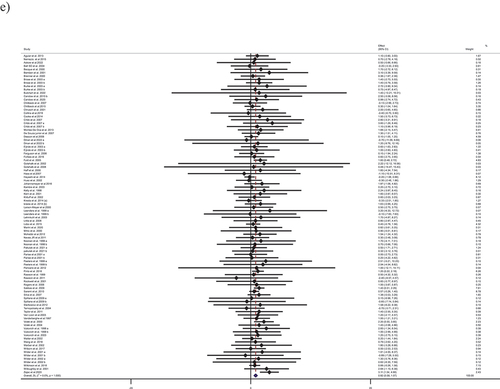
4.1.3. Effect of creatine supplementation on fat mass and body fat percentage
Pooled data from 62 effect sizes demonstrated no significant effect of creatine supplementation on fat mass (WMD: 0.05 kg; 95% CI: −0.24 to 0.35; p = 0.703) (), with no observed heterogeneity among the studies (I2 = 0.0%) (). Subgroup analysis failed to show any significant change in the results. According to the results from 89 effect sizes, creatine supplementation resulted in a very small reduction in body fat percentage (WMD: −0.28 %; 95% CI: −0.47 to − 0.09; p = 0.004) (). There was no heterogeneity among studies (I2 = 0.0%). Subgroup analysis revealed a significant reduction in body fat percentage in studies with supplementation dosages of more than 5 g/day, trained participants, and studies that used a combination of creatine supplementation with combined training. Also, studies that used creatine supplementation protocol with a maintenance dose or creatine monohydrate showed a significant reduction in body fat percentage ().
4.2. Sensitivity analysis
To ascertain the impact of each study on the overall effect size, each trial was excluded from the analysis step by step. Assessing the results of the sensitivity analysis indicated no significant alteration in the total effect of creatine supplementation on body mass, body mass index, fat-free mass, fat mass, and body fat percentage ().
Table 4. Publication bias and sensitivity analysis.
4.3. Publication bias
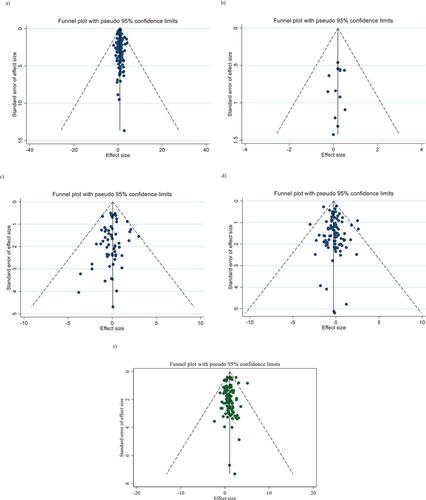
The overall results of Egger’s regression test and inspecting the funnel plots provided no evidence of publication bias () ().
Figure 3. Funnel plots for the effect of creatine supplementation on A) body weight (kg); B) BMI (kg/m2); C) FM (kg); D) BFP (%); and E) FFM (kg).
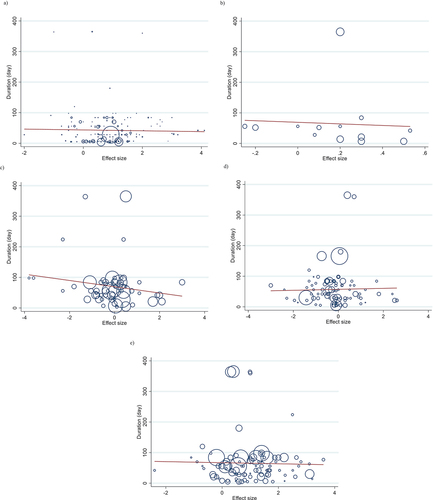
4.4. Non-linear dose-response analysis
The results of the dose-response analysis indicated a significant association between creatine doses with changes in fat mass (p = 0.039; and ) and fat-free mass (p = 0.008; and ). Also, a significant association between the duration of creatine supplementation and changes in body mass (p = 0.030; and ) was observed.
Figure 4. Non-linear dose-response relations between creatine supplementation and absolute mean differences. Dose-response relations between dose (g/day) and absolute mean differences in on A) body weight (kg); B) BMI (kg/m2); C) FM (kg); D) BFP (%); and E) FFM (kg).
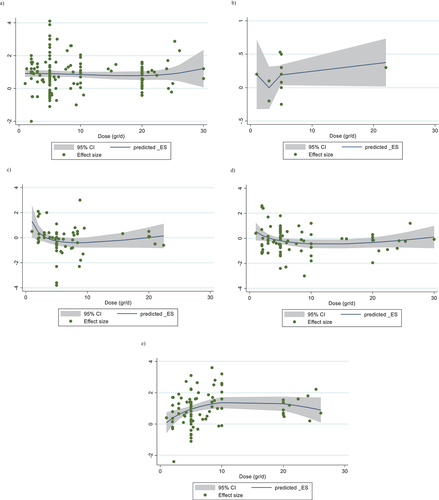
Figure 5. Non-linear dose-response relations between creatine supplementation and absolute mean differences. Dose-response relations between duration of intervention (week) and absolute mean differences in A) body weight (kg); B) BMI (kg/m2); C) FM (kg); D) BFP (%); and E) FFM (kg).
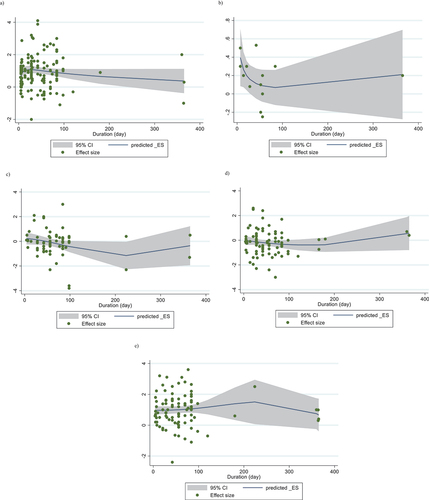
Table 5. Meta-regression and dose-response.
4.5. Meta-regression analysis
The results of the meta-regression test showed that there was no significant association between the dosage and duration of creatine supplementation and alterations in body composition variables (, ).
Figure 6. linear dose-response relations between creatine supplementation and absolute mean differences. Dose-response relations between dose (g/day) and absolute mean differences in A) body weight (kg); B) BMI (kg/m2); C) FM (kg); D) BFP (%); and E) FFM (kg).
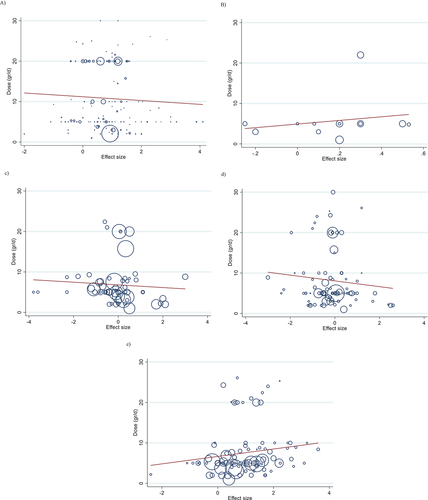
Figure 7. linear dose-response relations between creatine supplementation and absolute mean differences. Dose-response relations between duration of intervention (week) and absolute mean differences in A) body weight (kg); B) BMI (kg/m2); C) FM (kg); D) BFP (%); and E) FFM (kg).
4.6. GRADE analysis
The quality of evidence was assessed using the GRADE protocol in this meta-analysis. The quality of evidence in studies evaluating the creatine supplementation impact on body mass index and fat mass is regarded as moderate. Moreover, the evidence quality in studies aimed to estimate the influence of creatine supplementation on body mass, fat-free mass, and body fat percentage was upgraded to high ().
Table 6. GRADE profile of creatine supplementation on body composition in adults.
4.7. Discussion
Overall, the most important outcomes from this comprehensive systematic review and meta-analysis were that creatine supplementation results in a small favorable effect on measures of fat-free mass and body fat percentage over time. Sub-analyses revealed that fat-free mass was significantly increased when (1) creatine was ingested in conjunction with either combined concurrent (aerobic + resistance training) training or resistance training alone, (2) creatine monohydrate was used, and (3) a maintenance dose (with or without a loading phase) was implemented. Moreover, it was shown that research including a daily creatine intake of more than 5 g or studies combining aerobic and resistance training in their experimental design exhibited a significant reduction in body fat percentage. No significant differences were found in any of the variables when subgrouping was done based on sex. However, it was observed that men exhibited a 1.20 kg increase in fat-free mass, while females had a smaller rise of 0.54 kg. Age, training status, and study duration did not appear to influence any of the outcome variables.
5. Loading protocol of creatine supplementation and training intervention
5.1. Creatine and fat-free Mass
In support of several previous systematic reviews and meta-analyses [Citation5,Citation11,Citation12,Citation175–177], creatine supplementation significantly increased estimates of fat-free mass (overall) by 0.82 kg (95% CI: 0.57, 1.06). This was only evident when creatine monohydrate was combined with resistance training or combination of resistance and aerobic training. Alternative forms of creatine (creatine malate, creatine ethyl ester and creatine phosphate) did appear to have a similar mean change in fat-free mass (Monohydrate: 0.82 kg [95% CI: 0.57, 1.06]; Alternative forms: 0.91 kg [−3.06, 4.88]). Few studies have examined the ergogenic effects of creatine-based compounds such as creatine malate, creatine ethyl ester and creatine phosphate, which limits the ability to draw strong conclusions. Sterkowicz et al. conducted a trial to determine the effects of 6-weeks of training with creatine malate supplementation on anaerobic capacity and aerobic power and in judo specific fitness performance. Results showed no effects of supplementation with creatine malate on body composition indices and physical performance compared to control [Citation119]. In this study creatine malate was chosen due to its efficacy during absorption and digestion in the gastrointestinal tract. Another study examined the combined effects of creatine in the form of creatine ethyl ester and resistance training on body composition and muscle strength and power, when compared to creatine monohydrate, creatine ethyl ester failed to show significant improvements in body composition, muscle mass, and strength and power [Citation111]. However, due to the limited number of studies, lack of statistical power, and large variability the alternative forms of creatine did not statistically increase fat-free mass compared to the placebo. Therefore, based on the current meta-analysis, creatine monohydrate is well-studied (n = 89 RCTs), effective (p < 0.001), has a well-developed safety profile [Citation6], and is economical [Citation15]. Additionally, confirmed by a previous review [Citation178], creatine monohydrate is the only source of creatine that has substantial evidence to support bioavailability, efficacy, and safety recommended by professional societies and organizations. Future research may be warranted to explore alternative forms of creatine, however, presently it is clear that other forms of creatine are not superior to creatine monohydrate [Citation15].
A prior meta-analysis included 22 RCTs with 721 older adults (age: 57–70 years of age, both males and females) who demonstrated an increase in fat-free mass (~1.37 kg, 95% CI: 0.97–1.76 kg) when creatine was ingested during a resistance training program (training 2–3 times/week for 7 to 52 weeks) compared to resistance training and placebo [Citation5]. More recently, Delpino et al. (2022) included 35 studies with 1192 participants that revealed that creatine (with and without exercise) increased fat-free mass by 0.68 kg (95% CI: 0.26–1.11), however, sub-analyses demonstrated that gains in fat-free mass only occurred when creatine was ingested with resistance training (1.10 kg, 95% CI: 0.56–1.65) [Citation12]. In contrast to the present investigation, the findings of Delpino et al. (2022) did not provide a statistically significant disparity in fat-free mass when creatine supplementation was administered in conjunction with a mixed regimen of aerobic and resistance training. In support of our findings, there was no significant effect on fat-free mass when creatine was ingested alone (without exercise). However, it is important to note that some of the observed increases in fat-free mass may be due to increases in body water retention (both extra- and intracellular). It is worth mentioning that several tools were used to measure body composition, such as bioelectric impedance analysis (BIA), BOD POD, hydrostatic weighting, hydro densitometry, skinfold equations, and dual-energy X-Ray absorptiometry. Among them, BIA is an electrical method which has the potential of quantifying total body water, extracellular water, intracellular water in addition to FM, FFM. However, due to the limited number of included studies that used BIA as body composition measurement tools (8 of 143 studies) or provided body water data, more studies are needed to confirm body water retention changes following creatine supplementation. A recent systematic review and meta-analysis involving 10 studies showed that the combination of creatine supplementation and resistance training increased regional measures of muscle accretion (0.10 to 0.16 cm; as measured using ultrasound and peripheral quantitative computed tomography) compared to placebo [Citation23]. Mechanistically, greater fat-free mass from creatine is likely related to its ability to increase high-energy phosphate, glycogen, calcium, and protein kinetics, stimulation of satellite cells and growth factors, or by decreasing inflammation and oxidative stress over time [Citation2,Citation179]. In theory, creatine will allow you to train at a higher training volume, which may enhance training adaptations over time (for a comprehensive review on mechanisms of creatine to enhance muscle see [Citation5]).
5.2. Creatine and Body Fat
The overall pooled analysis in the current review revealed a very small, yet statistically significant decrease in body fat percentage following creatine supplementation (−0.28% [−0.47, −0.09]) compared to placebo. However, there were no significant changes in fat mass or body mass index. In theory, an increase in fat-free mass may increase energy expenditure and influence energy balance resulting in fat loss over time. In addition, in animal models there is evidence that a reduction in the availability of creatine in adipose tissue slows whole-body energy expenditure and increases fat accumulation [Citation19,Citation20]. Despite these potential mechanisms, based on the current review they do not appear to be sufficient to alter absolute fat mass in humans over time and support the notion that the change in body fat percentage is likely due to an increase in fat-free mass. Bonilla et al. provided 7.6 g/day of creatine for 56 days in young resistance-trained males. They found that creatine combined with resistance training increased fat-free mass and decreased body fat percentage over time [Citation148]. Sub-analyses revealed that high-dose creatine (>5 g/day), training status (i.e. being trained), exercise intervention, and the incorporation of a creatine maintenance dose following a creatine loading phase may influenced body fat percentage. In support of our findings, Forbes et al. (2019) observed a statistically significant decrease in body fat percentage when creatine was combined with resistance training [Citation21] without a significant change in absolute fat mass. Nevertheless, there is ongoing debate over the potential efficacy of creatine supplementation in relation to decreasing body fat. Several research investigations have shown that there is no statistically significant difference in FM, BFP, or BMI after the administration of creatine supplements, regardless of whether exercise training is included or not [Citation104,Citation106,Citation180–182]. The period of creatine supplementation in these studies was shorter than 30 days, which may be considered inadequate for achieving changes in body composition. Additionally, workout program was not created with the intention of establishing a well-rounded routine to effectively observe the intended effects on FM.
5.3. Creatine and body Mass
The observed rise in body mass following creatine supplements may be associated with intramuscular fluid retention that occurs due to the osmotic characteristics of creatine [Citation183]. Further, creatine supplementation combined with carbohydrates increases muscle glycogen storage, thereby further increasing water retention [Citation184]. These small alterations in water-induced cell swelling increase myogenic regulatory factors and activate satellite cells involved in muscle hypertrophy [Citation185]. Over time, the increase in body mass is likely due to a combination of water retention and an increase in lean tissue mass. In resistance-trained males (n = 27) receiving either creatine or placebo over 8 weeks had no changes in the ratio of skeletal muscle mass to intracellular water and only the creatine group had a decrease in the skeletal muscle mass to extracellular water ratio [Citation186]. In females, there may be variations in water retention based on the phase of the menstrual cycle [Citation173]. Thirty moderately active females were randomized to either creatine (20 g/day for 5 days) or placebo, with a menstrual phase crossover design. There were significant increases in total body water, extracellular fluid, and intracellular fluid in the creatine condition only during the luteal phase, while no condition differences were noted in the follicular phase. Despite these alterations in fluid retention, body mass was not different between conditions or across the menstrual cycle [Citation173]. These findings appear to support our current meta-analysis which found no sex-related differences. Collectively, creatine supplementation appears to increase body mass compared to placebo by ~0.86 kg.
In relation to the concept of loading protocol, it is worth noting that out of the total 154 research examined, a significant proportion of 48 studies did not include a maintenance phase subsequent to the loading phase. Interestingly, when comparing the collective impact of these studies that only focused on loading, it was shown that the effect on body mass was comparatively lower (0.54 kg) than the studies that used maintenance doses of creatine as part of their supplementation protocol. In accordance with the findings of Rogers et al. a research study used a creatine supplementation regimen of 3 g/d in conjunction with a strength training program spanning a duration of 12 weeks. The findings indicated a significant increase of 2 kg in body mass, which exhibited a notably greater magnitude in comparison to the control group receiving the placebo [Citation187]. Similarly, Herda et al. conducted a study in which they administered a maintenance dosage of creatine supplementation (5 g/d) without implementing any exercise program. The findings of this study demonstrated a notable augmentation in body mass after a 30-day period of creatine supplementation among the participants in the creatine group [Citation188].
A further study conducted by Delextrat et al. yielded findings indicating that a 28-day period of creatine supplementation, without the first loading phase, among athletes involved in rocket sports resulted in a significant rise in body mass within the creatine group. Conversely, no such gain was seen within the placebo or beta-alanine groups [Citation189]. Nevertheless, findings from a prior scoping study revealed that irrespective of varying doses of methods and exercises, favorable outcomes of creatine supplementation on muscular strength, muscle mass, and athletic performance were seen among young, healthy individuals [Citation190]. In terms of training modality, 40 studies included a mix of AT and RT in their training regimen. Additionally, 17 studies exclusively utilized AT, while 57 research employed RT as their primary training protocol. The subgroup analysis revealed that there was a positive effect on body mass across all subgroups when considering different types of exercise, means that despite of exercise types or even no exercise, creatine can increase body mass.
5.4. Dosage of creatine supplementation
Our results shows that studies using doses up to 5 grams of creatine daily (38 studies), demonstrated a statistically significant decrease in BFP. In this regard, after subgrouping based on dosage, the between subgroups heterogeneity was significant (p = 0.005) demonstrating dosage of creatine supplementation is the source of heterogeneity among included studies. however, different dosages did not change the effectiveness of creatine supplementation on FFM and body mass. Future studies should focus on finding the optimum dosage of creatine for attenuating body fat percentages.
5.5. Characteristics of participants that affect body composition indices due to creatine supplementation
Fat-Free Mass
The positive impacts of creatine on FFM were statistically significant irrespective of the age, sex, or whether the individuals were trained or untrained. In addition, participants with a normal body mass index (BMI:18.5 to 24.9) also showed a significant increase in FFM. Also, greater gains in FFM were shown in men. Accordingly, Delpino et al., 2022 did not find any influence from the dosage or type of creatine used or duration of supplementation on fat-free mass. However, they did report greater gains in fat-free mass in males compared to females (males: 1.46 kg [95% CI: 0.47, 2.46], females: 0.29 kg [95% CI: −0.43, 1.01]) [Citation12]. We also found much larger increases in fat-free mass in males (1.20 kg) compared to females (0.54 kg). While no sex mechanisms were determined across these reviews, differing results may be associated with differences in pre-supplementation intramuscular creatine levels [Citation191]. There is some evidence that females may have higher intramuscular creatine stores which may blunt their responsiveness to creatine supplementation [Citation192]. Coincidentally, the findings from the subgroup analysis in this research demonstrated a significant augmentation in the impact of creatine supplementation on FFM in studies with a baseline BMI within the normal range. Given that the BMI data was only available for a limited number of individuals in 16 out of the 95 studies that examined the impact of creatine supplementation on FFM, it is important to use care when interpreting this finding.
5.6. Body fat percentage
Our results showed a significant reduction in BFP in trained individuals, while other characteristics of participants did not affect BFP due to Creatine Supplementation. 37 out of 89 studies conducted on trained individuals indicating training background may be a potential factor affecting BFP after creatine supplementation. Although it is not clear to us why trained individuals may benefit more from creatine supplementation, but more FFM gains (1.31 kg) in these subjects following creatine supplementation may partially explain the reduction of fat percentage.
5.7. Body Mass
Our analysis examined creatine on body mass and included 154 effect sizes. Overall, participants gained 0.86 kg (95% CI: 0.76, 0.96) following creatine supplementation compared to placebo. Trial duration, creatine dose, sex, age, loading protocol, exercise type, type of creatine, and training status did not alter these findings, nor was there any observed heterogeneity between studies. Our findings are partially supported by other systematic reviews and meta-analyses [Citation21,Citation176,Citation193]. For example, Devries and Phillips (2014) conducted a systematic review and meta-analysis in older adults (N = 357, across 12 studies) ingesting creatine supplementation combined with resistance training and noted a significant increase in body mass compared to placebo (1.00 kg: 95% CI: 0.32–1.67 kg; p = 0.004) [Citation194]. In contrast, Forbes et al.. (2019) conducted a systematic review and meta-analysis in older adults (N = 609, across 19 studies) and found a non-significant increase in body mass (0.86 kg: 95% CI, −0.32–2.05 kg; p = 0.15) [Citation21].
5.8. Strengths and limitations
To our knowledge, this is the first meta-analysis that has evaluated the influence of various supplementation protocols, exercise types, training status, supplementation duration and dose, creatine type, sex, and age on body composition (body mass, fat-free mass, fat mass, body fat percentage and body mass index). Our systematic review included a comprehensive analysis of over 160 effect sizes, which increases the statistical power and certainty of our findings. Nevertheless, it is important to acknowledge limitations. Specifically, we found that a significant number of the RCTs included did not examine baseline intramuscular creatine concentrations or changes in creatine levels throughout the duration of the study, nor did they determine the dietary intake of creatine or total protein. One notable constraint of this meta-analysis was that the majority of studies used body composition measures as a secondary outcome. A further limitation is the absence of adequately structured RCTs that have assessed water retention, hence impeding our ability to elucidate the specific processes behind the increase in body mass and lean mass following to creatine supplementation. In future RCTs, it is warranted to assess both intra and extra-cellular hydration, as well as quantifying the intake of creatine from dietary sources. Additionally, it is crucial to use suitable dosages, exercise modalities, and loading protocols in the design of this research.
6. Conclusion
In summary, creatine supplementation has a very small effect on body mass, fat-free mass, and body fat percentage over time. These changes were apparent when creatine was combined with resistance training. Creatine appears to increase fat-free mass more in males compared to females. Collectively, variations in dosing protocols, training status, and age do not appear to influence the effectiveness of creatine supplementation. Based on previous research findings, which did not report any adverse effects related to the use of creatine supplements on the overall well-being of participants, it seems that people who are apparently healthy may experience benefits from the performance-enhancing properties of creatine supplementation.
Author contributions
MG, DAL, FD, and RB conceptualized and designed the study, interpreted the data, and prepared the manuscript. OA and MG analyzed the data and drafted the initial manuscript. FP, ZH and KG extracted data and drafted the initial manuscript. SF, FD, RB, and DC supervised the project and edited the initial manuscript. All authors contributed to the article and approved the submitted version.
Availability of supporting data
Data sharing is applicable.
Ethical approval and consent to participate
This is a review study, and there was no consent to participate.
Disclosure statement
D.G.C. has conducted industry-sponsored research involving creatine supplementation and received creatine donations for scientific studies and travel support for presentations involving creatine supplementation at scientific conferences. In addition, D.G.C. serves on the Scientific Advisory Board for Alzchem (a company that manufactures creatine) and as an expert witness/consultant in legal cases involving creatine supplementation.
Additional information
Funding
References
- Bonilla DA, Kreider RB, Stout JR, et al. Metabolic basis of creatine in health and disease: a bioinformatics-assisted review. Nutrients. 2021;13(4):1238. doi: 10.3390/nu13041238
- Wyss M, Kaddurah-Daouk R. Creatine and creatinine metabolism. Physiol Rev. 2000;80(3):1107–61. doi: 10.1152/physrev.2000.80.3.1107
- Buford TW, Kreider RB, Stout JR, et al. International society of sports nutrition position stand: creatine supplementation and exercise. J Int Soc Sports Nutr. 2007;4(1):1–8. doi: 10.1186/1550-2783-4-6
- Antonio J, Candow DG, Forbes SC, et al. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? J Int Soc Sports Nutr. 2021;18(1):13. doi: 10.1186/s12970-021-00412-w
- Chilibeck PD, Kaviani M, Candow DG, et al. Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: a meta-analysis. Open Access J Sports Med. 2017;8:213–226. doi: 10.2147/OAJSM.S123529
- Kreider RB, Kalman DS, Antonio J, et al. International society of sports nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2017;14(1):18. doi: 10.1186/s12970-017-0173-z
- Harris RC, Söderlund K, Hultman E. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci. 1992;83(3):367–374. doi: 10.1042/cs0830367
- Hultman E, Soderlund K, Timmons J, et al. Muscle creatine loading in men. J Appl Physiol. 1996;81(1):232–237. doi: 10.1152/jappl.1996.81.1.232
- Hickner RC, Dyck DJ, Sklar J, et al. Effect of 28 days of creatine ingestion on muscle metabolism and performance of a simulated cycling road race. J Int Soc Sports Nutr. 2010;7(1):26. doi: 10.1186/1550-2783-7-26
- Willoughby DS, Rosene JJM, Si S, et al. Effects of oral creatine and resistance training on myosin heavy chain expression. Med & Sci In Sports & Exercise. 2001;33(10):1674–1681. doi: 10.1097/00005768-200110000-00010
- Forbes SC, Candow DG, Ostojic SM, et al. Meta-analysis examining the importance of creatine ingestion strategies on lean tissue mass and strength in older adults. Nutrients. 2021;13(6):1912. doi: 10.3390/nu13061912
- Delpino FM, Figueiredo LM, Forbes SC, et al. The influence of age, sex, and type of exercise on the efficacy of creatine supplementation on Lean Body Mass: a systematic review and Meta-analysis of randomized clinical trials. Nutrition. 2022;103-104:111791. doi: 10.1016/j.nut.2022.111791
- Cooper R, Naclerio F, Allgrove J, et al. Creatine supplementation with specific view to exercise/sports performance: an update. J Int Soc Sports Nutr. 2012;9(1):33. doi: 10.1186/1550-2783-9-33
- KmdA N, Bertuzzi R, Correia-Oliveira CR, et al. Effect of creatine loading on oxygen uptake during a 1-km cycling time trial. Med & Sci In Sports & Exercise. 2015;47(12):2660–2668. doi: 10.1249/MSS.0000000000000718
- Fazio C, Elder CL, Harris MM. Efficacy of alternative forms of creatine supplementation on improving performance and body composition in healthy subjects: a systematic review. The J Strength & Cond Res. 2022;36(9):2663–2670. doi: 10.1519/JSC.0000000000003873
- Kreider RB, Jäger R, Purpura M. Bioavailability, efficacy, safety, and regulatory status of creatine and related compounds: a critical review. Nutrients. 2022;14(5):1035. doi: 10.3390/nu14051035
- Escalante G, Gonzalez AM, St Mart D, et al. Analysis of the efficacy, safety, and cost of alternative forms of creatine available for purchase on amazon. com: are label claims supported by science? Heliyon. 2022;8(12):e12113. doi: 10.1016/j.heliyon.2022.e12113
- Jäger R, Purpura M, Shao A, et al. Analysis of the efficacy, safety, and regulatory status of novel forms of creatine. Amino Acids. 2011;40(5):1369–1383. doi: 10.1007/s00726-011-0874-6
- Kazak L, Rahbani JF, Samborska B, et al. Ablation of adipocyte creatine transport impairs thermogenesis and causes diet-induced obesity. Nat Metab. 2019;1(3):360–370. doi: 10.1038/s42255-019-0035-x
- Kazak L, Chouchani ET, Jedrychowski MP, et al. A creatine-driven substrate cycle enhances energy expenditure and thermogenesis in beige fat. Cell. 2015;163(3):643–655. doi: 10.1016/j.cell.2015.09.035
- Forbes SC, Candow DG, Krentz JR, et al. Changes in fat mass following creatine supplementation and resistance training in adults≥ 50 years of age: a meta-analysis. J Funct Morphology And Kines. 2019;4(3):62. doi: 10.3390/jfmk4030062
- Candow DG, Prokopidis K, Forbes SC, et al. Resistance exercise and creatine supplementation on fat Mass in Adults< 50 years of age: a systematic review and meta-analysis. Nutrients. 2023;15(20):4343. doi: 10.3390/nu15204343
- Burke R, Piñero A, Coleman M, et al. The effects of creatine supplementation combined with resistance training on regional measures of muscle hypertrophy: a systematic review with meta-analysis. Nutrients. 2023;15(9):2116. doi: 10.3390/nu15092116
- Borenstein M, Hedges LV, Higgins JPT, et al. Introduction to meta-analysis. John Wiley & Sons; 2021. https://scholar.google.com/scholar_lookup?title=Introduction+to+meta-analysis&author=Borenstein+M&author=Hedges+LV&author=Higgins+JPT&author=Rothstein+HR.&publication+year=2011
- Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane; 2023. www.training.cochrane.org/handbook
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188. doi: 10.1016/0197-2456(86)90046-2
- Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. [2005 Apr 20];5(1):13. doi: 10.1186/1471-2288-5-13
- Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. [2003 Sep 6];327(7414):557–560. doi: 10.1136/bmj.327.7414.557
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. [2002 Jun 15];21(11):1539–1558. doi: 10.1002/sim.1186
- Tobias A. Assessing the influence of a single study in the meta-analysis estimate. Stata Tech Bull. 1999;47:15–17.
- Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi: 10.1136/bmj.315.7109.629
- Rockwell JA, Rankin JW, Toderico B. Creatine supplementation affects muscle creatine during energy restriction. Med Sci Sports Exerc. 2001 Jan;33(1):61–68. doi: 10.1097/00005768-200101000-00011
- Lobo DM, Tritto AC, da Silva LR, et al. Effects of long-term low-dose dietary creatine supplementation in older women. Exp Gerontol. 2015 Oct;70:97–104. doi: 10.1016/j.exger.2015.07.012
- Ööpik V, Pääsuke M, Saima T, et al. Effect of creatine supplementation during rapid body mass reduction on metabolism and isokinetic muscle performance capacity. Eur J Appl Physiol And Occup Physiol. 1998 04 22;78(1):83–92. doi: 10.1007/s004210050391
- Balsom P, Harridge S, Söderlund K, et al. Creatine supplementation per se does not enhance endurance exercise performance. Acta Physiologica Scandinavica. 1993;149(4):521–523. doi: 10.1111/j.1748-1716.1993.tb09649.x
- Mujika I, Chatard J-C, Lacoste L, et al. Creatine supplementation does not improve sprint performance in competitive swimmers. Med Sci Sports Exerc. 1996;28(11):1435–1441. doi: 10.1097/00005768-199611000-00014
- Vandenberghe K, Goris M, Hecke PV, et al. Long-term creatine intake is beneficial to muscle performance during resistance training. J Appl Physiol. 1997;83(6):2055–2063. doi: 10.1152/jappl.1997.83.6.2055
- Noonan D, Berg K, Latin RW, et al. Effects of varying dosages of oral creatine relative to fat free body mass on strength and body composition. The J Strength & Cond Res. 1998;12(2):104–108. doi: 10.1519/00124278-199805000-00009
- Kreider RB, Ferreira M, Wilson M, et al. Effects of creatine supplementation on body composition, strength, and sprint performance. Med Sci Sports Exerc. 1998 Jan;30(1):73–82. doi: 10.1097/00005768-199801000-00011
- Bermon S, Venembre P, Sachet C, et al. Effects of creatine monohydrate ingestion in sedentary and weight-trained older adults. Acta Physiologica Scandinavica. 1998 01 10;164(2):147–155. doi: 10.1046/j.1365-201X.1998.00427.x
- Kelly VG, Jenkins DG. Effect of oral creatine supplementation on near-maximal strength and repeated sets of high-intensity bench press exercise. The J Strength & Cond Res. 1998;12(2):109–115. doi: 10.1519/00124278-199805000-00010
- Vukovich MD, Michaelis J. Effect of two different creatine supplementation products on muscular strength and power. Res In Sports Med: An Int J. 1998;8(4):369–383. doi: 10.1080/15438629909512539
- Leenders N, Sherman WM, Lamb DR, et al. Creatine supplementation and swimming performance. Int J Sport Nutr Exerc Metab. 1999;9(3):251–262. doi: 10.1123/ijsn.9.3.251
- McKenna MJ, Morton J, Selig SE, et al. Creatine supplementation increases muscle total creatine but not maximal intermittent exercise performance. J Appl Physiol. 1999;87(6):2244–2252. doi: 10.1152/jappl.1999.87.6.2244
- Rawson ES, Wehnert ML, Clarkson PM. Effects of 30 days of creatine ingestion in older men. Eur J Appl Physiol Occup Physiol. 1999 Jul;80(2):139–144. doi: 10.1007/s004210050570
- Pearson DR, Russel DGHW, Harris T. Long-term effects of creatine monohydrate on strength and power. The J Strength & Cond Res. 1999;13(3):187–192. doi: 10.1519/00124278-199908000-00001
- Peeters BM, Lantz CD, Mayhew JL. Effect of oral creatine monohydrate and creatine phosphate supplementation on maximal strength indices, body composition, and blood pressure. The J Strength & Cond Res. 1999;13(1):3–9. doi: 10.1519/00124278-199902000-00001
- Francaux M, Poortmans JR. Effects of training and creatine supplement on muscle strength and body mass. Eur J Appl Physiol Occup Physiol. 1999 Jul;80(2):165–168. doi: 10.1007/s004210050575
- Schedel J, Tanaka M, Tanaka H, et al. Consequences of one-week creatine supplementation on creatine and creatinine levels in athletes’ serum and urine. Schweiz Z Fur Sportmed Und Sporttraumatologie. 2000 Dec 08;48:111–116.
- Deutekom M, Beltman JG, de Ruiter CJ, et al. No acute effects of short-term creatine supplementation on muscle properties and sprint performance. Eur J Appl Physiol. 2000 Jun;82(3):223–229. doi: 10.1007/s004210050675
- Larson-Meyer D, Hunter G, Trowbridge C, et al. The effect of creatine supplementation on muscle strength and body composition during off-season training in female soccer players. J Strength Cond Res. 2000 Jan 11;14(4):434. doi: 10.1519/1533-4287(2000)014<0434:TEOCSO>2.0.CO;2
- Brenner M, Rankin J, Sebolt DON. The effect of creatine supplementation during resistance training in women. J Strength Cond Res. 2000 Jan 05;14(2):207. doi: 10.1519/1533-4287(2000)014<0207:TEOCSD>2.0.CO;2
- Haff G, Kirksey K, Stone M, et al. The effect of 6 weeks of creatine monohydrate supplementation on dynamic rate of force development. J Strength Cond Res. 2000 Jan 11;14(4):426. doi: 10.1519/1533-4287(2000)014<0426:TEOWOC>2.0.CO;2
- Mihic S, MacDonald JR, McKenzie S, et al. Acute creatine loading increases fat-free mass, but does not affect blood pressure, plasma creatinine, or CK activity in men and women. Med Sci Sports Exerc. 2000 Feb;32(2):291–296. doi: 10.1097/00005768-200002000-00007
- Hamilton KL, Meyers MC, Skelly WA, et al. Oral creatine supplementation and upper extremity anaerobic response in females. Int J Sport Nutr Exerc Metab. 2000 Sep;10(3):277–289. doi: 10.1123/ijsnem.10.3.277
- Becque MD, Lochmann JD, Melrose DR. Effects of oral creatine supplementation on muscular strength and body composition. Med Sci Sports Exerc. 2000 Mar;32(3):654–658. doi: 10.1097/00005768-200003000-00016
- Volek JS, Duncan ND, Mazzetti SA, et al. No effect of heavy resistance training and creatine supplementation on blood lipids. Int J Sport Nutr Exerc Metab. 2000 Jun;10(2):144–156. doi: 10.1123/ijsnem.10.2.144
- Skare OC, Skadberg, Wisnes AR, et al. Creatine supplementation improves sprint performance in male sprinters. Scand J Med Sci Sports. 2001 Apr;11(2):96–102. doi: 10.1034/j.1600-0838.2001.011002096.x
- Parise G, Mihic S, MacLennan D, et al. Effects of acute creatine monohydrate supplementation on leucine kinetics and mixed-muscle protein synthesis. J Appl Physiol ( 1985). 2001 Sep;91(3):1041–1047. doi: 10.1152/jappl.2001.91.3.1041
- Kern M, Podewils L, Vukovich M, et al. Physiological response to exercise in the heat following creatine supplementation. JEPonline. 2001 Jan 04;4(2):18–27.
- Bemben MG, Bemben DA, Loftiss DD, et al. Creatine supplementation during resistance training in college football athletes. Med Sci Sports Exerc. 2001 Oct;33(10):1667–1673. doi: 10.1097/00005768-200110000-00009
- Green JM, McLester JR, Smith JE, et al. The effects of creatine supplementation on repeated upper- and lower-body wingate performance. J Strength Cond Res. 2001 Feb;15(1):36–41. doi: 10.1519/00124278-200102000-00007
- Wilder N, Deivert RG, Hagerman F, et al. The effects of low-dose creatine supplementation versus creatine loading in collegiate football players. J Athl Train. 2001 Jun;36(2):124–129.
- Chrusch MJ, Chilibeck PD, Chad KE, et al. Creatine supplementation combined with resistance training in older men. Med Sci Sports Exerc. 2001 Dec;33(12):2111–2117. doi: 10.1097/00005768-200112000-00021
- Hespel P, Op’t Eijnde B, Van Leemputte M, et al. Oral creatine supplementation facilitates the rehabilitation of disuse atrophy and alters the expression of muscle myogenic factors in humans. J Physiol. [2001 Oct 15];536(Pt 2):625–633. doi: 10.1111/j.1469-7793.2001.0625c.xd
- Willoughby DS, Rosene J. Effects of oral creatine and resistance training on myosin heavy chain expression. Med Sci Sports Exerc. 2001 Oct;33(10):1674–1681. doi: 10.1097/00005768-200110000-00010
- Wilder N, Gilders R, Hagerman F, et al. The effects of a 10-week, periodized, off-season resistance-training program and creatine supplementation among collegiate football players. J Strength Cond Res. 2002 Aug;16(3):343–352. doi: 10.1519/1533-4287(2002)016<0343:TEOAWP>2.0.CO;2
- Warber JP, Tharion WJ, Patton JF, et al. The effect of creatine monohydrate supplementation on obstacle course and multiple bench press performance. J Strength Cond Res. 2002 Nov;16(4):500–508. doi: 10.1519/00124278-200211000-00003
- Gotshalk LA, Volek JS, Staron RS, et al. Creatine supplementation improves muscular performance in older men. Med Sci Sports Exerc. 2002 Mar;34(3):537–543. doi: 10.1097/00005768-200203000-00023
- Cox G, Mujika I, Tumilty D, et al. Acute creatine supplementation and performance during a field test simulating match play in elite female soccer players. Int J Sport Nutr Exerc Metab. 2002 Mar;12(1):33–46. doi: 10.1123/ijsnem.12.1.33
- Kilduff LP, Vidakovic P, Cooney G, et al. Effects of creatine on isometric bench-press performance in resistance-trained humans. Med Sci Sports Exerc. 2002 Jul;34(7):1176–1183. doi: 10.1097/00005768-200207000-00019
- Burke DG, Chilibeck PD, Parise G, et al. Effect of creatine and weight training on muscle creatine and performance in vegetarians. Med Sci Sports Exerc. 2003 Nov;35(11):1946–1955. doi: 10.1249/01.MSS.0000093614.17517.79
- Eijnde BO, Van Leemputte M, Goris M, et al. Effects of creatine supplementation and exercise training on fitness in men 55-75 yr old. J Appl Physiol ( 1985). 2003 Aug;95(2):818–828. doi: 10.1152/japplphysiol.00891.2002
- Lehmkuhl M, Malone M, Justice B, et al. The effects of 8 weeks of creatine monohydrate and glutamine supplementation on body composition and performance measures. J Strength Cond Res. 2003 Aug;17(3):425–438. doi: 10.1519/00124278-200308000-00002
- Zajac A, Waśkiewicz Z, Poprzecki S, et al. Effects of creatine and hMß supplementation on anaerobic power and body composition in basketball players. J Hum Kinet. 2003;10:95–108.
- Watsford ML, Murphy A, Spinks WL, et al. Creatine supplementation and its effect on musculotendinous stiffness and performance. J Strength Cond Res. 2003 Feb;17(1):26–33. doi: 10.1519/00124278-200302000-00005
- Kambis KW, Pizzedaz SK. Short-term creatine supplementation improves maximum quadriceps contraction in women. Int J Sport Nutr Exerc Metab. 2003 Mar;13(1):87–96. doi: 10.1123/ijsnem.13.1.87
- Kutz MR, Gunter MJ. Creatine monohydrate supplementation on body weight and percent body fat. J Strength Cond Res. 2003 Nov;17(4):817–821. doi: 10.1519/00124278-200311000-00030
- Anomasiri W, Sanguanrungsirikul S, Saichandee P. Low dose creatine supplementation enhances sprint phase of 400 meters swimming performance. J Med Assoc Of Thail = Chotmaihet Thangphaet. 2004 Jan 10;87(Suppl 2):S228–32.
- Brose A, Parise G, Tarnopolsky MA. Creatine supplementation enhances isometric strength and body composition improvements following strength exercise training in older adults. J Gerontol A Biol Sci Med Sci. 2003 Jan;58(1):11–19. doi: 10.1093/gerona/58.1.B11
- Eckerson JM, Stout JR, Moore GA, et al. Effect of two and five days of creatine loading on anaerobic working capacity in women. J Strength Cond Res. 2004 Feb;18(1):168–173. doi: 10.1519/00124278-200402000-00025
- Kinugasa R, Akima H, Ota A, et al. Short-term creatine supplementation does not improve muscle activation or sprint performance in humans. Eur J Appl Physiol. 2004 Mar;91(2–3):230–237. doi: 10.1007/s00421-003-0970-8
- Javierre C, Barbany JR, Bonjorn VM, et al. Creatine supplementation and performance in 6 consecutive 60 meter sprints. J Physiol Biochem. 2004 Dec;60(4):265–271. doi: 10.1007/BF03167072
- Volek JS, Ratamess NA, Rubin MR, et al. The effects of creatine supplementation on muscular performance and body composition responses to short-term resistance training overreaching. Eur J Appl Physiol. 2004 May;91(5–6):628–637. doi: 10.1007/s00421-003-1031-z
- Fuld JP, Kilduff LP, Neder JA, et al. Creatine supplementation during pulmonary rehabilitation in chronic obstructive pulmonary disease. Thorax. 2005 Jul;60(7):531–537. doi: 10.1136/thx.2004.030452
- Eckerson JM, Stout JR, Moore GA, et al. Effect of creatine phosphate supplementation on anaerobic working capacity and body weight after two and six days of loading in men and women. J Strength Cond Res. 2005 Nov;19(4):756–763. doi: 10.1519/00124278-200511000-00006
- Mendel R, Blegen M, Cheatham C, et al. Effects of creatine on thermoregulatory responses while exercising in the heat. Calif) (Burbank, Los Angeles County. Nutrition. 2005 Jan 03;21(3):301–307. doi: 10.1016/j.nut.2004.06.024
- Pluim BM, Ferrauti A, Broekhof F, et al. The effects of creatine supplementation on selected factors of tennis specific training. Br J Sports Med. 2006 Jun;40(6):507–511; discussion 511-2. doi: 10.1136/bjsm.2005.022558
- Hoffman JR, Stout JR, Falvo MJ, et al. Effect of low-dose, short-duration creatine supplementation on anaerobic exercise performance. J Strength Cond Res. 2005 May;19(2):260–264. doi: 10.1519/00124278-200505000-00004
- Ferguson TB, Syrotuik DG. Effects of creatine monohydrate supplementation on body composition and strength indices in experienced resistance trained women. J Strength Cond Res. 2006 Nov;20(4):939–946. doi: 10.1519/00124278-200611000-00035
- Rogers ME, Bohlken RM, Beets MW, et al. Effects of creatine, ginseng, and astragalus supplementation on strength, body composition, mood, and blood lipids during strength-training in older adults. J Sports Sci Med. 2006;5(1):60–69.
- Norman K, Stübler D, Baier P, et al. Effects of creatine supplementation on nutritional status, muscle function and quality of life in patients with colorectal cancer–a double blind randomised controlled trial. Clin Nutr. 2006 Aug;25(4):596–605. doi: 10.1016/j.clnu.2006.01.014
- Hoffman J, Ratamess N, Kang J, et al. Effect of creatine and beta-alanine supplementation on performance and endocrine responses in strength/power athletes. Int J Sport Nutr Exerc Metab. 2006 Aug;16(4):430–446. doi: 10.1123/ijsnem.16.4.430
- Silva AJ, Machado Reis V, Guidetti L, et al. Effect of creatine on swimming velocity, body composition and hydrodynamic variables. J Sports Med Phys Fitness. 2007 Mar;47(1):58–64.
- Smith AE, Walter AA, Herda TJ, et al. Effects of creatine loading on electromyographic fatigue threshold during cycle ergometry in college-aged women. J Int Soc Sports Nutr. [2007 Nov 26];4(1):20. doi: 10.1186/1550-2783-4-20
- Chilibeck PD, Magnus C, Anderson M. Effect of in-season creatine supplementation on body composition and performance in rugby union football players. Appl Physiol Nutr Metab. 2007 Dec;32(6):1052–1057. doi: 10.1139/H07-072
- Hass CJ, Collins MA, Juncos JL. Resistance training with creatine monohydrate improves upper-body strength in patients with parkinson disease: a randomized trial. Neurorehabil Neural Repair. 2007 Mar-Apr;21(2):107–115. doi: 10.1177/1545968306293449
- Cribb PJ, Williams AD, Stathis CG, et al. Effects of whey isolate, creatine, and resistance training on muscle hypertrophy. Med Sci Sports Exerc. 2007 Feb;39(2):298–307. doi: 10.1249/01.mss.0000247002.32589.ef
- Cribb PJ, Williams AD, Hayes A. A creatine-protein-carbohydrate supplement enhances responses to resistance training. Med Sci Sports Exerc. 2007 Nov;39(11):1960–1968. doi: 10.1249/mss.0b013e31814fb52a
- Souza-Junior T, Dubas J, Pereira B, et al. Suplementação de creatina e treinamento de força: alterações na resultante de força máxima dinâmica e variáveis antropométricas em universitários submetidos a oito semanas de treinamento de força (hipertrofia). Revista Brasileira De Medicina Do Esporte - REV BRAS MED ESPORTE. 2007 Jan 10;13(5):303–309. doi: 10.1590/S1517-86922007000500005
- Eckerson JM, Bull AA, Moore GA. Effect of thirty days of creatine supplementation with phosphate salts on anaerobic working capacity and body weight in men. J Strength Cond Res. 2008 May;22(3):826–832. doi: 10.1519/JSC.0b013e31816a40ad
- Deacon SJ, Vincent EE, Greenhaff PL, et al. Randomized controlled trial of dietary creatine as an adjunct therapy to physical training in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. [2008 Aug 1];178(3):233–239. doi: 10.1164/rccm.200710-1508OC
- Gotshalk LA, Kraemer WJ, Mendonca MA, et al. Creatine supplementation improves muscular performance in older women. Eur J Appl Physiol. 2008 Jan;102(2):223–231. doi: 10.1007/s00421-007-0580-y
- Jäger R, Metzger J, Lautmann K, et al. The effects of creatine pyruvate and creatine citrate on performance during high intensity exercise. J Int Soc Sports Nutr. [2008 Feb 13];5(1):4. doi: 10.1186/1550-2783-5-4
- Walter AA, Smith AE, Herda TJ, et al. Effects of creatine loading on electromyographic fatigue threshold in cycle ergometry in college-age men. Int J Sport Nutr Exerc Metab. 2008 Apr;18(2):142–151. doi: 10.1123/ijsnem.18.2.142
- Little JP, Forbes SC, Candow DG, et al. Creatine, arginine alpha-ketoglutarate, amino acids, and medium-chain triglycerides and endurance and performance. Int J Sport Nutr Exerc Metab. 2008 Oct;18(5):493–508. doi: 10.1123/ijsnem.18.5.493
- Eliot KA, Knehans AW, Bemben DA, et al. The effects of creatine and whey protein supplementation on body composition in men aged 48 to 72 years during resistance training. J Nutr Health Aging. 2008 Mar;12(3):208–212. doi: 10.1007/BF02982622
- Herda TJ, Beck TW, Ryan ED, et al. Effects of creatine monohydrate and polyethylene glycosylated creatine supplementation on muscular strength, endurance, and power output. J Strength Cond Res. 2009 May;23(3):818–826. doi: 10.1519/JSC.0b013e3181a2ed11
- Sakkas GK, Mulligan K, Dasilva M, et al. Creatine fails to augment the benefits from resistance training in patients with HIV infection: a randomized, double-blind, placebo-controlled study. PLoS One. 2009;4(2):e4605. doi: 10.1371/journal.pone.0004605
- Bazzucchi I, Felici F, Sacchetti M. Effect of short-term creatine supplementation on neuromuscular function. Med Sci Sports Exerc. 2009 Oct;41(10):1934–1941. doi: 10.1249/MSS.0b013e3181a2c05c
- Spillane M, Schoch R, Cooke M, et al. The effects of creatine ethyl ester supplementation combined with heavy resistance training on body composition, muscle performance, and serum and muscle creatine levels. J Int Soc Sports Nutr. [2009 Feb 19];6(1):6. doi: 10.1186/1550-2783-6-6
- Saremi A, Gharakhanloo R, Sharghi S, et al. Effects of oral creatine and resistance training on serum myostatin and GASP-1. Mol Cell Endocrinol. [2010 Apr 12];317(1–2):25–30. doi: 10.1016/j.mce.2009.12.019
- Fukuda DH, Smith AE, Kendall KL, et al. The effects of creatine loading and gender on anaerobic running capacity. J Strength Cond Res. 2010 Jul;24(7):1826–1833. doi: 10.1519/JSC.0b013e3181e06d0e
- Camic CL, Hendrix CR, Housh TJ, et al. The effects of polyethylene glycosylated creatine supplementation on muscular strength and power. J Strength Cond Res. 2010 Dec;24(12):3343–3351. doi: 10.1519/JSC.0b013e3181fc5c5c
- Neves M Jr., Gualano B, Roschel H, et al. Beneficial effect of creatine supplementation in knee osteoarthritis. Med Sci Sports Exerc. 2011 Aug;43(8):1538–1543. doi: 10.1249/MSS.0b013e3182118592
- Rawson ES, Stec MJ, Frederickson SJ, et al. Low-dose creatine supplementation enhances fatigue resistance in the absence of weight gain. Nutrition. 2011 Apr;27(4):451–455. doi: 10.1016/j.nut.2010.04.001
- Smith AE, Fukuda DH, Ryan ED, et al. Ergolytic/ergogenic effects of creatine on aerobic power. Int J Sports Med. 2011 Dec;32(12):975–981. doi: 10.1055/s-0031-1283179
- Taylor L, Poole C, Pena E, et al. Effects of combined creatine plus fenugreek extract vs. Creatine plus carbohydrate supplementation on resistance training adaptations. J Sports Sciamp; Med. 2011 Jan 06;10:254–260.
- Sterkowicz S, Tyka A, Chwastowski M, et al. The effects of training and creatine malate supplementation during preparation period on physical capacity and special fitness in judo contestants. J Int Soc Sports Nutr. 2012 Mar 09;9(1):41. doi: 10.1186/1550-2783-9-41
- Zuniga JM, Housh TJ, Camic CL, et al. The effects of creatine monohydrate loading on anaerobic performance and one-repetition maximum strength. J Strength Cond Res. 2012 Jun;26(6):1651–1656. doi: 10.1519/JSC.0b013e318234eba1
- Hamid M, Rahnama N, Moghadasi M, et al. Effect of creatine supplementation on sprint and skill performance in young soccer players. Middle East J Sci Res. 2012 01 01;12:397–401.
- Aguiar AF, Januário RS, Junior RP, et al. Long-term creatine supplementation improves muscular performance during resistance training in older women. Eur J Appl Physiol. 2013 Apr;113(4):987–996. doi: 10.1007/s00421-012-2514-6
- Percário S, Domingues SPDT, Teixeira LFM, et al. Effects of creatine supplementation on oxidative stress profile of athletes. J Int Soc Sports Nutr. 2012 Dec 21;9(1):56. doi: 10.1186/1550-2783-9-56
- Kresta JY, Oliver JM, Jagim AR, et al. Effects of 28 days of beta-alanine and creatine supplementation on muscle carnosine, body composition and exercise performance in recreationally active females. J Int Soc Sports Nutr. 2014;11(1):55. doi: 10.1186/s12970-014-0055-6
- Gualano B, Macedo AR, Alves CR, et al. Creatine supplementation and resistance training in vulnerable older women: a randomized double-blind placebo-controlled clinical trial. Exp Gerontol. 2014 May;53:7–15. doi: 10.1016/j.exger.2014.02.003
- Cooke MB, Brabham B, Buford TW, et al. Creatine supplementation post-exercise does not enhance training-induced adaptations in middle to older aged males. Eur J Appl Physiol. 2014 Jun;114(6):1321–1332. doi: 10.1007/s00421-014-2866-1
- Deminice R, Rosa FT, Pfrimer K, et al. Creatine supplementation increases total body water in soccer players: a deuterium oxide dilution study. Int J Sports Med. 2016 Feb;37(2):149–153. doi: 10.1055/s-0035-1559690
- Aedma M, Timpmann S, Lätt E, et al. Short-term creatine supplementation has no impact on upper-body anaerobic power in trained wrestlers. J Int Soc Sports Nutr. 2015;12(1):45. doi: 10.1186/s12970-015-0107-6
- KmdA N, Oliveira CRC, AELd S. Suplementação de creatina e seus efeitos sobre o desempenho em exercícios contínuos e intermitentes de alta intensidade. R Educ Fís UEM. 2015;26(1):157–165. doi: 10.4025/reveducfis.v26i1.23888
- Chilibeck PD, Candow DG, Landeryou T, et al. Effects of creatine and resistance training on bone health in postmenopausal women. Med Sci Sports Exerc. 2015 Aug;47(8):1587–1595. doi: 10.1249/MSS.0000000000000571
- Candow DG, Vogt E, Johannsmeyer S, et al. Strategic creatine supplementation and resistance training in healthy older adults. Appl Physiol Nutr Metab. 2015 Jul;40(7):689–694. doi: 10.1139/apnm-2014-0498
- Forbes SC, Sletten N, Durrer C, et al. Creatine monohydrate supplementation does not augment fitness, performance, or Body composition adaptations in response to four weeks of high-intensity interval training in young females. Int J Sport Nutr Exerc Metab. 2017 Jun;27(3):285–292. doi: 10.1123/ijsnem.2016-0129
- Wilkinson TJ, Lemmey AB, Jones JG, et al. Can creatine supplementation improve body composition and objective physical function in rheumatoid arthritis patients? A randomized controlled trial. Arthritis Care Res (Hoboken). 2016 Jun;68(6):729–737. doi: 10.1002/acr.22747
- Johannsmeyer S, Candow DG, Brahms CM, et al. Effect of creatine supplementation and drop-set resistance training in untrained aging adults. Exp Gerontol. 2016 Oct;83:112–119. doi: 10.1016/j.exger.2016.08.005
- Collins J, Longhurst G, Roschel H, et al. Resistance training and Co-supplementation with creatine and protein in older subjects with frailty. J Frailty Aging. 2016;5(2):126–134. doi: 10.14283/jfa.2016.85
- Backx EMP, Hangelbroek R, Snijders T, et al. Creatine loading does not preserve muscle Mass or strength during leg immobilization in healthy, young males: a randomized controlled trial. Sports Med. 2017 Aug;47(8):1661–1671. doi: 10.1007/s40279-016-0670-2
- Wang CC, Fang CC, Lee YH, et al. Effects of 4-week creatine supplementation combined with complex training on muscle damage and sport performance. Nutrients. [2018 Nov 2];10(11):1640. doi: 10.3390/nu10111640
- Wilborn CD, Outlaw JJ, Mumford PW, et al. A Pilot study examining the effects of 8-week whey protein versus whey protein plus creatine supplementation on body composition and performance variables in resistance-trained women. Ann Nutr Metab. 2016;69(3–4):190–199. doi: 10.1159/000452845
- Karamat FA, Horjus DL, Haan YC, et al. The acute effect of beta-guanidinopropionic acid versus creatine or placebo in healthy men (ABC trial): study protocol for a randomized controlled trial. Trials. 2015 Feb 22;16(1):56. doi: 10.1186/s13063-015-0581-9
- Atakan MM, Karavelioğlu MB, Harmancı H, et al. Short term creatine loading without weight gain improves sprint, agility and leg strength performance in female futsal players. Sciamp; Sports. 2019 Jan 1;34(5):321–327. doi: 10.1016/j.scispo.2018.11.003
- Van Bavel D, de Moraes R, Tibirica E. Effects of dietary supplementation with creatine on homocysteinemia and systemic microvascular endothelial function in individuals adhering to vegan diets. Fundam Clin Pharmacol. 2019 Aug;33(4):428–440. doi: 10.1111/fcp.12442
- Delextrat A, Targen N, Impson-Davey G, et al. Effects of supplementation with creatine monohydrate and beta-alanine, alone or combined, on repeated sprint performance and physiological parameters in amateur team and racket sport players. Kinesiology. 2020 May 21;52(1):115–123. doi: 10.26582/k.52.1.15
- Arazi H, Eghbali E, Karimifard M. Effect of creatine ethyl ester supplementation and resistance training on hormonal changes, body composition and muscle strength in underweight non-athlete men. Biomed Hum Kinet. 2019;11(1):158–166. doi: 10.2478/bhk-2019-0022
- Almeida D, Colombini A, Machado M. Creatine supplementation improves performance, but is it safe? double-blind placebo-controlled study. J Sports Med Phys Fitness. 2020;60(7):1034–1039. doi: 10.23736/S0022-4707.20.10437-7
- Candow DG, Chilibeck PD, Gordon J, et al. Effect of 12 months of creatine supplementation and whole-body resistance training on measures of bone, muscle and strength in older males. Nutr Health. 2021 Jun;27(2):151–159. doi: 10.1177/0260106020975247
- Marini ACB, Motobu RD, Freitas ATV, et al. Short-term creatine supplementation May alleviate the malnutrition-inflammation score and lean body Mass loss in hemodialysis patients: a Pilot randomized placebo-controlled trial. JPEN J Parenter Enteral Nutr. 2020 Jul;44(5):815–822. doi: 10.1002/jpen.1707
- Anders JPV, Neltner TJ, Smith RW, et al. The effects of phosphocreatine disodium salts plus blueberry extract supplementation on muscular strength, power, and endurance. J Int Soc Sports Nutr. [2021 Sep 9];18(1):60. doi: 10.1186/s12970-021-00456-y
- Bonilla DA, Kreider RB, Petro JL, et al. Creatine enhances the effects of cluster-set resistance training on lower-limb body composition and strength in resistance-trained men: a Pilot study. Nutrients. [2021 Jul 4];13(7):2303. doi: 10.3390/nu13072303
- Pakulak A, Candow DG, Totosy de Zepetnek J, et al. Effects of creatine and caffeine supplementation during resistance training on Body composition, strength, endurance, rating of perceived exertion and fatigue in trained young adults. J Diet Suppl. 2022 Sep 3;19(5):587–602. doi: 10.1080/19390211.2021.1904085
- Almeida D, Pereira R, Borges E, et al. Creatine supplementation improves physical performance, without negative effects on health markers, in young weightlifters. J Sci In Sport And Exercise. 2022 Jan 31;4(3):255–265. doi: 10.1007/s42978-021-00147-9
- Vukovich MD, Peeters BM. RELIABILITY of AIR-DISPLACEMENT PLETHYSMOGRAPHY in DETECTING BODY COMPOSITION CHANGES AFTER WATER INGESTION and AFTER CREATINE SUPPLEMENTATION. J Exercise Physiol Online. 2003;6(2):115–122.
- Butchart S, Candow DG, Forbes SC, et al. Effects of creatine supplementation and progressive resistance training in stroke survivors. Int J Exerc Sci. 2022;15(2):1117–1132.
- Dinan NE, Hagele AM, Jagim AR, et al. Effects of creatine monohydrate timing on resistance training adaptations and body composition after 8 weeks in male and female collegiate athletes. Front Sports Act Living. 2022;4:1033842. doi: 10.3389/fspor.2022.1033842
- Askow AT, Paulussen KJM, McKenna CF, et al. Creatine monohydrate supplementation, but not Creatyl-L-Leucine, increased muscle creatine content in healthy young adults: a double-blind randomized controlled trial. Int J Sport Nutr Exerc Metab. [2022 Nov 1];32(6):446–452. doi: 10.1123/ijsnem.2022-0074
- Pinto CL, Botelho PB, Carneiro JA, et al. Impact of creatine supplementation in combination with resistance training on lean mass in the elderly. J Cachexia Sarcopenia Muscle. 2016 Sep;7(4):413–421. doi: 10.1002/jcsm.12094
- van Loon Lj, Oosterlaar AM, Hartgens F, et al. Effects of creatine loading and prolonged creatine supplementation on body composition, fuel selection, sprint and endurance performance in humans. Clin Sci (Lond). 2003 Feb;104(2):153–162. doi: 10.1042/cs1040153
- Terrillion KA, Kolkhorst FW, Dolgener FA, et al. The effect of creatine supplementation on two 700-m maximal running bouts. Int J Sport Nutr. 1997 Jun;7(2):138–143. doi: 10.1123/ijsn.7.2.138
- Maganaris CN, Maughan RJ. Creatine supplementation enhances maximum voluntary isometric force and endurance capacity in resistance trained men. Acta Physiol Scand. 1998 Jul;163(3):279–287. doi: 10.1046/j.1365-201x.1998.00395.x
- Eijnde BO, Hespel P. Short-term creatine supplementation does not alter the hormonal response to resistance training. Med Sci Sports Exerc. 2001 Mar;33(3):449–453. doi: 10.1097/00005768-200103000-00018
- Huso ME, Hampl JS, Johnston CS, et al. Creatine supplementation influences substrate utilization at rest. J Appl Physiol ( 1985). 2002 Dec;93(6):2018–2022. doi: 10.1152/japplphysiol.01170.2001
- Walter MC, Reilich P, Lochmüller H, et al. Creatine monohydrate in myotonic dystrophy: a double-blind, placebo-controlled clinical study. J Neurol. 2002 Dec;249(12):1717–1722. doi: 10.1007/s00415-002-0923-x
- Taes YE, Delanghe JR, De Bacquer D, et al. Creatine supplementation does not decrease total plasma homocysteine in chronic hemodialysis patients. Kidney Int. 2004 Dec;66(6):2422–2428. doi: 10.1111/j.1523-1755.2004.66019.x
- Tarnopolsky M, Mahoney D, Thompson T, et al. Creatine monohydrate supplementation does not increase muscle strength, lean body mass, or muscle phosphocreatine in patients with myotonic dystrophy type 1. Muscle And Nerve. 2004 Jan;29(1):51–58. doi: 10.1002/mus.10527
- Perret C, Mueller G, Knecht H. Influence of creatine supplementation on 800 m wheelchair performance: a pilot study. Spinal Cord. 2006 May;44(5):275–279. doi: 10.1038/sj.sc.3101840
- Ahmun RP, Tong RJ, Grimshaw PN. The effects of acute creatine supplementation on multiple sprint cycling and running performance in rugby players. J Strength Cond Res. 2005 Feb;19(1):92–97. doi: 10.1519/00124278-200502000-00016
- Ball S, Bowen-Thwaits J, Swan P. ORAL CREATINE SUPPLEMENTATION DOES NOT IMPROVE BODY COMPOSITION in RECREATIONALLY ACTIVE MEN DURING STRENGTH TRAINING. J Exercise Physiol Online. 2004;7(6):9–15.
- Hile AM, Anderson JM, Fiala KA, et al. Creatine supplementation and anterior compartment pressure during exercise in the heat in dehydrated men. J Athl Train. 2006 Jan-Mar;41(1):30–35.
- Kuethe F, Krack A, Richartz BM, et al. Creatine supplementation improves muscle strength in patients with congestive heart failure. Pharmazie. 2006 Mar;61(3):218–222.
- Wright GA, Grandjean PW, Pascoe DD. The effects of creatine loading on thermoregulation and intermittent sprint exercise performance in a hot humid environment. J Strength Cond Res. 2007 Aug;21(3):655–660. doi: 10.1519/00124278-200708000-00002
- Stout JR, Sue Graves B, Cramer JT, et al. Effects of creatine supplementation on the onset of neuromuscular fatigue threshold and muscle strength in elderly men and women (64 - 86 years). J Nutr Health Aging. 2007 Nov-Dec;11(6):459–464.
- de Oca R M-M, Farfán-González F, Camarillo-Romero S, et al. Effects of creatine supplementation in taekwondo practitioners. Nutr Hosp. 2013 Mar-Apr;28(2):391–399. doi: 10.3305/nh.2013.28.2.6314
- Hayashi AP, Solis MY, Sapienza MT, et al. Efficacy and safety of creatine supplementation in childhood-onset systemic lupus erythematosus: a randomized, double-blind, placebo-controlled, crossover trial. Lupus. 2014 Dec;23(14):1500–1511. doi: 10.1177/0961203314546017
- Moore SR, Gordon AN, Cabre HE, et al. A randomized controlled trial of changes in fluid distribution across menstrual phases with creatine supplementation. Nutrients. 2023Jan 13;15(2):429. doi: 10.3390/nu15020429
- Sewell DA, Robinson TM, Greenhaff PL. Creatine supplementation does not affect human skeletal muscle glycogen content in the absence of prior exercise. J Appl Physiol ( 1985). 2008 Feb;104(2):508–512. doi: 10.1152/japplphysiol.00787.2007
- Candow DG, Chilibeck PD, Forbes SC. Creatine supplementation and aging musculoskeletal health. Endocrine. 2014;45(3):354–361. doi: 10.1007/s12020-013-0070-4
- Devries MC, Phillips SM. Creatine supplementation during resistance training in older adults—a meta-analysis. Med & Sci In Sports & Exercise. 2014;46(6):1194–1203. doi: 10.1249/MSS.0000000000000220
- Dos Santos EEP, de Araújo Rc, Candow DG, et al. Efficacy of creatine supplementation combined with resistance training on muscle strength and muscle mass in older females: a systematic review and meta-analysis. Nutrients. 2021;13(11):3757. doi: 10.3390/nu13113757
- Kreider RB, Jäger R, Bioavailability PM, et al. Safety, and regulatory status of creatine and related compounds: a critical review. Nutrients. [2022 Feb 28];14(5):1035. doi: 10.3390/nu14051035
- Wall BT, Stephens FB, Constantin-Teodosiu D, et al. Chronic oral ingestion of l-carnitine and carbohydrate increases muscle carnitine content and alters muscle fuel metabolism during exercise in humans. J Physiol. 2011;589(4):963–973. doi: 10.1113/jphysiol.2010.201343
- Rawson ES, Wehnert ML, Clarkson PM. Effects of 30 days of creatine ingestion in older men [article]. Eur J Appl Physiol. 1999;80(2):139–144. doi: 10.1007/s004210050570
- Ball SD, Bowen-Thwaits J, Swan PD. Oral creatine supplementation does not improve body composition in recreationally active men during strength training [article]. J Exercise Physiol Online. 2004;7(6):9–15.
- Huso ME, Hampl JS, Johnston CS, et al. Creatine supplementation influences substrate utilization at rest [article]. J Appl Physiol. 2002;93(6):2018–2022. doi: 10.1152/japplphysiol.01170.2001
- Powers ME, Arnold BL, Weltman AL, et al. Creatine supplementation increases total body water without altering fluid distribution. J Athl Train. 2003 Mar;38(1):44–50.
- van Loon Lj, Murphy R, Oosterlaar AM, et al. Creatine supplementation increases glycogen storage but not GLUT-4 expression in human skeletal muscle. Clin Sci (Lond). 2004 Jan;106(1):99–106. doi: 10.1042/CS20030116
- Farshidfar F, Pinder MA, Myrie SB. Creatine supplementation and skeletal muscle metabolism for building muscle Mass- review of the potential mechanisms of action. Curr Protein Pept Sci. 2017;18(12):1273–1287. doi: 10.2174/1389203718666170606105108
- Ribeiro AS, Avelar A, Kassiano W, et al. Creatine supplementation does not influence the ratio between intracellular water and skeletal muscle mass in resistance-trained men. Int J Sport Nutr Exerc Metab. 2020;30(6):405–411. doi: 10.1123/ijsnem.2020-0080
- Rogers ME, Bohlken RM, Beets MW, et al. Effects of creatine, ginseng, and astragalus supplementation on strength, body composition, mood, and blood lipids during strength-training in older adults [article]. J Sports Sci Med. 2006;5(1):60–69.
- Herda TJ, Beck TW, Ryan ED, et al. Effects of creatine monohydrate and polyethylene glycosylated creatine supplementation on muscular strength, endurance, and power output [article]. J Strength Cond Res. 2009;23(3):818–826. doi: 10.1519/JSC.0b013e3181a2ed11
- Delextrat A, Targen N, Impson-Davey G, et al. Effects of supplementation with creatine monohydrate and beta-alanine, alone or combined, on repeated sprint performance and physiological parameters in amateur team and racket sport players [article]. Kines (Zagreb, Online). 2020;52(1):115–123. doi: 10.26582/k.52.1.15
- Wu SH, Chen KL, Hsu C, et al. Creatine supplementation for muscle growth: a scoping review of randomized clinical trials from 2012 to 2021. Nutrients. [2022 Mar 16];14(6):1255. doi: 10.3390/nu14061255
- Forsberg A, Nilsson E, Werneman J, et al. Muscle composition in relation to age and sex. Clin Sci. 1991;81(2):249–256. doi: 10.1042/cs0810249
- Syrotuik DG, Bell GJ. Acute creatine monohydrate supplementation: a descriptive physiological profile of responders vs. nonresponders. The J Strength & Cond Res. 2004;18(3):610–617. doi: 10.1519/00124278-200408000-00039
- Branch JD. Effect of creatine supplementation on body composition and performance: a meta-analysis. Int J Sport Nutr Exerc Metab. 2003;13(2):198–226. doi: 10.1123/ijsnem.13.2.198
- Devries MC, Phillips SM. Creatine supplementation during resistance training in older adults-a meta-analysis. Med Sci Sports Exerc. 2014 Jun;46(6):1194–1203. doi: 10.1249/MSS.0000000000000220