Organophosphate compounds, the most widely used insecticides worldwide, may cause serious poisoning. The inhibition (phosphorylation) of cholinesterase activity leads to the accumulation of acetylcholine at synapses. This pharmacological phenomenon further leads to over stimulation and disruption of impulse transmission in both the central and peripheral nervous system (Citation1).
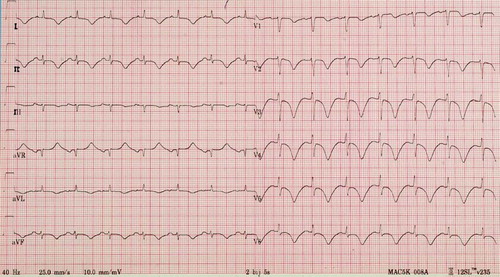
We report a 63 year old woman who ingested a 500 ml bottle of parathion. Intubation was necessary upon arrival of the emergency services due to massive salivation. The severity of poisoning is illustrated by prolonged extremely low serum cholinesterase activity, the necessity for high doses of both the reactivator pralidoxime (continually up to 1g/hour for 48 hours) and atropine, as well as a long duration of ventilation of 7 days. As early as 6 hours after ingestion up to 6 days after admission, impressive ECG changes were present in this case, as illustrated in . Other causes of these non-specific ST-segment and T-wave abnormalities were excluded (Citation2): normal echocardiography and coronary angiography as well as serial cardiac enzymes excluded myocarditis or myocardial ischemia. A CT-scan did not show subarachnoidal haemorrhage or pulmonary embolism. No electrolyte or acid-base disturbances, neither the intake of other drugs or hypothyroidism was present.
Fig. 1. The electrocardiogram demonstrates the “characteristic” diffuse ST-segment and T wave inversion and QTc-prolongation in this case of severe organophosphate poisoning. These electrocardiographic changes were present in this patient as early as 6 hours up to 6 days after admission, regardless of the treatment.
The ECG may indeed display a variety of abnormalities in acute organophosphate poisoning. In a large series, these so called “toxic repolarization anomalies” in the form of QTc prolongations and pathologic repolarization (diffuse ST- and T-inversion anomalies), were present in up to 134 out of 168 cases (Citation3). This high incidence of these ECG changes has been confirmed by others (Citation1,Citation4), eventually leading to polymorphic ventricular tachycardia of the torsade de pointe type (Citation4,Citation5). Moreover these impressive electrocardiographic changes mimicking severe ischemia have been reported from the first up to the twentieth day depending on the severity of the intoxication (Citation3). It has been proposed that this consists of different phases: a (brief) transient phase of intense increased sympathetic tone, resulting in serious tachycardia, followed by a prolonged period of extreme parasympathetic activity, causing sinus bradycardia, atrioventricular block, ST segment, and T wave abnormalities and QTc interval prolongation (Citation1,Citation5). As these changes have been described even during high-dose atropine treatment, the proposed protective effect of atropine on arrhythmias could not be verified.
As QTc prolongation is believed to originate from intense and unequal sympathetic stimulation of myocardial fibers, it is not surprising to find these ECG abnormalities in cases with severe organophosphate poisoning with autonomic discharge and/or altered consciousness. The inhibition of cholinesterase activity leads to over stimulation and disruption of impulse transmission in both the central and peripheral nervous system, also by interfering with synaptic transmission peripherally at muscarinic neuro effector junctions and nicotine receptors within sympathetic ganglia (Citation1).
References
- FR Chuang, SH Jang, JL Lin, MS Chern, JB Chen, and KT Hsu. (1996). QTc prolongation indicates a poor prognosis in patients with organophospahte poisoning. Am J Emerg Med 14:451–453.
- A Kumar, and D Lloyd-Jones. (2007). Clinical significance of minor nonspecific ST-segment and T-wave abnormalities in asymptomatic subjects: a systematic review. Cardiology in review 15:133–142.
- Z Kiss, and I Fazekas. (1979). Arrhythmias in organophosphate poisonings. Acta Cardiologica 34:323–330.
- P Karki, JA Ansari, S Bhandary, and S Koirala. (2004). Cardiac and electrocardiographical manifestations of acute organophosphate poisoning. Singapore Med J 45:385–389.
- A Ludomizsky, H Klein, P Sarelli, B Becker, S Hoffman, U Taitelman, and et al. (1982). QT-prolongation and polymorphous (torsade de pointes) ventricular arrhytmias associated with organophosphorus insecticide poisoning. Am J Cardiol 49:1654–1658.