
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Case attrition along the medico-legal referral pathway for sexual and domestic violence survivors has drawn attention worldwide. Despite much research about the prevalence of sexual and domestic violence in Kenya, little is known about factors impacting progress through the medico-legal referral pathway. To address this research gap, we analyzed data from the Wangu Kanja Foundation, based in Nairobi, to test which key case characteristics have explanatory power in predicting case progression. We used a sequential logit model to evaluate case progression as a series of distinct choices. Our analysis revealed that age of the survivor was the strongest predictor for all steps of the pathway, and that the presence of forensic evidence was also associated with increased odds of moving through each step. These findings reflect cultural ideas about what legitimizes a case of sexual or domestic violence and can be used to inform policy targeted at strengthening the case referral pathway in Kenya.
Introduction
In Kenya, as elsewhere, sexual violence (SV) and domestic violence (DV) affect the lives of people of all ages, particularly those of women and girls (Garcia-Moreno et al., Citation2005). Close to 41% of women in Kenya have experienced DV and/or SV at least once in their lifetime, with nearly 26% report having experienced it within the previous 12 months (Ministry of Health Kenya et al., Citation2015). For comparison, 25% of women in the United States and 30% of women in England and Wales have experienced lifetime DV and/or SV (Office for National Statistics [ONS], Citation2022; Truman et al., Citation2014).
Women and girls in Kenya are also at risk of SV from a young age. A third of females and nearly a fifth of males in Kenya experience childhood (i.e., age <18) SV according to the most recent population-based survey (UNICEF et al., Citation2012). For females, 18% have experienced SV by the age of 13, 39% by the ages of 14–15, and 43% by the ages of 16–17 years (UNICEF et al., Citation2012). Additionally, 24.3% of female survey respondents stated that they had experienced sexual intercourse against their will prior to the age of 18.
Despite these high rates of SV and DV, there is very little research on case adjudication in Kenya. What is known about SV and DV in Kenya originates largely from work seeking to measure prevalence using the Demographic and Health Survey (DHS). The DHS asks women if they have experienced violence using a modified version of the Conflict Tactics Scale, which lists some types of violence but excludes others, an approach that often underestimates the actual prevalence of violence (Ministry of Health Kenya et al., Citation2015).
To prevent and protect people from SV, Kenya passed The Sexual Offences Act in 2006. It defines acts that constitute sexual offences and sets minimum sentences. Nevertheless, sexual and gender-based violence (SGBV) convictions are rare in Kenya and the country has relatively high rates of SV and DV (Shadle, Citation2010; UN Women, Citation2016). The current research is the first to systematically study SV and DV case attrition along the medico-legal case referral pathway in Kenya, wherein cases reported by victim-survivors to the authorities are recorded and proceed from medical facilities to the police station, then the prosecutor’s office, and finally to the court system. To our knowledge, only two other studies have investigated case attrition in Africa (both in South Africa, (Artz & Smythe, Citation2007; Machisa et al., Citation2022). It is not altogether surprising that there is little research on SV and DV case attrition in Kenya. Research on this topic requires case-level data that are linked across multiple agencies. Data of this nature are typically unavailable in low-income countries.
Our analysis of SV and DV case attrition is based on data from SV survivors who sought services from the non-profit Wangu Kanja Foundation (WKF), a Kenyan NGO, between 2016–2020. The WKF supports adult and child survivors along the medico-legal case referral pathway, which in Kenya includes medical services, security services, and official justice via the police and courts.
The WKF dataset allowed us to analyze case attrition along the medico-legal case referral pathway among SV and DV survivors. In Kenya, cases proceed along the pathway in a stepwise fashion and in a predetermined order (i.e., the survivor must first obtain a medical report before reporting the crime to the police, and so forth). Thus, the data structure allows us to use sequential logit models to study case attrition (Buis, Citation2017). We studied case attrition across the pathway as a function of key case characteristics, such offense type, demographic information about the victim and perpetrator, and information about evidence in the case (i.e., DNA, clothing, weapon used) to test which have explanatory power in predicting case progression. The outcome variables tested included whether medical services were accessed, whether the case was reported to the police, whether the case proceeded to the prosecutors’ office, and whether the cases went to court. Sequential logit models were chosen because they allow for evaluating the effect of an explanatory variable (in this case engagement with steps along the case referral pathway) with the outcome (e.g., the case being reported to the police; Buis, Citation2017). Each interaction with a different step along the case referral pathway can be thought of as a transition to the next step, which means, for example, that to reach step three, the survivor must first have passed through steps one and two. The approach also allowed us to evaluate which case factors (e.g., evidence, relationship between the victim and perpetrator) influence each transition along the case referral pathway (Pattavina et al., Citation2021). By identifying which steps of the pathway are reached and what case factors are most likely to lead a victim through each step, targeted interventions can be designed and implemented at crucial points along the pathway.
Case attrition
Case attrition, which refers to the cases which are lost or dropped from the criminal justice process, is a problem that has been seen in sexual violence cases for decades (Gregory & Lees, Citation1996). In the 1980s, research showed that a high proportion of rape and sexual assault cases reported in the United Kingdom were categorized by the police as “no-crimes” and were not recorded as offenses, with similar research across multiple American cities finding that sexual assault complaints were often categorized by police as “unfounded,” meaning that the case was not regarded as constituting a crime (Gregory & Lees, Citation1996; Kerstetter, Citation1990; Spohn & Tellis, Citation2012). Additionally, the few cases that did proceed to court largely ended up either in a conviction for a less serious offence or in acquittal (Gregory & Lees, Citation1996; Hohl & Stanko, Citation2015; Smith & Skinner, Citation2017). While limited research on the decision to prosecute rape cases has been conducted in Kenya, research conducted elsewhere has found that there are a few factors that predict the filing of charges against a perpetrator. These include the presence of injuries to the victim, the use of a weapon during the assault, evidence that calls into question the victim’s moral character, and a timely report by the victim (Beichner & Spohn, Citation2005). Additionally, women who are perceived to have engaged in “risk-taking” behavior, such as hitchhiking, walking alone at night, being in a bar alone, or using alcohol or drugs are less likely to be seen as genuine victims, and thus are less likely to have their cases prosecuted (Spohn & Holleran, Citation2001).
Prior work has found that sexual violence cases are less likely to move through the case referral pathway from reporting to prosecution and then conviction than other types of offenses, often due to a combination of legal factors and extra-legal factors, with legal factors including whether the sexual assault charge is one of a number of charges and with extra- legal factors including perceived victim cooperation (Hester & Lilley, Citation2017; Lovell et al., Citation2021). Previous research has also revealed that a combination of factors can predict attrition at various points along the care-seeking pathway, including victim characteristics, the location or duration of the offense, and evidence of the attack (Lea et al., Citation2016). The relationship between the victim and offender and the perceived vulnerability of the victim have also been found to increase attrition in sexual violence cases, with cases involving intimate partners being treated differently by the criminal justice system than cases involving strangers or acquaintances (Hester & Lilley, Citation2017; Kerstetter, Citation1990; Spohn & Tellis, Citation2012). Case attrition can also occur due to the desires of the victims to no longer formally pursue the case, perhaps due to the perceived mental health burden of the process or threats from the perpetrator, although accurate numbers on this may be hard to determine due to a lack of clarity about whether the individuals themselves wanted to drop the case or whether they felt pressured to do so by police or others around them (Lea et al., Citation2003; Murphy et al., Citation2014). Additionally, other factors that predict case progression include the victim’s character and details about the offense that are consistent with rape myths, which are beliefs about rape that serve to discredit the victim’s claims, such as a woman’s revealing clothing being the reason she was assaulted, and are deeply entrenched in society (Murphy-Oikonen et al., Citation2022; Thelan & Meadows, Citation2022). Rape myth acceptance on the part of criminal justice practitioners, including the jurors selected for rape cases, has been associated with case attrition in upper-income (e.g., the US and the UK) as well as lower-income countries (Artz & Smythe, Citation2007; Leverick, Citation2020; Temkin et al., Citation2016; Withers et al., Citation2019).
There is considerable case attrition in Kenya, owing in part to the complex case referral pathway that is often challenging for victim-survivors to navigate. The Kenyan health system relies on the Division of Reproductive Health to provide policy and capacity development for SV cases; however, Kenya’s integrated approach to primary care, which aims to treat patients holistically rather than through specialization, is under-developed, making it difficult for survivors of SV to access the vital post-assault services they typically require (Kilonzo, Theobald, et al., Citation2009). These include forensic medical exams, pregnancy tests, and HIV prophylaxis, as well as legal assistance.
Facilities that offer post-rape services frequently lack proper protocols and confidential spaces for SGBV survivors to receive treatment, and there are poor reporting and procedural requirements. As a result, survivors are often evaluated improperly (i.e., in a manner that is inconsistent with government forensic protocols) and given insufficient counselling (Kilonzo, Theobald, et al., Citation2009). Additionally, survivors often face financial barriers, such as being asked to pay to print medical or legal forms, or for drugs and other services in public institutions (Kilonzo, Theobald, et al., Citation2009). There are also poor community structures for long-term follow-up with survivors. The infrastructure at health facilities for comprehensive SV services is inadequate and thus forensic evidence is collected improperly, and the linkage between the medical and legal sectors is weak (Temmerman et al., Citation2018). For instance, if medical professionals do not use an official government form to record their clinical notes, the information cannot be used as evidence in court (Kilonzo, Ndung’u, et al., Citation2009).
Additionally, the law requires that medical evidence is presented in court by an “expert witness”; however, medical professionals providing care to survivors are often not deemed to be experts by the courts (Kilonzo, Ndung’u, et al., Citation2009). Moreover, cases of rape or other forms of SV, usually in provinces outside of Nairobi, against both children and adults, are settled out of court through clan elders, which often results in a lack of medical treatment and justice for survivors (Mwangi et al., Citation2009; Wangamati et al., Citation2019). All these factors, along with corruption and low rates of reporting to the authorities, as well as financial, material, and infrastructural resource barriers, both for survivors and providers, contribute to few successful prosecutions in Kenya (Lekakeny, Citation2015; Wangamati et al., Citation2019).
Some previous research has shown that case characteristics have a significant effect on case outcomes. One such characteristic is the relationship between the victim and the perpetrator, with stranger rape often being taken more seriously than acquaintance rape, and the prior relationship between the defendant and the victim affecting the prosecutor’s decision as to whether to file charges (Spohn & Horney, Citation1993). Conversely, other research has shown that the most prominent factors relating to decisions made by police, prosecutors, and jurors, are legally relevant factors. For instance, the victim’s ability to identify the suspect, the use of a weapon, promptness of reporting, and the age of the victim have all been associated with case attrition in the Global North (LaFree, Citation1989). In the Kenyan context, case characteristics, such as long delays between the crime and attending a health facility, the relationship between the perpetrator and survivor, and number of perpetrators, have been identified as important details when determining whether a case will be processed (Anastario et al., Citation2014).
Data and methods
The data for this study were recorded from the case records of 514 survivors who were assisted by the Wangu Kanja Foundation between the years of 2016–2020, inclusive. The WKF is a non-profit organization founded in 2005 in Nairobi by Wangu Kanja, a rape survivor. The WKF aids survivors in accessing post-rape care services. In addition to its work in supporting survivors in the aftermath of SV and DV, the WKF advocates for initiatives pertaining to SGBV prevention, protection, and response throughout Kenya. The WKF collaborates with the Survivors of Sexual Violence in Kenya Network, which works to build survivor self-agency, amplify survivors’ voices across the country to address all forms of SV, and restore survivors’ dignity post-violation (Wangu Kanja Foundation, Citation2016). The WKF dataset is the most comprehensive dataset on SV and DV in Kenya (Ji et al., Citation2022). The dataset was gathered by the WKF over a four-year period, and it links case outcomes with the survivor’s account of the offense and other information about the offense from police and medical reports.
Gender defenders, survivors of SV and DV who provide support to victims and are trained by the WKF, interviewed survivors about their SV and DV ordeal. They gathered information including the time, date, and location of the incident, as well as information about the offense, including demographics of both the victim and perpetrator, the number of perpetrators committing the offense, the relationship between survivor and perpetrator, what (if any) post-assault services the survivor accessed, and what (if any) forensic evidence was available to criminal investigators, such as evidence of physical injury to the survivor, or biological specimens, such as semen or hair.
There were multiple ways that survivors could access support from the WKF. This included those walking into the WKF headquarters in Nairobi, using an SMS text platform, or using the foundation’s own mobile phone application, then called MobApp. Due to data availability, we focus on walk-ins only. Our data included 277 participants who were adults and 237 who were children, as defined by Kenya’s defilement law, which states that a person under 18 years of age is a child (Sexual Offences Act, Citation2006).
After further reviewing the data and excluding 111 cases for which the data were incomplete, we were left with 212 adults and 194 children for our statistical analysis.
provides descriptive statistics of the variables used in our analysis for combined sexual and domestic violence cases. Descriptive statistics for each type of violence can be found in appendix 1. We were interested in two outcome measures. First, whether the case was reported to the police. Second, whether the case proceeded to court. The case proceeding to court is the final procedural outcome for all cases progressing through the case referral system, with the final decision then being whether the perpetrator was sentenced. Our selection of variables captures details about the location of the attack, categorized as either public or private, whether the survivor knew the perpetrator at the time of the attack, if the survivor was a child, if there was forensic evidence present at the time of the medical examination, the survivor’s age, and if the survivor was a female. An important feature of our data is that the mean age is 20, in line with previous research indicating that significant proportions of both females and males in Kenya experience sexual violence before the age of 18 (UNICEF et al., Citation2012). Figures in the appendix indicate the distribution of ages in our data and makes clear that a substantial proportion of survivors in our sample are adolescents. The analyses were performed on the full sample (i.e., all case types considered together in the same model), as well as separately on each case type (i.e., SV and DV cases were analyzed in different models).
Table 1. Descriptive statistics.
Analytic approach
This secondary data analysis used a quantitative cross-sectional research design. The outcome variable for this analysis was how far the case progressed through the case referral pathway. We studied this for all crimes, and separately for DV and SV. Predictor variables used in this analysis include characteristics of both the victims and perpetrators, such as whether the victim was a child, age, relationship, and gender. It also included key evidentiary factors, namely the presence or absence of physical injury, and whether post-assault care services were accessed. These services include connection to medical services, counseling, psychosocial support, and support reporting the case to the police. All variables other than age, which is continuous, are binary.
Procedure
The data were collected via face-to-face interviews between the Gender Defenders and the survivors using a standardized data collection sheet. Information provided on the forms was read and coded by fellow researchers, and whenever missing data were discovered, the Wangu Kanja Foundation was contacted to attempt to complete the dataset, although this was often not possible owing to a lack of information in the case file.
Ethics
The secondary data used in this study was the property of the Wangu Kanja Foundation and the Survivors of Sexual Violence in Kenya Network. These organizations provided us with permission to analyze their data and all work adhered to the Kenyan Data Protection Act. The research was also approved by the STEM Ethics Committee at the University of Birmingham. None of the participants were placed at an increased risk of harm because of their participation.
The WKF provided the survivors who reported to them the opportunity to contact support services post-interview if required.
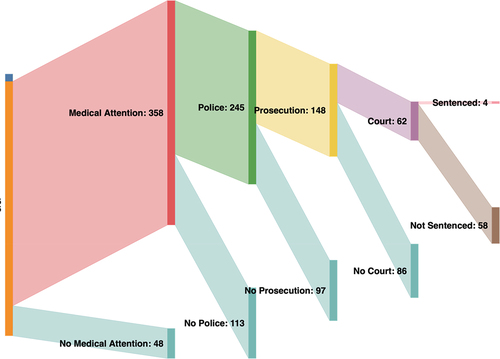
maps the case referral pathway for the full sample. At the first transition, the decision is made by the survivor to seek medical attention (coded as 1 = yes and 0 = no). Nearly the entire sample made it to this stage, the effects of which are explained later in the paper. After seeking medical help, survivors may choose to seek assistance from the police. This decision is made by the survivor, although they cannot progress to this stage until they have received medical attention and procured the appropriate forms that the police require to officially record the case. At the next stage, prosecutors might decide to file charges, which is the third stage in the case referral pathway, but this often depends on case characteristics, which are explained below. The final stage of the referral pathway, reflected in purple in , is the case proceeding to court. Although cases may proceed to court, many do not continue to the sentencing phase due to issues with the required medicolegal officials not being able to attend court and endless delays causing already traumatized survivors to lose confidence in the formal legal process. Cases that make it to this stage have the potential to move on to sentencing, although the diagram shows that few cases progress to this point.
Figure 1. Sexual and domestic violence case referral pathway.
Our research objective was to analyze these data to identify the factors associated with attrition from the case referral pathway. Our data contain the proportion of survivors by crime type who accessed medical, police, and judicial services. We used sequential logit models to study case attrition along the case referral pathway, which dictates that survivors should be referred from medical services to the police and then to judicial services.
Results
presents frequency data on case progression (top row) and attrition (bottom row) along the pathway. The key property of the medico-legal pathway, as evidenced in , is that it is ordered. Survivors must first attend medical care before proceeding to the police, and a prosecutor will not take up a case until the survivor has visited both medical and police officials and obtained the proper documents. Likewise, the decision to prosecute the perpetrator of the attack occurs before the case proceeds to court and after the police decide to charge the accused with the crime. The number of cases that progress to the stage versus those that fail at the stage are depicted. As can be seen, case attrition increases across the pathway when moving from left to right as evidenced by the decreasing size of the shaded areas in the top row of .
We used a sequential logit model to evaluate the correlates of survivors’ and the progression of their cases along the medical-legal pathway (Fullerton, Citation2009; Maddala, Citation1983; Mare, Citation1980). This model is appropriate because it models case progression as a series of distinct choices, whereas multinomial or nested logit models do not. For example, multinomial and nested logit models would categorize cases based on their final disposition (i.e., conviction, acquittal, dismissal). However, the complexity of the legal process and the many distinct choices made by different actors at different stages of the process that influence the final case outcome would not be captured if these modelling approaches were used. The decisions in help-seeking are made at different times given different information and are also made by different people. While the survivor decides to seek medical support and report the rape to the police, subsequent choices regarding how the case moves through the system are made by the police, public prosecutors, and the court. Further, we did not conduct multiple logistic regression analysis as it does not analyze case progression as a series of multiple distinct stages. In sum, sequential logit modelling allows for greater nuance in studying the challenges that survivors face along the medical-legal pathway. It provides a more accurate representation of the reality of the legal process and thereby allows the examination of the factors that impact case progression at each stage. By using this approach, we can better understand the challenges that survivors face. The stages we analyzed are provided in and . Very few cases led to a conviction; therefore, we do not include this stage in our statistical analysis.
Estimation of a sequential logit model amounts to jointly estimating a separate logit model for each node of the decision tree, noting that the coefficients should be identical if we estimate the models separately, but that estimating them jointly facilitates the decomposition exercise that is reported below (Buis, Citation2017). In particular, the coefficient estimates reported in will be identical. The advantage of the sequential logit procedure is that it allows the computation of the quantities, such as the gain, reported in and discussed below.
Table 2. Estimated weights for each stage of the medical-legal pathway, and their determinants.
Figure 2. Sequential logit estimates (all cases).
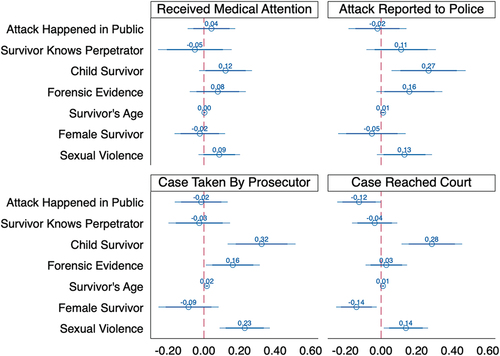
Figure 3. Sequential logit estimates (sexual violence cases).
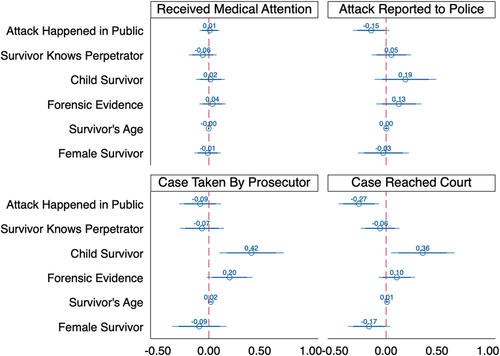
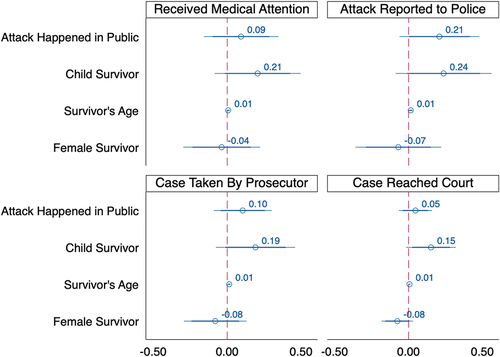
Figure 4. Sequential logit estimates (domestic violence cases).
Thus, we write the estimated probability of survivor receiving medical treatment
as:
Where is the logistic function and
are covariates describing key features of the case such as the survivor’s age and
are the associated regression coefficient estimates. Likewise, the probabilities of “success” for survivor i and their case at subsequent nodes are given as follows:
if
if
if
The results of this analysis are displayed in . The circles display the average marginal effects associated with each of the covariates while the narrow (and wide) horizontal line displays the 95% (and 99%) confidence interval of the average marginal effect (Wooldridge, Citation2010). These average marginal effects can be interpreted as the change in the probability of the outcome variable. Thus, an average marginal effect of 0.05 suggests that the outcome is 5% more likely, and so forth. For convenience, we also report the results numerically in in the appendix.
Looking first at the upper left panel of we can see that there are two statistically significant correlates of whether a survivor received medical attention. Survivors of SV were around 9% [ME = 0.09, p = .058] more likely to receive medical attention than DV survivors. Child survivors were also 12% more likely to receive medical attention [ME = 0.12, p = .035]. The lack of precise estimates for these, and particularly for the other correlates, may reflect the high proportion of survivors in our sample who received medical attention (89%) and thus there was a limited amount of variation.Footnote1
The results plotted in the upper right panel, for whether survivors report to the police, are more precise, perhaps because only 60% of all cases lead to a police report. Note that now our sample is different, it is now only those who received medical attention. This will be true for subsequent stages discussed below, the sample will only be those who progressed at the previous stage. As with the receipt of medical care, violence against children [ME = 0.27, p < .001]and SV [ME = 0.13, p = .029]] were both more likely to lead to a police report. The results also suggest that older survivors are also more likely to contact the police, with an additional year of age found to increase the chance of reporting by 1% [ME = 0.01, p = .006]. For clarity, in we report the estimated effect for an increase in five years of age. Note, given we also included a variable for whether the victim is a child in the model, the results suggest an older adult (or an older child) is more likely to make a police report. Perhaps, as might be expected, the availability of physical evidence is also positively correlated with contacting the police, [ME = 0.16, p =. 027].
The bottom left panel plots the results for whether, following a police report, a prosecutor decides to file charges. This happens in around 60% of such cases making it to this stage (or 36% of all attacks in our data). The results are like those for the decision to file a police report, but again more precise. We can see that SV compared to DV, and attacks against children compared to adults, are 23% [ME = 0.23, p < .001] and 33% [ME = 0.33, p < .001] more likely to lead to prosecution. The availability of forensic evidence is also again important, with cases with evidence being 16% [ME = 0.16, p = .006] more likely to be prosecuted. The effect of survivor age is now larger, with a survivor who is two years older being 3% more likely to have their case prosecuted [ME = 0.016, p < .001]. It is not statistically significant at conventional levels (i.e., p < .05), but as can be seen in , the results also hint that female compared to male survivors are less likely to have their case prosecuted, other things being equal.
The final, bottom right, panel plot results for whether the case proceeds to court. Again, we see that children [ME = 0.28, p < .001], survivors of SV [ME = 0.14, p = .004] and older survivors [ME = 0.01, p < .001] are more likely to see their cases come to court. However, other results are interestingly different at this stage compared to earlier stages. Firstly, evidence is no longer an important factor [ME = 0.29, p = .517]. This is not because all cases at this stage have it, indeed only 20% do. Instead, this likely reflects other, unmeasured, aspects of these cases. We also see that women are 14% less likely to have their cases tried in court [ME = −0.14, p = .002], and that assaults in public are 12% less likely to go to court [ME = −0.12, p = .010]. This may reflect that the survivor is less likely to know the perpetrator. Taken together, this suggests that assaults on young women in public places are much less likely to come to court, whereas SV against boys is much more likely to do so.
So far, we have established which factors predict a survivor’s case moving to the next stage of the pathway. But, given that only a small percentage of cases make it to court, and only 1% of our sample leads to a conviction it is useful to analyze which stages lead to case attrition. Such an analysis can not only help us understand better the reality of SV and DV in Kenya, but also potentially inform policy. Buis (Citation2017) shows that if we are willing to assign numerical values to each node of the tree above then we can define the expected outcome for survivor ,
, as:
Where here we treat each step symmetrically such that . That is, we are not choosing to weight some steps of the pathway as being more important than others.Footnote2
I.E.,
Then the impact of each explanatory variable on the overall outcome is given by the product of the estimated regression coefficient for that variable at each stage, with a weight
Where the weight is the product of the (predicted) proportion of survivors whose case will reaches that node, the discrimination of the node, and the difference in expected outcome of those who pass and those who do not. Thus, a given stage of the process will have a higher weight if it affects more survivors; the outcome is more varied (a stage at which almost every case continues or every case ends will do little to predict the overall outcome); and the difference in outcome between those cases that pass that stage and those that do not is larger (e.g., a stage matters less if almost every case that passes it fails at the next stage, and matters more if almost every case that passes it then is likely to lead to conviction, say). (See Eq 3. of Buis (Citation2017) for a formal statement.)
displays the estimated weights for each stage of the medical-legal pathway, and their determinants. The results suggest that the stage with the greatest weight is the decision to go to the police, which has weight 0.357 reflecting that this stage is reached by a large share of cases, but that only around ⅕ go on to be prosecuted, and that the expected outcome of those that do go to the police is relatively large at 1.8 stages further on average. This interpretation of this finding depends on why more cases do not go to the police.
If cases are not taken to the police due to a lack of resources, such as lack of trained SGBV professionals and/or inadequate evidence collection resources, then this suggests that addressing this resource issue could lead to a large increase in the number of cases prosecuted. On the other hand, if it is the case that survivors decide about whether to report their assault to the police based on knowledge (perhaps supplied by WKF) as to whether the case will be likely to be prosecuted, then this would suggest that the necessary policy response is to change police or prosecutor behavior. Or indeed, if prosecutor behavior reflects their knowledge of likely court outcomes, then activity should be focused there.
That the decision to prosecute has a weight of 0.2 and the decision to receive medical attention has a weight of 0.18 suggests that the importance of the decision to go to the police does not just reflect what may happen subsequently, and likewise the decision to receive medical attention does not just anticipate the police’s behavior. This implies that efforts to address bias cannot focus on just one stage. That the court stage is less important reflects not that it is unimportant per se, but rather the fact that almost no cases successfully lead to a conviction.
The subtlety of this point can be understood by analyzing further the weight of the medical attention node. Its weight reflects a balance between the fact that it discriminates few cases – over 90% of people receive medical attention – on one hand, and the fact that on the other if they do, then they on average will go 2.27 stages further in the process.
So far, we have combined and analyzed SV and DV cases together to maximize the statistical power of the available sample. However, there may be important differences in the determinants of case progression between the two crimes. To understand these differences, we analyzed the data separately and present the results for each in turn.
Sexual violence only
, report results now restricting our sample only to SV cases. Looking first at the results in the top left panel for whether survivors received medical attention, we see that none of the estimated coefficients are statistically significant, and all are close to zero. This likely reflects the fact that 95% of all SV survivors received medical attention, meaning there is relatively little variation to explain.
Looking now at the results for whether the survivor filed a police report in the top right panel, the estimates are still relatively noisy; but the coefficients are nevertheless informative. We see that an attack that happened in a public place is 15% [ME = −0.15 p = .034] less likely to lead to a police report. One explanation for this is that given the police have little forensic and investigative resources, survivors are less likely to file a report about an assault by a stranger given the low chance of a perpetrator being identified. The coefficients on child survivor and forensic evidence are not significant; but the estimated coefficients are relatively large at 19% and 13%, respectively, and suggestive of an increased probability of filing police reports in such cases [ME = 0.19, p = .11 and ME = 0.13, p = .145, respectively].
Interestingly, the results are quite different for whether prosecutors take up a case as shown in the bottom left panel. Unlike the decision to report an attack to the police, whether the assault happened in public is not important. But child survivor and forensic evidence are associated with large, 42% and 20% respectively, and precisely estimated coefficients [ME = 0.42, p < .001; ME = 0.20, p = .020]. Victim age is now, like the pooled sample, significant, and suggests that a survivor who was five years older is 9.23% more likely to have their case taken by the prosecutor [ME = 0.018 p = .022].
The pattern of coefficients changes again for whether a case comes to court in the bottom right panel. Cases that involve SV in a public place are 27% less likely to come to court. While cases in which the survivor is female are 17% less likely to do so. Cases in which the survivor was a child are 37% more likely to come to court. These results suggest that the cases which
reach trial are far from a representative sample and are much more likely to involve (male) children.
Domestic violence only
We now consider the results focusing on DV cases, which are reported in (and ). As for SV cases, the results are again somewhat noisy; but the results in the top left panel suggest that child survivors are about 21% more likely to receive medical attention. [ME = 0.21, p = .068] The results for whether a report is filed with the police (top right panel) are interesting, as they show that attacks in public are 20% more likely to lead to a police report than those in private [ME = 0.21, p = .047]. Older survivors are also more likely to file a police report, with a five-year age increase associated with a 7.4% increase in the probability of filing a report [ME = 0.015, p = .003]. Again, as shown in the bottom left panel, age and whether the survivor is a child predict whether the prosecutor takes forward the case [ME = 0.013, p < .001 and ME = 0.19, p = .066, respectively]. Gender and location are not found to be important. The same is true for whether a case comes to trial shown in the bottom right panel, although in common with the results above, the evidence is suggestive that female survivors are 8% less likely to see their case come to court, given a prosecutor has taken it up [ME = −0.076, p = .065].
Discussion
Our results show that there are numerous correlates of case progression through the medical-legal pathway in Kenya. These correlates differ based on the step in the pathway and the type of violence being examined, though there are correlates that are significant for multiple steps, no matter which type of violence is being studied.
Age, or whether the survivor was an adult or child, was a significant correlate for both SV and DV, and it was the strongest predictor for all steps of the pathway. Across all types of violence, age was found to be significant for receiving medical attention, reporting to the police, a prosecutor taking up the case, and the case proceeding to court when the types of violence are combined. For DV, age was associated with whether prosecutors took up the case and whether the case proceeded to court. For SV cases, age was associated with whether the survivor received medical attention, whether a prosecutor took up the case, and whether the case proceeded to court. The role of age in the survivor’s ability to access services and other support might be explained by differences in societal views of violence in relation to age. Children may be less likely to experience the same amount of stigma faced by adult survivors when reporting SV. Further, patriarchal views that serve to normalize abuse against a spouse or partner may be less likely to extend to children. Concerns about repercussions from the abuser may prevent some people from reporting violence against either themselves or their children; however, once a case against a child is brought into the system, it is far more likely to reach each step than a case against an adult.
When evaluating correlates for both types of violence combined in one model, SV was significant for the survivor receiving medical attention, reporting to the police, having their case taken up by the prosecutor, and having their case proceed to court. This means that for both types of violence combined, SV and the survivor being a child are significant correlates for all four steps along the case referral pathway. Additionally, older survivors are more likely to report their cases to the police and for their cases to proceed to court, while the presence of forensic evidence makes cases more likely to be prosecuted. Some possible explanations for this are that DV was most frequently perpetrated in our dataset against adults by a spouse or partner (80%), whereas SV against adults in our data set was most often perpetrated by strangers (43%) followed by acquaintances or friends (16%). Therefore, a survivor of SV would be more willing to report their case than a survivor of DV for the aforementioned reasons; namely, reporting a spouse might have dire financial consequences for one’s family. Older survivors may be more willing to report their cases to the police and for their cases to proceed to court because they have more community support and may be less financially reliant on others.
When evaluating SV separately from DV, our analysis was able to identify some correlates to case progression. There were no significant correlates of whether a survivor received medical attention, likely because the great majority of SV survivors did so. Public SV attacks are less likely to lead to a police report, perhaps because these were often perpetrated by someone unknown to the survivor, and hence, who could not be identified by the police. The survivor being a child and the presence of forensic evidence were correlated with an increased likelihood of the case being taken up by prosecutors, and for SV cases progressing to court, with the survivor being a child making the case 37% more likely to progress to this stage. This may reflect an idea in Kenya that defilement is a serious crime that deserves punishment, whereas rape is not, in line with the previously discussed ideas concerning the social acceptability of crime against a child. Additionally, without evidence, cases are unlikely to move through the case referral pathway, indicating that the victim’s testimony alone is not considered substantial evidence when pursuing a case (Rockowitz, Citationforthcoming).
In evaluating solely DV cases, the findings differed slightly from SV cases. Child survivors were once again more likely to receive medical attention than their adult counterparts. Public attacks and those involving older adult victims were more likely to lead to a police report, and older adults and children were more likely to have their cases taken up by prosecutors and for their case to proceed to trial. One possible explanation for this is that most DV cases are perpetrated by someone known to the victim, and this, might support the charges. Further, cases occurring in public may also be more likely to have bystanders to corroborate the survivors’ account, and research has found that cases where witnesses are present are more likely to progress through to prosecution (Bechtel et al., Citation2012). Further research is needed to assess this possibility. DV cases may have more witnesses than SV cases, as SV cases often occur in more private locations. DV cases also have less evidence, as SV may leave bodily fluids and ripped clothes that DV would not. Because evidence is a strong correlate of case progression, in the combined model SV is still a significant correlate for each step of the case referral pathway.
The law in Kenya is supposed to apply to all citizens of DV and SV equally, regardless of their age, their gender, or where the violence occurred (National Council for Law Reporting, 2009). Our data reveals, however, that SV and DV survivors who are children are far more likely to make it to every stage of the medical-legal pathway than adults, that SV survivors are more likely than DV survivors to make to every stage of the pathway, and that being an older adult also helps cases move through the medical-legal pathway. It is also important to note that while certain factors increase one’s likelihood of moving through the pathway all the way to court, which is the final step, still only 15% of the cases studied made it to court and only 1% resulted in a conviction. This means that while certain factors may help cases move further along the pathway, conviction is still extremely unlikely. This may be due to cases falling out of the system either due to the wishes of the survivor to end what is often a multi-year process where the survivor is burdened by administrative issues, or where the survivor is subject to bribery by the perpetrator or his family, or simply because judges and juries in Kenya often side with the perpetrator rather than the complainant.
The factors identified in this study that result in case attrition are also likely associated with ideologies embedded in rape myths and patriarchal cultures that are pervasive throughout Kenya. Rape myths are beliefs about rape’s “causes, context, consequences, perpetrators, victims, and their interaction” that are used to reject, lessen the significance of, or justify SV that men commit against women and shift the blame onto the victim rather than the perpetrator (Temkin et al., Citation2016; Zinzow et al., Citation2022). Rape myths are beliefs that operate outside conscious awareness that hold victims accountable for rape rather than perpetrators. Rape myths are often tied to victim blaming, which contributes to poor handling of rape cases, post-traumatic stress in rape survivors and can impede their recovery (Suarez & Gadalla, Citation2010). Rape myths also play a significant role in how SV cases are treated as they move through the medico-legal pathway, with providers often subconsciously adjusting their treatment of a victim based on foregone conclusions related to clothing, alcohol consumption, or previous behavior (Temkin et al., Citation2016). Future research should work with prosecutors to train them to identify rape myths in the courtroom and gender defenders to assess the impact of rape myths on a victim’s willingness to come forward.
Although rape myths are often studied in high-income contexts, they are pervasive around the world. In Western Kenya, research has found that five of the seven standard rape myth categories emerged in focus group discussions without prompting. These categories included that rape is a deviant event, that it was an accident because men are not able to control their sexual urges, and that the women were lying about being raped (Tavrow et al., Citation2013). With these in mind, it is perhaps clearer why there is such a focus on the presence of evidence for a case to be believable. If the standard opinion is that a woman is lying, the presence of evidence helps prove otherwise. For DV, beliefs about the husband’s alleged manliness or control may influence their violence perpetration, with men with lower self-esteem being more likely to be violent towards their spouse than men with higher self-esteem (Goodman, Citation2018). Knowing how important these ideologies are to the perpetration of violence, investigation of SV and DV cases should also include interviews with the perpetrators about these ideas, perhaps providing information that evidence (or the lack thereof) may not.
The results of this study can help to inform policy makers who are evaluating ways to strengthen the medico-legal case referral pathway in Kenya. We had a select dataset to work with of survivors who had interacted with the WKF, limiting the representativeness of our sample. Survivors who had assistance from the WKF are more likely to succeed than survivors navigating the system on their own, so our results are probably more positive than they would have been from a more general sample. However, due to our limited data it is unclear how survivors being helped by a similar organization would fare in their progression through the case referral pathway. Similar work should be conducted on a larger, more diverse sample to evaluate how these factors may affect survivors moving through the system without external assistance. Future research should also investigate how these findings apply to assaults of those beyond the gender binary, and how the factors included in the analysis may have affected a survivor’s willingness to accept a bribe to stop pursuing the case based on their perceptions of which case details are most beneficial to their case moving through the entire pathway.
Conclusion
With the known physical, mental, and social consequences of SV and DV, organizations such as the Wangu Kanja Foundation, in Kenya and beyond, provide important support through connecting their clients to medical and legal services. Despite efforts by the WKF, still very few survivors make it through the case referral pathway, and more needs to be done by the Kenyan government to ensure that all survivors are given equitable access to services and justice. It is also clear from the results that children are far more likely to make it to every step of the pathway than adults, and that for both adults and children, certain factors, such as SV versus DV and the presence of forensic evidence, increase the odds of moving along the case referral pathway. Survivors of sexual and physical violence should have equal access to medical, legal, and justice services regardless of their age, or the location of the attack. Work must be done in Kenya, as elsewhere, to strengthen the case referral pathway so that survivors of SV and DV are awarded equal access to services. This can be done in two key ways: firstly, by eliminating blockages on the case referral pathway so that more cases progress to court and conviction. Secondly, by improving equality of progression rates along the case referral pathway so that all survivors of SV and DV are afforded equal access to services.
Acknowledgments
We would like to thank the sexual and domestic violence survivors whose data is used for this project for sharing their stories and the Survivors of Sexual Violence in Kenya Network for facilitating data collection.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1. We tested for multicollinearity using a Variance Inflation Test. The maximum score was 3.21, with a mean of 1.78, comfortably below the conventional benchmark of 10.
2. If one had evidence on how survivors valued the different steps of the pathway then this assumption could – in principle – be relaxed, but we are aware of no such evidence.
References
- Anastario, M. P., Adhiambo Onyango, M., Nyanyuki, J., Naimer, K., Muthoga, R., Sirkin, S., Barrick, K., van Hasselt, M., Aruasa, W., Kibet, C., & Omollo, G. (2014). Time series analysis of sexual assault case characteristics and the 2007-2008 period of post-election violence in Kenya. PLoS ONE, 9(8), e106443. https://doi.org/10.1371/journal.pone.0106443
- Artz, L., & Smythe, D. (2007). Case attrition in rape cases: A comparative analysis. South African Journal of Criminal Justice, 20, 158–181. https://journals.co.za/doi/epdf/10.10520/EJC52915
- Bechtel, K. A., Alarid, L. F., Holsinger, A., & Holsinger, K. (2012, April 1). Predictors of domestic violence prosecution in a state court. Victims & Offenders, 7(2), 143–160. https://doi.org/10.1080/15564886.2012.657289
- Beichner, D., & Spohn, C. (2005). Prosecutorial charging decisions in sexual assault cases: Examining the impact of a specialized prosecution unit. Criminal Justice Policy Review, 16(4), 461–498. https://doi.org/10.1177/0887403405277195
- Buis, M. L. (2017). Not all transitions are equal: The relationship between effects on passing steps in a sequential process and effects on the final outcome. Sociological Methods & Research, 46(3), 649–680. https://doi.org/10.1177/0049124115591014
- Fullerton, A. S. (2009). A conceptual framework for ordered logistic regression models. Sociological Methods & Research, 38(2), 306–347. https://doi.org/10.1177/0049124109346162
- Garcia-Moreno, C., Jansen, H. A. F. M., Ellsberg, M., Heise, L., & Watts, C. (2005). WHO multi-country study on women’s health and domestic violence against women: Initial results on prevalence, health outcomes, and women’s responses. W. Press. https://apps.who.int/iris/handle/10665/43309
- Goodman, M. (2018). Domestic violence and social status: A Kenyan case study. The Conversation Trust UK Limited. https://theconversation.com/domestic-violence-and-social-status-a-kenyan-case-study-105746
- Gregory, J., & Lees, S. (1996). Attrition in rape and sexual assault cases. The British Journal of Criminology, 36(1), 1–17. https://doi.org/10.1093/oxfordjournals.bjc.a014060
- Hester, M., & Lilley, S.-J. (2017, June 1). Rape investigation and attrition in acquaintance, domestic violence and historical rape cases. Journal of Investigative Psychology and Offender Profiling, 14 (2), 175–188. https://doi.org/10.1002/jip.1469
- Hohl, K., & Stanko, E. A. (2015). Complaints of rape and the criminal justice system: Fresh evidence on the attrition problem in England and Wales. European Journal of Criminology, 12(3), 324–341. https://doi.org/10.1177/1477370815571949
- Ji, Z., Rockowitz, S., Flowe, H. D., Stevens, L. M., Kanja, W., & Davies, K. (2022). Reflections on increasing the value of data on sexual violence incidents against children to better prevent and respond to sexual offending in Kenya. Societies, 12(3), 89. https://doi.org/10.3390/soc12030089
- Kerstetter, W. A. (1990). Gateway to justice: Police and prosecutorial response to sexual assaults against women. The Journal of Criminal Law and Criminology, 81(2), 267. https://doi.org/10.2307/1143908
- Kilonzo, N., Ndung’u, N., Nthamburi, N., Ajema, C., Taegtmeyer, M., Theobald, S., & Tolhurst, R. (2009, January 1). Sexual violence legislation in sub-Saharan Africa: The need for strengthened medico-legal linkages. Reproductive Health Matters, 17 (34), 10–19. https://doi.org/10.1016/S0968-8080(09)34485-7
- Kilonzo, N., Theobald, S. J., Nyamato, E., Ajema, C., Muchela, H., Kibaru, J., Rogena, E., & Taegtmeyer, M. (2009, July). Delivering post-rape care services: Kenya’s experience in developing integrated services. Bulletin of the World Health Organization, 87(7), 555–559. https://doi.org/10.2471/blt.08.052340
- LaFree, G. (1989). Rape and criminal justice: The social construction of sexual assault.
- Lea, S. J., Callaghan, L., Grafton, I., Falcone, M. A., & Shaw, S. (2016). Attrition and rape case characteristics: A profile and comparison of female sex workers and non-sex workers. Journal of Interpersonal Violence, 31(12), 2175–2195. https://doi.org/10.1177/0886260515573575
- Lea, S. J., Lanvers, U., & Shaw, S. (2003). Attrition in rape cases. Developing a profile and identifying relevant factors. The British Journal of Criminology, 43(3), 583–599. https://doi.org/10.1093/bjc/43.3.583
- Lekakeny, R. (2015). The elusive justice for women: A critical analysis of rape law and practice in Kenya. University of Cape Town.
- Leverick, F. (2020). What do we know about rape myths and juror decision making? The International Journal of Evidence & Proof, 24(3), 255–279. https://doi.org/10.1177/1365712720923157
- Lovell, R., Overman, L., Huang, D., & Flannery, D. J. (2021, June 1). The bureaucratic burden of identifying your rapist and remaining “cooperative”: What the sexual assault kit initiative tells us about sexual assault case attrition and outcomes. AMerican Journal of Criminal Justice, 46(3), 528–553. https://doi.org/10.1007/s12103-020-09573-x
- Machisa, M., Jina, R., Labuschagne, G., Vetten, L., Loots, L., & Jewkes, R. (2022). Factors associated with rape case attrition in the South African criminal justice system: A national cross-sectional study. The British Journal of Criminology. https://doi.org/10.1093/bjc/azac044
- Maddala, G. S. (1983). Limited-dependent and qualitative variables in econometrics. Cambridge University Press. https://doi.org/10.1017/CBO9780511810176
- Mare, R. D. (1980). Social background and school continuation decisions. Journal of the American Statistical Association, 75(370), 295–305. https://doi.org/10.2307/2287448
- Ministry of Health Kenya, Kenya National Bureau of Statistics, National Aids Control Council, Kenya Medical Research Institute, & National Council for Population Development. (2015). Kenya demographic and health survey, 2014.
- Murphy, S. B., Edwards, K. M., Bennett, S., Bibeau, S. J., & Sichelstiel, J. (2014). Police reporting practices for sexual assault cases in which “the victim does not wish to pursue charges.” Journal of Interpersonal Violence, 29(1), 144–156. https://doi.org/10.1177/0886260513504648
- Murphy-Oikonen, J., Chambers, L., Miller, A., & McQueen, K. (2022). Sexual assault case attrition: The voices of survivors. SAGE Open, 12(4), 215824402211446. https://doi.org/10.1177/21582440221144612
- Mwangi, G. K., Jaldesa, G. W., & Sheikh, M. (2009). An assessment of sexual and gender based violence in Wajir district, North Eastern Kenya.
- Office for National Statistics. (2022). Domestic abuse in England and Wales overview.
- Pattavina, A., Morabito, M. S., & Williams, L. M. (2021). Pathways to sexual assault case attrition: Culture, context, and case clearance. Victims & Offenders, 16(8), 1061–1076. https://doi.org/10.1080/15564886.2021.1970661
- Rockowitz, S. (Forthcoming). University of Birmingham.
- The Sexual Offences Act. (2006).
- Shadle, B. (2010). Sexual offences in Kenya courts 1960s-2008.
- Smith, O., & Skinner, T. (2017). How rape myths are used and challenged in rape and sexual assault trials. Social & Legal Studies, 26(4), 441–466. https://doi.org/10.1177/0964663916680130
- Spohn, C., & Holleran, D. (2001). Prosecuting sexual assault: A comparison of charging decisions in sexual assault cases involving strangers, acquaintances, and intimate partners. Justice Quarterly, 18(3), 651–688. https://doi.org/10.1080/07418820100095051
- Spohn, C., & Horney, J. (1993). Rape law reform and the effect of victim characteristics on case processing. Journal of Quantitative Criminology, 9(4), 383–409. https://doi.org/10.1007/BF01064110
- Spohn, C., & Tellis, K. (2012, February 1). The criminal justice system’s response to sexual violence. Violence Against Women, 18(2), 169–192. https://doi.org/10.1177/1077801212440020
- Suarez, E., & Gadalla, T. M. (2010, November). Stop blaming the victim: A meta-analysis on rape myths. Journal of Interpersonal Violence, 25 (11), 2010–2035. https://doi.org/10.1177/0886260509354503
- Tavrow, P., Withers, M., Obbuyi, A., Omollo, V., & Wu, E. (2013, July). Rape myth attitudes in rural Kenya: Toward the development of a culturally relevant attitude scale and “blame index.” Journal of Interpersonal Violence, 28 (10), 2156–2178. https://doi.org/10.1177/0886260512471086
- Temkin, J., Gray, J. M., & Barrett, J. (2016). Different functions of rape myth use in court: Findings from a trial observation study. Feminist Criminology, 13(2), 205–226. https://doi.org/10.1177/1557085116661627
- Temmerman, M., Emilomo, O., Griffins, M., Iqbal, K., Mary, T., Kishor, N. M., Lou, D., Markus, M., & Peter, G. (2018). The gender-based violence and recovery centre at coast provincial general hospital, Mombasa, Kenya: An integrated care model for survivors of sexual violence. PLoS Medicine, 16(8), e1002886. https://doi.org/10.1371/journal.pmed.1002886
- Thelan, A. R., & Meadows, E. A. (2022). The Illinois rape myth acceptance scale—subtle version: Using an adapted measure to understand the declining rates of rape myth acceptance. Journal of Interpersonal Violence, 37(19–20), NP17807–NP17833. https://doi.org/10.1177/08862605211030013
- Truman, J. L., & Morgan, R. E., & United States. Bureau of Justice Statistics. (2014). Nonfatal domestic violence, 2003-2012 [ text]. U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics.
- UNICEF, Division of Violence Prevention, National Center for Injury Prevention and Control, US Centers for Disease Control and Prevention, & Kenya National Bureau of Statistics. (2012). Violence against children in Kenya: Findings from a 2010 national survey. Summary report on the prevalence of sexual, physical, and emotional violence, context of sexual violence, and health and behavioral consequences of violence experienced in childhood.
- UN Women. (2016). Prevalence data on different forms of violence against women. https://evaw-global-database.unwomen.org/en/countries/africa/kenya
- Wangamati, C. K., Sundby, J., Izgubara, C., Nyambedha, E. O., & Prince, R. J. (2019). Challenges in supporting survivors of child sexual abuse in Kenya: A qualitative study of government and non-governmental organizations [article]. Journal of Interpersonal Violence. https://doi.org/10.1177/0886260519846864
- Wangu Kanja Foundation. (2016). Survivors network. Retrieved December 12, from https://wangukanjafoundation.org/?page_id=1005
- Withers, M., Minkin, E., & Kyle, A. (2019). Rape myth acceptance leads to victim-blaming. Psychology Today. Retrieved November 20.
- Wooldridge, J. M. (2010). Econometric analysis of cross section and panel data. The MIT Press. http://www.jstor.org/stable/j.ctt5hhcfr
- Zinzow, H. M., Littleton, H., Muscari, E., & Sall, K. (2022, August 18). Barriers to formal help-seeking following sexual violence: Review from within an ecological systems framework. Victims & Offenders, 17(6), 893–918. https://doi.org/10.1080/15564886.2021.1978023
Appendix
Table A1. Logit regression of whole sample.
Table A2. Sequential logit estimates of sexual violence only.
Table A3. Sequential logit estimates of domestic violence only.
Table A4. Cases at risk of passing each transition for sexual violence only.
Table A5. Cases at risk of passing each transition for domestic violence only.