
Abstract
Many jurisdictions around the world have implemented Responsible Gambling (RG) programs for the purpose of preventing gambling-related harms. Using a research synthesis strategy, this paper examines the extant peer-reviewed empirical evidence underpinning RG strategies. Instead of reporting all available studies and then discarding many on the ground of methodological flaws, we used the following a priori set of inclusion criteria: (1) All studies must have been conducted within real gambling environments with ‘real’ gamblers; and studies must have included at least one of the following elements: (2) a matched control or comparison group; (3) repeated measures; and (4) one or more measurement scales. The results revealed that only 29 articles met at least one of the methodological criteria. These empirical studies revealed five primary RG strategies. These findings have practical implications for evidence-based implementation of RG activities.
Governments and industry operators have implemented responsible gambling (RG) initiatives and programs to prevent or minimize gambling-related harms. These RG initiatives and programs are designed to reduce the prevalence and incidence of gambling-related harms by assisting gamblers to maintain their gambling expenditure within affordable limits. Existing RG programs include, but are not limited to, a variety of strategies: self-exclusion programs; behavioral tracking of play patterns; loss and deposit limit setting (both player and corporate); player pre-commitment to deposits, losses, wins, or gambling time; warning messages; restricted game design; gambling education and information; and support services reflecting primary, secondary and tertiary prevention efforts. Unfortunately, the scientific evidence supporting many of these programs and initiatives is absent or weak.
The Reno Model (Blaszczynski et al. Citation2004) proposed the first strategic framework describing the fundamental principles necessary to guide the development of RG strategies as well as the responsibilities of industry operators, health service and other welfare providers, interested community groups, consumers, and governments and their related agencies. The Reno Model framework lays out a guide to the process of RG program adoption, implementation, and evaluation of empirically supported initiatives and strategies.
Given the public policy and legislative demands (e.g. ‘Bill H03697,’ 2011) requiring the implementation of these activities, there is a need to determine the efficacy of RG strategies. Unfortunately, regardless of the limited empirical evidence supporting the effectiveness of these programs (Williams et al. Citation2012), many presumptively effective RG activities continue to be implemented (Blaszczynski et al. Citation2004). In addition, where existing evidence does exist, inadequate methods, study samples, and design flaws often compromise the value of this research. Given the potential public health impact of RG programs, it is vital to evaluate the extant body of scientific evidence – instead of opinion-based arguments – to identify the strategies and activities that can guide the development and implementation of effective RG programs. The need for identifying this body of evidence has never been more necessary. As gambling has expanded around the world, jurisdictions are requiring RG programs and activities – without knowing which activities are safe and effective. In Massachusetts, for example, pre-commitment (i.e. a RG strategy where players set limits on expenditure at commencement of a session) is required despite the fact that there is little empirical evidence to support this strategy. Further complicating this matter, little research has been conducted with actual gamblers and gambling; instead researchers often employ laboratory settings and simulated gambling with college students who are not representative of the community in general or gamblers in particular (Shaffer et al. Citation2010, Citation2011; Gainsbury et al. Citation2014).
RG activities often include an educational component. Williams et al. (Citation2012) conducted a literature review evaluating the effectiveness of various educational initiatives, policies, and purported ‘best practice’ interventions for preventing problem gambling. These authors concluded that the estimated effectiveness of educational initiatives (i.e. type of RG initiative) is moderate with research data showing that prevention programs for children are generally effective in reducing misconceptions and increasing knowledge about gambling. However, the absence of long-term follow-up and behavioral measures makes it difficult to draw any conclusive statements about the effectiveness of these programs (Blaszczynski et al. Citation2004). In general, various risk reduction strategies, for example, information and awareness campaigns, on-site information/counseling centers, and statistical instruction have moderately low effectiveness (e.g. Tobler Citation1986; Ennett et al. Citation1994; Johnson et al. Citation2003; Hertwig et al. Citation2004; Fortune & Goodie Citation2012). Alternatively, the efficacy of restricting availability and access to gambling as a method of reducing harm is moderately high. Although it appears that some gambling-related harm prevention programs are more effective than others, the most commonly adopted ones tend to be the least effective (Williams et al. Citation2012).
The purpose of this research is to identify empirically grounded RG studies in an effort to create the beginnings of a foundation that can guide evidenced based effective RG strategies. This paper, however, is not intended to provide a comparative critique of methodologies and design used in identified studies (e.g. sampling, study design, response rates, sample size, etc.; readers interested in research design should see, for example, Campbell & Fiske Citation1959; Campbell & Stanley Citation1963; Borkovec & Castonguay Citation1998). The intent is to distill the core findings that are supported by evidence.
Although we reviewed the literature published prior to and after Williams et al.’s review, the current review differs from prior literature reviews in several important respects. Instead of examining all studies relevant to RG regardless of their methodological adequacy, the present review used a parsimonious and replicable a priori set of inclusion criteria designed to maximize the external validity of findings reported in different studies. By using a priori inclusion and exclusion criteria that focused the research sample on studies with a foundation of scientifically derived empirical evidence, we avoided the prospect of reporting about studies ultimately discarded on the grounds of methodological flaws, design limitations, and poor external validity. The inclusion criteria we selected for this evaluation represent standard methodological attributes that are related to acceptable research design and methods (e.g. Campbell & Stanley Citation1963; Rosenthal & Rosnow Citation1991; Cooper & Hedges Citation1994; Mosteller & Colditz Citation1996; Bangert-Drowns et al. Citation1997; Podsakoff et al. Citation2003; Shaffer et al. Citation2006). It is important to consider that these criteria represent minimal features of scientifically sound research methods; if we created a more demanding and rigorous inclusion criteria, the obtained study sample would be reduced in size. Although this approach is innovative in the field of gambling studies (Shaffer & Hall Citation1996; Shaffer et al. Citation1999), and unprecedented in the field of RG studies, using meta-analytic methods to take stock of a field is commonplace among other more mature scientific fields (Hunt Citation1997Citation2012).
Method
Search strategy
We employed two approaches to retrieve RG relevant articles. First, we conducted a systematic search of the primary academic databases PsychInfo, PubMed, Taylor and Francis Online, and ProQuest (all 44 data bases within ProQuest were included) for peer-reviewed publications using the following keywords: ‘responsible gambling’, ‘limit-setting’, ‘pre-commitment’, ‘warning messages’, ‘pop-up messages’, ‘game features’, ‘behavioral tracking’, ‘behavioral markers’, ‘behavioral indicators’, ‘self-exclusion’, ‘venue staff’, and ‘venue employees’. The term ‘responsible gambling’ was searched for independently as well as jointly with all the other terms. Second, to supplement this search, we targeted gambling-related journals directly to ensure that we captured all relevant articles not located in the selected databases. Individual journal searches were conducted for International Gambling Studies, Journal of Gambling Studies, and International Journal of Mental Health and Addiction, the main journals in the field. This search strategy targeted the period from 1962 to 31 October 2015. This approach identified 2548 publications.
Excluding the grey literature
From the 2548 identified articles, we excluded those not appearing in peer review journals. The extent to which articles appearing in the ‘grey’ literature could be validly claimed to have been independently peer-reviewed was not possible. Therefore, in the absence of peer review, the basic foundation for scientific publications, we excluded all ‘grey literature’. This decision does not in any way imply that such articles have no scientific merit; our concern was about the question of the scientific robustness and reliability of ‘grey’ literature – which is why the moniker of ‘grey’ is applied to this segment of the scientific literature.
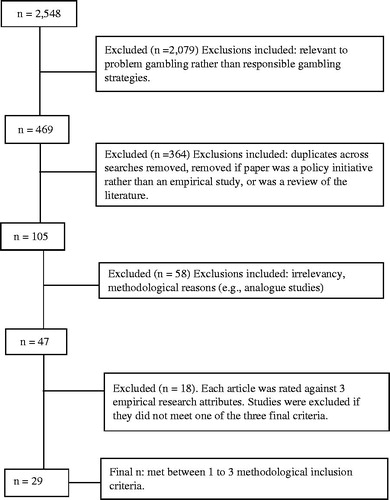
We excluded 2496 publications that were either in the ‘grey’ literature domain, duplicates, not relevant to RG, and those containing insufficient methodological information. summarizes the flowchart for exclusions at each step in the review process.
Figure 1. Flowchart illustrating the inclusion and exclusion of the studies reviewed at each step in the review.
Inclusion and exclusion criteria
In the next step of the review process, we retained studies if they met two criteria: (1) a specific focus on RG related topics and (2) evidence of an empirical approach toward evaluating RG strategies, initiatives, programs or theoretical content. There were 105 publications that were retained for further analysis.
Of those remaining studies, research conducted within real gambling environments with ‘real’ gamblers was retained. We excluded laboratory-based studies and simulations, and those using analog participants (e.g. university students) because these samples failed to represent actual gamblers and gambling. As a final step, we applied further methodological inclusion criteria; that is, did the investigators use at least one the following three methodologies: (1) matched control or comparison group; (2) repeated measures; and (3) one or more measurement scales (e.g. screening or diagnostic measures). Each of these criteria is fundamental to the conduct and scientific evaluation of RG programs. In the absence of these criteria, the ability to draw valid conclusions remains greatly limited. Of the 47 RG articles that remained, 29 articles (62%) met at least one of the three above methodological criteria.
Inter-rater reliability
Using the 47 articles that were relevant to RG interests, we conducted an inter-rater reliability test to examine the potential for rating biases during the coding and evaluation process. For this procedure, two colleagues (i.e. public health data analysts) independently rated a randomly selected subset of the 47 publications (n = 15; 32%) using a mutually exclusive 19-item scale. After each coder independently rated the same 15 publications, we calculated a Cohen’s Kappa (2012). Cohen’s Kappa represents the agreement between two raters classifying the items into the mutually exclusive categories. The 19 categories included: study design, year of publication, length of study, sample size, location, repeated measures, prospective design, real gamblers rather than simulation, setting of study, whether participants gambled with their own money, perception of control over gambling activities, gambling for money, gambling involvement (i.e. multiple games), measurement of negative consequences (i.e. severe emotional distress, functional impairment), measurement of severity of impairment, use of screening/diagnostic instruments, and self-report. The K value is obtained from a non-parametric test that evaluates the consistency between different judges or examiners independently administering the same test to the same subject or object. Cohen’s Kappa is a statistic that accounts for agreement occurring by chance and specifically measures inter-rater agreement for categorical variables. It is generally thought to be a more robust measure than a simple percent agreement calculation.
Cohen’s Kappa revealed a strong aggregate level of agreement across raters for study attributes: notably, a mean kappa of 0.913 (SD = 0.138). The minimum Kappa found was .505 (i.e. type of study design), reflecting moderate agreement while the maximum Kappa was 1.00 (e.g. study time period) representing complete agreement.
Results
RG study sample characteristics
From the search, 47 articles qualified as relevant to the topic of RG; however, 18 of these failed to meet any of the three key methodology inclusion criteria. Of the 29 (62%) qualifying as empirical studies, 11 (37%) used a matched-control or comparison group, while 22 (73%) were repeated measures studies, and 21 (73%) used measurement scales to evaluate participants. Only six of the 29 articles (21%) satisfied all three key methodology inclusion criteria: two of these were case-controls, and four were case-controls at baseline with a prospective cohort that followed. These studies evidence sound methodological strategies and the most research rigor from the body of RG studies identified.
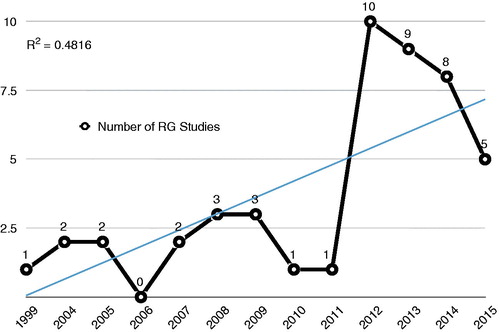
As Footnote1 shows, 32 of the 47 (i.e. 68%) RG articles were published after 2011, suggesting that research focusing on RG remains an increasingly popular (Kolmogorov–Smirnov; p<.001) but still nascent field of study. However, the rate of RG-related peer reviewed publications during this timeframe rapidly increased reaching a peak during 2012 and subsequently progressively declined.
Figure 2. Responsible Gambling peer-reviewed publications during 1999–2015. For 2015, data includes publications released during only part of October.
summarizes the results of our literature search. A content analysis reveals that these RG articles (N = 47) focused on the following five RG strategies: (1) identifying problem gamblers by using actual gambling behavioral characteristics or behavior patterns; (2) setting gambling limits; (3) self-exclusion programs; (4) venue staff responding to patron problem gambling; and (5) specific RG features.
Table 1. Inclusion criteria for study consideration.
Using our final sample of 29 empirical studies, a comparison with Williams et al. (Citation2012) revealed no difference in RG strategies (e.g. limit setting, self-exclusion, etc.; Chi Square = 2.02; df = 4; p>.73); however, there was a statistically significant difference between the research designs associated with the respective study samples (Chi Square = 9.83; df = 4; p<.05). This study included many more prospective and case control studies than did Williams et al. (Citation2012).
As shows, most RG research has focused on self-exclusion programs with the next commonly investigated areas being behavioral characteristics of actual gambling and RG game features, and limit setting. Limit setting and staff responses to gambling are the least studied. We will now review and discuss what is known about each of these five content areas based on the 29 studies meeting the methodological requirement as described above (see for the list of studies). We classified each study according to what was considered its primary area of RG focus.
Main findings and implications of five RG strategies
Despite using minimal methodological inclusion criteria, we were able to identify only 29 empirical studies focusing on RG. These studies represent only five RG strategies. Had we employed more rigorous inclusion criteria, our sample would have been even more limited. In the following section, we will identify and briefly describe these RG strategies. The main goal of this discussion is to (1) highlight the core elements of RG programs and initiatives that meet minimal scientific criteria, (2) describe their main findings, and more importantly (3) help different stakeholders to continue research that can determine the impact and effectiveness of these RG activities.
Self-exclusion programs
Self-exclusion programs offer gamblers the opportunity to voluntarily ban themselves from gambling venues. Individuals self-excluding from a particular venue authorize the staff to deny them access to the venue, remove them from premises if detected, and potentially to lay charges for trespass or impose some form of penalty. Ban lengths typically range from six months to five years or lifetime. As indicates, the literature search identified nine self-exclusion publications involving land-based or online gambling.
Xuan and Shaffer (Citation2009) examined behavioral patterns of actual Internet gamblers experiencing gambling-related problems and voluntarily closing accounts. This research showed that account closers experienced increasing monetary losses and stake per bet prior to the time of closure while evidencing a risk-averse shift in monetary involvement and chance preference that occurred concurrently during the last few days prior to voluntary closure of accounts.
Hing et al. (Citation2015b) studied outcome differences by comparing three gambling populations: self-excluders, self-excluders receiving counseling, and those receiving counseling only. The investigators found that outcomes did not differ for self-exclusion combined with counseling. Compared to non-excluders, more self-excluders abstained from their most problematic form of gambling and fewer had harmful consequences. Findings suggested that self-exclusion might have similar short-term outcomes in comparison to counseling alone.
Hayer and Meyer (Citation2010) conducted a cross-sectional analysis of self-excluders, with a subset of participants followed-up for 12 months. The authors reported an improvement in psychosocial functioning over time with changes evident four weeks after signing a self-exclusion agreement and maintained for one year.
Nelson et al. (Citation2010) studied the long-term effects of self-exclusion. They followed 113 self-excluders for a period of up to 10 years from their initial enrollment. Most self-excluders reported some positive outcomes. However, half the sample breached conditions after initial enrollment.
Ladouceur et al. (Citation2007) reported that self-exclusion had many positive outcomes. These authors observed changes between baseline and six-month follow-up on several variables, such as on urge to gamble, perceived control over gambling, and intensity of the negative consequences of gambling on daily activities, social life, work and mood. Also, both SOGS (Lesieur & Blume Citation1987) scores and DSM-IV scores were reduced. In light of these changes, it was concluded that the self-exclusion program had a beneficial impact. However, over time, participants seemed to perceive the self-exclusion program as less effective. In addition, at the six-month follow-up, more than half of the participants had returned to a casino or breached their self-exclusion contract.
Dragicevic et al. (Citation2015) compared demographic and behavioral characteristics of 347 on-line self-excluders to 871 non self-excluders from an Internet gambling data set. Statistically significant differences were not apparent for gender or time spent gambling. However, age differences between the two groups emerged: younger compared to older online players were more likely to self-exclude. Self-excluded gamblers experienced greater losses than non-excluders, supporting previous research that financial problems are one of the main reasons for participating in self-exclusion programs.
Tremblay et al. (Citation2008) designed a study to measure gamblers’ participation, satisfaction, and perceived usefulness and impacts. The findings indicated major improvements between the initial and final evaluation. There were noted improvements with regard to money spent, consequences of gambling, DSM-IV scores, and psychological distress.
Hing et al. (Citation2014) conducted an evaluation of Queensland’s self-exclusion program to examine use, motivations for take-up, barriers to use, experiences and perceptions of the program, and potential improvements. Investigators interviewed 103 self-identified problem gamblers of whom 53 had and 50 had not self-excluded. Motivations for joining a self-exclusion program included financial, relational, career, legal, and health-related concerns. Barriers to take-up were described as embarrassment, stigma of joining, and concerns about confidentiality and privacy, and inconvenience of having to register at each venue.
LaBrie et al. (Citation2007) examined 6599 people who joined a Missouri casino self-exclusion program. This study found that the annual number of self-exclusion enrollments increased during the first few years of the program, and then leveled off during the later years. During the time of this study, new casinos were introduced, which allowed for the examination of the immediate influence on proximity of new gambling opportunities on the self-excluding cohort. This study found that regional proximity had an effect on self-excluding rates. Specifically, self-exclusion was significantly correlated with regional vulnerability, exposure dose (i.e. distance of self-excluder from nearest casino), and with exposure potency (i.e. the number of casinos clustered). The results suggest a relationship between gambling proximity, gambling availability, and self-exclusion rates.
The effectiveness of self-exclusion is best determined by assessing for gambling abstinence, or at the least, a reduction in gambling after enrollment. Dragicevic et al. (Citation2015) conducted a process evaluation of a self-exclusion program examining the behavioral characteristics of on-line self-excluders but were unable to determine the effectiveness of these programs. Despite their inability to determine the effectiveness of the self-exclusion programs, the investigators observed statistically significant distinctions among the gambling behaviors of on-line players who self-exclude compared to those who do not; these differences could be used to develop a model for predicting the occurrence of self-exclusion.
Responsible gambling behavioral characteristics
Tracking gambling behavior provides the opportunity to develop behavior-based strategies for detecting and intervening with problem gamblers. Although tracking gambling behavior using on-line sites is relatively straightforward, tracking gambling behavior for land-based sites is more difficult. Eight empirical studies have focused on the development of behavior-based algorithms for predicting problem gambling.
Quilty et al. (Citation2014) assessed gambling frequency, expenditure, and duration of 228 community members and 275 psychiatric outpatients with the goal of developing a model that predicted gambling-related problems. Gambling involvement was assessed using the DSM-IV (American Psychiatric Association Citation1994) and Canadian Problem Gambling Index (CPGI: Ferris & Wynne Citation2001); 120 (24%) participants met criteria for lifetime pathological gambling. The results demonstrated that three gambling indicators predicted the presence or absence of problem gambling. However, cutoff points for determining problem gambling differed depending on the type of gambling activity assessed, suggesting that efforts for promoting RG should be tailored to each type of gambling offered by operators.
Delfabbro and Winefield (Citation1999) showed that larger wins disrupted participant gambling rates; in turn, this gave rise to larger post-reinforcement pauses. However, small rewards maintained response rates. These findings also showed that, compared with infrequent poker players, regular poker players held fixed views about the profitability of given machines and were less likely to vary their wagers.
In other studies, investigators examined the behavioral patterns of actual gamblers to identify characteristics they could use to develop prevention and early intervention programs for problem gamblers (Braverman & Shaffer Citation2012). These studies were the first to use cluster analyses to identify groups of gamblers at higher risk for reporting gambling related problems. The authors studied a proportion of the larger sample that closed their accounts during the two-year study period (about 50% of the sample). These results complement the findings of Xuan and Shaffer (Citation2009). They investigated the last segment of a prospective period of gambling, before gamblers closed their account because of gambling-related problems. Analyzing the first segment of a longitudinal sequence is more critical than later segments if the primary purpose of the research is to identify gamblers who might later develop problems.
Schellinck and Schrans (Citation2004a) studied behaviors and thoughts that people use to control the amount they gamble: development of budgets; avoiding locations that provide gambling; rewarding oneself for not gambling; and seeking help from others to gain control of their gambling. Two mediating variables, self-efficacy and situational temptation, were also assessed. Findings suggested a number of initiatives that might support gamblers in their efforts to moderate or eliminate their video lottery terminals (VLT) gambling.
Schellinck and Schrans (Citation2004b) conducted research to identify combinations of behavioral, physiological, and emotional responses to gambling, to help identify problem gamblers. Better identification of problem gamblers on site can help with intervention at a higher confidence.
The remaining studies relied on data reflecting account-based betting patterns from on-line sites. These studies focused on the examination of early behavioral characteristics of online gamblers who later triggered warnings as potential problem gamblers (Gray et al. Citation2012, Citation2015), and multi-game behavioral markers for early identification of potential problem gambling (Braverman et al. Citation2013).
To identify behavioral markers of problem gambling, Gray et al. (Citation2012) compared electronic gambling behavior records of bwin.party account holders who had triggered responsible gaming alert systems (n = 2066) with those who had not (n = 2066). Alerts were triggered if gamblers closed or re-opened their account, reported account problems, requested account limit changes above the maximum value, or requested customer service to impose access restrictions to online accounts. Findings revealed that non-monetary betting activity intensity (i.e. total bets placed, number of active betting days, and duration of activity), and monetary variables (i.e. total stake size and net losses) reliably discriminated gamblers triggering warnings from those who did not.
Braverman et al. (Citation2013) analyzed the data of 4056 bwin.party players to build a model focusing on betting activity, changes in betting patterns, gambling during specific times of the week, and use of promotional money for gambling. Of these online gamblers, 2042 had been identified previously as having entered a RG program because of various gambling patterns including account closure due to gambling problems, requesting a limit through customer service instead of on-line, requesting partial or full block of account, or being underage. Results revealed that players engaging in more than two types of gambling within their first month, and with high variability for wagers in casino gambling or live action sports betting were more likely to benefit from future RG program.
Setting gambling limits
Pre-commitment is a RG tool that applies to certain forms of gambling offered by both land-based and online gaming operators. The goal of this tool is to enable gamblers to pre-set monetary and time limits in a non-emotional state to assist them in spending only as much as they can afford to lose. Depending on the gaming venue or website, spending limits can include deposit, play, loss, win and bet limits. Time limits can be made for a session of play within daily, weekly, and monthly time frames. Five empirical studies have focused on setting gambling limits.
Auer and Griffiths (Citation2013) examined the betting patterns and voluntary limits setting of 5000 on-line gambling account holders. Their data were from the win2day gambling website and were comprised of lottery, casino, and poker players. All players who opened an account with win2day were required to set time and cash-in limits. Analyses were conducted to determine if gambling behavior was different in the 30 days after compared to the 30 days before limit setting. Setting voluntary limits significantly affected monetary spending for casino and lottery gaming players. Voluntary monetary limit setting was more effective than time limits in reducing gambling behavior.
Auer and Griffiths (Citation2014) also examined 100,000 online gamblers to measure theoretical loss as an indicator for gambling behavior. They found a correlation between the ‘bet size’ and the overall ‘theoretical loss’ across the eight game types. Although the correlation was statistically significant, the bet size alone explained only 72% of the variance associated with theoretical loss. Auer and Griffiths suggested that future studies measure their participants’ gambling intensity by incorporating the game-specific theoretical loss instead of using proxy measures such the bet size and/or the amount of money staked.
Broda et al. (Citation2008) studied limiting setting with a sample of Internet sports betting gamblers from bwin. This study indicates that current deposit limits affect only a very small minority of Internet sports bettors. The vast majority of Internet bettors seem to be able to regulate themselves and require little additional safeguards.
Hing et al. (Citation2015a) reported that the use of digital money contributed to higher rates of gambling and loss of control. Participants made greater use of self-limiting strategies than those available on gambling websites, such as deposit limits and self-exclusion. However, participants had variable success adhering to their own limits. Exceeding limits appeared a common experience among regular gamblers; nevertheless, problem gamblers were significantly more likely to exceed limits than lower-risk groups. Thus, the results support the tendency of regular gamblers to exceed self-imposed limits; this suggests that maintaining control over Internet gambling would benefit from operator-assisted mechanisms to enforce self-limits.
Nelson et al. (Citation2008) studied the self-limiting behavior of Internet gamblers. Specifically, they studied 18 months of betting transactions among gamblers who subscribed to an online betting site (N = 47,134), 567 of whom utilized the site’s self-limit feature. The results showed that self-limiting gamblers played a wider variety of games and placed more bets than others prior to self-limiting. After imposing limits, self-limiters reduced their activity, but did not reduce the amount they wagered per bet. Time spent gambling, not just money wagered, appears to be an important indicator of gambling problems.
Responsible gambling specific game features
RG game features refer to the structural characteristics of games that promote RG. Research in this area is limited; only four recent studies have been published. These focused on warning messages, and RG game features of electronic gaming machines.
Warning messages is a harm minimization strategy aimed at preventing or reducing gambling-related problems by assisting individuals to make informed choices about their gambling. Some studies have demonstrated the efficacy of warnings in facilitating RG. Gainsbury et al. (Citation2015) report on the effectiveness of warnings appearing either in the middle or on the periphery of electronic gaming machines (EGMs) screens in commercial gambling venues. Regular gamblers were surveyed to assess their recall of warning messages and the perceived impact of message placement. Messages appearing in the middle of screens were recalled to a greater extent, and respondents reported that these were more impactful and useful than messages on the periphery of screens.
Ladouceur and Sévigny (Citation2009) investigated the influence of three features of electronic gambling machines (i.e. clock, cash display, and pre-commitment on gambling time). Participants gambled with their own money within their natural environment. Using behavioral and self-reported measures, the study found that a majority of players reported the cash display as being a helpful feature for controlling gambling activities. However, participants did not report the clock or the pre-commitment on gambling time as being helpful. The authors concluded that the clock and pre-commitment on gambling time device might not be instrumental in promoting RG.
Munoz et al. (Citation2013) assessed the effectiveness of graphic versus text-only gambling warnings messages designed to promote RG using a survey technique. Message content focused on how excessive gambling disrupts family or personal finances. Graphic warnings enhanced the perceived severity of the size of loss, and the likelihood of being affected by the loss, regardless of message content. Short-term gambling behavioral intent was significantly decreased when graphic warnings were paired with family disruption content, and when text-only warnings contained financial disruption content.
Blaszczynski et al. (Citation2014) evaluated the effectiveness of five RG features for the Blue Gum gaming machine: responsible gaming messages, bank meters, alarm clocks, demo mode for playing without money, and a charity donation feature. The investigators collected data using structured interviews, questionnaires, and direct observation. Most participants were aware of at least one of the five RG features, however, only a small portion of them used any of these. The RG features did not influence gambling enjoyment with the exception of the RG messages affecting problem gamblers, with gamblers who used one feature were more likely to also use additional features.
Training of venue employees intervening with problem gamblers
Gambling venue employees have direct contact with patrons experiencing gambling-related problems. Problem gambling awareness training has expanded in many venues to increase venue staffs’ ability to recognize problem gambling. Only three empirical studies evaluated training of venue staff.
In an attempt to evaluate the casino employee RG training program, Play Responsibly, LaPlante et al. (Citation2012) surveyed 217 new employees before and after training. The baseline and follow-up assessments focused on employee characteristics, and gambling-related opinions and knowledge. After training, employees provided more knowledgeable responses. However, the training had a larger influence on increasing new knowledge than it did on correcting previous inaccurate beliefs held by venue staff.
Delfabbro et al. (Citation2012) assessed the reliability of venue staff perceptions of patrons’ problem gambling. Patrons (N = 303) completed a survey of gambling habits, EGM play, and the Problem Gambling Severity Index (Ferris & Wynne Citation2001). Of these participants, 230 were familiar to the venue staff and therefore included in the analyses that compared ratings between patrons’ self-reported behavior and observations from the venue staff. There was considerable disparity between staff and patron ratings of problem gambling. According to the Problem Gambling Severity Index, 22 of the patrons were classified as problem gamblers; however, only one was classified as having some problems by venue staff. Additionally, venue staff identified 15 patrons as problem gamblers when the Problem Gambling Severity Index scores indicated no risk or low risk for these players.
To explore the challenges that venue staff experience when responding to patrons with gambling problems, Hing and Nuske (Citation2012) conducted interviews with venue staff. When approached by patrons seeking information or assistance for a gambling problem, staff reported feeling awkward about discussing personal issues, in part, because of the patrons’ own embarrassment. Staff experienced difficulties approaching patrons because of the uncertainty of the patron having a gambling problem. Being approached by a third-party raised issues of privacy and interfering with personal relationships. Venue staff, in responding to problem gamblers, reported experiencing confusion, dilemmas, and apprehension.
Discussion
This study represents the first empirical investigation focusing on the impact and efficacy RG strategies. By using a systematic approach to identifying research studies, this project establishes a methodological foundation upon which other investigators can build. Establishing evidence-based RG practices is important because, ‘Unfortunately, the development, implementation, and evaluation of most of these initiatives have been a haphazard process. Most have been put in place because they “seemed like good ideas” and/or were being used in other jurisdictions, rather than having demonstrated scientific efficacy or being derived from a good understanding of effective practices in prevention (Williams et al. Citation2012, p. 6). The field remains without a systematic approach for evaluating the body of evidence related to RG. Consequently, this study provides an important contribution to the field of RG studies by creating a system for identifying studies by defining threshold level methods capable of demonstrating scientific efficacy that can support the use of RG activities.
Williams et al. (Citation2012) included only eight RG articles (17%) of the 47 RG studies retained for analysis identified by the present empirical literature review. Similarly, only seven of the final 29 empirical studies (i.e. 25%) identified by this study were included in the (Williams et al. (Citation2012) meta-analysis. Importantly, 23 RG articles were published after Williams et al. (Citation2012). Fifteen of these studies were published before Williams et al. (Citation2012) but not included in their review.
In this context, the current review differs from prior literature reviews in several respects. Instead of critically examining all studies relevant to RG regardless of their methodological adequacy, we used a limited a priori set of inclusion criteria designed to maximize the external validity of findings reported in different studies. By using a priori criteria, we avoided the lengthy discussion of studies that ultimately will be discarded on the grounds of methodological flaws, design limitations, and poor external validity. By using replicable inclusion and exclusion criteria, this study makes it possible to track the development and growth of the science associated with RG systematically. Absent a systematic approach to gathering the scientific literature about RG, it is difficult to develop evidence-based prevention, treatment or policy practices. Without systematic evaluation, it simply is impossible to determine the best available practices.
The main findings of the present review of RG literature, based on minimal methodological requirements, indicates five specific areas of scientific research that provide the opportunity to draw some best practice in using: (1) self-exclusion; (2) gambling behavior to develop algorithms that can identify sentinel events; (3) limit setting; (4) responsible gambling machine features; and (5) employees training.
In brief, self-exclusion programs demonstrate some effectiveness as a component of RG programs despite various limitations including low utilization rates, breaching the agreement, and minimal evidence about the long-term outcomes. Although there is an increase in research focusing on behavioral indicators of gambling-related problems, the current state of knowledge remains underdeveloped. There is a lack of conclusive evidence about integrating these tools within fully developed RG programs. There is a growing focus on algorithms and diagnostic criteria that might be effective for identifying potential gambling-related problems (2012). Unfortunately, some of the currently offered algorithms and diagnostic systems are not based on empirical evidence or actual gambling behaviors. Limit setting has been assessed in terms of monetary and time limits, and mandatory and voluntary limit setting. There is empirical evidence that suggests that limit setting can be effective for promoting RG. However, it is important to remember that limit setting only is effective for some individuals (Shaffer et al. Citation2010); it can increase gambling problems for others. Therefore, we recommend that stakeholders carefully and conservatively consider the potential consequences of limit setting efforts. Machine features are modestly effective for limiting excessive gambling. Finally, venue staff providing assistance to patrons experiencing problem gambling demonstrates partial effectiveness as a useful RG initiative.
Limitations
As with any study, there are limitations to this empirical review of the extant RG research. This systematic analysis and synthesis of the RG literature should be regarded a ‘first approximation’ to summarizing the literature while taking into account the methodological quality of studies. Some would differ with the logic of our coding system. Others would disagree by adding or subtracting items or algorithms to our methodological rating system. Still others would quarrel with our data weighting strategies or multi-method approach to drawing conclusions. Miller et al.’s (cf. Shaffer et al., in press) synthesis of the alcohol treatment literature included a caveat that also applies to this project: despite our multi-step ‘…review process to minimize errors, it is likely that …there are over-looked details, and surely judgment calls for specific studies on which reasonable colleagues would disagree’ (p. 31).
This study identified only 29 studies using only some of the scientific methods that provide the scientific rigor necessary to offer interpretive confidence; importantly, only six of these studies met all three inclusion criteria for scientific rigor. Further, we could have used more than three methodological inclusion criteria to identify even more stringent and optimal research methods. This approach would have yielded a sample of empirical studies so small that drawing any conclusions would be difficult at best. Consequently, the evidence reveals that the field of RG is nascent and there are few principles or RG activities that can be considered ‘best practices’. Presuming best practices is a risky undertaking; adopting perceived best practices might produce unintended adverse effects. Protecting gamblers from inadvertent harms (e.g. increasing the incidence or prevalence of gambling problems; increasing adverse levels of stress and anxiety) that can result from well-intentioned efforts to prevent problems must be the foundation of RG programs (Broda et al. Citation2008; Nelson et al. Citation2008).
In closing, the current evidence about RG initiatives and programs is very limited. Using minimal methodological criteria, this study identified a small sample of scientific research focusing on RG. Had we used more rigorous methodological inclusion criteria, we would have identified less than seven studies that focused on RG. This evidence reveals that the overall effectiveness and impact of these RG activities remains uncertain. Consequently, the field has not yet progressed to best practices that are supported by scientific evidence; RG programs mostly remain at the ‘seemed like a good idea’ stage of development. This observation and conclusion raise important concerns when we take into account the costs (e.g. time, money and other resources) associated with the RG programs already implemented in many gambling venues around the world. This contrast leads to the following conclusion and the steps that urgently need to be taken.
As there are few studies that meet rigorous criteria for the study of RG, we encourage RG activists to develop and implement programs that assure the wellbeing of gamblers who might be placed at inadvertent risk of harm from well-intended RG activities that fail to achieve their intended objectives. In this context, different stakeholders need to work in collaboration to develop – and more importantly to evaluate – the efficacy and impact of RG initiatives.
Acknowledgements
The authors jointly accept responsibility for the content of this article. None of these supporters or any of the authors has personal interests in bwin.party, La Loterie Romande, ClubNSW, or the National Lottery that would suggest a conflict of interest.
During the preparation of this article, Howard Shaffer received reimbursement from Laval University for travel expenses, but no honorarium. In addition, The Division on Addiction at the Cambridge Health Alliance has received funding support from a variety of sources, including the following: bwin.party Interactive Entertainment, AG; The Foundation for Advancing Alcohol Responsibility (FAAR); National Institutes of Health (i.e. NIDA, NIAAA, NIMH); Substance Abuse and Mental Health Services Administration (SAMHSA); The National Center for Responsible Gambling (NCRG); Massachusetts Council on Compulsive Gambling; The Massachusetts Gaming Commission; The University of Nevada, Las Vegas; and DraftKings. Dr. Shaffer has received funding for consultation from Las Vegas Sands Corp., Davies Ward Phillips & Vineberg, LLP, and the DUNES of Easthampton.
During the preparation of this article Robert Ladouceur received funding support for the International Group on Responsible Gambling from La Loterie Romande (Switzerland), ClubNSW (Australia), Camelot (United Kingdom), La Française des Jeux (France), Loto-Québec (Québec, Canada), and the National Lottery (Belgium). In addition, the Ontario Problem Gambling Research Center and Fonds Québécois Recherche sur la Société et Culture (Quebec) provided funding to Dr. Ladouceur for this project.
During the preparation of this article, Alex Blaszczynski obtained reimbursement from the project funders for expenses; he did not receive any honorarium for this work. Dr. Blaszczynski has had financial professional dealings with the gambling industry and various state and federal governments directly and indirectly over the last three years including research funding, personal fees for professional consultancy, honoraria for grant reviews and theses examination, royalties for published books, and research funding and expenses covered to attend and present at conference and government meetings from the following gambling industry operators including: La Loterie Romande (Switzerland), Svenska Spel (Sweden), Club NSW (Australia), Camelot (United Kingdom), La Française des Jeux (France), Loto-Québec (Québec, Canada), Casino Austria, National Lottery (Belgium), Sportsbet, British Columbia Lottery Corporation, and Aristocrat Leisure Industries. He also has had financial dealings with organizations that are funded directly or indirectly from the gambling industry or levies on the gambling industry including the Victorian Responsible Gambling Foundation, Ontario Problem Gambling Research Centre, the Responsible Gambling Trust, Manitoba Gambling Research Program, Ministerial Expert Advisory Group (federal government), and honoraria and expense reimbursement for training programs and workshops conducted from government-funded problem gambling counseling services. Government-funded agencies include the NSW Office of Liquor, Gaming, & Racing, Australian Institute of Family Studies, Gambling Research Australia, Australian Department Social Services and non-industry or government agencies including the National Association for Gambling Studies, National Council on Problem Gambling, and Le Comité d’organisation Congrès international sur les troubles addictifs.
During the preparation of this article, Paige Shaffer obtained reimbursement from the Laval University; she did not receive any honorarium for this work.
The authors extend special thanks to La Loterie Romande (Switzerland), ClubNSW (Australia), Camelot (United Kingdom), La Française des Jeux (France), Loto-Québec (Québec, Canada), and the National Lottery (Belgium) for supporting this project.
Disclosure statement
The authors declare that they have no competing interests.
Additional information
Funding
Notes
1 Dates might vary because publications can carry a publication date for release ahead of print and then a later date when the print version is released.
Related Research Data
References
- American Psychiatric Association. 1994. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: Author.
- Auer MM, Griffiths MD. 2013. Voluntary limit setting and player choice in most intense online gamblers: an empirical study of gambling behaviour. J Gamb Stud. 29:647–660.
- Auer MM, Griffiths MD. 2014. An empirical investigation of theoretical loss and gambling intensity. J Gamb Stud. 30:879–887.
- Auer MM, Griffiths MD. 2015. Testing normative and self-appraisal feedback in an online slot-machine pop-up in a real-world setting. Front Psychol. 6:339. doi: 10.3389/fpsyg.2015.00339.
- Bangert-Drowns RL, Wells-Parker E, Chevillard I. 1997. Assessing the methodological quality of research in narrative reviews and meta-analyses. In: Bryant KJ, Windle M, West SG, editors. The science of prevention: methodological advances from alcohol and substance abuse research. Washington (DC): American Psychological Association, p. 405–429.
- Bill H03697, 03697 1-157 § 21. (a) 16. 2011.
- Blaszczynski A, Gainsbury SM, Karlov L. 2014. Blue gum gaming machine: an evaluation of responsible gambling features. J Gamb Stud. 30:697–712.
- Blaszczynski A, Ladouceur R, Shaffer HJ. 2004. A science-based framework for responsible gambling: the Reno model. J Gamb Stud. 20:301–317.
- Borkovec TD, Castonguay LG. 1998. What is the scientific meaning of empirically supported therapy? J Consult Clin Psychol. 66:136–142.
- Braverman J, LaPlante DA, Nelson SE, Shaffer HJ. 2013. Using cross-game behavioral markers for early identification of high-risk Internet gamblers. Psychol Addict Behav. 27:868–877.
- Braverman J, Shaffer HJ. 2012. How do gamblers start gambling: identifying behavioral markers for high-risk Internet gambling. Eur J Public Health. 22:273–278.
- Broda A, Laplante DA, Nelson SE, Labrie RA, Bosworth LB, Shaffer HJ. 2008. Virtual harm reduction efforts for Internet gambling: effects of deposit limits on actual Internet sports gambling behavior. Harm Reduct J. 5:27.
- Campbell DT, Fiske DW. 1959. Convergent and discriminant validation by the mulitrait-multimethod matrix. Psychol Bull. 56:81–105.
- Campbell DT, Stanley JC. 1963. Experimental and quasi-experimental designs for research. Chicago: Rand McNally & Company.
- Cooper H, Hedges LV, editors. 1994. The handbook of research synthesis. New York: Russell Sage Foundation.
- Delfabbro PH, Borgas M, King D. 2012. Venue staff knowledge of their patrons' gambling and problem gambling. J Gamb Stud. 28:155–169.
- Delfabbro PH, Winefield AH. 1999. Poker-machine gambling: an analysis of within session characteristics. Br J Psychol. 90:425–439.
- Dragicevic S, Percy C, Kudic A, Parke J. 2015. A descriptive analysis of demographic and behavioral data from internet gamblers and those who self-exclude from online gambling platforms. J Gamb Stud. 31:105–132.
- Ennett ST, Tobler NS, Ringwait CL, Flewelling RL. 1994. How effective is drug abuse resistance education? A meta-analysis of project DARE outcome evaluations. Am J Public Health. 84:1394–1401.
- Ferris J, Wynne H. 2001. The Canadian problem gambling index: final report. Ottawa, ON: Canadian Centre on Substance Abuse.
- Fortune EE, Goodie AS. 2012. Cognitive distortions as a component and treatment focus of pathological gambling: a review. Psychol Addict Behav. 26:298–310.
- Gainsbury SM, Aro D, Ball D, Tobar C, Russell A. 2015. Determining optimal placement for pop-up messages: evaluation of a live trial of dynamic warning messages for electronic gaming machines. Int Gamb Stud. 15:141–158.
- Gainsbury SM, Russell A, Blaszczynski A. 2014. Are psychology university student gamblers representative of non-university students and general gamblers? A comparative analysis. J Gamb Stud. 30:11–25.
- Gray HM, LaPlante DA, Shaffer HJ. 2012. Behavioral characteristics of Internet gamblers who trigger corporate responsible gambling interventions. Psychol Addict Behav. 26:527–535.
- Gray HM, Matthew A, LaPlante DA, Shaffer HJ. 2015. Using opinions and knowledge to identify natural groups of gambling employees. J Gamb Stud. 31:1753.
- Hayer T, Meyer G. 2010. Internet self-exclusion: characteristics of self-excluded gamblers and preliminary evidence for its effectiveness. Int J Ment Health Addict. 9:296–307.
- Hertwig R, Barron G, Weber EU, Erev I. 2004. Decisions from experience and the effect of rare events in risky choice. Psychol Sci. 15:534–539.
- Hing N, Cherney L, Gainsbury SM, Lubman DI, Wood RT, Blaszcynski A. 2015a. Maintaining and losing control during Internet gambling: a qualitative study of gamblers' experiences. New Media Soc. 17:1075–1095.
- Hing N, Nuske E. 2012. Responding to problem gamblers in the venue: role conflict, role ambiguity, and challenges for hospitality staff. J Hum Resour Hospital Tour. 11:146–164.
- Hing N, Russell A, Tolchard B, Nuske E. 2015b. Are there distinctive outcomes from self-exclusion? An exploratory study comparing gamblers who have self-excluded, received counselling, or both. Int J Ment Health Addict. 13:481–496.
- Hing N, Tolchard B, Nuske E, Holdsworth L, Tiyce M. 2014. A process evaluation of a self-exclusion program: a qualitative investigation from the perspective of excluders and non-Excluders. Int J Ment Health Addict. 12:509–523.
- Hunt, M. 1997. How science takes stock: the story of meta-analysis. New York: Russell Sage Foundation.
- Johnson BT, Carey MP, Marsh KL, Levin KD, Scott-Sheldon LAJ. 2003. Interventions to reduce sexual risk for the human immunodeficiency virus in adolescents, 1985–2000: a research synthesis. Arch Pediatr Adolesc Med. 157:381–388.
- LaBrie RA, Nelson SE, LaPlante DA, Peller A, Caro G, Shaffer HJ. 2007. Missouri casino self-excluders: distributions across time and space. J Gamb Stud. 23:231–243.
- Ladouceur R, Sévigny S. 2009. Electronic gambling machines: influence of a clock, a cash display, and a precommitment on gambling time. J Gamb Issues. 23:31–41.
- Ladouceur R, Sylvain C, Gosselin P. 2007. Self-exclusion program: a longitudinal evaluation study. J Gamb Stud. 23:85–94.
- LaPlante DA, Gray HM, LaBrie RA, Kleschinsky JH, Shaffer HJ. 2012. Gaming industry employees’ responses to responsible gambling training: a public health imperative. J Gamb Stud. 28:171–191.
- Lesieur H, Blume SB. 1987. The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. Am J Psychiatry. 144:1184–1188.
- Mosteller F, Colditz GA. 1996. Understanding research synthesis (meta-analysis). Annu Rev Public Health. 17:1–23.
- Munoz Y, Chebat JC, Borges A. 2013. Graphic gambling warnings: how they affect emotions, cognitive responses and attitude change. J Gamb Stud. 29:507–524.
- Nelson SE, Kleschinsky JH, LaBrie RA, Kaplan S, Shaffer HJ. 2010. One decade of self-exclusion: Missouri casino self-excluders four to ten years after enrollment. J Gamb Stud. 26:129–144.
- Nelson SE, Laplante DA, Peller AJ, Schumann A, Labrie RA, Shaffer HJ. 2008. Real limits in the virtual world: self-limiting behavior of Internet gamblers. J Gamb Stud. 24:463–477.
- Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. 2003. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 88:879–903.
- Quilty LC, Avila Murati D, Bagby RM. 2014. Identifying indicators of harmful and problem gambling in a Canadian sample through receiver operating characteristic analysis. Psychol Addict Behav. 28:229–237.
- Rosenthal R, Rosnow RL. 1991. Essentials of behavioral research: methods and data analysis. 2nd ed. New York: McGraw-Hill Publishing Company.
- Schellinck T, Schrans T. 2004a. Gaining control: trends in the processes of change for video lottery terminal gamblers. Int Gamb Stud. 4:161–174.
- Schellinck T, Schrans T. 2004b. Identifying problem gamblers at the gambling venue: finding combinations of high confidence indicators. Gamb Res. 16:8–24.
- Shaffer HJ, Gray HM, Nelson SE, LaPlante DA. in press. Technology, the Internet, and gambling: how the medium can facilitate addiction, adaptation, and intervention. In: Faust D, Faust K, Potenza MN, editors. The Oxford handbook of digital technologies and mental health. Oxford University Press.
- Shaffer HJ, Hall MN, Vander Bilt J. 1999. Estimating the prevalence of disordered gambling behavior in the United States and Canada: a research synthesis. Am J Public Health. 89:1369–1376.
- Shaffer HJ, Hall MN. 1996. Estimating the prevalence of adolescent gambling disorders: a quantitative synthesis and guide toward standard gambling nomenclature. J Gamb Stud. 12:193–214.
- Shaffer HJ, Peller AJ, LaPlante DA, Nelson SE, LaBrie RA. 2010. Toward a paradigm shift in Internet gambling research: from opinion and self-report to actual behavior. Addict Res Theory. 18:270–283.
- Shaffer HJ, Peller AJ, LaPlante DA, Nelson SE, LaBrie RA. 2011. Research using actual behavior encourages and confirms accurate self-report: a response to Griffiths’ (2010) further comments. Addict Res Theory. 19:87–88.
- Shaffer HJ, Stanton MV, Nelson SE. 2006. Trends in gambling studies research: quantifying, categorizing, and describing citations. J Gamb Stud. 22:427–442.
- Tobler NS. 1986. Meta-analysis of 143 adolescent drug prevention programs: quantitative outcome results of program participants compared to a control or comparison group. J Drug Issues. 16:537–567.
- Tremblay N, Boutin C, Ladouceur R. 2008. Improved self-exclusion program: preliminary results. J Gamb Stud. 24:505–518.
- Williams RJ, West BL, Simpson RI. 2012. Prevention of problem gambling: a comprehensive review of the evidence, and identified best practices. [Internet]. Available from: http://hdl.handle.net/10133/3121
- Xuan Z, Shaffer HJ. 2009. How do gamblers end gambling: longitudinal analysis of Internet gambling behaviors prior to account closure due to gambling related problems. J Gamb Stud. 25:239–252.
- Adami N, Benini S, Boschetti A, Canini L, Maione F, Temporin M. 2013. Markers of unsustainable gambling for early detection of at-risk online gamblers. Int Gamb Stud. 13:1–17. doi: http://dx.doi.org/10.1080/14459795.2012.754919.
- Blaszczynski A, Ladouceur R, Nower L. 2007. Self-exclusion: a proposed gateway to treatment model. Int Gamb Stud. 7:59–71.
- Gainsbury SM. 2014. Review of self-exclusion from gambling venues as an intervention for problem gambling. J Gamb Stud. 30:229–251.
- Gainsbury SM, Blankers M, Wilkinson C, Schelleman-Offermans K, Cousijn J. 2014. Recommendations for international gambling harm-minimisation guidelines: comparison with effective public health policy. J Gamb Stud. 30:771–788.
- Hing N, Nuske E. 2012. The self-exclusion experience for problem gamblers in South Australia. Aust Soc Work. 65:457–473.
- Hing N, Nuske E, Holdsworth L. 2013. How gaming venue staff use behavioural indicators to assess problem gambling in patrons. J Gamb Issues. 28:1–25.
- Jardin BF, Wulfert E. 2012. The use of messages in altering risky gambling behavior in experienced gamblers. Psychol Addict Behav. 26:166–170.
- Kim HS, Wohl MJA, Stewart MJ, Sztainert T, Gainsbury SM. 2014. Limit your time, gamble responsibly: setting a time limit (via pop-up message) on an electronic gaming machine reduces time on device. Int Gamb Stud. 14:266–278.
- Ladouceur R, Blaszczynski A, Lalande DR. 2012. Pre-commitment in gambling: a review of the empirical evidence. Int Gamb Stud. 12:215–230.
- Moodie C, Reith G. 2009. Responsible gambling signage on electronic gaming machines, before and after the implementation of the United Kingdom Gambling Act: an observational study. Int Gamb Stud. 9:5–17.
- Philander KS, MacKay TL. 2014. Online gambling participation and problem gambling severity: is there a causal relationship? Int Gamb Stud. 14:214–227.
- Rockloff MJ, Hing N. 2012. The impact of jackpots on EGM gambling behavior: a review. J Gamb Stud. 29:775–790.
- Rockloff MJ, Donaldson P, Browne M. 2015. Jackpot expiry: an experimental investigation of a new EGM player-protection feature. J Gamb Stud. 31:1505–1514.
- Walker DM, Litvin SW, Sobel RS, St-Pierre RA. 2015. Setting win limits: an alternative approach to ‘responsible gambling’? J Gamb Stud. 31:965–986.
- Wohl MJA, Gainsbury S, Stewart MJ, Sztainert T. 2012. Facilitating responsible gambling: the relative effectiveness of education-based animation and monetary limit setting pop-up messages among electronic gaming machine players. J Gamb Stud. 29:703–717.
- Wohl MJA, Santesso DL, Harrigan K. 2013. Reducing erroneous cognition and the frequency of exceeding limits among slots players: a short (3-minute) educational animation facilitates responsible gambling. Int J Ment Health Addict. 11:409–423.
Appendix
RG Articles
This appendix includes the 18 RG articles that failed to satisfy any of the three methodological criteria necessary for inclusion among the final set of empirical RG studies.