
Abstract
Objectives: This study evaluated the glycaemic response of three commonly consumed meals, and the resultant effect on postprandial plasma glucose response in type 2 diabetes mellitus patients at the University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu State, Nigeria.
Design: This was an experimental study on 100 consenting type 2 diabetes mellitus patients who were on medical nutrition therapy only, attending the University of Nigeria Teaching Hospital medical outpatient clinic between May 2012 and March 2013.
Subjects and setting: One hundred non-diabetic healthy University of Nigeria Teaching Hospital workers served as the control. Participants consumed served portions of each meal containing 50 g of glycaemic carbohydrate. Only the control consumed 50 g glucose to establish glycaemic response. The three test meals comprised pap and bambara nut pudding; meat and okro soup with fermented cassava dough; and meat, beans and corn pottage with spinach.
Outcome measures: Plasma glucose was measured quarter hourly, for two hours, from which glycaemic index (GI) and glycaemic load (GL) values were calculated per serving.
Results: Two meals, namely meat, beans and corn pottage with spinach; and pap and bambara nut pudding; provided a lower glycaemic response and reduced postprandial plasma glucose peak compared to meat and okro soup with fermented cassava dough at 30, 45, 60, 90 and 120 minutes in non-diabetic and type 2 diabetes mellitus patients (p-value < 0.050). The lowest GI and GL values per serving were attributed to the meat, beans and corn pottage with spinach (33.00 ± 1.25 and 4.76 ± 0.67), while the highest respective values were found for the meat and okro soup with fermented cassava dough (74.50 ± 4.91 and 21.59 ± 1.06).
Conclusion: Compared to the other two meals, the meal of meat, beans and corn pottage with spinach resulted in a lower glycaemic response, reduced postprandial plasma glucose in non-diabetic and type 2 diabetes mellitus patients, and constituted a healthy alternative to the other two.
Introduction
Glycaemic index (GI) and glycaemic load (GL) are two means of classifying glycaemic response to carbohydrate-containing foods. The GI is defined as the incremental area under the blood glucose response curve (IAUC) after the consumption of the carbohydrate portion of a test food, expressed as a percentage of the average IAUC response to the same amount of carbohydrate from a reference food, taken by the same subject on a separate occasion.Citation1 The GI of food is a scale used to classify the quality of carbohydrate consumed and ranks carbohydrate according to its potential to increase blood glucose levels; low GI foods are digested and absorbed slowly, and high GI foods are digested and absorbed rapidly.Citation2 Oral fat administration reduces the rate of gastric emptying, jejunal motility and postprandial flow rates in the upper small intestine, thereby decreasing the rate of increase in postprandial glucose.Citation3 Dietary fibre, especially soluble fibre, increases the viscosity of food, slowing gastric emptying rates, digestion and the absorption efficiency of the small intestine, causing absorption to occur over a longer time.Citation4 The GL per serving reflects the total glycaemic response by accounting for the quantity and quality of carbohydrate consumed.Citation5
A lower GI diet decreases postprandial glucose and insulin response, improves serum lipid concentrations, decreases total fat mass and reduces the risk of colon cancer in adults.Citation6 Consuming a high GI meal can lead to an exaggerated postprandial peak in the blood glucose,Citation7 which can result in diabetes-related complications, including heart disease, strokes, obesity, kidney disease, blindness, erectile dysfunction, amputations, mortalityCitation8 and cancer.Citation9 Knowledge of the GI value of locally available food helps diabetic patients to choose from less expensive healthy foods, and to improve diet quality without undue financial burden.Citation10 One half to two thirds of people in the south-eastern states of Nigeria consume pap and bambara nut pudding; meat and okro soup with fermented cassava dough; and meat, beans and corn pottage with spinach “almost every day” (food frequency questionnaire in 2013, unpublished). The purpose of conducting this study was to evaluate the glycaemic response of some commonly consumed meals and the resultant effect on postprandial plasma glucose response in type 2 diabetes mellitus patients at the University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu State, Nigeria.
Method
Ethics approval
The joint University of Ibadan/University College Hospital Ibadan Institutional Review Board and the University of Nigeria Teaching Hospital (Ituku-Ozalla) Institutional Review Board approved the study protocol (UI/EC/12/0275, IRB00002323). All of the procedures were conducted with an adequate understanding by, and the written consent of, the participants.
Participants
One hundred outpatients (45 men and 55 women), diagnosed with type 2 diabetes mellitus and recruited randomly from the diabetes clinic at the University of Nigeria Teaching Hospital, Ituku-Ozalla, participated in the study. Patients with type 2 diabetes mellitus were treated with medical nutrition therapy alone, and were aged 40-70 years [mean ± standard deviation (SD) of 55.64 ± 7.84 years], with a body mass index (BMI) of < 30 kg/mCitation2 (mean ± SD of 27.8 ± 4.52). The duration of diabetes mellitus was ≤ 5 years, with fasting plasma glucose < 11.2 mmol/l. The participants had not experienced dyslipidaemia, hypertension, acute illness, fever, undue stress, gastrointestinal disease, autonomical dysfunction or severe hypoglycaemic episodes during the past year, nor taken oral or inhaled prednisone or cortisone medication in the previous 30 days. One hundred apparently healthy non-diabetic University of Nigeria Teaching Hospital workers who were matched in age and sex with the type 2 diabetes mellitus patients formed the control group. They had a BMI < 30 kg/mCitation2 (mean ± SD of 23.14 ± 4.13), fasting plasma glucose < 5.8 and > 3.3 mmol/l and > 7.7 mmol/l (why three values here?) 120 minutes after the ingestion of 75 g oral glucose. Individuals with coronary heart disease, a history of renal and liver disease, surgery in the six months preceding the study, or who were currently on any medication were ineligible to participate. Eligible participants attended a screening visit.
Test meals
Three different meals were used for testing:
Pap and bambara nut pudding.
Meat and okro soup, with fermented cassava dough.
Meat, beans and corn pottage with spinach.
Test meal 1: Pap and bambara nut pudding
Yellow maize was fermented, grinded, sieved and squeezed to create a wet slurry. The slurry was further dissolved in water to result in an even thinner slurry. Boiling water was poured into it to produce a gelatinised pap. Bambara nut pudding was prepared by reconstituting the sieved flour of bambara nut seeds with hot water, in which fresh pepper, palm oil and salt were added for palatability. An acceptable quantity was poured into banana leaves (Thaumatococcus daniellii) wrapped and steamed for one hour. The product was bambara nut pudding (okpa) and was consumed, together with maize pap.
Test meal 2: Meat and okro soup, with fermented cassava dough
The soup ingredients included okro (Abelmoschus esculentus), fluted pumpkin leaves, beef meat, onions, fresh pepper, salt, palm oil, a stock cube, dry hake, dry fish and ground crayfish. The sieved fermented cassava paste was moulded and boiled in hot water twice and pounded twice. Okro soup was cooked with the above ingredients. Cooked fermented cassava dough (foofoo) was consumed with a bowl of soup.
Test meal 3: Meat, beans and corn pottage with spinach
Beans were soaked overnight and cooked with fresh whole corn. Fresh pepper, onions, salt, a stock cube, crayfish and palm oil were added to the cooking mixture. The beans and corn pottage was consumed with spinach leaves and boiled beef meat.
The macronutrient composition of the meals in cooked weight basis was determined according to the Association of Analytic Communities method ().
Table I: Macronutrient composition of each test meal per 100 g edible portion
The meals were provided in portions equivalent to 50 g glycaemic carbohydrate, which is defined as total sugars plus starch, according to the recommendation of the Joint Food and Agricultural Organization of the United Nations/World Health Organization expert consultation.Citation11 The test meals portion weights are presented in .
Table II: Macronutrient composition of each test meal and glucose used in a cohort of 100 type 2 diabetes mellitus patients and 100 non-diabetic subjects
The required portion of each test meal was measured and prepared by the same dietician on each test day. Fifty grams of glucose dissolved in 240 ml of water served as the reference food for the non-diabetics (control group).
Protocol
Subjects were tested on three separate occasions. A washout period of one week was allowed, which preceded the next test. The non-diabetics (control group) presented at the hospital for a fourth and fifth weekly visit for the 50 g glucose administration. Each participant arrived at 7h00 after a 12-hour overnight fast. Fasting plasma glucose readings were taken twice, and the average of the two values was recorded. Subjects were randomly given one of the three meals to consume with 240 ml of water within 15 minutes. The non-diabetics also consumed 50 g glucose within this time. The subjects remained sedentary, with the exception of trips to the bathroom, during the two-hour study period. All of the participants completed the study.
Blood samples were drawn through an intravenous catheter placed in the upper arm in the antecubital vein before the consumption of the test meal 15, 30, 45, 60, 90 and 120 minutes after starting to eat. Venous blood glucose (plasma with potassium oxalate and sodium fluoride anticoagulant) was measured in the University of Nigeria Teaching Hospital chemical pathology laboratory by a medical laboratory scientist using the glucose oxidation method (Roche/Hitachi 902® auto analyzer, Roche Diagnostics, Japan). Participants received compensation for travel, time and effort upon study completion.
Statistical analysis
The GI and the IAUC, excluding the area below the fasting baseline, were calculated using the trapezoid rule. The GI for each non-diabetic subject (control) was calculated by determining the average IAUC of the reference food, and then dividing the IAUC of the test meal by the average IAUC of the reference food, multiplied by 100.Citation12 The GL per serving was calculated by taking the product of the GI and the grams of carbohydrate per serving and dividing the product by 100.Citation13 The mean GI and GL per serving were determined only in non-diabetic subjects (control).
Data were expressed as mean ± SD. One-way analysis of variance was used to determine the meal and timing effects on glucose. Student’s t-test was used to compare the IAUC between the groups. A p-value < 0.050 was considered to be significant in all of the statistical tests. Statistical analysis was performed with Statistical Package for Social Sciences® version 20.
Results
Fasting plasma glucose was significantly higher in type 2 diabetes mellitus patients than in the control group (p-value < 0.050). However, the values were not significantly different within the two groups (p-value > 0.050) ( and ). The IAUC for glucose was significantly lower for all the meals in the non-diabetics than type 2 diabetes mellitus patients (p-value < 0.050) (). There were significant differences in the mean plasma postprandial glucose levels at 30 and 60 minutes in the non-diabetic participants ().
Figure 1: Mean plasma glucose concentrations at 0, 15, 30, 45, 60, 90 and 120 minutes after the consumption of glucose or the test meals by the non-diabetic subjects (control group)*
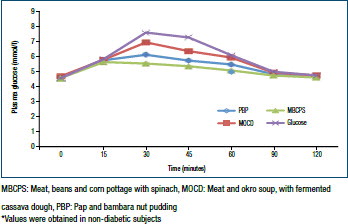
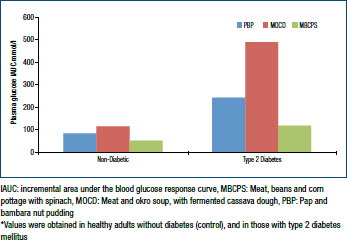
The ingestion of 50 g glucose resulted in a significant increase (p-value < 0.050) in the IAUC at 153.62 ± 18.77 for 50 g glycaemic carbohydrate in the meals of meat and okro soup with fermented cassava dough (114.45 ± 18.58), pap and bambara nut pudding (61.65 ± 14.24) and meat, beans and corn pottage with spinach (50.70 ± 10.34) (). This resulted in a GI value for meat and okro soup with fermented cassava dough of 74.50 ± 4.91, pap and bambara nut pudding of 40.13 ± 2.86, and meat, beans and corn pottage with spinach of 33.00 ± 1.25. The GI values of pap and bambara nut pudding; and meat, beans and corn pottage with spinach, were considered to be low GI, while a high GI was recorded for the meat and okro soup with fermented cassava dough. The GL values for a serving (one milk tin) of meat, beans and corn pottage with spinach at 4.76 ± 0.67, and pap and bambara nut pudding at 7.05 ± 0.61, were significantly lower (p-value < 0.050) than that for meat and okro soup with fermented cassava dough at 21.59 ± 1.06. The IAUC for blood glucose in the meal of meat, beans and corn pottage with spinach was significantly lower at 120.90 ± 17.59, than that in the pap and bambara nut pudding at 270.30 ± 19.54, and meat and okro soup with fermented cassava dough at 448.10 ± 21.52 (p-value < 0.050) in patients with type 2 diabetes mellitus (). The consumption of meat, beans and corn pottage withspinachsignificantlydecreasedtheplasmaglucoseconcentration, reaching a maximum value of 8.85 ± 1.06 mmol/l (159.30 mg/ dl) at 60 minutes. The consumption of meat and okro soup with fermented cassava dough gradually increased the postprandial peak glucose at 60 minutes, reaching a maximum value of 12.97 mmol/l (233.46 mg/dl), while the pap and bambara nut pudding reached a maximum value of 10.18 mmol/l (183.24 mg/dl) (p-value < 0.050). The meals of meat, beans and corn pottage with spinach; and pap and bambara nut pudding, produced a smaller postprandial plasma glucose peak compared to the meal of meat and okro soup with fermented cassava dough at 30, 45, 60, 90 and 120 minutes (p-value < 0.050) (). Therefore, these two were more effective in reducing the postprandial glucose peak.
Figure 2: Mean fasting and postprandial plasma glucose concentrations after the consumption of the test meals by the subjects with type 2 diabetes mellitus*
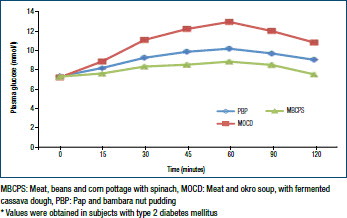
Figure 3: Mean incremental area under the blood glucose response curve for plasma glucose after the consumption of the test meals by non-diabetic and type 2 diabetes mellitus subjects*
Discussion
Excessive and prolonged postprandial blood glucose peaks are a serious health problem for individuals with diabetes mellitus owing to the risk of micro- and macrovascular damage. As a result, changes in lifestyle have been suggested as the main strategy for controlling the biochemical abnormalities associated with type 2 diabetes mellitus.Citation14 The results of this study showed that a low glycaemic response was achieved with meat, beans and corn pottage with spinach, and that this meal also resulted in the postprandial blood glucose peak being minimised. Thus, this meal should be recommended to patients with type 2 diabetes mellitus.
Many characteristics of a meal affect the glycaemic response, including the quantity and quality of carbohydrate, meal preparation method, rate of gastric emptying and the presence of other nutrients in the meal, such as fibre, fat and protein.Citation15 A significantly higher GI, GL per serving, peak plasma postprandial glucose, greater IAUC, higher sugar and starch content, and thus more glycaemic carbohydrate, was realised with the meal of meat and okro soup with fermented cassava dough, compared to that in the other two meals for the same serving size of one milk tin. As the GI was also higher, the GL per serving was also more than double that of the other meals. This is because cassava root is a storage organ, cannot be used for vegetative propagation, and is a concentrated source of carbohydrate, especially when it is fermented.
Glycaemic response increased with the length of fermentation. During fermentation, the action of microbes on the starches in the tuber root favours the amount of monosaccharide which can be formed from the starch in the food, thus speeding up digestion in the body.Citation16 Cassava root which is cooked as a starch has a low GI value of 46, just like sweet potato with purple skin and white flesh. However, when the cassava root is ground and dried to a powder or processed into pearls (also called tapioca), the GI almost doubles to 80 for tapioca flour, and 81 for tapioca pudding, owing to the processing. Most flour made by the milling of low-GI, intact wholegrains, e.g. barley, wheat and corn, are high GI, owing to the processing.Citation17 A positive association between the carbohydrate amount (especially when the GI is high, yielding a high-GL diet) and the incidence of diabetes mellitus has been reported in ChineseCitation18 and JapaneseCitation19 women. A diet high in carbohydrate and with a high GI (implying a high-GL diet) was associated with a higher risk of type 2 diabetes mellitus.Citation18
Lowest glycaemic response was recorded with the meal of meat, beans and corn pottage with spinach because the cooked corn and beans were intact and whole, resulting in a slower rate of digestion. The slowly digestible behaviour may relate to restricted enzymatic availability and enzyme inhibition because of the compact food structure. The meal of meat, beans and corn pottage with spinach may contain soluble fibre, which is associated with delayed gastric emptying. Delayed absorption may be linked to a delayed gastric emptying rate and the slow release of starch in the small intestine.Citation20
In one study, soluble fibre was significantly inversely associated with metabolic syndrome.Citation21 The meal of meat, beans and corn pottage with spinach was also not very dense in carbohydrates, contained moderate fat, and should be recommended for optimal glycaemic control in type 2 diabetes mellitus patients.
The meal of pap and bambara nut pudding was high in fat composition, and should be recommended with caution during menu planning for type 2 diabetes mellitus patients, despite its low glycaemic response. The fat content of this meal could be reduced by using less palm oil than the amount used in the traditional recipe. Dietary fat, especially saturated fat and trans-fat, is associated with an increased risk for several chronic diseases, including type 2 diabetes mellitus, hypertension, cardiovascular disease and cancer.Citation22 The meal of pap and bambara nut pudding probably had a low GI as it contained bambara nut seeds, and a low GI is usually reported for seeds. Its high fat content may also delay gastrointestinal transit, leading to a lesser glycaemic response.Citation23 More vegetables could be added to this meal to help increase its fibre content and volume, and to lower the GL per serving.
The meals differed in their GL values per serving, even when they were approximately the same in terms of energy content with respect to a serving size (one starch exchange). In this context, the same glycaemic effect (GL value per serving of approximately 10) could be achieved with three evaporated milk tins of meat, beans and corn pottage with spinach, one and a half milk tins of pap and bambara nut pudding, and half a milk tin of meat and okro soup with fermented cassava dough. Kitchen scales are inaccessible in most Nigerian homes. Thus, households measures, e.g. a milk tin, serve as an alternative device to estimate the size of meals. Type 2 diabetes mellitus patients should consume two milk tins of meat, beans and corn pottage with spinach as a single meal portion for optimal glycaemic control, as this meal is high in fibre and contains more slowly digestible (low GI) sugar and starch, is less dense in carbohydrates, and thus has a low GL per serving. It also contains moderate fat content.
Target goals for postprandial blood glucose levels have been established. The International Diabetes Federation recommends a two-hour postprandial glucose of < 140 mg/dl (< 7.8 mmol/l),Citation24 and the American Diabetes Association a peak postprandial glucose of < 180 mg/dl (< 10.0 mmol/l) generally 1-2 hours after commencement of a meal.Citation25 The meal of meat and beans and corn pottage with spinach caused blood glucose peaks below that recommended by the ADA. The European Diabetes Working Group set the maximum postprandial glucose peak to not exceed 160 mg/dl (9.0 mmol/l) to reduce microvascular risk.Citation26 The consumption of a meal of meat and beans and corn pottage with spinach could reduce the incidence of kidney disease, blindness, erectile dysfunction, amputation and mortality in patients with type 2 diabetes mellitus.
Conclusion
It was revealed in the present study that compared to the other two meals, the meal of meat, beans and corn pottage with spinach was less dense in carbohydrates, while being high in fibre and slowly digestible carbohydrates, contained cooked, intact grain, and had a moderate fat content and a significantly lower GI and GL value per serving, as well as peak plasma postprandial blood glucose and IAUC. The meal of meat, beans and corn pottage with spinach is a healthy alternative to the other two. Hence, its consumption is recommended in patients with type 2 diabetes mellitus for optimal glycaemic control. As a result of this study, it is recommended that a meal comprising two milk tins of meat, beans and corn pottage with spinach should be consumed as a single meal portion as this will serve to help improve glycaemic control in patients with type 2 diabetes mellitus.
References
- Wolever TMS. Carbohydrate and the regulation of blood glucose and metabolism. Nutr Rev. 2003;61(5 Pt 2):S40–S48. doi: 10.1301/nr.2003.may.S40-S48
- Brand-Miller J, Petocz P, Hayne S, Colagiuri S. Low-glycemic index diets in the management of diabetes: a meta-analysis of randomized controlled trials. Diabetes Care. 2003 26(8):2261–2267. doi: 10.2337/diacare.26.8.2261
- Owen B, Wolever TMS. Effect of fat on glycaemic responses in normal subjects: a dose-response study. Nutr Res. 2003;23:1341–1347. doi: 10.1016/S0271-5317(03)00149-0
- McKeown NM, Meigs JB, Liu S, et al. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham offspring cohort. Diabetes Care. 2004;27(2):538–546. doi: 10.2337/diacare.27.2.538
- Sheard NF, Clark NG, Brand-Miller JC, et al. Dietary carbohydrate (amount and type) in the prevention and management of diabetes: a statement by the American Diabetes Association. Diabetes Care. 2004;27(9): 2266–2271. doi: 10.2337/diacare.27.9.2266
- Davis MS, Miller CK, Mitchell DC. More favorable dietary patterns are associated with lower glycaemic load in older adults. J Am Diet Assoc. 2004;104(12):1828–1835. doi: 10.1016/j.jada.2004.09.029
- Dong KR, Wanke CA, Tang AM, et al. Dietary glycemic index of human immunodeficiency virus-positive men with and without fat deposition. J Am Diet Assoc. 2006;106(5):728–732. doi: 10.1016/j.jada.2006.02.007
- Gonzalez AB, Salas D, Umpierrez GE. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Cur Med Res Opin. 2011;27(5):969–979. doi: 10.1185/03007995.2011.563505
- Augustin LS, Dal Maso L, La Vecchia C, et al. Dietary glycemic index and glycemic load and breast cancer risk: as case-control study. Ann Oncol. 2001;12(11):1533–1538. doi: 10.1023/A:1013176129380
- Nansel T, Haynie D, Lipsky L, et al. Little variation in diet cost across wide ranges of overall dietary quality among youth with type 1 diabetes. J Acad Nutr Diet. 2015;115(3):433–439. doi: 10.1016/j.jand.2014.07.035
- Food and Agriculture Organization of the United Nations, World Health Organization. Carbohydrate in Human Nutrition. Rome. Italy: FAO/WHO, 1998.
- Torres N, Palacios-Gonzalez B, Noriega-López N, Tovar AR. Glycemic index, glycemic load insulinemic index and soy beverage with low and high in Carbohydrates. Rev Invest Clin. 2006;58(5):487–497.
- Wolever TMS, Vorster HH, Bjorck I, Brand-Miller J, et al. Determination of the glycaemic index of foods: interlaboratory study. Eur J Clin Nutr. 2003;57(3):475–482. doi: 10.1038/sj.ejcn.1601551
- Hodge AM, English DR, O’Dea K, Giles GG. Glycemic index and dietary fiber and the risk of type 2 diabetes. Diabetes Care. 2004;27(11):2701–2706. doi: 10.2337/diacare.27.11.2701
- Miller CK, Gabbay RA, Dillon J, et al. The effect of three snack bars on glycemic response in healthy adults. J Am Diet Assoc. 2006;106(5):745–748. doi: 10.1016/j.jada.2006.02.003
- Ihediohanma NC. Determination of the glycaemic indices of three different cassava granules (garri) and the effect of fermentation period on their glycemic responses. Pak J Nutr. 2011;10(1):6–9. doi: 10.3923/pjn.2011.6.9
- Foster-Howell K, Holt HA, Brand-Miller JC. International table of glycemic index and glycemic load values. Am J Clin Nutr. 2002;76(1):5–56.
- Villegas R, Liu S, Gao YT, et al. Prospective study of dietary carbohydrates, glycemic index, glycemic load, and incidence of type 2 diabetes mellitus in middle-aged Chinese women. Arch Intern Med. 2007;167(21):2310–2316. doi: 10.1001/archinte.167.21.2310
- Nanri A, Mizoue T, Noda M, et al. Rice intake and type 2 diabetes in Japanese men and women: the Japan Public Health Center-based Prospective Study. Am J Clin Nutr. 2010;92(6):1468–1477. doi: 10.3945/ajcn.2010.29512
- Hallifrisch J, Behall KM. Improvements in insulin and glucose responses related to grains. Cereal Foods World. 2000;45:66–69.
- Liese AD, Roach AK, Sparks KC, et al. Whole grain intake and insulin sensitivity: the Insulin Resistance Atherosclerosis Study. Am J Clin Nutr. 2003;78(5):965–971.
- Wahlqvist ML. Dietary fat and the prevention of chronic disease. Asia Pac J Clin Nutr. 2005;14(4):313–318.
- Wolever TMS, Jenkins DJA, Jenkins AL, Josse RG. The glycemic index: methodology and clinical implications. Am J Clin Nutr. 1991;54(4):846–854.
- International Diabetes Federation. Guideline for management of post-meal glucose. Brussels: International Diabetes Federation, 2007.
- American Diabetes Association. Standard of medical care in diabetes – 2010. Diabetes Care. 2010;33(Suppl 1):S11–S61.
- Pearce KL, Noakes M, Keogh J, Clifton PM. Effect of carbohydrate distribution on postprandial glucose peaks with the use of continuous glucose monitoring in type 2 diabetes. Am J Clin Nutr. 2008;87(3):638–644.