
Abstract
Objectives: To determine the dietary and nutrient intakes of bank employees in Accra in relation to recommended dietary intake for the control of cardiovascular diseases (CVD).
Design: The study was a cross-sectional study.
Methodology: A structured validated questionnaire was used to obtain demographics. A 3-day 24-hour dietary recall and usual food intake questionnaire were used to obtain information on food intakes and dietary pattern of the respondents. Food models, household measures and photos of common dishes as well as household cups and measures were used in order to obtain accurate information regarding the types and quantities of foods and beverages consumed.
Subjects: Convenient sampling was used to select bank branches while simple random sampling by ballot without replacement was used to select 119 bank employees who consented to participate in the study.
Outcome measures: Data were analysed using Statistical Package for the Social Sciences software. Esha FPro software was used to analyse food nutrients. The nutrient intakes were compared with a standard dietary guideline for adults.
Results: Findings showed significant (p < 0.05) differences in mean energy intake between males and females. Also, the bank employees were consuming more fat (32%) compared with the recommended intake. The average intake of dietary sodium and cholesterol was within the recommended intake levels. All the participants in the study had a mean intake of dietary potassium, fibre, fruits and vegetables below the recommended levels. The major cooking oils used in meal preparation were vegetable and palm oil (46%), followed by vegetable oil (31.9%) and palm oil (21.8%).
Conclusions: The study evaluated the dietary intake of bank employees, which is an important risk factor for chronic diseases. There is a need to develop plans to provide nutrition education and counselling for adequate nutrient intake and prevention of chronic diseases among bank employees.
Layman's summary: Obtaining an adequate diet and avoiding overconsumption of food helps to maintain health. Intake of foods containing high energy and fats without corresponding energy expenditure through physical activity could result in obesity, heart diseases, diabetes and other health challenges. Inadequate intake of micronutrients as well could result in deficiency diseases, and depresses the immune system and health of individuals. Bank employees and all other individuals need to pay attention to what they eat to live a healthy and longer life. Regular physical activity, following the dietary approaches to avoid hypertension and regular medical check-up are essential for cardiovascular health.
Strong lay message: Inadequate or overconsumption of nutrients can cause chronic heart diseases.
Introduction
The disease burden caused by modifiable risk factors is a global problem. It is estimated that modifiable risk factors are responsible for about 80% of coronary heart disease and cardiovascular diseases (CVDs).Citation1 Behavioural risk factors of CVDs include unhealthy diet, physical inactivity, alcohol consumption and tobacco use while biological risk factors include raised blood cholesterol, hypertension (raised blood pressure), overweight, obesity and type 2 diabetes.Citation2,Citation3
Scientific evidence increasingly supports the view that alterations in diet impact positively and/or negatively on health throughout life.Citation4 Most importantly, dietary modification may not only influence present health, but may contribute to an individual not developing such diseases as CVDs, diabetes and cancer in older age. Unhealthy dietary practices such as high consumption of saturated fats, refined carbohydrates as well as low consumption of fruit and vegetables tend to increase the risk of CVD.Citation5 Fruits and vegetables contain many nutrients such as vitamins, minerals and fibre, which may individually or in combination provide protection against cardiovascular diseases and certain cancers.Citation5 It has been reported that consumption of green leafy vegetables and vitamin C-rich fruits and vegetables protect against coronary heart disease (CHD).Citation6 The cardioprotection of green leafy vegetables may be due to high levels of antioxidants such as lutein.Citation6,Citation7 Furthermore, studies have shown that lutein protects against progression of atherosclerosis by lowering LDL levels in the blood.Citation7
It has been reported that the banking occupation carries with it the risk of unhealthy dietary habits such as snacking on pastries (high in trans fats), eating fast-foods, drinking of soft drinks high in refined sugar and late-night eating because most employees return late from work, especially in Ghana.Citation8 The health implication of this dietary habit coupled with the sedentary lifestyle imposed on them by the nature of their job may manifest in an individual as high blood pressure, raised blood lipids, overweight and obesity.Citation5 This had been confirmed from a study in India among bank employees.Citation8 The study in India revealed that body mass index (BMI), blood pressure, plasma cholesterol and glucose levels were significantly high among bank employees.Citation8 Bank employees in Ghana are one of the groups of employees that wake early to go to work and return late to their houses. Also, most of them sit for long hours attending to customers and thus have little time for physical activity and sleep, which is a CVD risk factor reported in a similar study in India.Citation8 Combinations of these risk factors are likely to have multiple effects that are capable of accelerating the rate at which the individual develops non-communicable chronic diseases (NCDs) including CVDs. Most food consumption studies in Ghana focused on other sectors of the workforce. Bank employees have been a neglected group of workers in most nutrition studies because it is believed that they earn a lot of money and can afford to eat whatever they desire. The most common type of malnutrition in Ghana is undernutrition, thus studies have concentrated on undernutrition studies among children, women and other vulnerable groups. However, this study had to shift its focus from the usual group for nutrition research to the unusual (bank employees). There is an increasing prevalence of NCDs in developing countries.Citation9 Unhealthy diet is one of the CVD risk factors but a dearth of studies on the nutrient intake of bank employees in Ghana. Hence, the study determined the dietary and nutrient intakes of bank employees in Accra in relation to recommended dietary intake for the control of cardiovascular diseases, especially the dietary component of Dietary Approaches to Stop Hypertension (DASH).
Methods
Study design and site description
The study was a cross-sectional study in five branches of a bank in Accra. The bank had 160 branches and 2 158 staff nationwide. The five branches in Accra were conveniently sampled based on the recommendation and consent of the Human Resource manager for the branches to participate in the study. All the bank branches used in this study were located in the Greater Accra region of Ghana.
Sampling techniques
Using the Statscalc function of Epi Info™ statistical software (CDC, Atlanta, GA, USA), a confidence interval of 95%, estimated prevalence of risk factor of 10% and a worst acceptable estimate of 5% gave a sample size of 138. Simple random sampling by ballot without replacement was used to select participants for the study. An estimated 80% (138) of the employees were therefore targeted in the five branches. Pregnant and lactating women were excluded from the study. The summary of the distribution of sample from different banks is given in .
Table 1: Distribution of sample from different branches of the bank
Dietary assessment
Information on food intake was collected using a three-day (two weekdays and one weekend) 24-hour recall method. This method requires an individual to remember the specific foods and amounts of food they consumed in the past 24 hours.Citation9 With this approach, subjects were asked to provide detailed information on all the foods and beverages consumed including cooking methods in the past 24 hours by a registered dietitian (the principal investigator) on three different occasions at the different branches of the bank. During the interview, food models, household measures (commonly used measuring tools in Ghana households) and photos of common dishes as well as household cups and measures were used to estimate amounts, in order to obtain accurate information regarding the types and quantities of foods and beverages consumed. Also, the usual food intake questions (such as types of food the respondents usually consume at each mealtime during the day) were asked to obtain information on the frequency of the foods reported in the 24-hour dietary recall including fruit and vegetable consumption. The usual food consumption question was designed in the form of 24-hour recall so that each participant's intake was cross-checked with the 24-hour recall reported by the respondents. The foods reported in the three-days24-hour recall was entered into Esha FPro software (ESHA, Salem, OR, USA). This software uses a food processor analysis tool to analyse menus, diets, foods and recipes. The software basically uses the United States Department of Agriculture (USDA) dietary database as reference, but for some foods that were local to Ghana not found in the Esha FPro software, the nutrient composition was added to Esha FPro software using a local food composition table for Ghana or Food and Agricultural Organization food composition table for use in West Africa as reference.Citation10,Citation11
Data and statistical analysis
Esha FPro software was used for dietary data analysis to determine the mean nutrient intake by each individual. Statistical analyses were performed using the Statistical Package for the Social Sciences (version 16, SPSS Inc, Chicago, IL, USA) software. Tabulations of frequencies (and percentages) and graphical presentations were done using SPSS® (version 16.0). For continuous variables, the data were checked for normality before analysis. An independent samples t-test was used to test the mean difference in nutrient intakes. A two-sample t-test for proportion was used to test the significant difference between proportions. All statistical tests were conducted as two-sided and declared significant at p-value < 0.05 or p < 0.01 respectively.
Ethics
The study protocol was reviewed and approved by the College of Health Sciences Ethical Review Board, University of Ghana (Ref. no. SAHS/10256520). All participants gave written informed consent and procedures were carried out according to the approved protocol.
Results
Nutrient intakes
Nutrient intakes were calculated from the three-day 24 hour recalls.
Macronutrient intake
There were no significant (p < 0.01) differences between mean intakes of protein, cholesterol and fat between genders. On the other hand, significantly higher intakes were observed in mean intakes of energy (p < 0.01), carbohydrate (p < 0.01), and dietary fibre (p < 0.01) in men compared with women. A summary of the findings of macronutrient intake is reported in .
Table 2: Mean daily intake of macronutrients
Micronutrient intake
lists the mean daily intake of micronutrients. There were no significant differences in the mean daily intake of sodium, calcium, magnesium, folate and vitamin C. However, mean iron intakes were significantly higher (p < 0.05) in men than in women.
Table 3: Mean daily intake of micronutrients
Comparison with population nutrient intake goals
(a, b, c) shows comparison of nutrient intake with population nutrient goals,Citation12 which are established recommended dietary intake with the aim of preventing or reducing the risk of diet-related chronic diseases such as CVD.
Table 4: Comparison with recommended dietary intake
Dietary sodium and potassium
Almost all the participants (99.2%) had a dietary sodium intake within recommended daily intakes (< 2 400 mg). However, dietary potassium intakes in all the participants were below recommended population nutrient goals (> 4 700 mg). These findings are presented in a.
Fruit and vegetable intake
The frequency of consumption of fruits and vegetables is presented in (a and b). In the total population, 78.2% (n = 93) of participants reported daily consumption of fruits. Of this number, 78.8% of males and 78.3% of females reported that they consumed about 1–2 servings of fruit per day. Participants who consumed an average of 3–4 servings per day were 15.2% and 18.3% for males and females, respectively.
Figure 1: (a) Distribution of fruit servings per day; (b) distribution of vegetable servings per day.
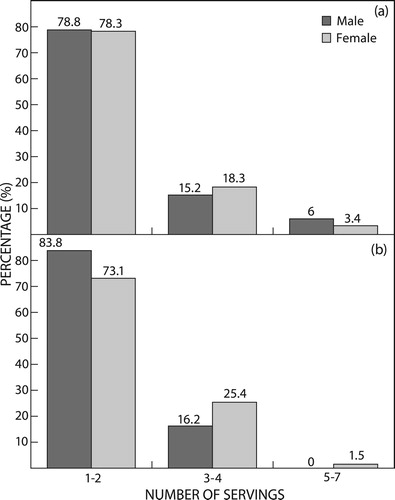
Similarly, most of the employees (76.9%; n = 80), comprising 83.3% males and 73.1% of females, consumed an average of 1–2 serving of vegetables per day (b). The average fruit intake per day for men was significantly higher (p < 0.05) than that for women, whereas average vegetable intake was significantly lower (p < 0.05) in men when compared with women. Overall, the majority of the study participants had low fruit and vegetable intakes (fruit intake, 89.9%; vegetable intake, 94%) and did not meet the recommended daily intakes of 4–5 servings a day. These findings are given in b.
Dietary fibre and cholesterol intakes
Mean dietary fibre intake of the total population was 22.2 g (men; 26.8 g, women; 19.5 g). The mean intake in the total population was below the recommended nutrient intake of 25–30 g/day. The majority of employees (89.9%; n = 107) had a dietary fibre intake below the minimum limit of 25 g per day. The mean intake for men was, however, within recommended intakes of dietary fibre per day. In the total group, mean dietary cholesterol intake (177 mg) was found to be less than 300 mg as recommended in the population nutrient goals. These findings are given in c.
Type of oil used
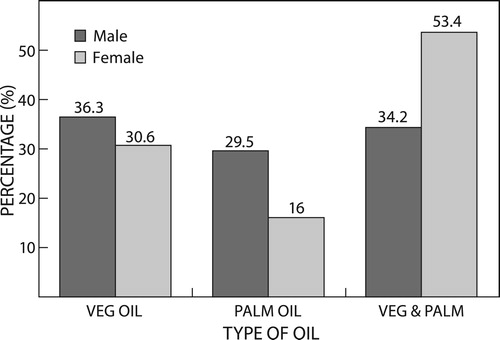
shows the type of oil most commonly used by the participants. The major cooking oils used in meal preparation were vegetable and palm oil 46% (53.4% females; 34.2% males), followed by vegetable oil 31.9% (36.3% males; 30.6% females) and palm oil 21.8%.
Figure 2: Most common type of oil used.
Discussion
The energy-giving food nutrients (carbohydrates, fats and proteins) evaluated in this study perform major functions in the body. A positive energy balance leads to overweight and obesity and thus contributes to the morbidity of cardiovascular diseases. Fat especially is being modified in CVD's as well as the total energy intake of individuals.Citation13 Findings of this study showed a significant difference in mean energy intake between males and females. The energy requirement for a male is higher due to higher metabolic rate and activity.Citation12 A review of the published literature shows that dietary changes differ according to the population group investigated.Citation7,Citation14,Citation15 Nevertheless, the percentage contribution of fat (men 31%, and women 32%) to the total energy in this study was similar to intakes among male (33%) and female (35%) Ghanaian migrants reported in Sydney, Australia.Citation14
In the prevention and control of diet-related chronic disease, it is recommended that an individual's nutrient intake should be within established recommended dietary intake levels.Citation5 According to the nutrient goals, fats, protein and carbohydrate consumption should contribute 15–30%, 10–15% and 55–75% of the total calories per day respectively. The findings of this study shows that the bank employees were consuming more fat (32%) compared with the WHO's recommendation of 15–30% nutrient goals for good health.Citation5 In the DASH guideline, it is recommended that fat should not exceed 27% of total energy intake per day.Citation12 A high fat intake has detrimental effects on health.Citation12 Clinical trials have provided evidence suggesting that reduction or modification of dietary fat intake reduces the incidence of combined cardiovascular events by 16% (rate ratio 0.84; 95% CI 0.72 to 0.99).Citation15 Other studies have also shown that higher fat intakes modify the body’s metabolism in ways that favour fat accumulation.Citation16,Citation17 It has been reported that altered diets coupled with diminished physical activity are critical factors contributing to the acceleration of CVD epidemics.Citation18
Dietary cholesterol intakes between men and women in this study were not significantly different. Generally, the mean intakes were within the recommended daily intake of < 300 mg a day.Citation4,Citation5 The effect of diet on serum lipids and lipoproteins has been studied extensively in various clinical and epidemiological trials. Although the dietary content is clearly an important determinant, several environmental and metabolic factors intervene to modulate the dietary effect.Citation6 However, recent studies indicate that excessive dietary carbohydrate intake, especially simple sugars, can promote atherogenic dyslipidaemia.Citation19 In the NHANES III study, higher intakes of carbohydrates were found to be positively associated with serum triglycerides and negatively associated with serum HDL-cholesterol.Citation20
The micronutrients analysed in this study are essential components of the Dietary Approaches to Stop Hypertension (DASH) diet.Citation12 These micronutrients are also modified in CVDs, especially sodium, potassium, magnesium and calcium.Citation12 Hypertension is one of the most common CVDs in Ghana.Citation14 It could precipitate other cardiovascular diseases as well as renal disease.Citation12
Consumption of dietary iron among the respondents was significantly higher in males than in females. However, both genders’ intake of iron was higher than the recommended dietary intake but did not exceed the upper adult tolerable level of 45 mg/day.Citation12 This could be attributed to the consumption of meat, fish and poultry, which are rich in iron.Citation12 Adequate dietary iron intake will ensure prevention of anaemia and boosts the immune system.Citation12
Micronutrients such as excess intake of sodium and low potassium intake are strongly related to the risk of developing CVD.Citation12 Findings of the study showed that the mean intake of dietary sodium (773 mg) of all the bank employees was within the recommended intake (< 2 400 mg). Dietary sodium has long been labelled as a dietary factor in the pathogenesis of high blood pressure.Citation21 Sodium is positively associated with blood pressure, therefore the mean intake found in this study is favourable for health.Citation12 However, these results should be interpreted with caution since the dietary assessment method of estimating sodium intake is less reliable as it may be associated with misreporting and some people cook with different levels of salt. The software used in analysing the nutrient composition did not make use of foods cooked in Ghana. Therefore a 24-hour urinary sodium excretion test is a better measure for assessing dietary sodium.Citation22 The 24-hour urinary sodium excretion test was not within the scope of this study.
All the participants in the study had a dietary potassium intake (841 mg) below the recommended intake of 4 700 mg of dietary potassium per day. This may partly be due to the low intake of fruits and vegetables among the bank employees. Fruits and vegetables affect cardiovascular risk through their high potassium levels that serve to modulate blood pressure.Citation23 Potassium has a negative association with blood pressure.Citation24,Citation25 Therefore low intakes of dietary potassium may predispose to the high prevalence of hypertension.
The majority of the bank employees had a daily intake of fruits and vegetables below the daily recommended intakes of 4–5 servings a day for each, respectively, in the dietary approaches to stop hypertension.Citation4,Citation12 The recommendation for fruits and vegetables was for individuals to eat at least three servings of fruit and at least four servings of vegetables each day for adults.Citation26 Making a choice from fresh, frozen, dried or canned forms and a variety of colours and kinds is encouraged. Also, intake of dark-green leafy vegetables, orange fruits and vegetables, and cooked dry beans and peas is often recommended.Citation26 It is established that fruits and vegetables contain many nutrients such as minerals, vitamins, fibre and antioxidants, which may individually or in combination provide a protective effect against CVD.Citation27 An epidemiological study has shown that intakes of fruits and vegetables more than three times or three servings a day compared with one serving a day was significantly associated with a 27% lower incidence of stroke (p < 0.01) and 48% lower stroke mortality (p < 0.05).Citation28 This suggests a strong inverse association between fruit and vegetable intake and the risk of subsequent CVD.Citation28 Therefore low consumption of fruits and vegetables among the bank employees in this study could increase their risk of developing morbidity associated with CVD.
The suggested dietary intake (RDI) of fibre was based on WHO/FAOCitation5 and American Heart Association recommendations.Citation4 The mean dietary fibre intake of men in this present study was significantly higher when compared with the mean intake of women. This may be attributed to the higher food requirements of men to meet their energy needs in addition to their higher consumption of servings of fruits per day. Also, in Ghana, most of the diets are based on cereals and whole grains, which are also a good source of fibre. Dietary fibre intake has been consistently associated with a lower risk of CVD.Citation29 In the dietary guidelines, a daily intake of 25–30 g of dietary fibre was recommended to prevent diet-related diseases such as CVD.Citation4,Citation5 It was found that the majority of the bank employees (89.5%) had dietary intakes below the recommended level (25–30 g). Studies have reported that high dietary fibre intake helps to maintain a lower total body fat as it is inversely associated with body mass index (BMI) and waist–hip ratio (WHR)Citation30 and also helps to decrease serum total and low-density lipoprotein cholesterol concentrations.Citation31
Oils are a good and cheap source of fats in our meals. In Ghana, the cheapest source of Vitamin A is palm oil.Citation10,Citation11 Most of the vegetable oils in Ghanaian markets are made from different seeds such as safflower seeds, sunflower seeds or groundnuts, while some are made from palm olein. The oils from tree seeds are a rich source of monounsaturated fatty acids and essential fatty acids which confer cardioprotective effects.Citation4,Citation12 Omega-3 fatty acids provide a cardioprotective effect by reducing the LDL cholesterol and increasing the HDL cholesterol.Citation12 Vitamin A, found in palm oil, boosts the immune system and prevents the incidence of blindness that results from Vitamin A deficiency.Citation12 Oils, however, provide concentrated energy in the form of fats, thus excess consumption of fats could predispose an individual to fat accumulation, dyslipidaemia, obesity and consequently CVDs.Citation12 The fat intake of the bank employees in this study exceeded the recommended levels in the Dietary Approaches to Stop Hypertension.Citation12 It is important to note that oils in the food are the major contributor of fats in Ghanaian dishes.
Conclusion
The study concluded from the dietary assessment of bank employees in Accra that fat intake exceeded the DASH recommendation for dietary fat. Citation12 However, dietary cholesterol intake was within the accepted levels. The majority of the employees had dietary intakes below the recommendation in the DASH guideline.Citation12 It was also established that fruit and vegetable consumption, which provides a protective effect against CVD risk factors, was inadequate. All the participants had a low dietary potassium intake. Findings of the study thus demonstrates the need to develop plans for regular nutrition education to bank employees to ensure a healthy workforce for national development. A more in-depth study using a weighed food intake among the employees in Accra is recommended.
Limitation of study
The software ESHAFPro used in analysing the nutrient intake of the respondents was based on food composition tables for use in the United States, thus the nutrients measured could be below or above the values generated in this study. However, this provided a good insight into the nutrient intakes of bank employees in Ghana. Some of the selected respondents declined consent, which reduced the sample size of the study. The use of 24-hour recall is not exhaustive in the determination of nutrient intake because it relies on memory, therefore conducting a weighed food intake study will supplement the method used. However, because of the busy life of the group of respondents, weighed food intake measurement was not possible. To determine the actual nutrient composition of foods in Accra, a nutrient analysis is required because there is no single recipe for foods consumed in Ghana; different households and restaurants have their individual recipes. However, the budget of the study could not support analysing all the foods identified in the study. Nonetheless, the software ESHA FPro used in the study is a reliable tool that has been used in other studies both in Ghana and developed countries.
Ethics approval and consent to participate
The study was approved by the Ethical Review Board of the School of Allied Health Sciences (ref SAHS/10256520). Prior to initiating the protocols of the study, potential risks were discussed with the Human Resource Manager of the bank. All participants gave written informed consent and procedures were carried out according to the approved protocol.
Competing interests
The authors declare that they have no competing interests
Acknowledgements
The authors would like to thank all the participants who consented to be part of the study, as well as all the research assistants who helped with the data collection and analysis.
ORCID
Matilda Asante http://orcid.org/0000-0003-3488-7087
Aloysius Nwabugo Maduforo http://orcid.org/0000-0001-7290-5632
Additional information
Funding
References
- WHO. Cardiovascular diseases. 2007. Fact sheet No 317.
- Yusuf S, Hawhen S, Ounpuu S, et al. On behalf of the INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART Study): case-control study. Lancet. 2004;364:937–52. doi: 10.1016/S0140-6736(04)17018-9
- Kruger HS, Venter CS, Vorster HH, et al. Physical inactivity is the major determinant of obesity in black women in the North West Province, South Africa: the THUSA study. Nutrition. 2002;18:422–7. doi: 10.1016/S0899-9007(01)00751-1
- Lichtenstein AH. Diet and lifestyle recommendations revision 2006: A scientific statement from the American Heart Association Nutrition Committee. Circulation. 2006;114:82–96. doi: 10.1161/CIRCULATIONAHA.106.176158
- World Health Organization/Food and Agricultural Organization. Diet, Nutrition and the Prevention of Chronic Diseases. Report of a Joint WHO/FAO Expert Consultation. Geneva: WHO, 2003.WHO Technical Report series 916.
- Joshipura KJ, Hu FB, Manson JE, et al. The effect of fruit and vegetable intake on risk for coronary heart disease. Ann Intern Med. 2001;134:1106–14. doi: 10.7326/0003-4819-134-12-200106190-00010
- Alves-Rodrigues A, Thomas B. Fruit and vegetable intake and coronary heart disease. Ann Intern Med. 2002;137(2):143. doi: 10.7326/0003-4819-137-2-200207160-00019
- Sarkar AK, Adak SK, Bhattacharya P, et al. Risk assessment of cardiovascular disease among bank employee – a biochemical approach. Occup Med. 1999;49:313–18. doi: 10.1093/occmed/49.5.313
- Hammond K. Assessment: dietary and clinical data. In: Mahan LK, Escott-Stump S, editors. Krause’s food and nutrition therapy. 12th ed. New York: Saunders Elsevier Inc.; 2008. pp. 397.
- Eyeson KK, Ankrah EK, Sundararajan AR, et al. Composition of foods commonly used in Ghana. Council for and Industrial Research (CSIR). Accra: CSIR Food Research Institute Ghana; 1975.
- Food and Agriculture Organization of The United Nations. West African food composition table. Rome, Italy: FAO Publication; 2012.
- Nelms MN, Sucher K, Lacey K, et al. Nutrition therapy and pathophysiology. 2nd ed. Belmont, CA: Wadsworth, Cengage Learning; 2011.
- Food and Agriculture Organization. Fats and fatty acids in human nutrition report of an expert consultation. Rome: Food and Agriculture Organization of The United Nations, 2010.
- Saleh A, Amanatidis S, Samman S. Cross-sectional study of diet and risk factors for metabolic diseases in a Ghanaian population in Sydney, Australia. Asia Pac J Clin Nutr. 2002;11:210–16. doi: 10.1046/j.1440-6047.2002.00293.x
- Hooper L, Summerbell CD, Higgins JPT, , et al. Dietary fat intake and prevention of cardiovascular disease: systemic review. BMJ. 2001;322:757–68. doi: 10.1136/bmj.322.7289.757
- Adult Treatment Panel III: Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Final Report), September 2002. NIH Publication No 02-5215.
- Astrup A, Toubro S, Raben A, et al. The role of low-fat diets and fat substitutes in body weight management: what have we learned from clinical studies? J Am Diet Assoc. 1997;97: S82–7. doi: 10.1016/S0002-8223(97)00737-2
- Reddy KS. Cardiovascular diseases in the developing countries: dimensions, determinants, dynamics, and directions for public health action. Public Health Nutr. 2002;2:231–7. doi: 10.1079/PHN2001298
- Lairon D, Arnault N, Bertrais S, et al. Dietary fibre intake and risk factors for cardiovascular disease in French adults. Am J Clin Nutr. 2005;82:1185–94. doi: 10.1093/ajcn/82.6.1185
- Castro TG, Gimeno SGA, Ferreira G, et al. Association of dietary fiber with temporal changes in serum cholesterol in Japanese-Brazilians. J Nutr Sci Vitaminol. 2006;52:205–10. doi: 10.3177/jnsv.52.205
- McCarron DA. Dietary sodium and cardiovascular and renal disease risk factors: dark horses or phantom entry? Nephol Dial Transport. 2008;23:2133–7. doi: 10.1093/ndt/gfn312
- El-Bokl MA, Senousy BE, El-Karmouty KZ, et al. Spot urinary sodium for assessing dietary sodium restriction in cirrhotic ascites. World J Gastroenterol. 2009;15:3631–5. doi: 10.3748/wjg.15.3631
- Lock K, Pomerleau J, Causer L, et al. Low fruit and vegetable consumption. In: Ezzati M, Lopez AD, Rodgers A, Murray CJL, editors. Comparative quantification of health risks: Global and regional burden of disease attributable to selected major risk factors. Geneva: World Health Organization, 2004: 597–728.
- INTERSALT: The INTERSALT Study. An International co-operative study of electrolyte excretion and blood pressure: further results. J Hum Hypertens. 1989;3:279–407.
- Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336:1117–24. doi: 10.1056/NEJM199704173361601
- U.S. Department of Agriculture, Centre for Nutrition Policy and Promotion. The food guide pyramid. Home and Garden Bulletin. 1996;253. Retrieved from https://health.gov/dietaryguidelines/dga2000/document/build.htm
- Schneider M, Norman R, Steyn N, et al. Estimating the burden of disease attributable to low fruit and vegetable intake in South Africa in 2000. S Afr Med J. 2007;97:717–23.
- Bazzarro LA, Larraire JH, Ogden LG, et al. Fruit and vegetable intake and risk of cardiovascular disease in US adults: the first National Health and Nutrition Examination Survey. Epidemiologic Follow-up study. Am J Clin Nutr. 2002;76:93–9. doi: 10.1093/ajcn/76.1.93
- Kocaoglu B, Moschonis G, Dimitriou M, et al. Parental educational level and cardiovascular disease risk factors in school children in large urban areas of Turkey: directions for public health policy. BMC Public Health. 2005;5:1087 doi: 10.1186/1471-2458-5-13
- Krauss RM, Blanche PJ, Rawlings RS, et al. Separate effects of reduced carbohydrate intake and weight loss on atherogenic dyslipidemia1–3. Am J Clin Nutr. 2006;83:1025–31. doi: 10.1093/ajcn/83.5.1025
- Yang EJ, Chung HK, Kim WY, et al. Carbohydrate intake is associated with diet quality and risk factors for cardiovascular disease in U.S. adults: NHANES III. J Am Coll Nutr. 2003;22:71–9. doi: 10.1080/07315724.2003.10719278