
Abstract
Objectives:
This study was undertaken to identify stakeholder needs and wants in relation to an Infant and Young Child Feeding, Social and Behaviour Change Communication (SBCC) strategy for the 16 Southern African Development Community (SADC) member states during Covid-19 lockdowns and travel restrictions.
Design:
A rapid-assessment mixed-methods approach using qualitative and quantitative studies was adopted. Secondary data sources supported in-field findings.
Setting/Subjects: Qualitative approaches included 17 key informant interviews from 7 SADC member states. Quantitative methods of an online survey elicited feedback from 61 participants from 11 SADC member states.
Outcome measures: More strategic, best practice, infant and young child feeding SBCC programmes are recommended in SADC.
Results:
Programme challenges included increased demands on health systems from Covid-19, poor attitudes and beliefs toward IYCF behaviours, the dual burden of undernutrition and overnutrition, and financial and human resource capacity challenges to implement and evaluate SBCC campaigns at scale. Opportunities were also identified for improved detection, better meeting IYCF nutritional needs from locally sourced foods, training and capacity building for greater engagement of front-line field staff, effective policy development to support parent-friendly hospitals and workplaces, and improved regional integration.
Conclusions:
The needs assessment demonstrated that priority programme planning can continue while the health sector deals with a pandemic threat. The adaptation to virtual support provided a variety of learnings for research designs, data collection and analysis, albeit over an extended timeframe of six months. A number of innovative approaches were identified in the resultant SBCC strategy for SADC along with opportunities for regional efficiencies in adapting existing, best practice SBCC creative and programming approaches.
Introduction
Global estimates identify 47 million children under 5 being wasted in 2019, of whom 14.3 million were severely wasted with 144 million being stunted.Citation1 Around 45% of deaths among children under 5 years of age are linked to undernutrition, which mostly occurs in low- and middle-income countries (LMICs).Citation2 Child stunting and other forms of malnutrition are associated with lower dietary diversity, with food insecurity and poor household food choices contributing to the lack in meeting children’s nutrient requirements.Citation2,Citation3 Additionally, malnutrition is seen to occur predominantly in regional hotspots where there is limited access to high-protein foods, poor vegetation cover and low rainfall or drought.Citation4 UNICEF reports that in nearly every part of the world families face economic, political, market, social or cultural barriers to providing nutritious, safe, affordable and sustainable diets to young children.Citation5–7 Socioeconomic determinants in many countries play a significant role in food insecurity and diversity of food choices, which lead to childhood and maternal malnutrition.Citation8
The Southern African Development Community (SADC) is a regional economic development community comprising 16 member states in the southern African and Indian Ocean region. These are Angola, Botswana, Comoros, Democratic Republic of Congo, Eswatini, Lesotho, Madagascar, Malawi, Mauritius, Mozambique, Namibia, Seychelles, South Africa, United Republic of Tanzania, Zambia and Zimbabwe. SADC’s overall goal is to promote and achieve equitable and sustainable development through increased regional integration. The 16 SADC member states in the southern African region are also seen as having a responsibility to support nutritional initiatives given the multi-layered influences that impact on food choices, with government policies, priorities and assistance programmes operating at an individual level, while sociocultural, community, environmental, agricultural, industry and market influences are also seen as impacting on healthier nutritional behaviours.Citation9 These challenges are exacerbated in humanitarian situations in the poorest and most fragile economies where access to nutritious food, clean drinking water and good quality health services is limited, and the resources and capacities of caregivers are already stretched.
Young children and their caregivers in the region are seen to be increasingly exposed to foods of low nutritive value, including commercial complementary foods and processed foods high in added sugar, salt and saturated fats and trans fats, due to their low cost, ubiquity and the ease of feeding to young children.Citation3 Thus, the developmental, economic, social and health impacts of the burden of malnutrition are serious, with acute malnutrition remaining stubbornly high across the region with rates of 2–8.1%.Citation10 With the added impact of COVID-19, acute malnutrition —stunting, wasting or overweight—across the region was predicted to increase by 25% or more by 2021.Citation10
Given the considerable challenges, SADC, with funding from European Union and support of the Global Alliance for Improved Nutrition (GAIN) and UNICEF, is developing a Social and Behavioural Change Communication (SBCC) Strategy for Improved Infant and Young Child Feeding (IYCF). SBCC for nutrition is a set of interventions that systematically combines elements of interpersonal communication (IPC), social change and community mobilisation activities, mass media and advocacy to support individuals, families, communities, institutions and countries in adopting and maintaining high-impact nutrition-specific and nutrition-sensitive behaviours or practices.Citation11 To inform the design of the SBCC strategy a needs assessment was undertaken.
Study design
The initial stage of formative research included a literature review to identify the scale of the problem and inform the development of a discussion agenda for consultations with key informants to follow. The elicitation research was designed to gather information from key stakeholders from SADC member states who were essentially the clients for the strategy design as well as to explore key issues for future formative research with programme beneficiaries. The next stage of the study comprised semi-structured interviews (SSIs), acknowledging the busy professional standing of respondents. Given travel restrictions imposed soon after project inception, interviews were arranged through online conference calls with researchers participating at various times from locations in Sydney, Australia; Gaborone, Botswana; Philadelphia, USA; and Geneva, Switzerland.
The methodological guidelines for the needs assessment included selection of Tier 1–2 SADC countries identified by their current capacity to implement nutrition programmes addressing IYCF and those that had conducted landscape analysis on complementary feeding. Nutrition representatives were interviewed on their needs and wants from the seven member states of Botswana, Malawi, Mozambique, South Africa, Tanzania, Zambia and Zimbabwe.
A standardised discussion agenda was developed to address key issues identified from the literature review with a number of items derived for the discussions emanating from the predominant classical and novel behavioural theories. These included constructs to identify problem behaviours and build risk perceptionsCitation12 to set the programme agenda and support the need to address malnutrition, while accepting that in vulnerable groups risk appraisal may be weighed against coping appraisals before making adaptive or maladaptive responses. Beneficiary capabilityCitation13 was also considered, emphasising the importance of modelling desired behaviours,Citation14 while accounting for existing social norms,Citation15 and building self-efficacyCitation16—skills, confidence and perceived behavioural control,Citation17 which are key drivers in influencing attitudes and intentions toward nutrition behaviours. Other considerations included the importance of identifying opinion leaders and key influencers for the diffusion of IYCF nutrition innovationsCitation18 and adoption of practices by other community members that may challenge existing cultural or social norms. Additionally, identification of where most participants may be located on the behaviour change continuumCitation19 was a consideration. This is based on the understanding that change often takes time, and people may go through a number of ‘stages-of-change’ before eventually changing previously entrenched behaviours.Citation20 Last was an investigation of factors related to motivating and mobilising participants and communities, acknowledging the added value to SBCC initiatives in providing positive incentives to motivate or ‘nudge’ participants toward the desired changes.Citation21
Given the challenges in developing an SBCC strategy during a pandemic lockdown, the potential for quantitative data to support qualitative approaches was explored. An online survey tool was developed: the Southern African Development Community (SADC) Infant and Young Child Feeding (IYCF) Media Audit for a SBCC strategy, to provide more specific empirical findings on SBCC strategy implementation, evaluation and advocacy approaches.
The online survey tool, which was reviewed for ethics clearance by SADC/GAIN management prior to administration, contained 32 items including the stakeholder title and organisation, their country of operation, the scale, number and nature of existing IYCF programmes and materials developed, M&E frameworks, programme partners, and attitudes and opinions regarding their country priority for IYCF nutrition programmes and HR capacity and funding expectations. Other items with five-point scales examined opportunities for provision of easily adaptable SBCC campaign resources and online tools available through a web portal to achieve greater economies of scale and engagement in SBCC approaches. Finally, a media audit requested links to existing resources and inclusion on a future mailing list for advocacy of approaches.
Study participants
Participants for the SSIs included 17 nutrition stakeholders, consultants and representative from international NGOs, civil society and the private sector in the region, while 61 participants from 11 SADC member states responded to the online survey, with an additional 2 participants from other African countries—Kenya and Uganda—also responding to the online survey.
Data collection
The study tools and instruments were designed to provide a consistent range of indicators to inform the SBCC strategy design. Discussion agendas for stakeholders and beneficiaries were designed to elicit responses to a number of key performance indicators, including awareness of existing programmes, knowledge and attitudes towards diet, physical activity and chronic diseases, perceptions of body image and food consumption patterns, motivation, capability, perceptions, intentions and behaviours. As well as assessing the behavioural determinants of malnutrition,Citation22 exploration was also conducted of social determinantsCitation23 related to income, access to services and media channels. All groups were conducted in the English language. In instances where participants’ predominant language was French or Portuguese, the calls were supported with translators provided by the SADC member state’s nutrition stakeholders.
Field notes of stakeholder interviews were compiled in single-spaced Word-format transcripts (IBM Corp, Armonk, NY, USA) using a question-by-question format to capture accurately what respondents had to say regarding each topic. Although recordings of interviews were made using digital online conference tools, the approach to compiling the dataset was in line with RAR approaches designed to accumulate evidence rapidly in resource-constrained settings, where mission times may be short or there may be other challenges. As such, given adequate moderation and typing skills, transcripts of each interview were usually completed by the conclusion of the interview. In cases where there was some ambiguity on what was said during data cleaning, missed information was inserted following review of the audio recordings. Secondary sources reviewed to supplement the fieldwork included a number of National and Regional NCD strategy documents and landmark reports from the predominant donors UNICEF, GAIN, the World Bank and the WHO. International peer-reviewed literature and UN reports were also reviewed as were predominant behavioural theories to support the design of the formative research instruments, tools and creative approaches.
Analysis
The analysis was conducted in two iterative stages to build theory from the data. An examination of SSIs with key informants was first conducted to explore patterns identified across individual and group cases.Citation24 Much of the investigative approach has emanated from ‘Grounded Theory’, where constant comparative methods are used to define and separate themes through continuous reading of the raw dataCitation25 in a systematic way from the perspective of those experiencing the phenomena.Citation26 The within-case analysis involved identifying and summarising key issues emanating from discussions across stakeholder and beneficiary cases, while the second step involved individually analysing responses from each of the cases.Citation27 Notes on the key issues and cases were then compiled, followed by cross-case analysis. Qualitative findings (n = 17) were triangulated with quantitative findings from the online survey (n = 63) and secondary data sources to provide a comprehensive overview of knowledge, attitudes and beliefs regarding SBCC strategic approaches in SADC, to better inform the design and evaluation of strategy.
Results
The literature identifies that along with inadequate care and feeding practices, household food insecurity, unhealthy household environments and inadequate health services are all behaviour-related problemsCitation4 with the need for more rigorous formative research to understand the optimal dietary patterns to tackle the challenges of maternal health, child development, infection risk and non-communicable diseases.Citation28
In terms of identifying regional priorities, the SADC 16-member state profiles identify considerable variance in country development status,Citation29 culture—72 language groups were identified across the regionCitation30—differences in literacy, educational attainment,Citation31 GDP income and growth factors.Citation32 Five SADC member states are identified as upper middle-income countries, i.e. Botswana, Mauritius, Namibia, Seychelles, South Africa, while another six are designated as lower-middle income countries, i.e. Angola, Eswatini, Lesotho, United Republic of Tanzania, Zambia and Zimbabwe. Five SADC member states, i.e. Comoros, Democratic Republic of Congo, Madagascar, Malawi and Mozambique, are designated as having low-income status.Citation33
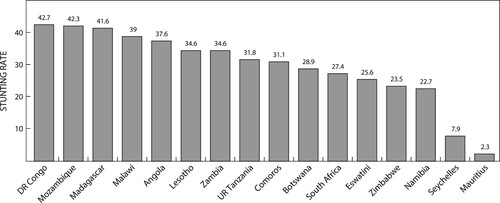
The variance in development indicators and IYCF country risk profiles also confirms the considerable differences (> 20% variance) in stunting prevalence between the lowest and highest income countries where children are not growing well.Citation16 Recent SADC country dataCitation10 identify a high prevalence of stunting in children (22–29%) occurring in Namibia, Zimbabwe, Estwatini (Swaziland), South Africa and Botswana, with very high stunting prevalence (31–43%) in Comoros, United Republic of Tanzania, Lesotho, Zambia, Angola, Malawi, Mozambique and Democratic Republic of Congo (see ), with wasting prevalence in the region ranging from 2% to 7%.Citation21
Figure 1: SADC member state stunting rates: Very Low < 2.5%; Low 2.5 < 10%; Medium 10% < 20%; High 20% < 30%; Very High ≥ 30%. Data provided courtesy of SADC Synthesis Report on the State of Food and Nutrition Security in the Region.
GAIN reviews on access to complementary foods in a number of regional country settings have also identified considerable differences in dietary nutrient gaps among children aged 6–23 months and priority affordable complementary foods to meet dietary nutrient gaps. The dietary recommendations also often differ by country settings, such as: Mozambique (eggs), Zambia (dairy), South Africa (highly fortified maize porridge), and Tanzania (poultry). The foods selected in each country meet at least one important nutrient gap and their promotion aligns with government priorities and local preferences.Citation34 Minimum Dietary Diversity (MDD) is another regional indicator demonstrating the considerable disparities in country capacity to meet the dietary needs of children. Furthermore, relatively few children in SADC member states aged 6–23 months eat at least 5 of 8 food groups to achieve MDD, with low-MDD countries (17–18%) including Lesotho and Zambia, mid-range MDD regional countries (21–28%) including Tanzania, Namibia, Lesotho and Malawi, while countries with greater dietary diversity (29–48%) include Angola, South Africa and Eswatini.Citation21
The literature also points to a number of other behaviour-related, institutional, technical capacity and cultural challenges,Citation35 as well as identifying behaviours that can improve nutrition outcomes.Citation36 Behavioural factors for SBCC include the complex range of IYCF recommendations related to breastfeeding, complementary feeding, infant feeding in the context of HIV/AIDS and feeding children with special needs.Citation37 Coupled with the scarcity of resources to incentivize women and their family members to actively engage in the SBCC programmes, these impediments will require highly creative and innovative solutions to achieve the project aims and behavioural objectives within a regional strategy design.
Covid-19
Covid-19 is not the first, nor will it be the last pandemic to ravage Africa and other regions of the world. SADC member states have suffered and continue to battle with serious pandemic threats and country epidemics of HIV/AIDS, drug- resistant TB and malaria, which are all major contributors to nutrition-related comorbidities. The evidence to date indicates that Covid-19 and other epidemics will also significantly hamper any nutritional gains made in the past decade through job and income loss, in populations most at risk of malnutrition.Citation38 Challenges are exacerbated by the redirection of critical health and infrastructure resources from priority health areas of prevention and control, within already stretched health systems.
Behavioural challenges and opportunities
The needs assessment and literature review identified a number of SBCC programme milestones and achievements, but also ongoing challenges and opportunities for continuous improvement of the strategy and regional synergies. Programme challenges included the additional demands on health systems and human resources from pandemic threats such as Covid-19, poor attitudes and beliefs toward IYCF behaviours by some programme beneficiaries, additional challenges from the burden of undernutrition, the rapidly emerging burden of overnutrition and overweight, and financial resource capacity challenges to implement and evaluate SBCC campaigns at scale (see ).
Table 1: Nutrition strategy challenges identified from stakeholder feedback
Opportunities for the SBCC strategy were also identified by member state nutrition stakeholders. These included opportunities for SBCC to lead to improved early detection for wasting, better meeting IYCF nutritional needs from locally sourced, inexpensive nutrient-dense foods, training and capacity building of front-line field staff and other stakeholders, which could be engaged in the process, the inclusion of men in SBCC activities, given their role in supporting better IYCF behaviours, effective policy development to support parent-friendly hospitals and workplaces, and improved regional integration (see ).
Table 2: Nutrition strategy opportunities identified from stakeholder feedback
Findings from the quantitative survey identified that 63 participants had responded to the survey with 61 participants from 11 SADC member states. The majority came from the United Republic of Tanzania (32.69%; n = 17); while Mozambique (25.00%; n = 13), South Africa (13.46%; n = 7) and Madagascar (13.46%; n = 7), also attracted a moderate number of participants. Malawi (7.69%; n = 4), Zambia (7.69%; n = 4); Zimbabwe (7.69%; n = 4), Lesotho (3.85%; n = 2), Botswana (1.92%; n = 1), Comoros (1.92%; n = 1) and the Seychelles (1.92%; n = 1) attracted four or fewer participants, while other African country representatives from Kenya and Uganda (3.85%; n = 2) also participated in the online survey.
Of the participants who provided their organisation details, the majority of participants represented government agencies (34.55%; n = 19), while other participants including UN agencies (29.09%; n = 16), international NGOs (18.18%; n = 10), university or other academic institution representatives (12.73%; n = 7), national NGO or civil society organisations (5.45%; n = 3). One private sector organisation (Creative or Media Agency) representative also participated. Most of the participants identified that their country already had a nutrition strategy that included IYCF (54.72%; n = 29) and media materials or had implemented behaviour change programmes for IYCF in the past 3 years (84.31%; n = 43), with a broad range of themes covered including Breastfeeding (97.67%; n = 42); Early introduction of Breastfeeding First Hour (81.40%, n = 35); Exclusive Breastfeeding 0–5 Months (93.02%; n = 40); Continued Breastfeeding through 2 Years (90.70%; n = 39); Complementary Feeding (93.02%; n = 40); Introducing Food at 6 Months (90.70%; n = 39); and Diversified Diets (at least 5 Food Groups/Day—86.05%; n = 37). SBCC resources for IYCF mainly focused on Community Health Workers/Mother’s Groups or Other Interpersonal Communication (86.05%; n = 37) and Health Worker Training (76.74%; n = 33); while Posters (69.77%; n = 30); Billboards/Other Outdoor Media (23.26%; n = 10); Flip Charts or other Aids (62.79%; n = 27); Radio Spots (81.40%; n = 35); TV Spots/Programmes (58.14%; n = 25); Social Media/SMS/Digital Media (62.79%; n = 27) were also popular options. The majority of respondents (60.53%; n = 23) reported from 1 to 3 campaigns had been implemented in their countries of operation, from less than 2 weeks’ duration (16.67%; n = 6) to more than 12 months’ duration (30.56%; n = 11). Only 35.14% (n = 13) of participants reported a routine monitoring system, while 21.05% (n = 8) reported impact evaluations conducted on specific SBCC nutrition campaigns or other interventions.
A number of items relating to SBCC campaign indicators, online tools and resources were rated on five-point Likert scales. Two ‘top-box’ findings identified that an online dashboard tool comparing major IYCF indicators across the region was seen as very/extremely useful by 73.68% (n = 22) participants; an interactive interface that walks users through the decisions and steps in developing an IYCF campaign strategy was seen as very/extremely useful by 91.90% (n = 34) participants; an indicative media plan to account for different sized budgets was seen as very/extremely useful by 83.34% (n = 30) participants; sample messages and creative concepts that can be adapted were seen as very/extremely useful by 88.88% (n = 32) participants, while sample management tools such as budget templates, creative briefs or workplans were seen as very/extremely useful by 94.59% (n = 35) participants; and A monitoring & evaluation framework with key indicators and sample data collection tools was seen as very/extremely useful by 94.59% (n = 35) participants (see ).
Table 3: SADC stakeholder online survey findings (5-point Likert scales) on usefulness of SBCC components on IYCF web portal (n = 63)
Discussion
The needs assessment implemented during the height of the Covid-19 pandemic demonstrates that priority nutrition programme strategic planning can continue while the health sector deals with other global health priorities. The adaptation to virtual support by international advisers and donors located in multi-country settings, working in conjunction with national staff, provided a variety of learnings. This included the potential for technical capacity building, and data collection and analysis, efficiently conducted through virtual support, albeit over an extended time-frame of six months.
The approach also demonstrated that a greater amount of programme intelligence may be able to be collected in formative research implemented during these periods, given the predilection of stakeholders to rapidly adapt to online platforms for communication in the face of travel restrictions and lockdowns keeping staff at home during the pandemic. The needs assessment allowed for qualitative dialogue on key aspects of the SBCC strategy, while also providing indicators on regional stakeholder needs and wants. Triangulation of feedback from the literature review, key informant interviews and quantitative data sources from the online survey provided a comprehensive overview of the programme gaps and challenges, as well as opportunities for continuous improvement and integration.
Recommendations from the SBCC strategy developed from the needs assessment findings confirms that programmers do not have to ‘reinvent the wheel’ with strategic approaches and IYCF messaging.Citation39 There are a number of efficiencies in simply reviewing best-practice communication campaigns and brands from other parts of the world and ‘culturally adapting’ for regional approaches. Recommendations for increased efficiencies achieved through regional integration are also apparent with enquiry on online survey tools and approaches being very positively received in the SADC (16 member states), with these efficiencies also being explored by the WHO, in the Eastern Mediterranean Region (22 member states).Citation40
Furthermore, findings from the needs assessment identified the considerable challenges in reversing the worrying trends in malnutrition in the region, which are expected to rise with challenges faced by the pandemic. Opportunities are identified in the strategy for the development of best-practice SBCC campaigns to achieve population-level impact, adapting and evaluating the SBCC campaigns for their efficacy in a number of member states, while building technical capacity and political will to adapt resources and implement programme interventions at scale.
A key recommendation towards achieving greater regional integration is to identify and implement policy initiatives that will facilitate the dissemination of critical campaign messages to achieve effective reach and frequency at scale, such as those in Turkey,Citation41 which can highlight that sustainable mass media programming mechanisms can also be successfully enacted in SADC to support dissemination of IYCF and other priority health programmes. This can be facilitated through the establishment of a priority health programming calendar, which can be institutionalised across a number of SADC regional member states. Innovation is also identified in the strategy as a key factor in supporting new and different ways of approaching challenges as well as the sharing of lessons learned across the region.
Lastly, a critical factor to the success of a regional SBCC strategy to address IYCF problem behaviours is the need to seek endorsement and support from key donors and support agencies in the region, for the full term of the strategy. This will allow for capacity building, implementation and evaluation of a number of communication campaigns, and the application of findings to address behavioural gaps in future phases of the strategy. It is only through the adoption of more integrated, evidence-based, long-term, strategic approaches, which have the potential for regional application, that policy initiatives and other SBCC interventions can achieve behavioural impact and other efficiencies. Coupled with the SBCC programming efficiencies are opportunities to advocate for a greater level of regional programming sustainability, afforded through fiscal policy measures applied to a range of unhealthy products that are currently increasing NCD risk in the African region.
Conclusion
The needs assessment demonstrated that priority programme planning can continue while the health sector deals with a pandemic threat like Covid-19 and other health emergencies. The adaptation to virtual support provided a variety of learnings for research designs, data collection and analysis, albeit over an extended timeframe of six months. A number of innovative approaches were identified in the resultant SBCC strategy for SADC along with opportunities for regional efficiencies in adapting existing, best-practice SBCC creative and programming approaches.
Limitations
Limitations of the rapid assessment study approach relate to the reduced level of academic rigour able to be applied to some aspects of the fieldwork method, data collection and analysis. Time and budgetary constraints required data analysis from field notes compiled as the discussions took place. Although this process may be critiqued, it could also be argued that the benefits of directly taking part in the discussions and manually recording notes may provide greater insights than could be achieved through analysis of recorded materials by those not directly involved in the process of investigation. Additionally, a limitation of the quantitative survey is the lack of comprehensive responses from all SADC member-state representatives and a sample size that may limit the findings.
Disclosure of interest
The authors declare no conflicts of interest and have not entered into any agreements with the study sponsors that may have interfered with authors’ access to all of the study’s data or their ability to analyse and interpret the data, or to prepare and publish manuscripts independently when and where they choose. Perceived conflicts of interest may include the principal author’s consultancy to the sponsors of this study, SADC and GAIN, who funded the project.
Acknowledgements
The authors would like to acknowledge the support towards this study of the Southern African Development Community (SADC), with the financial support of the European Union, the Global Alliance for Improved Nutrition (GAIN) and UNICEF (United Nations Children’s Fund).
References
- UNICEF/WHO/World Bank Group. Levels and trends in child malnutrition. Joint child malnutrition estimates: Key findings of the 2020 edition. 2020. https://data.unicef.org/resources/jme-report-2020/.
- Haddad L, et al. The double burden of malnutrition in SE Asia and the Pacific: priorities, policies and politics. Health Policy Plan. 2015;30:1193–1206.
- Mahmudiono T. Child stunting in households with double burden of malnutrition: applications of behavioural epidemiology. Ann Arbor: ProQuest Dissertations Publishing; 2016. 10127361.
- Kinyoki DK, et al. Assessing comorbidity and correlates of wasting and stunting among children in Somalia using cross-sectional household surveys: 2007 to 2010. BMJ Open. 2016;6:e009854.
- United Nations Children’s Fund (UNICEF). Improving Young Children’s Diets during the complementary feeding period. New York: UNICEF Programming Guidance; 2020.
- Lassi ZS, et al. Impact of education and provision of complementary feeding on growth and morbidity in children less than 2 years of age in developing countries: a systematic review. BMC Public Health. 2013;13:S13.
- Arikpo D, et al. Educational interventions for improving primary caregiver complementary feeding practices for children aged 24 months and under. Cochrane Database Syst Rev. 2018;5:CD011768.
- Mostafa Kamal SM. Socio-economic determinants of severe and moderate stunting among under-Five children of rural Bangladesh. Mal J Nutr. 2011;17:105–118.
- Mozaffarian D, et al. Role of government policy in nutrition—barriers to and opportunities for healthier eating. Br Med J. 2018;361.
- Southern African Development Community. Synthesis report on the state of food and nutrition security and vulnerability in Southern Africa, 2020. BTS65782 WF RVAA Synthesis Report_PREFLIGHTPASSED.pdf (sadc.int).
- USAID. Multi-sectoral nutrition strategy 2014–2025: Technical guidance brief effective at-scale nutrition social and behaviour change communication, 2014. Effective At-Scale Nutrition Social and Behavior Change Communication: Technical Guidance Brief | U.S. Agency for International Development (usaid.gov).
- Boer H, et al. Protection motivation theory. In: M Conner, P Norman, editor. Predicting health behaviour. Buckingham: Open University Press; 1996. p. 95–120.
- West R, et al. A brief introduction to the COM-B Model of behaviour and the PRIME Theory of motivation. 2020. https://www.qeios.com/read/WW04E6.2.
- Bandura A. Social cognitive theory for personal and Social change by enabling media. In: A Singhal, M.J, et al. editor. EA's communication series. entertainment-education and social change: history, research, and practice. Hillsdale: Lawrence Erlbaum; 2004. p. 75–96.
- Bandura A. Social cognitive theory of mass communication. In: J Bryant, D Zillman, editor. Media effects: advances in theory and research, 2nd ed. Hillsdale: Lawrence Erlbaum; 2001. p. 121–153.
- Bandura A. Self-efficacy: Toward a unifying theory of behavioural change. Psychol Rev. 1977;84:191–215.
- Ajzen I. The theory of planned behaviour. Organ Behav Hum Decis Process. 1991;50:179–211.
- Rogers EM. Diffusion of innovations. 5th Ed New York: Free Press; 1983.
- Bettinghaus EP. Health promotion and the knowledge-attitude-behaviour continuum. Prev Med. 1986;15:475–491.
- Prochaska JO, DiClemente CC. Stages of change in the modification of problem behaviours. In: M Hersen, RM Eisler, PM Miller, editor. Progress in behaviour modification. New York: Academic Press; 1992. p. 183–218.
- Sunstein C, et al. Nudge: Improving decisions about health, wealth, and happiness. Yale: Yale University Press; 2008. 312.
- Rennie KL, et al. Behavioural determinants of obesity. Best Pract. Res. Clin. Endocrinol. Metab. 2005;19:343–358.
- WHO. A Conceptual framework for action on the Social determinants of health. Geneva: WHO; 2010; ConceptualframeworkforactiononSDH_eng.pdf (who.int).
- Sperber D. Metarepresentations in an evolutionary perspective. In: Sperber D, editor. Metarepresentations: a multidisciplinary perspective. Oxford: Oxford University Press; 2000. p. 117–137.
- Eisenhardt KM, et al. Theory building from cases: opportunities and challenges. Acad Manage Journal. 2007;50:25–32.
- Strauss A, et al. Basics of qualitative research. Thousand Oaks: Sage Publications; 1998.
- Schreiber RS. The ‘how to’ of grounded theory: avoiding the pitfalls. In: Schreiber RS, Stern PN, editor. Using grounded theory in nursing. New York: Springer; 2001. p. 191–209.
- Mozaffarian D, et al. History of modern nutrition science—implications for current research, dietary guidelines, and food policy. Br Med J. 2018;361, https://doi.org/10.1136/bmj.k2392.
- Southern African Development Community. SADC selected economic and social indicators. (2018). file:///C:/Users/tturk/Documents/projects/SADC/reference/SADC_Selected_Indicators_2018.pdf.
- Kamwendo G. The SADC protocol on education and training: linguistic implications and complications. Language Matters. 2009;40:4–17.
- UNESCO. SADC Education for all (EFA) Profile. Regional Bureau for Education in Africa. 2012. Microsoft Word - RECProfile - SADC ENG.docx (unesco.org).
- Arndt C, et al. Key issues in regional growth and integration in Southern Africa. Dev South Afr. 2018;35:297–314.
- World Bank. World Bank list of lower to middle income countries. 2020. World Bank Country and Lending Groups – World Bank Data Help Desk.
- GAIN/UNICEF. Comprehensive nutrient Gap assessment (conga) findings for children 6–23 months In: South Africa, Ethiopia, Mozambique. Geneva: GAIN; 2019.
- USAID. Factors that influence Multi-Sectoral Nutrition behaviours. USAID Factsheet; 2020.
- USAID. Behaviours to improve nutrition. USAID Factsheet; 2020.
- Ministry of Health Tanzania. Infant and Young Child Feeding guidelines. Dar-es-Salaam: Tanzania Food and Nutrition Centre; 2013.
- FAO. Impact of COVID-19 on people's livelihoods, their health and our food systems. 2020. Available from Impact of COVID-19 on people's livelihoods, their health and our food systems DevelopmentAid.
- Turk T. Regional SBCC strategy to support nutrition interventions in SADC 2020–25. Program guidance to build regional capacity and improved efficiencies for evidence-based population-level nutrition interventions. (Internal Report) Southern African Development Community(SADC), Gaborone, Botswana. 2020.
- Turk T. Regional monitoring tool on health promotion and social determinants of health in EMR. (Internal report). Cairo: WHO (EMRO); 2019.
- Vital Strategies. How Turkey’s game-changing legislation delivers powerful free airtime for anti-tobacco campaigns. 2018. How Turkey’s Game-Changing Legislation Delivers Powerful Free Airtime for Anti-Tobacco Campaigns - Vital Strategies.