
ABSTRACT
Objectives. Restless Legs Syndrome is a movement disorder characterized by unpleasant sensations in the legs described as a burning, tingling, etc. Symptoms become worse in the evening and are relieved by moving the limbs. The idiopathic form of the disease is associated with a lack of dopamine, and the secondary form is associated with iron deficiency anemia, pregnancy, and kidney disease. The aim of this study was to investigate the incidence of iron deficiency anemia in pregnant women and non-pregnant women suffering from RLS.
Methods. The study was conducted on a sample of 231 pregnant women aged 18–50. The pregnant women were interviewed at the outpatient clinic of the Department of Gynaecology and Obstetrics. This study also included a control group of 231 age-compatible non-pregnant women. Women who met the international criteria for diagnosing the syndrome filled in a sociodemographic questionnaire.
Results. A statistically significant association between the existence of iron deficiency anemia and RLS in the sample of the examined women was proven (p < 0.001). It was also shown that RLS is more frequent in a sample of anemic pregnant women than non-anemic pregnant women (p = 0.008).
Conclusion. Iron deficiency anemia is related with RLS. Pregnant women with RLS are more likely to be anemic than pregnant women without RLS.
Introduction
Restless Legs Syndrome or Willis–Ekbom's Disease is a movement disorder characterized by a strong drive to move the legs due to unpleasant sensations therein. The unpleasant feelings are described very subjectively, most commonly as tingling, pricking, burning, muscle tightness, etc. International criteria for diagnosing the illness [Citation1] were defined in 1995 and were revised by the American National Institute of Health (NIH) in 2003. These include:
An urge to move the limbs, with or without sensation
Alleviation of symptoms during motion
Worsening of the symptoms at rest
Worsening of the symptoms in the evening or at night.
The aetiology of RLS has only been partially clarified. We differentiate the primary (idiopathic) and secondary forms of the syndrome. The primary RLS aetiology is still unknown and is associated with dysfunction of the nigrostriatal dopaminergic system and decreased dopamine levels, a lack of iron in the body and heredity. The most common causes of secondary RLS are iron deficiency anemia, uremia (renal disease patients), and pregnancy [Citation2]. Iron is a cofactor of enzymes involved in dopamine synthesis and dopamine receptor regulation and its deficiency can cause RLS symptoms [Citation3]. This paper examines the frequency of iron deficiency anemia in pregnant women and non-pregnant women with RLS.
Research objectives are:
To compare the frequency of iron deficiency anemia in pregnant women with RLS and pregnant women without RLS.
To compare the frequency of iron deficiency anemia in non-pregnant women with RLS and non-pregnant women without RLS.
Materials and methods
Respondents
This study was conducted on a sample of 462 women aged 18–50. Pregnant women (N = 231) were interviewed in a pregnancy outpatient clinic of Department of Gynaecology and Obstetrics following an appointed gynecological examination. The control group consisted of age-compatible women (N = 231) who were not pregnant. The research was approved by the relevant Ethics Commissions. All participants were informed of the research goals, potential benefits, and risk of research and signed a consent form for participation in the research.
Methods
During the interview with the researcher, respondents answered questions about their RLS-related problems, and those who met the international criteria were asked to complete a sociodemographic questionnaire (designed by the researcher for this study). In the sociodemographic questionnaire for the pregnant population, respondents answered questions about age, occupation, gestational age, number of prior pregnancies, Caesarean sections in prior pregnancies, spontaneous abortions, iron deficiency anemia, kidney diseases, RLS in the family, sleep quality (graded 1–5) and the use of medication during pregnancy. In the sociodemographic questionnaire of the control group, questions regarding pregnancy were left out, as the control group consisted of women between the ages of 18 and 50 who were not pregnant.
Statistical analysis
SPSS was used for statistical data processing. A total of 462 subjects were classified according to RLS and pregnancy (). The statistical analysis methods used here are descriptive (relative numbers, mean values, graphs) and inferential methods of statistical analysis (chi-square tests and t-tests of differences between ratios for independent samples). Conclusions regarding differences and correlations among variables were made at the usual level of significance of 0.05 (p < 0.05), that is, a reliability of 95%.
Table 1. Number of respondents according to the presence of restless legs syndrome and pregnancy (N = 462).
Results
shows the presence of iron deficiency anemia and RLS in surveyed women, in cardinal numbers and percentages, and the results of the Chi-square test of independence. The percentages show that 29% of women with RLS are anemic, while only 10% women with no RLS are anemic. The results of the Chi-square test of independence show that there is a statistically significant correlation between the existence of iron deficiency anemia and RLS (χ2 = 17,351, df = 1, N = 462, p < 0.001). For the purposes of estimating the frequency of iron deficiency anemia in the surveyed women, t-tests of differences between ratios for independent samples were performed. The results of these tests are listed in . The first test relates to pregnant women, while the second test relates to non-pregnant women. The results show that RLS was present in 17.6% of pregnant women who were not anemic and 38.6% of anemic women. Therefore, RLS is more common in anemic pregnant women. This difference is not accidental but statistically significant (t = 2.67, p = 0.008). From the table, it was apparent that RLS was present in 8.4% of non-pregnant women who were not anemic and 23.5% of non-pregnant women who were anemic. This difference, although quite large, is still random, i.e. it is not statistically significant (t = 1.45, p = 0.150). shows the percentage of RLS in subgroups of pregnant and non-pregnant women who suffer from/do not suffer from iron deficiency anemia. The statistically significant result is shown in bold figures.
Figure 1. Frequency of RLS in the subgroup of pregnant women (first pair of columns) and in the subgroup of non-pregnant women (second pair of columns) in %.
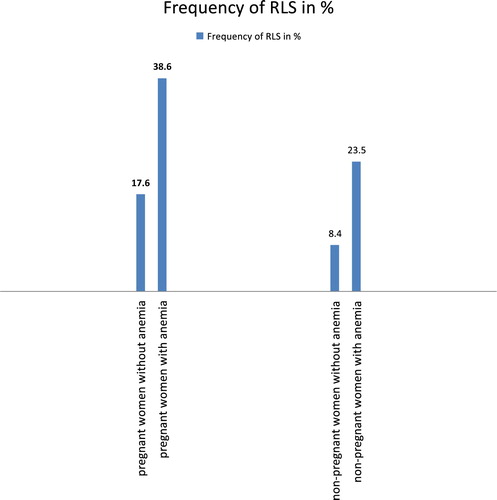
Table 2. Number of women surveyed according to the presence of iron deficiency anemia.
Table 3. Results of t-tests of differences between ratios.
Discussion
An analysis of the frequency of iron deficiency anemia in women with RLS showed that 29% of women with RLS had iron deficiency anemia, and only 10% of women who did not suffer from RLS were anemic. Iron is an important metal in biological processes in the central nervous system and its deficiency plays a role in the pathophysiology of some neurodegenerative diseases, such as Parkinson's and Alzheimer's, and is also associated with the occurrence of RLS [Citation4]. Lowered iron and ferritin concentrations in cerebrospinal fluid have been demonstrated in affected people [Citation5], and similar results have been obtained with post-mortem analyses [Citation6]. Iron is essential for oxidative processes in ferrite mitochondria, therefore its reduction affects the neuronal metabolism and the formation of RLS [Citation7]. The most endangered group are those with an excessive loss of iron (women with abnormally heavy menstrual bleeding, elderly people with gastrointestinal bleeding), people with reduced iron resorption and those with an increased demand for iron (pregnant women). The results of this study show that 38.6% of anemic pregnant women suffer from RLS, as well as 17.6% of pregnant women who are not anemic. We can conclude that pregnant women with RLS are more likely to be anemic than pregnant women without RLS. The aetiology of RLS in pregnancy is still insufficiently researched. It is most common in the third trimester of pregnancy, and the symptoms of most women are alleviated following delivery [Citation8]. In addition to iron deficiency, important aetiological factors are: a positive family history, a disturbed circadian rhythm of dopamine with a decrease in concentration in the evening, and hormonal changes, primarily the rise of estradiol in the third trimester, which acts as an inhibitor to the dopaminergic system [Citation9]. The results obtained for the non-pregnant group show that RLS is more common in anemic women, but they cannot be taken into account because they are not statistically significant (p > 0.05). It is certain that pregnancy, as an additional factor, affects the occurrence of RLS, which may explain the differences in results obtained in groups of pregnant and non-pregnant women, and provides a starting point for further investigation of this issue. RLS is one of the most common movement disorders but is unfortunately often undiagnosed [Citation10]. The aetiology of this disease has not been fully clarified, but iron deficiency and kidney disease are considered to be among the most important causes of secondary RLS [Citation11]. This study has proven a statistically significant connection between the existence of iron deficiency anemia and RLS in the sample of examined women. Also, it has been shown that RLS is more frequent in a sample of examined pregnant women with iron deficiency anemia than in non-anemic pregnant women, and that pregnancy and iron deficiency anemia are associated precipitating factors for the development of RLS. It should be noted that RLS can also occur in non-anemic women, both pregnant and non-pregnant. These women often have kidney disease, a positive family history, or an iron deficiency that is not severe enough to decrease hemoglobin levels. Some of them take antidepressants, antipsychotics, anti-nausea drugs, or other medications that decrease dopamine levels. Therefore, every woman suspected of having RLS should be minutely examined for a family history of similar symptoms, medication use, and the presence of other symptoms or medical conditions. Uncomfortable sensations occur mostly in the evening and are alleviated by moving the extremities [Citation12]. Due to getting up at night frequently, those affected have an impaired sleep quality and thus an impaired quality of life [Citation13,Citation14]. Sufferers should be educated about the nature of their illness and advised on changing their life habits (stopping smoking, reducing the intake of caffeinated drinks, moderate physical activity), advising them as to the importance of adequate sleep hygiene and, if necessary, prescribing adequate medication therapy [Citation15]. It is very important to determine iron values in women of reproductive age, especially in pregnant women, and to prevent and treat iron deficiency anemia with adequate nutrition and, where necessary, substitution in oral or IV forms. If the non-pharmacological approach or iron substitution do not reduce the symptoms of RLS, then a pharmacological approach should be considered for further management, but only in non-pregnant women. The medications that are used to reduce the symptoms of RLS include: dopaminergic agents, benzodiazepines, opioids, and anti-epileptic agents [Citation16]. The efficacy and safety of these medications for treating RLS during pregnancy have not been clearly established and they need to be explored further [Citation17]. Every physician must consider the effect of medication on the fetus, especially the possibility of congenital malformations. Special emphasis should be placed on the education of pregnant women, due to the limitations of medication therapy [Citation18]. It is important to recognize and diagnose the disease as early as possible and to begin with the treatment, thereby easing the patients’ symptoms and improving the quality of their lives. All this points to the importance of education at all levels, given that RLS is still insufficiently well known, and is thus an unrecognized, and often even untreated, disease.
Acknowledgments
The authors would like to thank the patients who volunteered and participated in this study as well as all the staff of the University Hospital Centre Zagreb for their cooperation and valuable help during the course of the study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Notes on contributors
Srđana Telarović, neurologist, primarius is employed at the School of Medicine, University of Zagreb, and at the Department of Neurology, Movement Disorders Unit, University Hospital Center Zagreb. Her area of expert, scientifical and educational work are extrapyramidal diseases, from which are the master's thesis “The effect of atypical neuroleptic clozapine on resistant tremor in Parkinson's disease” and Ph.D. thesis “The long-term safety and efficacy of botulinum toxin Type A in the treatment of focal dystonia.". She has published a number of different publications and has been invited lecturer at numerous domestic and international conferences.
Lucija Čondić is a graduate of University of Zagreb, School of Medicine. She is waiting for her internship to start. Her clinical interests include neurology and gynecology.
ORCID
Srdjana Telarović http://orcid.org/0000-0002-1287-6144
Lucija Čondić http://orcid.org/0000-0002-7819-236X
Related Research Data
References
- Ekbom K, Ulfberg J. Restless legs syndrome. Intern Med. 2009;266(5):419–431. doi:10.1111/j.1365-2796.2009.02159.x.
- Cotter PE, O’Keeffe ST. Restless leg syndrome: is it a real problem? Ther Clin Risk Manag. 2006;2(4):465–475. doi: 10.2147/tcrm.2006.2.4.465
- Patrick LR. Restless legs syndrome: pathophysiology and the role of iron and folate. Altern Med Rev. 2007;12(2):101–112.
- Telarović S, Šarac H. Hereditarni i sekundarni sindrom nemirnih nogu u bolesnika sa sideropeničnom anemijom. Neurol Croat. 2011;60(1):35–41.
- Godau J, Klose U, Di Santo A, et al. Multiregional brain iron deficiency in restless legs syndrome. Mov Disord. 2008;23:1184–1187. doi:10.1002/mds.22070.
- Connor JP, Ponnuru P, Lee BY, et al. Postmortem and imaging based analyses reveal CNS decreased myelinisation in restless legs syndrome. Sleep Med. 2011;12:614–619. doi:10.1016/j.jsmc.2015.05.022 doi: 10.1016/j.sleep.2010.10.009
- Snyder AM, Wang X, Patton SM, et al. Mitochondrial ferritin in the substantia nigra in restless legs syndrome. J Neuropatol Exp Neurol. 2009;68:1193–1199. doi:10.1097/NEN.0b013e3181bdc44f.
- Tan M, Bourjeily G. Shaking up perspectives of restless legs syndrome in pregnancy. J Clin Sleep Med. 2017;13(7):857–858. doi:10.5664/jcsm.6648.
- Neau JP, Marion P, Mathis S, et al. Restless legs syndrome and pregnancy: follow-up of pregnant women before and after delivery. Eur Neurol. 2010;64:361–366. doi:10.1159/000322124.
- Vishal KC, Snehal PS. Restless legs syndrome, the pitfall: hardly diagnosed and rarely treated neurological disease. Austin J Clin Neurol. 2017;4(5):1118.
- Quinn C, Uzbeck M, Saleem I, et al. Iron status and chronic kidney disease predict restless legs syndrome in an older hospital population. Sleep Med. 2011;12:295–301. doi:10.1016/j.sleep.2010.08.014.
- Fida A, Egbe S, Scheid D, et al. In adults what is the best diagnostic test for restless leg syndrome? J Okla State Med Assoc. 2014;107(8):432–434.
- Demircioğlu D T, Kavadar G, Esen Öre Ö, et al. Relationship between restless leg syndrome and quality of life in uremic patients. Agriculture. 2015;27(2):73–78. doi:10.5505/agri.2015.
- Abetz L, Allen R, Follet A, et al. Evaluating the quality of life of patients with restless legs syndrome. Clin Ther. 2004;26(6):925–935. doi:10.1016/j.sleep.2007.11.024 doi: 10.1016/S0149-2918(04)90136-1
- Einollahi B, Izadianmehr N. Restless leg syndrome: a neglected diagnosis. Nephrourol Mon. 2014;6(5):e22009. doi:10.5812/numonthly.22009.
- Gupta R, Dhyani M, Kendzerska T, et al. Restless legs syndrome and pregnancy: prevalence, possible pathophysiological mechanisms and treatment. Acta Neurol Scand. 2016;133(5):320–329. doi:10.1111/ane.12520.
- Srivanitchapoom P, Pandey S, Hallett M. Restless legs syndrome and pregnancy: A review. Parkinsonism Relat Disord. 2014;20(7):716–722. doi:10.1016/j.parkreldis.2014.03.027.
- Grover A, Clark-Bilodeau C, D’Ambrosio CM. Restless leg syndrome in pregnancy. Obstet Med. 2015;8(3):121–125. doi:10.1177/1753495X15587452.