
ABSTRACT
Background
Calcium plays a key role in many bio-homeostasis functions. Previous studies indicated that serum calcium is associated with diseases such as anaemia. However, the evidence on the association between serum calcium levels and anaemia risk is limited. Thus, the purpose of our study is to investigate the relationship between serum calcium and anaemia in US adults.
Methods
This cross-sectional study used data from the National Health and Nutrition Examination Survey (NHANES) including 15,519 participants, aged ≥18 years. The analyses were performed using multivariate logistic regression and a generalized additive model (GAM). Subgroup analysis, stratified by gender and age, was also performed.
Results
Among the sample of 15,519 individuals, 1565 (10.8%) had been diagnosed with anaemia. Both the univariate logistic regression model and multivariate logistic regression model showed a reverse relationship between serum calcium and anaemia risk. Moreover, a non-linear association between serum calcium and anaemia risk was observed using GAM and smooth curve fitting. The inflection point of serum calcium was at 2.3 mmol/L. GAM with penalized splines suggested a reverse association between serum calcium and the prevalence of anaemia when the concentration of serum calcium was below 2.3 mmol/L. In contrast, we found no statistically significant difference when serum calcium concentration was higher than the inflection point (2.3 mmol/L).
Conclusion
Lower serum calcium levels were associated with increased risk of anaemia risk. Moreover, we observed non-linear associations between serum calcium and anaemia risk. Our results need to be confirmed in future prospective studies.
KEYWORDS:
Introduction
Anaemia is widespread worldwide, especially among the elderly and women. Epidemiologic studies have reported that anaemia was related to a series of chronic diseases including cardiovascular disease [Citation1], autoimmune diseases [Citation2], chronic kidney disease [Citation3], and cancer [Citation4]. Moreover, evidence from studies suggested that a range of chronic diseases had been linked to the risk of anaemia [Citation5–7]. Given the harmful effects of anaemia, early identification of risk factors for anaemia and its prevention and management would be beneficial. Recently, epidemiological studies have shown that dietary patterns and lifestyle were important risk factors that may influence the prevalence of anaemia [Citation8]. However, the potential influence of nutritional factors on the risk of anaemia had not been given enough attention.
Calcium plays a crucial role in many bio-homeostasis functions, such as nerve conduction, coagulation factor regulation, activating enzymes, regulating blood pressure, hormone regulation and contracting muscle. Calcium in the diet is obtained mainly from dairy products. The daily dietary intake of calcium is approximately 800 mg/day in Americans, which is below the recommended dietary allowance (RDA) of 1000–1200 mg/day in adults. Data from a review indicate that adolescents and the elderly are at risk of insufficient calcium intake [Citation9]. Previous studies have shown that calcium had both beneficial and adverse effects on health. A multi-provincial cohort study indicated that high serum calcium may decrease the risk of retinopathy among participants without diabetes [Citation10]. On contrary, growing data from prospective studies pointed out high serum calcium was associated with cardiovascular and metabolic disease risk [Citation11,Citation12]. However, studies exploring the association between calcium and anaemia risk are limited. The study aimed to evaluate the association between serum calcium levels and anaemia prevalence in American adults.
Materials and methods
Study population
In this analysis, the data were acquired from NHANES (the National Health and Nutrition Examination Survey). The survey was conducted by the Centers for Disease Control and Prevention (CDC) and the National Health Center, which is based on the national population. All data and materials are publicly accessible on the National Center for Health Statistics website (https://www.cdc.gov/nchs/nhanes/index.htm). All participants over the age of 18 received informed consent ().
Figure 1. The flow chart of the study.
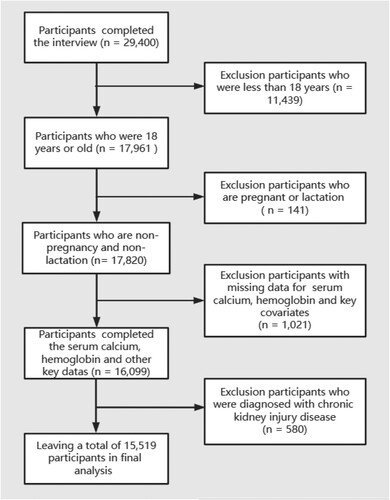
In our study, we used three continuous cycles of NHANES (2011–2016). We excluded younger than 18 years old and those who were in pregnancy or lactation. Participants with missing data on serum calcium, haemoglobin concentration and other covariates (n = 542) were also excluded. Finally, 15,519 participants were enrolled in the study.
Total calcium in serum
Blood samples were collected and stored in mobile devices by certified laboratory professionals. Total calcium was measured as part of the Synchro LX20 Conventional Biochemical profile (Beckman Coulter, Inc.) or UniCelR DxC 800 Synchro (Beckman Coulter, Inc.), both of which measured serum calcium concentrations indirectly (or diluted) using an ion-selective electrode method. The unit of serum calcium was mmol/L. More details of the lab programme have been described at https://wwwn.cdc.gov/nchs/nhanes/default.aspx (accessed October 7, 2022).
The definition of anaemia
Anaemia was determined by a haemoglobin concentration of <120 g/L for women and <130 g/L for men.
Covariates
Demographic information included age, gender (female and male), race/ethnicity (Mexican American, other Hispanic, non-Hispanic black, non-Hispanic white, and other races), and education levels (college or above, high school, and below high school). Self-reported smoking status (current smokers, former smokers, and never smokers), and physical activity (light activity, moderate activity and vigorous activity) were obtained from a questionnaire. Dietary data including alcohol consumption, total dietary food energy, protein, fibre, vitamin D, calcium, and magnesium intake, came from 24 h dietary interviews. Serum calcium (mmol/L) was obtained from laboratory tests. Body mass index (BMI) was calculated by dividing their weight in kilograms by their square height in metres (kg/m2).
Statistical analysis
All analyses were conducted following NHANES recommendations. Categorical and continuous variables were presented as numbers (n) with percentages (%) and as means with standard deviations. Two-tailed Student’s t-test and chi-squared test were used. Logistic regression was used to estimate the association between serum calcium and the risk of anaemia. To interpretate the results, serum calcium was transformed 10 times expansion. A serum calcium quartile was utilized to measure the stability of the results. The linear trend test was also performed in the model. To explore potential nonlinear correlation, a generalized additive model (GAM) with penalty splines was used. The potential confounding factors are gradually adjusted in the logistic regression model. Model 1 was adjusted for none. Model 2 was adjusted for age, gender, and race/ethnicity. Model 3 was adjusted for gender, age, race/ethnicity, PIR, education level, BMI, waistline, magnesium, energy, protein, fibre; calcium, vitamin D, alcohol consumption, work activity and smoking status. We also examined possible modifications to the effect of gender-stratified analyses to estimate the relationship between serum calcium and anaemia. Stratified analyses were conducted to estimate the relationship between serum calcium and anaemia risk by age (20–39, 40–59 or 60–80 years), and gender (male or female). To evaluate the robustness of our results, several sensitivity analyses were also performed. First, the continuous variable of serum calcium was converted into a categorical variable quartile. Second, the penalty curve method and generalized additive model (GAM) were used to address the potential non-linear relationship between serum calcium and the risk of anaemia. The recursion algorithm of the inflection point was calculated, and then a weighted two-stage linear model was established on both sides of the inflection point. Finally, the optimal model was established according to p-value of the log of the likelihood ratio.
The statistics involved in the study were performed using the R statistical software package (http://www.R-project.org, The R Foundation) and Free Statistics software version 1.4. A two-sided P-value of <0.05 was considered statistically significant.
Results
The characteristics of the study are summarized in . Among 15,519 participants, 1565 were anaemia cases (10.8%). Anaemia participants tended to be female, older than 60 years old, had lower PIR and had lower serum calcium levels compared with those who were non-anaemic. The association between serum calcium and anaemia risk is shown in . In model 3, when adjusted for sex, age and race, PIR, education level, BMI, waistline, magnesium, energy; protein, fibre; calcium, vitamin D, alcohol consumption, work activity and smoking status, the OR (95% CI) was 0.52 (95%CI 0.48–0.57). Compared to the lowest quintile, participants in the highest quintile of serum calcium had a 76% reduction in anaemia risk, and P for trend was significant (p for trend <0.001). In , this association was analyzed when stratified by gender and age. After adjusting for the same covariates (all listed in ), serum calcium was inversely associated with the risk of anaemia both in different ages and gender. The ORs (95% CI) for anaemia in the female and male groups were 0.56 (95% CI: 0.51, 0.62) and 0.56 (95% CI: 0.46, 0.64), respectively and P for trend was significant (p for trend <0.001). The ORs (95% CI) for anaemia in different ages were 0.59 (0.51–0.69), 0.55 (0.48–0.63), and 0.67 (0.59–0.75), respectively and P for trend was also significant (p for trend <0.001). GAM model and smooth curve fitting (penalty curve method) were performed to assess the potential nonlinear relationship between serum calcium and anaemia risk (). We found a reverse association at <2.4 mmol/L serum calcium. But, there was no significant difference at serum calcium >2.4 mmol/L. A threshold effect between serum calcium and anaemia was found ().
Figure 2. The relationship between serum calcium and anaemia based on the generalized additive model (GAM).
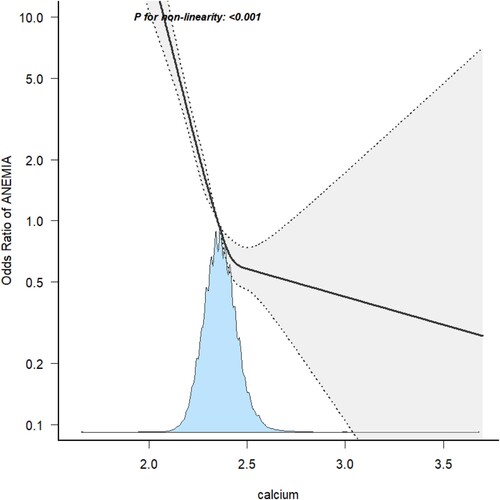
Table 1. The characteristics of the study grouped by anaemia.
Table 2. Odds ratios (95% confidence intervals) of anaemia across quartiles of serum calcium.
Table 3. Odds ratios (95% confidence intervals) of anaemia across quartiles of serum calcium stratify by gender and age, NHANES 2011–2016.
Table 4. Threshold effect analysis of serum calcium on anaemia based on the segmented linear regression model.
Discussion
In this study, we utilized the data from NHANES (2011–2016), a nationally representative sample of the U.S. population and found that both the univariate logistic regression model and multivariate logistic regression model showed a reverse relationship between serum calcium and anaemia. Moreover, a non-linear association of serum calcium with anaemia prevalence was observed after performing a smooth curve fitting and a weighted two-piecewise linear model. The inflection point of serum calcium was at 2.4 mmol/L. GAM with penalized splines suggests that there was a reverse association between serum calcium and the prevalence of anaemia when serum calcium is at <2.4 mmol/L. In contrast, there is no significant association between serum calcium and anaemia risk when serum calcium concentration is higher than inflection point. In addition, to the best of our knowledge, it is the first investigation to explore the relationship between serum calcium and anaemia risk based on the general population.
Calcium is an essential nutrient for the human body. In addition to affecting bone mineralization, calcium plays a role in a wide range of biological functions by regulating different cellular processes by signalling systems [Citation13]. A study from Ethiopia found a statistically significant association between low calcium concentration in serum and low dietary calcium intake and preeclampsia [Citation14]. A similar study indicated that calcium supplements may reduce the risk of preeclampsia and high blood pressure during pregnancy [Citation15]. A large Chinese cohort study suggested that fracture risk was inversely associated with calcium intake in women. Higher dietary calcium intakes in women were associated with fewer vertebral fractures in people compared with lower normal calcium intakes [Citation16]. A cross-sectional study among 4595 participants concluded that the relationship between serum calcium and lumbar bone density in men was a U-shaped curve [Citation17]. T Mariko Doi et al. suggested that cord blood calcium level may be related to birth length and may affect foetal growth during pregnancy [Citation18]. There is no clear significant association between calcium intake and liver fibrosis among adults in the United States [Citation19]. A prospective study showed that lower baseline blood calcium levels were associated with an increased risk of all-cause and cardiovascular mortality in a Chinese coronary heart disease cohort [Citation20].
In addition to the benefits of calcium, adverse effects of calcium supplementation were also found. A growing number of studies in recent years have reported that serum calcium levels were positively associated with the risk of cardiovascular disease, including myocardial infarction [Citation21,Citation22]. Similarly, some observational studies found that calcium supplementation can lead to hypercalcaemia, which is associated with an increased risk of coronary artery calcification events [Citation22–24]. In the present study, we concluded that serum calcium was negatively correlated with anaemia when serum calcium concentration was lower than 2.4 mmol/L. Our results may provide a reference for possible safe upper limits of calcium status about anaemia risk. There were few epidemiological studies to assess the relationship between calcium levels in serum and anaemia prevalence. In support of our results, a study including more than 8000 haemodialysis patients showed that calcium levels in serum were positively associated with hsemoglobin levels [Citation25]. Another study concluded that there was an association between serum calcium and anaemia prevalence in a cohort with 382 individuals with chronic kidney disease [Citation26]. However, the existing studies mostly focused on a subset of special populations, thus affecting the extensibility of the conclusions. In our study, a non-linear relationship between serum calcium and the risk of anaemia in a general population was examined.
Although studies found that calcium is involved in the process of proliferation and differentiation of erythropoietin-induced erythropoietin progenitor cells in vitro as early as 40 years ago [Citation27], the exact biological mechanism of the role of calcium in anaemia is still largely unknown. Some studies explained that low serum calcium decreases erythropoietin reactivity [Citation28–30]. Recently, it has been reported that calcium plays an important role in the signalling pathway activated by the binding of erythropoietin to its receptor by activating some type of transient receptor potential channel [Citation31]. Therefore, calcium levels in serum may affect anaemia by promoting erythrocyte production. These hypotheses require further experimental studies in future.
We first observed a non-linear association between serum and anaemia in a representative sample of the general US adult. To date, this is the largest study assessing the association between serum calcium and anaemia. Linear and nonlinear statistical analyses were used in our study, and the findings are robust and educational for anaemia prevention. However, our study still shows some limitations. Firstly, with respect to the characteristics of a cross-sectional study, our conclusion could not reflect a causal relationship. Secondly, serum calcium levels are single measurements, which may fluctuate due to other factors such as transfer, and not reflect long-term conditions. Finally, unmeasured confounding cannot be completely excluded although we adjusted for as many as possible. More prospective cohort studies or randomized controlled clinical trials in future are needed to confirm our findings.
Conclusions
A negative and non-linear relationship between serum calcium levels and anaemia was found. Serum calcium levels are significantly decreased anaemia risk when calcium in serum is below the inflection point. Our findings suggest that maintaining appropriate serum calcium levels has a potentially beneficial role in reducing the risk of anaemia.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- De Lima J, Gowdak L, David-Neto E, et al. Diabetes, cardiovascular, and cardiovascular risk in patients with chronic kidney disease. High Blood Press Cardiovasc Prev. 2021;28:159–165. DOI:10.1007/s40292-021-00434-0
- Weiss G, Ganz T, Goodnough LT. Anemia of inflammation. Blood. 2019;133:40–50. DOI:10.1182/blood-2018-06-856500
- Del FP, Luthi JC, Carrera E, et al. Anemia and chronic kidney disease are potential risk factors for mortality in stroke patients: a historic cohort study. Bmc Nephrol. 2010;11:27. DOI:10.1186/1471-2369-11-27
- Sganzerla JT, Krueger GF, Oliveira MC, et al. Relationship between anemia and oral cancer: a case-control study. Braz Oral Res. 2021;35:e85. DOI:10.1590/1807-3107bor-2021.vol35.0085
- Goodnough LT, Schrier SL. Evaluation and management of anemia in the elderly. Am J Hematol. 2014;89:88–96. DOI:10.1002/ajh.23598
- Stauder R, Valent P, Theurl I. Anemia at older age: etiologies, clinical implications, and management. Blood. 2018;131:505–514. DOI:10.1182/blood-2017-07-746446
- Ferrucci L, Semba RD, Guralnik JM, et al. Proinflammatory state, hepcidin, and anemia in older persons. Blood. 2010;115:3810–3816. DOI:10.1182/blood-2009-02-201087
- Purnamasari SD, Hsu CY, Chen YT, et al. Combined low plant and high animal dietary pattern is associated with a lower risk of anemia among dyslipidemic adult women in Taiwan: a retrospective study from 2001 to 2015. Int J Environ Res Public Health. 2022;19; DOI:10.3390/ijerph19106231
- Romero-Marco P, Perez-Gallardo LL. Adequacy of calcium intake in Spanish population according age groups. Arch Osteoporos. 2020;15:161. DOI:10.1007/s11657-020-00831-3
- Li J, Zhao D, Deng Q, et al. Reduced serum calcium is associated with a higher risk of retinopathy in non-diabetic individuals: the Chinese multi-provincial Cohort Study. Front Endocrinol (Lausanne. 2022;13:973078. DOI:10.3389/fendo.2022.973078
- Dong H, Hu P, Wang J, et al. Associations of serum calcium, magnesium levels, and their ratio with apolipoproteins in Chinese adults with coronary artery disease: a cross-sectional study. Biol Trace Elem Res. 2022;200:4221–4229. DOI:10.1007/s12011-021-03015-3
- Larsson SC, Burgess S, Michaelsson K. Association of genetic variants related to serum calcium levels with coronary artery disease and myocardial infarction. JAMA. 2017;318:371–380. DOI:10.1001/jama.2017.8981
- Berridge MJ, Bootman MD, Roderick HL. Calcium signalling: dynamics, homeostasis and remodelling. Nat Rev Mol Cell Biol. 2003;4:517–529. DOI:10.1038/nrm1155
- Gebreyohannes RD, Abdella A, Ayele W, et al. Association of dietary calcium intake, total and ionized serum calcium levels with preeclampsia in Ethiopia. BMC Pregnancy Childbirth. 2021;21:532. DOI:10.1186/s12884-021-04005-y
- Sun X, Li H, He X, et al. The association between calcium supplement and preeclampsia and gestational hypertension: a systematic review and meta-analysis of randomized trials. Hypertens Pregnancy. 2019;38:129–139. DOI:10.1080/10641955.2019.1593445
- Wang L, Yin L, Cheng X, et al. The association of calcium intake with osteoporotic vertebral fractures in a large Chinese cohort. Aging (Albany NY). 2020;12:5500–5515. DOI:10.18632/aging.102974
- Liu M, Yao X, Zhu Z. Associations between serum calcium, 25 (OH)D level and bone mineral density in older adults. J Orthop Surg Res. 2019;14:458. DOI:10.1186/s13018-019-1517-y
- Doi M, Rekha RS, Ahmed S, et al. Association between calcium in cord blood and newborn size in Bangladesh. Br J Nutr. 2011;106:1398–1407. DOI:10.1017/S0007114511001747
- Tao MH, Fulda KG. Association of magnesium intake with liver fibrosis among adults in the United States. Nutrients. 2021;13:142. DOI:10.3390/nu13010142
- Chen Q, Zhang Y, Ding D, et al. Associations between serum calcium, phosphorus and mortality among patients with coronary heart disease. Eur J Nutr. 2018;57:2457–2467. DOI:10.1007/s00394-017-1518-8
- Reid IR, Gamble GD, Bolland MJ. Circulating calcium concentrations, vascular disease and mortality: a systematic review. J Intern Med. 2016;279:524–540. DOI:10.1111/joim.12464
- Rohrmann S, Garmo H, Malmstrom H, et al. Association between serum calcium concentration and risk of incident and fatal cardiovascular disease in the prospective AMORIS study. Atherosclerosis. 2016;251:85–93. DOI:10.1016/j.atherosclerosis.2016.06.004
- Barry EL, Mott LA, Melamed ML, et al. Calcium supplementation increases blood creatinine concentration in a randomized controlled trial. Plos One. 2014;9:e108094. DOI:10.1371/journal.pone.0108094
- Anderson JJ, Kruszka B, Delaney JA, et al. Calcium intake from diet and supplements and the risk of coronary artery calcification and its progression among older adults: 10-year follow-up of the Multi-Ethnic Study of Atherosclerosis (MESA). J Am Heart Assoc. 2016;5. DOI:10.1161/JAHA.116.003815
- Bacchetta J, Zaritsky JJ, Sea JL, et al. Suppression of iron-regulatory hepcidin by vitamin D. J Am Soc Nephrol. 2014;25:564–572. DOI:10.1681/ASN.2013040355
- Boronat M, Santana A, Bosch E, et al. Relationship between anemia and serum concentrations of calcium and phosphorus in advanced non-dialysis-dependent chronic kidney disease. Nephron Clin Pract. 2017;135:97–104. DOI:10.1159/000450892
- Misiti J, Spivak JL. Erythropoiesis in vitro. Role of calcium. J Clin Invest. 1979;64:1573–1579. DOI:10.1172/JCI109618
- Tonelli M, Blake PG, Muirhead N. Predictors of erythropoietin responsiveness in chronic hemodialysis patients. Asaio J. 2001;47:82–85. DOI:10.1097/00002480-200101000-00017
- Diskin CJ, Stokes TJ, Dansby LM, et al. Can acidosis and hyperphosphataemia result in increased erythropoietin dosing in haemodialysis patients? Nephrology (Carlton). 2006;11:394–399. DOI:10.1111/j.1440-1797.2006.00674.x
- Kalantar-Zadeh K, Lee GH, Miller JE, et al. Predictors of hyporesponsiveness to erythropoiesis-stimulating agents in hemodialysis patients. Am J Kidney Dis. 2009;53:823–834. DOI:10.1053/j.ajkd.2008.12.040
- Tong Q, Hirschler-Laszkiewicz I, Zhang W, et al. TRPC3 is the erythropoietin-regulated calcium channel in human erythroid cells. J Biol Chem. 2008;283:10385–10395. DOI:10.1074/jbc.M710231200