
Abstract
Introduction:
The prevalence and risk factors of type 2 diabetes vary across the urban and rural milieus of Ghana's Ashanti Region, yet no study has been conducted to synthesise the available studies.
Methods:
A comprehensive literature search was carried out in PubMed, CINAHL, Scopus and Web of Science with hand searches in Google Scholar and grey literature between May 15, 2021 and June 30, 2021. Searches were made for articles published between January 1, 2011 and December 31, 2020 on type 2 diabetes mellitus in the Ashanti region of Ghana. MeSH terms and keywords, separated by some Boolean operators, were used.
Results:
The searches yielded a total of 268 articles, of which 12 studies were selected for the final review. Physical inactivity and obesity were identified as the major risk factors of type 2 diabetes in the region. Higher prevalence of the disease was also identified in females. More so, in terms of rural and urban divides, type 2 diabetes mellitus was found predominantly among urban dwellers.
Conclusion:
Findings from the study call for mass sensitisation and awareness creation in respect of diabetes, to ensure that people are well informed on the dynamics of the disease in the region and, by extension, the country at large.
Introduction
Diabetes remains one of the most prominent diseases of public health concern in the twenty-first century. According to the International Diabetes Federation (IDF),Citation1 1 in every 11 people worldwide, the equivalent of about 463 million people globally, suffers from the disease. Similarly, the World Health Organization (WHO)Citation2 also indicates that, globally, diabetes has claimed over 4.2 million lives since the beginning of the twenty-first century. For the year 2019, the IDFCitation1 reports that over US$ 760 billion has been committed to combating diabetes globally. Despite this attempt, the WHOCitation2 noted that over 374 million more people presently are at high risk of developing complications related to diabetes. In the same way, the IDFCitation1 projected that, by end of 2045, over 700 million people across the world are likely to be suffering from the disease due to changing psychosocial and institutional factors. These recent developments have resulted in diabetes being listed as one of the top four non-communicable diseases of the twenty-first century.Citation1
Being the most common type of diabetes, type 2 diabetes mellitus currently accounts for over 90% of all diabetes cases worldwide.Citation3–5 Though commonly associated with ageing and older adults, the disease is gradually becoming pervasive among young adults and adolescents,Citation5,Citation6 which, according to ArandaCitation7 and Arnett et al.,Citation8 is as a result of physical inactivity, poor eating habits and obesity. Even though the health disorder is a global phenomenon, Thomas et al.Citation9 noted that it is gradually becoming predominant in developing countries, particularly those in Africa and Asia. According to the IDF,Citation1 China has the largest type 2 diabetes population in the world at about 120 million people.
Type 2 diabetes cases in Africa have not been different from the global picture.Citation3 With a prevalence rate of 3.9%, the IDFCitation10 report indicates that an estimated 19.4 million adults are living with the disease in the region, which according to the IDFCitation1 is likely to increase to 45 million by end of 2045. Similarly, the WHOCitation2 reported that about 45 million adults in Africa between the ages of 20 and 79 years have impaired glucose tolerance, which predisposes them to a high risk of developing type 2 diabetes in the near future. This figure has been estimated to rise to 110 million by 2045 if the necessary interventions are delayed.Citation2 Given that, in 2019, only US$ 9 billion was allocated to combating the disease on the African continent (which is equivalent to just 1% of the total health expenditure for the 2019 financial year), the scientific community foresees a gloomy future for the disease in Africa.Citation4,Citation11–13 It has therefore become imperative that unprecedented actions are taken by member countries and the international community, to ensure that the continent is freed from the burden of this deadly disease. According to the IDF,Citation5 a victory over the surge of type 2 diabetes on the African continent will be a great milestone towards achieving sustainable development goal (SDG) 3 by end-of-year 2030. As a result, some member countries in Africa have in recent times committed a substantial proportion of health budgets to combating the disease within their geopolitical boundaries.Citation3,Citation14–16
Type 2 diabetes has a long history in Ghana. However, very little was known about the disease in that country until the latter part of the twentieth century.Citation17,Citation18 In their nationwide study on the disease, Amoah et al.Citation17 found a generally held misconception that diabetes is a disease of the rich. This, according to Aikins et al.,Citation19 restrained all locally targeted actions to mitigate the disease in the past. Conversely, the advent of the Millennium Development Goals (2000–2015) and the Sustainable Development Goals (2015–2030) by the United Nations Organization (UNO), brought a rebirth of knowledge on the menace of type 2 diabetes at national, regional and district levels in Ghana.Citation17,Citation19,Citation20
The literature contains copiously advanced knowledge on diabetes in the Ashanti region of Ghana. This region currently has the highest level of scientific writing on type 2 diabetes in the country.Citation21–24 For instance, Addo et al.Citation25 found that diabetes prevalence increases with increasing level of education in urban Kumasi. In the same regard, Agbogli et al.Citation26 found sedentary lifestyle activities, overweight and obesity to be major risk factors for diabetes in the Oforikrom Municipality. Psychosocial risk factors (lifestyle and behavioural) such as physical inactivity, unhealthy dietary practices, over-consumption of alcohol, unhealthy food intake, overeating, smoking and eating late at night have also been established by Aikins et al.Citation19 as the major cause of type 2 diabetes mellitus in the region. However, as far as this study is concerned, no single scholarly work exists in the study area, which synthesised all primary research on type 2 diabetes mellitus to ascertain the most prevalent risk factors of the disease. The relevance of knowledge synthesis in any given subject area cannot be underestimated. According to Wohlin,Citation27 systematic reviews help to identify, evaluate and summarise the findings of all relevant individual studies on a health-related issue, thereby making the available evidence more accessible to decision-makers. Against this background, this study seeks to fill this crucial research gap by ascertaining and examining the disease prevalence and the most common risk factors of type 2 diabetes mellitus in the Ashanti region of Ghana.
Figure 1: Flowchart of all synthesised literature.
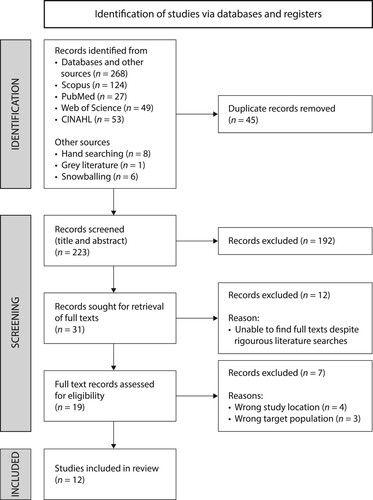
Table 1: Summary of findings of studies included in the review to examine the risk factors of type 2 diabetes mellitus among adult Ghanaians in the Ashanti region of Ghana
Methods
The generally accepted Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) was followed as a guide for conducting the study.
Literature search
A rigorous literature search was carried out in four well-known bibliographic databases (). These were Web of Science, Scopus, Medline (PubMed) and CINAHL. Hand searches were also done in Google Scholar and the grey literature (theses) for relevant supplementary material. Searches were conducted for articles published from January 1, 2011 to December 31, 2020 on type 2 diabetes mellitus in the Ashanti region of Ghana. This timeframe was chosen because much research was found to have been conducted on the subject matter within the period, thereby making the issue shoot into the limelight in Ghana. Reference lists of some downloaded articles were consulted to identify other relevant articles. Key words and medical subject headings (MeSH) terms were used for the searches in the above-listed bibliographic databases. Boolean operators (‘AND’ and ‘OR’) were used to separate MeSH terms and keywords. Based on the objective of the study, the following MeSH terms were used: ‘Diabetes mellitus’, ‘Type 2 diabetes’, ‘Diabetes mellitus, type 2’, ‘Risk factors’ and ‘Prevalence’. The key words included ‘type 2 diabetes’, ‘type II diabetes’, ‘T2D’, ‘T2DM’, ‘DM2’, ‘diabetes mellitus’, ‘prevalence’, ‘risk factors’ and ‘Ashanti region’. The searches focused on articles published on adult diabetes patients (18 years and above). This was because, in Ghana, one is considered an adult when he/she is above 18 years of age.Citation28 Searches were also narrowed to articles published only in English for two key reasons. First, because English is the official language in Ghana and, second, due to financial constraints coupled with the difficulty of accessing the services of language translators. Authors and experts who have over the years contributed significantly to the literature on diabetes were contacted to inquire about any additional published and unpublished materials. The searches started on May 15, 2021 and were completed on June 30, 2021.
Study selection and quality assessment
After downloading all necessary articles, the study employed the United States Preventive Services Task Force Procedure (USPSTF) manual to determine whether the articles were relevant to meet the overriding objective of the study.Citation29 In this regard, a multi-stage screening procedure was adopted to minimise errors, to enhance transparency of outcomes and, above all, to make the study producible. Two reviewers reviewed all the articles at all stages. First and foremost, the reviewers read through the titles and abstracts of all retrieved articles for relevance by broadly applying the inclusion criteria. In the event of uncertainties as to whether an article should be included, the reviewers erred strictly on the side of the inclusion criteria. The decision to either include or exclude such articles was made after agreements were reached between the two independent reviewers.
The final screening process commenced when all included articles were established. The two reviewers independently screened the full-text articles for further relevance based on studies’ population, exposure/risk and outcomes (PEO).Citation30 Articles were further excluded, with reasons, where the main text failed to provide relevant information to achieve the objective of the study. Potential articles to be included in the study were assigned a mutually agreed unique code, to facilitate further assessment.
Data extraction
A standardised form was generated for the study using some generic items and relevant information unique to the study. Details on the form included: author(s) name(s), year of publication, characteristics of respondents, sampling technique, study area, and findings/results of the studies. The two independent reviewers sifted this information concurrently. Differences in opinions regarding some risk factors were resolved by agreement. Finally, to ensure validity and reliability of the instrument, the form was pre-tested on three different studies before adopting it for data extraction.
Setting
The Ashanti Region is the third largest of the 16 regions in Ghana. With a total land surface area of 24,389 km2, the region occupies about 10% of the total land surface area of the country.Citation31 Even though the region has the largest population among the other regions, Kumasi, which is its capital, accounts for nearly one-third of the region's population. The region has a population density of 148.1 persons per square kilometre.Citation31 In terms of vegetation, it is located in the moist semi-deciduous forest belt. However, due to the rapid rate of urbanisation, climate change and bush burning, the north-eastern part of the region has been reduced to guinea savanna.Citation31 Due to the region's abundant mineral and agricultural resources, coupled with its strategic geographical location (between longitude 0.15W and 2.25W, and latitude 5.50N and 7.46N) and spatial interaction with other regions, it is largely referred to as the business hub of the country.Citation32
Despite its population density, Katey et al.Citation33 and Ashiagbor et al.Citation34 found that access to health facilities is one of the major problems facing its people. However, access to primary health care facilities has been judged as very efficient. Information on the levels of educational attainment and literacy show that between 40.0% and 50.0% of the population in the region, particularly females, either have no formal education or have only pre-school education.Citation34 The proportion of the population with basic education varies from 67.7% in the Kumasi metropolis to 86.9% in the Amansie West District.Citation31
Results
Literature search
Literature searches carried out in the four bibliographic databases produced a total of 253 results (PubMed = 27; CINAHL = 53; Scopus = 124; Web of Science = 49). A total of 15 articles were also retrieved through snowballing (= 6); hand searching (= 8); and grey literature (= 1). Therefore, in all, a total of 268 articles were retrieved. Of these, 45 were identified as duplicates and hence were excluded, leaving a total of 223 articles for the first phase of the screening process (screening for title and abstract relevance). At this stage, a total of 192 reports were also excluded as neither their titles nor abstracts contained any useful information as far as the objective of the study was concerned, leaving 31 articles for further screening. The next phase of the screening process commenced with the downloading and screening of the 31 full-text articles. After a series of attempts, including emailing authors for full-text articles as well as using Find@UNC online literature search platform, 19 full-text articles were retrieved and assessed for eligibility. At the end of the screening process, 12 articles met all the inclusion criteria and thus were included in the final analysis.
Summary of included articles
Of the 12 articles, 10 employed probability sampling techniques (7 simple random, 3 multistage stratified) while 2 employed a convenient sampling method (see for details). Three of the studies were nationwide surveysCitation35–37 while the remaining 9 were all study-area specific. The minimum age of respondents was 18 years with the maximum age being 40 years and above. In terms of spatial distribution, some of the studies were conducted in rural communities of Adankwame,Citation22 Akwaaduo and DenyaseCitation19, Citation25 whereas others were conducted in urban centres of the Kumasi Metropolis,Citation21,Citation23,Citation38 Oforikrom Sub-MetroCitation26 and Obuasi Municipal.Citation19
All studies conducted in rural parts of the Ashanti Region found an increasing rate of diabetes among older adults.Citation19,Citation25 However, in terms of gender disparity, Addo et al.Citation25 found the prevalence of diabetes to be higher in females than in their male counterparts, particularly in females with higher levels of education. This finding is slightly different from what Sarfo-Kantanka et al.Citation21 found in the Kumasi Metropolis, which indicated diabetes prevalence in both males and females as grossly underpinned by increasing age and body mass. In their nationwide survey, Minicuci et al.Citation37 found diabetes prevalence in women to be higher than in their male counterparts at a rate of 4.4% and 3.2% respectively. However, a later study conducted by Agbogli et al.Citation26 noted that diabetes prevalence was similar in both males and females.
In terms of risk factors, Addo et al.,Citation25 Agbogli et al.,Citation26 Gatimu et al.,Citation35 Tarekegne et al.Citation36 and Titty et al.Citation38 all found changing psychosocial risk factors to be major risk factors of diabetes among older adults in the Ashanti region. Aikins et al.Citation19 also found factors such as unhealthy dietary pattern, overeating and high alcohol consumption to be prominent among adult diabetic patients. Agbogli et al.,Citation26 Danquah et al.,Citation23 Frank et al.,Citation39 Minicuci et al.Citation37 and Tarekegne et al.Citation36 all found obesity and high intake of sweets, meat and starchy vegetables (corn and peas) also to be high risk factors for diabetes. Some studies also found a high rate of physical inactivity among diabetic patients.Citation35,Citation36 Whereas diabetes has been judged as predominant among obese patients in the region, Danquah et al.Citation23 found that the disease is more prevalent among obese patients with low socioeconomic standing than in patients with high socioeconomic standing. However, Tarekegne et al.Citation36 found a higher prevalence among people with high socioeconomic standing (financially) and also among people with high levels of education. They further ascertained that diabetic patients who were employed were 0.45 times more likely to report diabetes diagnoses and treatments compared with unemployed diabetic patients. It has also been established that urban residents are more susceptible to type 2 diabetes as compared with their rural counterparts.Citation36,Citation37,Citation39 Doherty et al.Citation24 also found a high level of diabetes knowledge among patients with diabetes as well as high adherence to diabetes management precautions in the region.
Discussion
With the overriding objective of ascertaining and examining the most common risk factors for type 2 diabetes among older adults in the Ashanti Region of Ghana, this study systematically reviewed 12 articles that met certain predefined inclusion criteria. Findings from the study are discussed below.
Physical inactivity as a risk factor for type 2 diabetes
From the extensive literature review, physical inactivity has generally been identified as the predisposing risk factor for diabetes mellitus among adults in the region. This could be explained by the high concentration of the region's population in urban areas, particularly in Kumasi, which is the second largest metropolitan agglomeration in the country. According to the Ghana Statistical Service (GSS) report,Citation40 about 53.5 of the region's population live in urban areas. As a result of this, most people are engaged in commercial activities which are sedentary in nature.Citation19 According to Gato et al.,Citation41 most market women and people employed in the formal sector spend more than half of their active hours sitting down at workplaces and in the domestic environment. This has also been identified as a major cause of type 2 diabetes mellitus in the Ho Municipality of Ghana.Citation42
Obesity as a risk factor
Furthermore, obesity has also been identified as a prevalent risk factor for the disease among adult Ghanaians in the Ashanti Region. This could be as a result of the prevalent rate of obesity in the region (43.4%), a rate that is nearly equal to the national prevalence rate of 45.6%.Citation13 This can be explained by the recent rate of urbanisation in the region, which has led to several lifestyle and behavioural changes: sedentary socioeconomic activities and patronage of processed foods, among others. This underpinned the finding by Obirikorang et al.Citation43 of lifestyle changes as the major precursor of obesity in the region. Lifestyle changes are largely influenced by socioeconomic standing, hence the confirmation of the finding by Tarekegne et al.Citation36 that people living in urban areas are more susceptible to type 2 diabetes than their rural counterparts.
Prevalence of type 2 diabetes mellitus among adults in the Ashanti region
Regarding prevalence of diabetes, it has been established that type 2 diabetes is more prevalent in urban centres than in rural areas. Even though the national prevalence rate is only 2.5,Citation1 the average rate established in the literature within the Ashanti region is 3.8,Citation19,Citation37,Citation38 which is higher than the national average. This could be as a result of the predominance of the psychosocial risk factors in urban centres of the region.Citation19 Gudjinu and SarfoCitation14 intimated that due to the high cost of living in urban centres, people tend to spend more time working with little consideration of their eating habits. As a result, most adults finish work late, which eventually leads them to taking their supper late. This, coupled with a high intake of junk, processed and fast foods, weakens the immune systems of the majority thereby making them vulnerable to obesity, a key risk factor for diabetes. On the other hand, rural people, due to their active engagement in agrarian economic activities, are more physically active than their urban counterparts.Citation43 This explains their reduced vulnerability to type 2 diabetes in the region. However, it has also been reported that there is high adherence to diabetes management precautions in urban areas of the region as compared with rural areas.Citation24 This could be the result of the generally high levels of education in urban Ghana as compared with rural areas. The finding of diabetes being more prevalent in urban areas of the study area is in line with the findings of Asamoah-Boaheng et al.Citation12, Schulze et al.Citation44 and Vuvor et al.Citation45.
The prevalence of diabetes among females across the rural and urban milieus of the region has also been evident in the literature. The primary reason could be the result of the higher population of women than men in the region.Citation40 Cultural values and belief systems that recognise men as the head of families among all Akan tribes place the charge on men to be benefactors to their families. As a result, most men are associated with rigorous socioeconomic activities that are nomadic in nature. According to Asamoah-Boaheng et al.Citation12 and Obirikorang et al.,Citation43 their engagement in such activities reduces their risk and vulnerability to type 2 diabetes. On the other hand, females (particularly those in urban areas) engage largely in sedentary lifestyle activities such as food vending, provision store operations, babysitting and banking, among others.Citation25 Some of these activities have been reported as major causes of diabetes among adults in the region. Women are also regarded as baby-makers, hence are largely confined to homes and kitchens in some urban and rural communities in the region.Citation35,Citation37 This finding corroborates that of Asare-Anane et al.Citation46 and Bawah et al.,Citation42 who also identified a high prevalence of type 2 diabetes among urban females in Ghana. Despite this, the literature has expanded knowledge on the high susceptibility of urban dwellers to the disease. This can be attributed to the high rate of urbanisation in the region, coupled with changing socioeconomic status. According to Songsore,Citation47 the Ashanti region has one of the fastest rates of urbanisation in the country (53.2%), which is above the national average of 43.2%. Addo et al.Citation25, Aikins et al.Citation19 and Gato et al.Citation41 all identified the close association between increasing socioeconomic status (in terms of education and income levels) and the risk of developing type 2 diabetes mellitus.
Conclusion
As a result of the predominance of psychosocial risk factors of diabetes, specifically physical inactivity and obesity, in the Ashanti region of Ghana, there is a need for intensified public awareness creation on the menace of this disease in the region. All key stakeholders in the health sector, including the Ministry of Health and Ministry of Information in conjunction with media houses and governments at the local levels, have the responsibility to educate the entire population on diabetes, and its prevention, management and the available interventions. This would go a long way to help achieve massive reduction in diabetes cases in Ghana. Women also need to be educated on the need to exercise their bodies regularly to facilitate a reduction in their chances of developing type 2 diabetes. Finally, as part of adolescent education, there is a need to teach young people to avoid certain lifestyle choices such as smoking, excessive intake of alcohol, and too much intake of processed and fatty foods, which could predispose them to type 2 diabetes in old age.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- International Diabetes Federation [IDF]. What is diabetes. (2020). [cited 16 April 2021]. p. 1. https://www.idf.org/aboutdiabetes/what-is-diabetes.html.
- World Health Organization [WHO]. Diabetes. (2021). [cited 16 April 2021]. p. 1. https://www.who.int/news-room/fact-sheets/detail/diabetes.
- Mbaye MN. I.17 The diabetes Africa foot initiative (DAFI). Diabetes Res Clin Pract. 2014;103; https://doi.org/10.1016/s0168-8227(14)70018-x.
- Zimmet PZ. Diabetes and its drivers: The largest epidemic in human history? Clin Diabetes Endocrinol. 2017;3: Article #1. https://doi.org/10.1186/s40842-016-0039-3.
- International Diabetes Federation. Diabetes at a glance Middle East and North Africa, 2019. [cited 16 April 2021] https://www.idf.org/our-network/regions-members/middle-east-and-north-africa/diabetes-in-mena.html.
- Morgan AK, Cobbold J, Awafo BA, et al. COVID-19 and psychological distress among older adults in Ghana. In: Gabrielli F, Irtelli F, editors. Anxiety, uncertainty, and resilience during the pandemic period. London: Intechopen; 2021. p. 1–19.
- Aranda S. Ten threats to global health in 2019. World Health Organization. 2019; [cited 21 March 2021] https://www.one.org/international/blog/global-health-in-2019/.
- Arnett DK, Blumenthal RS, Albert MA, et al. ACC/AHA Guideline on the primary prevention of cardiovascular disease. J Am Coll Cardiol. 2019;74:e177–e232. https://doi.org/10.1016/j.jacc.2019.03.010.
- Thomas RL, Halim S, Gurudas S, et al. IDF diabetes atlas: A review of studies utilising retinal photography on the global prevalence of diabetes related retinopathy between 2015 and 2018. Diabetes Res Clin Pract. 2019;157: Article #107840. https://doi.org/10.1016/j.diabres.2019.107840.
- International Diabetes Federation [IDF]. The IDF Africa Region. International Diabetes Federation. 2015. [cited 21 March 2021] https://idf.org/our-network/regions-members/africa/welcome.html.
- Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388: article #10053. https://doi.org/10.1016/S0140-6736(16)31012-1.
- Asamoah-Boaheng M, Sarfo-Kantanka O, Tuffour AB, et al. Prevalence and risk factors for diabetes mellitus among adults in Ghana: A systematic review and meta-analysis. Int Health. 2019;11(2):83–92.
- Nomah DK. Prevalence of Hypertension, Obesity, and Diabetes in Rural Ghana: a cross-sectional study in the Birim central district of Ghana. 2019. [cited 21 March 2021] https://www.isglobal.org/documents/10179/8136729/Daniel/de5ce834-93d8-4058-974d-2981cfa33c5d.
- Gudjinu HY, Sarfo B. Risk factors for type 2 diabetes mellitus among out-patients in Ho, the volta regional capital of Ghana: A case-control study. BMC Res Notes. 2017;10(1):1–10.
- Atun R, Davies JI, Gale EAM, et al. Diabetes in sub-Saharan Africa: from clinical care to health policy. Lancet Diabetes Endocrinol. 2017;5(8):622–667.
- Shen J, Kondal D, Rubinstein A, et al. A multiethnic study of Pre-diabetes and diabetes in LMIC. Glob Heart. 2016; https://doi.org/10.1016/j.gheart.2015.12.015.
- Amoah AG, Owusu SK, Adjei S. Diabetes in Ghana: A community based prevalence study in Greater Accra. Diabetes Res Clin Pract. 2002;56(3):197–205.
- Amoah AG, Owusu SK, Saunders JT, et al. Facilities and resources for diabetes care at regional health facilities in southern Ghana. Diabetes Res Clin Pract. 1998;42(2):123–130.
- Aikins ADG, Id A, Dodoo F, et al. Knowledge and perceptions of type 2 diabetes among Ghanaian migrants in three European countries and Ghanaians in rural and urban Ghana: The RODAM qualitative study. PLoS ONE. 2019;14(4):1.
- Aikins ADG. Living with diabetes in rural and urban Ghana: A critical social psychological examination of illness action and scope for intervention. J Health Psychol. 2003;8(5):557–572.
- Sarfo-Kantanka O, Owusu-Dabo E, Adomako-Boateng F, et al. An assessment of prevalence and risk factors for hypertension and diabetes during world diabetes day celebration in kumasi, Ghana. East Afr J Public Health. 2014;11(2):805–815.
- Cook-huynh M, Ansong D, Steckelberg RC, et al. Prevalence of hypertension and diabetes mellitus in adults from a rural community in Ghana. Ethn Dis. 2012;22(3):347–352.
- Danquah I, Bedu-addo G, Terpe K, et al. Diabetes mellitus type 2 in urban Ghana: characteristics and associated factors. BMC Public Health. 2012;12(1):210.
- Doherty ML, Owusu-Dabo E, Kantanka OS, et al. Type 2 diabetes in a rapidly urbanizing region of Ghana, West Africa: A qualitative study of dietary preferences, knowledge and practices. BMC Public Health. 2014;14(1):1–8.
- Addo J, Agyemang C, de-Graft Aikins A, et al. Association between socioeconomic position and the prevalence of type 2 diabetes in Ghanaians in different geographic locations: The RODAM study. J Epidemiol Community Health. 2017;71(7):633–639.
- Agbogli HK, Annan R, Agyeman-Duah E, et al. Prevalence and risk factors of diabetes mellitus Among the inhabitants of Kumasi metropolis. Arch Clin Biomed Res. 2017;1(4):224–234.
- Wohlin C. Guidelines for snowballing in systematic literature studies and a replication in software engineering). EASE ’14: Proceedings of the 18th International Conference on Evaluation and Assessment in Software Engineering, 2014; Article # 38, p 1–10. https://doi.org/10.1145/2601248.2601268.
- Saleh K. The Health Sector in Ghana. The Health Sector in Ghana. 2012. https://doi.org/10.1596/978-0-8213-9599-8.
- United States Preventive Services Task Force [USPSTF]. USPSTF Procedure Manual. 2015 [cited 3 April 2021] https://www.uspreventiveservicestaskforce.org/uspstf/sites/default/files/inline-files/procedure-manual-2020_3.pdf.
- Kestenbaum B. Population, exposure, and outcome. In: Epidemiology and biostatistics. Cham; Springer International Publishing; 2019 [cited 3 April 2021]. p. 5–6. https://link.springer.com/chapter/10.1007/978-3-319-97433-0_2.
- Modern Ghana. Ghana Ashanti region. 2018. p. 1–34. https://www.modernghana.com/GhanaHome/regions/ashanti.asp?menu_id=6.
- Abass K, Afriyie K, Gyasi RM. From green to grey: the dynamics of land use / land cover change in urban Ghana. Landsc Res. 2018;44(8):909–921. https://doi.org/10.1080/01426397.2018.1552251.
- Katey D, Morgan AK, Asori M, et al. COVID-19 and the marginalized: an opinion piece on further measures to address COVID-19 in prisons in Sub-Saharan Africa. Int J Prison Health. 2021;17(3):373–379. https://doi.org/10.1108/IJPH-12-2020-0101.
- Ashiagbor G, Ofori-Asenso R, Forkuo EK, et al. Measures of geographic accessibility to health care in the Ashanti region of Ghana. Sci African. 2020;9:e00453. https://doi.org/10.1016/j.sciaf.2020.e00453.
- Gatimu SM, Milimo BW, Sebastian MS. Prevalence and determinants of diabetes among older adults in Ghana. BMC Public Health. 2016;16: article #1174. https://doi.org/10.1186/s12889-016-3845-8.
- Tarekegne FE, Padyab M, Schröders J, et al. Sociodemographic and behavioral characteristics associated with selfreported diagnosed diabetes mellitus in adults aged 50 + years in Ghana and South Africa: Results from the WHOSAGE wave 1. BMJ Open Diabetes Res Care. 2018;6(1):1–11. http://doi.org/10.1136/bmjdrc-2017-000449.
- Minicuci N, Biritwum RB, Mensah G, et al. Sociodemographic and socioeconomic patterns of chronic non-communicable disease among the older adult population in Ghana. Glob Health Action. 2014;7(1): article 21292. https://doi.org/10.3402/gha.v7.21292.
- Titty FK, Agyei-Frempong MT, Owiredu WKBA. Clinical and demographic characteristics of Ghanaian patients with diabetes mellitus. Ghana J Sci. 2011;51:57–63.
- Frank LK, Kröger J, Schulze MB, et al. Dietary patterns in urban Ghana and risk of type 2 diabetes. Br J Nutr. 2014;112(1):89–98.
- Ghana Statistical Service [GSS]. District Analytical Report, Kumasi Metropolitan Assembly. Accra,Ghana; 2014. https://en.wikipedia.org/wiki/Kumasi_Metropolitan_Assembly.
- Gato WE, Acquah S, Apenteng BA, et al. Diabetes in the cape coast metropolis of Ghana: An assessment of risk factors, nutritional practices and lifestyle changes. Int Health. 2017;9(5):310–316.
- Bawah AT, Abaka-Yawson A, Seini MM, et al. Prevalence of diabetes among homeless and slum dwellers in Accra, Ghana: A survey study. BMC Res Notes. 2019;12(1):1–5.
- Obirikorang C, Osakunor DNM, Anto EO, et al. Obesity and cardio-metabolic risk factors in an urban and rural population in the Ashanti region-Ghana: A comparative cross-sectional study. PLoS One. 2015;10(6):1–13.
- Schulze MB, Bedu-addo G, Mockenhaupt FP, et al. Dietary patterns in urban Ghana and risk of type 2 diabetes British journal of nutrition. Br J Nutr. 2014;112:89–98. https://doi.org/10.1017/S000711451400052X.
- Vuvor F, Steiner-Asiedu M, Armar-Klemesu M, et al. Population-based study of diabetic mellitus prevalence and its associated factors in adult Ghanaians in the Greater Accra region. Int J Diabetes Dev Ctries. 2011;31(3):149–153.
- Asare-Anane H, Bawah AT, Ofori EK, et al. Risk factors for gestational diabetes mellitus among Ghanaian women at the korle-Bu Teaching hospital. J Biol Agric Healthc. 2014;4(12):54–57.
- Songsore J. The Urban Transition in Ghana: Urbanization, National Development and Poverty Reduction. Legon-Accra: University of Ghana. 2009; pp. 1–71.