
Abstract
The main aim of this study was to investigate if exercisers' personality characteristics were associated with exercise dependence. Specifically, the purpose was to examine if anxiety, obsessive passion, and physical appearance orientation were associated to an increased risk for exercise dependence. Participants were 330 exercisers from exercise groups, sport clubs and university sport science classes in the southwest of Sweden. Data were analysed using CHAID (Chi-squared Automatic Interaction Detection) analysis. The CHAID analysis indicated that anxiety was the main predictor of exercise dependence. More specifically, 12.7% more exercisers who experienced high levels of anxiety symptoms (i.e. scores above 6), were, in comparison to the exercises experiencing low levels of anxiety, classified as “at risk for exercise dependence”. For exercisers that reported low levels of anxiety symptoms (i.e. scores below 7), obsessive passion for exercise was a positive statistically significant predictor (absolute risk difference = 8.6%). Overall, the results highlight anxiety as a main risk factor behind exercise dependence. Also, the risk of exercise dependence may increase either from obsessive passion or as a coping strategy for anxiety. Furthermore, results may illustrate two types of exercise dependence; “primary” exercise dependence driven mainly by an obsessive passion for exercise and “secondary” exercise dependence where exercise function as a strategy to cope with anxiety.
Introduction
Exercise dependence is described as a maladaptive pattern of exercise that is characterised by excessive amounts of exercise that may increase the risk for developing mental health problems such as depression (Hausenblas & Symons Downs, Citation2002a). Exercise dependence may be a widespread problem and recent research indicates that 7% of exercisers and 9% of athletes may be at risk (Marques et al., Citation2018). In another study, 6.2% of exercisers were at risk of becoming exercise dependent whereas 38.1% were classified as nondependent-symptomatic exercisers (Mónok et al., Citation2012). However, in some populations, as much as 42% of nonprofessional athletes have been estimated to be at risk for developing exercise dependence (Lejoyeux, Avril, Richoux, Embouazza, & Nivoli, Citation2008). Due to the potentially detrimental health effects of exercise dependence, knowledge about risk factors in its development is important.
Common documented symptoms of exercise dependence are (1) increased tolerance for exercise, (2) withdrawal symptoms, (3) longer and more frequent exercise sessions than initially intended, (4) lack of control over exercise habits, (5) excessive time spent exercising, (6) important social, occupational or recreational activities are given up or neglected in favour of exercise, and (7) exercise routine continues despite recurrent physical or psychological problems (Hausenblas & Symons Downs, Citation2002b). According to the Cognitive Appraisal Hypothesis (CAH) exercisers may use exercise as a strategy of coping with acute or chronic stress (Szabo, Citation1995). Similarly, the proposed interactional model emphasises that the development of excessive exercise habits may be initiated by “sudden or progressively intolerable life stress” (Egorov & Szabo, Citation2013, p. 205) where the major underlying motive for exercising is to reduce psychological pain, related to the stressful life event. In that sense, exercise functions as a therapeutic tool to increase (or maintain) mental health (Egorov & Szabo, Citation2013). People who already exercise for therapeutic reasons (e.g. to improve general health and/or prevent ill health) may be especially prone to use exercise as a tool to reduce life stress and anxiety (Egorov & Szabo, Citation2013). Moreover, if the exerciser, for some reason, is prevented from exercising, physical discomfort, distress, feelings of guilt and lowered self-esteem, are often experienced (Kerr, Lindner, & Blaydon, Citation2007). Consequently, the individual develops a strong need for exercise to maintain overall wellbeing and eventually life becomes dominated by exercise, often at the expense of family, social life, and work. In line with CAH, the Transient Hypofrontality Hypothesis (THH; Dietrich, Citation2006) suggests that physical exercise requires larger neural activation, which in turn, results in decreased neural activity in brain structures (e.g. the prefrontal cortex) that are less involved in such dynamic bodily movements. Thus, during exercise the neural activation in the prefrontal cortex is temporarily decreased. As a result, activities in brain areas associated with stress (i.e. the prefrontal cortex), anxiety, and negative moods are reduced during exercise, suggesting that exercise may provide a break from anxious thoughts and feelings. Whereas CAH and THH suggest an explanation for the maintenance of exercise dependence, they do not describe the specific factors that predict the use of exercise as a coping strategy (i.e. which factors characterise an individual who becomes exercise dependent) (Egorov & Szabo, Citation2013).
To develop effective intervention programs to prevent exercise dependence it is important to, first, identify risk factors. Several potential risk factors have been proposed in the current literature regarding exercise dependence. Specifically, anxiety and obsessive-compulsive behaviours (Grandi, Clementi, Guidi, Benassi, & Tossani, Citation2011; Gulker, Laskis, & Kuba, Citation2001) as well as body image disturbances (e.g. a strong urge to achieve body ideals) have been suggested as risk factors of exercise dependence (Hausenblas & Giacobbi Jr, Citation2004; Landolfi, Citation2013; Schreiber & Hausenblas, Citation2015). In general, previous studies have indicated that excessive exercise and exercise dependence are associated with anxiety in general as well as in exercise populations (e.g. Costa, Hausenblas, Oliva, Cuzzocrea, & Larcan, Citation2013; Ogden, Veale, & Summers, Citation1997; Spano, Citation2001). Moreover, exercisers defined as exercise dependent reported significantly higher levels of anxiety than non-exercise dependent exercisers (Grandi et al., Citation2011). Obsessive-compulsive behaviours are also shown to be significantly associated with excessive exercise (Landolfi, Citation2013; Schreiber & Hausenblas, Citation2015; Young, Rhodes, Touyz, & Hay, Citation2013).
One framework used to explain excessive exercising behaviours is the motivational construct of passion (Vallerand et al., Citation2003). Passion has been described as a motivational force and has been defined as “inclination toward an activity that people like, find important, and in which they invest time and energy” (Vallerand, Citation2008, p. 1). A passionate activity is self-defining to the individual and internalised as a central feature of the individual’s identity (Vallerand et al., Citation2003). As introduced by Vallerand et al. (Citation2003), the dualistic model of passion (DMP), postulates that passion can be divided into harmonious and obsessive passion. In harmonious passion the individual engages in an activity willingly and autonomously, and the involvement is not affecting other aspects of life negatively. In contrast, obsessive passion is characterised by intra- and/or interpersonal pressure to engage in the activity (e.g. feelings of self-esteem or social acceptance are attached to the activity) and feelings of guilt or anxiety when prevented from participating in the activity.
Specifically, obsessive passion for exercise is related to a higher frequency of strenuous exercise (e.g. Parastatidou, Doganis, Theodorakis, & Vlachopoulos, Citation2012). Similarly, whilst obsessive passion is positively associated with exercise intensity and exercise volume, harmonious passion is negatively related to these exercise outcomes in long-term exercisers (Kovacsik, Griffiths, et al., Citation2018). Moreover, Paradis, Cooke, Martin, and Hall (Citation2013) found that obsessive passion predicted all symptoms of exercise dependence (i.e. tolerance, withdrawal, intention effects, lack of control, time, reduction in other activities and continuance). Furthermore, several studies have shown that obsessive passion predicts exercise dependence in both competitive athletes and regular exercisers (i.e. de la Vega, Parastadiou, Ruíz-Barquín, & Szabo, Citation2016; Kovacsik, Soós, de la Vega, Ruíz-Barquín, & Szabo, Citation2018). In addition, Sicilia, Alcarez-Ibáñez, Lirola, and Burgueño (Citation2017) found that obsessive passion positively mediated the relation between exercise goal content and exercise dependence whereas harmonious passion acted as a negative mediator in this particular relationship. In sum, passion, especially obsessive passion, may serve as an important risk factor for the development of exercise dependence among regular exercisers (e.g. Kovacsik, Griffiths, et al. Citation2018; Parastatidou et al., Citation2012).
Exercise dependence may also be associated with a strong striving for physical attractiveness. Particularly, body dissatisfaction is related to exercise dependence symptoms (Schreiber & Hausenblas, Citation2015). The desire to achieve body ideals and the rewards of being looked upon as attractive may lead people to try to change their body size and shape by strenuous exercise (Hausenblas & Fallon, Citation2006). Also, Landolfi (Citation2013) states that physically appearance oriented people who place too much emphasis on body ideals tend to exercise excessively in order to sustain or pursue what they perceive as the perfect body.
In sum, theoretical models of exercise dependence, such as the CAH (Szabo, Citation1995) and the interactional model (Egorov & Szabo, Citation2013) both suggest that exercise may function as a tool to cope with life stress and anxiety. Previous studies have also highlighted anxiety (Costa et al., Citation2013), obsessive exercise behaviours (Paradis et al., Citation2013), and striving for body ideals (e.g. Schreiber & Hausenblas, Citation2015) as potential risk factors for developing exercise dependence. Given this background, the overall aim of the current study was to examine if anxiety, obsessive passion, and physical appearance orientation were associated with an increased risk for exercise dependence. Based on potential risk factors (anxiety, obsessive passion, and physical appearance orientation) that may influence the emergence of exercise dependence, the specific purpose of the study was to develop a model for the identification of persons at risk for exercise dependence.
Based on aforementioned theories (Egorov & Szabo, Citation2013; Szabo, Citation1995) and previous research (e.g. Costa et al., Citation2013; Landolfi, Citation2013; Paradis et al., Citation2013), it was hypothesised that high levels of anxiety, obsessive passion and physical appearance orientation would increase the risk for exercise dependence.
Method
Participants
The participants were 330 exercisers (162 males and 168 females) from exercise groups, sport clubs and university sport science classes in the southwest of Sweden. Participants were between 18 and 60 years of age (M = 30.10, SD = 10.571). Participants main sports included table tennis (n = 2), crossfit (n = 4), cycling (n = 17), dance (n = 3), soccer (n = 11), running (n = 82), golf (n = 1), gym training (n = 69), floor-ball (n = 5), orienteering (n = 31), swimming (n = 5) and triathlon (n = 12), the rest (n = 88) did not specify a main sport.
Exercise groups, sport associations, and sport science classes at a university, were approached by e-mail with information about the study and an invitation to participate in the study.
Meetings were set up with the groups that were initially interested in taking part in the study. At the meetings the study was presented for the exercisers and they were given information that the data would be treated confidentially, and that they had the right to withdraw from the study at any time. Each participant also got a letter of informed consent to sign. The study was approved by the University ethics committee (UI 2016/440). (See for respondents' exercise characteristics.)
Table 1. Descriptive and coefficient alphas of the study variables (n = 330).
Measures
Godin leisure-time exercise questionnaire (GLTEQ)
The GLTEQ (Godin & Shephard, Citation1985) consists of four questions that track the individual’s leisure time physical activity. The instrument measures frequency of activity per week with regards to strenuous, moderate and mild intensity and whether the individual exercises regularly (e.g. “During a typical 7-Day period (a week), how many times on the average do you do the following kinds of exercise for more than 15 min during your free time?”). Exercise frequency and intensity is calculated and analysed as a total score by summing the products of the separate components, as shown in the following formula; weekly leisure activity score = (9 × Strenuous) + (5 × Moderate) + (3 × Light). Strenuous exercise thus produces higher values than moderate exercise and moderate exercise gives higher values than mild exercise. Overall, high values indicate large amounts of exercise. The item considering how regularly the individual exercises is analysed separately (Godin & Shephard, Citation1985). In addition to GLTEQ we asked questions about average number of workouts per week (“On average, how many times per week do you work out?”), average length of workout (“On average, how many minutes does your workouts usually last?”) and average intensity of workout (“On average, what is the intensity of your workout sessions?”). The GLTEQ and additional questions regarding exercise habits were used for descriptive statistics.
Exercise dependence scale revised (EDS-R)
Exercise dependence was measured with a Swedish version (Lindwall & Palmeira, Citation2009) of the 21-item EDS-R (Symons Downs, Hausenblas, & Nigg, Citation2004). EDS-R is a multidimensional measure of exercise dependence based on the criteria for substance dependence in the American Psychiatric Association’s Diagnostic and Statistical Manual for Mental Disorders IV (DSM-IV); tolerance (e.g. “I continually increase my exercise frequency to achieve the desired effects/benefits”), withdrawal (e.g. “I exercise to avoid feeling irritable”), intention effect (e.g. “I exercise longer than I intend”), lack of control (e.g. “I am unable to reduce how long I exercise”), time (e.g. “I spend most of my free time exercising”), reductions in other activities (e.g. “I would rather exercise than spend time with family/friends”), continuance (e.g. “I exercise when injured”). Each statement is rated from 1 (never) to 6 (always) and higher scores indicate greater severity of exercise dependence symptoms. In addition, EDS-R may be used to categorise individuals as “at-risk for exercise dependence”, “nondependent symptomatic” or “nondependent asymptomatic”. To be classified into the at-risk for exercise dependence group, respondents have to score on average 5–6 on three of the seven DSM IV criteria. Individuals that score 3–4 on average (or 5–6 on some factors but fail to meet the criteria for the at-risk group) on a minimum of three factors are categorised as nondependent symptomatic. Respondents that score on average 1–2 on at least three of the factors are classified as nondependent asymptomatic. The Swedish version of the EDS-R has demonstrated good psychometric properties in previous studies (Lindwall & Palmeira, Citation2009). Cronbach’s alpha for the total scale was 0.86 in the current study.
Hospital anxiety and depression (HAD)
General anxiety was measured with HAD (Zigmond & Snaith, Citation1983), a 14-item instrument developed for screening for clinically significant anxiety and depression among medical patients outside psychiatry. HAD consists of two subscales; anxiety (HAD-A) (e.g. “I feel tense or wound up”) and depression (HAD-D) (e.g. “I have lost interest in my appearance”) on a four-point scale with range 0 (never) to 3 (always). In this study, only the 7-item subscale for anxiety (HAD-A) was used. According to the HAD-A scores between 0 and 6 indicate no symptoms of anxiety, scores from 7 to 10 mild to moderate anxiety and scores above 10 a potential anxiety disorder. In the main analysis we used a dichotomous variable where scores below 7 were considered as low level (coded as 0) of anxiety and equal or above 7 were considered as high level of anxiety (coded as 1).
The HAD-scale is a widely used instrument for assessing symptoms and severity of anxiety in both clinical and non-clinical populations and has demonstrated good validity and reliability in a large number of previous studies (see Bjelland, Dahl, Haug, & Neckelmann, Citation2002, for an overview of psychometric properties of HAD). In the present study, Cronbach’s alpha for the HAD-A scale was 0.82.
The passion scale (TPS)
The Passion Scale (Vallerand et al., Citation2003) was used to measure participants' passion for exercise. TPS includes two subscales measuring harmonious passion (e.g. “Exercise is in harmony with other activities in my life”) and obsessive passion (e.g. “I have a tough time controlling my need to exercise”). Responses are provided on a scale ranging from 1 (do not agree at all) to 7 (completely agree). Higher scores indicates higher levels of passion. In the present study, only the 6-item subscale for obsessive passion was used. The Swedish version of TPS (Gustafsson, Hassmén, & Hassmén, Citation2011) has been found to have acceptable internal consistency; in this study, Cronbach’s alpha was 0.86.
Multidimensional body-self relations questionnaire (MBSRQ)
To assess physical appearance orientation, the appearance orientation subscale of MBSRQ (Brown, Cash, & Mikulka, Citation1990; Cash, Citation2000) was used. The appearance orientation subscale is a 12-item scale on a five-point Likert scale (ranging from 1 strongly disagree to 5 strongly agree). Scale scores are calculated as means of constituent items. Physical appearance orientation measures the individual’s degree of investment in one’s appearance (e.g. “It is important that I always look good”, “I am always trying to improve my physical appearance”, “I check my appearance in a mirror whenever I can”). High scorers pay more attention to how they look, invest a lot of energy in taking care of their appearance and engage in extensive grooming behaviours. Low scorers are indifferent to their appearance, the way they look is not very important to them and they put no energy in their looks (Cash, Citation2000). Consistent with previous studies MBSRQ may be considered a valid and reliable instrument for assessing self-attitudinal aspects of body image (Brown et al., Citation1990). In the current study, Cronbach’s alpha was 0.86 for the appearance orientation scale.
Procedure
Time and place for data collections were scheduled with the groups who agreed to participate. Data collections took place at various sports associations, fitness centres, and at a university. Athletes and exercisers filled out the questionnaires prior to or after training and exercise. University students filled out questionnaires during class. One of the authors was present at each data collection.
Analyses
First, descriptive statistics and bivariate correlations were calculated. Then we used a decision tree analysis; CHAID (Chi-squared Automatic Interaction Detection analysis) to investigate exercisers' characteristics that may predict exercise dependence. The CHAID analysis is used to investigate associations between predictors (in the present study; anxiety, obsessive passion and appearance orientation) and the outcome variable (in the present study; exercise dependence) by searching for the predictors that differ the most on the outcome variable (Önder & Uyar, Citation2017). The variable that best explains the dependent variable is selected and, according to the selected variable, the data is classified into subgroups. Each subgroup continues to generate more subgroups based on the most significant predictor until the last significant predictor is used. In comparison to the more commonly used linear regression analyses, the CHAID analysis has advantages in relation to identification of predictors (Bittencourt et al., Citation2016). More specifically, one limitation with the commonly used linear regression analysis is a reductionist approach where “a phenomenon has been simplified into units and analysed as the sum of its basics parts” (Bittencourt et al., Citation2016, p. 1309). Given the complex interaction between variables that might influence the risk for exercise dependence, the CHAID analysis is better suited to recognise patterns of non-linear interactions between the included risk factors (Ivarsson & Stenling, Citation2019). As a result, the analysis produces a tree diagram that displays homogenous groups of exercisers based on the observed levels of the predictors and outcome variable (Chan, Cheing, Chan, Rosenthal, & Chronister, Citation2006). For all analyses a p-value <.05 was considered to indicate statistically significant results. All analyses were conducted in the IBM SPSS Statistics version 24 (SPSS Inc., Chicago, IL, USA).
Results
Descriptive statistics
Descriptive statistics are presented in . Participants reported that they exercise regularly, about five times a week. Average duration of workout was stated to be approximately 70 min and average workout intensity was estimated to be around 70% of a maximal 100% (see ). Frequencies and percentages of participants' anxiety sum scores: 0–6 = no anxiety problems (n = 197, 59.7%), 7–10 = mild to moderate anxiety (n = 84, 25.5%), > 10 = potential anxiety disorder (n = 49, 14.8%).
Correlational analyses
Statistically significant correlations were found between exercise dependence and all exercise variables. Moreover, the results also showed that exercise dependence was statistically significantly related to both obsessive passion and physical appearance orientation (see ).
Table 2. Correlations of the study variables.
CHAID analysis
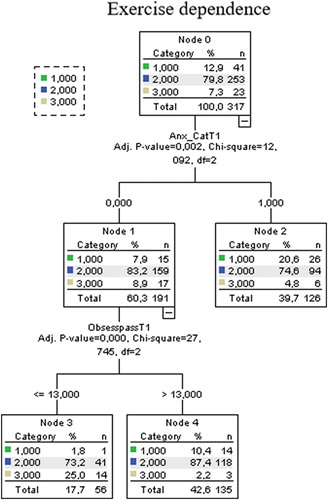
The association between exercisers' personality characteristics and exercise dependence was investigated using CHAID analysis. The CHAID decision tree analysis was completed with 2 branches and 4 nodes (see ). In the analysis, anxiety was found to be the main predictor of exercise dependence (x2 = 12.092, p = 0.002, df = 2). Specifically, 20.6% of exercisers who experienced anxiety were classified into the “at risk for exercise dependence” group whereas 7.9% of exercisers in the low anxiety group were categorised as “at risk for exercise dependence”. For exercisers who reported low levels of anxiety symptoms (scores below 7), obsessive passion for exercise was a positive statistically significant predictor (x2 = 27.745, p < 0.001, df = 2; absolute risk difference = 8.6%). Physical appearance orientation was not a significant predictor for exercise dependence and was, therefore, excluded in the model testing process. Among the “low anxiety exercisers”, 10.4% of the participants were classified as at risk for exercise dependence (in comparison to 1.8% of exercisers with low obsessive passion scores).
Figure 1. A CHAID decision classification tree analysis to identify predictors of exercise dependence. Note: For the exercise dependence groups, we used the following coding: 1 = at-risk for exercise dependence; 2 = nondependent symptomatic; 3 = nondependent asymptomatic.
Discussion
In an ambition to increase the understanding of the development of exercise dependence among exercisers and athletes, the major aim of the present study was to develop a model for the identification of persons at risk for exercise dependence. Overall, the key findings of the present study indicate that both anxiety and obsessive passion predict exercise dependence but anxiety was the main predictor, suggesting that especially anxiety poses an important risk for developing exercise dependence. Whereas the correlational analyses showed that exercise dependence was significantly related to physical appearance orientation, the CHAID analysis revealed that physical appearance orientation did not have a predictive ability when all three predictors were included simultaneously in the model.
In light of the CAH (Szabo, Citation1995), the interactional model (Egorov & Szabo, Citation2013) and the THH (Dietrich, Citation2006) a potential explanation of the relationship between exercise dependence and anxiety is that exercise may reduce activities in brain areas associated with stress, anxiety, and negative moods, making exercise a compelling coping strategy to control anxiety and worry (Dietrich, Citation2006). In the present study, approximately 25% experienced mild to moderate anxiety whilst as many as 15% were classified as having a potential anxiety disorder. The anxiety-reducing effect may eventually diminish, which means that the previous exercise dose needs to be increased in order to get the wanted effect. In addition, the experience of temporary stressful life-events may result in higher anxiety (Egorov & Szabo, Citation2013), that in turn, may generate a need to further extend the training programme (i.e. longer sessions and/or increasing levels of intensity). In general, theories of addiction and dependence often view addictive behaviour as a coping strategy to deal with stress, to reduce tension, and to self-medicate (Sinha, Citation2008). Similarly, excessive exercise may reflect an attempt to manage stress, worries and challenges in everyday life.
In line with previous studies that found obsessive passion as a predictor of exercise dependence (e.g. de la Vega et al., Citation2016; Kovacsik, Soós, et al., Citation2018), the results of the present study suggest that obsessive passion acts as a secondary predictor for exercise dependence. For exercisers who experience low levels of anxiety, an obsessive passion for exercise indicated an increasing risk for exercise dependence. A potential explanation may be that these obsessively passionate exercisers strongly identify themselves as serious “semi-professional” athletes, which may cause them to experience internal pressure to exercise, resulting in increasing difficulties to control exercise behaviours (e.g. choose to exercise instead of engaging in social activities) (Vallerand et al., Citation2003). Also, exercise may function as a way to strengthen and confirm this “professional” exercise identity, and in order to maintain this particular identity, exercise may eventually become compulsive. Additionally, they may experience negative emotions (e.g. guilt, shame, anxiety) on days when they are not able to exercise (Guérin, Fortier, & Williams, Citation2013; Vallerand et al., Citation2003), which in turn may result in an urge to extend exercise routines.
Previous research has suggested that people who place too much emphasis on body ideals and appearance tend to exercise excessively in order to pursue or maintain what they perceive as the perfect body (e.g. Landolfi, Citation2013). Even if physical appearance orientation was positively associated with exercise dependence, it was not a significant predictor of exercise dependence when analysed in a multiple model that also included obsessive passion and anxiety, suggesting that appearance orientation is not a key risk factor for exercise dependence. A potential explanation is that some risk factors may be more prominent in certain exercise activities while others play a less important role. In sports, where the main goal is to improve physical endurance (e.g. cycling, running, triathlon), anxiety may be a more important mechanism in the development of exercise dependence than physical appearance orientation. On the other hand, physical appearance orientation and striving for a specific body ideal may be more important in strength training (e.g. bodybuilding, athletic fitness, crossfit).
A possible interpretation of the results of the present study is that the risk of developing exercise dependence could increase either from obsessive passion or as a strategy to cope with anxiety. This could be linked to previous research on exercise dependence that suggests that exercise dependence may be understood as a primary (occurring on its own) or a secondary disorder (i.e. a weight management strategy for eating disorders) (Kerr et al., Citation2007; Veale, Citation1995). Hence, exercise dependence may be developed (i) as a “primary” disorder driven by an obsessive passion for exercise, or (ii) as a “secondary” disorder where exercise functions as a strategy to cope with anxiety.
Limitations
A limitation of the current study is the cross-sectional design that does not uncover causal relationships between exercise dependence and risk factors. Future studies could, therefore, continue to explore exercise dependence as a “primary” or a “secondary” disorder by investigating the relationship between exercise dependence and risk factors over time. In addition, qualitative studies would be helpful in the understanding of the development of primary and secondary exercise dependency in strength training as well as in endurance training.
Conclusions
Overall, the results of this study highlight anxiety as the main predictor of exercise dependence, indicating that anxiety, compared to obsessive passion, may be a more prominent risk factor in the development of exercise dependence. Relatedly, anxiety has been suggested as an important factor in the development and maintenance of behavioural addictions such as online gaming addiction (Mehroof & Griffiths, Citation2010), problem gambling (Barrault, Bonnaire, & Herrmann, Citation2017), and substance use disorders (Vorspan, Mehtelli, Dupuy, Bloch, & Lépine, Citation2015), indicating that anxiety is closely associated with a wide range of dependency symptoms and addictive behaviours.
Additional information
Funding
References
- Barrault, S., Bonnaire, C., & Herrmann, F. (2017). Anxiety, depression and emotion regulation among regular online poker players. Journal of Gambling Studies, 33(4), 1039–1050. doi: https://doi.org/10.1007/s10899-017-9669-3
- Bittencourt, N. F. N., Meeuwisse, W. H., Mendonca, L. D., Nettel-Aguirre, A., Ocarino, J. M., & Fonseca, S. T. (2016). Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition – narrative review and new concept. British Journal of Sports Medicine, 50, 1309–1314. doi: https://doi.org/10.1136/bjsports-2015-095850
- Bjelland, I., Dahl, A. A., Haug, T. T., & Neckelmann, D. (2002). The validity of the hospital anxiety and depression scale: An updated literature review. Journal of Psychosomatic Research, 52(2), 69–77. doi: https://doi.org/10.1016/S0022-3999(01)00296-3
- Brown, T. A., Cash, T. F., & Mikulka, P. J. (1990). Attitudinal body-image assessment: Factor analysis of the body-self relations questionnaire. Journal of Personality Assessment, 55(1–2), 135–144. doi: https://doi.org/10.1080/00223891.1990.9674053
- Cash, T. F. (2000). The multidimensional body-self relations questionnaire. MBSRQ users manual (3rd revision, pp. 1–10).
- Chan, F., Cheing, G., Chan, J. Y. C., Rosenthal, D. A., & Chronister, J. (2006). Predicting employment outcomes of rehabilitation clients with orthopedic disabilities: A CHAID analysis. Disability and Rehabilitation, 28(5), 257–270. doi: https://doi.org/10.1080/09638280500158307
- Costa, S., Hausenblas, H. A., Oliva, P., Cuzzocrea, F., & Larcan, R. (2013). The role of age, gender, mood states and exercise frequency on exercise dependence. Journal of Behavioural Addictions, 2(4), 216–223. doi: https://doi.org/10.1556/JBA.2.2013.014
- de la Vega, R., Parastadiou, I. S., Ruíz-Barquín, R., & Szabo, A. (2016). Exercise addiction in athletes and leisure exercisers: The moderating role of passion. Journal of Behavioural Addiction, 5, 325–331. doi: https://doi.org/10.1556/2006.5.2016.043
- Dietrich, A. (2006). Transient hypofrontality as a mechanism for the psychological effects of exercise. Psychiatry Research, 145(1), 79–83. doi: https://doi.org/10.1016/j.psychres.2005.07.033
- Egorov, A. Y., & Szabo, A. (2013). The exercise paradox: An interactional model for a clearer conceptualization of exercise addiction. Journal of Behavioral Addictions, 2(4), 199–208. doi: https://doi.org/10.1556/JBA.2.2013.4.2
- Godin, G., & Shephard, R. J. (1985). A simple method to assess exercise behavior in the community. Canadian Journal of Applied Sport Sciences, 10(3), 141–146.
- Grandi, S., Clementi, C., Guidi, J., Benassi, M., & Tossani, E. (2011). Personality characteristics and psychological distress associated with primary exercise dependence: An exploratory study. Psychiatry Research, 189(2), 270–275. doi: https://doi.org/10.1016/j.psychres.2011.02.025
- Guérin, E., Fortier, M. S., & Williams, T. (2013). “I just NEED to move … ”: Examining women’s passion for physical activity and its relationship with daily affect and vitality. Psychology of Well-Being: Theory, Research and Practice, 3(1), 4. doi: https://doi.org/10.1186/2211-1522-3-4
- Gulker, M. G., Laskis, T. A., & Kuba, S. A. (2001). Do excessive exercisers have a higher rate of obsessive-compulsive symptomatology? Psychology, Health & Medicine, 6(4), 387–398. doi: https://doi.org/10.1080/13548500126535
- Gustafsson, H., Hassmén, P., & Hassmén, N. (2011). Are athletes burning out with passion? European Journal of Sport Science, 11(6), 387–395. doi: https://doi.org/10.1080/17461391.2010.536573
- Hausenblas, H. A., & Fallon, E. A. (2006). Exercise and body image: A meta-analysis. Psychology & Health, 21(1), 33–47. doi: https://doi.org/10.1080/14768320500105270
- Hausenblas, H. A., & Giacobbi Jr, P. R. (2004). Relationship between exercise dependence symptoms and personality. Personality and Individual Differences, 36(6), 1265–1273. doi: https://doi.org/10.1016/S0191-8869(03)00214-9
- Hausenblas, H. A., & Symons Downs, D. (2002a). Exercise dependence: A systematic review. Psychology of Sport and Exercise, 3(2), 89–123. doi: https://doi.org/10.1016/S1469-0292(00)00015-7
- Hausenblas, H. A., & Symons Downs, D. (2002b). How much is too much? The development and validation of the exercise dependence scale. Psychology and Health, 17(4), 387–404. doi: https://doi.org/10.1080/0887044022000004894
- Ivarsson, A., & Stenling, A. (2019). Prediction of injury risk in sports. In N. Balakrishnan, T. Colton, B. Everitt, W. Piegorsch, F. Ruggeri, & J. L. Teugels (Eds.), Wiley StatsRef: Statistics reference online. doi:10.1002/9781118445112.stat08141.
- Kerr, J. H., Lindner, K. J., & Blaydon, M. (2007). Exercise dependence. Scottsdale, AZ: Holcomb Hathaway.
- Kovacsik, R., Griffiths, M. D., Pontes, H. M., Soós, I., de la Vega, R., Ruíz-Barquín, R., Demetrovics, Z., & Szabo, A. (2018). The role of passion in exercise addiction, exercise volume, and exercise intensity in long-term exercisers. International Journal of Mental Health Addiction. doi:10.1007/s11469-018-9880-1.
- Kovacsik, R., Soós, I., de la Vega, R., Ruíz-Barquín, R., & Szabo, A. (2018). Passion and exercise addiction: Healthier profiles in team than in individual sports. International Journal of Sport and Exercise Psychology, doi: https://doi.org/10.1080/1612197X.2018.1486873
- Landolfi, E. (2013). Exercise addiction. Sports Medicine, 43(2), 111–119. doi: https://doi.org/10.1007/s40279-012-0013-x
- Lejoyeux, M., Avril, M., Richoux, C., Embouazza, H., & Nivoli, F. (2008). Prevalence of exercise dependence and other behavioral addictions among clients of a Parisian fitness room. Comprehensive Psychiatry, 49(4), 353–358. doi: https://doi.org/10.1016/j.comppsych.2007.12.005
- Lindwall, M., & Palmeira, A. (2009). Factorial validity and invariance testing of the exercise dependence scale-revised in Swedish and Portuguese exercisers. Measurement in Physical Education and Exercise Science, 13(3), 166–179. doi: https://doi.org/10.1080/10913670903050313
- Marques, A., Peralta, M., Sarmento, H., Loureiro, V., Gouveia, ÉR, & de Matos, M. G. (2018). Prevalence of risk for exercise dependence: A systematic review. Sports Medicine, 1–12. doi: https://doi.org/10.1007/s40279-018-1011-4
- Mehroof, M., & Griffiths, M. D. (2010). Online gaming addiction: The role of sensation seeking, self-control, neuroticism, aggression, state anxiety, and trait anxiety. Cyberpsychology, Behavior, and Social Networking, 13(3), 313–316. doi: https://doi.org/10.1089/cyber.2009.0229
- Mónok, K., Berczik, K., Urbán, R., Szabo, A., Griffiths, M. D., Farkas, J., … Demetrovics, Z. (2012). Psychometric properties and concurrent validity of two exercise addiction measures: A population wide study. Psychology of Sport and Exercise, 13, 739–746. doi: https://doi.org/10.1016/j.psychsport.2012.06.003
- Ogden, J., Veale, D., & Summers, Z. (1997). The development and validation of the exercise dependence questionnaire. Addiction Research, 5(4), 343–355. doi: https://doi.org/10.3109/16066359709004348
- Önder, E., & Uyar, S. (2017). CHAID analysis to determine socioeconomic variables that explain students’ academic success. Universal Journal of Educational Research, 5(4), 608–619. doi: https://doi.org/10.13189/ujer.2017.050410
- Paradis, K. F., Cooke, L. M., Martin, L. J., & Hall, C. R. (2013). Too much of a good thing? Examining the relationship between passion for exercise and exercise dependence. Psychology of Sport and Exercise, 14(4), 493–500. doi: https://doi.org/10.1016/j.psychsport.2013.02.003
- Parastatidou, I. S., Doganis, G., Theodorakis, Y., & Vlachopoulos, S. P. (2012). Exercising with passion: Initial validation of the passion scale in exercise. Measurement in Physical Education and Exercise Science, 16(2), 119–134. doi: https://doi.org/10.1080/1091367X.2012.657561
- Schreiber, K., & Hausenblas, H. A. (2015). The truth about exercise addiction. Understanding the dark side of thinspiration. London, UK: Rowman & Littlefield.
- Sicilia, Á, Alcarez-Ibáñez, M., Lirola, M.-J., & Burgueño, R. (2017). Influence of goal content on exercise addiction: Analysing the mediating effect of passion for exercise. Journal of Human Kinetics, 59, 143–153. doi: https://doi.org/10.1515/hukin-2017-0154
- Sinha, R. (2008). Chronic stress, drug use, and vulnerability to addiction. Annals of the New York Academy of Sciences, 105–130. doi: https://doi.org/10.1196/annals.1441.030
- Spano, L. (2001). The relationship between exercise and anxiety, obsessive-compulsiveness, and narcissism. Personality and Individual Differences, 30(1), 87–93. doi: https://doi.org/10.1016/S0191-8869(00)00012-X
- Symons Downs, D., Hausenblas, H. A., & Nigg, C. R. (2004). Factorial validity and psychometric examination of the exercise dependence scale-revised. Measurement in Physical Education and Exercise Science, 8(4), 183–201. doi: https://doi.org/10.1207/s15327841mpee0804_1
- Szabo, A. (1995). The impact of exercise deprivation on well-being of habitual exercisers. The Australian Journal of Science and Medicine in Sport, 27, 68–75.
- Vallerand, R. J. (2008). On the psychology of passion: In search of what makes people's lives most worth living. Canadian Psychology/Psychologie Canadienne, 49(1), 1–13. doi: https://doi.org/10.1037/0708-5591.49.1.1
- Vallerand, R. J., Blanchard, C., Mageau, G. A., Koestner, R., Ratelle, C., Léonard, M., … Marsolais, J. (2003). Les passions de l’ame: On obsessive and harmonius passion. Journal of Personality and Social Psychology, 85(4), 756–767. doi: https://doi.org/10.1037/0022-3514.85.4.756
- Veale, D. (1995). Does primary exercise dependence really exist. Exercise addiction: Motivation for participation in sport and exercise (pp. 1–5).
- Vorspan, F., Mehtelli, W., Dupuy, G., Bloch, V., & Lépine, J. P. (2015). Anxiety and substance use disorders: Co-occurrence and clinical issues. Current Psychiatry Reports, 17(2), 4. doi: https://doi.org/10.1007/s11920-014-0544-y
- Young, S, Rhodes, P, Touyz, S, & Hay, P. (2013). The relationship between obsessive-compulsive personality disorder traits, obsessive-compulsive disorder and excessive exercise in patients with anorexia nervosa: a systematic review. Journal of eating disorders, 1, 1–13. Article no 16. doi: https://doi.org/10.1186/2050-2974-1-16
- Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67(6), 361–370. doi: https://doi.org/10.1111/j.1600-0447.1983.tb09716.x