
ABSTRACT
HIV/AIDS stigmatizing behaviors are a huge barrier to early detection and treatment of individuals with the AIDS virus. HIV/AIDS stigma and related consequences are debilitating, especially for vulnerable populations. This study sought to assess whether young women’s HIV/AIDS knowledge levels and exposure to mass media (television and radio) have an influence on their stigmatizing behaviors and role as agents of stigma towards individuals living with HIV and AIDS. The data used for this study originated from the Ghana Multiple Indicator Cluster Survey 2011. Binary and multiple (stepwise) logistic regression analyses were used to examine the associations between HIV/AIDS knowledge, frequency of exposure to mass media, and HIV/AIDS stigmatizing behaviors among young women aged 15–24 years in Ghana. Of the 3573 young women, 80% of 15–19-year-olds and 76% of 20–24-year-olds had at least one stigmatizing behavior towards persons living with HIV/AIDS (PLHA). Young women with increased knowledge regarding HIV/AIDS and frequent exposure to mass media (television and radio) had lesser tendency to stigmatize or act as agents of stigma towards PLHA (proportion with at least one stigmatizing behavior per subgroup – HIV/AIDS knowledge: those with highest knowledge score 579 [70.1%], those with lowest knowledge score 28 [90.3%]; mass media: those with daily exposure 562 [73.4%], those not exposed at all 249 [89.2%]). There was a graded negative ‘exposure–response’ association between the ranked variables: HIV/AIDS knowledge, mass media, and HIV/AIDS stigmatizing behaviors. The significant inverse association between HIV/AIDS knowledge, frequency of exposure to mass media, and HIV/AIDS stigmatizing behaviors persisted even after adjusting for all other covariates in the multiple logistic regression models. It is extremely important to increase HIV/AIDS-related knowledge and reduce stigma among young women in Ghana through targeted HIV/AIDS factual knowledge transfer. The use of mass media for communication of issues regarding HIV/AIDS, its mode of transmission, and associated stigma should be emphasized among women in Ghana.
Responsible Editor Jennifer Stewart Williams, Umeå University, Sweden
Background
Sub-Saharan Africa alone accounts for 71% of persons living with HIV and AIDS (PLHA). The pandemic has become a major public health issue in this region [Citation1] with very serious socioeconomic and psychological effects on PLHA, their families, and their countries.
Young people are generally considered to be the most vulnerable group with regard to HIV/AIDS, as they become sexually active and engage in risky sexual behaviors including unprotected sexual intercourse [Citation2,Citation3]. The burden of HIV and AIDS among young people continues to be on the rise [Citation4]. Young women (15–24 years) are at greater risk of being infected with HIV compared to their male counterparts. Although the prevalence of HIV and AIDS significantly dropped from 1.9% in 2013 to 1.6% in 2014 in Ghana [Citation5], the proportion of infected women is higher than that of men, with cases among young women accounting for more than half of the prevalence in young people [Citation5,Citation6].
Stigma plays a huge role as a barrier in the prevention and control of HIV/AIDS [Citation7–Citation10]. Factors contributing to HIV and AIDS stigma and discrimination include lack of education and knowledge concerning the etiology of HIV and AIDS and its mode of transmission [Citation11], misconceptions concerning the transmission, the life-threatening nature of the disease, and the epidemiology of the disease [Citation12–Citation16].
The stigma associated with the disease often excludes PLHA from seeking voluntary counseling and testing services, and accessing the highly effective antiviral drugs that exist [Citation7–Citation10,Citation17]. A growing number of studies in the past decade have addressed the issue of HIV/AIDS-related stigma [Citation18–Citation20].
One such study conducted in South Africa in 2004 and 2008 concluded that individuals with higher knowledge scores on HIV/AIDS, previously tested for HIV, as well as those who knew a family member or friend who was infected with HIV or had died of AIDS had significantly lower stigma scores [Citation19].
Among the Ghanaian population, voluntary counseling and testing for HIV are low, which in many studies is attributed to the stigma and discrimination associated with HIV [Citation5,Citation16,Citation21]. This is very detrimental to individuals’ health and the health of the community [Citation22].
Studies have shown that mass media (television, radio, etc.) is a powerful way of sending public health and health promotion messages to the population and particularly for sending culturally sensitive messages to young people [Citation23,Citation24]. However, no previous study has been conducted in young Ghanaian women concerning the relationship between exposure to mass media (television and radio), HIV/AIDS knowledge, and HIV/AIDS stigma. The aim of this study was thus to examine the extent to which knowledge of HIV/AIDS and its transmission and frequent exposure to mass media (television and radio) influenced stigmatizing behaviors among young Ghanaian women aged 15–24 years.
Methods
Study design, data collection, and study population
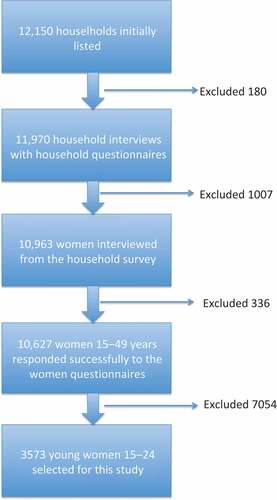
This cross-sectional study used data that originated from the women’s questionnaire included in the Ghana Multiple Indicator Cluster Survey (MICS) 2011 [Citation25]. The details of the data collection process have been outlined in . This current study used a sub-sample of 3573 young women aged 15–24 years, i.e. the most vulnerable group affected and infected by HIV/AIDS as well as its associated stigma. The sample included respondents from all the 10 administrative regions of Ghana.
Figure 1. Flow chart of sample selection process for this study using the 2011 Ghana MICS.
Measures
Outcome
HIV/AIDS stigmatizing behavior was the outcome of interest for this study. This study used indicators of social distancing to assess HIV/AIDS stigma in the form of potential behaviors, thoughts, feelings, and discriminatory attitudes that express prejudice against PLHA. Detailed explanation of all the measures is provided in the Supplemental Data.
Main exposures
HIV/AIDS knowledge
The variable HIV/AIDS knowledge was created using responses to nine questions on HIV/AIDS knowledge. The total HIV/AIDS knowledge score ranged from 0 to 9 (‘no question answered correctly’ to ‘all questions correctly answered’) where a score of zero represented no HIV/AIDS knowledge and a score of nine represented the highest HIV/AIDS knowledge. HIV/AIDS knowledge was further regrouped into six homogeneous subgroups (0 = least to 5 = highest knowledge; 0 [0], 1–2 [1], 3 [2], 4 [3], 5–7 [4], and 8–9 [5]) based on an initial analysis using box plots.
Frequency of exposure to mass media
Frequency of exposure to television and radio was independently assessed by the questions: (a) do you watch television?and (b) do you listen to radio?The response options were (1) almost every day, (2) at least once a week, (3) less than once a week, and (4) not at all.
Statistical analysis
The data were analyzed using Statistical Package for the Social Sciences version 22.0 (SPSS 22). Chi-squared tests and simple and multiple logistic regression were used for analyses. A p-value of 0.05 was chosen as the significance threshold.
Results
A total of 3573 young women were included in the study of which 1899 (53.2%) were 15–19 years old and 1674 (46.8%) were 20–24 years. About 1 out of 4 (23.5%) had the highest HIV/AIDS knowledge score whereas 0.9% scored 0 (the lowest). About 78% of the participants reported at least one stigmatizing behavior towards PLHA. Stigmatizing behavior against male PLHA in the workplace was slightly higher (49.7%) compared with female PLHA (43.1%). Stigmatizing behavior against PLHA was more prevalent in the community (70.1%) than in the family (28.6%). Detailed sample characteristics are provided in Table S2 in the Supplemental Data.
shows the proportions of different subgroups of young women who exhibited potential stigmatizing behaviors towards PLHA. Eighty percent of young women aged 15–19 years and 76% of those 20–24 years old had at least one stigmatizing behavior towards PLHA. About 70% of those with the highest HIV/AIDS knowledge score expressed at least one stigmatizing behavior towards PLHA compared with 90.3% among those with no HIV/AIDS knowledge. About 73% of participants who had daily access to mass media (television and radio) reported HIV/AIDS stigmatizing behaviors towards PLHA compared with 89.2% who reported not using mass media at all. Participants with secondary/higher education expressed lower stigmatizing behaviors towards PLHA (64.8%) compared to those with no education (89.2%).
Table 1. Prevalence (including p-values for square tests) of HIV/AIDS stigmatizing behaviors among different subgroups of young Ghanaian women aged 15–24 years in Ghana according to the Ghana MICS 2011.
shows the results (crude odds ratios, 95% confidence intervals) of the bivariate analyses for the different categorical variables with respect to HIV/AIDS stigmatizing behaviors. The odds of having stigmatizing behaviors increased with decreasing level of HIV/AIDS knowledge. Young women with very low HIV knowledge had more than three times higher odds of having HIV/AIDS stigmatizing behavior. The odds of having stigmatizing behaviors increased with decreasing frequency of use of mass media. Participants with no access to mass media had three times higher odds of HIV/AIDS stigmatizing behavior compared to those with daily access to mass media (television and radio).
Table 2. Logistic regression analysis showing the association between age, HIV/AIDS knowledge, frequency of exposure to mass media, education, wealth, and HIV/AIDS stigmatizing behaviors among young women aged 15–24 years in Ghana using the Ghana MICS 2011.
presents multivariate stepwise analyses of the association between HIV/AIDS knowledge and HIV/AIDS stigmatizing behaviors. Generally, young women with lesser HIV/AIDS knowledge were still at higher risk of stigmatizing PLHA.
Table 3. Multiple logistic regressions including adjusted odds ratios with 95% confidence intervals showing the association between HIV/AIDS knowledge, age, area, wealth, and education with HIV/AIDS stigmatizing behaviors among young women aged 15–24 years in Ghana.
shows the results of the multivariate stepwise analyses of the association between HIV/AIDS stigmatizing behavior and mass media exposure.
Table 4. Multiple logistic regressions including adjusted odds ratios with 95% confidence intervals showing the association between frequency of exposure to mass media, age, area, and education with HIV/AIDS stigmatizing behaviors among young women aged 15–24 years in Ghana.
The final model adjusted for age, region, ethnicity, area of residence, and education. ‘Not at all’ users of mass media were twice as likely to stigmatize PLHA compared to the reference group. The models that included mass media exposure were not adjusted for wealth status since calculation of the wealth index encompassed ownership of household assets such as television and radio.
Discussion
The study revealed a statistically significant association between increased HIV/AIDS knowledge and decreased HIV/AIDS stigmatizing behaviors among young women (15–24 years) in Ghana. A statistically significant association between more frequent exposure to mass media (radio and television) and decreased stigmatizing behaviors towards PLHA was also found in the same population.
The findings that HIV/AIDS stigmatizing behaviors were reduced among young women with the highest HIV/AIDS knowledge are consistent with those from previous studies [Citation16,Citation19,Citation26], showing that lack of factual knowledge about the mode of transmission of the AIDS virus and the corresponding myths associated with AIDS transmission contribute to the stigmatizing behaviors and discriminatory attitudes towards PLHA. Therefore, it is extremely important to promote efforts to increase young women’s HIV/AIDS-related knowledge. It is also critically important to create multiple avenues for young women to receive information on sexual reproductive health and rights issues such as HIV/AIDS knowledge, especially in settings where the opportunity for young women to be enrolled in formal education may be limited.
The present study also found that frequent exposure to mass media (TV and radio) decreases young women’s stigmatizing behaviors towards PLHA. This is consistent with previous studies that reported mass media as one of the important sources of HIV/AIDS information in terms of prevention and decreasing stigmatizing behaviors [Citation23,Citation27,Citation28]. Therefore, collaboration between the media companies and the various governmental and non-governmental organizations in Ghana to intensify HIV/AIDS messages to youth and to the entire Ghanaian population is highly recommended. The results indicate the need for restructuring and re-evaluating those programs already existing in the Ghanaian mass media, such as the ‘Heart to Heart’ HIV campaign and ‘Protect your Goal’ campaign [Citation29]. These efforts are mostly organized by PLHA to provide HIV/AIDS messages, themes, or stories of HIV/AIDS on prime-time and daytime entertainment such as telenovelas (television novels) to maximize their positive effects among the youth. Specifically designed programs could be initiated for targeting both the agents of stigmatization and the stigmatized. According to Xiao and colleagues [Citation28] and Singhal and Rogers [Citation30], mass media, especially television, is a powerful medium for communicating sensitive health messages as well as being able to effectively change health behaviors in individuals with low literacy levels who otherwise might find it difficult to process such messages. Health messages should be available and reinforced in already existing informal gatherings such as youth centers, churches, and community and market gatherings to help young women acquire the right HIV/AIDS knowledge for self-protection as well as acceptance of peers who are infected with the virus. Level of education may not only be a confounder but could be in the same causal chain, where exposure to media mediates the effect of education on discriminatory attitudes/behavior. Thus, raising the general level of education could be an important strategy for reducing stigma and discrimination against HIV-positive individuals.
The study also found that the majority of young women (70.1%) were unwilling to buy fresh vegetables from a person that they knew had the AIDS virus, but in contrast, most (71.4%) of them were willing to care for a family member infected with the AIDS virus. This finding is consistent with previous studies [Citation16,Citation19]. Therefore, young women could benefit from education that emphasizes detailed and correct knowledge about the AIDS disease and how to deal with stigma and discrimination.
Finally, there was a statistically significant association between increased formal education, being wealthy, and urban residence, and decreased HIV/AIDS stigmatizing behaviors. This requires appropriate intervention from the government to create opportunities aimed at bridging the socioeconomic gap among the youth, including young women. There should be periodic evaluation of the approaches used in countering HIV/AIDS stigmatizing behaviors among young women and tailored HIV/AIDS information and messages to specific cultures and groups. Further research is needed to examine the nature of the association between the use of social media or other mass media, including the Internet, as a tool for HIV/AIDS knowledge transmission and reduction of stigmatizing behaviors.
Methodological considerations
The comprehensive nature of the information available in the data-set and the representativeness of the entire 10 administrative regions of Ghana are major strengths for this study. Therefore, the results may be generalized to all Ghanaian young women who are 15–24 years of age. Additionally, this is the first study of its kind in Ghana to examine the impact of media exposure on HIV/AIDS stigmatizing behaviors. The graded negative association between the ranked HIV/AIDS knowledge, mass media exposure, and HIV/AIDS stigmatizing behaviors lends further support to the validity of the findings. Causality cannot be inferred between the covariates and HIV/AIDS stigmatizing behaviors due to the cross-sectional nature of the data. Also, the study used secondary data that were self-reported, which can be subject to bias. On the one hand, using an aggregated ‘series of questions’ to define stigmatizing behaviors could help minimize underreporting of the stigmatizing behaviors due to the socially sensitive nature of the issue. On the other, young women with higher HIV/AIDS knowledge could have underreported their potential stigmatizing behaviors, due to a bias towards social desirability.
Conclusion
The present study suggests an urgent need to reduce HIV/AIDS stigmatizing behaviors among young women in Ghana through comprehensive sexuality education using dynamic approaches. It is extremely important to promote programs that increase HIV/AIDS-related knowledge among young women, especially among those with low wealth and/or low education. The use of mass media for communication or knowledge transfer concerning issues related to HIV/AIDS, its mode of transmission, and associated stigma should be emphasized among women in Ghana.
Ethics and consent
The study analyzed data from the Ghana Multiple Indicator Cluster Survey conducted in 2011 by the Ghana Statistical Service. Ethical approval for the data collection was received from the Ghana Health Service Ethical Review Board. Access to use this data was given by UNICEF after submitting a written proposal for this study. The aims of the survey and the data collection approach were explained to participants before the commencement of the data collection.
Paper context
Previous studies in the general population have shown an association between low HIV/AIDS knowledge and stigma and discrimination towards persons living with HIV/AIDS (PLHA). In recent years, the Ghana AIDS Commission, UNAIDS, and PLHA have developed health messages concerning HIV/AIDS transmission, prevention, and associated stigma for various mass media campaigns, using PLHA as spokespersons. This is the first study that has been conducted in young Ghanaian women concerning the relationship between exposure to mass media (television and radio), HIV/AIDS knowledge, and HIV/AIDS stigma.
Supplemental data
Download ()Acknowledgments
We acknowledge the Demographic and Health Survey program and UNICEF, which provided the data-sets for this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Supplemental data
Supplemental data for this article can be accessed here.
Additional information
Funding
Notes on contributors
Charity Konadu Asamoah
CKA conceptualized and designed the study, acquired data, analyzed, and drafted the first version of the manuscript. BOA was involved in designing the study, analysis and interpretation, and writing and critical review of the manuscript. AA was involved in the conceptualization, design, interpretation, and critical review of the manuscript. All authors read and approved the final version of the manuscript.
Benedict Oppong Asamoah
CKA conceptualized and designed the study, acquired data, analyzed, and drafted the first version of the manuscript. BOA was involved in designing the study, analysis and interpretation, and writing and critical review of the manuscript. AA was involved in the conceptualization, design, interpretation, and critical review of the manuscript. All authors read and approved the final version of the manuscript.
Anette Agardh
CKA conceptualized and designed the study, acquired data, analyzed, and drafted the first version of the manuscript. BOA was involved in designing the study, analysis and interpretation, and writing and critical review of the manuscript. AA was involved in the conceptualization, design, interpretation, and critical review of the manuscript. All authors read and approved the final version of the manuscript.
Related Research Data
References
- Murray CJL, Ortblad KF, Guinovart C, et al. Articles: global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:1005–1070.
- Kirby DB, Laris BA, Rolleri LA. Review article: sex and HIV education programs: their impact on sexual behaviors of young people throughout the world. J Adolesc Health. 2007;40:206–217.
- Brody C, Tuot S, Chhea C, et al. Factors associated with sex work among at-risk female youth in Cambodia: a cross-sectional study. AIDS Care. 2016;28:339–346.
- UNICEF. Opportunity in Crisis: preventing HIV from early adolescence to young adulthood. New York: UNICEF; 2011.
- Ghana AIDS Commission: Country aids response progress report – Ghana: reporting period January 2013 to December 2014. In: Ghana AIDS commission; Accra; 2015 Mar 31.
- Glynn JR, Caraël M, Auvert B, et al. Why do young women have a much higher prevalence of HIV than young men? A study in Kisumu, Kenya and Ndola, Zambia. AIDS (London, England). 2001;15 Suppl 4:S51–S60.
- Pannetier J, Lelievre E, Le Coeur S. HIV-related stigma experiences: understanding gender disparities in Thailand. AIDS Care. 2015;1–9:1360–1451. (Electronic).
- Jean J, Coll A, Monda M, et al. Perspectives on safer conception practices and pre-conception counseling among women living with HIV. Health Care Women Int. 2016:37:1096–1118.
- Haire BG. Preexposure prophylaxis-related stigma: strategies to improve uptake and adherence - a narrative review. HIV/AIDS (Auckland, NZ). 2015;7:241–249.
- Relf M, Williams M, Barroso J. Voices of women facing HIV-related stigma in the deep south. J Psychoci Nurs Ment Health Serv. 2015;1–9:0279–3695. (Electronic).
- Nyblade L, Stangl A, Weiss E, et al. Combating HIV stigma in health care settings: what works? J Int AIDS Soc. 2009;12:15–15.
- Herek GM. Capitanio JP: public reactions to AIDS in the United States: a second decade of stigma. Am J Public Health. 1993;83:574–577.
- Rushing WA. The AIDS epidemic: social dimensions of an infectious disease. Colorado: Westview Press; 1995.
- Sontag S. Illness as metaphor and AIDS and its metaphors. New York: Macmillan; 2001.
- Parker R, Aggleton P. HIV AIDS-related stigma and discrimination: A conceptual framework and implications for action. Soc Sci Med. 2003;57:13–24.
- Tenkorang EY, Owusu AY. Examining HIV-related stigma and discrimination in Ghana: what are the major contributors? Sex Health. 2013;10:253–262.
- Taggart T, Grewe M, Conserve D, et al. Social media and HIV: a systematic review of uses of social media in HIV communication. J Med Internet Res. 2015;17:e248.
- Kayeyi N, Sandøy IF, Fylkesnes K. Effects of neighbourhood-level educational attainment on HIV prevalence among young women in Zambia. BMC Public Health. 2009;9:310.
- Mall S, Middelkoop K, Mark D, et al. Changing patterns in HIV/AIDS stigma and uptake of voluntary counselling and testing services: the results of two consecutive community surveys conducted in the Western Cape, South Africa. AIDS Care. 2013;25:194–201.
- Yang Y, Wang J, Lin F, et al. Stigma against HIV/AIDS among female sex workers and general migrant women in eastern China. BMC Women’s Health. 2015;15:2.
- Amo-Adjei J, Darteh EKM. Drivers of young people’s attitudes towards HIV/AIDS stigma and discrimination: evidence from Ghana. Afr J Reprod Health. 2013;17:51–59.
- Mahajan AP, Sayles JN, Patel VA, et al. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS. 2008;22 Suppl 2:S67–S79.
- LaCroix JM, Snyder LB, Huedo-Medina TB, et al. Effectiveness of mass media interventions for HIV prevention, 1986–2013: a meta-analysis. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2014; 66:S329–340.
- Nutbeam D, Harris E, Wise W. Theory in a nutshell: a practical guide to health promotion theories. Sydney: McGraw-Hill; 2010.
- Ghana Statistical Service. Multiple indicator cluster survey with an enhanced malaria module and biomarker. Monitoring the situation of children and women in Ghana. Final report. Acrra: Ghana statistical service; 2011.
- Collymore Y. Rooting out AIDS-related stigma and discrimination. Washington (DC): Population Reference Bureau; 2002.
- Romer D, Sznitman S, DiClemente R, et al. Mass media as an HIV-prevention strategy: using culturally sensitive messages to reduce HIV-associated sexual behavior of at-risk African American youth. Am J Public Health. 2009;99:2150–2159 2110p.
- Xiao Z, Li X, Lin D, et al. Mass media and HIV/AIDS prevention among female sex workers in Beijing, China. J Health Commun. 2015;20:1095–1106.
- Ghana AIDS Commission. Country Aids response progress report – Ghana: reporting period January 2012 to December 2013. Accra: Ghana AIDS Commission; 2014.
- Singhal A, Rogers EM. Entertainment-education: a communication strategy for social change. Mahwah, NJ: Lawrence Erlbaum associates; 1999.