
ABSTRACT
Switzerland is currently in a lockdown and other lockdowns are looming world-wide. Many countries in the West are now experiencing a third COVID-19 wave. While some scientists are aiming for Zero Covid, calls to learn to live with the virus are becoming prominent as anti-lockdown protests spread across Europe. A health system is defined as all organizations, institutions and resources that produce actions whose primary purpose is to improve health. A health care system on the other hand, is defined as institutions, people and resources involved in delivering health care to individuals. Many countries that have health systems previously thought to be world class, have also been tested, pushed to the edge and in some ways found wanting. The pandemic took all countries by some surprise and the discussion on appropriate national and global strategies is very diverse. Lessons from similar earlier outbreaks seem to suggest, that living and learning to live with the virus could be the way forward. Others argue that the virus is new, not like any other we have fought before, calling for novel ways of containing the virus. Irrespective of standpoint, being a high-, middle- or low-income country, pandemic fatigue is setting in, while new variants are being discovered. It is urgent and unprecedented. The pandemic is here and more pandemics are expected to follow. What does, ‘living with the virus,’ mean in practical terms? The purpose of this viewpoint is to stimulate debate on how we can move towards pandemic proof health care systems.
Responsible Editor Stig Wall
Background
Switzerland is currently in a lockdown and other lockdowns are looming world-wide [Citation1–3]. Many countries in the West are now experiencing a third COVID-19 wave. While some scientists are aiming for Zero Covid, calls to learn to live with the virus are becoming prominent as anti-lockdown protests spread across Europe. Zero Covid is defined as reducing infections to a point where it is possible to test, trace and isolate every single case that arises, so as to halt the spread of the virus [Citation4].
The USA (US) has extended travel restrictions from certain COVID-19 affected countries like Brazil, UK (UK) and China [Citation5]. Pandemic fatigue is being experienced in many countries [Citation6,Citation7]. Economic crises, stress and fear are threatening to become the next pandemics [Citation6,Citation7]. The tension is palpable and many are getting agitated as anti-lockdown protests spread across Europe [Citation8,Citation9].
A growing number of scientists are increasingly talking of the need to learn to live with this virus [Citation10–12]. What that means in practical terms, is not very clear. Some of the reasons for enforcing lockdowns have been to curb the spread of the virus and prevent a health system overload. Many countries that have health systems previously thought to be world class have also been tested, pushed to the edge and in some ways found wanting [Citation13,Citation14]. The pandemic took all countries by some surprise. China, Italy, Spain, France, Brazil, Mexico, USA, and the UK were hit hard. South Africa and recently Zimbabwe, have all borne the brunt of the pandemic, particularly the second wave from around Dec 2020 to Jan 2021. Currently (March 2021), the pandemic is plaguing both the northern and southern hemispheres, with new variants emerging in Brazil, UK, South Africa and India. Many people are working mostly from home and most universities and some schools have moved to online learning.
Societal issues, old versus young, value of life vs economy and science vs social media
The pandemic has made existing societal chasms more visible [Citation15,Citation16]. Unfortunately, too quickly and too often, dichotomies are created and amplified by the fact that infections and diseases are unevenly distributed across age groups, space and time. The divide between the young and the old was reported at the beginning of the pandemic[Citation15]. Young people initially thought they were less vulnerable and hence saw lockdowns as measures to prevent the vulnerable old, from getting the disease. Other older people saw the restless young as the ones refusing to adhere to social distancing rules, thereby spreading the disease [Citation15]. Our interconnectedness and the value of life iitself have been tested by the pandemic. Debates on saving lives versus economic interests have not been exhaustive either[Citation17]. The need for information, on a novel virus SARS-CoV-2, led to a scramble to know what the latest facts are, what works best and where, pitting science (studies take time to generate knowledge) against social media. As is the nature of scientific inquiry, the multiple views of scientists on the same issues, complicates the matter even further[Citation17]. The dichotomy carries on with pro-vaccine and anti-vaccine groups to date.
Living with the virus and emergent variants
The proposed strategies range from aiming for No-Covid [Citation18], to living with the virus. Others argue that the virus is new, not like any other we have fought before, calling for novel ways of containing the virus. On the other hand, calls for living with the virus are becoming more prominent, based on lessons from previous pandemics [Citation10–12,Citation19]. Irrespective of standpoint, pandemic fatigue is setting in while new variants are being discovered. It`s urgent and unprecedented. What does living with the virus mean in real terms? Which measures need to be put in place, maintained and what role does vaccination and the overall concept of herd immunity play? COVID-19 is not that simple, since it is both an infection with a severe acute respiratory syndrome and an array of non-communicable diseases too [Citation20]. Contexts differ and countries across the globe will respond differently. The purpose of this viewpoint is to stimulate debate on how pandemic proof health care systems look like.
Health system and health care system definitions
A health system is part of the overall social system in any setting and is defined as all organizations, institutions and resources that produce actions whose primary purpose is to improve health [Citation21]. A health care system on the other hhand is defined as institutions, people and resources involved in delivering health care to individuals [Citation21]. For clarity reasons, we are going to use the term health care system (institutions, people, and resources) throughout this paper. See
Table 1. Summary of policy, structural and operational issues that might need attention
What does a pandemic proof health care system look like?
Institutions
The institutions include health facilities; among others clinics, medical practices and hospitals. The pandemic challenges us not only on the conceptual levels but very practically as discussed below.
Curative services
What kind of health care services will institutions provide? Are we going to see a need for the expansion of telemedicine from triage, diagnosis and follow up services covering all conditions (acute to chronic)? Are we going to see institutions moving into taking care where the people are- through home-based care services? Will institutions adapt and become centres of knowledge dissemination- telemedicine and all possibilities of e- and m-health and provide knowledge to people at home, on what symptoms to look out for, where to test, how to self-care etc? for other conditions too and not only COVID-19? What telemedicine services will be incorporated into every day practice after the pandemic? Telemedicine expansion seems inevitable-are we going to see big health system investments into telemedicine technology in both low-and high-income countries? See above
Preventive and promotive health services
Staying at home has brought about new opportunities and challenges too. Lockdowns have also meant closure of sport facilities including gyms for those that afforded these. Fitness, diet and exercise choices have been left mostly to individuals. The pandemic has demonstrated that having an underlying condition like diabetes, hypertension or obesity predisposes one to complications, long hospital stays and mortality. Due to the above reasons, COVID-19 has been termed a syndemic rather than a pandemic [Citation20]. Addressing COVID-19 is indeed complex. This entails addressing obesity, diabetes, cancer, chronic respiratory diseases and hypertension [Citation20], notwithstanding the broader socio-economic challenges.
Health is wealth [Citation22] – are we going to see a more concrete recognition of this notion? Are institutions going to tap into this and provide preventive and promotive health services like boosting one’s immune system through diet, exercise and supplements, in different formats, online, face to face or through home visits? See above
Mental health services
Mental health issues during the pandemic are threatening to become the next pandemic. Stress and mental health issues related to lockdowns affect everyone but tend to affect the weaker segments of the society more severely. The poor often have limited space to accomodate homeoffice and home schooling, not to mention the additional weight of economic effects and job insecurities [Citation23,Citation24] .
Long COVID
Some people that recovered from COVID-19 are still experiencing its effects-long covid with some now in need of dialysis and others developing diabetes. The uncertainties and anxiety accompanied by confinement to homes is creating new health needs [Citation20,Citation25].
Our societies need hope [Citation20]. Drugs or vaccines alone cannot solve the syndemics we are faced with. Are we going to see athe systems thinking approach that incorporates housing, health, employment, food, environment and educational issues [Citation20]?
Are institutions going to expand their services to include preventive and promotive mental health services as well as mobile dialysis teams? In what format? Online, face to face, home visits or blended? See above.
Infrastructure
Health care system infrastructure is often built with centralized ventilation systems that could promote the spread of viruses such as COVID-19. Structural change e.g. air filters and a re-think on patient flows seem imminent. The waiting rooms might need to be adapted to having preferably few persons at a time and the rooms be disinfected and aerated after each patient. Some waiting rooms have no windows that can be opened-what will happen to these? In some countries in the North, winters are hard and heating is expensive. Can practices and institutions afford to open windows after each patient in winter? If high volumes of people fall ill at the same time, institutions might run out of the beds and even oxygen as was experienced by some countries. So, do the pandemic proof institutions have to be restructured, to take health care to where the sick are-to homes rather? See above
Resources
Disinfectants and PPE
Disinfectant use is one component among strategies being used to curb the spread of the virus. Are we going to see development of environmentally friendly disinfectants or is the world going to wake up to other multi-resistant bugs due to indiscriminate use of disinfectants? Many institutions had COVID-19 wards or infectious disease units as in some hospitals in Africa [Citation26]. If COVID-19 were to be everywhere-does that mean all health care workers in all units will need to wear full protective personal equipment (PPE) gear daily? Is that affordable? The world is already drowning in plastic. Our seas are flooded. Can we afford to keep producing daily tonnes of plastic through disposable PPE now and in future pandemic states? Are we going to see more local production of sustainable and reusable PPE? See above
Testing kits
There are initiatives and moves towards self-testing. That might become the order of the day. Who should test, how often and when, needs to be answered? The PCR test costs to date have been borne by the governments in some countries. Will that remain so? This is important, as the cost of tests can hinder testing, bearing in mind the economic strains borne by many, that have suffered in multiple ways during the pandemic. See above
Vaccines
With whole populations at risk, are vaccinations going to become the norm? Are we going to see institutions adapting to include ongoing vaccination services across all age groups, from the infants to the elderly? Viral mutations occur and they do threaten the efficacy of vaccines. Are we going to see investment into surveillance systems including genetic sequencing and parallel investments in second and third generation vaccines? See above
People
A system is made up of people and a system is as good as the people in the system. The world is already experiencing a health workforce crisis. Health care workers resigned due to fear of getting infected at the height of the pandemic. PPE shortages were to blame in some instances and this was blamed on pandemic unpreparedness, as very few if any, anticipated its extent and magnitude. Fatigue and burn-out were experienced by many and some intensive care unit (ICU) nurses ended up looking after 5 patients as compared to a 1:1 ratio. Some nurses were even assigned to work in unfamiliar units like intensive care unit (ICU) without any training [Citation27]. The impact this had on quality of care was attributed to high mortality rates in some cases [Citation28,Citation29]. In the context of such health worker shortages, are we soon going to see robots caring for people at home and in institutions-robotic telemedicine? See above
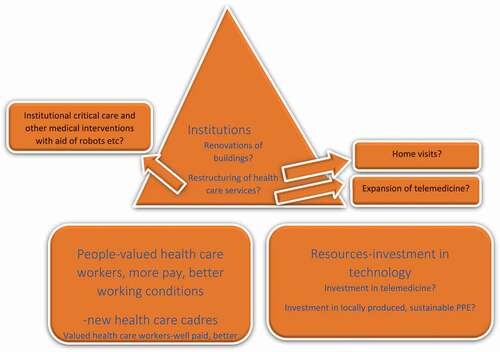
What needs to happen to make our health care systems pandemic proof wwith regard to health care workers? How can the constant supply of health care workers be ensured? Online training of low level cadres, like the health care workers and clinical associates in Africa [Citation30]? Are we going to see more health care workers trained to provide home based care and home visits and teach patients self-care, not only in COVID-19 contexts but other conditions as well? [Citation30]. Many countries applauded the health care workers during the peak of the first wave. Are we going to see health care workers valued more, with better pay and working conditions? See for the depiction of a pandemic proof health care system.
Figure 1. A pandemic proof health care system
Both low- and high-income countries were affected
The poor always pay more but the divide between the low and the high-income countries was blurred by the virus. Both hemispheres were ravaged, with some high-income countries suffering more casualties as compared to the low-income countries to date. The vaccine availability and roll-out might change the dynamic particularly, the COVAX facility. Are we going to see more cooperation between the low- and high-income countries in future? See for a summary of policy, structural and operational issues.
Conclusion
The purpose of this view point is to stimulate debate. SARS-CoV-2 has changed our world in multiple ways. We wake up each day to a new normal. What does a pandemic proof health care system look like, is meant to stimulate debate and create an impetus for changes that our health care systems might need to make, as the pandemic drags on and new variants emerge. Assessing the course of the pandemic also shows us that the changes to be made in and for the health systems need to be tailored to the respective settings; no ‘one size fits all’ approaches are possible. High-, middle- and low-income countries will respond differently. The health system implications as outlined are far reaching, ranging from conceptual, policy, considerations of effective surveillance-response systems to the very operational and structural issues including health infrastructure construction in relation to patients’ needs. The pandemic has clearly revealed policy, structural and functional gaps; a chance and an opportunity. Besides all this, the health care system is part of the larger socio-ecological system in any country, and hence the overall challenge remains in identifying environmentally sustainable ways towards more effective and equitable health systems, sensitive to individual as well as societal needs. The pandemic is here and more pandemics are expected in future. Irrespective of aiming for No Covid, Zero Covid or for living with the virus, or being a high-, middle- or low-income country, what needs to be done as both uncertainty and the pandemic linger on? We acknowledge that this is indeed a mammoth task. What does a pandemic proof health care system look like, is meant to stimulate debate.
Author contributions
JM had the initial concept and TCS and MT were involved in developing the concept further. All authors were involved in writing the manuscript.
Paper context
Pandemic fatigue is setting in. The tension is palpable and many are agitated as anti-lockdown protests spread across Europe. Scientists are divided. Irrespective of aiming for No Covid, Zero Covid or for living with the virus, being a high-, middle- or low-income country, what needs to be done as both uncertainty and the pandemic linger on? The purpose of this manuscript is to stimulate debate on what a pandemic proof health care system looks like.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- National lockdown: Stay at Home. GOV UK. cited 2021 Jan 30. Available form: https://www.gov.uk/guidance/national-lockdown-stay-at-home
- Zaken M, Van A. Netherlands to remain in lockdown until at least 9 February inclusive – news item-Government.nl2021. cited 2021 Jan 30. available From: https://www.government.nl/latest/news/2021/01/12/netherlands-to-remain-in-lockdown-until-at-least-9-february-inclusive
- Zimbabwe Extends Lockdown, Dusk-to-Dawn Curfew Amid Surge in COVID19 Cases. Voice of America – english. cited 2021 Jan 30. available From: https://www.voanews.com/covid-19-pandemic/zimbabwe-extends-lockdown-dusk-dawn-curfew-amid-surge-covid19-cases
- Zero Covid: What It Means and How We Get There. People Profit 2020. cited 2021 Apr 19. available From: https://www.pbp.ie/zero-covid-what-it-means-and-how-we-get-there
- January 2021 PW. Biden team says US travel restrictions will remain. Flight Glob. cited 2021 Jan 30. available From: https://www.flightglobal.com/safety/biden-team-says-us-travel-restrictions-will-remain/142027.article
- Overcoming pandemic fatigue: How to reenergize organizations for the long run. McKinsey. cited 2021 Jan 30. available From: https://www.mckinsey.com/business-functions/organization/our-insights/overcoming-pandemic-fatigue-how-to-reenergize-organizations-for-the-long-run#
- WHO. Pandemic fatigue – reinvigorating the public to prevent COVID-19. Policy framework for supporting pandemic prevention and management. 2020 cited 2021 Apr 19. available From: https://apps.who.int/iris/handle/10665/337574
- Dutch Police Clash with Anti-Lockdown Protesters. Time. cited 2021 Jan 30. available From: https://time.com/5933061/dutch-police-covid-19-protest
- What Germany’s anti-lockdown protests reveal about the country. cited 2021 Jan 30. available From: https://www.newstatesman.com/world/europe/2020/11/what-germany-s-anti-lockdown-protests-reveal-about-country
- Ottawa`s top doctor says it is time to learn to live with COVID-19. CTV News. cited 2021 Jan 30. available From: https://ottawa.ctvnews.ca/ottawa-s-top-doctor-says-it-is-time-to-learn-to-live-with-covid-19-1.5172031
- ‘We need to learn how to live with COVID-19ʹ. cited 2021 Jan 30. available From: https://www.unicef.org/niger/stories/we-need-learn-how-live-covid-19
- “We’re going to have to learn to live with virus,” says EU health boss. Euronews 2020. cited 2021 Jan 30. available From: https://www.euronews.com/2020/09/11/we-re-going-to-have-to-learn-to-live-with-virus-says-eu-health-boss
- Germany’s Health Minister Says Nation In “Hardest Phase of the Pandemic”. Voice of America - English. cited 2021 Jan 30. available From: https://www.voanews.com/covid-19-pandemic/germanys-health-minister-says-nation-hardest-phase-pandemic
- Coronavirus: the situation in Switzerland. SWI Swissinfo.ch. cited 2021 Jan 30. available From: https://www.swissinfo.ch/eng/covid-19_coronavirus–the-situation-in-Switzerland/45592192
- Coronavirus and the divide between young and old. EurotopicsNet. cited 2021 Jan 30. available From: https://www.eurotopics.net/en/237597/coronavirus-and-the-divide-between-young-and-old
- Conger K, Griffith E As life moves online, an older generation faces a digital divide. New York Times 2020. cited 2021 Apr 19. available From: https://www.nytimes.com/2020/03/27/technology/virus-older-generation-digital-divide.html
- Smithson M Data from 45 countries show containing COVID vs saving the economy is a false dichotomy. The Conversation. cited 2021 Feb 08. available From: http://theconversation.com/data-from-45-countries-show-containing-covid-vs-saving-the-economy-is-a-false-dichotomy-150533
- Horton R. Offline: the case for No-COVID. Lancet. 2021;397:359.
- Brown M Why we need to learn to live with COVID-19. cited 2021 Apr 19. available From: https://www.ualberta.ca/folio/2020/06/why-we-need-to-learn-to-live-with-covid-19.html
- Horton R. Offline: COVID-19 is not a pandemic. Lancet. 2020;396:874.
- WHO. Health systems. World Health Report 2003. cited 2021 Feb 10. available From: https://www.who.int/whr/2003/en/
- Michel J, Tanner M Poverty is not poverty: the reality on the ground including the Rural-Urban divide and how we can turn the tide on NCDs. Lifestyle epidemiol - poverty cardiovasc dis double burd afr popul 2021.
- Michel J, Stuber R, Müller M, et al. COVID-19 and HIV testing: different viruses but similar prejudices and psychosocial impacts. J Glob Health Rep. 2021;5:e2021022.
- Millett GA. New pathogen, same disparities: why COVID-19 and HIV remain prevalent in U.S. communities of colour and implications for ending the HIV epidemic. J Int AIDS Soc. 2020;23:e25639.
- After COVID-19 Diagnosis, nearly 1 In 5 Are Diagnosed with Mental Disorder. NPROrg. cited 2021 Dec 15. available From: https://www.npr.org/sections/coronavirus-live-updates/2020/11/11/933964994/after-covid-diagnosis-nearly-1-in-5-are-diagnosed-with-mental-disorder
- Writer S A look at South Africa’s new Covid-19 ‘module’ facility – which was built in just months. cited 2021 Apr 19. available From: https://businesstech.co.za/news/business/461602/a-look-at-south-africas-new-covid-19-module-facility-which-was-built-in-just-months
- As a nurse, my hospital’s leaders frighten me more than Covid-19. STAT 2020. cited 2021 Jan 31. available From: https://www.statnews.com/2020/05/06/nurse-frightened-hospital-administrators-more-than-covid-19
- Morciano M, Stokes J, Kontopantelis E, et al. Excess mortality for care home residents during the first 23 weeks of the COVID-19 pandemic in England: a national cohort study. BMC Med. 2021;19:71.
- Ochieng N, Chidambaram P, 2021. Factors associated with COVID-19 cases and deaths in long-term care facilities: findings from a literature review. KFF. cited 2021 Apr 19. available From: https://www.kff.org/coronavirus-covid-19/issue-brief/factors-associated-with-covid-19-cases-and-deaths-in-long-term-care-facilities-findings-from-a-literature-review
- Doherty J, Conco D, Couper I, et al. Developing a new mid-level health worker: lessons from South Africa’s experience with clinical associates. Glob Health Action. 2013;6:19282.