
ABSTRACT
Background
The COVID-19 pandemic has stricken mental health worldwide. Marginalized populations in low- and middle-income countries have been the most affected, as they were already experiencing barriers to accessing mental health care prior to the pandemic and are unequally exposed to the stressors associated with the health emergency, such as economic ravages or increased risk of complicated disease outcomes.
Objective
The aim of this paper is to describe a comprehensive initiative resulting from a public-civil partnership to address the increased burden of mental health illness associated with the COVID-19 pandemic in rural Chiapas, Mexico.
Methods
To address the emerging health needs of the general population and health professionals resulting from the pandemic, Compañeros En Salud (CES), a non-profit civil society organization based in Chiapas, implemented a comprehensive strategy to compensate for the shortage of mental health services in the region in collaboration with the Chiapas Ministry of Health. The strategy included three components: capacity building in mental health care delivery, psychosocial support to the general population, and provision of mental health care to CES collaborating staff. In this capacity building article, implementers from CES and the government share descriptive information on the specific interventions carried out and their beneficiaries, as well as a critical discussion of the strategy followed.
Results
Through this strategy, we have been successful in filling the gaps in the public health system to ensure that CES-served populations and CES-collaborating health professionals have access to mental health care. However, further studies to quantify the impact of this intervention in alleviating the burden of mental health illnesses associated with the pandemic are needed.
Conclusions
The current situation represents an opportunity to reimagine global mental health. Only through the promotion of community-based initiatives and the development of integrated approaches will we ensure the well-being of marginalized populations.
Responsible Editor
Julia Schröders
Background
COVID-19 has affected health, social, and economic matters in devastating ways, negatively impacting mental health worldwide [Citation1]. Research shows that the pandemic has increased levels of depression, anxiety, insomnia [Citation2,Citation3], post-traumatic stress disorder [Citation4], and suicide ideation amongst the general population [Citation5], as well as psychological distress amongst frontline health workers [Citation6,Citation7]. Increased demand for mental health care has coincided with the disruption of mental health services; according to a survey conducted by the World Health Organization (WHO) in mid-2020, mental health services had been disrupted by the pandemic in 93% of the 130 participating countries [Citation8].
Evidence shows that financially vulnerable populations in low-and-middle income countries (LMICs) have a higher risk of developing mental health conditions related to the pandemic. In LMICs, individuals have more impediments to practicing social distancing, face barriers to accessing health care, and are more likely to be affected by the economic impacts of lockdowns [Citation9].
As COVID-19 threatens to widen the mental health treatment gap in LMICs, rural communities with profound barriers to access healthcare are most likely to suffer. Chiapas, the southernmost state in Mexico and one of its poorest, with half of its population living in rural areas [Citation10], has high rates of mental health disorders and limited health services. Before the pandemic, the prevalence of depression in the Fraylesca and Sierra regions – the areas that we serve – was estimated at 7.9% [Citation11], whereas the Mexican national average remained in 4.0–4.5% [Citation12]. As for younger populations, 35.8% of adolescents suffer from depression or generalized anxiety disorder, and 32.1% with both mental disorders report having attempted suicide [Citation13]. Furthermore, the lifetime prevalence of Intimate Partner Violence (IPV) in the region is 54.7% among ever-partnered women, with significant associations between depressive symptoms and both IPV and Sexual Violence (SV) [Citation14].
Several interventions are being undertaken to address mental health in LMICs during the pandemic [Citation9], but attention is still focused on the Global North [Citation15]. In this piece, we depict a series of mental health interventions implemented from March 2020 to February 2021 by the Ministry of Health and the non-profit organization Compañeros en Salud (CES) in rural Chiapas. This is not an empirical research paper, but a description and discussion of the integration of mental health services during the COVID-19 pandemic, aiming to expand the literature on mental health interventions in low resource settings.
The public health sector response to the mental health burden associated to the pandemic
With the advent of the COVID-19 pandemic, many of the health services were reimagined and adapted to meet the population’s needs and to respond to the suspension of services and reduction of personnel in the Mexican healthcare system. Chiapas’ Ministry of Health (MoH) transformed 14 clinical spaces – ranging from vaccination centers to abandoned Intensive Care Units – into COVID-19 clinics [Citation16]. However, providing mental health care in the midst of a pandemic with an already deficient system was challenging. In the Mexican public health sector, only 2% of healthcare expenditure is allocated to mental healthcare with 80% going to hospitals, leaving the primary care level underserved [Citation17].
In June 2020, a Post-COVID Psychology Rehabilitation Center was inaugurated in Tuxtla Gutiérrez, the capital city of Chiapas, to provide mental healthcare for patients, their relatives, and front-line health providers affected by COVID-19. In addition, 93 psychosocial hotlines were created for crisis management and emotional support [Citation18]. However, these services were not available for those living in rural areas or those lacking mobile phone reception, such as the Sierra and Fraylesca regions. Although the local health district attempted to provide coping tools and burnout prevention skills to the staff in the clinics, there was no concrete plan for the provision of mental health support at COVID-19 clinics.
Compañeros En Salud: a key player in addressing mental health disparities exacerbated by the pandemic
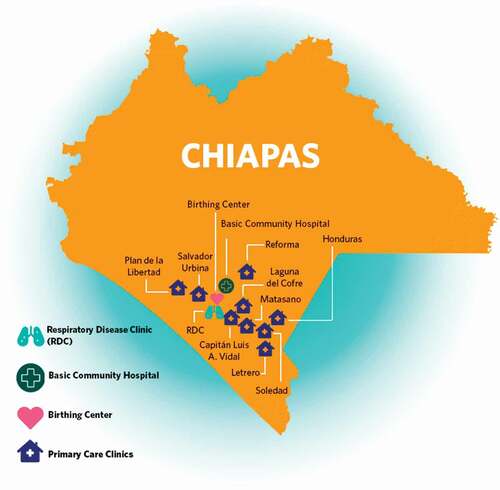
CES is the Mexican sister organization of the international non-profit organization Partners In Health (PIH), and has been working in collaboration with the MoH since 2011 to strengthen the healthcare system in Mexico. CES provides access to high quality services by working in ten MoH primary care clinics in nine rural communities and in a birthing center, a basic community hospital and, most recently, a Respiratory Disease Clinic (RDC) in the small town of Ángel Albino Corzo, all located in the Fraylesca and Sierra regions of Chiapas (see ).
Figure 1. Facilities supported by Compañeros En Salud in Chiapas, México
In 2014, CES launched the mental health program in response to the high burden of mental health conditions in the area. The program is based on task-sharing [Citation19], stepped care [Citation20], and collaborative care models [Citation21]. The activities of the mental health program are embedded in other CES projects, which consist of sexual and reproductive health, community health, referral to specialized services, continuous medical education, community-based mental healthcare (psychosocial and pharmacological treatments), and staff wellbeing.
In CES’ catchment area, there were several factors that helped to identify that these communities were at a potential risk of developing mental health conditions related to COVID-19: 1) financial instability, 2) lack of access to mental health services, and 3) previous high prevalence of mental health conditions. These factors justified the need for a preventative and therapeutic psychosocial intervention.
In response, CES launched a mental health intervention aligned with PIH’s broader initiative called ‘STOPCOVID,’ which aimed to prepare vulnerable populations to combat COVID-19 in contexts where social distancing and safe quarantine and isolation are oftentimes not feasible [Citation22]. We will present three strategies that comprise CES’ mental health response to COVID-19 based on the Inter-Agency Standing Committee’s Guidelines on Mental Health and Psychosocial Support in Emergency Settings (see ) and on the following principles: a) capacity building, b) psychosocial support, and c) staff mental health care [Citation23].
Figure 2. Psychosocial support services. Adapted from the Inter-Agency Standing Committee’s Intervention Pyramid for mental health and psychosocial support in emergencies [Citation23]. RDC: Respiratory Disease Clinic, CMHWs: community mental health workers, PPE: personal protection equipment
![Figure 2. Psychosocial support services. Adapted from the Inter-Agency Standing Committee’s Intervention Pyramid for mental health and psychosocial support in emergencies [Citation23]. RDC: Respiratory Disease Clinic, CMHWs: community mental health workers, PPE: personal protection equipment](/cms/asset/229c1db9-a0c4-4dfe-bd45-ae3d94fd240f/zgha_a_1997410_f0002_oc.jpg)
Capacity building
A fundamental aspect of CES’ COVID-19 response was the training of non-specialists in mental health skills for meeting the emotional needs at the community and in-patient unit levels.
Psychological First Aid training for all staff members
All the clinical and non-clinical staff were trained on Psychological First Aid (PFA), an intervention that provides immediate support to individuals experiencing distress related to a recent crisis. PFA can be provided by anyone who has received proper training and who can make referrals to mental health professionals when required [Citation24]. Although systematic reviews report that there is no direct evidence of PFA effectiveness, indirect evidence supports its delivery in a variety of settings [Citation25,Citation26].
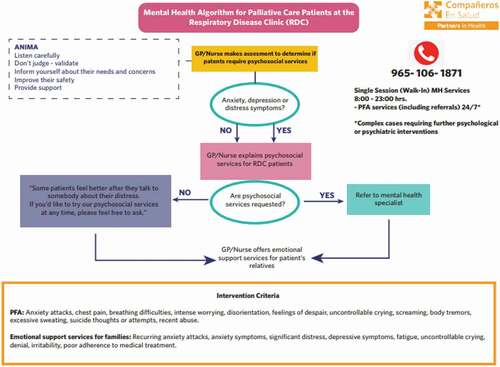
Training was provided to 292 people, both from CES and the MoH, from March 2020 to January 2021. These PFA workshops were based on the WHO’s PFA orientation guidelines [Citation27] and included a theoretical explanation of common reactions to stressful events, a practical review of relevant nonverbal cues, how to provide PFA (through modeling and peer practice), the referral system (see ), and self-care strategies. Because of the briefness of these trainings, a pocket field guide was designed for community staff, which was culturally adapted for both community health workers (CHWs) and community mental health workers (CMHWs).
Figure 3. Pathway of care of COVID-19 response at the Respiratory Disease Clinic. GP: general practitioner, MH: mental health, PFA: Psychological First Aid
Psychosocial training for Respiratory Disease Clinic staff
Besides the PFA training, physicians and nurses from the RDC were trained in the following topics: basic psychosocial support [Citation28], effective communication for conflict prevention and management, mental health referral criteria, bereavement and thanatological support, occupational therapy and COVID-19 rehabilitation [Citation29].
Training for Community Health Workers and adolescent volunteers
Currently, there are more than 80 CHWs and five CMHWs working in CES-supported rural communities. As a response to the increasing cases of COVID-19 in the communities, 44 CHWs and all of the CMHWs were trained in contact tracing. The home-visit questionnaire included three questions that explored mood, anxiety and suicidal thoughts. If people answered positively to the latter, they would be referred to a CMHW for further evaluation. Though both the CHWs and CMHWs were trained in grief and bereavement, CMHWs received a more in-depth training on this topic [Citation30]. In addition, 11 adolescent mental health volunteers participated in an introductory training to mental health and COVID-19 with a gender perspective, allowing them to provide information to their peers and refer other adolescents with mental health conditions to the health clinic.
Psychosocial support for the general population
This support constituted one of the pillars of CES’ mental health intervention during the pandemic, since specialized care was provided to patients with psychological needs in Ángel Albino Corzo and in the nine rural communities supported by CES.
Respiratory disease clinic
Hospitalized patients
Daily visits were made to hospitalized patients to assess their mental health, provide counseling (including thanatological accompaniment) and create rehabilitation plans. A total of 94 patients benefited from this support. Additionally, during these months, 23 occupational therapy kits were provided to patients, as a way of facilitating behavioral activation and improving the psychological well-being of hospitalized patients [Citation29]. These kits included activities such as: embroidery, reading, drawing, writing, listening to music, board games, relaxation exercises, and writing postcards for their loved ones. Refer to for the pathway of mental healthcare at the RDC.
When the pace of work allowed it, some of the activities were shared with the RDC health personnel, thus strengthening the doctor/nurse-patient trust relationship and reducing staff stress.
Communication with family members and psychoeducation
As a way of building communication bridges between the health personnel and the patients’ families at the RDC, a psychologist approached family members by providing psychoeducation and information for them to make informed decisions on issues such as hospital transfers, discharges, how to receive thanatological support, orientation on post-COVID-19 care, and strategies for adherence to treatment. In some cases, brief mental health counseling was also provided to family members.
Community
Psychosocial toolkits
With the aim of fostering well-being strategies for youth and families while socially distancing, two kinds of psychosocial toolkits were created: one for adolescents and one for families. More than 100 kits were sent to the rural primary care clinics for distribution by the physician. While both toolkits included mindfulness exercises and psychoeducation information, the youth toolkit consisted of occupational activities and the family toolkit of activities to foster family cohesion during lockdown [Citation31].
Material Support
Acknowledging that quarantine caused loss of working days, inability to access food supplies was a key determinant to be tackled for food security and decreasing stress. Right after people with suspected COVID-19 infection or their contacts received the recommendation to quarantine, they were screened for social support. Some of them met criteria for social vulnerability and 77 households received food packages and 179 hygiene kits as social aid. The hygiene kits included bleach and detergent, key to protecting other household members from infection.
Community mental health workers
CMHWs have been a crucial part of the COVID-19 mental health response as they have been providing. Problem Management Plus (PM+), a brief, low-intensity psychotherapy intervention developed by the WHO [Citation32]. Apart from this psychological intervention, they provided mental healthcare for patients who were grieving, in addition to palliative mental healthcare, as new ways of accompanying bereaved families had to be created due to COVID-19 [Citation33,Citation34]. During 2020, 43 patients were attended to by CMHWs due to a COVID-19-associated mental health condition.
Outpatient psychological accompaniment
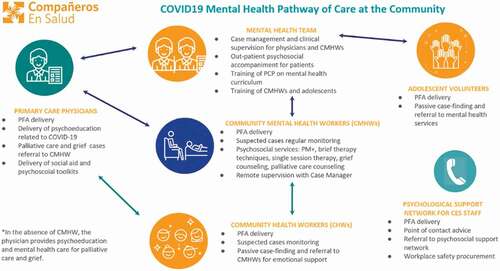
Several people began seeking psychological support, sometimes due to COVID-19-related emotional distress. In response, CES set up outpatient emotional support consultations provided by a physician and three psychologists. From April 2020 to February 2021, 89 patients have been enrolled and 203 consultations were provided. Refer to for the pathway of mental healthcare at the community level. Outpatient psychological accompaniment was also offered to patients residing in the town of Ángel Albino Corzo.
Figure 4. Mental health pathway of care at the community. PFA: Psychological First Aid, CMHW: community mental health workers, PCP: primary care physician
Staff mental health care
Part of the strategy to fight COVID-19 included the creation of psychosocial support structures for the organization’s clinical and non-clinical staff, given that isolation and increased distress and social adversity were being experienced.
Point of contact
Every person from the staff was allocated to a professional from the mental health team as a ‘point of contact’. The points of contact, if approached by a staff member, were instructed to offer advice around the organization’s psychosocial resources, including: a) psychological orientation, b) single session therapy, c) referral to CES´ psychosocial support network or to PIH´s remote psychosocial services, such as Konterra [Citation35], which included virtual mental health care in Spanish. From March 2020 to February 2021, over a fifth of CES´ staff (n = 46) have approached their point of contact at least once.
Mental health specialist network
A network of four psychologists and six psychiatrists comprised a virtual platform to which staff cases could be referred to for teleconsultations. In some cases, these experts were volunteers, and in other cases CES covered several consultations without cost for the user. These consultations included a risk assessment scale (from 0–3) that indicated whether or not the person’s own safety, the safety of others or their work duties were at risk, and if organizational support was needed. In cases where pharmacological treatment was needed, CES supplied it. During 2020, 53 people approached the network and over 155 consultations were provided.
Virtual wellbeing groups
During 2020, six open virtual meetings for all staff members were offered, during which mental health coping techniques were provided. These meetings were facilitated by a mental health team member or by a staff member that volunteered to share a topic with the group.
Debriefing and defusing groups
At the RDC, ongoing debriefing and defusing groups were organized with the staff members to encourage reflection on actions taken while managing complex patient care situations. Debriefing groups aimed at improving future performance and strengthening group cohesion [Citation36], while defusing groups, opened a safe space for professionals to have emotional catharsis and relieve stress [Citation37].
Workplace safety
Other supportive measures were implemented, such as providing staff with personal protective equipment (PPE), training them on how to use it, protocoling COVID-19 measures, and ensuring the creation of supervision and support channels, all of which contributed to building a safe workplace. Although these measures were not directly targeted at mental health, there is evidence that they prevent emotional distress among frontline workers [Citation38].
Discussion
The public health sector has been overwhelmed by the sudden and exponentially increasing burden of disease in Chiapas, resulting in a difficulty to prioritize mental health in an already under-resourced system. For this reason, the MoH has collaborated with civil society organizations, such as CES, to strengthen mental health services and address the recent mental health needs associated with the COVID-19 pandemic. This collaboration is possible through an interdisciplinary team of mental health specialists, primary care health providers, and CHWs (especially CMHWs).
One of the strengths of the CES model is that it provides on-site mental health care rather than waiting for financially vulnerable patients living in rural communities to seek services. This is a necessary shift in the healthcare paradigm that we achieved by integrating mental health care into the RDC and by providing community mental health care, in the primary care clinics and by interventions delivered by CMHWs.
The high burden of mental health issues among suspected and confirmed COVID-19 patients and their family members, especially hospitalized patients, makes it crucial to provide mental health services in facilities treating COVID-19 patients [Citation39]. Although there is little evidence for the efficacy of interventions addressing COVID-19 inpatient mental health [Citation40], two randomized controlled trials (RCTs) conducted in China demonstrated significant improvement in anxiety symptoms using relaxation routines among these patients [Citation41,Citation42]. Supporting public health facilities to address the mental health needs of COVID-19 inpatients and their companions has been one the pillars of the response of CES to the pandemic, but also of other NGOs in Latin America, such as Doctors Without Borders [Citation43].
In our work, we observed that not only did COVID-19 patients and their families experience the stress of uncertainty and the need to travel long distances to seek medical care, but also the financial burden of traveling and lodging. Therefore, intersectoral supportive programs that address the out-of-pocket expenses of patients and their families need to be contemplated. Once patients and their families return home, maintaining social support is critical to encourage people to maintain quarantine and prevent food insecurity related stress.
Since we began implementing the CES mental health response to COVID-19, we corroborated the importance of providing community-based mental health services. In many cases, CES services have been the only mental healthcare option for rural areas that could not access other services as these were unavailable. In addition, by providing mental healthcare through an all-female workforce of hired CMHWs, CES helps promote the creation of social and economic capital for women in these communities, ensures that the provided care is socio-culturally appropriate, and enables patients to benefit from the lived experiences of providers.
Globally, CHW programs are well established in many low-resource settings. Providing psychosocial support to communities through these professionals, who can also act as a liaison between community members and primary healthcare providers for more advanced mental health resources, may be a highly feasible alternative to respond to the reduced accessibility to mental health services and the increased burden of mental health issues due to the COVID-19 pandemic, as it can be more cost-effective than other alternatives [Citation44,Citation45]. Apart from our intervention, during the pandemic there have been other initiatives aimed at empowering communities to address mental health issues associated with the pandemic in LMICs, such as the BasicNeeds Pakistan initiative, which has trained over 3,600 community members as ‘Mental Health First Aiders’ [Citation46], or the United Nations Refugee Agency (UNHCR) in Iraq, which provides psychosocial support to people living in refugee camps during the health emergency through CHWs, most of them refugees who provide PM+ psychotherapy [Citation47].
Interventions should also be focused and tailored to groups at higher risk of developing mental health conditions due to COVID-19, such as women, adolescents, and frontline healthcare workers.
Studies from different areas of the world indicate that female gender is being significantly associated with worse mental health outcomes during the COVID-19 pandemic [Citation48–51]. Women have a higher prevalence of risk factors for mental issues than men that have intensified during the virus outbreak, such as chronic environmental stress [Citation52], preexisting prevalence of depressive and anxiety disorders [Citation53], and intimate partner violence [Citation54]. In addition, fear of perinatal complications due to COVID-19 infection or difficulties in accessing perinatal care have significantly increased the incidence of mental health issues among pregnant women worldwide during the pandemic [Citation55,Citation56]. This highlights the importance of implementing mental health interventions with a gender perspective. In our working context, many female patients have mentioned an increased workload; in addition to taking care of the household and children, women must now ensure that their children do their homework and that they care for family members with COVID-19. Additionally, the temporary suspension of some church activities has hampered women’s social networks, one of the few spaces where women socialize [Citation14], which threatens to leave women living with domestic violence more isolated. Women are also the most affected by the economic stress associated with the pandemic [Citation57], so it is essential to address gender-based social inequalities by improving women’s access to communication technologies and creating fair employment opportunities.
In relation to adolescents, different studies have identified more depressive and anxious symptoms compared to pre-pandemic estimates among this population around the globe [Citation58]. In a poll conducted by UNICEF in Latin America and the Caribbean in mid-2021, 27% of adolescent and youth participants reported feeling symptoms of anxiety and 15% of depression in the seven days prior to the survey [Citation59]. One of the main reasons behind these alarming figures is the fact that this population is under greater stress and suffers from a lack of activity due to the suspension of face-to-face school activities [Citation60]. In the specific case of Chiapas, schools have opted to grade assignments that require searching the web, without considering that some adolescents have difficulty accessing mobile devices or covering the costs associated with internet access. This concern adds to a greater burden of responsibilities such as household chores or agricultural work. There is a global need to ameliorate the effects of the pandemic on the mental health of adolescents by improving the availability and accessibility of mental healthcare services for this population. This should be done through the collaboration of adolescents, their parents, health professionals, civil society actors and the government, and by reconciling epidemiological control measures with the specific needs of the adolescent population [Citation60].
Worldwide, frontline healthcare professionals have suffered from a severe shortage of PPE and lack of comprehensive training in the care of COVID-19 patients, raising concerns about risk of infection, which has negatively impacted their mental health. In addition, the safety of their families and friends, the death of their colleagues, ethical concerns in clinical practice and excessive work hours have added to the detrimental effect of the pandemic on the mental wellbeing of these professionals [Citation39,Citation61]. Due to the impossibility of meeting these demands by overwhelmed public health sectors, the support of civil society organizations can be key in supporting the MoH in addressing them, as exemplified by our interventions and others from LMICs [Citation62,Citation63].
Finally, we also acknowledge that providing mental health care and health personnel capacity building during the pandemic in areas with poor access to digital devices and Information and Communications Technologies (ICTs) might be challenging and labor-intensive. To ensure participant safety, it has been necessary to limit several face-to-face mental health-related activities. However, in settings with good access to digital devices and ICTs, some of these activities can be adapted to be delivered remotely [Citation64,Citation65]. In our case, due to lack of internet access psychoeducation groups and patient involvement in behavioral activation activities had to be suspended. As for the health personnel training, poor internet connection resulted in having to facilitate several small group trainings in person.
From our work during the pandemic we conceived a broader idea of what kinds of interventions may be more appropriate to prevent and address the effects of the pandemic on people’s mental health in our context. However, the described intervention is limited to our context given the available resources, the barriers and the facilitators for implementing which might be diverse in different settings. For instance, the CES model relies on donations which are used to provide stipends for the staff and ensure the availability of supplies. This model also operates with highly motivated staff and ongoing training adapted to our particular context so that staff can acquire clinical competency. CES also has a successful collaboration with the MoH that allows operation within government facilities and collaboration with their staff. Hence, this paper is limited to describing and discussing our fieldwork experiences. We plan to assess the impact of our interventions in a future study that compares mental health outcomes in CES-supported areas with non-CES-supported areas during the pandemic period. This study will be the first to report on the effectiveness of mental health interventions in low-income rural communities with very limited access to digital devices and ICT during the COVID-19 pandemic and to report the experience of delivering mental health services within a COVID inpatient unit such as the RDC.
Conclusions
There is a lack of mental health services for rural communities impacted by COVID-19 in Chiapas. Through a comprehensive strategy, CES addresses this gap and complements the available services created by the MoH, while caring for the wellbeing of the professionals who deliver the services. In marginalized communities, there is an urgent need to: 1) address the social determinants that increase their vulnerability to suffering from mental health conditions related to the pandemic, and 2) adapt mental health services to follow sanitary measures and be accessible to those living in rural and inaccessible areas with poor access to technology. In addition, psychosocial support is necessary to prevent and contain the mental health effects of the pandemic. Therefore, it is urgent that healthcare professionals have ongoing training in basic psychosocial support skills and for interventions to meet the needs of vulnerable populations – such as people with disabilities, older adults, children, and adolescents – that involve the voice of communities.
COVID-19 has made the need to prioritize mental health services more visible, and presents an opportunity to reimagine global mental health by building health systems using a task-sharing approach.
Ethics and consent
Due to the descriptive nature of this work, institutional review board approval was not applicable in this case. Nevertheless, all interventions implemented by CES and the MoH described in the manuscript received approval from the management of the basic community hospital of Ángel Albino Corzo when applicable and from the authorities of the Health Jurisdictions IV and X of Chiapas, always within the framework of the ethical guidelines stipulated by the MoH.
Paper context
The mental health of marginalized populations has been most affected by the COVID-19 pandemic due to the limited human, economic, and social resources available. This article describes a public-civil partnership initiative to address the increased burden of mental illness in rural Mexico through capacity building and mental health care for health professionals and provision of psychosocial support for the general population. This is an opportunity to reimagine global mental health through comprehensive community-based initiatives.
Acknowledgments
We thank Paola Rodriguez-Cuevas for her support in the design of the figures included in this manuscript. We thank Vivian Chung and specially Gerogina Miguel-Esponda and Harvey Aspelling-Jones for proofreading the manuscript prior to submission. We greatly appreciate the hard work of the community mental health workers who have made it possible to combat the mental health burden associated with the pandemic in the rural communities supported by CES.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Ana Cecilia Ortega
FGRC, ACO, EV and ZA contributed equally in the design of the work, the drafting, review and editing of the work, and revising the article. GP and SM contributed equally to the design of the work and drafting. All co-authors are accountable for all aspects of the work.
References
- Zhang Y, Lange KW. Coronavirus disease 2019 (COVID-19) and global mental health. Glob Heal J [Internet]. 2021 Mar;5:31–12. [cited 2021 Apr 26].
- Wu T, Jia X, Shi H, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2021;281:91–98. Elsevier B.V.
- Serafini G, Parmigiani B, Amerio A, et al. The psychological impact of COVID-19 on the mental health in the general population. QJM An Int J Med [Internet]. 2020 Aug 1;113:531–537. [cited 2021 Apr 26]. Available from: https://academic.oup.com/qjmed/article/113/8/531/5860841
- González RLP, Martínez ARJ, Hernández-Gonzalez M, et al. Psychological distress and signs of post-traumatic stress in response to the COVID-19 health emergency in a mexican sample. Psychol Res Behav Manag [Internet]. 2020 Jul 22;13:589–597. [cited 2021 Apr 26]. Available from: https://www.dovepress.com/psychological-distress-and-signs-of-post-traumatic-stress-in-response–peer-reviewed-article-PRBM
- Mamun MA, Sakib N, Gozal D, et al. The COVID-19 pandemic and serious psychological consequences in Bangladesh: a population-based nationwide study. J Affect Disord. 2021 Jan 15;279:462–472.
- Salameh P, Badro DA, Abou Selwan C, et al. Mental health outcomes of the COVID-19 pandemic and a collapsing economy: perspectives from a developing country. Psychiatry Res. 2020 Dec 1;294:113520.
- Cai Q, Feng H, Huang J, et al. The mental health of frontline and non-frontline medical workers during the coronavirus disease 2019 (COVID-19) outbreak in China: a case-control study. J Affect Disord. 2020 Oct 1;275:210–215.
- World Health Organization. COVID-19 disrupting mental health services in most countries, WHO survey [Internet]. 2020 [cited 2021 Apr 26]. Available from: https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey
- Kola L, Kohrt BA, Hanlon C, et al. COVID-19 mental health impact and responses in low-income and middle-income countries: reimagining global mental health. Lancet Psychiatry [Internet]. 2021 Feb 24;8:535–550. [cited 2021 Mar 19]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/33639109
- Instituto Nacional de Estadística y Geografía. Resumen. Chiapas [Internet]. 2019 [cited 2021 Apr 26]. Available from: http://www.cuentame.inegi.org.mx/monografias/informacion/chis/default.aspx?tema=me&e=07
- Elliott ML, Aguerrebere M, Elliott PF. Depression in rural communities and primary care clinics in Chiapas, Mexico. J Epidemiol Glob Health [Internet]. 2019 Jun 1;9:103–106. [cited 2020 Oct 21].
- Belló M, Puentes-Rosas E, Medina-Mora ME. Prevalencia y diagnóstico de depresión en población adulta en México. Salud Publica Mex [Internet]. 2005;47. [cited 2021 Apr 26]. Available from: https://saludpublica.mx/index.php/spm/article/view/4683
- Serván-Mori E, Gonzalez-Robledo LM, Nigenda G, et al. Prevalence of depression and generalized anxiety disorder among Mexican indigenous adolescents and young adults: challenges for healthcare. Child Psychiatry Hum Dev [Internet]. 2021 Feb 1;52:179–189. [cited 2021 Apr 26]. Available from: https://link.springer.com/article/10.1007/s10578-020-01001-9
- Aguerrebere M. Understanding intimate partner violence, sexual abuse, and mental health in non-indigenous rural chiapas: implications for global mental health practice [Internet]. Harvard Med School. 2018. [cited 2021 Apr 26]. Available from: https://dash.harvard.edu/handle/1/37365183
- Holmes EA, O’Connor RC, Perry VH, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science [Internet]. Lancet Psychiatry Elsevier Ltd. 2020;7:547–560. [cited 2021 Apr 26]. Available from: www.thelancet.com/psychiatry
- Secretaría de Salud de Chiapas. Estrategias contra COVID-19 y sólida integración del sector salud, fortalezas de Chiapas: JMCC [Internet]. 2020 [cited 2021 Apr 26]. Available from: https://saludchiapas.gob.mx/noticias/post/estrategias-contra-covid-19-y-solida-integracion-del-sector-salud-fortalezas-de-chiapas-jmcc
- World Health Organization, Secretaría de Salud de México. Informe de la evaluación del sistema de salud mental en México utilizando el Instrumento de Evaluación para Sistemas de Salud Mental de la Organización Mundial de la Salud [Internet]. México; 2011 [cited 2021 Apr 26]. Available from: https://www.who.int/mental_health/who_aims_country_reports/who_aims_report_mexico_es.pdf
- Secretaría de Salud de Chiapas. Atención a la salud mental, eje principal durante la pandemia de COVID-19 [Internet]. 2020 [cited 2021 Apr 26]. Available from: https://saludchiapas.gob.mx/noticias/post/atencion-la-salud-mental-eje-principal-durante-la-pandemia-de-covid-19
- van Ginneken N, Tharyan P, Lewin S, et al. Non-specialist health worker interventions for the care of mental, neurological and substance-abuse disorders in low- and middle-income countries [Internet]. Vol. 2013, Cochrane Database of Systematic Reviews. John Wiley and Sons Ltd. 2013 [cited 2021 Apr 26]. Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD009149.pub2/full
- Belkin GS, Unützer J, Kessler RC, et al. Scaling up for the “bottom billion”: “5x5” Implementation of community mental health care in low-income regions [Internet]. Psychiatric Serv American Psychiatric Association. 2011;62:1494–1502. [cited 2021 Apr 26]. Available from: https://pubmed.ncbi.nlm.nih.gov/22193798/
- Acharya B, Ekstrand M, Rimal P, et al. Collaborative care for mental health in low- and middle-income countries: a WHO health systems framework assessment of three programs. Psychiatr Serv [Internet]. 2017 Sep 1;68:870–872. [cited 2021 Apr 26]. Available from: http://psychiatryonline.org/doi/10.1176/appi.ps.201700232
- Partners In Health. StopCOVID: PIH Mental Health and Psychosocial Response (Boston: Partners In Health). 2020.
- Inter-Agency Standing Committee. IASC guidelines on mental health and psychosocial support in emergency settings [Internet]. Geneva. 2007 [cited 2021 May 3]. Available from: https://www.who.int/mental_health/emergencies/guidelines_iasc_mental_health_psychosocial_june_2007.pdf
- Minihan E, Gavin B, Bd K, et al. COVID-19, mental health and psychological first aid [Internet]. Ir J Psychol Med Cambridge University Press. 2020;37:259–263. [cited 2021 Apr 26]. Available from: https://www.cambridge.org/core/journals/irish-journal-of-psychological-medicine/article/covid19-mental-health-and-psychological-first-aid/865E40C7E9D71AF37BE6CAD751DDCF37
- Bisson JI, Lewis C. Systematic review of psychological first aid [Internet]. 2009 [cited 2021 Apr 26]. Available from: https://www.researchgate.net/publication/265069490_Systematic_Review_of_Psychological_First_Aid
- Dieltjens T, Moonens I, Van Praet K, et al. A systematic literature search on psychological first aid: lack of evidence to develop guidelines. Matsuoka Y, editor. PLoS One [Internet]. 2014 Dec 12;9:e114714. [cited 2021 Apr 26]. Available from: https://dx.plos.org/10.1371/journal.pone.0114714
- World Health Organization. Psychological First Aid: guide for field workers [Internet]. 2011 [cited 2021 Apr 26]. Available from: https://apps.who.int/iris/bitstream/handle/10665/44615/9789241548205_eng.pdf%3Bjsessionid=D13BC24B5197D91DDE76E6EFCF79A53A?sequence=1%3Bhttps://apps.who.int/iris/bitstream/handle/10665/102380/9789241548618_eng.pdf?sequence=1
- Inter-Agency Standing Committee. Habilidades Psicosociales Básicas: guía para personal de Primera Línea de Respuesta a la COVID-19 [Internet]. 2020 [cited 2021 Apr 26]. Available from: www.unocha.org/story/ocha-releases-
- Colegio Profesional de Terapeutas Ocupacionales de la Comunidad de Madrid. Guía clínica de intervención de terapia ocupacional en pacientes con COVID-19 [Internet]. 2020. [cited 2021 Apr 26]. Available from: https://coptocam.org/wp-content/uploads/2020/05/Guía-clínica-de-TO-covid-19-.pdf
- Rolland JS. Helping couples and families navigate illness and disability: an integrated approach. New York: Guilford Publications; 2018.
- León L. Más de 150 juegos para divertirse dentro y fuera del hospital: porque que sonrían también es urgente. Barcelona: Grupo Planeta; 2016.
- World Health Organization. Problem Management Plus (PM+): individual psychological help for adults impaired by distress in communities exposed to adversity [Internet]. Geneva; 2018 [cited 2021 Mar 22]. Available from: https://apps.who.int/iris/bitstream/handle/10665/206417/WHO_MSD_MER_16.2_eng.pdf;jsessionid=4D41459E6012AB4432FD478DB5490AF8?sequence=1
- Jacobson NC, Lord KA, Newman MG. Perceived emotional social support in bereaved spouses mediates the relationship between anxiety and depression. J Affect Disord. 2017 Mar 15;211:83–91.
- Carr D, Boerner K, Moorman S. Bereavement in the Time of Coronavirus: unprecedented Challenges Demand Novel Interventions. J Aging Soc Policy [Internet]. 2020 Jul 3;32:425–431. [cited 2021 Apr 26]. Available from: https://www.tandfonline.com/action/journalInformation?journalCode=wasp20
- Konterra Group. Konterra group – clarity. Resilience. Learning [Internet]. 2021; [cited 2021 Apr 26]. Available from: https://konterragroup.net/
- Patient Safety Network. Debriefing for Clinical Learning [Internet]. 2019 [cited 2021 Apr 26]. Available from: https://psnet.ahrq.gov/primer/debriefing-clinical-learning
- Prada AA. Mindfulness y Autocompasión para Profesionales de la Salud que enfrentan al COVID 19 [Internet]. Bogotá; 2020 [cited 2021 Apr 26]. Available from: http://www.colegiomedico.cl/wp-content/uploads/2020/05/Manual-para-Profesionales_compressed.pdf
- Kisely S, Warren N, McMahon L, et al. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: rapid review and meta-analysis. BMJ [Internet]. 2020 May 5;369:m1642. [cited 2021 Apr 26].
- Krishnamoorthy Y, Nagarajan R, Saya GK, et al. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. 2020 Nov 1;293:113382.
- Damiano RF, Di Santi T, Beach S, et al. Mental health interventions following COVID-19 and other coronavirus infections: a systematic review of current recommendations and meta-analysis of randomized controlled trials. Brazilian J Psychiatry [Internet]. 2021 Apr 12; [cited 2021 Oct 7]. Available from: http://www.scielo.br/j/rbp/a/Md4wRMM9q9wCgbQShGzNbnf/?lang=en
- Wei N, Huang B, Lu S, et al. Efficacy of internet-based integrated intervention on depression and anxiety symptoms in patients with COVID-19. J Zhejiang Univ Sci B [Internet]. 2020 May 1;21:400. [cited 2021 Oct 7]. Available from: http://pmc/articles/PMC7203540/
- Liu K, Chen Y, Wu D, et al. Effects of progressive muscle relaxation on anxiety and sleep quality in patients with COVID-19. Complement Ther Clin Pract. 2020 May 1;39:101132.
- ReliefWeb. Honduras: providing psychosocial support to COVID-19 patients [Internet]. 2020 [cited 2021 Apr 26]. Available from: https://reliefweb.int/report/Honduras/Honduras-providing-psychosocial-support-covid-19-patients
- Mistry SK, Harris-Roxas B, Yadav UN, et al. Community health workers can provide psychosocial support to the people during COVID-19 and beyond in low- and middle- income countries. Front Public Health. 2021;800.
- Vaughan K, Kok MC, Witter S, et al. Costs and cost-effectiveness of community health workers: evidence from a literature review. Hum Resour Heal 2015 [Internet]. 2015 Sep 1;13:1–16. [cited 2021 Oct 7]. Available from: https://human-resources-health.biomedcentral.com/articles/10.1186/s12960-015-0070-y
- Yasmeen F. BasicNeeds Pakistan: supporting mental health in under-resourced communities during the COVID-19 pandemic [Internet]. Mental Health Innovation Network. 2020 [cited 2021 Apr 26]. Available from: https://www.mhinnovation.net/blog/2020/may/12/basicneeds-Pakistan-supporting-mental-health-under-resourced-communities-during
- Rasheed Hussein Rasheed. Los refugiados brindan servicios de salud mental a campamentos cerrados en Irak [Internet]. Alto Comisionado de las Naciones Unidas para los Refugiados. 2020 [cited 2021 Apr 26]. Available from: https://www.acnur.org/noticias/historia/2020/7/5f063ce14/los-refugiados-brindan-servicios-de-salud-mental-a-campamentos-cerrados.html
- Wang C, Pan R, Wan X, et al. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int J Environ Res Public Health [Internet]. 2020 Mar 1;17:1729. [cited 2021 Oct 7]. Available from: http://pmc/articles/PMC7084952/
- Liu N, Zhang F, Wei C, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. 2020 May 1;287:112921.
- García-Fernández L, Romero-Ferreiro V, Padilla S, et al. Gender differences in emotional response to the COVID-19 outbreak in Spain. Brain Behav [Internet]. 2021 Jan 1;11:e01934. [cited 2021 Oct 7]. Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/brb3.1934
- Miguel‐Puga JA, Cooper‐Bribiesca D, Avelar‐Garnica FJ, et al. Burnout, depersonalization, and anxiety contribute to post‐traumatic stress in frontline health workers at COVID‐19 patient care, a follow‐up study. Brain Behav [Internet]. 2021 Mar 15;11:e02007. [cited 2021 Apr 27]. Available from: https://onlinelibrary.wiley.com/doi/10.1002/brb3.2007
- Street AE, Dardis CM. Using a social construction of gender lens to understand gender differences in posttraumatic stress disorder. Clin Psychol Rev. 2018 Dec;1:97–105.
- Hao F, Tan W, Jiang L, et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav Immun. 2020 Jul 1;87:100–106.
- Campbell AM. An increasing risk of family violence during the Covid-19 pandemic: strengthening community collaborations to save lives. Forensic Sci Int Rep. 2020 Dec 1;2:100089.
- Wu Y, Zhang C, Liu H, et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am J Obstet Gynecol [Internet]. 2020 Aug 1;223:240.e1–240.e9. [cited 2021 Oct 7]. Available from: http://www.ajog.org/article/S0002937820305342/fulltext
- Berthelot N, Lemieux R, Garon-Bissonnette J, et al. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet Gynecol Scand [Internet]. 2020 Jul 1;99:848–855. [cited 2021 Oct 7]. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/aogs.13925
- UN Women – Americas and the Caribbean. The Economic Impact of COVID-19 on Women in Latin America and the Caribbean [Internet]. 2020 [cited 2021 Apr 27]. Available from: https://lac.unwomen.org/en/noticias-y-eventos/articulos/2020/11/impacto-economico-covid-19-mujeres-america-latina-y-el-caribe
- Samji H, Wu J, Ladak A, et al. Review: mental health impacts of the COVID-19 pandemic on children and youth – a systematic review. Child Adolesc Ment Health. 2021 [cited 2021 Oct 7]. [Internet]. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/camh.12501
- UNICEF Latin America and Caribbean. The impact of COVID-19 on the mental health of adolescents and youth [Internet]. 2021 [cited 2021 Oct 7]. Available from: https://www.unicef.org/lac/en/impact-covid-19-mental-health-adolescents-and-youth
- Singh S, Roy D, Sinha K, et al. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res [Internet]. 2020 Nov 1;293:113429. [cited 2021 Oct 7]. Available from: http://pmc/articles/PMC7444649/
- Da Silva FCT, Neto MLR. Psychological effects caused by the COVID-19 pandemic in health professionals: a systematic review with meta-analysis. Prog Neuro Psychopharmacol Biol Psychiatry. 2021 Jan 10;104:110062.
- Barrientos E. Historias desde Chile: experiencias de atención en salud mental y apoyo psicosocial durante la pandemia [Internet]. Mental Health Innovation Network. 2020 [cited 2021 Apr 27]. Available from: https://www.mhinnovation.net/blog/2020/oct/23/historias-desde-Chile-experiencias-de-atención-en-salud-mental-y-apoyo-psicosocial
- Mental Health Innovation Network. Pursukoon Zindagi “Peaceful Life” COVID-19 Mental Health Response [Internet]. 2020 [cited 2021 Apr 27]. Available from: https://www.mhinnovation.net/innovations/pursukoon-zindagi-peaceful-life-covid-19-mental-health-response
- Graham AK, Weissman RS, Mohr DC. Resolving key barriers to advancing mental health equity in rural communities using digital mental health interventions. JAMA Heal Forum [Internet]. 2021 Jun 4;2:e211149–e211149. [cited 2021 Oct 7]. Available from: https://jamanetwork.com/journals/jama-health-forum/fullarticle/2781098
- Gillian SS, Kassam I, Sequeira L, et al. Digital interventions to support population mental health in canada during the COVID-19 pandemic: rapid review. JMIR Ment Heal [Internet]. 2021;8:e26550. [cited 2021 Oct 7]. Available from: https://mental.jmir.org/2021/3/e26550