
ABSTRACT
Background
Sub-Saharan Africa (SSA) faces a critical shortage of pediatric surgical providers. International partnerships can play an important role in pediatric surgical capacity building but must be ethical and sustainable.
Objective
The purpose of this study is to perform a scoping literature review of international pediatric surgery partnerships in SSA from 2009 to 2019. We aim to categorize and critically assess past partnerships to aid in future capacity-building efforts.
Methods
We performed a scoping literature review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) guidelines. We searched the PubMed and Embase databases for articles published from 2009 to 2019 using 24 keywords. Articles were selected according to inclusion criteria and assessed by two readers. Descriptive analyses of the data collected were conducted in Excel.
Results
A total of 2376 articles were identified. After duplicates were removed, 405 articles were screened. In total, 83 articles were assessed for eligibility, and 62 were included in the review. The most common partnership category was short-term surgical trip (28 articles, 45%). A total of 35 articles (56%) included education of host country providers as part of the partnership. Only 45% of partnerships included follow-up care, and 50% included postoperative outcomes when applicable.
Conclusions
To increase sustainability, more partnerships must include education of local health-care providers, and short-term surgical trips must be integrated into long-term partnerships. More partnerships need to report postoperative outcomes and ensure follow-up care. Educating peri-operative providers, training general surgeons in common pediatric procedures, and increasing telehealth use are other goals for future partnerships.
Responsible editor
Jennifer Stewart Williams
Background
An estimated five billion people worldwide do not have access to surgical and anesthesia care. The disparity in surgical care availability disproportionately affects sub-Saharan Africa (SSA), where an estimated 93% of the population do not have access [Citation1]. When addressing the shortage of surgical care in SSA, specific consideration must be given to the pediatric population. According to UNICEF’s Generation 2030 Africa 2.0 report, 47% of Africa’s population is under 18 years old (yo), which accounts for 25% of the world’s children. Children currently represent more than half of the total population in one-third of the countries in Africa. By 2030, Africa’s under-18 population will increase by 170 million [Citation2].
Most of the child population increase in the continent will occur in SSA. By the end of the century, births in Western and Eastern Africa will account for two-thirds of all births in the continent. The proportion of the continent’s births that occur in Northern Africa has decreased since 1950, with decline projected to continue [Citation2].
To address the overall shortage of surgical providers in low-and-middle-income countries (LMICs), the Lancet Global Surgery 2030 report recommends that each country scale up their surgical workforce to 20 surgical providers per 100,000 population by 2030. To achieve this goal, approximately 1.27 million additional surgical providers will need to be trained [Citation1]. When considering pediatric surgery, in the United States it is estimated that one pediatric surgeon is needed for every 100,000 children 0–15 yo, yet in Africa there is an estimated one pediatric surgeon for every six million children 0–14 yo [Citation3].
For many years, global health initiatives have prioritized individual and communicable diseases, while relatively less attention has been given to scaling up surgical care in LMICs [Citation1,Citation4,Citation5]. However, surgical conditions comprise 28–32% of the global disease burden. In 2010, more lives were lost worldwide from surgical conditions than from HIV/AIDS, tuberculosis, and malaria combined, and the non-communicable disease burden will continue to increase in coming years [Citation1].
The Lancet Global Surgery 2030 report points out the important role that global health efforts, non-governmental organizations (NGOs), and other international partners can play in scaling up surgical capacity in LMICs, particularly regarding education and training [Citation1]. Given the great disparity in surgical care in SSA and the current and future need for pediatric surgery in the region, increasing pediatric surgery capacity in SSA should be a global health priority.
In recent years, the strategy of global health efforts has shifted from short-term initiatives with little long-term impact towards more sustainable models that prioritize the needs of the local community [Citation6]. The downfalls of short-term global health initiatives are particularly apparent in surgery, including a lack of follow-up care after visiting surgeons leave, variable long-term benefit, and a lack of accountability for poor postoperative (post-op) outcomes, among others [Citation6–8]. Recommendations for ethical, sustainable global surgery efforts suggest that all initiatives have a training component for local health-care providers, that post-op outcomes be monitored and reported, and that short-term trips should be part of long-term partnerships [Citation1,Citation6].
Considering the important role that global health initiatives may play in addressing the unmet need for pediatric surgical care in SSA, it is important to assess the quality of previous international pediatric surgery partnerships in the region. This is essential for planning ethical and effective partnerships in the future. To date, there have only been two other literature reviews published on the subject. The first was a systematic literature review published in 2014 appraising literature published from 1990 to 2012 in three databases, which found 31 articles representing only 16 countries in SSA. From these, the authors defined four broad categories of pediatric surgery partnerships. None of the articles reviewed included data on training local health-care providers, and none measured any outcomes from the partnership activities [Citation8]. The second was a general review article from 2016 about developing pediatric surgery in LMICs that did not follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, report methods, nor specify a date range for the articles reviewed [Citation3].
The purpose of this study is to perform a scoping literature review of international pediatric surgery partnerships in SSA published from 2009 to 2019. We will categorize and critically assess all types of partnership activities in order to aid in the development of effective and sustainable global surgery efforts. This review will specifically address how many international pediatric surgery partnerships include education or training of local health-care providers, how many of these report educational outcomes, how many report post-op follow-up and patient outcomes, how many assess the attitudes of participants from SSA, how many include training of non-surgeon health-care providers, and how many report a funding source.
Methods
Search strategy and selection criteria
This study is a scoping literature review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) guidelines. Using the PubMed and Embase databases, we searched for articles published in English, French, and Portuguese from January 2009 – December 2019 that had a full text available. Searches were performed using 24 key words () each combined with the additional search terms ‘surgery AND Africa AND (pediatric OR child)’. For articles published in French and Portuguese, Google Translate was used to translate abstracts and articles to English when an English version was not available.
Table 1. Keywords used in database searches.
Inclusion criteria: article published in a peer-reviewed journal; article describes a specific surgery partnership between one country in SSA and another country either in SSA or a different continent (we used the Library of Congress Africana Collections list of countries in SSA [Citation9]); article either specifically focuses on a pediatric patient population or includes demographic data showing patient age that includes patients <18 yo; and the article was a primary source for the surgery partnership described (not a review article).
The first author (AW) performed the initial data extraction, and the second author (CS) evaluated all articles along with AW to determine inclusion. The third author (BH) resolved any conflicts over article inclusion.
Data analysis
All results of each search from both databases were imported into EndNote. We used EndNote software to identify and eliminate duplicate articles. Each full-text article included in the final review was read in-depth two to three times to determine if it included qualitative, descriptive information about training of health-care providers in SSA as part of the partnership activity, and if any educational outcomes were reported. Educational outcomes are defined as any measure of skill transfer, performance (such as exam scores), number of providers trained, or any other form of measured improvement reported after partnership activities took place.
Other data extracted included post-op patient outcomes, whether post-op follow-up was present, funding sources, education of non-surgeon providers including the type of provider, how long short-term surgical trips lasted and if they recurred in the same location, and if the article assessed the attitudes and perspectives of SSA partners. Descriptive analyses of the data collected were conducted in Excel.
Funding information
There was no funding source for this study. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
Database searches identified a total of 2403 articles. After duplicates were removed, 421 articles were screened. In total, 87 full-text articles were assessed for eligibility, and 63 articles were included in the review. The database searches yielded significantly more English articles than French or Portuguese (). In total, 18 categories of international pediatric surgery partnerships were identified (). In total, 34 articles were assigned to more than one category [Citation10–43]. The most common category was short-term surgical trip [Citation13,Citation18,Citation20,Citation25–50] (29 articles, 46%) followed by NGO partnership [Citation10,Citation11,Citation13,Citation19–24,Citation26–30,Citation32–34,Citation36–43,Citation51–53] (28 articles, 44%). Within the short-term surgical trip category, trips ranged from three days to three months, with ten days and two weeks being the most common lengths. Twenty of the articles (71%) described short-term trips that recurred in the same location [Citation12,Citation21,Citation25,Citation27–32,Citation34–37,Citation39,Citation41–44,Citation46,Citation47] (see ).
Figure 1. PRISMA 2020 flow diagram showing study selection and number of articles from each publication language.
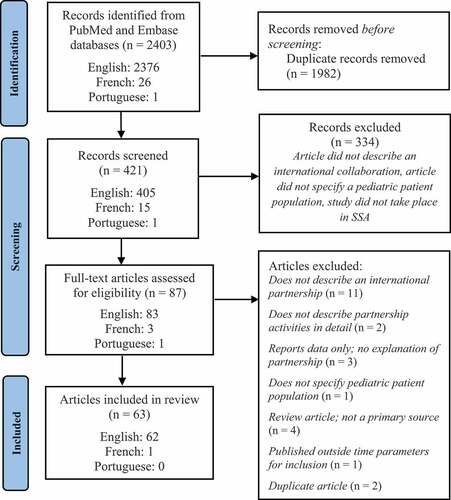
Table 2. Categories of partnerships identified with definitions, results breakdown, and notes.
Thirty-seven countries in SSA were represented (). In this review, the term ‘host country’ refers to a country in SSA where partnership activities take place, and ‘partner country’ refers to another country (either in SSA or another region) that travels to the host country for partnership activities. Fifteen partner countries were identified (). In two articles, a partner country was another country in SSA (South Africa [Citation17] and Kenya [Citation10]). In three articles, a partner country was another LMIC outside the SSA region (Brazil [Citation16], Egypt [Citation50], and India [Citation47]). The most common host countries were Kenya (12 articles [Citation11,Citation14,Citation25,Citation35,Citation38,Citation46,Citation49,Citation51,Citation52,Citation54–56]:) and Ethiopia (11 articles [Citation10,Citation13,Citation25,Citation28–30,Citation40,Citation42,Citation51,Citation52,Citation57]:). The most common partner countries were the USA (US) (27 articles [Citation10,Citation11,Citation13,Citation14,Citation16,Citation22,Citation25,Citation30,Citation32–34,Citation37,Citation39,Citation45–48,Citation51,Citation52,Citation54,Citation55,Citation58–63]:) and the UK (11 articles [Citation25,Citation28,Citation35,Citation36,Citation40,Citation42,Citation47,Citation56,Citation61,Citation64,Citation65]:).
Figure 2. Heat map indicating the number of articles in which each country in SSA is mentioned.
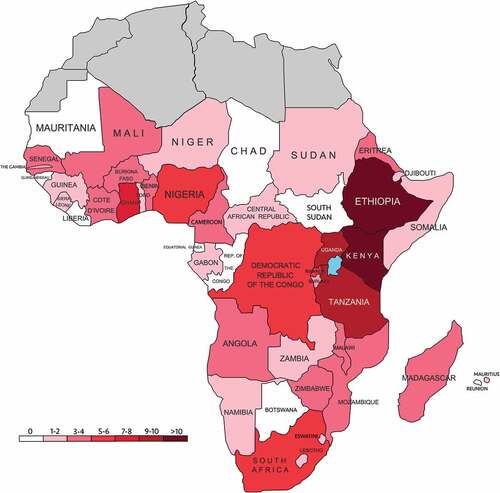
Table 3. Partner countries and how many articles in which each appears.
Twelve surgical specialties were represented, with cardiac surgery (21 articles, 34%) [Citation14,Citation15,Citation17–20,Citation22,Citation25,Citation29,Citation32,Citation37,Citation39–42,Citation47,Citation48,Citation53,Citation61,Citation66,Citation67] and general pediatric surgery (14 articles, 23%) [Citation14,Citation16,Citation27,Citation31,Citation45,Citation50,Citation54,Citation56,Citation58,Citation60,Citation63–65,Citation68] being the most common ().
Figure 3. Types of surgery and the number of articles in which each appears. *Cleft lip and palate surgery can be performed by multiple surgical specialists, so when the type of surgeon was not defined these were included in a cleft lip and palate category.
Thirty-six articles (57%) included education or training of host country health-care providers as part of the partnership activities [Citation10–17,Citation22,Citation25–27,Citation29,Citation31,Citation33–36,Citation38,Citation42–45,Citation54,Citation56–62,Citation64,Citation66–69]. Of these, 19 articles (53%) reported an outcome measure for the educational activities [Citation10,Citation14–16,Citation22,Citation25,Citation31,Citation33,Citation36,Citation38,Citation42,Citation43,Citation45,Citation54,Citation57,Citation59,Citation62,Citation64,Citation68] (for a list of educational outcomes reported, see ). In the short-term surgical trip category, 15 of 29 articles (52%) included education, followed by NGO partnership (13/28, 46%), long-term surgical volunteers (1/3, 33%), and international patient transfer (1/6, 17%). Five articles (8%) included training general surgeons in pediatric surgical techniques [Citation31,Citation33,Citation34,Citation60,Citation64]. In total, 17 articles (27%) included education or training for non-surgeon, peri-op health-care providers, such as nurses or anesthetists [Citation10,Citation11,Citation15,Citation16,Citation22,Citation26,Citation28,Citation31,Citation33,Citation36,Citation38,Citation42,Citation58–60,Citation62,Citation64] (see for the types of peri-op providers trained).
In 15 articles, partnership activities focused on education only or did not involve direct operation on host country patients. For these articles, post-op follow-up and patient outcomes were deemed not applicable [Citation10,Citation11,Citation13,Citation14,Citation16,Citation45,Citation54–56,Citation60,Citation61,Citation64,Citation66–68]. In the remaining 48 articles, 21 (45%) included post-op follow-up care [Citation12,Citation15,Citation17,Citation18,Citation20–23,Citation27,Citation30,Citation32,Citation33,Citation35,Citation41,Citation42,Citation44,Citation49,Citation53,Citation58,Citation70,Citation71] and 31 (66%) included post-op patient outcomes [Citation15,Citation17,Citation18,Citation20–23,Citation27,Citation28,Citation30–36,Citation39,Citation41,Citation42,Citation44,Citation46,Citation49,Citation51–53,Citation58,Citation59,Citation65,Citation69–71]. The most reported outcomes were mortality (22/31 articles, 71%) and post-op complications (17/31 articles, 55%) (for a list of outcomes reported, see ).
Thirty-three articles (52%) identified a funding source for the partnership activities described [Citation10,Citation15–17,Citation19–25,Citation27–30,Citation33,Citation38–40,Citation42,Citation45,Citation52,Citation53,Citation55,Citation56,Citation58,Citation60,Citation62,Citation65,Citation68,Citation70–72]. The most common funding source was an NGO (27/33 articles, 81%) (for a list of funding sources, see ). Four articles (6%) included an assessment of the attitudes and perspectives of host country participants about the partnership [Citation11,Citation29,Citation45,Citation68] (for a list of factors assessed, see ). In two articles, no outcome measures were found (no education, follow-up, patient outcomes, or funding source) [Citation48,Citation63].
Discussion
While the articles included in this review do not cover all international partnerships in pediatric surgery that have taken place in SSA, they represent a snapshot of partnership work in the past decade. An essential consideration in evaluating global health partnerships is whether they include education of local health-care providers. The Lancet Global Surgery 2030 report recommended that all international surgery partnerships contain a training component outside of the acute crisis setting [Citation1]. Just over half of the articles in this review included education of host country providers. This is an improvement compared to a previous systematic review done on this subject in which no articles contained data on training of host country providers outside of four programs that sent surgeons from SSA to train in the US [Citation8]. However, much work needs to be done to ensure that all partnerships contain education in the future.
Of note, only half of the articles that did include education provided measures of educational outcomes. The most frequently reported outcome, reported in only seven of the articles, was the ability of host country surgeons and trainees to perform surgeries independently [Citation10,Citation12,Citation15,Citation25,Citation31,Citation33,Citation59]. To ensure that training during international partnerships is effective, partnerships need to design and report educational outcome measures. The ability of host country providers to operate independently is a good benchmark for all partnerships to strive for.
Short-term surgical trips were the most common category of partnerships encountered. This is not surprising, as short-term trips have dominated global surgery efforts for years [Citation3,Citation7]. There are many potential pitfalls of the short-term surgical trip. They are often not sustainable or have limited impact on the overall burden of disease for a community [Citation7], may disrupt and overburden the local healthcare system [Citation3], and may leave patients and their local physicians without adequate provisions for follow-up care [Citation3,Citation73]. To ensure sustainability, short-term trips should include a training component. However, only half of the short-term surgical trips in this review included education [Citation12,Citation25,Citation26,Citation28,Citation29,Citation31,Citation33–36,Citation38,Citation42,Citation44,Citation45]. Short-term trips are more sustainable when they recur in the same location more than once as part of a long-term partnership [Citation6], and more than two-thirds (71%) of the short-term surgical trips in this review did recur. When planning future short-term surgical trips, aiming for a long-term investment in one location is vital.
Post-op follow-up is often an essential component of surgical care and is of particular importance in short-term trips, when surgeons may depart soon after operations are performed. Less than half of the short-term surgical trips included post-op follow-up care for patients when applicable [Citation12,Citation18,Citation21,Citation23,Citation30,Citation32,Citation33,Citation35,Citation41,Citation42,Citation44,Citation49]. Among all categories, less than half (45%) of articles reported post-op follow-up when applicable. This represents a serious shortcoming that future pediatric surgery partnerships in SSA must address.
One strategy that could aid in the provision of follow-up after surgical partnerships is the use of telemedicine. Only three articles in the review utilized this platform. The two used telemedicine to jointly pre-select patients with host-country partners for surgery on short-term trips [Citation12,Citation43], and one of these also used telemedicine for follow-up after the trips [Citation12]. This is a cost-effective way to ensure adequate follow-up care and to build mutual partnering relationships with providers in SSA. The third article utilized telemedicine as a way for general surgeons to consult pediatric specialist surgeons in a partner country without the need for either partner to travel [Citation69]. This could be an effective way for surgeons in partner countries to support pediatric surgery development in SSA at minimal cost and while maintaining the autonomy of the host country provider.
Closely related to follow-up care are post-op surgical outcomes. Data suggests that operations performed through humanitarian platforms may have higher complication rates and poorer clinical outcomes than those performed in high-income-country (HIC) hospitals [Citation73]. There can also be a lack of accountability for poor outcomes when visiting surgeons leave the host country [Citation3,Citation37]. For these reasons, it is imperative that all international partnerships report patient outcomes when applicable. Of the 48 articles in which patient outcomes were applicable (partnership activities involved operating on host country patients), the majority (66%) reported them. However, this still leaves a large proportion of partnerships that did not report patient outcomes, highlighting another area requiring improvement in future partnerships. In addition to mortality and complications, guidelines suggest that quality-of-life outcomes should also be reported for global surgery initiatives [Citation6]. Only seven articles included quality of life outcomes (functionality [Citation23,Citation27,Citation35,Citation44,Citation69], ability to attend school or work [Citation70], feelings of shame and acceptability in society [Citation71], and being teased by others [Citation70]).
An important consideration when designing truly sustainable surgical initiatives is the availability of the necessary peri- and post-op staff including nurses, anesthetists, technicians, and so on. Only a minority of articles (17%) described surgical initiatives that included specific training of non-surgeon peri-op providers [Citation10,Citation11,Citation15,Citation16,Citation22,Citation26,Citation28,Citation31,Citation33,Citation36,Citation38,Citation42,Citation58–60,Citation62,Citation64], indicating that this may be an important focus of future capacity-building efforts. In addition, many surgeries may also require intensive care unit (ICU)-level care post-op. Two articles highlighted the challenges of caring for patients postoperatively with inadequate ICU infrastructure. In one, a local, general pediatrician in Ghana was left to manage open-heart surgery patients post-op who required ICU-level specialist care that both he and the hospital were not equipped to provide [Citation37]. In another, a visiting neurosurgeon in Kenya found that the surgery he provided was not beneficial if patients could not receive the necessary level of peri-op care. He subsequently spent most of his time training local nurses and physicians in neuro-ICU patient management [Citation38]. Ensuring that local hospitals have adequate peri-op staff and post-op infrastructure for the surgeries performed is an essential consideration for international surgery partnerships.
Considering the length of time it takes to become a fully certified pediatric surgeon, one way to increase pediatric surgery capacity in SSA is to train general surgeons in high-yield pediatric surgery techniques. This may be the most efficient way to ensure more equitable access to pediatric surgery for patients in the region. Only 5 articles in the review included the training of general surgeons in pediatric surgery procedures [Citation31,Citation33,Citation34,Citation60,Citation64]. Future partnerships should consider incorporating this strategy into their plans.
When assessing the efficacy of international pediatric surgery partnerships, it is important to consider the attitudes and perspectives of host country participants. However, only four articles included such an assessment [Citation11,Citation29,Citation45,Citation68]. In one, Canadian and Kenyan pediatric surgery fellows who participated in an exchange program filled out detailed surveys after the program. The results revealed that Kenyan fellows experienced more challenges in the exchange program and rated the exchange lower in every category compared to the Canadian fellows. Lower ratings were attributable to the fact that it was more difficult for Kenyan fellows to get full licensure to perform surgery in Canada, so some had to only observe surgeries for the whole program. All Canadian fellows were able to participate fully in surgeries in Kenya [Citation68].
A survey of Ethiopian surgeons after a short-term surgical trip showed that they felt overseas missions should enter into an agreement with the Federal Ministry of Health before arriving and should limit the number of people on visiting teams so that more Ethiopian providers could participate. They also commented that visiting surgeons should plan to operate on many patients with a similar diagnosis so that Ethiopian surgeons could gain the repetition needed to master a single type of procedure [Citation29].
The insights gained from these assessments of local participants’ perspectives show critical needs for improvement in future partnership activities. Assessing the viewpoints of SSA partners could help identify blind spots in the partnership by pointing out problems and different perspectives between the visitors and hosts. Addressing these areas could lessen any unintended harm from the visiting surgical team, improve outcomes, and secondarily strengthen the partnership. Thus, moving forward, every partnership should evaluate the perspectives of their SSA partners.
Finally, to promote maximal transparency, publications on international pediatric surgery partnerships should disclose the funding source(s) for the partnership and/or how funding was raised. Just over half (52%) of the articles in this review identified a funding source, but more partnerships need to do so in the future.
The limitations of this study include that we only evaluated two databases and did not conduct a search of the grey literature. Directions for future study include investigating initiatives to train anesthesia and peri-op nursing providers in SSA, as well as specific initiatives to train pediatricians in SSA to manage peri-op care, and reviewing the literature on pediatric surgery partnerships in southeast Asia, another region with great unmet need for surgical care [Citation1].
Conclusions
In conclusion, international partnerships can play an important role in helping to scale up the critically low pediatric surgery capacity in SSA. We recommend that all partnerships include an element of education for host country surgeons and that they measure and report educational outcomes. Education should also extend to peri-op staff and general surgeons. All partnerships should ensure adequate follow-up care for patients after visiting surgeons depart, and all should report post-op patient outcomes. The perspectives of participants from SSA should be regularly evaluated. Publications about partnership activities should disclose funding sources. Currently, too few partnerships are meeting these recommendations, pointing to the need for improvement when planning future initiatives.
All the points we have raised stress the need to form true partnerships with leaders from the SSA sites. They must be involved and have the leading voice at every level of the partnership, from building the necessary infrastructure, training appropriate personnel, selecting the appropriate patients and procedures, ensuring needed follow-up, and assessing outcomes.
Paper context
Only two prior review articles have been published on this topic to date. One was a systematic review of articles from 1990 to 2012. Another was a general review about pediatric surgery in LMICs which did not report any methods. This study focuses on more recent literature to provide an updated review following PRISMA guidelines. It provides a more detailed categorization of pediatric surgery partnerships and previously unreported data about education, post-operative follow-up, outcomes, and funding sources.
Acknowledgments
We would like to thank Dr. Tina Slusher (University of Minnesota) and Dr. Burton Lee (University of Pittsburgh) for their edits and guidance. We would also like to thank Dr. Mary Carter (University of Louisville) for her help in inspiring this project and for her excellent mentorship.
Disclosure statement
There was no funding source for this paper, and we have no conflicts of interest to disclose.
Additional information
Funding
Notes on contributors
Charles Shofner
AW performed the initial database searches and data extraction. AW and CS evaluated all articles to determine eligibility for inclusion. BH resolved any conflicts over article inclusion. AW drafted the text of the manuscript and all tables and figures. CS and BH critically revised the manuscript. All three authors approved of the final version and are accountable for all aspects of the work.
References
- Meara JG, Leather AJM, Hagander L, et al. Global surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386:569–14.
- Anthony D, You D, Hug L, et al. Generation 2030 Africa 2.0 UNICEF. 2017.
- Butler MW. Developing pediatric surgery in low- and middle-income countries: an evaluation of contemporary education and care delivery models. Semin Pediatr Surg. 2016;25:43–50.
- Citron I, Chokotho L, Lavy C. Prioritisation of surgery in the national health strategic plans of Africa: a systematic review. Lancet. 2015;385:S53.
- Greenberg SLM, Ng-Kamstra JS, Ameh EA, et al. An investment in knowledge: research in global pediatric surgery for the 21st century. Semin Pediatr Surg. 2016;25:51–60.
- Grimes CE, Maraka J, Kingsnorth AN, et al. Guidelines for surgeons on establishing projects in low-income countries. World J Surg. 2013;37:1203–1207.
- Martiniuk AL, Manouchehrian M, Negin JA, et al. Brain gains: a literature review of medical missions to low and middle-income countries. BMC Health Serv Res. 2012;12:134.
- Ekenze SO, Onumaegbu OO, Nwankwo OE. The current status of international partnerships for child surgery in sub-Saharan Africa. Int Surg. 2014;99:616–622.
- Zellers JM, Batiste A, Harper ML, et al. Africana Collections 2018 [cited 2021 Mar 30]. Available from: https://www.loc.gov/rr/amed/guide/afr-countrylist.html.
- Qureshi MM, Piquer J, Young PH. Mobile endoscopy: a treatment and training model for childhood hydrocephalus. World Neurosurg. 2013;79:S24.e1–4.
- Kantar RS, Ramly EP, Almas F, et al. Sustainable cleft care through education: the first simulation-based comprehensive workshop in the Middle East and North Africa region. Cleft Palate-Craniofacial J. 2018; 56: 735–743.
- Ambroise B, Benateau H, Prevost R, et al. The contribution of telemedicine to humanitarian surgery. J Craniomaxillofac Surg. 2018;46:1368–1372.
- Isaacson G, Buchinsky FJ. More than a surgical mission-pediatric otolaryngology in Ethiopia. Int J Pediatr Otorhinolaryngol. 2011;75:1018–1019.
- O’Neill JA. A model for humanitarian outreach in today’s world. J Pediatr Surg. 2018;53:21–24.
- Nunes MAS, Magalhaes MP, Uva MS, et al. A multinational and multidisciplinary approach to treat CHD in paediatric age in Angola: initial experience of a medical-surgical centre for children with heart disease in Angola. Cardiol Young. 2017;27:1755–1763.
- Noormahomed EV, Mocumbi AO, Ismail M, et al. The medical education partnership initiative effect on increasing health professions education and research capacity in Mozambique. Ann Glob Health. 2018;84:47–57.
- Shidhika FF, Hugo-Hamman CT, Lawrenson JB, et al. The Namibian children’s heart project: a south-south partnership to provide cardiac care. Cardiol Young. 2019;29:206–213.
- Ferratini M, Marianeschi S, Santoro F, et al. Valvulopathies in sub-Saharan African children: patterns, humanitarian interventions and cardiac surgical problems. Int J Cardiol. 2013;165:237–241.
- Kamdem F, Kedy Koum D, Hamadou B, et al. Clinical, echocardiographic, and therapeutic aspects of congenital heart diseases of children at Douala general hospital: a cross-sectional study in sub-Saharan Africa. Congenit Heart Dis. 2018;13:113–117.
- Gouton M, Lucet V, Bical O, et al. Late management of truncus arteriosus: 20 years of humanitarian experience. Cardiol Young. 2018;28:302–308.
- Veyssiere A, Ambroise B, Traore H, et al. Management of large maxillomandibular osteofibrous dysplasia as part of a humanitarian mission. J Oral Maxillofacial Surg. 2017;75:436.e1–.e10.
- Rusingiza EK, El-Khatib Z, Hedt-Gauthier B, et al. Outcomes for patients with rheumatic heart disease after cardiac surgery followed at rural district hospitals in Rwanda. Heart. 2018;104:1707–1713.
- Baldan M, Gosselin RA, Osman Z, et al. Chronic osteomyelitis management in austere environments: the International Committee of the Red Cross experience. Trop Med Int Health. 2014;19:832–837.
- Guifo ML, Essiene A, Ngo Nsoga M, et al. Surgical management of chronic wounds in a buruli ulcer endemic area in Central Africa. World J Surg. 2016;40:1041–1046.
- Yankah C, Fynn-Thompson F, Antunes M, et al. Cardiac surgery capacity in sub-saharan Africa: quo vadis? Thorac Cardiovasc Surg. 2014;62:393–401.
- Tahmeedullah, Abenavoli FM, Altacera M, et al. Humanitarian cleft mission to Central Africa - experience and suggestions. J Postgrad Med Inst. 2011;25:373–375.
- de Buys Roessingh AS, Dolci M, Zbinden-Trichet C, et al. Success and failure for children born with facial clefts in Africa: a 15-year follow-up. World J Surg. 2012;36:1963–1969.
- Rodgers W, Lloyd T, Mizen K, et al. Microvascular reconstruction of facial defects in settings where resources are limited. Br J Oral Maxillofacial Surg. 2016;54:51–56.
- Tefera E, Nega B, Yadeta D, et al. Humanitarian cardiology and cardiac surgery in sub-Saharan Africa: can we reshape the model? World J Pediatr Congenit Heart Surg. 2016;7:727–731.
- Isaacson G, Melaku A. Results of pediatric tympanoplasty on short-term surgical missions. Laryngoscope. 2016;126:1464–1469.
- Calisti A, Belay K, Mazzoni G, et al. Promoting major pediatric surgical care in a low-income country: a 4-year experience in Eritrea. World J Surg. 2011;35:760–766.
- Nwiloh J, Edaigbini S, Danbauchi S, et al. Cardiac surgical experience in northern Nigeria. Cardiovasc J Afr. 2012;23:432–434.
- Coburger J, Leng LZ, Rubin DG, et al. Multi-institutional neurosurgical training initiative at a tertiary referral center in Mwanza, Tanzania: where we are after 2 years. World Neurosurg. 2014;82:e1–8.
- Wilson DA, Garrett MP, Wait SD, et al. Expanding neurosurgical care in northwest Tanzania: the early experience of an initiative to teach neurosurgery at Bugando Medical centre. World Neurosurg. 2012;77:32–38.
- Cousins GR, Obolensky L, McAllen C, et al. The Kenya orthopaedic project: surgical outcomes of a travelling multidisciplinary team. J Bone Joint Surg Br Vol. 2012;94:1591–1594.
- Edwards D, Heard J, Latenser BA, et al. Burn injuries in eastern Zambia: impact of multidisciplinary teaching teams. J Burn Care Res. 2011;32:31–38.
- Nguah SB. Ethical aspects of arranging local medical collaboration and care. J Clin Ethics. 2014;25:314–316.
- Spanu F, Piquer J, Panciani PP, et al. Practical challenges and perspectives for the development of neurosurgery in a peripheral east African hospital during a one-volunteer midterm mission. World Neurosurg. 2018;111:326–334.
- Thiagarajan RI, Scheurer MA, Salvin JW. Great need, scarce resources, and choice: reflections on ethical issues following a medical mission. J Clin Ethics. 2014;25:311–313.
- Boolkah S. Children at heart. Nurs Stand. 2010;24:25.
- Grimaldi A, Ammirati E, Karam N, et al. Cardiac surgery for patients with heart failure due to structural heart disease in Uganda: access to surgery and outcomes. Cardiovasc J Afr. 2014;25:204–211.
- Tefera E, Qureshi SA, Bermudez-Canete R. Successful training of self-sufficient interventional paediatric cardiology team in a sub-Saharan setting: a multicentre collaborative model. Cardiol Young. 2015;25:874–878.
- Bénateau H, Traoré H, Chatellier A, et al. Child care management in maxillofacial humanitarian mission. Rev Stomatol Chir Maxillofac Chir Orale. 2015;116:250–260.
- Faldini C, Prosperi L, Traina F, et al. Surgical treatment of neglected congenital idiopathic talipes equinovarus after walking age in Eritrea: an Italo-Eritrean cooperation. Musculoskelet Surg. 2016;100:133–137.
- Hayton RA, Donley DK, Fekadu A, et al. Surgical volunteerism as a collaborative teaching activity can benefit surgical residents in low-middle income countries. Int J Surg. 2017;48:34–37.
- Pearce EC, Mainthia R, Freeman KL, et al. The usefulness of a yearly head and neck surgery trip to rural Kenya. Otolaryngol Head Neck Surg. 2013;149:727–732.
- Nwafor IA, Chinawa JM, Adiele DK, et al. Management of complex CHD at the national cardiothoracic center of excellence, University of Nigeria teaching hospital, Enugu: the role of foreign cardiac missions in 3.5 years. Cardiol Young. 2017;27:1174–1179.
- Small BM, Hurley J, Placidi C. How do we choose? J Clin Ethics. 2014;25:308–310.
- Claros P, Sobolewska AZ, Claros A. Bilateral cleft lip and cleft nose. A rare association: our experience. Revue de Laryngologie Otologie Rhinologie. 2017;138:57–61.
- Hasanin A, Sherif N, Elbarbary M, et al. Providing medical care in unfamiliar settings; experience of an Egyptian campaign in Uganda. Pan Afr Med J. 2014;17:111.
- Hamze H, Mengiste A, Carter J. The impact and cost-effectiveness of the Amref health Africa-Smile Train cleft lip and palate surgical repair programme in eastern and central Africa. Pan Afr Med J. 2017;28:35.
- Poenaru D. Getting the job done: analysis of the impact and effectiveness of the SmileTrain program in alleviating the global burden of cleft disease. World J Surg. 2013;37:1562–1570.
- Mirabel M, Lachaud M, Offredo L, et al. Cardiac surgery in low-income settings: 10 years of experience from two countries. Arch Cardiovasc Dis. 2017;110:82–90.
- Pollock JD, Love TP, Steffes BC, et al. Is it possible to train surgeons for rural Africa? A report of a successful international program. World J Surg. 2011;35:493–499.
- Dale EL, Mueller MA, Wang L, et al. Epidemiology of operative burns at Kijabe Hospital from 2006 to 2010: pilot study of a web-based tool for creation of the Kenya burn repository. Burns. 2013;39:788–795.
- Rode H, Kyambi J, Lakhoo K. The history of the formation of the pan African paediatric surgical association (PAPSA). Pediatr Surg Int. 2018;34:499–504.
- Girma B, Bitew A, Kiros N, et al. High-density otologic camps in regions of sparse expertise. Ann Otol Rhinol Laryngol. 2018;127:327–330.
- Blair GK, Duffy D, Birabwa-Male D, et al. Pediatric surgical camps as one model of global surgical partnership: a way forward. J Pediatr Surg. 2014;49:786–790.
- Fuller AT, Haglund MM, Lim S, et al. Pediatric neurosurgical outcomes following a neurosurgery health system intervention at Mulago national referral hospital in Uganda. World Neurosurg. 2016;95:309–314.
- Amado V, Martins DB, Karan A, et al. Global general pediatric surgery partnership: the UCLA-Mozambique experience. J Pediatr Surg. 2017;52:1528–1533.
- Kinsley RH, Edwin F, Entsua-Mensah K. The Paediatric cardiac centre for Africa—proceedings of the March 2012 symposium. 2013;World J Pediatr Congenit Heart Surg. 4:182–185.
- Haglund MM, Warf B, Fuller A, et al. Past, present, and future of neurosurgery in Uganda. Neurosurgery. 2017;80:656–661.
- Bickler SW. Out of Africa: insights from a prospective pediatric surgery database. J Pediatr Surg. 2017. Epub 2017/11/28. DOI: 10.1016/j.jpedsurg.2017.10.009.
- Lakhoo K, Msuya D. Global health: a lasting partnership in paediatric surgery. 2015;Afr J Paediatr Surg. 12:114–118.
- Ford K, Poenaru D, Moulot O, et al. Gastroschisis: bellwether for neonatal surgery capacity in low resource settings? J Pediatr Surg. 2016;51:1262–1267.
- Jacobs JP, Tchervenkov CI, Stellin G, et al. History of the world society for pediatric and congenital heart surgery: the first decade. World J Pediatr Congenit Heart Surg. 2018;9:392–406.
- Tchervenkov CI, Stellin G, Kurosawa H, et al. The world society for pediatric and congenital heart surgery: its mission and history. Semin Thorac Cardiovasc Surg Pediatr Card Surg Ann. 2009; 12: 3–7.
- Baird R, Poenaru D, Ganey M, et al. Partnership in fellowship: comparative analysis of pediatric surgical training and evaluation of a fellow exchange between Canada and Kenya. J Pediatr Surg. 2016;51:1704–1710.
- Bertani A, Launay F, Candoni P, et al. Teleconsultation in paediatric orthopaedics in Djibouti: evaluation of response performance. Orthop Traumatol Surg Res. 2012;98:803–807.
- White MC, Randall K, Avara E, et al. Clinical outcome, social impact and patient expectation: a purposive sampling pilot evaluation of patients in Benin seven years after surgery. World J Surg. 2018;42:1254–1261.
- White M, Alcorn D, Randall K, et al. Evaluation of patient satisfaction, impact and disability-free survival after a surgical mission in Madagascar: a pilot survey. World J Surg. 2017;41:364–369.
- Barbier O, Pasquier P, Racle M, et al. Dynamic insights on surgical activity in a new modern warfare: the French role 2 in Bangui, Central African Republic. Mil Med. 2017;182:e1756–e61.
- Shrime MG, Sleemi A, Ravilla TD. Charitable platforms in global surgery: a systematic review of their effectiveness, cost-effectiveness, sustainability, and role training. World J Surg. 2015;39:10–20.
Appendix:
additional tables
Table A1: Length of time of short-term surgical trips and the number of articles in which each occurs. Number of short-term trips that recur in the same location and the periodicity with which they recur.
Table A2: Educational outcomes reported and the number of articles in which each is reported. (SSA = sub-Saharan Africa).
Table A3: Non-surgeon health-care providers trained during partnership activities and the number of articles in which each is mentioned.
Table A4: Post-operative outcomes reported and the number of articles in which each was reported (DALY = disability adjusted life years, ICU = intensive care unit).
Table A5: Sources of funding identified for partnership activities and the number of articles in which each is reported.
Table A6: The attitudes and perceptions of host country participants about the partnership activities and the number of articles in which each measure was reported.
