
ABSTRACT
Background
Young migrants face multiple challenges that can affect their mental, sexual and reproductive health.
Objective
To assess the prevalence of self-reported poor mental health and its associated demographic, post-migration and sexual risk behaviour factors among young migrants (aged 15–25) in Sweden.
Methods
Data were drawn from a cross-sectional survey conducted with migrants aged 15–65 years old in Sweden between December 2018 and November 2019 (n = 6449). Among these, 990 participants aged 15–25 were eligible for the study. Mental health was measured using the Refugee Health Screener-13. Missing data indicator analysis and multivariable logistic regression models were conducted to estimate the association between mental health, sexual risk behaviour, demographic and migration-related variables.
Results
Of the 990 participants, 59% reported poor mental health. Participants reporting poor mental health were more likely to be female (AOR:1.63, 95% CI:1.18–2.25), to have lived in Sweden more than three years (AOR:2.16, 95% CI:1.17–3.97), to engage in any sexual risk behaviour (AOR:1.99, 95% CI:1.25–3.17), and to live alone (AOR:1.95, 95% CI:1.25–3.03) or with friends they already knew (AOR:1.60, 95% CI:1.37–4.91). People arriving from the Americas (AOR:0.54, 95% CI:0.33–0.88), Asia (AOR:0.44, 95% CI:0.22–0.86), Europe (AOR:0.30, 95% CI:0.14–0.61) and Africa (AOR 0.37, 95% CI: 0.23–0.60) had lower odds of poor mental health than those arriving from Syria.
Conclusion
The prevalence of poor mental health among young migrants in Sweden was high, with specific subgroups (women, asylum seekers, people arriving from Syria, and those residing longer in Sweden) being particularly vulnerable. Our results indicate the interconnectedness between poor mental health and sexual risk behaviour in this population. Thus, policies targeting young migrants should ensure that healthcare services screen for both poor sexual and mental health at the same time.
Responsible Editor Stig Wall
Introduction
The World Health Organization (WHO) defines mental health as the state of well-being in which individuals can achieve their abilities and cope with everyday stress while working and living a productive life within their community [Citation1]. Recent data found that mental disorders were among the top ten leading causes of the global burden of disease, with no evidence of the burden decreasing [Citation2]. For example, the percentage of the population affected by major depressive or anxiety disorders ranged from 9.7% to 36% during the COVID-19 pandemic [Citation3]. In addition, research has indicated a higher prevalence of mental health disorders such as post-traumatic stress and depression among certain migrant populations, such as refugees and asylum seekers [Citation4].
Mental health is determined by a combination of individual characteristics (such as genetics and educational level), community conditions (including exposure to violence and poverty, etc.), and broader structural factors (climate change, limited access to health services, etc.) [Citation5]. Among these, migration and forced displacement due to conflicts and political oppression have been recognised as the key structural factors for increasing the risk of poor mental health [Citation5,Citation6].
The global number of migrants in 2021 totalled 281 million, of which 11% were young migrants (≤25 years) [Citation7]. Migrants comprise a heterogeneous group ranging from voluntary migrants to displaced people leaving their countries due to war, poverty, or political instability [Citation8].
Migrants often face unique challenges predisposed by their migration experience, and these challenges are often shaped by contextual factors before, during, and after a person leaves their home [Citation9–12]. For example, before migration, people can experience conflict-related trauma or feel a profound uncertainty about the safety of the journey. These experiences can lead to post-traumatic stress disorder (PTSD) and anxiety [Citation10,Citation11,Citation13,Citation14]. During migration, migrants, particularly vulnerable populations like women, children, young people, and LGBTQ+ individuals, can risk exploitation, discrimination, physical and sexual violence, and human trafficking [Citation15–19]. After settling in the host country, factors such as cultural differences, language barriers, discrimination, uncertain legal status (such as lack of work or residence permit), lack of social networks, and limited access to health care have been shown to impair migrants´ mental health [Citation9–11,Citation14,Citation20–24]. In particular, time living in the host country has been identified as a contributing factor to the increasing substance and alcohol abuse incidence among migrants living in Sweden [Citation25]. Poor living conditions (e.g. living in refugee housing or being separated from family) were also associated with higher levels of psychological distress in a study conducted among refugees in Germany [Citation26].
Poor sexual health, including sexual risk behaviours, is also associated with mental health and migration [Citation15,Citation16]. The interrelationship between sexual risk behaviour and mental health is complex, as one can catalyse the other [Citation27,Citation28]. For example, sexual risk behaviours in the form of unprotected sex with strangers can generate anxiety due to fears of contracting a sexually transmitted infection (STI) [Citation29]. On the other hand, mental disorders and the medication used to treat them can increase sexual risk behaviours or impair sexual desire and people´s abilities to enjoy pleasurable sexual relations [Citation28].
The challenges faced by many migrants in their host countries could influence their sexual health, including increased sexual risk behaviour. For example, engaging in sexual risk behaviours has been reported as a coping strategy to deal with feelings of loneliness and financial challenges or as a pathway to feel more integrated into a new society with more tolerant norms towards sex and sexuality [Citation15,Citation21,Citation30–36]. Consequently, recognising and understanding the mental health challenges among young migrant populations is essential for improving their sexual and reproductive health (SRH) and vice versa [Citation10,Citation14,Citation37].
Sweden is a multicultural society where approximately 19.7% of Swedish residents are foreign-born [Citation38]. Previous studies have shown that first- and second-generation young migrants have an increased risk for poor mental health compared to their Swedish-born peers [Citation22,Citation24,Citation39]. For instance, young refugees diagnosed with poor mental health have a higher risk of PTSD and reported lower medication uptake than their Swedish-born counterparts [Citation24,Citation40]. Although previous studies in Sweden have provided key data on the demographic risk factors (e.g. age, age at migration, country of origin, education, etc.) for poor mental health among this vulnerable population, few studies have assessed if sexual risk behaviours, post-migration conditions (living arrangements, years living in Sweden, reason for migration and residency status) increase the odds of poor mental health among young migrants in Sweden [Citation22,Citation24,Citation40]. Thus, our study aimed to fill this research gap by mapping the prevalence of self-reported poor mental health and its associated demographic, post-migration, and sexual risk behaviours factors among young migrants (aged 15–25) in Sweden. Our findings will help inform policies to design comprehensive health services for young migrants, including mental and sexual health screening and treatment in Sweden and elsewhere.
Methods
Study population
The data used for this paper comes from a larger project that aimed to map the sexual, reproductive, and mental health of migrants aged 15–65 years living in Stockholm, Sweden [Citation31,Citation41]. A migrant was defined as ‘any person changing their country of residence who has moved from their usual place of residence, either in-country or across the border, for various reasons’ [Citation8].
Sample and data collection
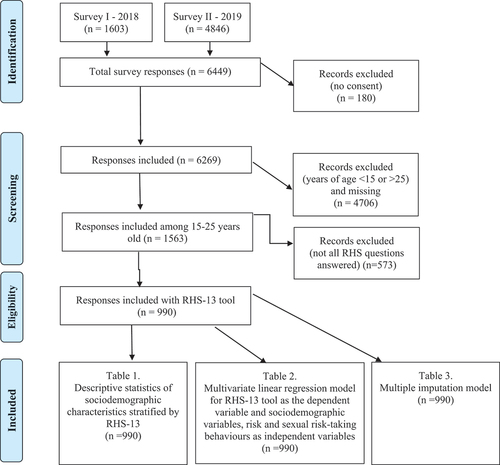
Data for the project above were collected between December 2018 and November 2019 using an anonymous, self-administered cross-sectional survey. The target population was migrants attending schools offering Swedish language training for foreigners and upper-middle secondary schools in Stockholm. The data was collected in collaboration with two non-governmental organisations (NGOs), The World Values Survey (WVS) and Invandraindex [Citation42,Citation43]. Both NGOs collect health, demographic, and migration-related data from thousands of migrants in Sweden. In total, 6449 people aged 15–65 answered the survey. We excluded 180 people who did not consent to participate in the survey. For our paper, we selected only those aged 15–25 years, thus excluding 4706 people and 573 who did not complete all the questions for Refugee Health Screener-13 (RHS-13), which is the main tool for the outcome of this paper (see full definition and description below). Thus, the final sample for analysis was 990 participants (see Supplementary file, ).
Figure 1. Flowchart of the number of participants, responses, and tables.
Data collection
The survey was available in Arabic, English, Farsi, Tigrinya, Spanish, Swedish, and Somali. It was tested in 2018 for language correctness, translated, and back-translated for accuracy. The survey was administered in the teacher’s classroom, where the participants answered it using a personal or school-provided digital device. A research assistant was present to clarify any questions. The participants were given approximately 60 minutes to complete the survey. Additional details on participant recruitment and the study sample are described elsewhere [Citation31,Citation41].
Variables
Dependent variable
The main outcome variable, self-reported mental health, was measured using the RHS-13 [Citation44]. The RHS-13 is a self-rating screening instrument used to identify people with high risk for mental health problems. It has been used and validated in Sweden and elsewhere [Citation45,Citation46]. The RHS-13 has good internal validity (Cronbach’s α = 0.95), sensitivity, and specificity when compared to other specific mental health diagnostic tools (PTSD: sensitivity 0.81/specificity 0.87, anxiety: 0.94/0.86, and depression: 0.95/0.89) [Citation44]. The RHS-13 consists of 13 questions describing poor mental health signs and symptoms rated using a Likert scale ranging from 0 = not at all to 4 = extreme. The overall scale ranges from 0 to a maximum score of 52. As suggested by the literature, a cut-off of 11 points or above on the scale was used to define poor mental health [Citation44].
Independent variables
Sexual risk behaviour
Past-year sexual risk behaviour (yes, no, haven´t had sex) was assessed by combining the positive responses to any of the following three questions: 1) had sex without a condom; 2) had sex in exchange for gifts/money; or 3) had sex with a casual partner under the influence of drugs. We combined these variables to facilitate analysis since it has been reported that sexual risk behaviours among young people usually cluster together [Citation47].
Demographic variables
We measured demographic variables previously shown to influence mental health [Citation24,Citation45,Citation48]: Sex (male, female); Age (years); Education measured as years in school (<3 years, 4–6 years, 7–9 years, 10 years or longer); Religion (Christianity, Islam, no religion/other); and Country of birth, grouped into seven categories based on the main settings that participants came from 1) Asia, 2) Americas, 3) Europe, 4) Africa, 5) the Middle East, North Africa (MENA, including Algeria, Bahrain, Egypt, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Qatar, Saudi Arabia, Palestine, Tunisia, United Arab Emirates, Yemen), 6) Syria, and 7) Afghanistan. Syria and Afghanistan were analysed separately (Syria was excluded from MENA region countries) due to the more significant number of survey participants (28% and 16%, respectively) that came as refugees and asylum seekers to Sweden in 2016 (when the study data was collected) [Citation49,Citation50]. Under Africa, we predominantly mean countries of sub-Saharan Africa.
Post-migration-related variables
We measured four variables: Main reason for coming to Sweden (asylum seeker/refugee, work/study, family reunion, other), Having a Swedish residence permit (no, yes, already an EU/EEA resident), Number of years living in Sweden (<1 year, 1, 2, 3, 4, or ≥5 years), and Current living arrangements (alone, married or cohabiting, other family, with friends they already knew, or refugee home).
Analysis
The descriptive analysis results are reported as percentages, means, and standard deviation (SD). Pearson chi-square and t-tests were used to compare differences between groups.
Multivariable logistic regression was used to estimate adjusted odds ratios (AOR) and 95% confidence intervals (CIs) for the association between poor mental health (dichotomised RHS-13 score) and the independent variables. Independent variables were included in the model if they have been shown to be associated with poor mental health among this population [Citation10,Citation14,Citation22,Citation23,Citation39].
The independent variables had different patterns of missingness ranging from 12% for demographic variables up to 56% for the sexual risk behaviour variable. Thus, we used a missing data indicator analysis to use the entire data set containing the complete RHS-13 score by adding the option ‘missing’ to all covariables with missing data. As a sensitivity analysis, we conducted multiple imputations of all categorical variables assumed to be missing at random using chained equations (MICE) and estimates combined with Rubin’s rule [Citation51,Citation52]. Data were analysed using Stata version 17 (StataCorp, College Station, Texas).
Ethics and consent
The study was approved by the Regional Ethical Review Board in Stockholm (2017/2030–31 and 2018/1002–32) and follows the ethical principles of the Declaration of Helsinki 1964. The participants were given verbal and written information about the study and informed that participation was voluntary and anonymous and that they could quit at any time. According to Swedish law, children aged 15 years or above could participate in the study without parental/guardian consent (The Act on Ethical Review, §18-Lag (2003:460)).
Results
Sample characteristics
Among the study participants, 54% were male. The mean age was 19.6 years (SD = 2.7) (). A third (29%) had resided in Sweden for four years and a third came from Syria (27%), followed by Africa (18%). Most came as asylum seekers/refugees (53%). Of those reporting having had sex (n = 435), 35% had any sexual risk behaviours in the last year ().
Table 1. Descriptive statistics of the study cohort (15–25 years old) and bivariate analysis of independent variables by RHS-13 (n = 990).
Bivariate analysis
The prevalence of poor mental health was 59% (55% in male and 44% in female participants). Poor mental health (RHS-13 score ≥ 11) was significantly associated (p < 0.05) with education, the number of years of living in Sweden, religion, country born and raised, reasons to come to Sweden, current living arrangements, and sexual risk behaviour. There was no bivariate association with sex and residence permit in Sweden ().
Multivariable logistic regression and multiple imputation analysis
Results from the multivariable logistic regression analysis are shown in , Model 1. Factors associated with increased odds for poor mental health were: being female (OR 1.63, 95% CI:1.18–2.25), living in Sweden for more than three years (OR: 2.16, 95% CI: 1.17–3.97), engaging in any sexual risk behaviours (OR:1.99, 95% CI: 1.25–3.17) and living alone (OR:1.95, 95% CI: 1.25–3.03) or with friends they already knew (OR: 2.60, 95% CI: 1.37–4.91) compared to living with other family members. Coming from Asia, the Americas, Africa, and Europe decreased the odds of poor mental health compared to coming from Syria.
Table 2. Association between demographic, migration-related, and sexual risk behaviour variables with poor mental health (RHS-13 ≥ 11); adjusted odds ratios (AOR) and 95% confidence intervals (CI) shown (n = 990).
The multiple imputation analysis (, Model 2) showed that all variables significant in Model 1 had the same direction of association (risk or protective factor) and similar magnitude (AOR) and confidence intervals in the imputed analysis.
Discussion
Our main findings showed that six out of ten young migrants screened positive for poor mental health. Our multivariable analysis identified several factors associated with our main outcome. We observed increased odds for poor mental health in female rather than male participants. Living in Sweden for four years compared to living for less than one year and engaging in sexual risk behaviour in the last 12 months increased the odds of reporting poor mental health. Lastly, in those currently living alone or with friends they already knew, we observe higher odds of poor mental health than those living with family. Compared to those arriving from Syria, participants reporting to come from the Americas, Africa, Europe, or Asia had lower odds of poor mental health. In the following, we will discuss these findings in depth.
The high prevalence of poor mental health in our study sample aligns with previous studies in Sweden and elsewhere [Citation22,Citation23,Citation33,Citation53–55]. Our finding can be explained by the composition of our sample, where 53.8% were refugees or asylum seekers, and 28% reported Syria as their home country. This migrant subgroup is likely to have been exposed to conflict-related trauma, as reported in other studies globally [Citation22,Citation24,Citation40,Citation56–58]. During migration, refugees and asylum seekers often face exclusion, discrimination, financial challenges, and exposure to different forms of violence (physical, sexual, etc.), which can be detrimental to migrants´ mental health [Citation22,Citation33,Citation59]. In Sweden, previous studies have found that refugees had a higher risk of schizophrenia and psychiatric hospitalisation than other migrant groups [Citation39,Citation60]. The discussion above can also explain why, when compared to Syria, arriving from other geographical regions was a protective factor against poor mental health in our study findings.
In our study, females had higher odds of poor mental health than males, in line with previous studies conducted in Europe and Sweden [Citation58,Citation61,Citation62]. One possible explanation is the gendered exposure to violence that migrants (and people in general) face. For example, one study found that female refugees were more likely to report sexual violence and family violence (from a partner or other family member) than males [Citation63]. Another possible explanation is that female migrants´ dependency on their partner for a visa or residency permit can be used by violent partners/family members to control and abuse them, as reported in an Australian study and elsewhere [Citation64–66]. The gendered nature of our findings implies that programmes aiming to improve the mental health of migrants must make efforts to prioritise women in their interventions.
Our findings also showed that the risk for poor mental health increased with the number of years living in Sweden. This is in line with another study conducted in Sweden showing a decline in the mental health of migrant populations, especially those with culturally distinct backgrounds from Sweden [Citation22]. A possible explanation for our results is that as migrants spend more time in Sweden, they are faced with new challenges associated with the acculturation process, higher exposure to discrimination, limited access to health services, delayed resolution of the migration status, family separation, and poor employment opportunities which will negatively impact their mental health [Citation13,Citation22,Citation67]. As mentioned, these challenges can have an impact on their sexual risk behaviours, causing a vicious cycle of poor health. Thus, policies aiming to improve the mental health of migrants must include long-term follow-ups and provide appropriate access to mental health services.
The living arrangements of migrants in our data were also associated with their poor mental health. Those living alone or with friends had worse mental health than those living with family members, which aligns with the findings reported in other studies [Citation9,Citation13,Citation33,Citation68]. A possible explanation for this finding is loneliness due to family separation and lack of instrumental or emotional family support, as shown in other studies [Citation10,Citation34,Citation53,Citation69].
Our analysis also showed that those engaging in sexual risk behaviours had higher odds of poor mental health than those who did not. Our findings align with studies conducted in Sweden and elsewhere [Citation16,Citation21,Citation70,Citation71]. One possible explanation is that in the acculturation process, migrants could adopt a more open stance to casual sex and other sexual risk behaviours to integrate better into the new society [Citation21]. However, these risky behaviours can be detrimental to young people´s mental health as they might worry about the negative social and health consequences of their actions, as shown in a study among youth in Sweden [Citation29]. The cross-sectional nature of our data does not allow us to establish a temporal or causal association; however, the association between poor mental health and sexual risk behaviours must be addressed in intervention aiming to tackle poor mental health among migrants. This means mental health services should consider screening for sexual risk behaviours and vice versa.
Limitations
The generalisation of our results is limited since our sample did not include migrants with lower literacy levels, undocumented, or those not attending Swedish language schools. In addition, the prevalence of poor mental health in our study might be underestimated if those excluded from the analysis due to incomplete data on the outcome variable had worse mental health than those completing the data. The cross-sectional nature of our data did not allow us to establish a causal association between the outcome and independent variables. Questions about behaviours during the last 12 months may produce recall bias.
Conclusions
Our findings highlight the prevalence of poor mental health among young migrants in Sweden, with specific subgroups, such as young women, asylum seekers, and those residing longer in Sweden, being particularly vulnerable. Furthermore, our results indicate the interconnectedness with sexual risk behaviour among young migrants. These findings have important implications for the Swedish healthcare system.
First, policies and programmes must ensure young migrants’ right to health, including the availability and accessibility of mental health services. Second, mental care services should consider policies to detect and address sexual risk behaviours in this population. Third, policies addressing the needs of vulnerable subgroups must be strengthened, considering the higher risk of poor mental health than others.
Our findings also call for longitudinal and qualitative research to better understand and address factors predisposing young migrants to poor mental and sexual health. Such research can inform the development of effective interventions and strategies.
Authors’ contributions
Substantial contributions to the conception and design of the work, acquisition, analysis, and interpretation of the data for the work; Drafting the work and revising it critically for important intellectual content; Final approval of the version to be published; Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (all authors).
Paper context
Young migrants in Sweden can face challenges impacting their mental, and sexual and reproductive health. We assessed a sample of 990 migrants aged 15–25 for mental health prevalence, including associations with sexual risk behaviours and migration-related factors. Poor mental health (prevalence = 59%) was linked to female gender, longer stay in Sweden, sexual risk behaviour, risk propensity, and lower education levels. These findings call for accessible mental health services, prevention of risk behaviour, and targeted support.
Flow diagram.doc
Download MS Word (48 KB)Author Bio.docx
Download MS Word (11.5 KB)Acknowledgments
The authors want to thank the participants who took part in this research. We also thank Veronika Tirado, PhD candidate at Karolinska Institutet, for her input and support in different phases of the project implementation. We also thank Invandrar Index, David Saleh, and Maria Stålgren for assisting with data collection.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary data
Supplemental data for this article can be accessed online at https://doi.org/10.1080/16549716.2023.2294592.
Additional information
Funding
References
- World Health Organization (WHO). Mental health - key terms and definitions [Internet]. Available from: https://www.who.int/southeastasia/health-topics/mental-health/key-terms-and-definitions-in-mental-health#health
- Global, regional and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global burden of disease study 2019. Lancet Psychiatry. 2022;9:137–11. doi: 10.1016/S2215-0366(21)00395-3
- Santomauro DF, Mantilla Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398:1700–1712. doi: 10.1016/S0140-6736(21)02143-7
- Blackmore R, Boyle JA, Fazel M, Ranasinha S, Gray KM, Fitzgerald G, et al. The prevalence of mental illness in refugees and asylum seekers: a systematic review and meta-analysis. PLOS Med. 2020;17:e1003337. doi: 10.1371/journal.pmed.1003337
- World Health Organization. The world mental health report: transforming mental health for all [Internet]. 2022. Available from: http://hdl.handle.net/10713/20295
- Percival V, Thoms OT, Oppenheim B, Rowlands D, Chisadza C, Fewer S, et al. The Lancet commission on peaceful societies through health equity and gender equality. Lancet [Internet]. 2023 Sep;402:1661–1722. Available from: https://linkinghub.elsevier.com/retrieve/pii/S014067362301348X
- UN DESA. International migrant stock 2020, population division [Internet]. [cited 2022 Jan 26]. Available from: https://www.un.org/development/desa/pd/content/international-migrant-stock
- IOM. Glossary on migration [Internet]. 2019. Available from: https://publications.iom.int/system/files/pdf/iml_34_glossary.pdf
- Fazel M, Wheeler M, Danesh J, Wheeler J, Danesh J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review. Lancet [Internet]. 2005 Apr;365:1309–1314. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673605610276
- Bogic M, Njoku A, Priebe S. Long-term mental health of war-refugees: a systematic literature review. BMC Int Health Hum Rights [Internet]. 2015 Dec 28;15:29. doi: 10.1186/s12914-015-0064-9
- Kien C, Sommer I, Faustmann A, Gibson L, Schneider M, Krczal E, et al. Prevalence of mental disorders in young refugees and asylum seekers in European countries: a systematic review. Eur Child Adolesc Psychiatry [Internet]. 2019 Oct 1;28:1295–1310. doi: 10.1007/s00787-018-1215-z
- Giacco D. Identifying the critical time points for mental health of asylum seekers and refugees in high-income countries. Epidemiol Psychiatr Sci [Internet]. 2019 Oct 2;29:e61. Available from: https://www.cambridge.org/core/product/identifier/S204579601900057X/type/journal_article
- Fazel M, Reed RV, Panter-Brick C, Stein A. Mental health of displaced and refugee children resettled in high-income countries: risk and protective factors. Lancet [Internet]. 2012 Jan 21;379:266–82. doi: 10.1016/S0140-6736(11)60051-2
- Porter M, Haslam N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons. JAMA [Internet]. 2005 Aug 3;294:602. doi: 10.1001/jama.294.5.602
- Yu B, Chen X, Elliott AL, Wang Y, Li F, Gong J. Social capital, migration stress, depression and sexual risk behaviors among rural-to-urban migrants in China: a moderated mediation modeling analysis. Anxiety, Stress Coping [Internet]. 2019 Jul 4;32:362–375. doi: 10.1080/10615806.2019.1596673
- Koegler E, Kennedy CE. A scoping review of the associations between mental health and factors related to HIV acquisition and disease progression in conflict-affected populations. Confl Health [Internet]. 2018 Dec 1;12:20. doi: 10.1186/s13031-018-0156-y
- Bendavid E, Boerma T, Akseer N, Langer A, Malembaka EB, Okiro EA, et al. The effects of armed conflict on the health of women and children. Lancet [Internet]. 2021 Feb 6;397:522–532. doi: 10.1016/S0140-6736(21)00131-8
- Kahn S, Alessi EJ. Coming out under the gun: exploring the psychological dimensions of seeking refugee status for LGBT claimants in Canada. J Refug Stud [Internet]. 2018 Mar 1 [cited 2023 Mar 9];31:22–41. Available from: https://academic.oup.com/jrs/article/31/1/22/4055916
- Nematy A, Namer Y, Razum O. Lgbtqi + refugees’ and asylum seekers’ mental health: a qualitative systematic review. Sex Res Soc Policy 2022 [Internet]. 2022 Mar 29; 1–28. doi: 10.1007/s13178-022-00705-y
- de Haas H. The determinants of international migration: conceptualising policy, origin and destination effects. IMI Work Pap Ser [Internet]. 2011;32:35. Available from: https://www.imi.ox.ac.uk/publications/wp-32-11
- Meston CM, Ahrold T. Ethnic, gender, and acculturation influences on sexual behaviors. Arch Sex Behav [Internet]. 2010 Feb 17 [cited 2023 Mar 18];39:179–189. Available from: http://search.ebscohost.com/login.aspxdirect=truedb=psyhAN=2010-01867-016site=ehost-livescope=sitemestonpsy.utexas.edu
- Honkaniemi H, Juárez SP, Katikireddi SV, Rostila M. Psychological distress by age at migration and duration of residence in Sweden. Soc Sci Med [Internet]. 2020 Apr;250:112869. doi: 10.1016/j.socscimed.2020.112869
- Berg L, Gustafsson NK, Honkaniemi H, Juárez SP. Health risk behaviours among migrants by duration of residence: protocol for a systematic review and meta-analysis. BMJ Open. 2020;10: doi: 10.1136/bmjopen-2020-038388
- Björkenstam E, Helgesson M, Norredam M, Sijbrandij M, de Montgomery CJ, Mittendorfer-Rutz E. Common mental disorders among young refugees in Sweden: the role of education and duration of residency. J Affect Disord [Internet]. 2020 Apr;266:563–571. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0165032719330605
- Harris S, Dykxhoorn J, Hollander ACC, Dalman C, Kirkbride JB, Alegria M. Substance use disorders in refugee and migrant groups in Sweden: a nationwide cohort study of 1.2 million people. PLOS Med [Internet]. 2019;16:e1002944. doi: 10.1371/journal.pmed.1002944
- W L, F LM, S J, von S C. Living conditions and the mental health and well-being of refugees: evidence from a large-scale German survey. J Immigr Minor Heal [Internet]. 2020;22:903–913. doi: 10.1007/s10903-019-00968-5.pdf
- Mialon A, Berchtold A, Michaud PA, Gmel G, Suris JC. Sexual dysfunctions among young men: prevalence and associated factors. J Adolesc Heal. 2012;51:25–31. doi: 10.1016/j.jadohealth.2012.01.008
- Montejo AL, Montejo L, Baldwin DS. The impact of severe mental disorders and psychotropic medications on sexual health and its implications for clinical management. World Psychiatry. 2018;17:3–11. doi: 10.1002/wps.20509
- Nielsen A, De Costa A, Gemzell-Danielsson K, Boman J, Salazar M. “Repeat testing without having ‘the talk’ is not meaningful”—healthcare providers’ perceptions on finding a balance between chlamydia trachomatis testing and primary prevention strategies. A qualitative study in Stockholm, Sweden. BMJ Open. 2020;10:e034179. doi: 10.1136/bmjopen-2019-034179
- Kane JC, Elafros MA, Murray SM, Mitchell EMH, Augustinavicius JL, Causevic S, et al. A scoping review of health-related stigma outcomes for high-burden diseases in low- and middle-income countries. BMC Med [Internet]. 2019 Dec 15;17:17. doi:10.1186/s12916-019-1250-8
- Causevic S, Salazar M, Orsini N, Kågesten A, Ekström AM. Sexual risk-taking behaviors among young migrant population in Sweden. BMC Public Health [Internet]. 22: 2022 Dec 30; 625. doi: 10.1186/s12889-022-12996-2
- Khan N, Cailhol J. Are migration routes disease transmission routes? Understanding hepatitis and HIV transmission amongst undocumented Pakistani migrants and asylum seekers in a Parisian suburb. Anthropol Med [Internet]. 2020 Oct 1 ;27(4):395–411. doi: 10.1080/13648470.2019.1695170
- Mangrio E, Sjöström K, Grahn M, Zdravkovic S. Risk for mental illness and family composition after migration to Sweden Cheung JCS, editor. PLoS One [Internet]. 2021 May 7;16:e0251254. doi: 10.1371/journal.pone.0251254
- Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. 2017 Nov 1;152:157–171. doi: 10.1016/j.puhe.2017.07.035
- Paat YF, Torres LR, Morales DX, Srinivasan SM, Sanchez S. Sensation seeking and impulsivity as predictors of high-risk sexual behaviours among international travellers. Curr Issues Tour [Internet]. 2020 Nov 1;23:2716–2732. doi: 10.1080/13683500.2019.1666808
- Cobb-Clark DA, Dahmann SC, Kettlewell N. Depression, risk preferences and risk-taking behavior. 2019 [cited 2022 Jan 19]. Available from: https://docs.iza.org/dp12285.pdf
- Hollander AC, Mackay E, Sjöqvist H, Kirkbride JB, Bäärnhielm S, Dalman C. Psychiatric care use among migrants to Sweden compared with Swedish-born residents: a longitudinal cohort study of 5 150 753 people. BMJ Glob Heal [Internet]. 2020 Sep 24;5: e002471. Available from: 10.1136/bmjgh-2020-002471
- Statistikmyndigheten SCB. 2022 [cited 2023 Mar 12]. Utrikes födda i Sverige. Available from: https://www.scb.se/hitta-statistik/sverige-i-siffror/manniskorna-i-sverige/utrikes-fodda-i-sverige/
- Hollander AC, Dal H, Lewis G, Magnusson C, Kirkbride JB, Dalman C. Refugee migration and risk of schizophrenia and other non-affective psychoses: cohort study of 1.3 million people in Sweden. BMJ [Internet]. 352: 2016 Mar 15; i1030. doi: 10.1136/bmj.i1030
- Tinghög P, Malm A, Arwidson C, Sigvardsdotter E, Lundin A, Saboonchi F. Prevalence of mental ill health, traumas and postmigration stress among refugees from Syria resettled in Sweden after 2011: a population-based survey. BMJ Open [Internet]. 2017 Dec 29 ;7:e018899. doi: 10.1136/bmjopen-2017-018899
- Causevic S. Sexual risk behaviors among young migrants and key populations in Sweden [Internet]. Karolinska Institutet; 2023. Available from: https://openarchive.ki.se/xmlui/handle/10616/48537?_ga=2.61677487.2092886193.1694159395-1007904496.1692870431&pk_vid=46fcb1cfe85649a51694159396709237
- World Value Survey [Internet]. Available from: https://www.iffs.se/world-values-survey/migrant-wvs/#:~:text=Migrant World Values Survey %28mWVS%29 omfattar samma frågor,hösten 2018 i ett urval om 54 kommuner
- Invandrar Index [Internet]. Available from: http://www.invandrarindex.se/
- Hollifield M, Toolson EC, Verbillis-Kolp S, Farmer B, Yamazaki J, Woldehaimanot T, et al. Effective screening for emotional distress in refugees. J Nerv Ment Dis [Internet]. 2016 Apr;204:247–253. doi: 10.1097/NMD.0000000000000469
- Bjärtå A, Leiler A, Ekdahl J, Wasteson E. Assessing severity of psychological distress among refugees with the refugee health screener, 13-item version. J Nerv Ment Dis [Internet]. 2018 Nov 1 [cited 2023 Mar 18];206:834. Available from: http://pmc/articles/PMC6221387/
- Sarkadi A, Bjärtå A, Leiler A, Salari R. Is the refugee health Screener a useful tool when screening 14- to 18-year-old refugee adolescents for emotional distress? J Refug Stud [Internet]. [2019 Dec 1];32:i141–50. Available from: https://academic.oup.com/jrs/article/32/Special_Issue_1/i141/5688816
- Meader N, King K, Moe-Byrne T, Wright K, Graham H, Petticrew M, et al. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health. 2016;16: doi: 10.1186/s12889-016-3373-6
- Amin R, Rahman S, Dorner TE, Björkenstam E, Helgesson M, Norredam ML, et al. Country of birth, time period of resettlement and subsequent treated common mental disorders in young refugees in Sweden. Eur J Public Health [Internet]. 2020 Dec 11; 30:1169–1175. doi: 10.1093/eurpub/ckaa140.
- Migrationsverket. Applications for Asylum Received [Internet]. 2016. Available from: https://www.migrationsverket.se/download/18.7c00d8e6143101d166d1aab/1485556214938/Inkomnaansökningaromasyl2015-Applicationsforasylumreceived2015.pdf
- Migrationsverket. Asyl [Internet]. 2021 [cited 2021 Apr 1]. Available from: https://www.migrationsverket.se/Om-Migrationsverket/Statistik/Asyl.html
- Azur MJ, Stuart EA, Frangakis C, Leaf PJ. Multiple imputation by chained equations: what is it and how does it work? Int J Methods Psychiatr Res [Internet]. 2011 Mar;20:40–49. doi: 10.1002/mpr.329
- Rubin DB. Basic ideas of multiple imputation for nonresponse [Internet]. Surv Methodol. 1986;12:37–47. Available from: https://www150.statcan.gc.ca/n1/en/pub/12-001-x/1986001/article/14439-eng.pdf?st=6eB6lSXd
- Leiler A, Bjärtå A, Ekdahl J, Wasteson E. Mental health and quality of life among asylum seekers and refugees living in refugee housing facilities in Sweden. Soc Psychiatry Psychiatr Epidemiol [Internet]. 2019 May 22;54: 543–551. doi: 10.1007/s00127-018-1651-6
- Juárez SP, Honkaniemi H, Dunlavy AC, Aldridge RW, Barreto ML, Katikireddi SV, et al. Effects of non-health-targeted policies on migrant health: a systematic review and meta-analysis. Lancet Glob Health [Internet]. 2019 Apr 1; 7:e420–35. doi: 10.1016/S2214-109X(18)30560-6
- Juárez SP, Drefahl S, Dunlavy A, Rostila M. All-cause mortality, age at arrival, and duration of residence among adult migrants in Sweden: a population-based longitudinal study. SSM - Popul Heal [Internet]. 2018 Dec;6:16–25. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2352827318300053
- Priebe S, Giacco D, El-Nagib R. Public health aspects of mental health among migrants and refugees: a review of the evidence on mental health care for refugees, asylum seekers and irregular migrants in the WHO European Region. Heal Evid Netw Synth Rep 47 [Internet]. 2016: ix-pp. Available from: http://www.euro.who.int/__data/assets/pdf_file/0003/317622/HEN-synthesis-report-47.pdf?ua=1
- Okenwa-Emegwa L, Saboonchi F, Mittendorfer-Rutz E, Helgesson M, Tinghög P. Prevalence and predictors of low future expectations among Syrian refugees resettled in Sweden. Heliyon [Internet]. 2019 Oct;5:e02554. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2405844019362140
- Mohwinkel LM, Nowak AC, Kasper A, Razum O. Gender differences in the mental health of unaccompanied refugee minors in Europe: a systematic review. BMJ Open [Internet]. 2018 Jul 30;8: e022389. doi: 10.1136/bmjopen-2018-022389
- Leiler H, Wasteson B. Suicidal ideation and severity of distress among refugees residing in asylum accommodations in Sweden. Int J Environ Res Public Health [Internet]. 2019 Aug 1;16:2751. doi: 10.3390/ijerph16152751
- Manhica H, Almquist Y, Rostila M, Hjern A. The use of psychiatric services by young adults who came to Sweden as teenage refugees: a national cohort study. Epidemiol Psychiatr Sci [Internet]. 2017 Oct 29;26:526–534. Available from: https://www.cambridge.org/core/product/identifier/S2045796016000445/type/journal_article
- Kosidou K, Hellner-Gumpert C, Fredlund P, Dalman C, Hallqvist J, Isacsson G, et al. Immigration, transition into adult life and social adversity in relation to psychological distress and suicide attempts among young adults Braitstein P, editor. PLoS One [Internet]. 2012 Oct 3;7:e46284. doi: 10.1371/journal.pone.0046284
- Delilovic S, Hagström A, Shedrawy J, Lönnroth K. Centrum för epidemiologi och samhällsmedicin, Region Stockholm. 2020 [cited 2021 Sep 9]. Screening av psykisk ohälsa med Refugee Health Screener – En Uppföljning Från Region Stockholm. Available from: https://www.folkhalsoguiden.se/globalassets/verksamheter/forskning-och-utveckling/centrum-for-epidemiologi-och-samhallsmedicin/folkhalsoguiden/rapporter-och-faktablad/rapport-2020.2-screening-av-psykisk-ohalsa-med-refugee-health-screener.pdf
- Mundy SS, Foss SLW, Poulsen S, Hjorthøj C, Carlsson J. Sex differences in trauma exposure and symptomatology in trauma-affected refugees. Psychiatry Res. 2020;293. doi: 10.1016/j.psychres.2020.113445
- Voolma H. “I must be silent because of residency”: barriers to escaping domestic violence in the context of insecure immigration status in England and Sweden. Violence Against Women [Internet]. 2018 Dec 25 24:1830–1850. doi: 10.1177/1077801218755974
- Pongthippat W, Darvishpour M, Kijsomporn J, Östlund G. Broken dreams of a better life in Sweden: Thai women’s lived experiences of intimate partner violence by Swedish men in international marriages. Glob Health Action [Internet]. 2018 Jan 3;11: 1496889. doi: 10.1080/16549716.2018.1496889
- Vasil S. “I came here, and it got worse day by day”: examining the intersections between migrant precarity and family violence among women with insecure migration status in Australia. Violence Against Women. 2023;107780122311594. doi: 10.1177/10778012231159414
- Helgesson M, Johansson B, Nordquist T, Vingård E, Svartengren M. Healthy migrant effect in the Swedish context: a register-based, longitudinal cohort study. BMJ Open [Internet]. 2019 Mar 15;9:e026972. doi: 10.1136/bmjopen-2018-026972
- Andersson LMC, Hjern A, Ascher H. Undocumented adult migrants in Sweden: mental health and associated factors. BMC Public Health [Internet]. 2018 Dec 12;18:1369. doi: 10.1186/s12889-018-6294-8
- Dykxhoorn J, Hollander AC, Lewis G, Dalman C, Kirkbride JB. Family networks during migration and risk of non-affective psychosis: a population-based cohort study. Schizophr Res [Internet]. 2019 Jun 1; 208:268–275. doi: 10.1016/j.schres.2019.01.044
- Fakoya I, Álvarez-Del Arco D, Woode-Owusu M, Monge S, Rivero-Montesdeoca Y, Delpech V, et al. A systematic review of post-migration acquisition of HIV among migrants from countries with generalised HIV epidemics living in Europe: implications for effectively managing HIV prevention programmes and policy. BMC Public Health [Internet]. 2015 Dec 19;15:561. doi: 10.1186/s12889-015-1852-9
- Karle A, Agardh A, Larsson M, Arunda MO. Risky sexual behavior and self-rated mental health among young adults in Skåne, Sweden – a cross-sectional study. BMC Public Health [Internet]. 2023 Jan 3; 23:9. doi: 10.1186/s12889-022-14823-0