
ABSTRACT
Women in Bangladesh share a greater risk of Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) infection compared to men. Levels of knowledge and awareness largely contribute to the prevalence of the HIV epidemic and its consequences. So, it is required to conduct studies based on most recent data to explore the determinants of HIV awareness. Therefore, we aimed to find the awareness level and factors influencing HIV related awareness among the married women in Bangladesh. We used data from 2014 Bangladesh Demographic and Health Survey (BDHS). About two-third of total respondents who heard about the HIV/AIDS were selected and interviewed successfully (n = 12,593) about 11 basic questions related to individual’s awareness. A score of the respondent’s knowledge and awareness was determined based on these questions. We used logistic regression models for analysing the data. We found about 62% of the respondents had an adequate knowledge and consciousness about the HIV/AIDS. Respondents’ education status, mass-media access, place of living, and working status played significant role on the awareness. As expected, respondents with higher education were more aware than those with no education (odds ratio (OR) = 3.56, 95% confidence interval (CI): 2.99–4.23). Moreover, respondents who had access to the mass media were more likely to be aware compared to those who did not have the access (OR = 1.14, 95% CI: 1.04–1.26). Although a sizeable proportion of women had an adequate knowledge and awareness regarding the HIV/AIDS, we recommend implementing educational programmes related to HIV/AIDS in the curriculum to ensure a standard level of awareness throughout the nation. Since the respondents from rural areas scored significantly lower than the urban areas, awareness through mass media, particularly in rural areas, is of prime concern for raising awareness.
Introduction
Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) is one of the most pandemic spreading diseases in worldwide. In 2016, there were roughly 1.8 million new HIV infections – a decline from 2.1 million new infections in 2015 (UNAIDS, Citation2018b). Despite the progress made across the world with a decline in new infections, the Joint United Nations Programme on HIV/AIDS (UNAIDS) warned that progress in combating viral transmission is still not happening fast enough to meet global targets (UNAIDS, Citation2018b).
In Asia and Pacific regions, people (age 15–49) living with HIV up to 2016 was 5.1 million with a prevalence of 0.2%. In that case, the number of newly infected cases was 2.7 million (UNAIDS, Citation2018a) Although Bangladesh has one of the lowest rates of HIV in the Southeast Asian region (World Health Organization, Citation2012), the number of infected people increased from 2014 (11,000) to 2016 (12,000) (UNAIDS, Citation2018c).
Although Bangladesh falls in the category of countries bearing low HIV risk, due to rapid urbanisation and migration (both internal and external), rising unemployment and economic problems in the recent decade, the chance of further expansion of HIV should not be underestimated. Moreover, the risk of HIV remains high in Bangladesh due to widespread prevalence of the risk factors like, poor medical facilities, lack of sufficient screening practices, and unsafe sexual practices, (Azim et al., Citation2008; Hossain, Mani, Sidik, Shahar, & Islam, Citation2014; Khosla, Citation2009; Rahman, Kabir, & Shahidullah, Citation2009; Sarkar et al., Citation2006). Previous studies revealed that the prevalence of HIV is relatively high among people who are unaware of the potential routes of transmission (Aliyu et al., Citation2010; Appiah-Agyekum & Suapim, Citation2013). In addition, the risk of future expansion remains high due to its high prevalence of our neighbour countries like India, Myanmar, Nepal, and Thailand. For example, India alone has 2.1 million people living with HIV (40.5% women) and 0.26% adult HIV prevalence (Joint United Nations Programme on, 2011; National institute of medical statistics Icmr & Family welfare, 2015).
Worldwide young women are especially at risk of getting infected by HIV with 59% of new infections among young people aged 15–24 occurring among this group (UNAIDS, Citation2018b). Similar to the current global trend, women in Bangladesh share a greater risk of HIV infection and mortality compared to men ((NIPORT), Associates, & International, Citation2007). They are considered as a high-risk group due to lack of opportunity for general and health education (Asaduzzaman, Higuchi, Sarker, & Hamajima, Citation2016). Moreover, sexual behaviour of married men living long time in abroad or in different cities for their work may put their wives at risk for HIV/AIDS infections (Mercer, Khanam, Gurley, & Azim, Citation2007).
According to UNAIDS, in Bangladesh, number of women living with HIV was 2800 in 2012, which become 3900 in 2016 [3], indicating an increasing trend of HIV infections among women in Bangladesh. Since there is currently no cure for HIV, higher degree of awareness and proactive measures are needed to avert it. A number of studies have been conducted from time to time to find out the level of awareness among women in Bangladesh using both primary and secondary data (Asaduzzaman et al., Citation2016; Rahman et al., Citation2009). Most of the studies tried to find socio-demographic factors and trends of AIDS among married women in Bangladesh (Asaduzzaman et al., Citation2016; Hosain & Islam, Citation2016; Yaya, Bishwajit, Danhoundo, Shah, & Ekholuenetale, Citation2016). In this situation, further research is required to know the present HIV knowledge status in Bangladesh. Hence, we have intended to investigate the knowledge and awareness of HIV among married women in Bangladesh, using most recent 2014 Bangladesh Demographic and Health Survey (BDHS) dataset, which serves only female data. Our main objective was to assess the extent of HIV knowledge among women in Bangladesh. We also aimed at identifying the responsible factors for changing knowledge, attitudes and intensity about HIV/AIDS, making a comparison between current and previous extent of HIV knowledge, and finding the spans where further improvement is required to enhance the consciousness of HIV knowledge.
Methods
The survey and data source
The Demographic and Health Surveys (DHSs) are nationally representative surveys, which were designed to collect data from households to monitor and evaluate the nutrition, population and health status of developing countries ((NIPORT), Associates, & International, Citation2014). In Bangladesh, the survey has been carried out since 1993 in a three-year interval under the authority of the National Institute for Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare. The financial support for the survey was provided by the United States Agency for International Development (USAID), Bangladesh. The data are free and available for research. In this study, we used the latest available data of 2014 BDHS.
Sampling design and sample size
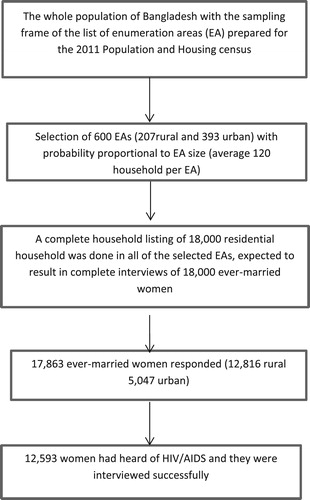
The BDHS 2014 survey is based on a two-stage stratified sample of households. The data were collected from seven administrative divisions: Barisal, Chittagong, Dhaka, Khulna, Rajshahi, Rangpur, and Sylhet. The survey used the list of enumeration areas (EAs) of 2011 Population and Housing Census (PHC) of the People’s Republic of Bangladesh, provided by the Bangladesh Bureau of Statistics (BBS). In the first stage, 600 EAs were selected with probability proportional to the EA size, with 207 EAs in urban areas and 393 in rural areas. The survey selected 18,000 residential households, which were expected to result in complete interviews with about 18,000 ever-married women. Among them17, 863 women responded to the study with a response rate of 99.24%. Among them, 12,593 (34.5% urban, 65.5% rural) women were found to have heard of HIV/AIDS. As HIV is a Sexually Transmitted Disease (STD) and women in Bangladesh usually become sexually active after marriage, only ever-married women who heard about HIV/AIDS were recruited to ask questions about HIV related awareness. The complete procedure of sample design and sample selection is shown in .
Figure 1. Study population and sample selection.
Outcome
Respondents who ever heard of AIDS were asked 11 HIV knowledge and awareness related questions (). For each question, a score of 1 was assigned to each ‘correct’ answer and a score of 0 for ‘incorrect’ answer. ‘Don’t know’ was coded as ‘incorrect’. No deductions were made for any answer. ‘Knowledge score’ variable was constructed based on the summation of these scores and used as outcome variable. This had a possible range of 0 to 11, whereby higher scores indicated greater knowledge of HIV. Finally, scores greater than or equals to the median (Sarkar et al., Citation2006) were assigned to ‘High score’ category and the rest scores were treated as to fall in the category, ‘Low score’ (Talwar & Rahman, Citation2015).
Covariates
A set of covariates such as ten years age group, type of place of residence, respondent’s education, region, wealth index, husband’s education, working status, access to mass media, religion, and sex of household head were used. Two back to back 5-years age groups were merged to compute new 10 years age group variable. The variable access to mass media was constructed upon the condition that a respondent have access to at least one of three mediums television, newspaper or radio. Details including levels of covariates are provided in .
Table 1. HIV/AIDS knowledge and awareness score status at different levels of covariates.
Statistical analysis
Bivariate analysis (Chi-square test for association) was conducted to assess the association between score categories and socio-demographic characteristics of respondents at the individual level. A binary logistic regression model was used to get an insight of the impact of different socio-demographic variables on the score status of respondents. The final logistic regression model was selected based on a backward elimination procedure. Variables with a probability of its score statistic less than 0.05 were included in the model. It has taken 4 steps to reach the ultimate fitted model. The ultimate model output was represented in a forest-plot.
Results
represents the score of respondents by their socio-demographic characteristics affecting the levels of HIV knowledge including p-values from chi-square test. Overall, 61.6% respondents scored ‘high score’ and the rest 38.4% scored ‘low score’ regarding HIV/AIDS awareness. We found score status (low or high) varied significantly among different categories of age group, residence type, educational attainment and access to mass media, wealth index, geographical location and husband’s education level. Younger respondents had a higher score than the older respondents. Percentages of ‘High Score’ for age groups 15–24, 25–34, 35–44 and ≥45 were 62.6%, 63.2%, 59.7% and 54.6%, respectively. Altogether 80% of Individuals with higher educational level had the ‘High Score’, only 50.1% of respondents with a status of no education had the ‘High Score’. A similar trend was found in case of respondent’s spouse’s educational achievement. As compared to poor and middle class individuals, richest subjects were less likely to get ‘Low Score’. Married women from Dhaka division got the highest percentage (64.5%) of ‘High Score’, which was close to Khulna division (63.3%). However, subjects from Sylhet division made the lowest percentage (51.5%) of ‘High Score’.
depicts that, that respondents from the urban area had a higher percentage of ‘High Score’ than their rural counterparts in each division. Among different religious groups, Christian’s showed a higher percentage (75.0%) of ‘High Score’. shows a comparison of correct response rate between the years 2011 and 2014. Percentages of the correct response to questions about HIV/AIDS related knowledge have fallen for each of the questions with an exception of the question about the possibility of getting HIV from mosquito bites (47.3% to 54.1%). Highest fall in correct response (85.5% to 79.8%) was found in case of knowledge about transmission of HIV during pregnancy.
Figure 2. Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) awareness score status by place of residence.
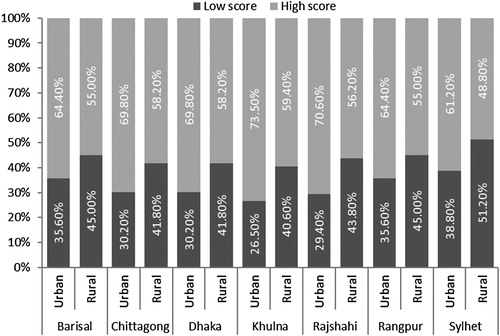
Table 2. Comparison of correct response rate between two consecutive BDHSa survey.
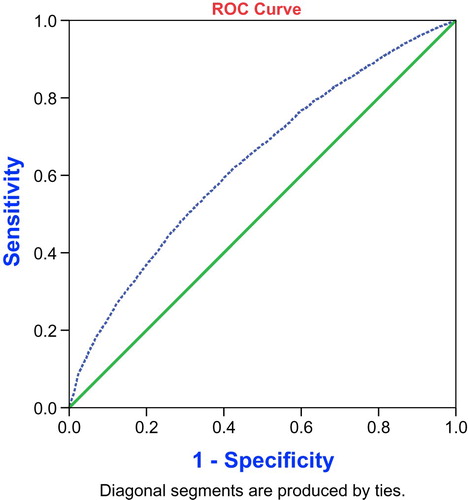
portrays the results of binary logistic regression analysis of HIV/AIDS related awareness, including 95% CI for odds ratio (OR). Individuals with younger age, having higher education and access to mass media, currently working outside the home, and living in mostly urbanised areas were subjected to get ‘High Score’ more frequently; compared to their counterparts. To illustrate, respondents aged 25–34 years were 1.23 (95% CI: 1.06–1.43) times more likely to get ‘High Score’ than the respondents aged ≥45 years old. As expected, respondents with higher education had 3.56(95% CI: 2.99–4.23) times more chance to obtain ‘High Score’ than those with no education and it was easier to get ‘High Score’ for women who had access to mass media (OR = 1.14, 95% CI: 1.04–1.26) and currently working(OR = 1.11, 95% CI: 1.02–1.20). Moreover, subjects from the urban area were more likely to achieve ‘High Score’ (OR = 1.22, 95% CI: 1.11–1.33) compared to subjects from a rural part of the country. Our model fitting criteria Hosmer and Lemeshow (H-L) showed the p-value of 0.744 meaning that it was not statistically significant and therefore the model was quite a good fit. Moreover, the AUC of receiver operating characteristic curve (ROC) was found to be 0.64 (Asymptotic p-value: 0.000 and 95% CI: .63–.66) indicating the final selected model showed a good fit of the data ().
Figure 3. Forest plot of Odds ratios (ORs) and 95% confidence intervals (CIs) for knowledge and awareness of Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS).
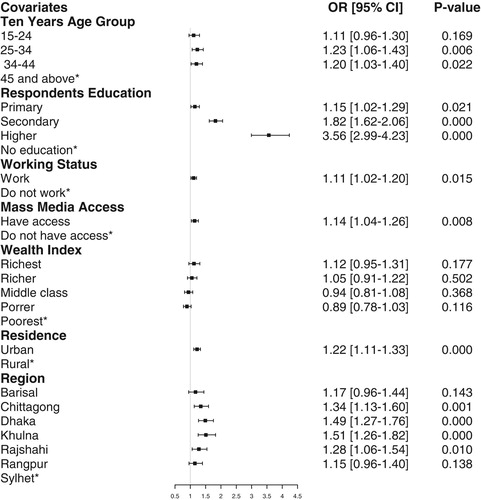
Figure 4. Sensitivity analysis of fitted final multivariable logistic regression model.
Discussion
We investigated the knowledge and level of consciousness about HIV/AIDS among sexually active women of Bangladesh. We observed that a large portion of the women (61.6%) had high score regarding HIV-related knowledge and awareness. This finding is in line with the previous BDHS reports in 2011 and 2007 (National Institute of Population Research and Training (NIPORT), Mitra and Associates, and Macro International, Citation2007; (NIPORT), Associates, & International, Citation2011). Moreover, this figure is higher than that of the other two countries, India and Pakistan of this sub-continent (Arnold, Parasuraman, Arokiasamy, & Kothari, Citation2009; (NIPS) & International, Citation2013). However, this percentage is higher in the largest Muslim country Indonesia than Bangladesh (Statistik—BPS), (BKKBN), (Kemenkes—MOH), & International, Citation2013). We also found a strong impact of education, mass-media access and place of living, and working status on the respondent’s HIV knowledge and awareness.
We observed that sex of household head and religion had no significant association with HIV knowledge score. However, in an earlier study, sex of household head was found to be significantly associated with HIV knowledge (Yaya et al., Citation2016). This may be due to success of women empowerment in recent years in Bangladesh and hence, more women are being educated and participating in decision making than before.
We also revealed that correct response to almost every HIV/AIDS awareness indicator has fallen compared to 2011 (Yaya et al., Citation2016). Lack of sufficient effective publicity of correct and specific HIV knowledge related information might be responsible for this situation. In all administrative division, respondents from rural area were less likely to get high HIV knowledge score than urban people; as rural people have little access to mass media. Moreover, lack of educational institutions deprives them of being aware of the HIV. These simultaneous events make countryside people less aware of HIV than their counterparts in cities.
Overall younger respondents were found to be more aware of HIV than older ones belonging to age group 45 or above, reflecting similarities with previous studies (Mondal, Rahman, Rahman, & Akter, Citation2012; Yaya et al., Citation2016). Since, members of the young generation commonly get in touch with social media and all other mediums of mass media, which help them to know information regarding the HIV. Level of educational attainment was a major influencing factor to awareness of HIV/AIDS. Level of awareness rose significantly with years of schooling. This finding is consistent with previous studies (Rahman & Rahman, Citation2007; Sultana, Citation2009; Yaya et al., Citation2016). Access to mass media also played important role in determining the state of subject’s awareness about HIV/AIDS. Respondents with access to at least one of three mediums, Television, Radio and Newspaper or magazine, achieved a higher level of awareness score. Earlier publications contain similar information about the influence of mass media on HIV/AIDS awareness of Bangladeshi women (Rahman & Rahman, Citation2007). Richest respondents were found to perceive higher HIV score compared to their poorest counterparts. Because of the members of the wealthy family enjoy easy access to mass media and are usually well educated.
Strengths and limitations
To the best of our knowledge, this is the first study based on most recent BDHS data in the context of HIV/AIDS awareness among Bangladeshi married women. We used a sufficiently large nationally representative dataset, which represents the general population of Bangladesh. We also considered a wide range of factors that are influencing the concerned awareness. Additionally, we assessed model-fitting criterions, which were generally missing in the literature. Despite that, our study had some limitations. As we used secondary data, selection of variables, quality of data and measurement indicators were beyond control. Moreover, the survey was conducted three years ago; in the meantime, level of respondent’s awareness may have changed.
Conclusion
The study focused on the level and influencing factors of HIV/AIDS awareness among married women from both rural and urban area of Bangladesh. Strong impact of education, mass-media accessibility, place of living, wealth index, and working status on respondent’s HIV knowledge and awareness was detected. Although a considerable number of women had an adequate knowledge regarding consciousness about the HIV, initiatives should be taken to enlarge the participation of masses in higher education. Adding HIV/AIDS related knowledge to higher-secondary text-books could be a valuable step towards enlightenment of common people about this pandemic. Moreover, awareness raising campaigns should be promoted in places like Schools, Mosques/Temples/Churches, and workplaces on a regular basis. Furthermore, utilising the popularity of mass media (Television, Newspaper and Radio) to raise awareness through specially designed programmes suitable for people wherever they live in urban or rural regions is recommended. Finally, a strong social movement against spreading HIV/AIDS risk factors is needed to tackle this tremendous epidemic.
Acknowledgments
We would like to express our gratitude to MEASURE DHS and National Institute of Population Research and Training (NIPORT), Bangladesh for giving opportunity to use the data set.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Md. Ashiqul Haque http://orcid.org/0000-0002-6486-5367
Muhammad Abdul Baker Chowdhury http://orcid.org/0000-0002-2145-0938
Md Jamal Uddin http://orcid.org/0000-0002-8360-3274
References
- Aliyu, G., Mohammad, M., Saidu, A., Mondal, P., Charurat, M., Abimiku, A. L., … Blattner, W. (2010). Hiv infection awareness and willingness to participate in future HIV vaccine trials across different risk groups in Abuja, Nigeria. AIDS Care, 22(10), 1277–1284. doi: 10.1080/09540121003692219
- Appiah-Agyekum, N. N., & Suapim, R. H. (2013). Knowledge and awareness of HIV/AIDS among high school girls in Ghana. HIV/AIDS (Auckland, NZ), 5, 137–144.
- Arnold, F., Parasuraman, S., Arokiasamy, P., & Kothari, M. (2009). National Family Health Survey (NFHS-3) India 2005–06.
- Asaduzzaman, M., Higuchi, M., Sarker, M. A. B., & Hamajima, N. (2016). Awareness and knowledge of HIV/AIDS among married women in rural Bangladesh and exposure to media: A secondary data analysis of the 2011 Bangladesh demographic and health survey. Nagoya Journal of Medical Science, 78(1), 109–118.
- Azim, T., Chowdhury, E. I., Reza, M., Faruque, M. O., Ahmed, G., Khan, R., … Strathdee, S. A. (2008). Prevalence of infections, HIV risk behaviors and factors associated with HIV infection among male injecting drug users attending a needle/syringe exchange program in Dhaka, Bangladesh. Substance use & Misuse, 43(14), 2124–2144. doi: 10.1080/10826080802344583
- Hosain, M. T., & Islam, M. Z. (2016). Factors affecting knowledge, attitudes and behavior of HIV/AIDS: A study on Bangladesh. Australian Journal of Business Science Design & Literature, 09(02).
- Hossain, M., Mani, K. K., Sidik, S. M., Shahar, H. K., & Islam, R. (2014). Knowledge and awareness about STDs among women in Bangladesh. BMC Public Health, 14(1), 775. doi: 10.1186/1471-2458-14-775
- Khosla, N. (2009). Hiv/AIDS interventions in Bangladesh: What can application of a social exclusion framework tell us? Journal of Health, Population and Nutrition, 27(4), 587–597. doi: 10.3329/jhpn.v27i4.3404
- Mercer, A., Khanam, R., Gurley, E., & Azim, T. (2007). Sexual risk behavior of married men and women in Bangladesh associated with husbands’ work migration and living apart. Sexually Transmitted Diseases, 34(5), 265–273.
- Mondal, M. N. I., Rahman, M. M., Rahman, M. O., & Akter, M. N. (2012). Level of awareness about HIV/AIDS among ever married women in Bangladesh. Food and Public Health, 2(3), 73–78. doi: 10.5923/j.fph.20120203.03
- National Institute of Population Research and Training (NIPORT), Mitra and Associates, and Macro International. (2007). Bangladesh demographic and health survey 2007. Dhaka, Bangladesh and Calverton, Maryland, USA: National Institute of Population Research and Training, Mitra and Associates, and Macro International.
- National Institute of Population Research and Training (NIPORT), Mitra and Associates, and Macro International. (2011). Bangladesh demographic and health survey 2011. Dhaka, Bangladesh and Calverton, Maryland, USA: National Institute of Population Research and Training, Mitra and Associates, and Macro International.
- National Institute of Population Research and Training (NIPORT), Mitra and Associates, and Macro International. (2014). Bangladesh demographic and health survey 2014. Dhaka, Bangladesh and Calverton, Maryland, USA: National Institute of Population Research and Training, Mitra and Associates, and Macro International.
- National Institute of Population Studies (NIPS) [Pakistan] and ICF International. (2013). Pakistan demographic and health survey 2012–13. Islamabad, Pakistan, and Calverton, Maryland, USA: NIPS and ICF International.
- Rahman, M. M., Kabir, M., & Shahidullah, M. (2009). Adolescent knowledge and awareness about AIDS/HIV and factors affecting them in Bangladesh. Journal of Ayub Medical College, Abbottabad, 21(3), 3–6.
- Rahman, M. S., & Rahman, M. L. (2007). Media and education play a tremendous role in mounting AIDS awareness among married couples in Bangladesh. AIDS Research and Therapy, 4(1), 4–10. doi: 10.1186/1742-6405-4-10
- Sarkar, K., Bal, B., Mukherjee, R., Chakraborty, S., Niyogi, S. K., Saha, M. K., & Bhattacharya, S. K. (2006). Epidemic of HIV coupled with hepatitis C virus among injecting drug users of Himalayan West Bengal, Eastern India, bordering Nepal, Bhutan, and Bangladesh. Substance use & Misuse, 41(3), 341–352. doi: 10.1080/10826080500410991
- Statistics Indonesia (Badan Pusat Statistik—BPS), National Population and Family Planning Board (BKKBN), and Kementerian Kesehatan (Kemenkes—MOH), and ICF International. (2013). Indonesia demographic and health survey 2012. Jakarta, Indonesia: BPS, BKKBN, Kemenkes, and ICF International.
- Sultana, N. (2009). Awareness on HIV/AIDS among the blood donors of a city hospital. Ibrahim Medical College Journal, 3(2), 63–66.
- Talwar, P., & Rahman, M. F. B. A. (2015). Assessment of HIV knowledge among university students using the HIV-KQ-18 scale: A cross-sectional study. South East Asia Journal of Public Health, 5(1), 33–38. doi: 10.3329/seajph.v5i1.24849
- UNAIDS. (2018a). Asia and Pacific. Retrieved from http://www.unaids.org/en/regionscountries/asiaandpacific.
- UNAIDS. (2018b). Fact sheet - Latest statistics on the status of the AIDS epidemic. Retrieved from http://www.unaids.org/en/resources/fact-sheet.
- UNAIDS. (2018c). UNAIDS-Bangladesh. Retrieved from http://www.unaids.org/en/regionscountries/countries/bangladesh.
- World Health Organization, Regional Office for South-East Asia. (2012). HIV/AIDS in the South-East Asia region: Progress report 2011. http://www.searo.who.int/entity/hiv/documents/hiv-aids_in_south-east_asia.pdf.
- Yaya, S., Bishwajit, G., Danhoundo, G., Shah, V., & Ekholuenetale, M. (2016). Trends and determinants of HIV/AIDS knowledge among women in Bangladesh. BMC Public Health, 16(1), 812. doi: 10.1186/s12889-016-3512-0