
1. Introduction
The Ovation (Endologix Inc. Irvine, CA, USA) aortic endograft has been introduced in the field of endovascular aneurysm repair (EVAR) as a design with the unique concept of disengaging sealing and fixation mechanisms [Citation1]. The initial design achieved active suprarenal fixation via a long nitinol stent and infrarenal sealing via a pair of polymer-filled inflatable rings with a proximal mid-crown PTFE segment containing Nitinol located between the stent and the rings [Citation1]. As a matter of fact, the sealing relies basically only on the proximal ring while the distal one is a reservoir that effectively helps in achieving the pressure-volume equilibrium when the polymer is being injected.
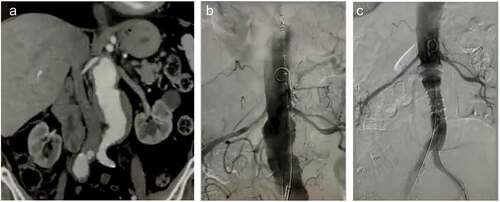
The Ovation endograft has documented excellent technical and clinical results even in a wide range of infrarenal neck irregularities, including conical morphology, circumferential calcification and significant thrombus onto the neck surface [Citation2,Citation3]. The recently FDA approved Ovation Alto design lacks the nitinol-containing fabric contained in the previous Ovation iX platform, repositioning the maximum diameter of the proximal sealing ring at 7 mm below the lowermost renal artery [Citation4]. The key-point in the Alto design is the integration of a compliant balloon in the delivery system to compensate for the lack of the stented mid-crown, facilitating the deployment of the sealing rings and, secondarily, achieving optimal apposition immediately after the polymer filling (). The accommodation of the sealing rings immediately below the renal arteries provides literally the shortest sealing zone for EVAR, thus broadening the indications—compared to any other stent graft- to include more complex abdominal aortic aneurysms (AAA) as well [Citation4–7].
Figure 1. (a) A 55 mm abdominal aortic aneurysm with short neck (average diameters of 27.6 mm and 32.7 mm at 7 mm at 10 mm diameter below the lowermost renal artery, respectively). (b). Efficient sealing relies on the accurate apposition of the first sealing ring immediately below the renal arteries. (c). Intraoperative completion angiography demonstrating technical success, i.e. aneurysm exclusion without endoleak (image courtesy of Dr. Kapoulas).
2. The new design of Ovation Alto: challenging the challenging cases
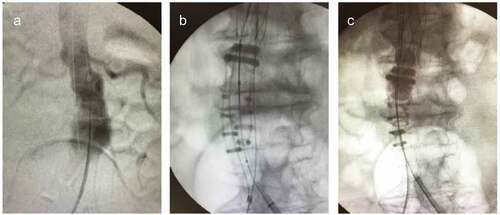
Gregory et al. have recently described the new Ovation Alto endograft for the treatment of AAA [Citation4]. The first published cases in the literature reported by Holden and Lyden report excellent technical success, yet in AAA with adequate length of infrarenal neck of 11–35 mm [Citation5]. Additionally, de Donato et al., have just documented satisfying technical results with the use of the new Ovation Alto platform in 11 AAA cases, mainly with short necks, ≤10 mm [Citation6]. The Alto design facilitates the sealing in shorter necks (≥7 mm) in contrast to the instructions for use (IFU) of other commercially available endografts [Citation7]. Furthermore, this unique configuration deems ideal for conical-shaped necks, which have been associated with proximal failure of standard endovascular repair () [Citation8]. On the other hand, the definition/description of neck conicity as >10% difference in neck diameter from the inferior renal artery to the level 7 mm caudally or a gradual neck dilation >2 mm may not fit within a unique endograft size, leaving the selection to the physician; for example, a neck diameter discrepancy from 22 mm at the renal level to 24.5 mm at 7 mm caudally falls in the 26 mm and 29 mm endograft size, accordingly. Therefore, the experienced physician should study very carefully the apposition sites of the rings in order to predict for the optimal endograft size.
Figure 2. (a). A 52 mm abdominal aortic aneurysm with conical neck (diameters of 21.7 mm and 24 mm at 7 mm at 10 mm diameter below the lowermost renal artery, respectively). (b). Efficient sealing relies on the adjusted apposition on the conical irregularities of the neck. (c). The balloon is slightly advanced 5–7 mm cranially to inflate and facilitate accurate sealing (image courtesy of Dr. Georgakarakos).
Yet, the unique Alto design may also prove beneficial in cases of wide necks ≥30 mm, which comprise an independent factor for neck-related adverse events even in midterm follow-up, with endoleak Type 1a being the predominant [Citation9–11]. Admittedly, the causes of post-EVAR aortic neck dilatation have not been clearly identified. Factors such as the nitinol-based continuous radial force have been suggested, as well as the degree of graft oversizing or the ongoing degenerative aneurismal process. While none of these has been clearly identified to be a dominant and independent factor, it seems though that the wide necks are affected to a greater degree from the aforementioned and have a greater rate of dilatation over time [Citation12]. Of note, although there has been no strong association with this regard in the literature, a short neck correlates more likely with wider neck diameter [Citation13]. Therefore, a new concept of more proximal sealing with minimal radial force provided by Alto seems appealing also for wide necks.
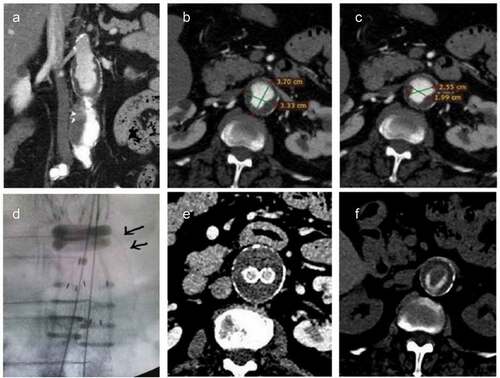
Notably, while in nitinol-based endografts the outer-to-outer wall diameter determines the size of the stent-graft, the measurement for the Ovation size involves the lumen diameter plus half the thrombus thickness on both sides but to a maximum value of 2 mm. Given that the thrombus layers are not of equal density or mechanical properties, the Ovation size achieves optimal apposition of the rings against a partially compressed thrombus [Citation14,Citation15]. This promising, yet ambitious apposition/sealing concept is of paramount importance and presumably the key to clinical success, since the thrombus burden is the only sealing surface in the wide necks of juxtarenal aneurysms. presents a juxtarenal AAA of 55 mm with a wide infrarenal neck starting immediately below the renal arteries ()), with the external diameter (outer-to-outer) of the neck at the level 7 mm below the lowermost renal artery, being 33–37 mm ()). Due to the heavy intraluminal thrombus burden, the true lumen dimensions were estimated 19–25 mm ()). It is crucial to delineate that the sizing philosophy of the Ovation sealing rings takes into account for sizing of the endograft the lumen diameter plus half the thrombus thickness on both sides but to a maximum value of 2 mm (provided that the total thickness of thrombus does not exceed 8 mm) which puts the AAA outside the IFU. Hence the patient was treated with a 26 mm endograft, with the sealing rings landing at the transition of the aneurysm sac ()). The 1-month postoperative computed tomography angiography shows successful exclusion of the aneurysm sac ()) with the radiopaque-polymer rings ()) sealing against the thrombus surface. Long-term results on the durability of sealing are mandatory to affirm whether the management of complex AAA will be revolutionized toward this direction.
Figure 3. (a). A 55 mm juxtarenal Abdominal Aortic aneurysm in a 70 year-old female patient ineligible to sustain open repair or complex endovascular solution. (b). The outer-to-outer wall of the infrarenal neck wall reaches a maximum diameter of 37 mm at 7 mm infrarenally. (c). Yet, the lumen diameter differs significantly from the outer diameter, estimated 19–25 mm. (d). An Ovation Alto achieved successful sealing in the distended neck, deployed actually within the aneurysm. The arrows depict the transition of the aneurysm extending proximally to the infrarenal level. (e). Absence of endoleaks confirmed 1-month postoperatively in computed tomography with intravenous contrast. (f). The landing of the radiopaque polymer-filled ring within the lumen against the burden of the thrombus surface in the non-contrast computed tomography (image courtesy of Dr. Georgakarakos).
The great challenge for the Alto platform is the successful application on juxtarenal aneurysms, where the infrarenal sealing zone can be absent, short and/or wide and carrying a significant burden of intraluminal thrombus. The current guidelines of the European Society for Vascular Surgery dictate the fenestrated approach for juxta- or pararenal AAA, leaving as a bailout solution the parallel grafts option (periscope/chimney technique), provided that the latter is limited to a maximum of two parallel grafts in order to provided an acceptable clinical success rate when performed in specialized, dedicated vascular centers [Citation16].
3. Limitations to use of Ovation Alto
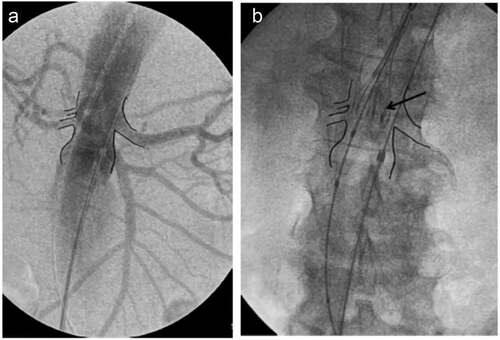
A concern associated with the use of Ovation in EVAR is the options to manage central endoleaks, since the stiffening of the polymer-filled rings precludes the effective use of cuffs or stents to distend them due to the polymer solidification. The sealing agents most effectively used are glue and coil embolization since type 1A endoleaks cannot be treated well with cuffs, unless the aortic body has been deployed in a significantly distal position [Citation17]. Therefore, it is imperative that the sealing rings are deployed absolutely according to plan so that the seal as planned at 7 mm immediately infrarenally is indeed achieved at this precise site and not more caudally. In order to do so, the beginning of deployment should begin ‘aggressively’ against the renal arteries ().
Figure 4. (a). Intraoperative angiography of an aneurysm to mark the orifice of the renal arteries. (b). In order to achieve very precise sealing at 7 mm infrarenally, it is advisable to begin deployment with the proximal markers (arrow) of the top end of the graft aggressively at the level of the renal arteries – or even more centrally- in order to counterbalance an anticipated small caudal migration upon completion of the deployment (image courtesy of Dr. Georgiadis).
Additionally, as Gregory et al. underline, the Alto modification was launched by Endologix as a direct modification of the previous Ovation iX platform, based on the satisfactory 5 year results of the latter [Citation17]. Yet, the relocation of the sealing rings more centrally, omitting the nitinol-based fabric zone, may render the caudal unsupported fabric segment prone to significant kinking in AAA with marked infrarenal angulation, especially if the orientation and apposition of the sealing rings is affected by the axis of the long suprarenal stent in marked suprarenal angles [Citation18]. Therefore, additional caution may be needed when treating AAA of short and angulated necks with Alto.
While leakage of the injected polymer in the Ovation endograft outside the filling channels has been rarely reported and implicated in anaphylactic reactions ranging from transient hypotension response to cardiovascular collapse, this was stent-graft damage incurred during the loading process in the 29 mm Ovation aortic body earlier, fabricated within a specific time period [Citation19,Citation20]. Manufacturing measurements were taken and the FDA closed the action in December 2014 [Citation21].
Since the great challenge is to widen successfully the range of AAA anatomies amenable to EVAR with Alto, strict adherence to the IFU is needed. As presented and discussed above, the limits of neck thrombus, the issues of neck shape and calcification as well as proper deployment should be considered with caution and respect; The Alto device should be chosen if the planning surgeon is absolutely sure and has studied thoroughly the AAA anatomy; in other words, if there are any doubts, we suggest choice of a different device!
4. Expert opinion
The Ovation Alto design is a promising modification that is expected to expand the eligibility of short- or conical necked AAA to endovascular treatment. Mid- and long-term results are awaited to assess the clinical performance of this new modification in the challenging necks and address any issues associated with the absence of the nitinol-containing zone seen in the previous design. Apart from proximal parallel neck length ≥7 mm with angulation ≤60°, other challenging anatomical characteristics such as the conical morphology and the wide diameter ≥28 mm are to be addressed with the new improvement of the polymer-based sealing philosophy. The maintenance of sealing of the rings against the thrombus of infarenal neck utilizing minimal radial force will be a concept that can evolve the management of challenging AAA when no other option is feasible.
Admittedly, in real-world practice many experience a rather relatively lower uptake of the Ovation platform reserving it for AAA cases ineligible for other endografts. Likewise, many physicians insist on expensive and complex fenestrated or chimney procedures where Alto could theoretically likely perform sufficiently, e.g. instead of complex procedures just for a short neck. Furthermore, from an academic standpoint, the consideration for a randomized controlled trial to compare fenestrated interventions versus Alto in selected complex AAA cases could be of value. Still, we believe that cautious use in experienced hands may revolutionize the treatment of very challenging anatomies such as in juxtarenal AAA in carefully selected patients.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Additional information
Funding
References
- Trellopoulos G, Georgakarakos E, Pelekas D, et al. Initial single-center experience with the Ovation stent-graft system in the treatment of abdominal aortic aneurysms: application to challenging iliac access anatomies. Ann Vasc Surg. 2015;29(5):913–919.
- Morgan-Bates K, and Chaudhuri A. Use of the Ovation endograft system to treat abdominal aortic aneurysms with hostile anatomy. Eur J Vasc Endovasc Surg. 2020;60(5):786–787.
- Greaves NS, Moore A, and Seriki D, et al. Outcomes of endovascular aneurysm repair using the ovation stent graft system in adverse anatomy. Eur J Vasc Endovasc Surg. 2018;55(4):512–517
- Gregory M, Metcalfe M, Steiner K. Profile of the Ovation ALTO abdominal stent graft for the treatment of abdominal aortic aneurysms: overview of its safety and efficacy. Expert Rev Med Devices. 2021;18(12):1145–1153.
- Holden A, Lyden S. Initial experience with polymer endovascular aneurysm repair using the Alto stent graft. J Vasc Surg Cases Innov Tech. 2020;6(1):6–11.
- de Donato G, Pasqui E, Panzano C, et al. Early experience with the new ovation alto stent graft in endovascular abdominal aortic aneurysm repair. EJVES Vasc Forum. 2021; 54: 7–12.
- Schoretsanitis N, Georgakarakos E, Argyriou C, et al. A critical appraisal of endovascular stent-grafts in the management of abdominal aortic aneurysms. Radiol Med. 2017;122(4):309–318.
- Pitoulias GA, Valdivia AR, Hahtapornsawan S, et al. Conical neck is strongly associated with proximal failure in standard endovascular aneurysm repair. J Vasc Surg. 2017;66(6):1686–1695.
- Oliveira NFG, Bastos Gonçalves FM, Van Rijn MJ, et al. Standard endovascular aneurysm repair in patients with wide infrarenal aneurysm necks is associated with increased risk of adverse events. J Vasc Surg. 2017;65(6):1608–1616.
- McFarland G, Tran K, Virgin-Downey W, et al. Infrarenal endovascular aneurysm repair with large device (34- to 36-mm) diameters is associated with higher risk of proximal fixation failure. J Vasc Surg. 2019;69(2):385–393.
- Kouvelos GN, Spanos K, and Nana P, et al. Large diameter (≥29 mm) proximal aortic necks are associated with increased complication rates after endovascular repair for abdominal aortic aneurysm. Ann Vasc Surg. 2019;60:70–75 .
- Kouvelos GN, Antoniou G, Spanos K, et al. Endovascular aneurysm repair in patients with a wide proximal aortic neck: a systematic review and meta-analysis of comparative studies. J Cardiovasc Surg (Torino). 2019;60(2):167–174.
- Stark M, Suresh A, Alexander J, et al. An analysis of variables affecting aortic neck length with implications for fenestrated endovascular repair of abdominal aortic aneurysm. Ann Vasc Surg. 2014;28(4):808–815.
- Gasser TC, Görgülü G, Folkesson M, et al. Failure properties of intraluminal thrombus in abdominal aortic aneurysm under static and pulsating mechanical loads. J Vasc Surg. 2008;48(1):179–188.
- Georgakarakos E, Koutsoumpelis A, Tasopoulou KM, et al. Tips to ensure optimal ring apposition of the ovation stent graft in challenging necks of abdominal aortic aneurysms. Aorta (Stamford). 2019;7(2):67–69.
- Wanhainen A, Verzini F, Van Herzeele I, et al. European society for vascular surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019;57(1):8–93.
- Georgakarakos E, Papatheodorou N, and Argyriou C, et al. An update on the ovation abdominal stent graft for the treatment of abdominal aortic aneurysms: current evidence and future perspectives. Expert Rev Med Devices. 2020;17(12):1249–1256 .
- Georgakarakos E, Ioannou CV, Trellopoulos G, et al. Immediate change in suprarenal neck angulation after endovascular aneurysm repair: comparison of the ovation stent-graft inflatable sealing rings to a conventional self-expanding stent-graft. J Endovasc Ther. 2015;22(4):613–619.
- Siani A, Accrocca F, De Vivo G, et al. anaphylactic reaction during implantation of ovation abdominal stent graft in patients with abdominal aortic aneurysm. Ann Vasc Surg. 2017;39:289.e1–289.e4.
- Sfyroeras GS, Moulakakis KG, and Antonopoulos CN, et al. Anaphylactic reaction during implantation of the ovation stent-graft system in a patient with abdominal aortic aneurysm. J Endovasc Ther. 2015 Aug;22(4):620–622.
- Koutsoumpelis A, Georgakarakos E, Tasopoulou KM, et al. A clinical update on the mid-term clinical performance of the Ovation endograft. Expert Rev Med Devices. 2019;16(1):57–62.