
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Background: Resilience is discussed to constitute a protective buffer against stress, thus fostering health. Methods: This study aimed to assess resilience both via traditional questionnaire and in everyday life on a momentary basis, and to relate these measures to autonomic functioning (heart rate variability, HRV) in 38 male firefighters during a weekday. Stressful operations, non-stressful operations and routine work at the firestation were coded during 24 hours. Momentary negative affect, feelings of resilience, and HRV were recorded via ecological momentary assessment. Findings: Questionnaire-assessed resilience was significantly positively associated with aggregated momentary resilience (r = .58, p < .001), but unrelated to HRV. However, controlling for multiple confounders (e.g., age, smoking, bodily movement, waist-to-height ratio) momentary resilience was associated with attenuated HRV and lower negative affect during stressful encounters only. Discussion: The findings suggest that momentary feelings of resilience are accompanied by vagal withdrawal to stress, possibly indicating psychological flexibility and adaptive responding to stress.
Resilience seems to be key to a healthy life (e.g., Bonanno, Citation2004). Although research is far from a unified theoretical framework of resilience, recent theorizing suggests that resilience results from a dynamic process of adaptation and must not be considered a stable personality trait (Kalisch et al., Citation2017; Rutten et al., Citation2013). Hence, resilience manifests as successful adaptation following episodes of severe stress, thus constituting a buffer for health.
However, the pathways linking resilience with health are not well understood. Besides behavioral adjustments psychobiological mechanisms are likely (e.g., Oken, Chamine, & Wakeland, Citation2015). In search for psychobiological correlates of resilience, Walker, Pfingst, Carnevali, Sgoifo, and Nalivaiko (Citation2017) identified heart rate variability (HRV), the immune system, cardiovascular recovery, and Dehydroepiandrosterone (DHEA), among others, as promising candidates. Importantly, these authors proposed that both baseline activity and stress responses are equally important for understanding the health-protective effects of resilience. Noteworthy, both basal resting levels and rapid responses to challenging encounters together with an efficient shut-off of responses after stressor termination has been suggested to characterize an adaptive system fostering health (e.g., Dienstbier, Citation1989). Recent theorizing suggests that the ability of the organism to flexibly switch from restorative function to immediate action and vice versa (so-called allostasis; McEwen, Citation1998) constitutes a marker of a healthy organism. Importantly, sensitively attending to various contexts, flexibly selecting an appropriate regulatory strategy, and monitoring and potentially modifying a strategy as needed, is considered highly adaptive and corresponds with flexible adjustment in times of severe stress as proposed by recent theories of resilience (Bonanno & Burton, Citation2013). Of note, psychological flexibility implying rapid and flexible responding to changing environmental circumstances has been discussed as a health protective feature in human development in general (e.g., Kashdan & Rottenberg, Citation2010).
In line with this reasoning, the polyvagal theory (Porges, Citation2007) and the theory of neurovisceral integration (Thayer & Lane, Citation2009) emphasize the capability of the organism to prepare for action within milliseconds via the fast myelinated vagus nerve, without necessitating the innervation of the slower acting sympathetic branch of the autonomic nervous system, thus ensuring rapid adaptation. HRV is particularly well-suited to assess vagal activity both during rest and stressful periods (e.g., Penttilä et al., Citation2001; Shaffer, McCraty, & Zerr, Citation2014). Together a reduced basal HRV and a flattened response or even vagal augmentation during challenge have been related to chronic fatigue, social phobia, depressive and aggressive symptoms, thus signaling a maladaptive response pattern (Paret, Bailey, Roche, Bureau, & Moran, Citation2015; Rottenberg, Clift, Bolden, & Salomon, Citation2007; Scott & Weems, Citation2014; Yaroslavsky, Bylsma, Rottenberg, & Kovacs, Citation2013). On the contrary, an elevated vagal tone during rest together with a rapid reduction during stress (so-called vagal withdrawal) seems to be associated with a more flexible attention regulation to threat (e.g., Park & Thayer, Citation2014; Schwerdtfeger & Derakshan, Citation2010) and has been discussed to be particularly adaptive and health-protective (e.g., Gentzler, Santucci, Kovacs, & Fox, Citation2009; Muhtadie, Koslov, Akinola, & Mendes, Citation2015; Porges, Citation2007; Stange, Hamilton, Fresco, & Alloy, Citation2017). Recently, Schwerdtfeger and Gerteis (Citation2014) could show that within-person fluctuations in positive affect were accompanied by momentary changes in HRV such that positive activated affect (i.e., feeling dynamic, awake and interested) predicted HRV decrease, thus possibly preparing the individual for action. In a similar vein, Spangler (Citation1997) could show that resilience in students was accompanied by a more flexible vagal control during an oral exam as indexed by a rapid HRV reduction during stress together with a rapid recovery, thus substantiating the assumption of a more adaptive stress-related adjustment in resilient individuals.
This study aimed to analyze psychophysiological concomitants of resilience (in particular, HRV) in everyday life using traditional questionnaire and ecological momentary assessment (EMA) in a sample exposed to a potentially stressful work environment (firefighters). Grounding on the framework of psychological flexibility as a foundation of resilience it was hypothesized that resilience would be associated with a stronger reduction in HRV during stressful periods in daily life. We aimed to analyze both questionnaire assessed resilience as a trait variable and momentary assessed feelings of resilience as a more dynamic measure of within-person psychological flexibility.
Methods
Participants
The study sample comprised of 43 male firefighters in a metropolitan area in Germany. They had a mean age of 32.71 years (SD = 6.90) and a mean waist-to-height ratio (WHtR) of 0.49 (SD = 0.04). The majority of the sample (89%) was married or cohabiting. There were 9 smokers (24%) and 50% of the sample reported habitual physical exercise (at least 3–4 times/week). Work experience (seniority) varied between 1 and 29 years (M = 8.71 years, SD = 6.83). About half of the sample (53%) was appointed to fire safety service and 47% to emergency rescue service. Exclusion criteria were use of cardioactive or other medication and self-reported psychological disorders.
Study Design
The study was approved by the local ethics committee. An EMA design was applied with parallel recording of cardiac (via physiological data recorders) and psychological variables (via smartphone app) throughout one weekday (24 hours). For sampling psychological and contextual variables in daily life, the app-software movisensXS (movisens, Karlsruhe, Germany) was used. Prompts were given signal-contingent about every 60 minutes with a random component of 30 minutes. On average, each participant answered 16 prompts across the 24 hours (623 prompts in total). If individuals were unable to answer a given prompt, they were instructed to postpone their answer by self-initializing the EMA when appropriate (10.16% of the cases). Moreover, they could also self-initialize a prompt whenever they felt necessary. Overall, 38% of the prompts were self-initialized. Work episodes were coded with each prompt as either covering routine work at the firestation (period 1; 66% of the prompts), low-stressful routine operations (period 2; 17% of the prompts) or high-stressful emergency operations (period 3; 12% of the prompts). There were 199 operations in total (M = 5.24 per participant) of which 40% were coded as highly stressful. In order to define a standard baseline, each participant worked on questionnaires for 10 minutes, during which cardiac activity was recorded to obtain a basal reference (period 0, baseline).
Variables and Instruments
Sociodemographic variables
Self-reported habitual physical exercise was assessed by asking participants how often per week they engaged in physical exercise of at least 30 minutes. Answers were given on a categorical scale with the options ‘daily’, ‘more than 4 times’, ‘3–4 times’, ‘2–3 times’, ‘1–2 times’ and ‘never’. Answers were dichotomized prior to analysis at 3 to 4 times per week or more often (1) or less (0). Participants were also asked whether they smoke (0 = no, 1 = yes), whether they use prescribed drugs for physical or mental disorders (0 = no, 1 = yes), and whether they suffer from any chronic psychological or physical disease. Waist circumference and height were measured via an elastic centimeter belt by the experimenter and WHtR was calculated.
Resilience
Resilience was assessed via traditional questionnaire (resilience scale, RS-25; (Wagnild & Young, Citation1993) and on a momentary basis using 4 items adapted from the resilience scale. Questionnaire assessed resilience showed good reliability (Cronbach’s alpha = .91), which was comparable to the original publication (Cronbach’s alpha = .94; Wagnild & Young, Citation1993). Items reflecting momentary feelings of resilience in daily life were adapted in order to account for momentary appropriateness irrespective of the context. Moreover, due to the repeated assessment throughout a weekday we aimed for a brief measure reflecting a comparably broad coverage of the original scale. The following items were answered on 7-point Likert scales between the poles 1 (‘not at all’) and 7 (‘very much so’): ‘I am determined’, ‘I am cheerful’, ‘I am content’, ‘I am interested in the things I am doing’. The mean score across participants and occasions was M = 5.16 (SD = 1.19), thus indicating rather elevated levels of momentary feelings of resilience. Reliability of this measure is reported in the Results section.
Negative affect (NA)
NA was assessed on a momentary basis using 5 items, which were taken out of the positive and negative affect schedule (PANAS; Watson, Clark, & Tellegen, Citation1988). Response format was the same like for momentary feelings of resilience. The following items were selected: ‘I am upset’, ‘I feel distressed’, ‘I feel agitated’, ‘I feel tense’, ‘I am nervous’. The mean score across participants and situations was M = 1.41 (SD = 0.55), thus indicating rather low levels of NA.
Momentary smoking
In order to control for the effects of momentary smoking on cardiac activity (see, Karakaya et al., Citation2007; Schwerdtfeger & Gerteis, Citation2014), smokers were repeatedly asked whether they smoked in a given situation (no = 0, 1 = yes).
Cardiac activity
An electrocardiogram (ECG) was recorded continuously throughout the 24 hours via physiological ambulatory monitoring devices (EcgMove3, movisens GmbH, Karlsruhe, Germany). The device is small (62.3 mm x 38.6 mm x 11.5 mm), lightweight (26 gr) and easy to use. The ECG was sampled with 12 bit resolution, stored with 1024 Hz and analyzed offline via software (DataAnalyzer, movisens GmbH, Karlsruhe, Germany). Segments with artefacts were discarded (2% of all segments). In order to account for metabolic-related changes in HRV, bodily movement was recorded with 64 Hz via an integrated 3-dimensional accelerosensor. In combination with an integrated pressure sensor, activity energy expenditure (AEE) in kcal can be reliably calculated and served as a covariate.
HRV was analyzed using established time domain (RMSSD, SDNN) and frequency domain measures (absolute power in the low frequency [LF, 0.04 – 0.15 Hz] and high frequency range [HF, 0.15 – 0.4 Hz]), according to published guidelines (Berntson et al., Citation1997; Laborde, Mosley, & Thayer, Citation2017; Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology, Citation1996). Frequency-domain measures were calculated using Fast Fourier Transform (FFT) after resampling the RR intervals with 4 Hz and detrending. RMSSD and HF reflect short-term, respiratory changes in cardiac activity, presumably indicating vagal efference. SDNN and LF are more sensitive to long-term adjustments within the autonomic nervous system reflecting both vagal and sympathetic function (Laborde et al., Citation2017; Shaffer et al., Citation2014; Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology, Citation1996). Due to the skewed distribution of the HRV measures, they were log-transformed prior to analyses.
Data Parametrization and Analysis
Each prompt was paired with a 6-minute segment of HRV, antecedent to each prompt. In order to assess reliability of momentary resilience and NA, Generalizability Theory (GT) was applied (Brennan, Citation2001; for a review see, Shrout & Lane, Citation2012). Both within-person (RKR) and between-person (RC) reliabilities were calculated in accordance with Shrout and Lane (Citation2012).
Bayesian multilevel modeling was applied to predict HRV in daily life using the statistical program R (version 3.4.2; R Development Core Team, Citation2017) and the package brms (version 2.1.0; Bürkner, Citation2017). We decided for Bayesian statistics instead of the commonly applied frequentist approach, because of the moderate sample size and our a priori assumption that stressful episodes in daily life should be accompanied by a comparably strong reduction in HRV. Accordingly, a normal prior for stressful episode was specified with a mean of −0.3 and a variance of 0.3. Furthermore, assumptions about the psychophysiological correlates of psychological flexibility led us to conclude that resilience should be accompanied by a vagal withdrawal to stress, which is considered particularly adaptive. However, we were hesitant to specify other, more informative priors for the resilience by stress period interaction due to a lack of previous research. Although we regard a Bayesian approach within this study as appropriate, it should be noted that analyses were also conducted using a frequentist approach (linear mixed effects modeling; package nlme [version 3.1–131.1; Pinheiro, Bates, DebRoy, & R Core Team, Citation2018]), which confirmed the Bayesian findings (data available upon request). Age, WHtR, physical exercise, and RS-25 (all grand mean centered) were entered as level 2 fixed effects. Bodily movement (AAE, divided by 1000 to facilitate interpretability of effect estimates), current smoking, NA, and momentary feelings of resilience (all mean centered) were entered as level 1 predictors. Moreover, period (period 1: work within the firestation; period 2: low stressful operations; period 3: highly stressful operations) was included with baseline set as reference. Interactions between resilience and period served as the effects of interest. Of note, random slopes for period were specified for each participant.
Due to the unevenly spaced prompts, a continuous autoregressive error structure was specified. Samples were derived by Markov Chain Monte Carlo (MCMC) algorithm, 4 chains with 5,000 iterations (5000 warm-up samples for each chain) and 10,000 samples were used. Hypothesis tests were applied for the interaction of momentary resilience and stressful operations (period 3). Unstandardized effect estimates (b), 95% credible intervals (CI), and the potential scale reduction factor on split chains (Rhat) are reported. For Rhat, values close to 1 indicate that the number of iterations was sufficient and chains converged. Finally, the Bayes factor was calculated for the interaction between momentary resilience and period in order to estimate whether the effect was more likely under H1 as compared to its alternative. In particular, the Bayes factor is the evidence ratio of a posterior probability under the hypothesis against its alternative (i.e., the relationship is more likely to be negative than positive). According to Jeffreys (Citation1961) a Bayes factor between 10 and 30 corresponds to a strong evidence in favor of H1 and a Bayes factor between 30 and 100 corresponds to a very strong evidence.
Overall, 5 participants were excluded from analysis due to withdrawal from participation (n = 2), technical failure (n = 1), and excessive artefacts (n = 2), thus leaving a total von 38 participants for analysis.
Results
Preliminary Analyses
GT analyses revealed that both momentary resilience and NA could be assessed with sufficient reliability (). Specifically, between-person reliability was very good for momentary resilience (RKR = .95) and NA (RKR = .95). Moreover, within-person changes across occasions showed satisfactory reliability for both momentary resilience (RC = .74) and NA (RC = .78). In order to examine validity of momentary resilience, an aggregate score was calculated for each individual, which was correlated with the RS-25. The corresponding Pearson correlation was r = .58 (p < .01), thus suggesting a large effect with considerable overlap between measures.
Table 1. Variance decomposition of resilience and negative affect items and summary estimates of reliability.
Predicting RMSSD and HF-HRV by Momentary Feelings of Resilience
Of note, the RS-25 was unrelated to HRV and there were no Period by RS-25 interactions for neither HRV variable (data available upon request). Hence, for reasons of parsimony and in order not to over-specify the models, RS-25 was excluded from further analyses. It should be noted though, that findings were virtually unchanged when RS-25 was included as an additional predictor.
The findings for RMSSD are depicted in (random effects) and (fixed effects). Bayesian multilevel modeling revealed that period 3 was associated with lower RMSSD as compared to baseline (b = −0.23, lower CI = −0.39, upper CI = −0.08), thus documenting vagal withdrawal to stressful operations. Moreover, a negative association could be observed between momentary feelings of resilience and RMSSD during period 3 relative to the baseline (b = −0.14, lower CI = −0.30, upper CI = 0.01), suggesting that RMSSD during stressful operations was lower when momentary feelings of resilience were higher (). A hypothesis test revealed that the likelihood for lower RMSSD with higher feelings of momentary resilience is about 32 times more likely under H1 than given a positive relationship (evidence ratio: 31.79; b = −0.14, SE = 0.08, lower CI = – Inf., upper CI = −0.02). In accordance with (Jeffreys, Citation1961) the evidence in favor of H1 may be considered very strong. Of note, the relationship with momentary resilience was not robust during other periods (see ). Furthermore, the higher momentary AAE the lower RMSSD was (b = −0.10, lower CI = −0.13, upper CI = −0.07), and age was negatively related with RMSSD (b = −0.03, lower CI = −0.05; upper CI = −0.02).
Figure 1. Slopes and corresponding credibility intervals between momentary resilience and lnRMSSD (top) and lnSDNN (bottom) for each period (baseline (left), stressful operations (right)).
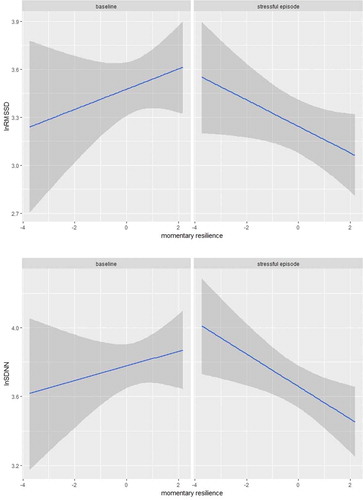
Table 2. Bayesian multilevel model predicting lnRMSSD: random effects.
Table 3. Bayesian multilevel model predicting lnRMSSD: fixed effects.
Importantly, analysis of HF-HRV revealed similar findings. Specifically, AAE was associated with lower HF-HRV (b = −0.18, lower CI = −0.24, upper CI = −0.12) and age was also negatively associated with HF-HRV (b = −0.08, lower CI = −0.12, upper CI = −0.03). Of note, HF-HRV substantially decreased in response to period 3 (b = −0.28, lower CI = −0.56, upper CI = −0.01), thus complementing the finding for RMSSD. Again, the interaction between momentary feelings of resilience and stressful episodes appeared reliable (b = −0.33, lower CI = −0.64, upper CI = −0.01). The Bayes factor suggested that the finding was 47 times more likely under H1 than under its alternative (b = −0.33, SE = 0.16, lower CI = -Inf., upper CI = −0.07), thus indicating a very strong evidence in favor of H1. Together, the findings for RMSSD and HF-HRV suggest that momentary feelings of resilience were accompanied by a stronger vagal withdrawal during highly stressful operations.
Predicting SDNN and LF-HRV by Momentary Feelings of Resilience
Analyses of SDNN and LF-HRV largely substantiated the findings on RMSSD and HF-HRV. (random effects) and (fixed effects) depict the findings for SDNN in more detail. Of note, the interaction of momentary feelings of resilience and stressful episodes relative to baseline revealed a negative effect (b = −0.14, lower CI = −0.26, upper CI = −0.01), indicating that this findings was 53.5 times more likely under H1 (b = −0.14, SE = 0.06, lower CI = Inf., upper CI = −0.03). According to Jeffreys (Citation1961) this effect might be considered very strong. The interaction is visualized in ). Some other predictors could be identified. As in the previous analyses, AAE (b = −0.07, lower CI = −0.10, upper CI = −0.05) and age (b = −0.03, lower CI = −0.04, upper CI = −0.01) were negatively associated with SDNN.
Table 4. Bayesian multilevel model predicting lnSDNN: random effects.
Table 5. Bayesian multilevel model predicting lnSDNN: fixed effects.
The findings for LF-HRV were comparable. Specifically, both bodily movement (AAE; b = −0.11, SE = 0.03, lower CI = −0.16, upper CI = −0.06) and increasing age (b = −0.05, SE = 0.01, lower CI = −0.08, upper CI = −0.02) were associated with lower LF-HRV, and momentary smoking predicted higher LF-HRV (b = 0.26, SE = 0.13, lower CI = 0.01, upper CI = 0.52). Importantly, there was an interaction between momentary resilience and stressful operations relative to baseline (b = −0.26, SE = 0.13, lower CI = −0.51, upper CI = −0.001), suggesting that a lower LF-HRV together with higher momentary feelings of resilience was 36.5 times more likely under H1 (b = −0.26, SE = 0.13, lower CI = -Inf., upper CI = −0.04), which may be interpreted as a very strong evidence in favor of the hypothesis according to Jeffreys (Citation1961).
Additional Analysis
In a final step, NA instead of HRV was treated as a criterion variable in order to examine whether momentary feelings of resilience were associated with psychological function during stress. The predictors of the previous models were entered as specified above. In short, stressful operations were accompanied by elevated NA (b = 0.21, SE = 0.09, lower CI = 0.02, upper CI = 0.39). Momentary resilience was unrelated to NA, however, there was a significant interaction with period 3 relative to baseline (b = −0.18, SE = 0.09, lower CI = −0.35, upper CI = −0.01), indicating that momentary feelings of resilience were associated with lower NA during stressful operations. The evidence ratio was 42.4 in favor of the hypothesis of reduced stress-related NA with increasing resilience, thus suggesting very strong evidence. There were no reliable interactions with the other periods. Hence, the findings on NA seemed to complement the findings on HRV, thus documenting that momentary resilience covaried with psychophysiological adjustment during severely stressful episodes only as evidenced by lower HRV and lower NA.
Discussion
The aim of this study was to examine associations between questionnaire-assessed and momentary assessed resilience on the one hand and HRV on the other hand, in a highly demanding work environment. Specifically, we expected a more flexible responding to stressful periods when resilience was high. In accordance with recent guidelines we calculated time domain and frequency domain measures of HRV (Laborde et al., Citation2017) in order to get a more comprehensive view on the robustness of the data. As expected, stressful episodes predicted stronger reductions in both RMSSD and HF-HRV and an increase in NA, suggesting that we succeeded in capturing stressful operations within the sample. Importantly, questionnaire-assessed resilience was unrelated to HRV, while momentary feelings of resilience predicted stronger HRV reductions during stressful operations only. Of note, this finding was substantiated by different HRV variables and comprised indicators of vagal function (HF-HRV and RMSSD) as well as indicators sensitive to both sympathetic and vagal efference (LF-HRV, SDNN). According to common suggestions, this evidence could be considered strong or even very strong.
Importantly, additional analysis for NA complemented the findings on HRV. Momentary resilience was also related with lower NA during stressful operations, which is in line with the protective psychological function associated with resilience (e.g., Bonanno, Citation2004). This result further substantiates the assumption that HRV reductions to stress do not signal maladjustment or exaggerated stress responses, but must be considered an adaptive, flexible responding to challenging environmental demands (e.g. Gentzler et al., Citation2009; Spangler, Citation1997; Thayer & Lane, Citation2009). In line with Schwerdtfeger and Gerteis (Citation2014) we would interpret this response pattern as signaling behavioral approach via metabolic adjustment (i.e., preparing the individual for action). Thus, this finding is in line with the assumption that resilience involves approach motivation (e.g., Spangler & Friedman, Citation2015) and is related with a more flexible adaptation to stress (Spangler, Citation1997). It should be noted that lower HRV as found during stressful operations in this study has been associated with morbidity and mortality in previous research (e.g., Dekker et al., Citation2000; Hillebrand et al., Citation2013; Singh et al., Citation1998; Zulfiqar, Jurivich, Gao, & Singer, Citation2010), thus challenging the positive interpretation in terms of higher flexibility. However, this evidence stems from studies examining interindividual associations derived from recordings during rest or across 24 hours, thus relating dispositional differences in HRV to outcome variables. Contrary to that, our approach was to evaluate within-person trajectories relative to a baseline. Importantly, inferences from within-person to between-person correlations and vice versa (so-called ergodicity) are dependent upon certain conditions (e.g., identical means, variances and covariances within the population and within the individual), which are rarely met in psychological studies (e.g., Hamaker, Citation2012). Hence, associations between dispositional measures of resilience and HRV could be positive and not negative. For example, divergent findings for between-person and within-person associations between positive affect and HRV have been demonstrated by Schwerdtfeger and Gerteis (Citation2014).
It should be emphasized that this study found no effect regarding between-person associations of resilience and HRV. Noteworthy, a recent narrative review suggest evidence for a positive relationship between resilience and resting HRV (Carnevali, Koenig, Sgoifo, & Ottaviani, Citation2018). This lack of association might be attributed to either the comparably small sample size with a lack of statistical power to detect moderate associations or to validity concerns. Although previous research seemed to agree that resilience could be assessed with sufficient validity as a dispositional variable (e.g., Chmitorz et al., Citation2018; Windle, Bennett, & Noyes, Citation2011), the trait-approach has been challenged recently (Kalisch et al., Citation2017). Moreover, it should be noted that resilience was generally high and homogeneous in this sample, thus leading to lower effect estimates due to restricted between-person variance. Certainly, more research is warranted in order to examine within-person and between-person associations of resilience and psychophysiological stress reactivity in more detail.
Limitations
The current findings need to be discussed in light of some limitations. First, the sample size was rather moderate, thus calling for replication studies. Relatedly, it should be emphasized that due to a male only sample generalizability to women needs further research. Second, due to environmental constraints and personal involvement during highly demanding operations, prompts within highly stressful operations could often not be answered timely, but rather delayed. Hence, the time-frame of 6 minutes prior to each prompt might be considered too short to capture peak stress. Unfortunately, we did not assess the time delay between self-initialized prompts and the stressful operations. However, it should be noted that vagally mediated HRV reductions and NA elevation during stressful episodes were evident and support the validity of this approach. Third, due to the restricted recording period (one day only), findings might not generalize to other days. Hence, future research should aim for extended recording periods across 3 to 4 days to ensure reliability and contextual diversity. Fourth, it would be reasonable to assume that in accordance with a person-by-situation fit model both state and trait variables could interact to predict psychophysiological stress responding. In particular, momentary resilience might be more strongly associated with psychophysiological stress responses when trait resilience is high as well. Due to a lack of power, the current study did not analyze cross-level interactions. Therefore, we would recommend to examine trait-state interactions in future large scale research. Finally, it should be emphasized that this study followed a correlational design, thus precluding causal interpretations. Although the rationale of this study suggests that the physiological stress response constitutes a consequence or marker of psychological beliefs and attitudes, it could also be assumed that psychological states follow physiological function. Specifically, Bandura (Citation1977) identified emotional/physiological arousal as a source for anxiety and self-efficacy beliefs. Likewise, reductions in HRV could inform the individual about challenging physiological states, thus calling for psychological adjustments. Furthermore, hidden third variables (e.g., genes, personality characteristics) could have driven the association between momentary resilience and HRV. Certainly, more research is needed to elucidate the directionality of this effect.
Conclusion
Notwithstanding the above mentioned limitations, the findings of this study document that momentary feelings of resilience are accompanied by reductions in HRV and NA to highly stressful operations in daily life in firefighters, thus providing evidence for a dynamic, flexibility-related approach toward resilience. This result corroborates studies suggesting that the ability to rapidly withdraw vagal efference and thus, prepare the organism for action is an adaptive response to stress, potentially protecting physical health.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215.
- Berntson, G. G., Bigger, J. T., Eckberg, D. L., Grossman, P., Kaufmann, P. G., Malik, M., & Van Der Molen, M. W. (1997). Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology, 34(6), 623–648.
- Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events?. The American Psychologist, 59(1), 20–28.
- Bonanno, G. A., & Burton, C. L. (2013). Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspectives on Psychological Science, 8(6), 591–612.
- Brennan, R. L. (2001). Generalizability theory. New York, NY: Springer. doi:10.1007/978-1-4757-3456-0
- Bürkner, P.-C. (2017). brms: An {R} Package for Bayesian multilevel models. Journal of Statistical Software, 80(1), 1–28.
- Carnevali, L., Koenig, J., Sgoifo, A., & Ottaviani, C. (2018). Autonomic and brain morphological predictors of stress resilience. Frontiers in Neuroscience, 12, 228.
- Chmitorz, A., Wenzel, M., Stieglitz, R.-D., Kunzler, A., Bagusat, C., Helmreich, I., … Tüscher, O. (2018). Population-based validation of a German version of the Brief Resilience Scale. PloS one, 13(2), e0192761.
- Dekker, J. M., Crow, R. S., Folsom, A. R., Hannan, P. J., Liao, D., Swenne, C. A., & Schouten, E. G. (2000). Low heart rate variability in a 2-minute rhythm strip predicts risk of coronary heart disease and mortality from several causes: the aric study. atherosclerosis risk in communities. Circulation, 102(11), 1239–1244.
- Dienstbier, R. A. (1989). Arousal and physiological toughness: Implications for mental and physical health. Psychological Review, 96(1), 84–100.
- Gentzler, A. L., Santucci, A. K., Kovacs, M., & Fox, N. A. (2009). Respiratory sinus arrhythmia reactivity predicts emotion regulation and depressive symptoms in at-risk and control children. Biological Psychology, 82(2), 156–163.
- Hamaker, E. L. (2012). Why researchers should think “within-person”: A paradigmatic rationale. In M. R. Mehl & T. S. Conner (Eds.), Handbook of research methods for studying daily life (pp. 43–61). London: The Guilford Press.
- Hillebrand, S., Gast, K. B., Mutsert, R. D., Swenne, C. A., Jukema, J. W., Middeldorp, S., & Dekkers, O. M. (2013). Heart rate variability and first cardiovascular event in populations without known cardiovascular disease: Meta-analysis and dose-response meta-regression. Europace, 15(5), 742–749.
- Jeffreys, H. (1961). Theory of probability (3rd ed. ed.). Oxford, UK: Oxford University Press.
- Kalisch, R., Baker, D. G., Basten, U., Boks, M. P., Bonanno, G. A., Brummelman, E., … Kleim, B. (2017). The resilience framework as a strategy to combat stress-related disorders. Nature Human Behaviour, 1(11), 784–790.
- Karakaya, O., Barutcu, I., Kaya, D., Esen, A. M., Saglam, M., Melek, M., … Kaymaz, C. (2007). Acute effect of cigarette smoking on heart rate variability. Angiology, 58(5), 620–624.
- Kashdan, T. B., & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30(7), 865–878.
- Laborde, S., Mosley, E., & Thayer, J. F. (2017). Heart rate variability and cardiac vagal tone in psychophysiological research - Recommendations for experiment planning, data analysis, and data reporting. Frontiers in Psychology, 8, 213.
- McEwen, B. S. (1998, Jan 15). Protective and damaging effects of stress mediators. New England Journal of Medicine, 338(3), 171–179.
- Muhtadie, L., Koslov, K., Akinola, M., & Mendes, W. B. (2015). Vagal flexibility: A physiological predictor of social sensitivity. Journal of Personality and Social Psychology, 109(1), 106–120.
- Oken, B. S., Chamine, I., & Wakeland, W. (2015). A systems approach to stress, stressors and resilience in humans. Behavioural Brain Research, 282, 144–154.
- Paret, L., Bailey, H. N., Roche, J., Bureau, J.-F., & Moran, G. (2015). Preschool ambivalent attachment associated with a lack of vagal withdrawal in response to stress. Attachment & Human Development, 17(1), 65–82.
- Park, G., & Thayer, J. F. (2014). From the heart to the mind: Cardiac vagal tone modulates top-down and bottom-up visual perception and attention to emotional stimuli. Frontiers in Psychology, 5, 278.
- Penttilä, J., Helminen, A., Jartti, T., Kuusela, T., Huikuri, H. V., Tulppo, M. P., … Scheinin, H. (2001). Time domain, geometrical and frequency domain analysis of cardiac vagal outflow: Effects of various respiratory patterns. Clinical Physiology, 21(3), 365–376.
- Pinheiro, J., Bates, D., DebRoy, S., & R Core Team. (2018). nlme: Linear and Nonlinear Mixed Effects Models. R package version 3.1-137. Retrieved from https://CRAN.R-project.org/package=nlme.
- Porges, S. W. (2007). The polyvagal perspective. Biological Psychology, 74(2), 116–143.
- R Development Core Team. (2017). R: A language and environment for statistical computing. Vienna, Austria: the R Foundation for Statistical Computing. ISBN: 3-900051-07-0. Available online at http://www.R-project.org/.
- Rottenberg, J., Clift, A., Bolden, S., & Salomon, K. (2007). RSA fluctuation in major depressive disorder. Psychophysiology, 44(3), 450–458.
- Rutten, B. P. F., Hammels, C., Geschwind, N., Menne-Lothmann, C., Pishva, E., Schruers, K., … Wichers, M. (2013). Resilience in mental health: Linking psychological and neurobiological perspectives. Acta Psychiatrica Scandinavica, 128(1), 3–20.
- Schwerdtfeger, A., & Derakshan, N. (2010). The time line of threat processing and vagal withdrawal in response to a self-threatening stressor in cognitive avoidant copers: Evidence for vigilance-avoidance theory. Psychophysiology, 47(4), 786–795.
- Schwerdtfeger, A. R., & Gerteis, A. K. S. (2014). The manifold effects of positive affect on heart rate variability in everyday life: Distinguishing within-person and between-person associations. Health Psychology, 33(9), 1065–1073.
- Scott, B. G., & Weems, C. F. (2014). Resting vagal tone and vagal response to stress: Associations with anxiety, aggression, and perceived anxiety control among youths. Psychophysiology, 51(8), 718–727.
- Shaffer, F., McCraty, R., & Zerr, C. L. (2014). A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Frontiers in Psychology, 5, 1040.
- Shrout, P. E., & Lane, S. P. (2012). Psychometrics. In M. R. Mehl & T. S. Conner (Eds.), Handbook of research methods for studying daily life (pp. 302–320). London: The Guilford Press.
- Singh, J. P., Larson, M. G., Tsuji, H., Evans, J. C., O’Donnell, C. J., & Levy, D. (1998). Reduced heart rate variability and new-onset hypertension: Insights into pathogenesis of hypertension: The framingham heart study. Hypertension, 32(2), 293–297.
- Spangler, D. P., & Friedman, B. H. (2015). Effortful control and resiliency exhibit different patterns of cardiac autonomic control. International Journal of Psychophysiology, 96(2), 95–103.
- Spangler, G. (1997). Psychological and physiological responses during an exam and their relation to personality characteristics. Psychoneuroendocrinology, 22(6), 423–441.
- Stange, J. P., Hamilton, J. L., Fresco, D. M., & Alloy, L. B. (2017). Flexible parasympathetic responses to sadness facilitate spontaneous affect regulation. Psychophysiology, 54(7), 1054–1069.
- Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology. (1996). Heart rate variability. European Heart Journal, 17(suppl 2), 28–29.
- Thayer, J. F., & Lane, R. D. (2009). Claude Bernard and the heart-brain connection: Further elaboration of a model of neurovisceral integration. Neuroscience and Biobehavioral Reviews, 33(2), 81–88.
- Wagnild, G. M., & Young, H. M. (1993). Development and psychometric evaluation of the Resilience Scale. Journal of Nursing Measurement, 1(2), 165–178.
- Walker, F. R., Pfingst, K., Carnevali, L., Sgoifo, A., & Nalivaiko, E. (2017). In the search for integrative biomarker of resilience to psychological stress. Neuroscience and Biobehavioral Reviews, 74(Pt B), 310–320.
- Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality & Social Psychology, 54(6), 1063–1070. 2.
- Windle, G., Bennett, K. M., & Noyes, J. (2011). A methodological review of resilience measurement scales. Health and Quality of Life Outcomes, 9, 8.
- Yaroslavsky, I., Bylsma, L. M., Rottenberg, J., & Kovacs, M. (2013). Combinations of resting RSA and RSA reactivity impact maladaptive mood repair and depression symptoms. Biological Psychology, 94(2), 272–281.
- Zulfiqar, U., Jurivich, D. A., Gao, W., & Singer, D. H. (2010). Relation of high heart rate variability to healthy longevity. The American Journal of Cardiology, 105(8), 1181–1185.