
ABSTRACT
Young people’s engagement with digital health technologies is dominated by risk narratives. Yet, there are very limited understandings, from the perspectives of young people, about the health-related issues and opportunities generated by digital health technologies. This article presents new evidence on the types of health-related apps and devices young people find, select and use, and the reasons for their choices. Data were generated from a participatory mixed method design with 245 young people (age 13–18). The data were analysed using a content-led pedagogical framework. The data illustrate, vividly, young people’s agency in digital health contexts and the complexity and fluidity of young people’s decision-making. Schools, PE lessons and sport, as well as family members and peers, were powerful influencers on young people’s digital health-related knowledge and behaviours. It is argued that better understanding young people’s agency in digital health contexts offers important insights into developing effective health-related pedagogies.
Contemporary youth are spending significant proportions of their time finding, selecting and using mobile digital applications (‘apps’) (see Third et al. Citation2014, Citation2017). In line with reported improvements to access and the quality of apps in recent years (Lupton Citation2017; Ofcom Citation2017), it has been argued that young people are becoming app-dependent and are turning to apps as a preferred source of information, communication and entertainment (Beckman, Bennett, and Lockyer Citation2014; Gardner and Davis Citation2014). Evidence suggests that young people value the specific affordances of accessibility and efficiency, the immediacy of information and interaction, and the ability to access personalised information that they perceive to be tailored to their individual needs (Gardner and Davis Citation2014; Third et al. Citation2014).
There are currently over 160,000 health apps available on the major apps stores that are focused on aspects of wellness, diet and exercise (Lupton Citation2017). Health-related apps are reported to be of particular interest to young people, even though most of these are designed for adults (Wartella et al. Citation2016; Third et al. Citation2017). This interest is partially generated through young people’s extensive use of social media with its surplus of easily available information about different aspects of health (Holmberg et al. Citation2018; Third et al. Citation2017). Aligned with this interest in health-related apps is young people’s reported interest in health-related wearable devices (Wartella et al. Citation2016; Goodyear Citation2017). Wearable health-related devices – such as the Fitbit or the Nike Fuel Band – can be paired with health-related apps to monitor, track and record health-related behaviours, such as exercise, diet, sleep and water intake (Lomborg and Frandsen Citation2016). There is evidence of young people’s engagement with health-related material on the internet and social media (Wartella et al. Citation2016; Goodyear, Armour, and Wood Citation2018; Holmberg et al. Citation2018), particularly in the area of sexual health (Albury Citation2013; Robinson et al. Citation2014). Yet although these studies offer helpful insights for this research, there are few robust empirical accounts of young people’s uses of apps and wearable devices in the specific health-related areas of wellness, diet and exercise (Wartella et al. Citation2016; Radovic et al. Citation2018). For example, there are very few robust accounts of the types of wellness, diet and exercise apps and devices that young people find, select and use, or why and how they use them. As a result, we currently have limited understandings of the role of digital health technologies as a learning resource for young people in these areas.
The narratives around young people’s engagement with a whole range of digital technologies are dominated by risk (Third et al. Citation2014, Citation2017), the potential for negative impacts (Fullagar, Rich, and Francombe-Webb Citation2017; Rich and Miah Citation2017), and the large gaps that exist between the ways in which adults and young people understand, use and experience digital technologies (boyd Citation2014; McKee et al. Citation2018). Digital health technologies are a particular concern for many adults because they disrupt the flow of traditional forms of health knowledge that adults are familiar with (Rich and Miah Citation2014, Citation2017; Rettberg Citation2014). These types of technologies are spaces where commercial, government, community and individual contexts overlap (Freishtat and Sandlin Citation2010; Williamson Citation2015) and where reductionist, normative and neo-liberal constructs of health are promoted extensively (Rettberg Citation2014; Depper and Howe Citation2017). Yet, and as we have found in our research on social media (Goodyear, Armour, and Wood Citation2018), beyond a focus on sensitive topics, such as sexual health (Albury Citation2013), there is little mention in current education/childcare policies about the role of digital health technologies in young people’s lives (Rich and Miah Citation2017, Citation2014; Third et al. Citation2017) and very limited guidance on how apps and wearable devices might be adapted for use by young people (Bakker et al. Citation2016; Bevelander et al. Citation2018). In turn, relevant adults (including teachers, parents/guardians, health practitioners, policy makers) find it difficult to offer young people the guidance they need to use digital health-related technologies effectively and appropriately (Third et al. Citation2017; Radovic et al. Citation2018). Thus, it is unsurprising to find that many young people are largely unsupported in their uses of digital health technologies (Third et al. Citation2017).
This article presents new evidence on the types of health-related apps and devices young people find, select and use, and the reasons for their choices. The focus is on understanding, from the perspectives of young people, the health-related opportunities and issues generated by digital health technologies. Data were generated from a large data set drawn from 245 young people who engaged in a participatory and iterative research design. The new data offer insights into the ways in which young people use apps and wearable devices as part of the wider landscape in which they learn about health and this, in turn, challenges existing theories about pedagogy in physical activity and health settings. The research questions were: (i) What digital health apps and devices do young people use to inform their health-related understandings and behaviours? (ii) What digital health information do young people attend to/ignore and how do these choices inform their reported health understandings and behaviours?
Theoretical background: pedagogy
Across disciplines, research on digital technologies has been dominated by a focus on the medium(s) and user/participant responses to varying technological affordances (Couldry Citation2012; Miller et al. Citation2016). In turn, there is an overwhelming tendency to report on how digital health technologies are either successful or unsuccessful as behaviour change devices (Fors and Pink Citation2017). It is argued here, however, that we could usefully move away from the methodological certainty of analysing ‘positive’ and ‘negative’ effects in order to better understand the role of technology as a resource that opens up new possibilities for young people to learn about and develop their health. So, following on from Albury (Citation2013) and Fors and Pink (Citation2017), a pedagogically informed conceptual framing was adopted for this study. In so doing, our approach sought to take into account the broader contexts in which young people learn about health.
Although definitions of pedagogy vary, pedagogy is often referred to as a complex learning process that is shaped by the dynamic interaction between three dimensions: teachers/teaching, learners/learning and knowledge in context (see Armour Citation2014). In self-directed technological environments – such as apps – (Gardner and Davis Citation2014) the interaction between these three dimensions is made even more complex by the absence of a formal ‘teacher/instructor’ (Andersson and Olson Citation2014), the mobility of devices (Hillman and Säljö Citation2016), and the dynamism of digital data assemblages in which humans-devices-software-data-space-time align (Lupton Citation2017). To explain pedagogy in relation to technology, a growing body of influential work has used the concept of public pedagogies as an analytical device (Rich and Miah Citation2014). Often grounded in the works of Giroux (Citation2004), the concept of public pedagogies acknowledges learning as an experience that is influenced by culture, inclusive of the media, internet, films and television (Burdick and Sandlin Citation2013). Yet, many of the current conceptual framings of public pedagogies are grounded in its roots in passive media (Reid Citation2010; Andersson and Olson Citation2014). As a result, analytical framings tend to be dominated by a focus on audience, power, ideology and/or discourses (Rich and Miah Citation2014), that do little to move beyond simplistic ideas of behavioural change (Fors and Pink Citation2017), or acknowledge the role of the individual in shaping their educational experiences (Andersson and Olson Citation2014). Similar to the experiences of other researchers (see Andersson and Öhman Citation2017; Rich and Miah Citation2014; Fullagar, Rich, and Francombe-Webb Citation2017), we faced challenges in seeking to apply the original concept of public pedagogies to data on apps and wearable devices.
Recently, some scholars have pushed the concept of pedagogy and public pedagogies further to account for the role of the user and particularly the highly dynamic ways in which digital health technologies can be used. For example, Rich and colleagues (Fullagar, Rich, and Francombe-Webb Citation2017; Rich and Miah Citation2014, Citation2017) see public pedagogy as embodied and relational, where engagement is shaped by and shapes relations with other discourses, bodies, sites and pedagogies. Fors and Pink (Citation2017) and Lupton (Citation2018) have argued that attention should be focussed on the process of learning, and the sensorial, embodied and emplaced dimensions of engagement. Similarly, in the field of sexual health and communication studies, Albury (Citation2013) and Lomborg and Frandsen (Citation2016) stress the importance of focusing on digital practices and what users do in their engagement with digital technologies. Indeed, a consistent message from a broad range of theories – including anthropological, communication, media-based, materialist and post-structuralist – is the need to focus on the affective and lived experiences of digital health technologies. However, while advances have been made, the concepts of pedagogy and public pedagogies in relation to technology have become very broad and there is a lack of clarity on the dimensions of pedagogy that shape learning (Fullagar, Rich, and Francombe-Webb Citation2017; Savage Citation2014). We found that returning to an established definition of pedagogy in formal educational settings – as previously outlined – was helpful in developing a pedagogical analytical framing for this study.
Building on our earlier research on young people’s engagement with health-related social media (Goodyear, Armour, and Wood Citation2018), a focus on content in the context of pedagogy provided an analytical lens to interpret distinctive elements of pedagogy that shape health-related knowledge and behaviours. In our content-led framework, the pedagogical dimensions of teachers/teaching, learners/learning and knowledge in context (see Armour Citation2014) remain relevant, although they exist in different forms and configurations. Content is conceptualised as knowledge in context, and is representative of a broader topic, practice, or material that is relevant to the learner. Content is placed at the centre of the pedagogical framework (see ) and is shaped by the interplay between: (i) interactive functions (i.e., the teaching dimension, where technology has particular cognitive, social and affective potentials): and (ii) users’ interactions with the technology (i.e., the learning dimension, where learners needs, knowledge, contexts and situations shape their engagement). A focus on content therefore aligned well with our research questions, in terms of better understanding the health-related apps and devices young people find, select and use, and why and how they use them.
Figure 1. The operation of pedagogy in a digital media context (Goodyear, Armour, and Wood Citation2018).
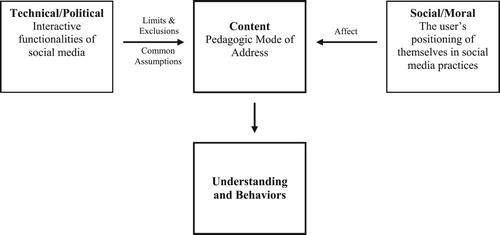
To develop the content-led framework, we drew on anthropological and communicative theories (see Miller et al. Citation2016; Lomborg Citation2017) to position content as something that users do, which seems to align with the work of Albury (Citation2013) and Lomborg and Frandsen (Citation2016) on digital practices. Lomborg (Citation2017) and Miller et al. (Citation2016) suggest that content is created through different and multiple genres (i.e., styles of use or participation). Genres are constituted at the interplay between different interactive functionalities of the software and/or the device and the social purposes that orientate individuals to particular digital practices (Lomborg Citation2017). Our focus on content, therefore, builds on conceptualisations of affordances (Lupton Citation2017, Citation2018); i.e., the technological, aesthetic and social potentials that are defined through use and formed by the needs of the user (Lomborg and Frandsen Citation2016). While the content-led framework is still a work in progress, the value of this framework is that it enables the concept of affordances to be aligned with the concept of pedagogy in order to add further insights into the dynamic ways in which learning is generated. Furthermore, given that content is formed from multiple genres (Miller et al. Citation2016), a focus on content can provide insights into broader forms of content that persist across different assemblages of technologies and contexts (Miller et al. Citation2016; Lupton Citation2017), and this focus also aligns well with the concept of relationality (Rich and Miah Citation2014) and process-based learning (Fors and Pink Citation2017). A focus on content in our preliminary framework (), therefore, bridges established (Armour Citation2014), media-based (Giroux Citation2004) and more current conceptualisations of learning (Albury Citation2013), and pedagogy (Fors and Pink Citation2017; Rich and Miah Citation2014).
Methods
A participatory and iterative research design was adopted to generate rich, in-depth and detailed insights into young people’s experiences of using health-related apps and devices. Young people were active participants in the research and a multi-method approach was used to engage with multiple and varying sample sizes of young people at different stages.
Ethics
A culturally responsive relational and reflexive approach to ethics was adopted (Sparkes and Smith Citation2014). This approach ensures that ethical decision-making is contextualised within the digital cultures and contexts inhabited by young people (Goodyear Citation2017). Following this approach (Sparkes and Smith Citation2014), care for participants involved creating and using data collection methods that ensured participant safety, privacy and dignity, and that promoted participant autonomy. University ethical approval was granted and informed consent or assent was obtained from participants. Legal conditions for apps were adhered to by using university accounts and devices, and ensuring participants were aged 13 or over.
Context and participants
Data collection took place with 245 young people (age 13–18) from 10 UK schools located in the West Midlands and the South of England. Of the 10 schools, 2 were private, 3 were state, and 5 were academies, 2 of which were faith schools.Footnote1 The schools were located in diverse socio-demographic areas and included students from a range of ethnic backgrounds, with just under a third of students across these schools speaking English as a second language.
Data collection
Data collection was framed by an initial focus on health-related apps and devices in the areas of physical activity, diet/nutrition, body image and sleep. A conceptually restricted focus on health-related content was taken to provide clarity for participants and to ensure depth in the data on the types of health-related content young people accessed and attended to.
Data collection took place over 10 months and across three iterative phases where data generated from each phase informed data collection techniques in the next phase. An overview of methods used in each of the three phases is provided in .
Table 1. Data collection methods.
The purpose of phase 1 was to create, develop and pilot the data collection methods to ensure that they were robust and practical, and were capable of generating rich data on young people’s perspectives of health-related apps and devices. This involved a group of 10 young people (age 16–18; m = 6, f = 4) who were not involved in phases 2–3. This process occurred over two months during class-based lessons. The young people supported the creation and piloting of participatory class activities to be used in phases 2–3, that included the creation of group tasks, iBook content, questionnaires and interview questions.
The purpose of phase 2 was to generate data on broad understandings from young people about the varying ways in which they use and experience health-related apps and devices. This involved 12 school classes of young people (n = 235; age 13–15; m = 100, f = 135) participating in participatory class activities () that had been piloted in phase 1. The classes were single sex (m = 3, f = 5) or mixed gender (n = 4) and data collection took place in physical education (PE) (n = 10) or citizenship lessons (n = 2). Initially, participatory class activities were led by a researcher and took place in a one-hour lesson. Data were generated from questionnaires and an app that the young people created (see ).
The purpose of phase 3 was to generate a deeper understanding of the health-related apps young people find, select and use, and the reasons for their choices. Nineteen focus group interviews (n = 83; m = 42, f = 41) were conducted. Data from the participatory class activities informed the selection of focus groups and the focus of the interview questions (see ). A combination of elicitation and semi-structured techniques were used.
Analysis
Analysis was ongoing and iterative throughout the study to facilitate data collection across the three phases. At the end of the study, analysis took place in two overarching phases and the coding processes are outlined in and .
Table 2. An illustration of the process of coding in phase 1 of analysis.
Table 3. An illustration of the process of coding in phase 1 of analysis.
Phase 1 (see ) involved organising the data in to three main data sets. First, the health apps and devices young people used or were aware of were identified. Percentages were calculated for frequencies, and the total number of apps and devices coded as ‘used’ or ‘aware of’. Second, questionnaire and interview data were coded inductively to identify different types of uses, experiences and health-related understandings and behaviours. Third, data generated from the app creation task were organised into the categories on the app creation task sheet (see ): aim; target audience; how does it work; paid or free. This categorised data set was then coded inductively.
In phase 2 () the focus of the analysis was on pedagogy, using existing theories of pedagogy and the content-led pedagogical framework previously outlined (Goodyear, Armour, and Wood Citation2018; ). The data sets from phase 1 () were interrogated in order to identify different forms of content. Consistent with the understanding that content is shaped by genres and both the technology and the individual (Miller et al. Citation2016; Lomborg Citation2017) the data sets were coded by: (i) interactive functionalities and (ii) user purposes (see ). The interplay between the interactive functionalities and the individual purposes was then examined and this process identified several genres and illustrated how the technical and user features worked together to construct content. For example, the interplay between (i) time, money, and body image (user) and (ii) short-duration exercises/diets, simplicity of information, and schedules (interactive), was associated with a genre (i.e., style of use) of information seeking. To determine the forms of content that were developed from different and multiple genres, consistent with Ito et al. (Citation2010), the genres were coded to identify different modes of relating to technologies. In particular, data were coded by: individuals’ needs (Couldry Citation2012) and institutional, cultural and social activities (Fullagar, Rich, and Francombe-Webb Citation2017; Fox and Bale Citation2017), such as school, family and peers (Rich and Miah Citation2014). The interplay between the user, the interactive functionalities and experience of using the technology was, therefore, central to our understandings of how and why young people find, select, and use health-related apps and devices. From analysing these three dimensions of content, three categories of content were selected as the main themes and will be discussed in the results section.
In all stages of the analysis, a deliberative strategy (see Goodyear, Kerner, and Quennerstedt Citation2017) was used. The goal of the deliberation was to form a collective agreement where all co-authors were given the possibility to make judgments in relation to different alternatives, views and arguments. The researchers independently constructed codes and these became the basis for deliberation. The authors’ different backgrounds and experiences together with the respectful endeavour to clarify points of agreement/disagreement are indicators of quality in a deliberative process.
Validity
A relativist approach to validity aimed to extend the robustness of traditional measures of quality and validity (Smith and McGannon Citation2018). In this study, the list of characterising traits that guided validity (Smith and McGannon Citation2018) included the following criteria: the worthiness of the topic; the significant contribution of the work; width – meaning the comprehensiveness of evidence from a wide sample of participants from diverse contexts, as well as multiple data and in-depth collection methods; credibility, through the iterative phased design and the co-constructed methods with young people, alongside the analytical process constructed between the researchers regarding the fairness, appropriateness and believability of the interpretations offered; and coherence, reflecting the ways in which the study’s purpose, theory, methods and results are aligned.
Results
Data from the questionnaire revealed that out of the total sample of 235 respondents, 35% of the young people currently use either an app or a wearable device that they associate with health (Questionnaires). Of the 35%, most of the young people reported using a health-related app (27%), with only a small proportion reporting that they use a health-related wearable device (9%) (Questionnaires). Only 5% reported using both a health-related app and a wearable device (Questionnaires). Yet, while the majority of young people reported that they did not currently use health-related apps and devices, the questionnaire provided evidence that many young people were aware of a vast number of health-related apps (118 different health-related apps were identified across the 235 sample of respondents) (). The interview data provided further evidence that many of the young people had previously downloaded, and/or used health-related apps and devices, indicating that variability in the current uses of these technologies was related to other factors.
I have one {Fitbit]. I haven’t used it in ages. (Interview, School 2, Male)
I have some fitness apps … Yeah had them, I don’t anymore. (Interview, School 10, Female)
I use 7 Minute Workout and I also use the Apple Health app to track steps and stuff.
I don’t really use any. I might use the Health one just to see how far I’ve gone, but not specifically for my health, just to see the distance … .
Use and delete them, mainly, because sometimes they’re not very helpful. (Interview, School 8)
The data indicated that young people would be most interested in using apps related to exercise and diet/nutrition. The questionnaire data provided evidence that young people were interested in improving their water intake (55%), calorie intake (50%), number of active minutes (49%), and sleep duration (47%) (Questionnaires). This interest was similar to data collected from the app creation task, where the health-related focus of the apps young people created was related primarily to exercise (38%) and/or had a combined focus on exercise, diet/nutrition and water intake (37%) (App Creation Task). Yet the reasons young people gave for using apps were broader than simply seeking information on a specific type of health-related behaviour (i.e., exercise or diet/nutrition). The data revealed three important features of content that young people reported had an influence on their uses of health-related apps and devices: (i) efficient and easy content; (ii) personalised content; and (iii) social content. It was apparent that engagement with such content was shaped by how the young people perceived they could use apps and devices in relation to their health, and whether they were relevant to their individual needs, situations and contexts.
Easy and efficient content
This theme refers to how young people’s engagement with health-related apps and devices was influenced by the capabilities of these technologies to deliver health-related information in ways that were quick and easy to understand and use. Easy and efficient content was mainly related to fitness/exercise apps, particularly where young people reported that they didn’t have enough time to engage with exercise and/or didn’t want to spend much money on it. For example, apps related to fitness/exercise were described as being relevant to ‘people who work out and don’t have time to go to the gym’ (Interview, School 8, Male); where, ‘instead of going like “Okay I need to go to the gym tonight”, you can just go on the app’ (Interview, School 1, Female); and ‘without buying, without spending lots of money … you can have a gym at your house’ (Interview, School 2, Male). For some young people, notification features on apps were important and sometimes necessary because they reminded them to engage with exercise. For example, a number of the apps created by young people themselves in the study included statements such as: ‘send notification to do five exercises for three minutes each’ (School 4, Group 1); ‘alarm every hour for water’ (School 5, Group 3); ‘reminders of workouts’ (School 1, Group 1); ‘tells you when to exercise … makes sure everyone exercises for one hour a day, otherwise locks your phone’ (School 9, Group 3) (App Creation Task). For some young people, their experiences of using fitness/exercise apps that included reminders and exercises that could be completed in a short duration led to the development of an understanding that apps/devices are an efficient way to engage with exercise and, in turn, lose weight and/or improve their body image.
I have a 30-day fitness app, so I have like a five-minute workout every day and basically if I can’t be bothered, it will give me a reminder on my phone. So, okay, I’m going to keep getting this reminder unless I do it, so it helps me … because knowing it’s there, like I’m going to have to do this. And I just do it. (Interview, School 1, Female)
I think for teenagers, because you’re not spending so much time on it, it’s quick and it works. So it’s easy to use, and it’s not difficult. So I think it’s just more efficient than like longer workouts. (Interview, School 3, Female)
[7-minute workout app] It’s like very intense, short amount of time to just do it. So I guess it’s kind of like for someone who doesn’t have much time for doing it, they like really want to lose weight and get like that perfect body then it’s like for them. For dedicated people, I guess.
[7-minute workout app] I think it’s more effective. It’s better for us, like people who don’t want to waste too much time on exercise. (Interview, School 5)
Fitness/exercise apps, such as the 7-minute workout, were also appealing because the information was easy to follow, and the variety of exercises was found to be engaging; ‘I like the change of every 30 seconds, I like the different changes’ (Interview, School 4, Male); ‘it’s easy to follow’ (Interview, School 6, Female). The importance of exercises that were easy to follow was further reflected in the design of apps by the young people. For example, one of the apps created was called Easy Exercise and focused on ‘motivation and inexpensive menus’ (Interview, School 1, Female), where the user of the app would ‘show workouts and gives food tips’ (App Creation Task, School 1, Group 3). This group explained that these features and the name ‘Easy Exercise’ was ‘a good selling point’ (Interview, School 1, Female). In other apps, statements that reflected easy and efficient content included: ‘Fit by Friday – exercise videos – easy to understand’ (School 10, Group 4); ‘Quick Fit’ (School 9, Group 3), ‘health at your doorstep’ (School 10, Group 1); ‘workout schedule and ideas in a short amount of time’ (School 5, Group 2) (App Creation Task).
Differences existed, however, between how the young people viewed the effectiveness of fitness/exercise apps to improve their health. Notably, the short-duration exercises were critiqued by some: ‘I don’t think you can accomplish much in seven minutes’ (Interview, School 2, Male); ‘If you only exercise for five minutes, it isn’t going to do anything, you need to exercise for a longer duration’ (Interview, School 5, Female). Other young people judged the effectiveness of fitness/exercise apps when they were able to feel some effect from the exercises: ‘I actually like the idea … I woke up and I could feel it’ (Interview, School 4, Male); ‘It hurt. I think if it hurts it works’ (Interview, School 6, Female).
Even though short-duration exercises were able to overcome time-related barriers to engagement with physical activity for some young people, others reported that they did not have sufficient time to use fitness/exercise apps and devices. School and homework pressures and/or engagement with other physical activities limited the time some young people had available:
I kind of didn’t like it … Because with exercise apps you’ve got to kind of like do it every day. And I kind of find it hard like after school and my homework, it’s kind of hard to actually find the strength to actually do the exercise. (Interview, School 3, Female)
No, I like fitness, it’s just I don’t want to go out of my way to open up an app and then do all the app search, if you want to be fit I’d rather just do a team sport. (Interview, School 2, Male)
Why don’t you use those apps?
I don’t have time
I do loads of sports so there is no need to do it. (Interview, School 6)
Health-related apps and devices provide content that is easy to understand and quick to use. These interactive features met some young people’s individual needs by providing access to health-related information that they can engage with in a time-efficient manner. Other young people critiqued health-related apps, suggesting that easy and efficient content would have limited effects on their health. For some young people, school and engagement with sports teams limited their time or inclination to use digital health technologies.
Personalised content
This theme refers to how young people’s engagement with health-related apps and devices was influenced by whether the young people perceived that the health-related information could improve their health-related behaviours. For example,
So why do you use apps – health and wellbeing apps?
To test yourself
To lose some weight, because we’re going through that stage, we need to lose more weight …
Get fit, isn’t it? …
To live longer
To be like healthy on the inside as well. (Interview 1, School 7)
I’ve had the 7-Minute one before …
Why did you decide to download those apps
To scale up my stamina
Felt like I needed to tone up and to strengthen my muscles …
I just wanted to look nice to be honest … toned. (Interview 2, School 10)
Tracking, monitoring and recording features of apps were important to young people. In many of the apps created by the participants, positive student statements included: ‘tracks how much you walk’ (School 9, Group 2); ‘tracks calorie intake and distance travelled’ (School 7, Group 3) (App Creation Task). The interview data reinforced the point:
When you start becoming a teenager, that’s when like sleep is … You don’t really have much of a schedule, you’re kind of like going to bed really late and you don’t have as much sleep as you need. So I think using those apps would be helpful. (Interview, School 3, Female)
I’ve got one it’s called Pacer … it tracks how many steps you do … and how many calories you’ve lost
I use one, 30-day fitness
What do you have to do?
Cardiovascular … push-ups, everything … it’s like a morning routine … like get up eat, have your breakfast and go for jogs. (Interview, School 7)
Although health-related apps helped some young people to regulate their health-related behaviours, others reported that they did not require an app or device to manage or improve their health. For example, where young people reported being satisfied with their health-related activities, knowledge and understanding – often through school – apps and devices were not considered a useful additional source of information:
I think it’s for people that something’s happened, so they’re not healthy. I think I’m healthy enough so I don’t need them at all …
I mean personally I don’t need them, there’s no need for them. So what’s the point in getting them. I am already healthy, and I sleep well, so I don’t think that I need them … you can exercise whenever you want, so there’s no point to having it. If I want to exercise I’ll just exercise for seven minutes, what’s the point in having an app taking all that storage. (Interview, School 3)
We don’t really have to manage it as much ourselves, because we get healthy lunches at school, and PE and games and things …
Like in PE sessions you know how to workout, or if you go to the gym … just like how to do sit ups and press ups. (Interview, School 2)
It was also reported that many health-related apps failed to provide health-related information that was personalised. Health-related apps were critiqued for the absence of health-related information that was specific to the age-related needs of young people and/or the shortage of health-related information that was tailored to their individual bodies and/or choices. Some young people were also aware that the use of generic health-related information, that was often targeted at adult populations, could lead to harmful effects on their bodies.
Health and wellbeing apps are very broad, and they’re meant to cover a lot of different people. Children are a lot different from adults. (Interview, School 1, Female)
People want to do different workouts. You might want to work on your arms and you want to do a specific workout because you know that that’s your weak point … if you can’t personalise it, it becomes a lot harder to do because you’re just going through a big list of things to find a workout that has it in.
And I think it feels nice to have your part in what your workout is, rather than being told what to do. It might be a feel a bit boring. (Interview, School 8)
You just do workouts that it’s telling you to do [7-minute workout]. It’s not based around what you want or you need. (Interview, School 5, Male)
Like if there’s one app that’s targeted for all the ages that uses weights or something like that and since you’re still growing, it might mess you up in that kind of sense. (Interview, School 5, Male)
The importance of access to personalised health information was further reflected in young people’s discussions about the design of apps. In many of the apps created by young people, explanatory statements for users referred to: ‘workout depends on age and suited to abilities’ (School 5, Group 2); ‘personalised goals’ (School 2, Group 3), or ‘personalised fitness’ (School 1, Group 2) (App Creation Task). The interest in accessing information specifically tailored to ‘improving’ an individual’s body was also evident. For example, the ‘Instabod’ app designed by one group was based around the idea to ‘choose an ideal body shape and the app tailors a programme’ (School 8, Group 2, App Creation Task). This app was described to work by the user ‘upload[ing] an image of current body and desired body’ and the app would then ‘recommend workouts/diets’ (School 8, Group 2, App Creation Task). This individual improvement interest was also reflected in explanatory statements for potential users about the design of apps the young people created. Examples include: ‘workout videos to help loose or gain weight’ (School 10, Group 3); and ‘list of body options you can target’ (School 8, Group 4) (App Creation Task). The data from the interviews reinforced these points. Health-related content that was focused on improvement and included progressive exercises and workouts was found to be influential. There was also a clear indication that young people wanted to be able to customise the health-related information that they could access and use.
Have an app that’s more specialized for children or like teenagers that are wanting to work out, because a lot of them are aimed at adults. (Interview, School 1, Female)
You should put your age down and then it does things around your age, not things that other people should be doing who are older than you. (Interview, School 5, Male)
We asked you to create your own app, do you remember what you did?
It’s for stages. It started off as just simple workouts. It was ‘WorkOUTS’ and then the next one was ‘Workout Pal’. You could choose your own workout …
Customise your workout and it would survey hills in your local area. You could match and where stuff is. So whether you’d want to go around, you could do that, or if you didn’t mind doing hills so you can plan running routes as well. (Interview, School 8)
In summary, the health-related apps and devices were used by young people if the content met their perceived personal health-related needs. For some, their health was sufficiently supported in the contexts of school and/or PE, and apps were disregarded as useful health-related learning resources. There was also evidence that young people drew on their prior knowledge to judge whether the health-related information available on health-related apps and devices was personalised and, in particular, if it was specific to their age and/or tailored to their individual bodies and choices. In addition, there was a level of disappointment evident in the data where these digital health technologies appeared to promise much but could not deliver.
Social content
This theme demonstrates that young people compared their uses of health-related apps and devices to their peers and family members’ uses of these technologies. The data showed that peers and family members influenced young people to use apps and devices through promoting understandings that they were ‘cool’ (Male 1), ‘in trend’ (Male 2) (Interview, School 2), and/or ‘popular’ (Interview, School 3, Female). There was also evidence that health apps and were ‘recommended’ by peers of family members (Interview, School 10, Female).
Peers’ uses of and recommendations for health-related apps and devices were an important and interpersonal source of evaluative information for young people: ‘if you know people who always use it, you can ask them about it, they always like recommend apps you should use’ (Interview, School 7, Male). ‘I used it [Pokemon Go- exercise game app], like when everyone was using it’ (Interview, School 5, Male); ‘I just don’t need it, none of my friends have it so it doesn’t have a purpose’ (Interview, School 8, Male). Some of the young people used health-related apps to engage with physical activities and/or diets with their peers, and there was evidence that this provided a valued form of support and motivation. Yet there was also evidence that peers did not have a sustained influence on young people’s interest in health-related apps, with many reporting that they discontinued using apps after a period of time. The lack of perceived influence of peers on the longer-term uses of apps was also apparent in the apps created by young people. The data indicated that none of the apps created by young people included social features (e.g., sharing information, chat features) and/or any reference to peers or family members.
Me and my friend had it [Pokemon Go app – exercise game app] and we did it and we would go out and do it … then it got boring. (Interview, School 6, Female)
My friend wanted to do it first, because she wants to lose weight [diet app]. So I thought I’d be a nice friend and join with her because I’m very nice I started doing it. (Interview, School 5, female)
We had like a stage where we would like fully workout all the time, and we’d text each other like, ‘Okay, we need to workout now … ’. And stuff like that, and then it just kind of failed … You think honestly I can’t be bothered and then you delete it [abb workout app]. (Interview, School 5, Male)
Despite limited evidence of sociability in the apps created by young people, for some participants, family members were powerful influencers on the health-related apps and devices they were aware of and used. Parents, older siblings, aunts or uncles, and grandparents were reported to own and use health-related apps and/or devices: ‘My Dad has UnderArmour, MyFitness Pal’ (Female) … ‘My Dad uses Fitbit … and my Mum uses 7 Minute-workout’ (Male) (Interview, School 5). In turn, some young people considered that these technologies were relevant and effective, and could be used to improve their health:
I followed it [Fitbit device and app] off my brothers because they go to the gym and all that, so I thought I might as well do something that contributes to my wellbeing. (Interview, School 5, Male)
My uncle uses it [7-minute workout app] sometimes because he always goes jogging in the morning; he’s quite a healthy guy. And I saw him using it, so I said it’s quick and it’s reliable so why not try it. And then we tried it and it helps, so we use it every time. (Interview; School 3)
How did you hear about the squat app?
My nan. My nan just found it on Facebook
Why did you decide to do the squat one?
To get a bigger bum. (Interview, School 6)
I use stuff that’s simply called Virtual gym because my family are very like sports interested. We do a lot of like sports and like fitness and it basically shows you how to do different exercises step by step and it targets different parts of your body so like your core, your legs, your obliques, like that sort of stuff. So that’s what I use. (Interview, School 9, Female)
There was evidence that the uses of health-related apps and devices by family members motivated young people to engage with physical activity. It was also apparent in the data that parents encouraged and purchased health-related apps and/or devices for their children. Health-related apps and devices, in some instances, were a source of health-related data used to communicate weight loss or sleep pattern to parents.
When it gets nearer the end of the day, it has like goals and you can go against each other on it. So like my nan has one and my mum has one [Fitbit device and app]. So we’ll all go against each other and it will just motivate you to try to beat each other. (Interview, School 1, Female)
When I left year six I realised that I was getting fat, and so I was thinking, ‘Oh gosh, I’m actually getting big’. So my dad bought me like a Fitbit watch, a surge one. And then it helps me like … The more steps you do, the more healthy you get. (Interview, School 4, Male)
Mine [Fitbit device and app] helped me feed back to my parents about how I’m going when I’m sleeping, because I used to go to bed at 4:00 in the morning and wake up at 6:00. Now it’s like 1:00 and 6:00 and it’s slowly getting better. It helped my parents understand how many hours I’m getting and what I need to be getting. (Interview, School 1, Female)
Health-related apps and devices were used by young people if the content was considered to be socially relevant. Young people drew on their peers’ and family members’ uses to make judgements about whether and how to use health-related apps and devices. If health-related apps and devices were used and encouraged by peers and/or family members, then many young people were prepared to join in with or try out digital health technologies. Here again, however, there is clear evidence of young people’s agency in the decision-making process.
Discussion
This study provides new evidence on the types of health-related apps and devices young people find, select and use, and the reasons for their choices. New evidence is provided on: (i) the types of health-related information young people access and attend to; and (ii) and the variance in the ways in which young people report the influence of health-related apps and devices on their behaviours. The data present challenges to the dominant risk-related narratives that surround young people’s uses of digital technologies (Fullagar, Rich, and Francombe-Webb Citation2017; Rich and Miah Citation2017), by providing further evidence (see Goodyear, Kerner, and Quennerstedt Citation2017; Goodyear, Armour, and Wood Citation2018) that young people are critical users. There was evidence that young people find, select and use health-related apps and devices that are perceived as meeting health-related needs at specific moments in time. Yet, the health-related apps and devices available to young people clearly failed to cater for all their perceived needs and/or interests given that the data showed that only one-third of young people were active users of apps and devices related to exercise, diet and wellness. Moreover, many young people were apparently able to disregard content they regarded as irrelevant, and/or potentially harmful to their bodies, and/or just ‘boring’ to use over time. While in policy and practice it is often assumed that health-related apps and devices will be engaging and attractive to young people (Goodyear, Kerner, and Quennerstedt Citation2017), the findings of this study suggest that similar to other technologies and the internet (see Fors and Pink Citation2017; Livingstone and Third Citation2017), health-related apps and devices are largely viewed by young people as an adult resource. Clear evidence is therefore provided from this study on the need to ‘rethink’ deterministic viewpoints of ‘positive’ and ‘negative’ effects and acknowledge that many young people are critical participants of digital health technologies who are able to judge the relevance of information to their age and their bodies, and navigate inappropriate content.
In contrast to most existing evidence (Goodyear, Kerner, and Quennerstedt Citation2017; Depper and Howe Citation2017), the findings demonstrate that potentially positive and negative health-related impacts do not stem solely from access to unregulated content, and/or regulatory and disciplinary practices of digital health technologies. It was evident that young people’s health-related needs, understandings and behaviours vary over time, and that engagement in schools, PE lessons and sport, and with family members and peers, are also powerful influencers. This finding is consistent with those of a number of scholars researching digital health technologies (Albury Citation2013; Fullagar, Rich, and Francombe-Webb Citation2017; Lupton Citation2018), and draws further attention to the importance of concepts such as embodiment and relationality (Rich and Miah Citation2017). The findings further emphasise that the uses of digital technologies are shaped by and shape relations with other discourses, bodies, sites and pedagogies (Albury Citation2013; Rich and Miah Citation2014). Similar to Albury’s (Citation2013) accounts of young people’s engagement with digitalised sexual health information, the evidence from this study suggests that apps and devices are highly accessible and they have the advantage of offering ‘private’ spaces in which to engage with health-related practices, particularly where young people find communal activity spaces intimidating. In particular, these digital health technologies can appear to be highly relevant when curiosity about health-related apps and devices is aligned with a growing personal and peer-group interest in the body. For all these reasons, health-related apps and devices offer something potentially valuable to some young people who are curious and keen to learn about themselves.
Looking across the data, it can be argued that digital health technologies should be understood as an important component of the broader and more complex landscapes of different pedagogical sites of learning. There was evidence, for example, of apps and devices being used enthusiastically by family members and also data sharing between them to generate competition and motivation. Yet, other young people rejected the technologies because they felt they had better opportunities for learning and engagement in, for example, school PE, while others tried the technologies because they were popular with peers – but soon rejected them when they were found wanting. What seems clear from the data is that young people’s needs for information and engagement change across time, place and transient perceptions of need. Indeed, similar to adults’ uses of food tracking apps (Lupton Citation2018), the technology (i.e., apps) and the human (i.e., young person) work together to generate affective forces and agential capabilities, that are continuously made and reconfigured over time. Furthermore, and as argued by Fullagar, Rich, and Francombe-Webb (Citation2017, 99) ‘neither the users, nor the technologies themselves can be considered to have particular attributes, but rather they are thought together in terms of emerging capabilities which are shaped by a pedagogical orientation’. The key advantage of such entanglements, affective arrangements (Fullagar, Rich, and Francombe-Webb Citation2017) and the mobility of apps and devices (Albury Citation2013) is that, unlike more passive forms of information, young people find that these apps and devices can help them to translate knowledge into personalised action at specific points in time, when it becomes ‘needed’ and without the requirement for an adult instructor.
To interpret learning as seen in the data in this research, the content-led pedagogical framework adopted was informed by pedagogical, anthropological and communication theories (see Goodyear, Armour, and Wood Citation2018). This framework directed attention toward what young people do in their engagement with digital health technologies. Indeed, as noted earlier, a focus on content provided a distinctive focus on pedagogy that enabled us to consider affordances (Lupton Citation2017) in relation to pedagogy. In particular, the framework provided a way to interpret the digital data assemblages (which bring together humans-devices-software-data-space-time) (Lupton Citation2017) that shape and frame engagement, knowledge, and behaviours. For example, the framework foregrounded a focus on how the functionalities of technology (e.g., short duration, simplicity) interacted with user needs (e.g., lack of time due to school, body image), to form particular ways of using technologies (e.g., information seeking, self-improvement) that led to the creation of different forms of content (e.g., easy and efficient content, personalised content). Based on the data from this study and our earlier research on social media (see Goodyear, Armour, and Wood Citation2018), we argue that in self-educated technology-based environments, content plays a leading role in any understanding of pedagogy. In turn, that content is formed from the interplay between key technological features (that offer teaching potentials) and how users interact with the technology (learner needs/potentials).
Further evidence for the importance of a focus on content is provided by the new insights that were generated into young people’s learning and agency in digital/online contexts, where their capabilities to think and act were captured. What the data illustrated, vividly, was the complexity and fluidity of young people’s decision-making around the use of health-related apps and devices. Moreover, some young people had developed very high levels of knowledge, understanding and discriminatory skills in this space. In some cases, motivation to engage with health-related knowledge or behaviours linked to apps or devices led to a process of trial and error where young people adopted, adapted and/or dismissed these technologies. Indeed, it was apparent across the data set that interest in apps and devices was often not sustained. Similar to previous research on wearable devices (Goodyear, Kerner, and Quennerstedt Citation2017), a novelty period exists and it seems likely that this lack of sustained engagement is, in part, down to the design of the technologies and their focus on adults’ needs (Livingstone and Third Citation2017). These findings further emphasise the importance of adding an analytical focus on content to those insights that already exist (e.g., Albury Citation2013; Rich and Miah Citation2014; Fors and Pink Citation2017; Lupton Citation2017, Citation2018), in order to generate pedagogically informed understandings about digital health technologies. Extending previous research in this field, a focus on content provides insights into not only agential capabilities, affective forces, and relationality (Lupton Citation2018), but also new and nuanced understandings of the cognitive elements that are operating in users’ assessments of health apps. In this study, there was evidence that in some cases, far from receiving information passively or being manipulated, young people were thinking through their uses of health-related apps in impressive and well-informed ways.
Based on the data generated, a key message for relevant adults is that they are likely to be more effective in supporting young people to use the available technologies effectively and positively if they acknowledge and work with young people’s agency. A focus on agency provides relevant adults with a way of framing and supporting the affective and cognitive elements that were found to influence young people’s critical skills and their orientation toward different forms of health-related content. At the same time, the data suggest that relevant adults may require professional support and appropriate forms of health education themselves in order to develop and promote young people’s agency. There was evidence, for example, that schools and family members both constrain and enable to the development of appropriate health-related knowledge and behaviours.
Methodologically, this study has contributed to a developing evidence-base on the importance of understanding young people’s experiences of and perspectives on digital health technologies (Third et al. Citation2017; Goodyear, Kerner, and Quennerstedt Citation2017; Goodyear, Armour, and Wood Citation2018). The paper has reported participatory methods that were constructed with young people that can be used in future research to generate valuable insights into how adults can better support young people’s learning. Conceptually, and consistent with Miller et al. (Citation2016), the data from this study show the value of applying a content-led pedagogical framework to add to the insights that already exist. A content-led framework that was developed in the context of social media was applied to the contexts of apps and wearable devices, where some consistencies in the forms of content young people access and attend to were apparent (see Goodyear, Armour, and Wood Citation2018). Given the sheer pace of technological advancement, a content-led conceptual framework can endure through changes to specific technologies and be used to capture data on user experiences across a range of digital health-related platforms and software (Miller et al. Citation2016). It is also important to recognise the limitations of this study. Even though the study design included a range of different methods and iterative phases of data collection and analysis, the bulk of the evidence comprises of young people’s retrospective reporting of views and experiences of how digital content influenced their health-related understandings and behaviours. Future research should seek to explore young people’s situated, real-time experiences with and of digital health-related technologies to further understand the operation of pedagogy in digital health-related contexts, and particularly the wide range of informed participatory behaviours.
Conclusion
Digital health technologies are, potentially, a valuable source of learning for young people and the data suggest that they can have important impacts on health-related knowledge and behaviours. The digital health landscape is expanding at an unprecedented rate, making the need for adults to provide support for young people both necessary and important. By focusing on agency, and working alongside young people, relevant adults can help young people to better manage their engagement with digital health technologies. Agency involves ensuring that young people have access to appropriate forms of health education and opportunities to critically examine their subjective feelings about their health and their bodies. Schools, PE lessons and sport, as well as family members and peers, are powerful contexts where such forms of agency education can be optimised. In all these contexts, the development of effective pedagogies can be enhanced by learning lessons from the ways in which young people access, select and use digital health technologies. In other words, the ways in which young people use digital technologies to inform their own health-related learning should inform the ways in which we frame pedagogy as a concept.
Disclosure statement
No potential conflict of interest was reported by the authors.
Notes on contributors
Dr Victoria A. Goodyear is a Lecturer in Pedagogy in the School of Sport, Exercise and Rehabilitation Sciences, University of Birmingham, UK. Victoria’s research focuses on understanding and enhancing young people’s health and wellbeing through research on pedagogy and digital technologies. Her work utilises participatory digital methods and digital ethical procedures. Victoria’s research has been supported by research councils, trusts and industry, and she has published in pedagogy, education and qualitative research journals. Victoria has given keynotes and invited talks in numerous countries around the world, as well as communicating her research to policy and the media. Victoria serves on the editorial boards for a number of leading journals in the field. Victoria can be found on Twitter: @VGoodyear and an example of her research can be accessed at http://opencpd.net/Guidelines.html.
Professor Kathleen M. Armour was formerly Head of the School of Sport, Exercise and Rehabilitation and is now Pro-Vice Chancellor Education. Kathleen’s research is in education and in career-long professional learning, and she is particularly interested in bridging the gaps between theory/research and practice. Kathleen has received over £2.5 million of research funding from research councils, charities and industries and she is Co-I on the Goodyear projects focused on apps and social media. In her most recent books, Kathleen has developed a new translational mechanism – ‘pedagogical cases’ – to support practitioner learning. This mechanism was recently applied to digital technologies to offer fresh insights into young people’s learning. Alongside publishing widely in the field, Kathleen was a REF2014 panelist, is a Fellow of the Academy of Social Sciences and is International Fellow of the National Academy of Kinesiology.
Hannah Wood worked as a Research Associate at the University of Birmingham in the School of Sport, Exercise and Rehabilitation Sciences. Hannah’s research background is diverse, having begun her career working in sport policy before moving into the area of pedagogy, young people, health and digital technologies. Hannah now works for The Active Wellbeing Society as an Insight Analyst on the Active Communities project.
ORCID
Victoria A. Goodyear http://orcid.org/0000-0001-5045-8157
Kathleen M. Armour http://orcid.org/0000-0002-1430-7420
Hannah Wood http://orcid.org/0000-0001-8219-0546
Additional information
Funding
Notes
1 For an overview of the characteristics of different types of schools in the UK please see https://www.gov.uk/types-of-school.
Related Research Data
References
- Albury, K. 2013. “Young People, Media and Sexual Learning: Rethinking Representation.” Sex Education 13 (1): S32–S44. doi: 10.1080/14681811.2013.767194
- Andersson, E., and J. Öhman. 2017. “Young People’s Conversations About Environmental and Sustainability Issues in Social Media.” Environmental Education Research 23: 465–485. doi: 10.1080/13504622.2016.1149551
- Andersson, E., and M. Olson. 2014. “Political Participation as Public Pedagogy – The Educational Situation in Young People’s Political Conversations in Social Media.” Journal of Social Science Education 13: 115–126.
- Armour, K. M. 2014. Pedagogical Cases in Physical Education and Youth Sport. London: Routledge.
- Bakker, D., N. Kazantzis, D. Rickwood, and N. Rickard. 2016. “Mental Health Smartphone Apps: Review and Evidence-Based Recommendations for Future Developments.” JMIR Mental Health 3 (1): e7. doi: 10.2196/mental.4984
- Beckman, K., S. Bennett, and L. Lockyer. 2014. ““Understanding Students’ Use and Value of Technology for Learning.” Learning, Media and Technology 39 (3): 346–367. doi: 10.1080/17439884.2013.878353
- Bevelander, K. E., C. R. Smit, T. J. van Woudenberg, L. Buijs, W. J. Burk, and M. Buijzen. 2018. “Youth’s Social Network Structures and Peer Influences: Study Protocal MyMovez Project – Phase 1.” BMC Public Health 18: 504. doi: 10.1186/s12889-018-5353-5
- boyd, d. 2014. It’s Complicated: The Social Lives of Networked Teens. London: Yale University Press.
- Burdick, J., and J. A. Sandlin. 2013. “Learning, Becoming, and the Unknowable: Conceptualizations, Mechanisms and Processes in Public Pedagogy Literature.” Curriculum Inquiry 43: 142–177. doi: 10.1111/curi.12001
- Couldry, N. 2012. Media, Society, World: Social Theory and Digital Media Practice. Cambridge: Polity.
- Depper, A., and P. D. Howe. 2017. “Are We Fit Yet? English Adolescent Girls’ Experiences of Health and Fitness Apps.” Health Sociology Review 26 (1): 98–112. doi: 10.1080/14461242.2016.1196599
- Fors, V., and S. Pink. 2017. “Pedagogy as Possibility: Health Interventions as Digital Openness.” Social Sciences 6: 59. doi: 10.3390/socsci6020059
- Fox, N. J., and C. Bale. 2017. “Bodies, Pornography and the Circumscription of Sexuality: A New Materialist Study of Young People's Sexual Practices.” Sexualities. 1–17.
- Freishtat, R. L., and J. A. Sandlin. 2010. “Shaping Youth Discourse About Technology: Technological Colonization, Manifest Destiny, and the Frontier Myth in Facebook’s Public Pedagogy.” Educational Studies 46 (5): 503–523. doi: 10.1080/00131946.2010.510408
- Fullagar, S., E. Rich, and J. Francombe-Webb. 2017. “New Kinds of (Ab)normal?: Public Pedagogies, Affect, and Youth Mental Health in a Digital Age.” Social Sciences 6 (3): 99. doi: 10.3390/socsci6030099
- Gardner, H., and K. Davis. 2014. The App Generation. London: Yale University Press.
- Giroux, H. A. 2004. “Public Pedagogy and the Politics of Neo-Liberalism: Making the Political More Pedagogical.” Policy Futures in Education 2: 494–503. doi: 10.2304/pfie.2004.2.3.5
- Goodyear, V. A. 2017. “Social Media, Apps, and Wearable Technologies: Navigating Ethical Dilemmas and Procedures.” Qualitative Research in Sport, Exercise and Health 9 (3): 285–302. doi: 10.1080/2159676X.2017.1303790
- Goodyear, V. A., K. M. Armour, and H. Wood. 2018. “Young People and Their Engagement with Health-related Social Media: New Perspectives.” Sport, Education and Society. 1–16. doi: 10.1080/13573322.2017.1423464
- Goodyear, V. A., C. Kerner, and M. Quennerstedt. 2017. “Young People's Uses of Wearable Healthy Lifestyle Technologies; Surveillance, Self-surveillance and Resistance.” Sport, Education and Society. 1–14.
- Hillman, T., and R. Säljö. 2016. “Learning, Knowing and Opportunities for Participation: Technologies and Communicative Practices.” Learning, Media and Technology 41 (2): 306–309. doi: 10.1080/17439884.2016.1167080
- Holmberg, C., C. Berg, J. Dahlgreen, L. Lissner, and J. E. Chaplin. 2018. “Health Literacy in a Complex Digital Media Landscape: Pediatric Obesity Patients’ Experiences with Online Weight, Food, and Health Information.” Health Informatics Journal.
- Ito, M., S. Baumer, M. Bittanti, d. boyd, R. Cody, B. H. Stephenson, and H. A. Horst. 2010. Hanging Out, Messing Around, and Geeking Out: Kids Living and Learning with New Media. Cambridge, MT: MIT Press.
- Livingstone, S., and A. Third. 2017. “Children and Young People’s Rights in the Digital Age: An Emerging Agenda.” New Media & Society 19 (5): 657–670. doi: 10.1177/1461444816686318
- Lomborg, S. 2017. Social Media, Social Genres. London: Routledge.
- Lomborg, S., and K. Frandsen. 2016. “Self-tracking as Communication.” Information, Communication and Society 19 (7): 1015–1027. doi: 10.1080/1369118X.2015.1067710
- Lupton, D. 2017. “Lively Data, Social Fitness and Biovalue: The Intersections of Health Self-Tracking and Social Media.” In The Sage Handbook of Social Media, edited by J. Burgess, A. Marwick, and T. Poell, 562–578. London: Sage.
- Lupton, D. 2018. “‘I Just Want it to be Done, Done, Done!’ Food Tracking Apps, Affects and Agential Capacities.” Multimodal Technologies and Interaction 29 (2): 1–15.
- McKee, A., K. Albury, J. Burgess, B. Light, K. Osman, and A. Walsh. 2018. “Locked Down Apps Versus the Social Media Ecology: Why Do Young People and Educators Disagree on the Best Delivery Platform for Digital Sexual Health Entertainment Education?” New Media & Society. 1–19.
- Miller, D., E. Costa, N. Haynes, T. McDonald, R. Nicolescu, et al. 2016. How the World Changed Social Media. London: UCL Press.
- Ofcom. 2017. Children and Parents: Media Use and Attitudes Report. https://www.ofcom.org.uk/__data/assets/pdf_file/0020/108182/children-parents-media-use-attitudes-2017.pdf
- Radovic, A., C. A. McCarty, K. Katzman, and L. P. Richardson. 2018. “Adolescents’ Perspectives on Using Technology for Health: Qualitative Study.” JMIR Pediatrics and Parenting 1 (1): e2. doi: 10.2196/pediatrics.8677
- Reid, A. 2010. “Social Media, Public Pedagogy and the End of Private Learning.” In Handbook of Public Pedagogy, edited by J. A. Sandlin, B. D. Shultz, and J. Burdick, 194–200. London: Routledge.
- Rettberg, J. W. 2014. Seeing Ourselves Through Technology: How We Use Selfies, Blogs and Wearable Devices to See and Shape Ourselves. New York, NY: Palgrave Mamillian.
- Rich, E., and A. Miah. 2014. “Understanding Digital Health as Public Pedagogy: A Critical Framework.” Societies 4 (2): 296–315. doi: 10.3390/soc4020296
- Rich, E., and A. Miah. 2017. “Mobile, Wearable and Ingestible Health Technologies: Towards a Critical Research Agenda.” Health Sociology Review 26 (1): 84–97. doi: 10.1080/14461242.2016.1211486
- Robinson, K. H., P. Bansel, N. Denson, G. Ovenden, and C. Davies. 2014. Growing Up Queer: Issues Facing Young Australians Who Are Gender Variant and Sexuality Diverse. Melbourne: Young and Well Cooperative Research Centre.
- Savage, G. C. 2014. “Chasing the Phantoms of Public Pedagogy: Political, Popular and Concrete Publics.” In Problematizing Public Pedagogy, edited by J. Burdick, J. A. Sandlin, and M. P. O’Malley, 79–90. London: Routledge.
- Smith, B., and K. R. McGannon. 2018. “Developing Rigor in Qualitative Research: Problems and Opportunities Within Sport and Exercise Psychology.” International Review of Sport and Exercise Psychology 11 (1): 101–121. doi: 10.1080/1750984X.2017.1317357
- Sparkes, A., and B. Smith. 2014. “Ethical Issues in Qualitative Research.” In Qualitative Research Methods in Sport, Exercise and Health: From Process to Product, edited by A. Sparkes, and B. Smith, 206–237. London: Routledge.
- Third, A., D. Bellerose, U. Dawkins, E. Keltie, and K. Pihl. 2014. Children’s Rights in the Digital Age: A Download From Children Around the World. Melbourne: Young and Well Cooperative Research Centre.
- Third, A., D. Bellerose, J. D. D. Oliveira, G. Lala, and G. Theakstone. 2017. Young and Online: Children’s Perspectives on Life in the Digital age. Sydney: Western Sydney University.
- Wartella, E., V. Rideout, H. Montague, L. Beaudoin-Ryan, and A. Lauricella. 2016. “Teens, Health, and Technology: A National Survey.” Media and Communications 4 (3): 12–23. doi: 10.17645/mac.v4i3.515
- Williamson, B. 2015. “Algorithmic Skin: Health-Tracking Technologies, Personal Analytics and the Biopedagogies of Digitized Health and Physical Education.” Sport, Education and Society 20 (1): 133–151. doi: 10.1080/13573322.2014.962494